")
Back to Journals » Infection and Drug Resistance » Volume 15
Efficacy and Safety of Ceftaroline Fosamil in Hospitalized Patients with Community-Acquired Pneumonia in China: Subset Analysis of an International Phase 3 Randomized Controlled Trial
Authors Zhuo C, Huang Y, Liu W, Xu JF , Zhu WY , Stone GG, Yan JL, Mohamed N
Received 3 October 2021
Accepted for publication 20 January 2022
Published 23 February 2022 Volume 2022:15 Pages 605—617
DOI https://doi.org/10.2147/IDR.S342558
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Chao Zhuo,1 Yijiang Huang,2 Wenyuan Liu,3 Jin-Fu Xu,4 Wei Yun Zhu,5 Gregory G Stone,6 Jean Li Yan,7 Naglaa Mohamed8
1State Key Laboratory of Respiratory Disease, National Clinical Research Center of Respiratory Diseases, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Respiratory Clinical Medical Center, Hainan Cancer Hospital, Hainan, People’s Republic of China; 3Respiratory Department, Sichuan Provincial People’s Hospital, Chengdu, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 5Medical Department, Pfizer Investment Co. Ltd., Beijing, People’s Republic of China; 6Biopharmaceuticals Group, Pfizer Inc., Groton, CT, USA; 7Biopharmaceuticals Group, Pfizer Inc., Cambridge, MA, USA; 8Biopharmaceuticals Group, Pfizer Inc., New York, NY, USA
Correspondence: Chao Zhuo, Email [email protected]
Background: Ceftaroline fosamil has demonstrated superior clinical efficacy versus ceftriaxone for hospitalized adults with moderate-to-severe community-acquired pneumonia (CAP) in a Phase 3 trial in Asia and in a meta-analysis of three trials in Asia, North America, and Europe. Efficacy and safety outcomes for the subset of patients in China in the ASIA CAP trial were analyzed to determine if the same conclusions hold in the China subpopulation.
Methods: Hospitalized adults with Pneumonia Outcomes Research Team risk class III–IV CAP were randomized (1:1) to receive either intravenous ceftaroline fosamil 600 mg every 12 h or ceftriaxone 2 g every 24 h for 5– 7 days. The primary efficacy variable was clinical response at test-of-cure (TOC) in the clinically evaluable (CE) population. Secondary endpoints included microbiological responses and safety.
Results: Of 302 patients randomized in China, 205 were included in the CE population. Clinical cure rates at TOC were 80/105 (76.2%) for ceftaroline fosamil and 61/100 (61.0%) for ceftriaxone (difference 15.2%, 95% CI 2.5, 27.6), thereby meeting predefined non-inferiority and superiority criteria for the overall study. Subgroup analyses of the primary endpoint demonstrated consistency of favourable efficacy of ceftaroline fosamil across age groups, Pneumonia Outcomes Research Team risk classes and CURB-65 scores. Microbiological responses were presumed from clinical outcomes. Adverse events were consistent with the study treatments’ known safety profiles.
Conclusion: The China subset results are consistent with the overall study population, despite the smaller sample size. Ceftaroline fosamil was both non-inferior and superior to ceftriaxone for empiric treatment of Chinese patients with moderate-to-severe CAP.
Trial Registration: ClinicalTrials.gov identifier NCT01371838.
Keywords: ceftriaxone, CURB-65, treatment outcomes, clinical trial
Introduction
Community-acquired pneumonia (CAP) is among the leading global causes of morbidity and mortality.1 Common CAP pathogens include Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae and, to a lesser extent, Pseudomonas aeruginosa, Klebsiella pneumoniae and Acinetobacter baumannii.1–5 Atypical pathogens, such as Chlamydophila pneumoniae, Mycoplasma pneumoniae and Legionella pneumophila, can also be implicated in CAP.2,3,6
Antimicrobial resistance profiles and epidemiology of CAP pathogens vary geographically and can change over time.2 Although some differences in pathogen epidemiology and susceptibility/resistance profiles have been reported for CAP pathogens in Asian countries including China versus Europe and North America,2,7–11 interpretation is limited by scarcity of data, the low rate of isolation of CAP pathogens in practice, and variability in the capabilities of available diagnostic methods.8 Accordingly, antimicrobial therapy for CAP is generally initiated empirically and guided by local pathogen susceptibility profiles and patients’ clinical status, including assessments of disease severity and risk stratification. Guidelines for empiric antibiotic therapy of moderate-to-severe CAP in Europe,12 Asia2,13–15 and the US16 include broad-spectrum β-lactam/cephalosporins with or without coverage for atypical pathogens. Ceftaroline fosamil, an intravenous cephalosporin, is approved for the treatment of CAP in Europe (in adults and paediatric patients of all ages, from birth onwards)17 and the US (in adults and in paediatric patients aged ≥2 months).18 In adults, these approvals were based on data from two Phase 3 trials in hospitalized patients with moderate-to severe CAP (FOCUS 1 and 2), which demonstrated non-inferiority of ceftaroline fosamil versus ceftriaxone, a standard treatment in this setting.19,20 Another similar Phase 3 trial in Asian patients (ASIA CAP) demonstrated superiority of ceftaroline fosamil versus ceftriaxone,21 and this was also confirmed in a meta-analysis of the three trials.22 Population pharmacokinetic (PK) modelling incorporating patient PK data from the ceftaroline clinical development programme, including the above trials in patients with CAP, has demonstrated high probability (90%) of pharmacodynamic target attainment for standard ceftaroline fosamil doses in adults with CAP against common CAP pathogens, and showed that patient factors including age and race had a negligible impact on ceftaroline PK (in contrast, renal function is a key factor affecting clearance of ceftaroline necessitating dose adjustments for patients with estimated creatinine clearance <50 mL/min).23,24 The ASIA CAP trial randomized 771 patients in China, India, South Korea, Taiwan, and Vietnam, approximately 36% of whom were enrolled at study sites in China.21
In the FOCUS 1 and 2 and ASIA CAP trials, a key patient inclusion criterion was Pneumonia Outcomes Research Team (PORT) class III–IV CAP, corresponding to a pneumonia severity index (PSI) severity classification of moderate (III) or severe (IV).25 However, in clinical practice, the CURB-65 score (calculated as one point each for confusion, urea >7 mmol/L, respiratory rate >30/min, low blood pressure [systolic <90 mm Hg or diastolic <60 mm Hg], and age ≥65 years)26 is more widely used and easier to implement than PSI/PORT, especially in China.16,27 This analysis of the ceftaroline fosamil ASIA CAP trial focuses on clinical and microbiological responses and safety in the subset of patients treated at study sites in China, including an exploratory evaluation of clinical efficacy by baseline CURB-65 score.
