Back to Journals » Cancer Management and Research » Volume 18

Efficacy and Safety of Nanoparticle Albumin-Bound Paclitaxel Compared to Docetaxel Plus Nedaplatin as Induction Chemotherapy for Locally Advanced Nasopharyngeal Carcinoma: A Propensity Score Matching Analysis
Authors Sun QQ, Chen J, Ye ZM ![]() , Hua YH, Liu LY, Liu T
, Hua YH, Liu LY, Liu T
Received 27 November 2025
Accepted for publication 27 February 2026
Published 10 March 2026 Volume 2026:18 578665
DOI https://doi.org/10.2147/CMAR.S578665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Quan-Quan Sun,1,2 Jing Chen,1,2 Zhi-Min Ye,1,2 Yong-Hong Hua,1,2 Lu-Ying Liu,1,2 Tongxin Liu1,2
1Department of Radiation Oncology, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Hangzhou Institute of Medicine (HIM), Chinese Academy of Science, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Tongxin Liu, Department of Radiation Oncology, Zhejiang Cancer Hospital, NO.1, EAST Banshan Road, Hangzhou, Zhejiang, 310022, People’s Republic of China, Email [email protected]
Purpose: This study aimed to compare the long-term efficacy and safety of nanoparticle albumin-bound paclitaxel plus nedaplatin (NP) versus docetaxel plus nedaplatin (TP) as induction chemotherapy (IC) for locally advanced nasopharyngeal carcinoma (LA NPC).
Methods: In this retrospective analysis, treatment-naïve patients with stage III–IVa NPC who received IC with either NP or TP regimen between December 2018 and January 2021 were enrolled. Propensity score matching (PSM) was applied to balance baseline characteristics, resulting in 70 matched pairs. Efficacy endpoints included overall survival (OS), locoregional relapse-free survival (LRFS), and distant metastasis-free survival (DMFS). Treatment-related adverse events (AEs) were graded per CTCAE v5.0.
Results: After a median follow-up of 68.6 months, the 5-year OS (89.98% vs 86.98%, P=0.610), LRFS (94.06% vs 96.69%, P=0.424), and DMFS (91.33% vs 85.61%, P=0.308) rates were comparable between the NP and TP groups. Multivariable analysis confirmed that the treatment regimen was not an independent prognostic factor. The toxicity profiles, however, differed significantly. The TP group had a higher incidence of any-grade neutropenia (68.6% vs 50.0%, P=0.047), while the NP group was associated with more frequent any-grade peripheral sensory neuropathy (57.1% vs 0.0%, P< 0.001) and myalgia (45.7% vs 1.4%, P< 0.001). The rates of severe (grade 3– 4) hematological toxicities were similar between the groups.
Conclusion: The NP regimen demonstrated comparable long-term survival outcomes to the TP regimen as IC for LA NPC, with a distinct toxicity profile. NP may serve as a valuable alternative, offering a favorable hematological toxicity profile and eliminating the need for corticosteroid premedication, albeit with a higher incidence of low-grade neurotoxicity and myalgia.
Keywords: nasopharyngeal carcinoma, neoadjuvant chemotherapy, concurrent chemoradiotherapy
Introduction
Nasopharyngeal carcinoma (NPC), a malignancy arising from the nasopharyngeal epithelium, exhibits a strong etiological association with Epstein-Barr virus (EBV) infection and demonstrates a geographically skewed incidence, with endemic prevalence in Southeast Asia and southern China.1,2 Evidence has demonstrated that both plasma EBV DNA and anti-EBV serum antibodies serve as effective biomarkers for the early detection of NPC.3 Given its unique anatomical constraints and inherent radiosensitivity, radiotherapy serves as the cornerstone therapeutic modality for NPC patients.4,5 A meta-analysis of 12 randomized trials (n=4856) established that concurrent chemoradiotherapy (CCRT) confers a 6.2% absolute survival benefit at 5 years compared to radiotherapy alone in locally advanced NPC (LA NPC).6 Nevertheless, the incremental benefits of incorporating induction chemotherapy (IC) or adjuvant chemotherapy into CCRT remain contentious.
IC is hypothesized to confer distinct pathophysiological advantages over adjuvant approaches, including tumor volume reduction, eradication of occult micrometastases, and superior tolerability profiles.7 Contemporary Phase III multicenter trials have validated the clinical efficacy of IC regimens incorporating TPF (cisplatin 75 mg/m2 d1, fluorouracil 750 mg/m2/d d1–5, docetaxel 75 mg/m2 d1, q3w), PF (cisplatin 100 mg/m2 d1, fluorouracil 1000 mg/m2/ d d1–5, q3w) or GP (gemcitabine 1000 mg/m2 d1,8, cisplatin 80 mg/m2 d1, q3w) when combined with CCRT, demonstrating significant improvements in 3-year overall survival (OS), progression-free survival (PFS), and distant metastasis-free survival (DMFS).7–10 Notably, a trial by Wang et al established non-inferiority of TP regimen versus TPF regimen in 3-year failure-free survival (80.3% vs 82.1%, p<0.001 for non-inferiority), while significantly reducing grade ≥3 hematological toxicities (neutropenia: 28.3% vs 41.7%; anemia: 6.2% vs 13.4%) and treatment-related diarrhea (2.1% vs 9.8%).11 Consequently, the TP regimen has emerged as a recommended IC option for NPC, particularly in patients with compromised hematological reserve.
Cisplatin-based chemotherapy remains the cornerstone therapeutic regimen for LA NPC.7,12,13 However, its clinical utility is substantially limited by cumulative toxicities, with gastrointestinal reactions, nephrotoxicity, neurotoxicity and ototoxicity. These toxicities consistently result in suboptimal treatment adherence and contraindicate use in patients with pre-existing renal insufficiency.14,15 Nedaplatin, a second-generation platinum analog featuring a cyclobutane-1,1-dicarboxylate ligand substitution, demonstrates distinct pharmacodynamic properties. Compared to cisplatin, its modified molecular structure reduces non-specific DNA adduct formation and renal tubular uptake, translating to lower incidence of gastrointestinal toxicity, nephrotoxicity risk and ototoxicity.16 Furthermore, our previous research, alongside other studies, has firmly established the therapeutic non-inferiority of nedaplatin compared to cisplatin in treating NPC.17,18 This evidence supports nedaplatin as an effective alternative of cisplatin.
