Back to Journals » ImmunoTargets and Therapy » Volume 14
Efficacy and Safety of Different Sequences for mFOLFIRINOX (or SOXIRI) and Gemcitabine Plus Albumin-Bound Paclitaxel in Unresectable Pancreatic Cancer
Authors Huang S, Huang L, Zhang D, Jiang Q, Wang F, Guo G ![]()
Received 24 April 2025
Accepted for publication 28 July 2025
Published 2 October 2025 Volume 2025:14 Pages 1097—1110
DOI https://doi.org/10.2147/ITT.S530434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jadwiga Jablonska
Silan Huang,1,* Lingli Huang,1,* Dongsheng Zhang,2 Qi Jiang,1 Fenghua Wang,2 Guifang Guo1
1VIP Department, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China; 2Department of Medical Oncology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guifang Guo, VIP Department, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China, Email [email protected] Fenghua Wang, Department of Medical Oncology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Aim: This study aimed to evaluate and compare the therapeutic efficacy and adverse effects of two sequential treatment strategies in patients with unresectable advanced pancreatic cancer (aPC), albumin-bound-paclitaxel plus gemcitabine administered follow by mFOLFIRINOX or SOXIRI (AG-F(S)FXm) versus the reverse sequence regimen F(S)FXm-AG.
Methods: In this retrospective analysis, patients with unresectable advanced pancreatic cancer (aPC) who received either AG-F(S)FXm or F(S)FXm-AG were included. Key endpoints were overall survival (OS), progression-free survival (PFS), and treatment-related toxicity. Survival outcomes were assessed using Kaplan-Meier curves, and differences between groups were examined through hazard ratios (HR) and corresponding p-values.
Results: A total of 107 patients were analyzed, including 49 who underwent AG-F(S)FXm and 58 who received F(S)FXm-AG. The median OS was 14.60 months for F(S)FXm-AG and 12.20 months for AG-F(S)FXm (HR: 1.04, 95% CI: 0.69– 1.57, p= 0.86). Median PFS1, median PFS2 and median total PFS (tPFS) were 5.20 months versus 4.83 months (HR: 0.81, 95% CI: 0.54– 1.21, p= 0.3), 4.53 months versus 5.77 months (HR: 1.15, 95% CI: 0.71– 1.88, p= 0.60) and 13.80 months versus 12.80 months (HR: 0.90, 95% CI: 0.55– 1.48, p= 0.67) for F(S)FXm-AG versus AG-F(S)FXm. Given their comparable efficacy, we further compared the safety profiles of both regimens. The toxicity profiles differed between the two sequential treatments. Leukopenia was more common with first-line AG, while gastrointestinal toxicity, fatigue, and sensory neuropathy were more frequent with first-line F(S)FXm. Additionally, elevated aspartate aminotransferase was more often reported with second-line AG.
Conclusion: Both AG-F(S)FXm and F(S)FXm-AG demonstrated comparable efficacy in treating aPC, with F(S)FXm-AG showing a trend toward improved outcomes. The choice of sequential treatment should be guided by toxicity profiles and patient-specific factors. Further prospective studies are warranted to optimize treatment sequencing and personalize therapy for improved patient outcomes.
Keywords: advanced pancreatic cancer, AG, mFOLFIRINOX, SOXIRI and efficacy
Introduction
Pancreatic cancer is one of the deadliest malignancies, characterized by a five-year survival rate of only 5% to 10%-the lowest reported among all major cancer types.1–3 Despite advancements in both medical therapies and surgical techniques, the overall survival rate has improved only marginally in recent decades. Surgical resection remains the only potentially curative option. However, merely 15%-20% of patients are diagnosed at a stage where surgery is feasible.4 The majority of patients present with advanced stage, either with locally advanced or metastatic pancreatic adenocarcinoma (aPC), for which systemic chemotherapy remains the cornerstone of treatment. Furthermore, up to 80% of patients who undergo surgery experience disease recurrence within five years,5 necessitating further chemotherapy. In short, chemotherapy plays a critical role in the treatment of pancreatic cancer.
The emergence of multi-drug chemotherapy protocols has notably influenced the therapeutic landscape of aPC. Among these, FOLFIRINOX (a combination of fluorouracil, leucovorin, irinotecan, and oxaliplatin) and the combination of albumin-bound-paclitaxel with gemcitabine (AG) are now recognized as standard first-line therapies for advanced disease.6 Compared to the earlier standard of gemcitabine monotherapy, both combination regimens have shown superior survival benefits.7–9 However, given the frequent occurrence of grade 3–4 toxicities associated with FOLFIRINOX, several studies have explored dose-modified FOLFIRINOX (mFOLFIRINOX), offering comparable efficacy with improved safety profiles.10–12 Moreover, several Phase II trials, including our published study, have shown that the SOXIRI regimen (S-1, oxaliplatin, and irinotecan) offers similar efficacy to mFOLFIRINOX and may be better tolerated as a first-line therapy for patients with locally advanced or metastatic disease.13–16
However, despite these advances, the optimal sequencing of chemotherapy regimens remains unclear and continues to be an active area of research. Selecting the most appropriate first-line treatment and determining the subsequent therapeutic approach after disease progression are key factors that impact patient outcomes. Real-world data on the effectiveness and toxicity profiles of different treatment sequences are crucial for guiding clinical decisions and improving outcomes.
This retrospective analysis seeks to evaluate the efficacy and safety of sequential chemotherapy using mFOLFIRINOX (FFXm) or SOXIRI and AG regimens in patients with aPC treated at a single center. The findings are expected to enhance the current evidence base and contribute to the optimization of therapeutic strategies for this aggressive malignancy.
Methods
For more detailed methods, please refer to the Supplementary Materials.
Study Design and Population
This retrospective cohort study included patients with unresectable (locally advanced or metastatic) pancreatic cancer who were administered first-line (1L) FFXm or SOXIRI (F(S)FXm) followed by second line (2L) AG, or 1L AG followed by 2L FFXm or SOXIRI at Sun Yat-sen University Cancer Center between January 2015 to December 2022.
The inclusion criteria were as follows: 1) age ≥ 18 years, 2) receipt of at least one cycle of both AG and either FFXm or SOXIRI, 3) histologically confirmed pancreatic adenocarcinoma, 4) measurable pancreatic adenocarcinoma and/or metastatic lesions without prior chemotherapy for unresectable disease, or patients who had completed neoadjuvant or adjuvant chemotherapy more than six months prior, 5) Eastern Cooperative Oncology Group (ECOG) performance status score of 0 or 1, 5) adequate bone marrow, liver and renal function (details are shown in Supplementary methods).
Exclusion criteria included: pancreatic acinar or endocrine carcinoma, a history of other significant malignancies, brain metastases, breastfeeding or pregnancy, and active infection.
All consecutive patients meeting the inclusion criteria within this period were enrolled to minimize selection bias.
Chemotherapy Regimens
Patients were categorized into two groups based on the sequence of treatment received: AG-F(S)FXm group: Patients who received albumin-bound-paclitaxel plus gemcitabine followed by mFOLFIRINOX or SOXIRI.
F(S)FXm-AG group: Patients who received mFOLFIRINOX or SOXIRI followed by albumin-bound-paclitaxel plus gemcitabine.
F(S)FXm refers to a triplet chemotherapy regimen consisting of either modified FOLFIRINOX or SOXIRI: oxaliplatin at 65 mg/m2 or 85 mg/m2, irinotecan at 150 mg/m2 or 180 mg/m2, respectively, combined with 5-fluorouracil (5-FU) administered as a 46–48 hour continuous intravenous infusion at 2400 mg/m2, or oral tegafur at 40 mg twice daily for 2 consecutive weeks. AG is a doublet regimen combining gemcitabine (1000 mg/m2) and albumin-bound-paclitaxel (125 mg/m2), administered on day 1 and day 8 of a 3-week cycle. Dose reductions of one or more agents (by 20–25%) were permitted at the discretion of the treating physician in cases of grade 4 toxicity.