Methods
Full details of the Phase 3 trial of ceftaroline fosamil versus ceftriaxone in Asian patients with CAP (ASIA CAP; ClinicalTrials.gov identifier NCT01371838), including study methods and efficacy and safety data for the overall study population, have been reported.21
Patients, Treatments, and Assessments
Full inclusion and exclusion criteria are available in the primary study publication.21 In brief, hospitalized adult patients with moderate-to-severe (PORT class III–IV) CAP (confirmed by clinical signs and symptoms and evidence of pneumonia on chest X-ray) were eligible for inclusion provided they did not have evidence of non-community acquired pathogens or viral, fungal or mycobacterial infection, documented non-infectious causes of pulmonary infiltrates, or pleural empyema.
Following baseline screening and eligibility assessments, which included clinical signs and symptoms of CAP, chest X-rays, PORT score evaluations and sputum and/or pleural fluid and blood samples for microbiological analysis. Eligible patients were randomized (1:1) to receive either intravenous ceftaroline fosamil 600 mg every 12 h or ceftriaxone 2 g every 24 h for 5–7 days and were followed-up for 21–35 days after the last dose of study drug. Clinical signs and symptoms of CAP were monitored daily during the study treatment period, and microbiological samples were obtained as clinically indicated. Efficacy evaluations included assessment of clinical and microbiological responses at end-of-treatment (EOT) and at the test-of-cure (TOC; 8–15 days after last dose of study drug) and late-follow-up (LFU; 21–35 days after last dose of study drug) visits. Safety assessments included adverse event (AE) reporting, clinical chemistry evaluations and vital signs monitoring up to the LFU visit.
Statistical Methods
The primary efficacy endpoint was the proportion of patients with clinical cure (ie, total resolution of all signs and symptoms of CAP, or improvement to such an extent that further antimicrobial therapy is not necessary) at the TOC visit in the clinically evaluable (CE) population. In the prespecified analysis plan for the overall study, non-inferiority of ceftaroline fosamil to ceftriaxone was to be inferred if the lower limit of the two-sided 95% confidence interval (CI) for the difference in clinical cure rates (clinical cure rate in the ceftaroline group minus clinical cure rate in the ceftriaxone group) was >–10%21 (definitions of the analysis populations and clinical outcomes categories are included in the Supplementary Methods). If non-inferiority was established, ceftaroline fosamil was determined to be superior to ceftriaxone if the lower limit of the 95% CI for the difference was >0%.
Predefined subgroup analyses of the primary efficacy endpoint explored the effects of various baseline characteristics including age, renal function, PORT risk class and prior antimicrobial use on treatment outcomes. Given the widespread use of CURB-65 scores in China, a post hoc exploratory subgroup analysis of the primary efficacy endpoint for the China subset was done for baseline CURB-65 scores derived from information collected in case report forms (confusion, blood urea nitrogen >19 mg/dL [>7 mmol/L], respiratory rate ≥30 beats per minute, systolic blood pressure <90 mmHg or diastolic blood pressure ≤60 mmHg, and age ≥65 years). Secondary efficacy endpoints analysed for the overall study and the China subset included clinical cure rates at TOC in the modified intention-to-treat (MITT), microbiological modified intention-to-treat (mMITT) and microbiologically evaluable (ME) populations; per-pathogen clinical cure and microbiological response rates at TOC in the ME population; clinical relapse rate at the LFU visit in the CE population; and microbiological re-infection/recurrence rate at the LFU visit in the ME population.
Results
Patient Population
The ASIA CAP trial was carried out between December 2011 and April 2013 at 64 study sites in China, India, Korea, Vietnam, and Taiwan.21 In China, a total of 23 participating sites randomized 302 patients (Figure 1). Following Good Clinical Practice (GCP) inspection findings (in July 2018), the sponsor conducted a sensitivity analysis of the primary efficacy endpoint for the overall study excluding all patients randomized at a single study site in China (site 1314; n = 31). For the current analyses, data for all patients randomized at site 1314 were excluded from efficacy analyses but retained in safety summaries. The safety population for the China subset (including site 1314) included 300 patients, and the MITT mMITT, CE and ME populations (excluding site 1314) included 269, 68, 205 and 54 patients, respectively (Figure S1).