Docetaxel, a semi-synthetic taxoid derivative, exhibits pronounced hydrophobicity, necessitating formulation with pharmaceutically active solubilizing agents- polysorbate 80 and dehydrated ethanol. These agents, while facilitating its delivery, are pharmacokinetically active and can lead to numerous adverse effects.19 Consequently, patients often require pre-treatment with corticosteroids over several days to mitigate severe allergic reactions and fluid retention associated with the docetaxel solvent. Nanoparticle albumin-bound paclitaxel (nab-paclitaxel) represents a unique, solvent-free protein formulation where paclitaxel is bound to albumin.20,21 This innovative approach leverages the inherent biological properties of albumin to significantly enhance the concentration and retention of paclitaxel within tumor tissues.22,23 It achieves this through a process involving albumin-binding glycoprotein (GP60)-mediated transmembrane transport across endothelial cells and the secreted protein acidic and rich in cysteine (SPARC) pathway.24 Therefore, nab-paclitaxel offers several advantages, including the elimination of the need for pre-treatment with corticosteroids or antihistamines, a shorter intravenous administration time, and minimal cytotoxicity to normal cells as well as reduced solvent-induced toxicity.
Nab-paclitaxel-based chemotherapy has been effectively utilized in treating a range of solid tumors, such as breast cancer, non-small cell lung cancer, gastric cancer, head and neck squamous cell carcinoma, and NPC.25–29 Notably, in patients with metastatic breast cancer, nab-paclitaxel has shown superior survival outcomes compared to docetaxel.30 Despite these promising results, there is still a paucity of data specifically addressing the safety and efficacy of nab-paclitaxel in comparison to docetaxel-based regimens for LA NPC. To fill this knowledge gap, we conducted a retrospective study designed to compare the efficacy and safety of nab-paclitaxel combined with nedaplatin versus docetaxel combined with nedaplatin in the treatment of LA NPC.
Patients and Methods
Patients
In this retrospective analysis, we examined patients with LA NPC who received IC combining either nab-paclitaxel or docetaxel with nedaplatin at Zhejiang Cancer Hospital, between December 2018 and January 2021. The study’s inclusion criteria encompassed: 1) NPC confirmed through histopathological examination, 2) clinical stage III–IVa, as defined by the American Joint Committee on Cancer (AJCC) 8th edition,31 3) a Karnofsky Performance Status (KPS) score of 70 or above, 4) age between 18 to 75 years old, 5) adequate bone marrow reserves and organ function (liver, kidney, lung, and heart), 6) absence of uncontrolled medical or psychiatric disorders, 7) no previous or concurrent other malignancies, with the exception of resolved cervical carcinoma in situ and thyroid papillary carcinoma, and 8) no prior history of antitumor therapies. The requirement for written informed consent was waived for this retrospective study, as it involved no more than minimal risk to the subjects and utilized only pre-existing clinical and demographic data collected during standard care. The study protocol received approval from the Independent Ethics Committee of Zhejiang Cancer Hospital (IRB-2025-383), which was performed in accordance with Declaration of Helsinki.
Chemotherapy
In the Nab-paclitaxel Group (NP), patients received 1–4 cycles of intravenous nab-paclitaxel (260 mg/m2) combined with nedaplatin (80 mg/m2) administered every 21 days. In the Docetaxel Group (TP), patients underwent 1–4 cycles of docetaxel (75 mg/m2) plus nedaplatin (75 mg/m2) on the same 21-day schedule, with mandatory dexamethasone premedication (8 mg orally twice daily for 3 days before chemotherapy). All patients commenced intensity-modulated radiotherapy (IMRT) or helical tomotherapy (TOMO) between 2 to 4 weeks following induction. Concurrently, patients received 1–2 cycles of nedaplatin (80–100 mg/m2 per cycle, 21-day intervals) during radiotherapy.
Radiotherapy
All patients received definitive radiotherapy via IMRT or TOMO delivered by 6 MV linear accelerators. Target volumes were delineated according to International Commission on Radiation Units (ICRU) Report 83 guideline Target Delineation. GTVnx: Encompassed nasopharyngeal primary lesions and involved retropharyngeal lymph nodes (short-axis ≥5 mm). GTVnd: Included metastatic cervical lymph nodes meeting radiologic criteria (necrosis, extracapsular spread, or short-axis ≥10 mm). CTV1 (High-risk): GTVnx + GTVnd with 5–10 mm isotropic expansion, covering: Entire nasopharyngeal mucosa, Lower 2/3 sphenoid sinus, Anterior 1/3 clivus, Pterygoid fossae, Posterior 1/3 nasal cavity/maxillary sinuses, Retropharyngeal/parapharyngeal spaces, Upper cervical nodal regions (levels II–Va). CTV2 (Low-risk): CTV1 + 3–5 mm margin extending to: Lower cervical (levels III–IV), Supraclavicular fossa. PTV: CTV/GTV + 3–5 mm geometric expansion accounting for setup uncertainties. Dose Prescription PGTVnx/PGTVnd: 6600–7000cGy. PTV1: 6000cGy. PTV2: 5400cGy. Doses were delivered in 30–33 fractions (2.0–2.12 Gy per fraction). Furthermore, maximum dose of each organ at risk was below its tolerance limit on the basis of the Radiation Therapy Oncology Group 0225 protocol.32
Follow-Up and Treatment Assessment
Treatment-related adverse events (AEs) were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0 (NCI CTCAE v5.0). Patients underwent weekly toxicity assessments during active treatment. During the treatment period, patients were assessed on a weekly basis, while post-treatment follow-up was systematically organized. This involved evaluations every three months for the first two years, transitioning to every six months from the third to the fifth year, and then annually after that, extending to either the patient’s death or their latest follow-up visit. Patients failing to attend more than two follow-up visits were excluded from the analysis. Each follow-up assessment was comprehensive, encompassing a detailed review of the patient’s medical history, physical examination, fiber-optic nasopharyngoscopy with biopsy, chest imaging via X-ray or CT scans, abdominal ultrasonography or CT, and MRI of the head and neck area. Furthermore, if patients exhibited bone pain symptoms, an in-depth whole-body bone scan was conducted.