Data Collection
Clinical data were obtained from electronic medical records and included patient demographics, baseline characteristics, treatment regimens, and follow-up outcomes. Collected baseline characteristics encompassed general information, disease status, comorbidities, anthropometric and biochemical measurements, as well as tumor markers. Detailed patient characteristics are shown in Supplementary methods.
End Points
The primary end points were overall survival (OS) and progression free survival (PFS). Additional endpoints included objective response rate (ORR), disease control rate (DCR) and treatment-related toxicity. OS was defined as the time from the start of first line (1L) treatment to death from any cause. PFS1 referred to the duration from the initiation of 1L therapy to either progression on first-line treatment or the commencement of second-line therapy. PFS2 was calculated from the start of second-line treatment to disease progression on second-line therapy, the beginning of third-line treatment or death from any cause. Total PFS (tPFS) was defined as PFS1 plus PFS2. Treatment response was evaluated by the clinician in accordance with Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Adverse events (AEs) were assessed at the start of each treatment cycle and graded based on the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. For each type of toxicity, the highest grade observed during treatment was documented and used for comparison between groups.
Statistical Analysis
Baseline characteristics and treatment-related variables were summarized using descriptive statistical methods, including frequencies and percentages for categorical variables and medians with interquartile ranges for continuous variables. To evaluate survival outcomes-including OS, PFS1, PFS2 and tPFS, Kaplan-Meier survival curves were constructed. Differences between groups were assessed using the Log rank test. Subgroup analyses were performed based on key baseline variables such as age, ECOG performance status, liver metastasis, albumin levels, and treatment duration. Survival outcomes were compared using Cox proportional hazards models within each subgroup. To account for potential confounding factors, multivariate analyses were performed using Cox proportional hazards regression models. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated for OS, PFS1, PFS2, and tPFS, with adjustments for clinically relevant covariates such as age, sex, ECOG performance status, and tumor stage at baseline. Adverse events were evaluated based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. The incidence of adverse events was compared between treatment groups using either the chi-square test or Fisher’s exact test, depending on the sample size and distribution characteristics of the data. Statistical analyses were conducted using R software, with significance defined as p < 0.05.
Results
Patient Characteristics
This study enrolled 107 patients diagnosed with locally advanced or metastatic pancreatic cancer who underwent sequential chemotherapy. Among them, 58 patients received the F(S)FXm-AG regimen, SOXIRI or FFXm as first-line (1L) therapy followed by AG as second-line (2L) therapy, while 49 patients were treated with the AG-F(S)FXm regimen, receiving AG in 1L and SOXIRI or FFXm in 2L. Specifically, in the first-line treatment setting, 25 patients received FFXm and 33 received SOXIRI. In the second-line treatment, 37 patients received FFXm and 12 received SOXIRI. Baseline characteristics for both groups are summarized in Table 1, with no significant differences observed between the two groups. The follow-up duration ranged from 1.97 to 60.43 months, with a median follow-up time of 12.27 months for the overall cohort. The median number of first-line treatment cycles was 6 in the AG-F(S)FXm group and 7 in the F(S)FXm-AG group. For second-line therapy, the median number of cycles administered was 3 in the AG-F(S)FXm group and 2.25 in the F(S)FXm-AG group. During first line treatment, all patients except one (1.7%) in the F(S)FXm-AG group underwent imaging evaluation. During second-line therapy, imaging assessments were not performed in 28.6% (n = 14) of patients in the AG-F(S)FXm group and 25.9% (n = 15) in the F(S)FXm-AG group. For these individuals, survival data were collected via telephone follow-up.
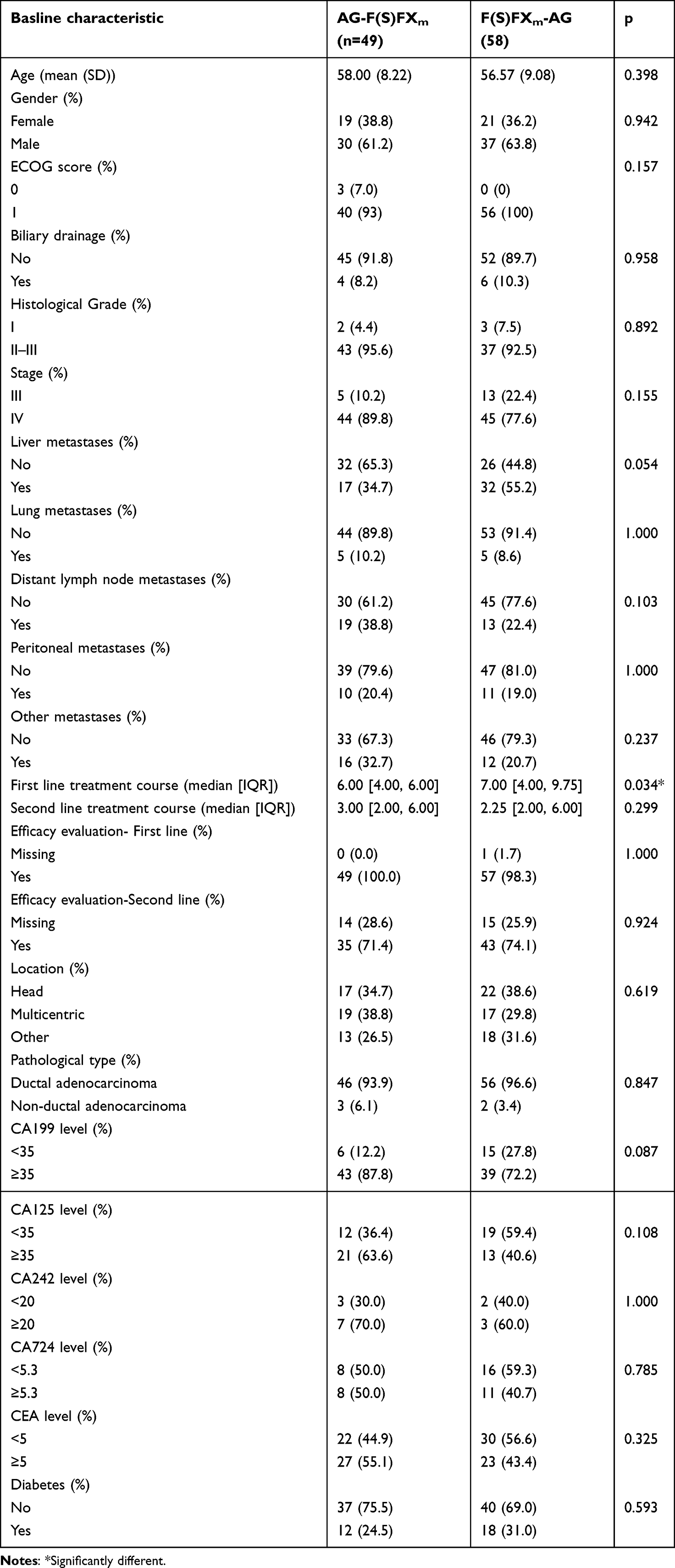 |
Table 1 Basline Characteristic of All Patients |
Univariate and Multivariate Analyses for the Whole Patients
Univariate and multivariate Cox regression analyses were conducted to identify independent prognostic factors for OS and PFS, based on baseline characteristics of all patients treated with either AG-F(S)FXm or F(S)FXm-AG (Tables S1–S4). In univariate analysis, the number of first-line treatment cycles was found to be an independent prognostic factor for both PFS1 (HR= 0.15, 95% CI: 0.09–0.24, p = 0.000) and tPFS (HR = 0.44, 95% CI: 0.26–0.72, p = 0.001). Meanwhile, the number of second-line treatment cycles was an independent predictor of PFS2 (HR = 0.6, 95% CI: 0.36–0.99, p = 0.045). After multivariate Cox regression adjustment, receiving ≥ 6 cycles of first-line therapy remained significantly associated with improved OS (HR = 0.48, 95% CI: 0.31–0.73, p = 0.001), as did receiving ≥ 6 cycles of second-line therapy (HR = 0.41, 95% CI: 0.25–0.68, p = 0.001). Conversely, baseline CA19-9 ≥ 35 U/mL was identified as an independent unfavorable prognostic factor for OS (HR = 2.49, 95% CI: 1.40–4.42, p = 0.002).