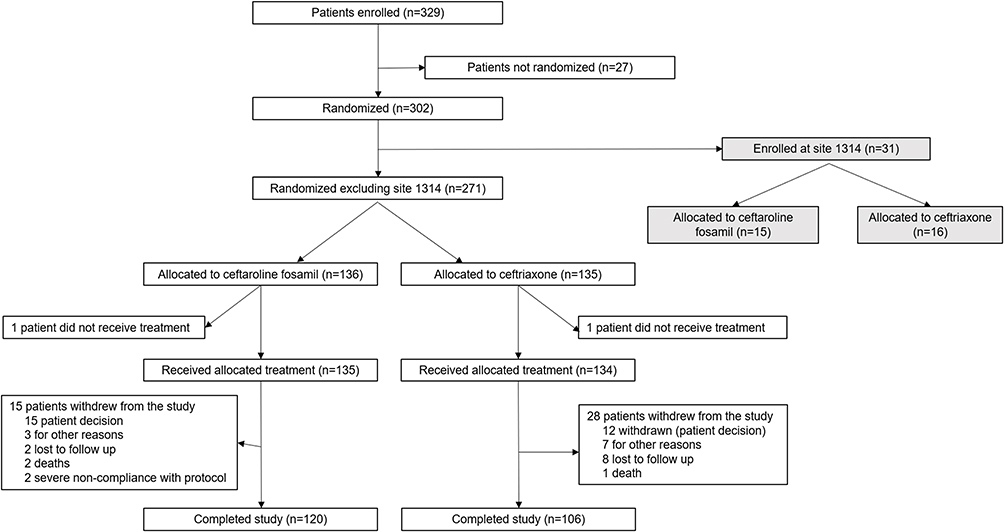 |
Figure 1 Patient disposition in the China subset. Notes: Due to GCP inspection findings in China (in July 2018), data for site 1314 were excluded from the efficacy analyses but retained in safety summaries. |
Baseline and demographic characteristics for patients in the China subset were similar across treatment groups (Table 1). The median (range) age was 69 (21–94) years, approximately 70% of patients were male, and >75% were PORT risk class III and had CURB-65 scores of 2 or 3. Fewer than 7% of patients received prior antibiotics in the 96 h before randomization; the most common were cefuroxime sodium (four patients) in the ceftaroline fosamil group, and cefuroxime sodium and piperacillin-tazobactam (two patients each) in the ceftriaxone group.
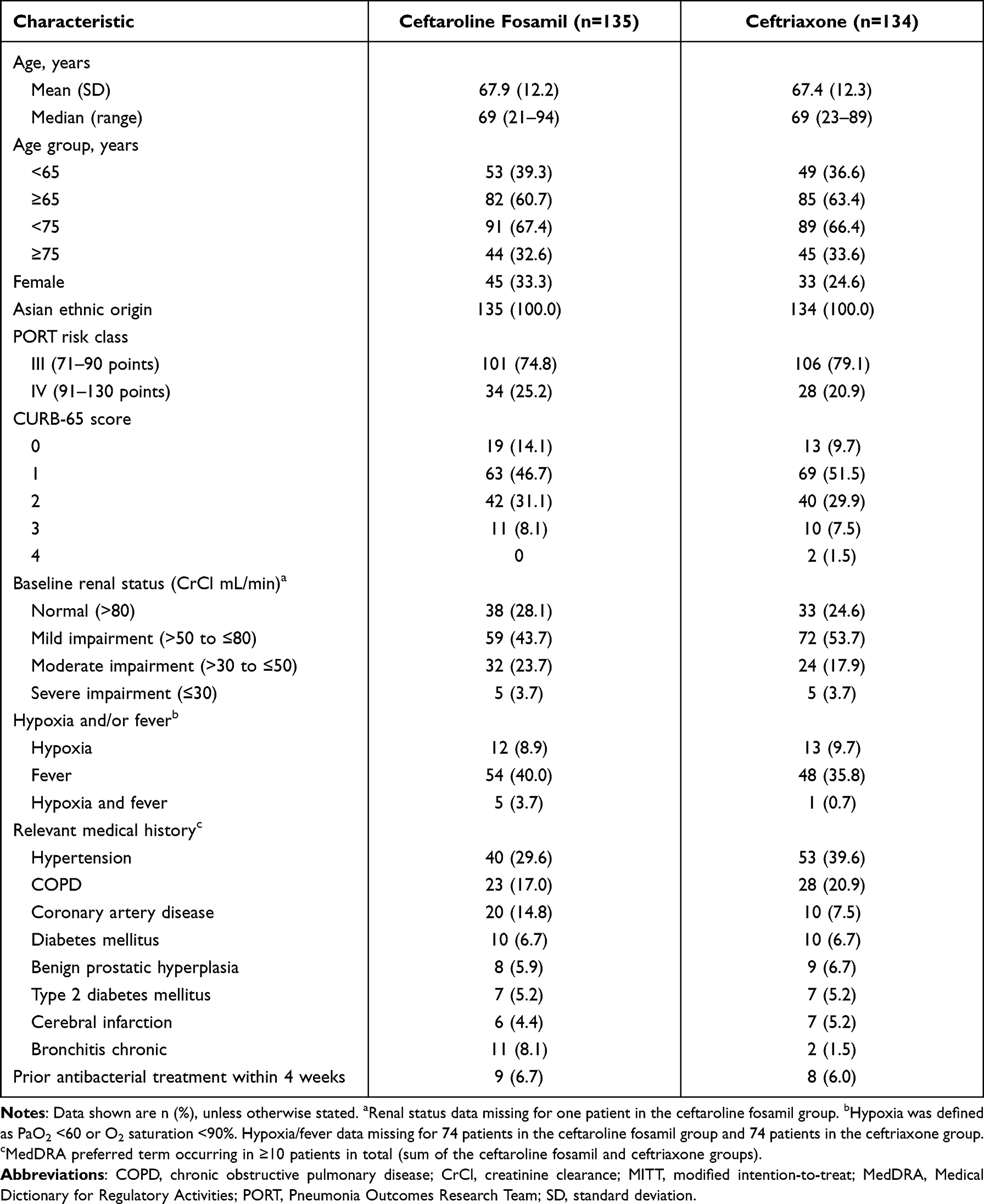 |
Table 1 Patient Baseline and Demographic Characteristics in the China Subset (MITT Population, Excluding Site 1314) |
The most common typical CAP pathogens identified at baseline were K. pneumoniae, S. pneumoniae and H. influenzae; S. aureus (methicillin-susceptible) and Haemophilus parainfluenzae were identified in two and seven patients, respectively, in the ceftriaxone group only (Table 2). Most S. pneumoniae were identified by urinary antigen testing (UAT) rather than by respiratory or blood culture (ceftaroline fosamil arm: four identified by UAT only and two by baseline culture from respiratory specimens; ceftriaxone arm: five identified by UAT only, two by baseline culture from respiratory specimens only, and one by both UAT and respiratory specimen). Among the respiratory/blood culture S. pneumoniae isolates, the number of multidrug-resistant strains was low and only one patient had a documented penicillin-resistant isolate. All isolates of S. pneumoniae, S. aureus, Haemophilus spp., Escherichia coli and K. pneumoniae obtained from patients in the China subset were susceptible to the study drugs based on the Clinical and Laboratory Standards Institute 2013 MIC interpretative criteria.28
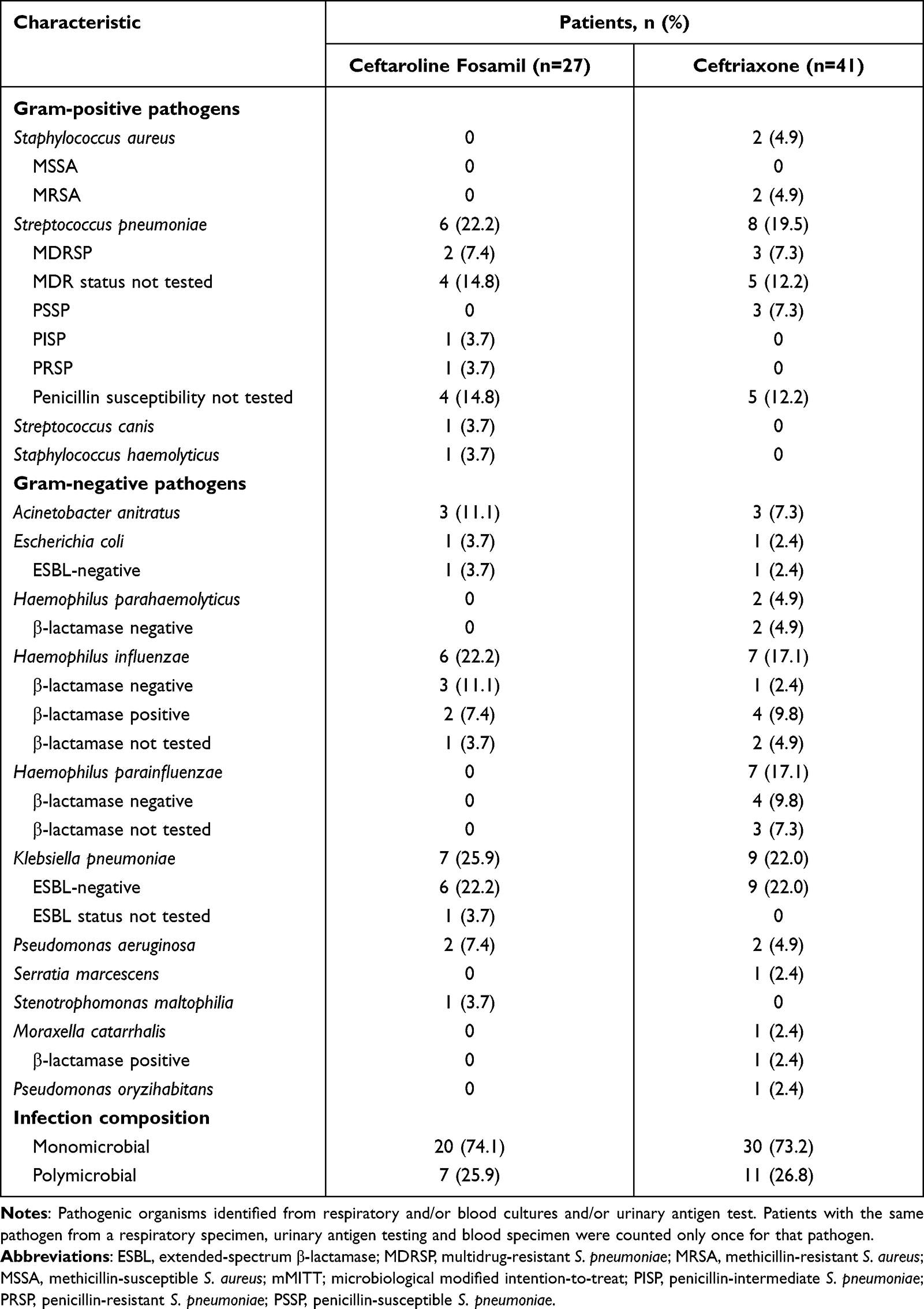 |
Table 2 Typical CAP Pathogens Identified and Infection Characteristics at Baseline in the China Subset (mMITT Population, Excluding Site 1314) |
Based on respiratory samples only and the exclusion of S. pneumoniae detected by UAT only, most patients in the mMITT population had a Gram-negative monomicrobial infection (Table 2). Across both treatment groups, positive serological results for the atypical pathogens M. pneumoniae and C. pneumoniae were obtained in 6/269 patients (2.2%) and 30/269 patients (11.2%), respectively (MITT population). These patients were excluded from the mMITT population. No positive results were obtained for L. pneumophila.