Statistical Analysis
Propensity score matching (PSM) was performed using logistic regression based on the following covariates: age, sex, pathology, T stage, N stage, clinical stage, KPS, EBV DNA copies, and IC cycle. Statistical analyses were conducted utilizing SPSS version 22.0 software (SPSS, Chicago, IL, USA). Patient characteristics were evaluated using either the chi-square test or Fisher’s exact test, as appropriate. Survival outcomes, including overall survival (OS), local relapse-free survival (LRFS), and distant metastasis-free survival (DMFS), were determined through the Kaplan–Meier method. To assess the impact of various factors on survival, a multivariate analysis was carried out using the Cox proportional hazards model. Two-sided P values<0.05 were considered to be statistically significant.
Results
Patient Characteristics
Between December 2018 and January 2021, a total of 227 treatment-naïve patients with LA NPC were enrolled in this retrospective analysis, all undergoing IC with either TP or NP regimen. The cohort demonstrated significant gender disparity, with male patients constituting 69.2% (157/227) of the study population compared to 30.8% (70/227) female representation. The median age at diagnosis was 51 years (range: 16–74). Following propensity score matching (PSM) implementation, 140 eligible patients (70 matched pairs) were allocated for intergroup comparisons. As summarized in Table 1, successful covariate balance was achieved across essential baseline characteristics, including: age, sex, T stage, N stage, clinical stage, Karnofsky Performance Status (KPS) assessments, EBV DNA copies, and completed induction chemotherapy (IC) cycles, with all between-group comparisons demonstrating non-significant differences (all P values > 0.05).
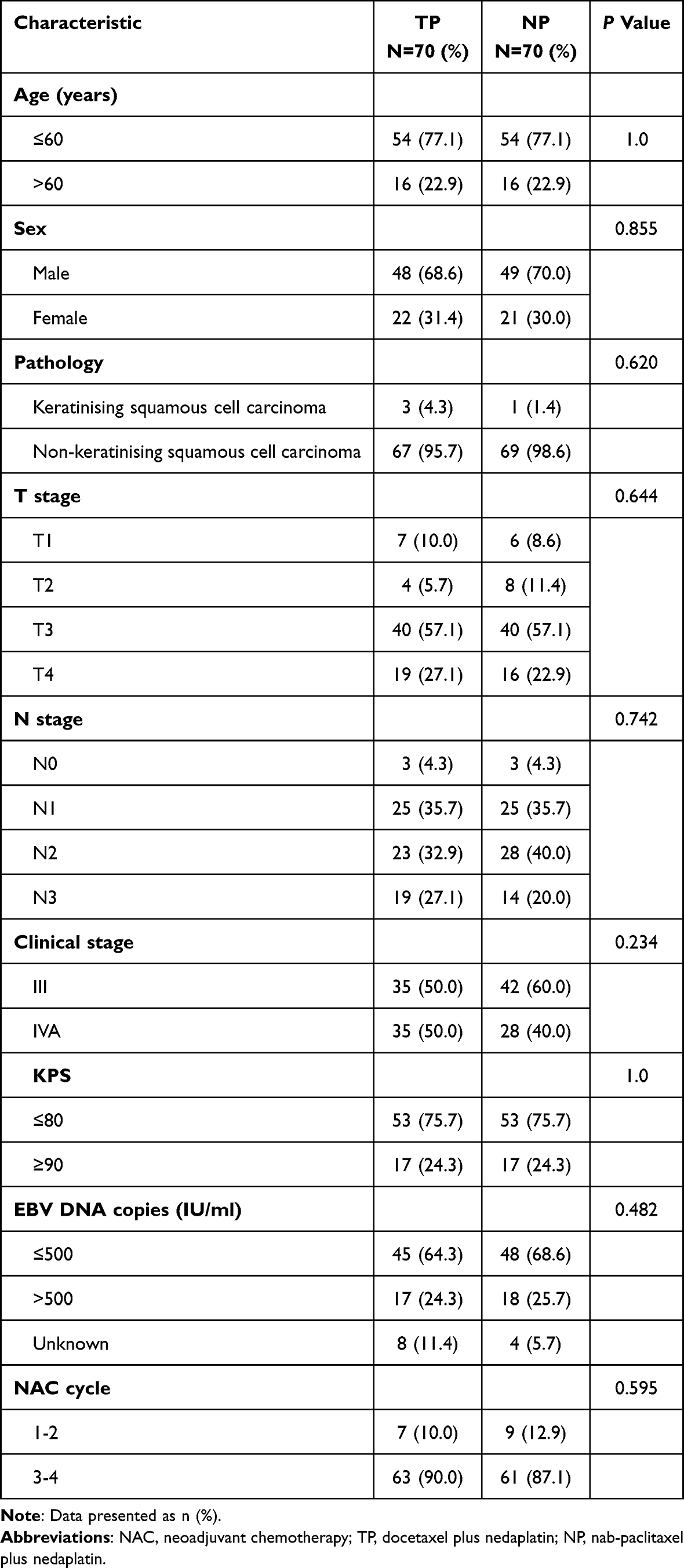 |
Table 1 Patient and Disease Characteristics |
Efficacy
Tumor response was assessed at 3 months post-radiotherapy according to Response Evaluation Criteria in Solid Tumors (RECIST v1.1), categorizing responses as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). As detailed in Table 2, the NP group exhibited a complete response (CR) rate of 95.7% (67/70), compared to 94.6% (66/70) in the TP group. The partial response (PR) rates were 4.3% (3/70) and 5.7% (4/70) for the NP and TP groups, respectively. Both cohorts attained an objective response rate (ORR) of 100% (70/70 in each group). No significant difference in overall tumor response was observed between the two groups (P = 1.0).