Efficacy of Two Reverse Sequential Treatments
No significant differences were observed in median OS, PFS1, PFS2 or tPFS between the two reverse sequential treatment groups-F(S)FXm-AG and AG-F(S)FXm. The median OS was 14.6 (95% CI: 12.10–18.80) for F(S)FXm-AG versus 12.2 (95% CI: 10.30–18.20) months for AG-F(S)FXm (HR: 1.04, 95% CI: 0.69–1.57; P = 0.86), respectively (Figure 1A). The median PFS1 was 5.20 (95% CI: 4.03–7.97) versus 4.83 (95% CI: 4.20–6.57) months (HR: 0.81,95% CI: 0.54–1.21; P = 0.83; Figure 1B). The median PFS2 was 4.53 (95% CI: 3.93–7.00) months versus 5.77 (95% CI: 4.83–10.00) months (HR: 1.15, 95% CI: 0.71–1.88, P = 0.60; Figure 1C). The median tPFS was 13.80 (95% CI: 9.47–15.90) months versus 12.80 (95% CI: 9.83–16.30) months (HR: 0.90, 95% CI: 0.55–1.48; P = 0.67; Figure 1D). Overall survival rates at 12, 24, and 36 months were similar between the two groups. For F(S)FXm-AG versus AG-F(S)FXm, the OS rates at 12, 24 and 36 months were 62.07%, 19.62%, 7.13% versus 52%, 20.35%, 9.89%, respectively (Table 2), the PFS rates of first-line treatment at 6 and 12 months were 45.80%, 11.1% versus 39.7%, 10.7%, respectively (Table 2), the PFS rates of second-line treatment at 6, 12 and 24 months were 41.8%, 11.20%, 11.20 versus 47.92%, 11.94%, 5.97%, respectively (Table 2). The total PFS rates at 6, 12 and 24 months were 87.30%, 58.20%, 13.3% versus 89.38%, 54.07%, 7.08%, respectively (Table 2). Overall, these results indicated that both sequences of therapy based on AG and F(S)FX regimens offer comparable efficacy in terms of OS and PFS.
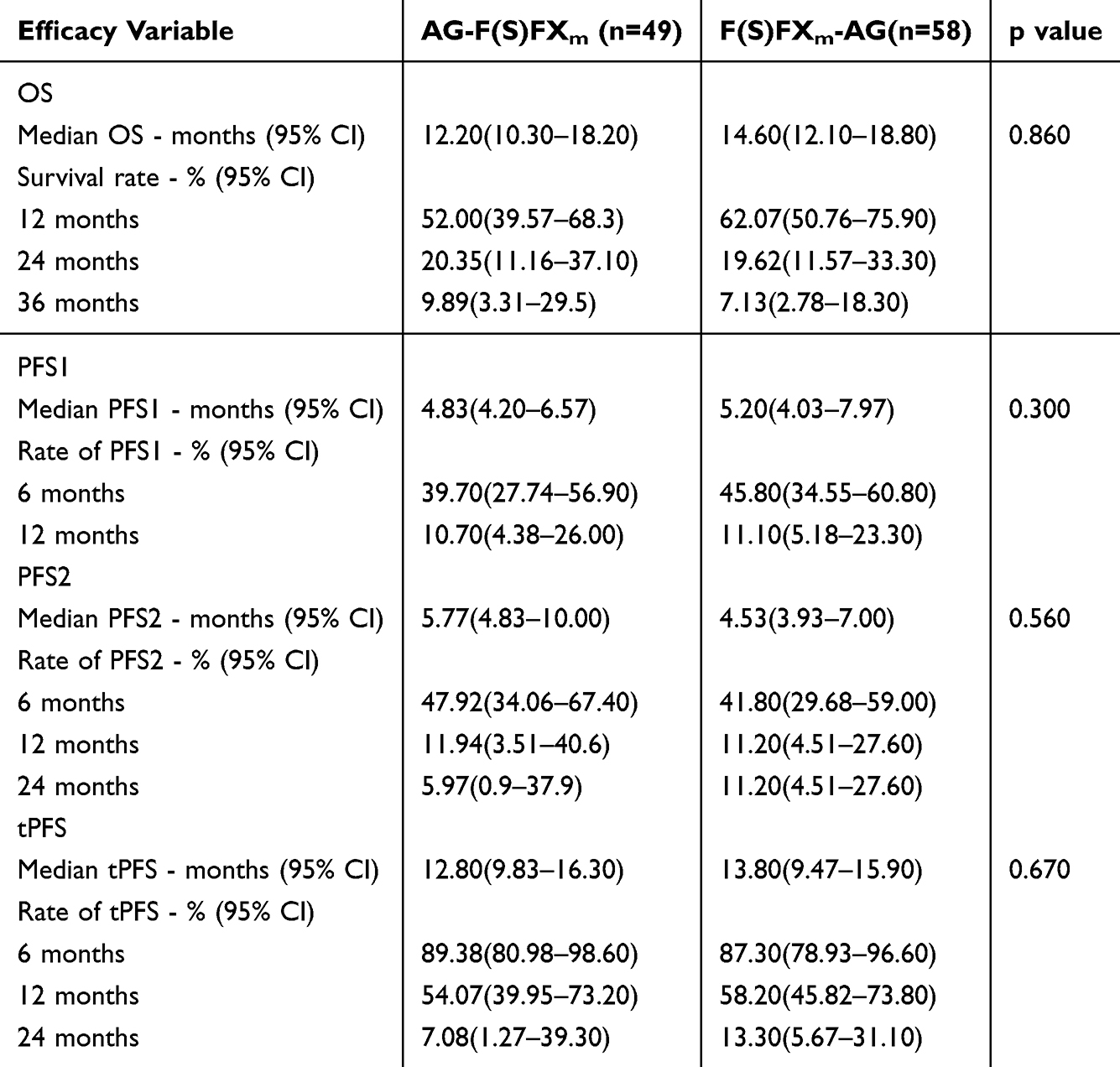 |
Table 2 OS and PFS of F(S)FXm-AG and AG-F(S)FXm |
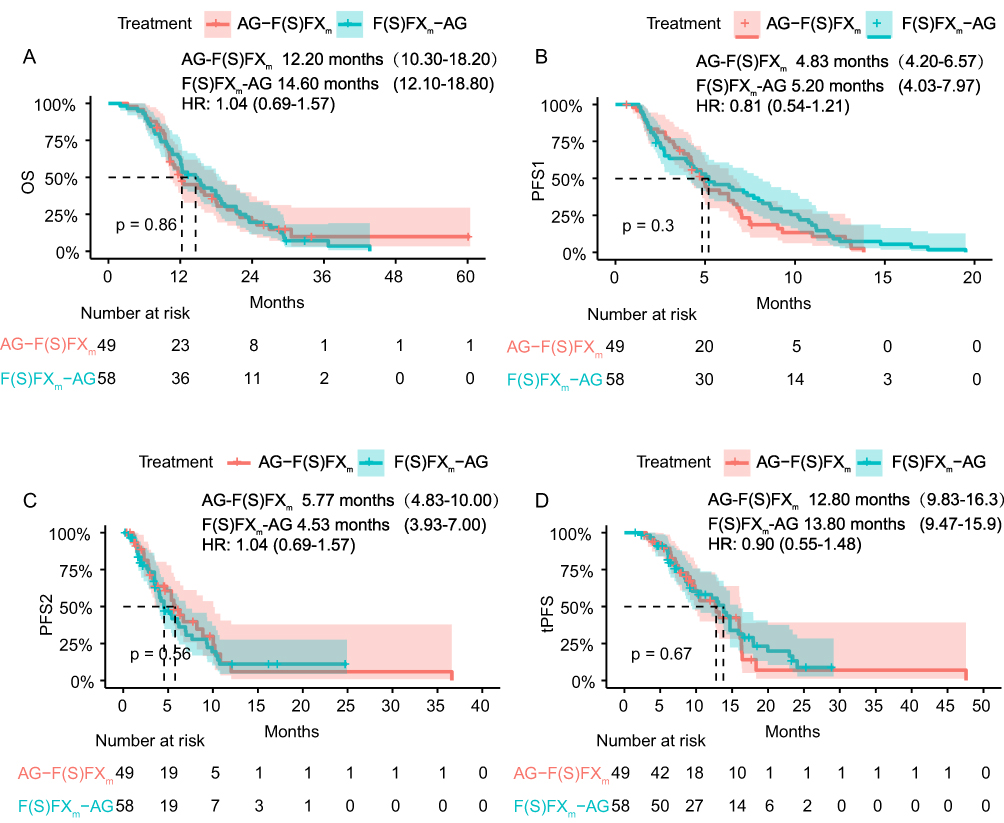 |
Figure 1 The overall survival (A) and progression free survival (B–D) between F(S)FXm-AG and AG-F(S)FXm; HR, hazard ratio; AG-F(S)FXm, AG (albumin-bound-paclitaxel plus gemcitabine) followed by FOLFIRINOX (fluorouracil, leucovorin, irinotecan, oxaliplatin) or SOXIRI (S-1, oxaliplatin, irinotecan); F(S)FXm-AG, FOLFIRINOX or SOXIRI followed by AG; OS, overall survival; PFS, progression-free survival. |