Efficacy
Primary Efficacy Analysis
In the overall ASIA CAP study, clinical cure at TOC in the CE population (excluding site 1314) was observed in 208/247 (84.2%) and 170/231 (73.6%) patients treated with ceftaroline fosamil and ceftriaxone, respectively (difference 10.6%; 95% CI 3.3, 18.0). In the CE population China subset (excluding site 1314), clinical cure rates at TOC were 80/105 (76.2%) for ceftaroline fosamil and 61/100 (61.0%) for ceftriaxone (difference: 15.2%; 95% CI 2.5, 27.6). Clinical failure occurred in 25/105 (23.3%) and 39/100 (39.0%) patients in the ceftaroline fosamil and ceftriaxone groups, respectively. Reasons for clinical failure were generally balanced across treatment groups and included persistence of clinical signs and symptoms of CAP (22 patients in the ceftaroline fosamil group and 33 patients in the ceftriaxone group); treatment-limiting AEs (one and five patients respectively); and death (two and one patients respectively).
Subgroup Analysis
Consistency of clinical response rates at TOC in the CE population (excluding site 1314) was examined across various patient subgroups (Figure 2). Clinical cure rates were numerically higher for ceftaroline fosamil versus ceftriaxone for all subgroups except for patients <65 years of age, and those with a CURB-65 score of 3. Compared with the difference in clinical cure rates (ceftaroline fosamil minus ceftriaxone) in the overall China subset analysis (ie, 15.2%) differences in clinical cure rates favouring ceftaroline fosamil were notably larger for elderly patients (≥65 or ≥75 years of age), those with PORT class IV CAP, and for patients who had not received prior antibiotics with 96 h. For the subgroup analysis by CURB-65 score, treatment differences (ceftaroline fosamil minus ceftriaxone) in clinical cure rates for the China subset were 5.6% for score 0, 28.5% for score 1, 12.0% for score 2 and –11.1% for score 3. There was only one patient in the CE population (in the ceftriaxone group) with a CURB-65 score of 4; this patient was a clinical cure at TOC.
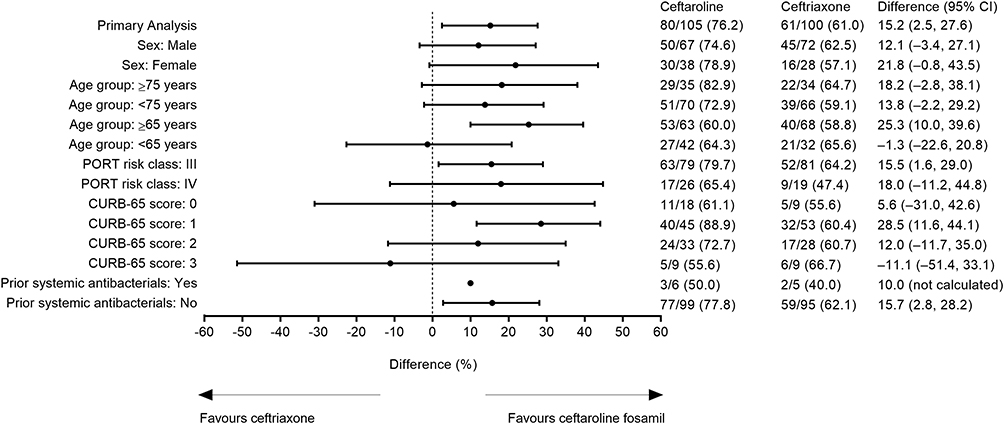 |
Figure 2 Subgroup analysis of clinical cure rates at the TOC visit in the China subset (CE population, Excluding Site 1314). Notes: CIs calculated using Miettinen and Nurminen method for unstratified designs. Subgroup analysis by CURB-65 scores was exploratory and not prespecified. Abbreviations: CE, clinically evaluable; CI, confidence interval; PORT, Pneumonia Outcomes Research Team; TOC, test-of-cure. |
Secondary Efficacy Endpoints
Clinical cure rates at the EOT visit in the CE population were consistent with those at TOC (82/105 patients [78.1%] in the ceftaroline fosamil group and 66/100 patients [66.0%] in the ceftriaxone group; difference 12.1%, 95% CI –0.2, 24.2). Clinical cure rates at TOC in the MITT, mMITT and ME populations showed consistent numerical differences favouring ceftaroline fosamil (Table 3).