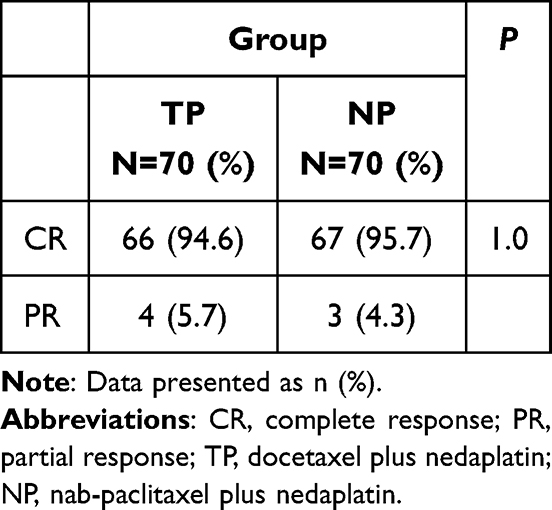 |
Table 2 Tumor Response Three Months After Chemoradiotherapy in NP or TP Group |
Acute Toxicity
Acute adverse events (AEs) for both treatment cohorts are summarized in Table 3. As for the hematologic toxicities, the incidence of any-grade neutropenia was significantly higher in the TP group (68.6%) compared to the NP group (50.0%, P = 0.047). However, the rates of grade 3–4 hematologic toxicities, including leukopenia, neutropenia, thrombocytopenia, and anemia, were comparable between the two groups (all P > 0.05). As for the non-hematologic toxicities, the NP group demonstrated a significantly higher incidence of any-grade peripheral sensory neuropathy (57.1% vs 0.0%, P < 0.001) and myalgia (45.7% vs 1.4%, P < 0.001). In contrast, the TP group had a significantly higher rate of any-grade dermatitis (100.0% vs 98.6%, P = 0.020). The incidences of other non-hematologic toxicities, including hepatotoxicity, nephrotoxicity, and gastrointestinal reactions, were similar between the groups. Most non-hematologic toxicities were mild to moderate (grade 1–2), with no significant differences in grade 3–4 events.
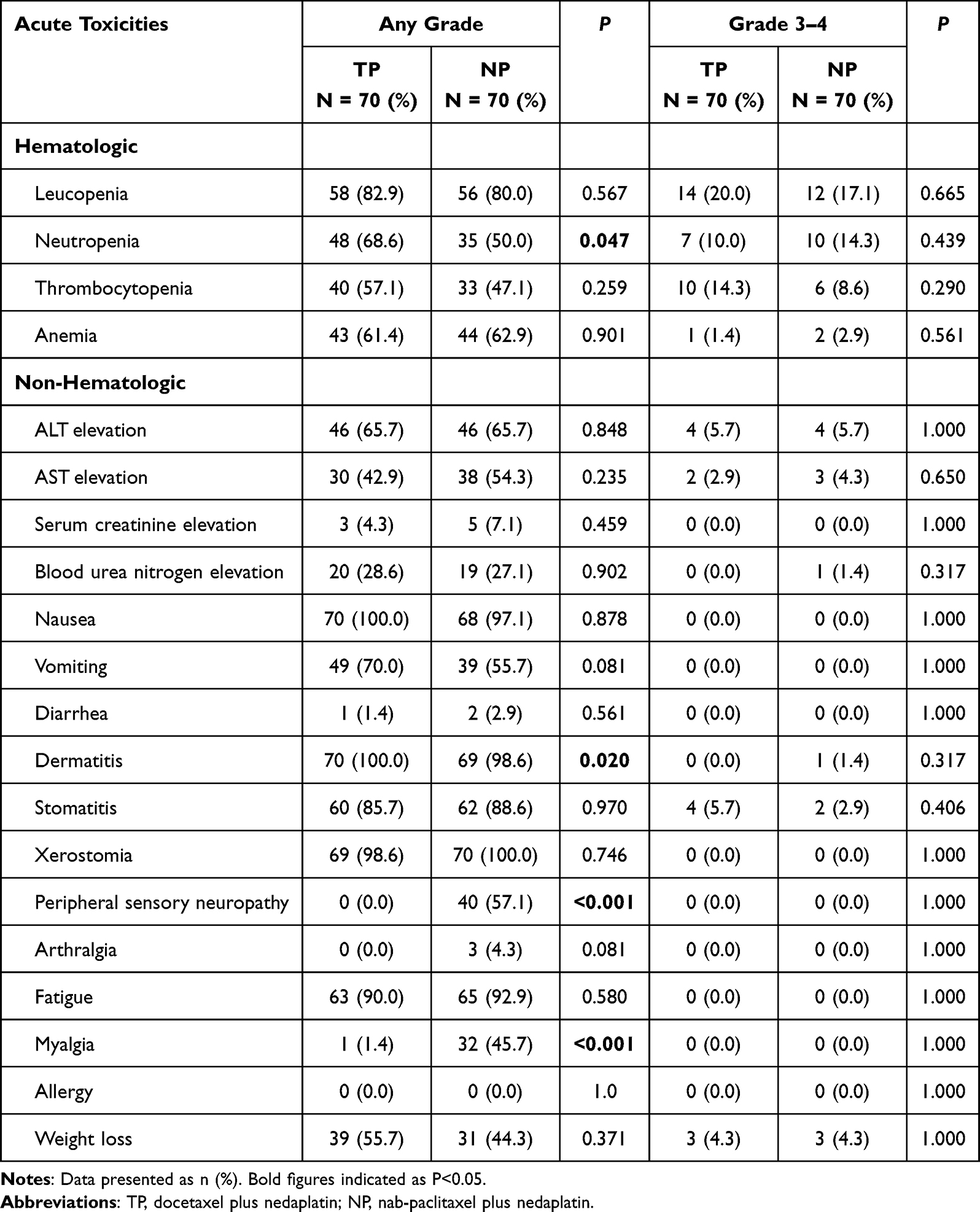 |
Table 3 Frequency of Acute Toxicities from the Two Groups by Type and Grade |
Treatment Outcomes
After a median follow-up of 68.6 months (range, 2.4–77.1), the 5-year OS (89.98% vs 86.98%, P = 0.610), LRFS (94.06% vs 96.69%, P = 0.424), and DMFS (91.33% vs 85.61%, P = 0.308) rates were not statistically different between the NP and TP groups (Figure 1 and Table 4).