We also compared the response rate between the groups. For first-line therapy, the ORR was 25.9% for F(S)FXm-AG and 32.7% for AG-F(S)FXm (p = 0.577), while the DCR was 63.8% versus 79.6% (p = 0.114). For second-line treatment, the ORR for F(S)FXm-AG versus AG-F(S)FXm was 1.7% versus 10.2% (p = 0.139), and the DCR was 41.4% versus 53.1% (p = 0.311) (Table 3). The waterfall plots illustrated individual tumor size changes, showing the most favorable response were distributed similarly across the two strategies (Figure 2). In summary, the response rates did not differ significantly between AG and F(S)FXm treatment sequences.
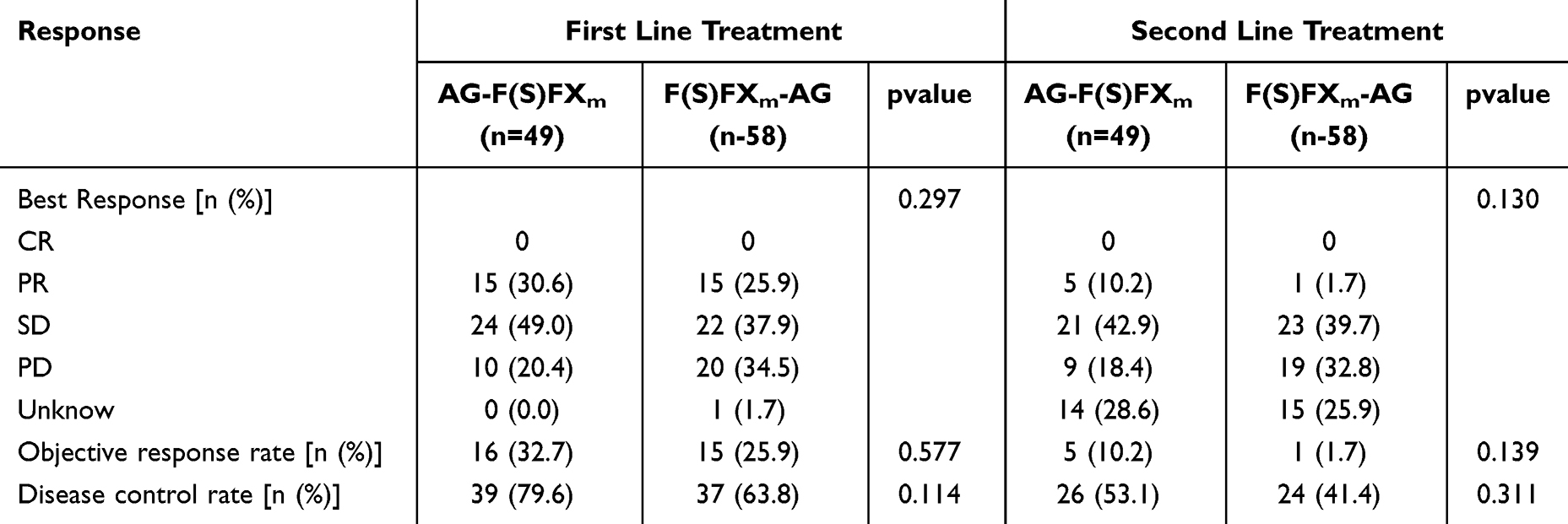 |
Table 3 Response of F(S)FXm-AG and AG-F(S)FXm |
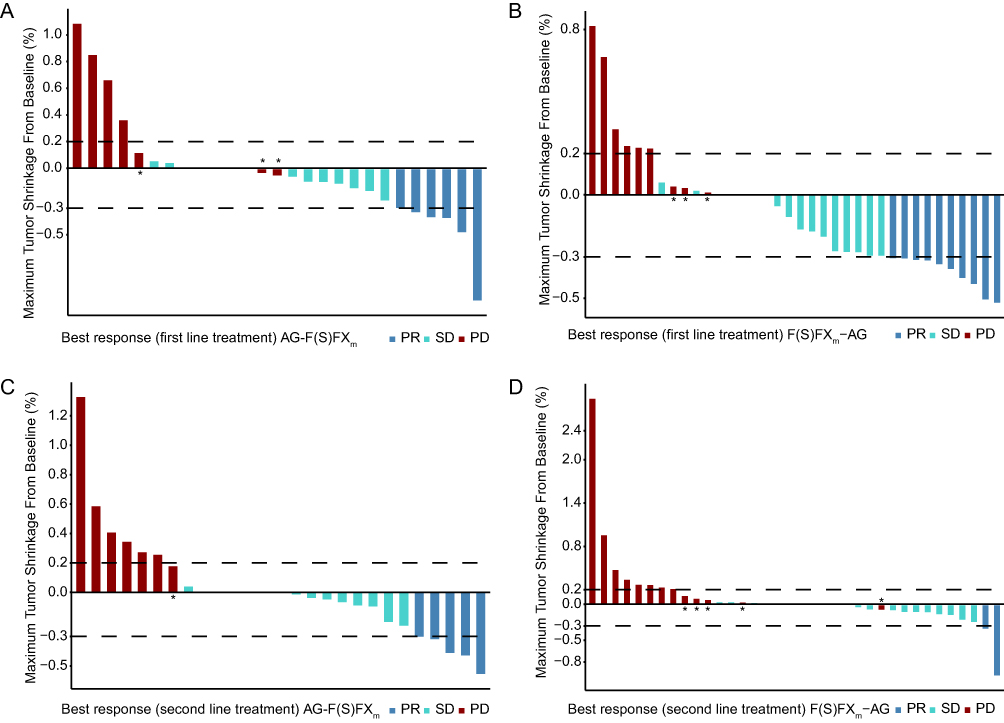 |
Figure 2 The best efficacy evaluation. The Waterfall plots of the best efficacy evaluation in the first-line treatment of AG-F(S)FXm group (A), and in first-line treatment of F(S)FXm-AG group (B). The Waterfall plots of the best efficacy evaluation of AG-F(S)FXm group (C), and F(S)FXm-AG group (D) in second-line treatment. *Patients who developed new metastatic sites even though the total diameter did not change by more than 20% during treatment. |
Subgroup Analysis
Subgroup analyses were conducted to find the potential baseline factors that predict the OS and PFS. Results are displayed in forest plots. For patients with history of biliary drainage (HR = 0.10, 95% CI: 0.01–0.96, P = 0.05), albumin smaller than 40 (HR = 0.16, 95% CI: 0.04–0.68, P = 0.01), DBIL larger than 7 (HR = 0.25, 95% CI: 0.07–0.91, P = 0.04), AST larger than 40 (HR = 0.34, 95% CI: 0.12–0.96, P = 0.04) and first-line treatment course smaller than 6 (HR = 0.56, 95% CI: 0.32–0.98, P = 0.04), F(S)FXm-AG appeared to provide a greater overall survival advantage compared to AG-F(S)FXm (Figure S1). For other subgroups, OS outcomes were comparable between the two regimens. In patients without distant lymph nodes metastases, F(S)FXm-AG may provide a greater PFS1 benefit compared to AG-F(S)FXm (HR = 0.55, 95% CI: 0.33–0.91, P = 0.02) (Figure S2). No significant differences were observed between groups in PFS2 and tPFS across subgroups (Figure S3, S4).