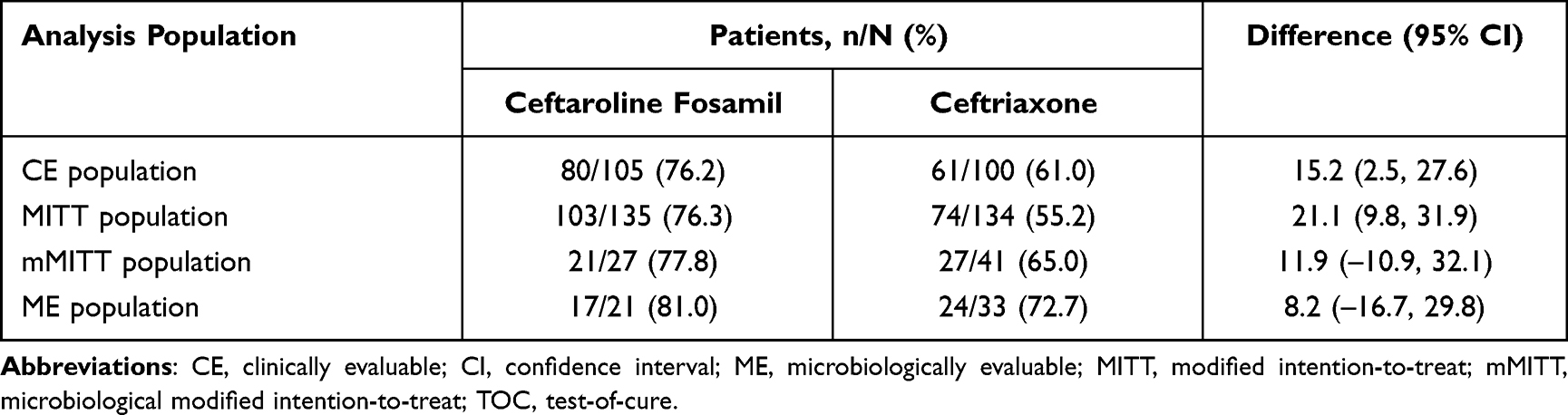 |
Table 3 Clinical Cure Rates at the TOC Visit in the China Subset (Excluding Site 1314) |
Clinical cure rates at TOC by baseline pathogen and infection composition in the ME population are shown in Table 4. At the TOC visit, microbiology specimens were only to be collected if medically indicated. If a suitable specimen was not collected, microbiological outcomes were presumed from clinical responses. Because of a lack of microbiological cultures, microbiological responses for all patients at the TOC visit in the China subset (and the overall study) were presumed from clinical responses; thus, for the ME population favourable microbiological response rates of (ie, presumed eradication) and treatment differences were the same as the per-patient (Table 3) and per-pathogen (Table 4) clinical response rates.
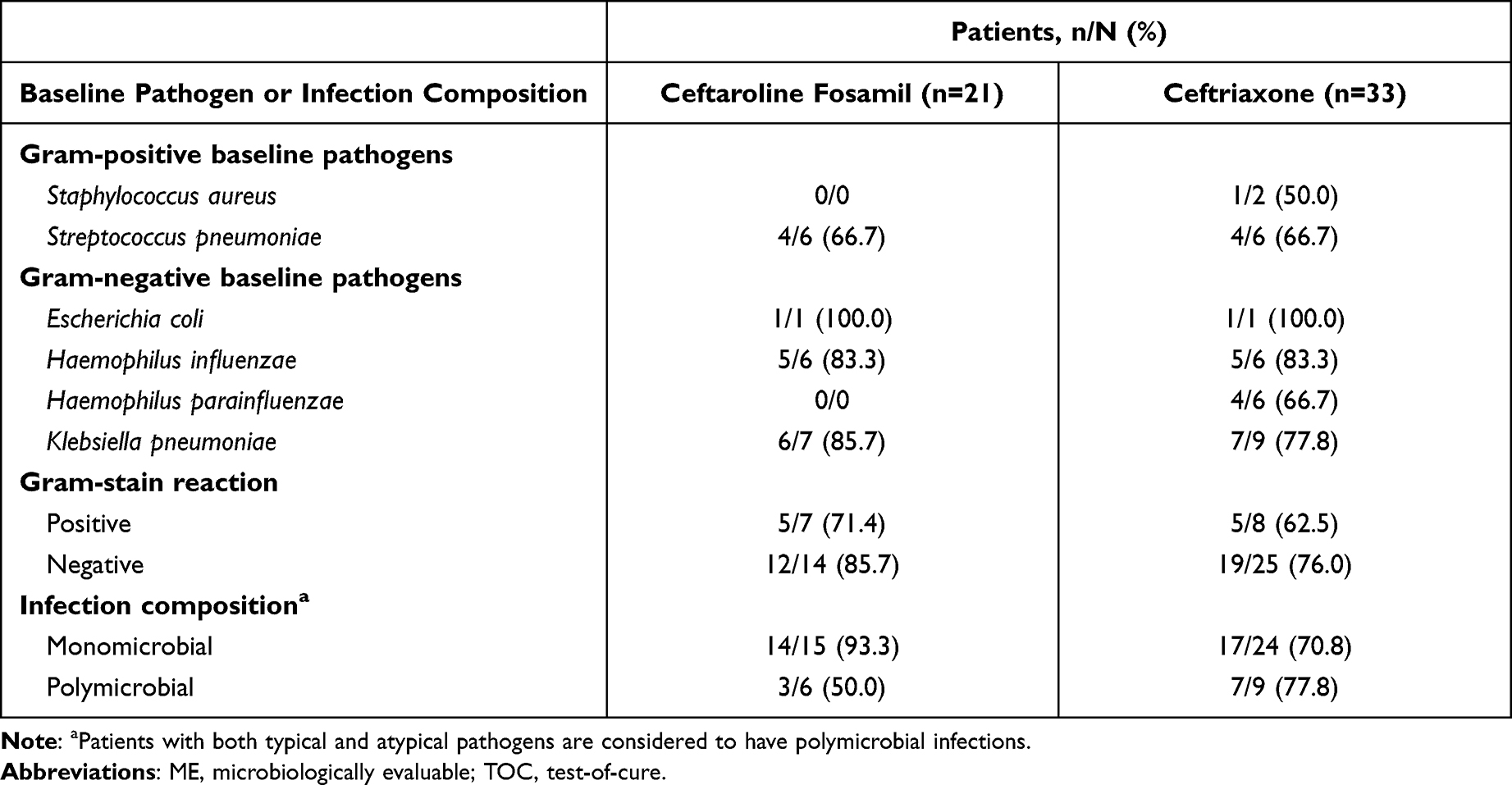 |
Table 4 Clinical Cure Rates at the TOC Visit by Baseline Pathogen and Infection Composition in the China Subset (ME Population, Excluding Site 1314) |
In the MITT population (which unlike the CE and ME populations did not exclude patients due to presence of a sole atypical pathogen or indeterminate Mycoplasma immunoglobulin M [IgM] immunofluorescence [IFA] serology), clinical cure rates in patients with evidence of an atypical pathogen, were 14/40 (70.0%) and 9/16 (56.3%), respectively (difference 21.6%, 95% CI 8.8, 33.6). Corresponding response rates for those without evidence of an atypical pathogen were 80/105 (76.2%) in the ceftaroline fosamil group and 59/108 (54.6%) in the ceftriaxone group (difference 16.7%, 95% CI –15.6, 46.7), and were 9/10 (90.0%) and 7/11 (63.6%), respectively (difference 26.4%, 95% CI –12.3, 58.5) in patients with indeterminate atypical pathogen status.