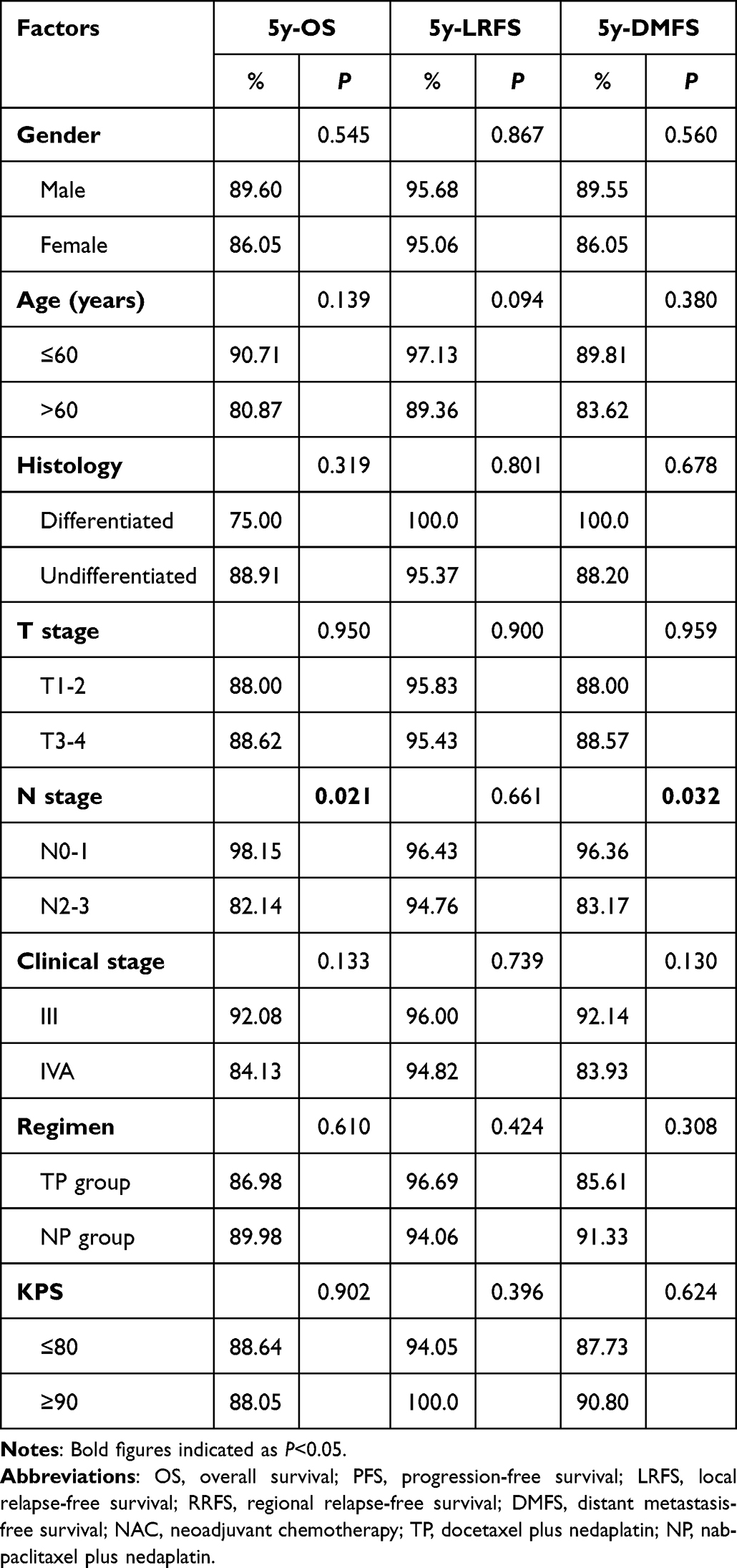 |
Table 4 Effect of Prognostic Factors on Survival in Univariate Analyses |
 |
Figure 1 Kaplan–Meier survival curves for induction chemotherapy with nanoparticle albumin-bound paclitaxel versus docetaxel plus nedaplatin followed by concurrent chemoradiotherapy in the 70 pairs of patients with locally advanced nasopharyngeal carcinoma. (A) Overall survival (OS). (B) Local relapse-free survival (LRFS). (C) Distant metastasis-free survival (DMFS). P-value were calculated using the Log rank test. |
Prognostic Factors
Univariate and multivariable analyses were used to assess factors associated with patient survival. Univariate analysis identified N stage as an adverse factor for OS (P=0.021) and DMFS (P=0.032) (Table 4). In a multivariable Cox model adjusting for sex, age, regimen, and T/N stage, N stage retained significance for OS (HR=13.285, 95% CI: 1.712–103.092, P=0.013) and DMFS (HR=5.901, 95% CI: 1.297–26.858, P=0.022). However, the treatment regimen (NP vs TP) was not an independent prognostic factor (Table 5).