Treatment Toxicity Analysis
We conducted a comprehensive comparison of treatment-related toxicities between the two groups, as shown in Tables 4 and 5.
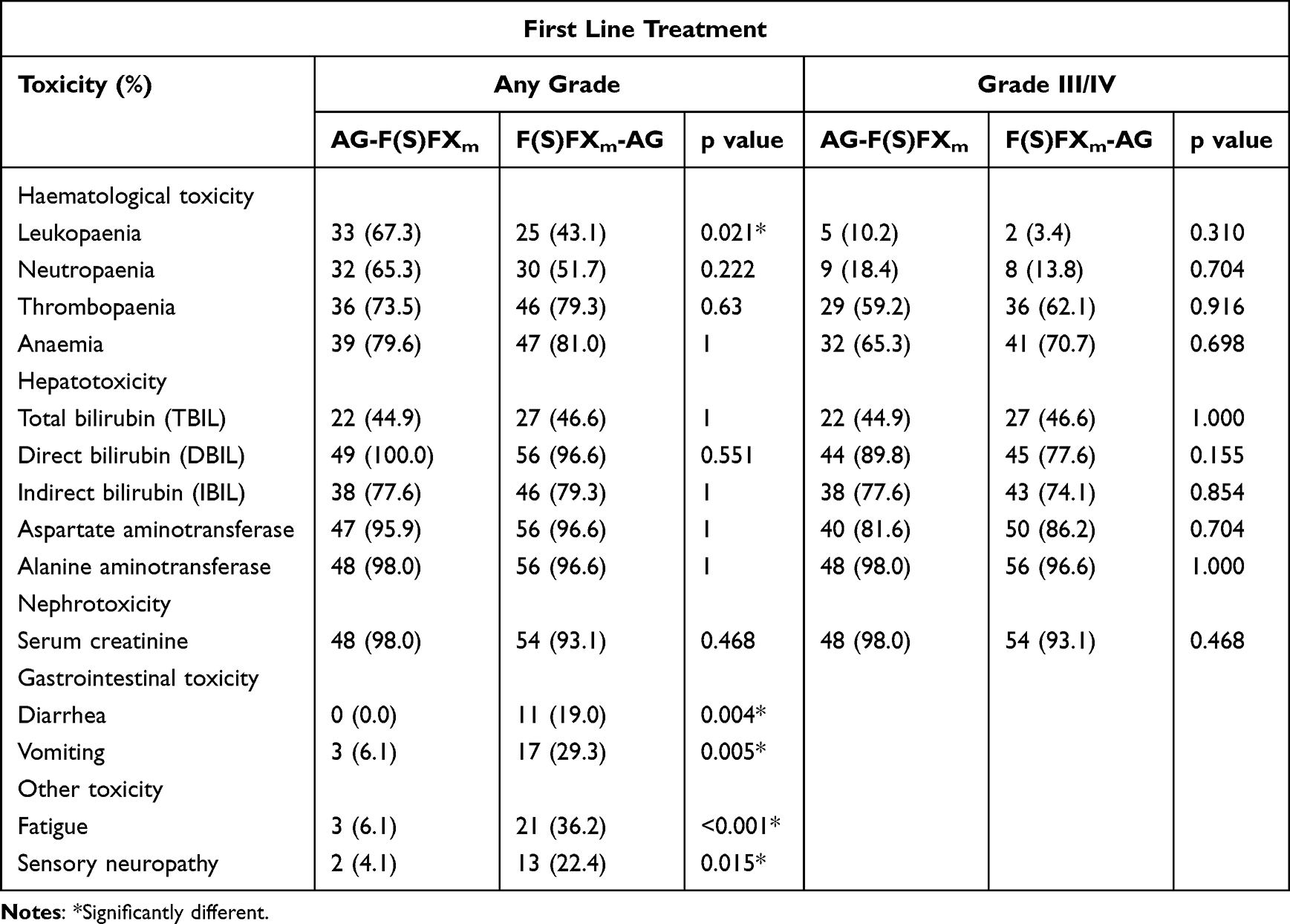 |
Table 4 Adverse Events of First-Line Treatment of AG-F(S)FXm and F(S)FXm-AG |
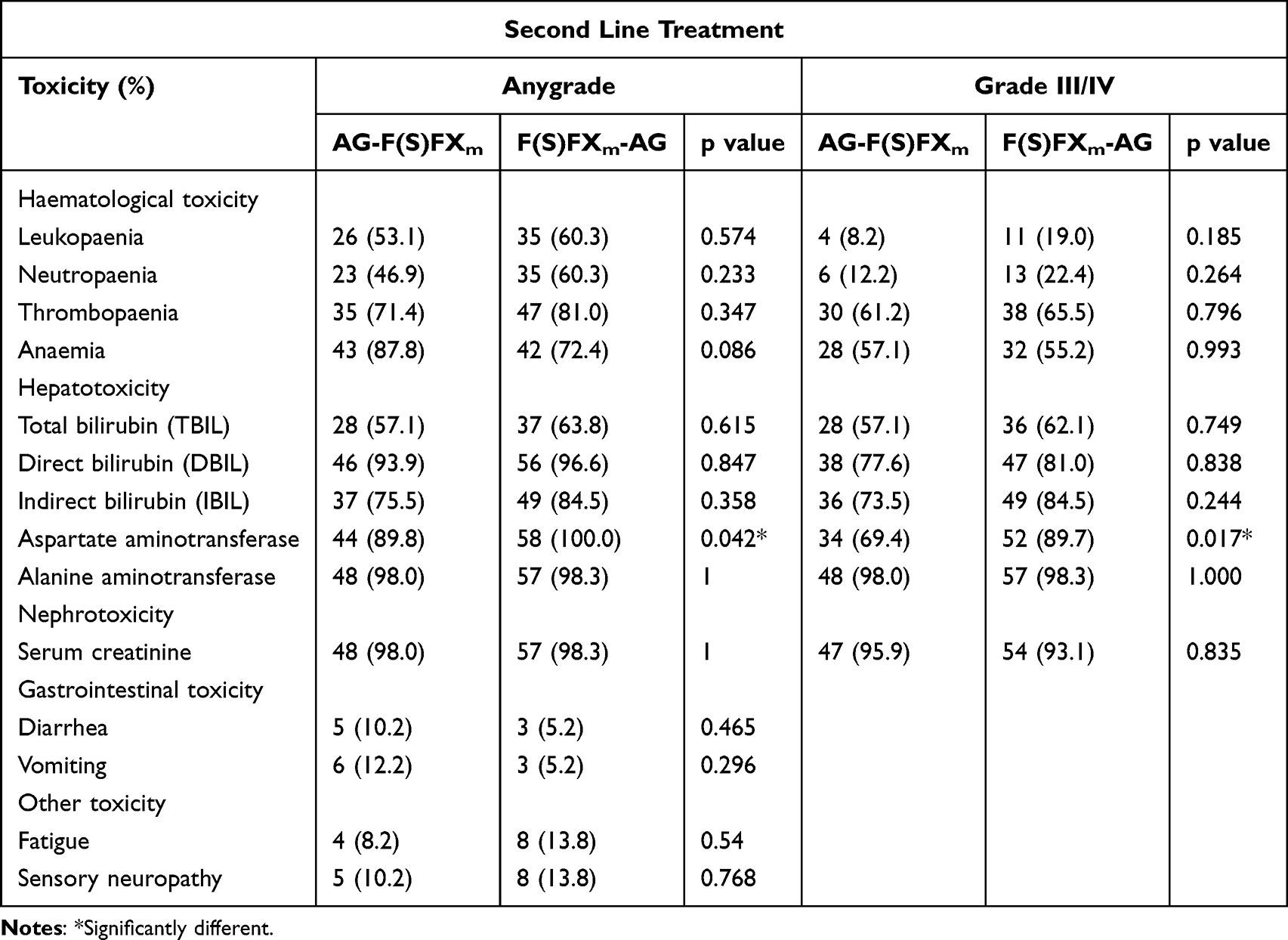 |
Table 5 Adverse Events of second-Line Treatment of AG-F(S)FXm and F(S)FXm-AG |
Hematological Toxicity
In the analysis of first-line treatment, patients in the AG-F(S)FXm group exhibited a notably higher rate of leukopenia of any grade compared to those in F(S)FXm-AG group (67.3% versus 43.1%, p = 0.021). However, no significant differences were observed between the two groups in terms of neutropenia, thrombocytopenia, and anemia. Similarly, the incidence of grade III/IV hematologic toxicities during first-line therapy showed no statistically significant variations. For second-line treatment, no significant differences were observed in any grade or grade III/IV hematological toxicities between the F(S)FXm-AG and AG-F(S)FXm groups.