The majority (≥90%) of patients in the CE population who were clinically cured at TOC remained clinically cured at the LFU visit in both treatment groups (72/80 [90.0%] in the ceftaroline fosamil group and 55/61 [90.2%] in the ceftriaxone group). One patient (1.3%) in the ceftaroline fosamil group and two patients (3.3%) in the ceftriaxone group experienced clinical relapse. Of the 41 patients in the ME population who had a favourable microbiological and clinical response at TOC (Table 3), only one patient (in the ceftriaxone group) experienced microbiological re-infection or recurrence at LFU.
Safety
In the China subset safety population (including site 1314), the median duration of treatment was 7.0 days for both ceftaroline fosamil (range 0.5–7.0 days) and ceftriaxone (range 0.5–7.5 days). AEs are summarized in Table 5. Overall, the frequencies of patients with ≥1 AE were similar for ceftaroline fosamil and ceftriaxone (57/150 [38.0%] versus 58/150 [38.7%]); study drug-related AEs (13/150 [8.7%] versus 12/150 [8.0%] patients respectively) and serious AEs (10/150 [6.7%] versus 6/150 [4.0%] respectively) were also similar across treatment groups. The most common AE for ceftaroline fosamil was abnormal hepatic function (Table S1). Other AEs reported in >2 patients in the ceftaroline fosamil group included constipation, diarrhoea, hypoalbuminaemia, hypokalaemia, leukopenia, pyrexia, rash and decreased white blood cell count. The most common AEs for ceftriaxone were liver injury, abnormal hepatic function, constipation, hypokalaemia, peripheral oedema, and rash. Most AEs were of mild intensity (37/150 patients [24.7%] for ceftaroline fosamil and 42/150 patients [28.0%] for ceftriaxone) or moderate intensity (15/150 [10.0%] and 12/150 [8.0%], respectively). All reported serious AEs were single incidences occurring in one patient (Table S2). None of the reported serious AEs were considered by the investigator to be related to study treatment. Potentially clinically significant changes in post-baseline laboratory findings and vital signs were infrequent (Table S3).