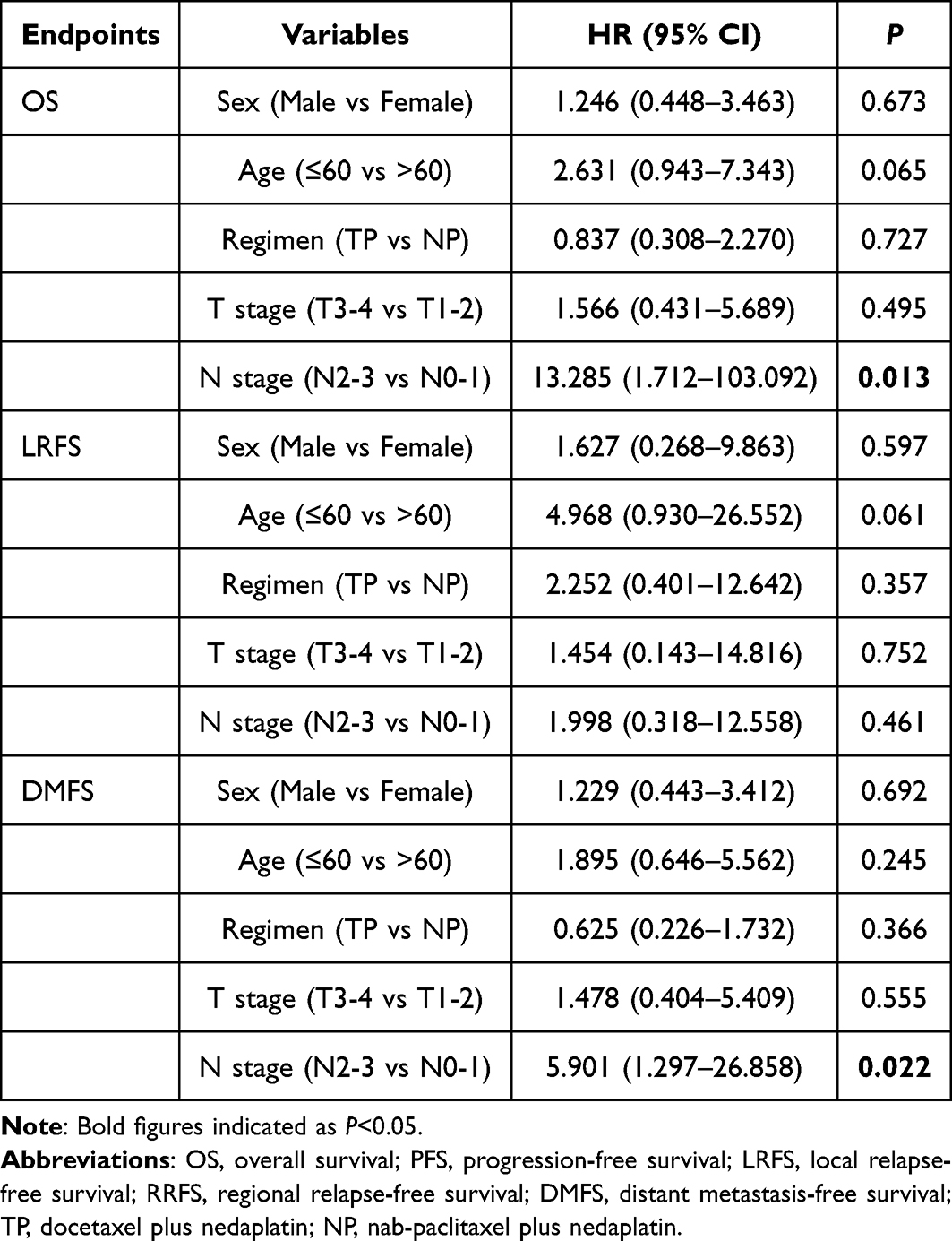 |
Table 5 Impact of Prognostic Factors on Treatment Results by Multivariate Analysis (P Value) |
Discussion
This PSM retrospective analysis represents, to our knowledge, the first direct comparative study evaluating the efficacy and safety of an IC regimen comprising NP versus the established TP regimen in patients with LA-NPC. The principal finding of our study is that the novel NP regimen demonstrated comparable long-term survival outcomes to the TP regimen, with 5-year OS, LRFS, and DMFS rates showing no statistically significant differences. However, the two regimens exhibited distinct and clinically relevant toxicity profiles, which may inform therapeutic selection in specific patient populations.
The equivalence in survival outcomes is a cornerstone of our findings. After a substantial median follow-up of 68.6 months, the NP and TP groups showed nearly identical rates of overall survival, local control, and distant metastasis prevention. This long-term data robustly suggests that the substitution of docetaxel with nab-paclitaxel, within a nedaplatin-based backbone, does not compromise therapeutic efficacy. Multivariable analysis further corroborated this, confirming that the treatment regimen was not an independent prognostic factor for survival, whereas advanced N stage (N2-3) remained a potent predictor of poorer OS and DMFS. The observed survival rates in both groups are also favorable when contextualized within the historical data of other induction regimens such as TPF and GP,7–10 reinforcing the position of taxane-nedaplatin combinations as effective treatment options for LA-NPC.
The divergence in safety profiles between the regimens, however, offers a critical basis for clinical decision-making. The significantly higher incidence of any-grade neutropenia in the TP group is consistent with the known hematological toxicity of solvent-based docetaxel.19,30 While the rates of severe (grade 3–4) hematologic events were comparable, the lower rate of any-grade neutropenia with NP may translate to a reduced need for supportive interventions such as granulocyte colony-stimulating factor in a real-world setting. Conversely, the NP regimen was associated with a markedly higher incidence of any-grade peripheral sensory neuropathy and myalgia. This is a well-characterized class effect of paclitaxel, and its prevalence with nab-paclitaxel is documented in studies across other malignancies.25–30 It is crucial to note that these neurotoxic and muscular events were predominantly low-grade, and their long-term impact on quality of life warrants further investigation. Importantly, these effects did not necessitate treatment delays or dose reductions. The near-universal, albeit low-grade, dermatitis in the TP group is a direct consequence of the premedication with high-dose corticosteroids, a requirement that is eliminated with the solvent-free nab-paclitaxel formulation. This key difference simplifies administration, reduces steroid-related comorbidities, and is particularly advantageous for patients with diabetes or other contraindications to corticosteroids.