Hepatotoxicity
During first-line treatment, the incidence of any grade or grade III/IV hepatotoxicity, as measured by bilirubin levels and liver transaminases, was comparable between the two groups. In second-line treatment, hepatotoxicity rates remained largely similar, with the exception of AST elevation. The F(S)FXm-AG group had a significantly higher incidence of both any-grade AST elevation (100% versus 89.8%, p = 0.042) and grade III/IV AST (89.7% versus 69.4%, p = 0.017) than AG-F(S)FXm group.
Nephrotoxicity
No significant differences in nephrotoxicity, as measured by serum creatinine levels (SCR), were observed between the AG-F(S)FXm and F(S)FXm-AG groups in either first-line or second-line treatment, regardless of toxicity grade.
Gastrointestinal Toxicity
In the first-line setting, gastrointestinal adverse events were significantly more frequent in the F(S)FXm-AG group. Specifically, diarrhea (19% versus 0%, p = 0.004) and vomiting (29.3% versus 6.1%, p = 0.005) occurred more common in this group. During second-line therapy, the incidence of gastrointestinal toxicities was similar between the two groups, with no statistically significant differences.
Other Toxicity
Fatigue and sensory neuropathy were significantly more prevalent in the F(S)FXm-AG group during first-line treatment (36.2% versus 6.1%, p < 0.001; 22.4% versus 4.1%, p = 0.015, respectively). However, fatigue and sensory neuropathy were not significantly different between the two groups during second-line therapy.
These findings demonstrated that certain hematological toxicities are more pronounced in the AG-F(S)FXm group during first-line treatment. In contrast, the F(S)FXm-AG group showed a higher incidence of gastrointestinal toxicities, fatigue and sensory neuropathy in the same setting. In the second-line setting, the toxicity profiles between the two regimens were generally comparable, with fewer significant differences.
Discussion
Previous studies have shown convincing results regarding AG and FFX as first- or second-line therapies in aPC. However, limited study has explored the superior sequencing of these two regimens. The SOXIRI regimen, comprising the oral fluoropyrimidine anti-cancer agent-S-1, oxaliplatin and irinotecan, is commonly used in Asian countries as an alternative to FFX or mFFX. Furthermore, previous studies, including a clinical trial conducted by our team in China, have indicated that SOXIRI offers comparable effectiveness and tolerability to FFX.16–18 Therefore, the current study compared the effectiveness and safety of two reverse sequence regimens, AG-F(S)FXm and F(S)FXm-AG, in patients with aPC. Given the limited therapeutic options available, understanding the nuances of these two sequential strategies is crucial. This study provides a comprehensive comparison based on both clinical outcomes and toxicity profiles.
No significant survival benefit was observed between the two treatment sequences, consistent with findings from two other retrospective studies, which also reported equivalent OS outcomes for sequential FOLFIRINOX (FFX) and AG treatment.19,20 Several retrospective studies have demonstrated that using second-line AG following FFX, or starting with first-line AG followed by FFX, results in comparable OS.21–26 Unlike previous studies, our analysis not only evaluated OS but also provided a more detailed assessment of disease progression and treatment-related toxicities. Additionally, we combined FFX and SOXIRI into a single category based on their similar components, efficacy, and toxicity. In clinical practice, the choice between FFXm and SOXIRI is typically guided by doctors, and also by the patient’s performance status and preference, which may lead to slight differences in their usage proportions. Although the proportion of patients receiving SOXIRI versus FFXm differed between the two treatment groups, additional analyses (data shown in Fig. S5) suggested that this variation did not significantly affect the overall findings. More importantly, our previously published study demonstrated that SOXIRI and modified FOLFIRINOX (FFXm) achieved comparable efficacy.16 Therefore, we believe that the different ratios of SOXIRI to FFXm between the two groups in this study likely had a minimal impact on the accuracy of the results.
While only one prior study suggested a trend favoring initial FFX over nab-p/gem in French population (in matched population, OS: 19 vs 9.5 months, P = 0.094; whole study population, OS: 21 versus 11 months, P = 0.11).27 Specifically, in Chinese clinical practice, modified FOLFIRINOX at lower doses is more commonly used due to better tolerability, while the AG regimen administration frequency also differs between the two studies. Additionally, our study involved a larger sample size and was conducted at a single, well-recognized center with strict and homogeneous clinical management, whereas the French study was a smaller, retrospective, multicenter analysis. These differences, along with variations in ethnicity, geographic location, treatment intensity, and supportive care strategies, as well as differences in study design and sample size, may contribute to the observed discrepancies. Nevertheless, considering that our results also showed a numerically longer survival (OS 14.6 versus 12.2 months) in the F(S)FXm-AG group compared to in the AG-F(S)FXm group, even though the difference was not statistically significant, we still recommend prioritizing F(S)FXm followed by AG in patients with good performance status.
In our study, 28.6% of patients in the AG-F(S)FXm group and 25.9% in the F(S)FXm-AG group did not undergo second-line efficacy assessment, potentially introducing bias in the PFS2 evaluation. However, since the proportions were comparable between the two groups, this potential bias is likely minimized in the direct comparison of treatment sequences. Despite these findings, prospective evidence remains limited, and further studies are needed to determine the optimal treatment sequence. Carrato A28 reported that sequential albumin-bound-P/G-mFOLFOX notably improved 12-month survival but increased treatment toxicity. Conversely, Rinaldi Y29 found that alternating gemcitabine plus nab-P with FOLFIRI.3 was both effective and tolerable. Nevertheless, prospective data on the use of FFX followed by AG are lacking, highlighting the need for future large-scale prospective trials to establish the most effective sequencing strategy.
Moreover, although no significant differences were observed in overall survival (OS) or progression-free survival (PFS) between the two sequential treatments, we also conducted subgroup analyses based on baseline characteristics to determine the potential benefit subgroup for any of regimens. The result showed that patients who received fewer than six cycles of first-line therapy were more likely to benefit from F(S)FXm-AG compared to AG-F(S)FXm. However, the difference in treatment cycles between the two groups may have influenced PFS1 outcomes, as multivariate analysis identified the number of cycles as an independent prognostic factor. Further analysis showed that patients with a history of biliary drainage, albumin smaller than 40 g/L, DBIL larger than 7 umol/L and AST larger than 40 U/L were more likely to benefit more from F(S)FXm-AG than AG-F(S)FXm. Several factors may explain these findings. Low albumin typically reflects poor nutritional status or systemic inflammation, whereas elevated DBIL and AST indicate biliary obstruction or liver dysfunction. Starting with the more intensive triplet regimen (F(S)FXm) may result in more effective early tumor debulking, potentially improving outcomes in patients with compromised liver function. Additionally, biliary obstruction or liver dysfunction can impair the metabolism and excretion of gemcitabine and albumin-bound-paclitaxel, resulting in impaired bioactivation of a prodrug and leading to reduced effectiveness and increased toxicity.30,31 This may result in treatment interruptions or reduced patient tolerance, ultimately compromising therapeutic efficacy. Furthermore, albumin-bound-paclitaxel is a formulation of paclitaxel bound to human serum albumin, forming nanoparticles that enter the tumor microenvironment via gp60-mediated endothelial transcytosis, and is primarily metabolized by enzymes such as CYP2C8 and CYP3A4.32 Low albumin levels may impair the transport and metabolism of albumin-bound paclitaxel, thereby reducing its antitumor efficacy. Importantly, patients with low albumin may tolerate F(S)FXm-AG better when given earlier, before further deterioration in performance status. This may partly explain the inferior outcomes observed in the AG-F(S)FXm sequence among these subgroups. In contrast, patients with grade II tumors appeared to derive greater PFS benefit from the AG-F(S)FXm sequence compared to F(S)FXm-AG. These results may inform clinical decision-making to some extent. However, the relatively small sample sizes in certain subgroups and the wide confidence intervals for some hazard ratios limit the statistical power and robustness of these findings. Thus, these exploratory results should be interpreted with caution, and validation in larger, prospective studies is warranted.
We further assessed the toxicity profiles for both sequential treatments, focusing on hematological toxicity, hepatotoxicity, nephrotoxicity, gastrointestinal toxicity, and other adverse effects. Previous studies have shown that AG, FFX and SOXIRI differ in their toxicity profiles despite similar efficacy. Consistent with previous reports,7,8,11,13,14,16,33–37 our study also found notable differences in toxicity between the AG-F(S)FXm and F(S)FXm-AG. Specifically, patients receiving AG as first-line treatment experienced higher incidences of leukopenia and neutropenia, whereas those who received F(S)FXm first were more likely to suffer from gastrointestinal toxicities and sensory neuropathy. These differences may be attributed to variations in drug sequencing, pharmacokinetics, cumulative toxicity, and the toxicity spectrum of each regimen. F(S)FXm, being more dose-intensive and comprising multiple cytotoxic agents (oxaliplatin, irinotecan, and fluorouracil), is more likely to induce gastrointestinal and neurologic toxicities. In contrast, AG tends to result in myelosuppression but is generally better tolerated in terms of non-hematologic side effects. The elevation of AST observed during second-line treatment in the F(S)FXm-AG group may be attributed to cumulative hepatic toxicity from prior chemotherapy, particularly considering the known hepatotoxic profiles of agents like oxaliplatin and irinotecan. Additionally, tumor progression or the presence of liver metastases in some patients may have further contributed to the increased AST levels. These side effects can severely impact patients’ quality of life and are critical considerations in treatment selection. Clinicians should carefully weigh efficacy against toxicity, patient comorbidities, and individual tolerance. For example, initiating treatment with AG may be more appropriate for frail patients or those with preexisting neuropathy, given its lower neurotoxicity risk. Conversely, for patients at high risk for hematologic complications or infections, first-line F(S)FXm may be more favorable. Ultimately, understanding the distinct toxicity patterns of each regimen is essential for guiding personalized treatment strategies that balance therapeutic efficacy with safety, thereby optimizing patient outcomes.
Nevertheless, several limitations of this study should be acknowledged. First, it was a retrospective analysis conducted at a single institution, which may introduce selection bias. Additionally, the relatively small sample size limits the statistical power and generalizability of the findings. Therefore, larger, multicenter prospective studies are warranted to validate these results. Future research should aim to refine treatment protocols by incorporating predictive biomarkers for response and toxicity, thereby enabling more personalized therapy in advanced pancreatic cancer (aPC). Furthermore, investigating the integration of novel agents, including targeted therapies or immunotherapies, may offer additional opportunities to improve patient outcomes.
Conclusion
This study reveals that both AG-F(S)FXm and F(S)FXm-AG sequential regimens exhibit similar therapeutic efficacy in advanced pancreatic cancer (aPC) management. Clinical decision-making should prioritize individualized treatment strategies based on comprehensive toxicity assessments and patient-specific clinical characteristics. Future investigations should focus on protocol optimization and the development of personalized therapeutic approaches to enhance clinical outcomes in aPC patients.
Ethics Statement
The study was approved by the Institutional Review Board of Sun Yat-sen University Cancer Center and was conducted in accordance with the Declaration of Helsinki, relevant laws, and institutional guidelines. Informed consent was obtained from all participants.
Acknowledgments
Silan Huang and Lingli Huang are co-first authors for this study. The authors express their gratitude to all patients, physicians, and study teams involved in this research.
Author Contributions
All authors contributed significantly to the conception and design, data acquisition, or data analysis and interpretation, participated in the drafting of the article or critically revising it for important intellectual content, agreed to submit to the current journal, gave final approval for the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Natural Science Foundation of Guangdong Provincial (grant no. 2023A1515010783 and 2021A1515012368).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet. 2020;395(10242):2008–2020. doi:10.1016/S0140-6736(20)30974-0
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. Ca a Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
4. Grossberg AJ, Chu LC, Deig CR, et al. Multidisciplinary standards of care and recent progress in pancreatic ductal adenocarcinoma. Ca a Cancer J Clin. 2020;70(5):375–403. doi:10.3322/caac.21626
5. Bednar F, Di Magliano M P. Chemotherapy and tumor evolution shape pancreatic cancer recurrence after resection. Cancer Discov. 2020;10(6):762–764. doi:10.1158/2159-8290.CD-20-0359
6. Tempero MA, Malafa MP, Al-Hawary M, et al. Pancreatic adenocarcinoma, version 2.2021, NCCN clinical practice guidelines in oncology. JNCCN. 2021;19:439–457.
7. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
8. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. doi:10.1056/NEJMoa1011923
9. Burris HA 3rd, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J clin oncol. 1997;15(6):2403–2413. doi:10.1200/JCO.1997.15.6.2403
10. Wang ZQ, Zhang F, Deng T, et al. The efficacy and safety of modified FOLFIRINOX as first-line chemotherapy for Chinese patients with metastatic pancreatic cancer. Cancer commun. 2019;39(1):26. doi:10.1186/s40880-019-0367-7
11. Li X, Ma T, Zhang Q, et al. Modified-FOLFIRINOX in metastatic pancreatic cancer: a prospective study in Chinese population. Cancer Lett. 2017;406:22–26. doi:10.1016/j.canlet.2017.07.012
12. Stein SM, James ES, Deng Y, et al. Final analysis of a phase II study of modified FOLFIRINOX in locally advanced and metastatic pancreatic cancer. Br J Cancer. 2016;114(7):737–743. doi:10.1038/bjc.2016.45
13. Akahori T, Sho M, Yanagimoto H, et al. Phase II study of the triple combination chemotherapy of SOXIRI (S-1/oxaliplatin/irinotecan) in patients with unresectable pancreatic ductal adenocarcinoma. Oncologist. 2019;24(6):749–e224. doi:10.1634/theoncologist.2018-0900
14. Nie K, Zhang L, You Y, et al. Irinotecan combined with oxaliplatin and S-1 in patients with metastatic pancreatic adenocarcinoma: a single-arm, three-centre, prospective study. Therapeut Adv Med Oncol. 2020;12:1758835920970843. doi:10.1177/1758835920970843
15. Wang F, Wang Y, Ren C, et al. Phase II study of SOXIRI (S-1/oxaliplatin/irinotecan) chemotherapy in patients with unresectable pancreatic ductal adenocarcinoma. Pancreatology. 2024;24(2):241–248. doi:10.1016/j.pan.2023.12.008
16. Li X, Huang J, Wang F, et al. Efficacy and safety of SOXIRI versus mFOLFIRINOX in advanced pancreatic cancer. Therapeut Adv Med Oncol. 2023;15:17588359231186029. doi:10.1177/17588359231186029
17. Kawamoto Y, Nakatsumi H, Harada K, et al. A phase I trial of oxaliplatin, irinotecan, and S-1 combination therapy (OX-IRIS) as chemotherapy for unresectable pancreatic cancer (HGCSG 1403). Oncologist. 2021;26(10):e1675–e1682. doi:10.1002/onco.13838
18. Yanagimoto H, Satoi S, Sho M, et al. Phase I study assessing the feasibility of the triple combination chemotherapy of SOXIRI (S-1/oxaliplatin/irinotecan) in patients with unresectable pancreatic ductal adenocarcinoma. Cancer Chemother Pharmacol. 2016;77(1):35–41. doi:10.1007/s00280-015-2928-z
19. Vogl UM, Andalibi H, Klaus A, et al. Nab-paclitaxel and gemcitabine or FOLFIRINOX as first-line treatment in patients with unresectable adenocarcinoma of the pancreas: does sequence matter? BMC Cancer. 2019;19(1):28. doi:10.1186/s12885-018-5240-6
20. Baron MK, Wang X, Nevala-Plagemann C, Moser JC, Haaland B, Garrido-Laguna I. Survival outcomes based on sequence of therapy using FOLFIRINOX and nab-paclitaxel + gemcitabine in metastatic pancreatic ductal adenocarcinoma. Pancreas. 2021;50(6):796–802. doi:10.1097/MPA.0000000000001844
21. Portal A, Pernot S, Tougeron D, et al. Nab-paclitaxel plus gemcitabine for metastatic pancreatic adenocarcinoma after Folfirinox failure: an AGEO prospective multicentre cohort. Br J Cancer. 2015;113:989–995.
22. Hayuka K, Okuyama H, Murakami A, et al. Gemcitabine plus nab-paclitaxel as second-line chemotherapy following FOLFIRINOX in patients with unresectable pancreatic cancer: a single-institution, retrospective analysis. Chemotherapy. 2021;66(3):58–64. doi:10.1159/000517244
23. Nguyen KT, Kalyan A, Beasley HS, et al. Gemcitabine/nab-paclitaxel as second-line therapy following FOLFIRINOX in metastatic/advanced pancreatic cancer-retrospective analysis of response. J gastrointest oncol. 2017;8(3):556–565. doi:10.21037/jgo.2017.01.23
24. Zhang H, Kellett C, Lambert P, Kim CA. Efficacy and tolerability of second-line nab-paclitaxel and gemcitabine after failure of first-line FOLFIRINOX for advanced pancreas cancer: a single-institution experience. Clin Colorectal Cancer. 2018;17(3):e451–e456. doi:10.1016/j.clcc.2018.03.003
25. Assenat E, de la Fouchardière C, Portales F, et al. Sequential first-line treatment with nab-paclitaxel/gemcitabine and FOLFIRINOX in metastatic pancreatic adenocarcinoma: GABRINOX phase Ib-II controlled clinical trial. ESMO open. 2021;6(6):100318. doi:10.1016/j.esmoop.2021.100318
26. Kunzmann V, Siveke JT, Algül H, et al. Nab-paclitaxel plus gemcitabine versus nab-paclitaxel plus gemcitabine followed by FOLFIRINOX induction chemotherapy in locally advanced pancreatic cancer (NEOLAP-AIO-PAK-0113): a multicentre, randomised, Phase 2 trial. Lancet Gastroenterol Hepatol. 2021;6(2):128–138. doi:10.1016/S2468-1253(20)30330-7
27. Williet N, Saint A, Pointet AL, et al. Folfirinox versus gemcitabine/nab-paclitaxel as first-line therapy in patients with metastatic pancreatic cancer: a comparative propensity score study. Ther Adv Gastroenterol. 2019;12:1756284819878660. doi:10.1177/1756284819878660
28. Carrato A, Pazo-Cid R, Macarulla T, et al. Nab-paclitaxel plus gemcitabine and FOLFOX in metastatic pancreatic cancer. NEJM Evidence. 2024;3:EVIDoa2300144.
29. Rinaldi Y, Pointet AL, Khemissa Akouz F, et al. Gemcitabine plus nab-paclitaxel until progression or alternating with FOLFIRI.3, as first-line treatment for patients with metastatic pancreatic adenocarcinoma: the federation francophone de cancérologie digestive-PRODIGE 37 randomised phase II study (FIRGEMAX). Eur J Cancer. 2020;136:25–34. doi:10.1016/j.ejca.2020.05.018
30. Noventa S, Cherri S, Zaniboni A. Chemotherapy in advanced pancreatic cancer with hyperbilirubinemia. Digest Med Res. 2020;3:18. doi:10.21037/dmr.2020.04.04
31. Vogel A, Kullmann F, Kunzmann V, et al. Patients with advanced pancreatic cancer and hyperbilirubinaemia: review and german expert opinion on treatment with nab-paclitaxel plus gemcitabine. Oncology Res Treatment. 2015;38(11):596–603. doi:10.1159/000441310
32. Desai N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxel concentrations, and endothelial cell transport of cremophor-free, albumin-bound paclitaxel, ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res. 2006;12(4):1317–1324. doi:10.1158/1078-0432.CCR-05-1634
33. Sadaka S, Iwashita T, Fujii H, et al. Impact of first-line FOLFIRINOX-induced peripheral neuropathy on the efficacy of second-line GnP in patients with unresectable advanced pancreatic cancer. J Clin Med. 2022;12(1):11. doi:10.3390/jcm12010011
34. Pitarokoili K, Höffken N, Lönneker N, et al. Prospective study of the clinical, electrophysiologic, and sonographic characteristics of oxaliplatin-induced neuropathy. J Neuroimag. 2019;29(1):133–139. doi:10.1111/jon.12557
35. Kim S, Signorovitch JE, Yang H, et al. Comparative effectiveness of nab-paclitaxel plus gemcitabine vs FOLFIRINOX in metastatic pancreatic cancer: a retrospective nationwide chart review in the United States. Advances in Therapy. 2018;35(10):1564–1577. doi:10.1007/s12325-018-0784-z
36. Kang J, Hwang I, Yoo C, et al. Nab-paclitaxel plus gemcitabine versus FOLFIRINOX as the first-line chemotherapy for patients with metastatic pancreatic cancer: retrospective analysis. Invest New Drugs. 2018;36(4):732–741. doi:10.1007/s10637-018-0598-5
37. Chiorean EG, Cheung WY, Giordano G, Kim G, Al-Batran SE. Real-world comparative effectiveness of nab-paclitaxel plus gemcitabine versus FOLFIRINOX in advanced pancreatic cancer: a systematic review. Therapeut Adv Med Oncol. 2019;11:1758835919850367. doi:10.1177/1758835919850367
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.