Our findings build upon the established rationale for using nedaplatin as a cisplatin alternative with a more favorable renal and gastrointestinal toxicity profile.16–18 By combining nedaplatin with nab-paclitaxel, we have further refined the regimen to mitigate solvent-related toxicities and hypersensitivity risks. The NP regimen thus emerges as a viable therapeutic alternative, especially for patients who are poor candidates for high-dose steroids or who have pre-existing conditions that could be exacerbated by the hematological toxicity profile of docetaxel. The recent integration of radiological extranodal extension (rENE) into the 9th edition of the AJCC staging system for NPC33 underscores the growing emphasis on refining risk stratification. Future studies could explore whether such imaging biomarkers, along with molecular markers like SPARC expression, which implicated in nab-paclitaxel tumor targeting,34 might help identify patients most likely to benefit from the NP regimen.
Several limitations of our study warrant consideration. Its retrospective and single-center nature inherently introduces potential for selection bias, despite our use of PSM to mitigate confounding factors. The sample size, while adequate for detecting large differences, may be underpowered for identifying smaller, yet clinically relevant, differences in survival or specific toxicities. Furthermore, patient-reported quality of life outcomes, which are crucial for fully evaluating the impact of differing toxicity profiles (especially neurotoxicity), were not available. Recent high-quality randomized trials, such as the one paperpublished recently investigating reduced-volume radiotherapy after IC,4 highlight the importance of prospective design and toxicity reduction as a key endpoint. Future prospective, randomized studies comparing NP and TP are needed to validate our findings and incorporate comprehensive quality-life metrics.
Accumulating evidence from large-scale clinical trials confirms that incorporating immunotherapy into radiochemotherapy significantly improves event-free survival (EFS) in NPC patients.35,36 In contrast to the existing literature, which is predominantly based on the gemcitabine and cisplatin (GP) regimen, our study specifically investigates the nab-paclitaxel and nedaplatin combination. Therefore, future research should focus on evaluating the efficacy and safety of triplet induction regimens comprising nab-paclitaxel, nedaplatin, and PD-1 inhibitors, with the goal of optimizing combination strategies to achieve superior clinical outcomes.
Conclusion
In conclusion, our study demonstrates that induction chemotherapy with NP yields long-term survival outcomes equivalent to those of the TP regimen in patients with LA NPC. The choice between these regimens can therefore be individualized based on their distinct toxicity profiles: TP is associated with a higher burden of neutropenia and requires corticosteroid premedication, whereas NP offers a simplified administration and a lower hematological toxicity burden at the cost of increased, though typically low-grade, neurotoxicity and myalgia. These findings provide clinicians with an evidence-based alternative for personalizing induction chemotherapy. Prospective randomized controlled trials are warranted to validate these results and to further explore predictive biomarkers for tailoring regimen selection.
Funding
This work was supported by the Phase 2 “Talent Revitalization” training project 30, Zhejiang Provincial Traditional Chinese Medicine Science and Technology Project (NO. 2025069972) and Zhejiang Medical and Health Science and Technology Project (NO. 2022503214).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen Y, Chan ATC, Le Q, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–11. doi:10.1016/S0140-6736(19)30956-0
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Lam WKJ, Ma BBY, King AD, Malki Y, Chan KCA, Chan ATC. Achieving control of nasopharyngeal carcinoma: the role of epstein-barr virus-based screening and vaccines. Nat Rev Clin Oncol. 2025;23(1):7–21. doi:10.1038/s41571-025-01079-x
4. Tang L, Chen L, Xu G, et al. Reduced-volume radiotherapy versus conventional-volume radiotherapy after induction chemotherapy in nasopharyngeal carcinoma: an open-label, noninferiority, multicenter, randomized Phase 3 trial. Ca Cancer J Clin. 2025;75(3):203–215. doi:10.3322/caac.21881
5. Tang L, Huang C, Lin S, et al. Target volume delineation of the neck for radiotherapy in nasopharyngeal carcinoma: CSTRO, CACA, CSCO, HNCIG, ESTRO, and ASTRO guidelines and contouring atlas. Lancet Oncol. 2025;26(9):e488–e498. doi:10.1016/S1470-2045(25)00327-4
6. Blanchard P, Lee A, Marguet S, et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the mac-npc meta-analysis. Lancet Oncol. 2015;16(6):645–655. doi:10.1016/S1470-2045(15)70126-9
7. Sun Y, Li W, Chen N, et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016;17(11):1509–1520. doi:10.1016/S1470-2045(16)30410-7
8. Frikha M, Auperin A, Tao Y, et al. A randomized trial of induction docetaxel-cisplatin-5fu followed by concomitant cisplatin-rt versus concomitant cisplatin-rt in nasopharyngeal carcinoma (gortec 2006-02). Ann Oncol. 2018;29(3):731–736. doi:10.1093/annonc/mdx770
9. Zhang Y, Chen L, Hu G, et al. Gemcitabine and cisplatin induction chemotherapy in nasopharyngeal carcinoma. N Engl J Med. 2019;381(12):1124–1135. doi:10.1056/NEJMoa1905287
10. Yang Q, Cao S, Guo L, et al. Induction chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: long-term results of a phase iii multicentre randomised controlled trial. Eur J Cancer. 2019;119:87–96. doi:10.1016/j.ejca.2019.07.007
11. Wang Y, Wang C, He S, et al. Induction chemotherapy regimen of docetaxel plus cisplatin versus docetaxel, cisplatin plus fluorouracil followed by concurrent chemoradiotherapy in locoregionally advanced nasopharyngeal carcinoma: preliminary results of an open-label, noninferiority, multicentre, randomised, controlled phase 3 trial. Eclinicalmedicine. 2022;53:101625. doi:10.1016/j.eclinm.2022.101625
12. Chen L, Hu C, Chen X, et al. Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2012;13(2):163–171. doi:10.1016/S1470-2045(11)70320-5
13. Zhang L, Huang Y, Hong S, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet. 2016;388(10054):1883–1892. doi:10.1016/S0140-6736(16)31388-5
14. Rybak LP, Mukherjea D, Jajoo S, Ramkumar V. Cisplatin ototoxicity and protection: clinical and experimental studies. Tohoku J Exp Med. 2009;219(3):177–186. doi:10.1620/tjem.219.177
15. Fung C, Dinh PJ, Ardeshir-Rouhani-Fard S, Schaffer K, Fossa SD, Travis LB. Toxicities associated with cisplatin-based chemotherapy and radiotherapy in long-term testicular cancer survivors. Adv Urol. 2018;2018:8671832. doi:10.1155/2018/8671832
16. Li Z, Li C, Yang D, et al. Comparing the efficacy and safety of cisplatin and other platinum-based chemotherapies in locally advanced nasopharyngeal carcinoma: a systematic review and meta-analysis. Bmc Cancer. 2022;22(1):616. doi:10.1186/s12885-022-09712-z
17. Liao W, Huang J, Wu Q, et al. Concurrent chemoradiotherapy with nedaplatin versus cisplatin in stage ii-ivb nasopharyngeal carcinoma: a cost-effectiveness analysis. Oral Oncol. 2019;93:15–20. doi:10.1016/j.oraloncology.2019.04.003
18. Liu T, Sun Q, Chen J, et al. Neoadjuvant chemotherapy with fluorouracil plus nedaplatin or cisplatin for locally advanced nasopharyngeal carcinoma: a retrospective study. J Cancer. 2018;9(20):3676–3682. doi:10.7150/jca.27198
19. Verweij J, Clavel M, Chevalier B. Paclitaxel (taxol) and docetaxel (taxotere): not simply two of a kind. Ann Oncol. 1994;5(6):495–505. doi:10.1093/oxfordjournals.annonc.a058903
20. Ibrahim NK, Desai N, Legha S, et al. Phase I and pharmacokinetic study of abi-007, a cremophor-free, protein-stabilized, nanoparticle formulation of paclitaxel. Clin Cancer Res. 2002;8(5):1038–1044.
21. Nyman DW, Campbell KJ, Hersh E, et al. Phase i and pharmacokinetics trial of abi-007, a novel nanoparticle formulation of paclitaxel in patients with advanced nonhematologic malignancies. J Clin Oncol. 2005;23(31):7785–7793. doi:10.1200/JCO.2004.00.6148
22. Desai N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxel concentrations, and endothelial cell transport of cremophor-free, albumin-bound paclitaxel, abi-007, compared with cremophor-based paclitaxel. Clin Cancer Res. 2006;12(4):1317–1324. doi:10.1158/1078-0432.CCR-05-1634
23. Gardner ER, Dahut WL, Scripture CD, et al. Randomized crossover pharmacokinetic study of solvent-based paclitaxel and nab-paclitaxel. Clin Cancer Res. 2008;14(13):4200–4205. doi:10.1158/1078-0432.CCR-07-4592
24. Gelderblom H, Verweij J, Nooter K, Sparreboom A. Cremophor el: the drawbacks and advantages of vehicle selection for drug formulation. Eur J Cancer. 2001;37(13):1590–1598. doi:10.1016/s0959-8049(01)00171-x
25. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379(22):2108–2121. doi:10.1056/NEJMoa1809615
26. Rizvi NA, Riely GJ, Azzoli CG, et al. Phase i/ii trial of weekly intravenous 130-nm albumin-bound paclitaxel as initial chemotherapy in patients with stage iv non-small-cell lung cancer. J Clin Oncol. 2008;26(4):639–643. doi:10.1200/JCO.2007.10.8605
27. Sasaki Y, Nishina T, Yasui H, et al. Phase II trial of nanoparticle albumin-bound paclitaxel as second-line chemotherapy for unresectable or recurrent gastric cancer. Cancer Sci. 2014;105(7):812–817. doi:10.1111/cas.12419
28. Adkins D, Ley J, Trinkaus K, et al. A phase 2 trial of induction nab-paclitaxel and cetuximab given with cisplatin and 5-fluorouracil followed by concurrent cisplatin and radiation for locally advanced squamous cell carcinoma of the head and neck. Cancer. 2013;119(4):766–773. doi:10.1002/cncr.27741
29. Ke L, Xia W, Qiu W, et al. A phase ii trial of induction nab-paclitaxel and cisplatin followed by concurrent chemoradiotherapy in patients with locally advanced nasopharyngeal carcinoma. Oral Oncol. 2017;70:7–13. doi:10.1016/j.oraloncology.2017.04.018
30. Gennari A, Sun Z, Hasler-Strub U, et al. A randomized phase ii study evaluating different maintenance schedules of nab-paclitaxel in the first-line treatment of metastatic breast cancer: final results of the ibcsg 42-12/big 2-12 snap trial. Ann Oncol. 2018;29(3):661–668. doi:10.1093/annonc/mdx772
31. Pan JJ, Ng WT, Zong JF, et al. Proposal for the 8th edition of the ajcc/uicc staging system for nasopharyngeal cancer in the era of intensity-modulated radiotherapy. Cancer. 2016;122(4):546–558. doi:10.1002/cncr.29795
32. Lee N, Harris J, Garden AS, et al. Intensity-modulated radiation therapy with or without chemotherapy for nasopharyngeal carcinoma: radiation therapy oncology group phase ii trial 0225. J Clin Oncol. 2009;27(22):3684–3690. doi:10.1200/JCO.2008.19.9109
33. Chakrabarty N, Mahajan A. Radiological extranodal extension in head and neck cancers: current evidence and challenges in imaging detection and prognostic impact. Bjr Open. 2025;7(1):tzaf21. doi:10.1093/bjro/tzaf021
34. Lipp H. [Nab-paclitaxel. Clinical value of an innovative taxane-containing formulation]. Med Monatsschr Pharm. 2013;36(1):14–24.
35. Liang Y, Liu X, Shen L, et al. Adjuvant pd-1 blockade with camrelizumab for nasopharyngeal carcinoma: the dipper randomized clinical trial. JAMA. 2025;333(18):1589–1598. doi:10.1001/jama.2025.1132
36. Liu X, Zhang Y, Yang K, et al. Induction-concurrent chemoradiotherapy with or without sintilimab in patients with locoregionally advanced nasopharyngeal carcinoma in China (continuum): a multicentre, open-label, parallel-group, randomised, controlled, phase 3 trial. Lancet. 2024;403(10445):2720–2731. doi:10.1016/S0140-6736(24)00594-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.