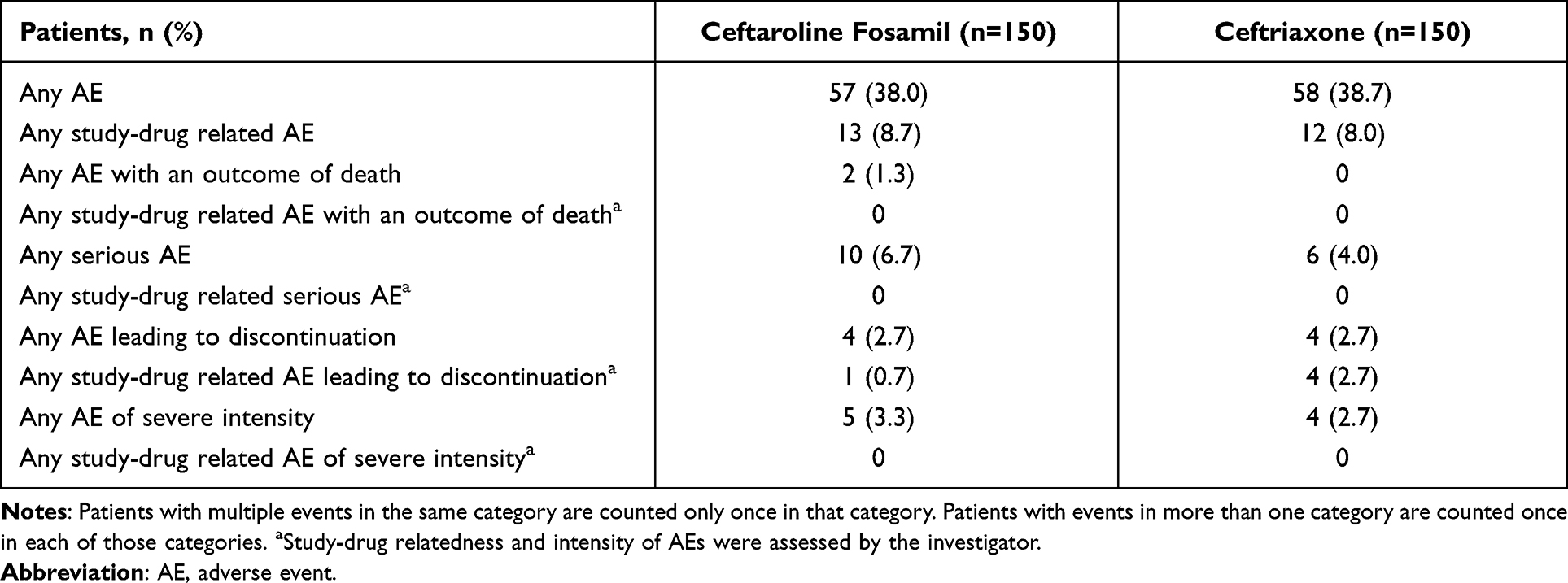 |
Table 5 Overview of AEs in the China Subset (Safety Population, Including Site 1314) |
Discussion
This subset analysis focused on the safety and efficacy of ceftaroline fosamil in patients with CAP in China, and forms part of the larger Phase 3 trial conducted in Asia.21 The objective was to assess whether the conclusions made for the overall ASIA CAP study are still applicable to the China subset in the context of excluding site 1314; no conclusions should be drawn beyond those made in the overall study. Although there are inherent limitations to this analysis because of the small size of the subset, it provides information on clinical efficacy and safety relevant for the intended use of ceftaroline fosamil in Chinese patients hospitalized with CAP.
In the overall study, clinical cure rates at TOC in the CE population (excluding site 1314) were 84.2% and 73.6% for patients treated with ceftaroline fosamil and ceftriaxone, respectively (difference 10.6%; 95% CI 3.3, 18.0). The lower limit of the 95% CI for the treatment difference was >0%, demonstrating non-inferiority and superiority of ceftaroline fosamil based on the protocol-defined primary efficacy analysis.21 Corresponding clinical cure rates at TOC including site 1314 were 84.1% for ceftaroline fosamil and 74.2% for ceftriaxone (difference 9.9%; 95% CI 2.8, 17.1).21 Hence, the post hoc sensitivity analysis excluding site 1314 did not impact the overall efficacy conclusions; as patients at site 1314 were retained in the safety analyses, previously reported safety findings21,29 were unchanged.
Clinical cure rates at TOC in the China subset CE population (76.2% versus 61.0%; difference: 15.2%; 95% CI 2.5, 27.6) are in line with those in the overall study, and despite the smaller sample size, the lower limit of the 95% CI was >0%, thus also meeting the predefined criteria for non-inferiority and superiority of ceftaroline fosamil. While clinical cure rates in the China subset were somewhat lower than in the overall study and in the earlier FOCUS 1 and 2 trials,19,20 the differences between treatments were comparable across trials. Therefore, the findings in the China subset are consistent with the overall study population,21 as well as the FOCUS 1 and 2 results and a meta-analysis of all three trials,22 and also demonstrate that the 2 g daily dose of ceftriaxone did not provide any greater benefit than the 1 g daily dose used in FOCUS 1 and 2. In the China subset, clinical cure rates consistently favoured ceftaroline fosamil in all analysis populations. Results of the subgroup analysis in the China subset, and secondary efficacy endpoints including clinical responses at the EOT visit and at LFU were also consistent with the overall study.21 Interpretation of the subgroup analysis by baseline CURB-65 score, which was a post hoc exploratory analysis for the China subset, is limited by the distribution of CURB-65 scores (most patients in the CE population had scores of 1 or 2), but the findings of this subgroup analysis were also generally consistent with the efficacy results in the China subset and overall study.
The China subset (excluding site 1314) comprised approximately 36% of the total study population. Compared with the overall study population, patients in China were slightly older with less severe disease (23% were in PORT risk class IV compared with 33% overall). Underlying lung disease was a feature of the Chinese patient subset (19% of patients had chronic obstructive pulmonary disease), although less pronounced than in the overall study (28%).21 Prior antimicrobial use was also lower in the China subset than in the overall study. These factors, along with regional differences in causative pathogens and susceptibility profiles, may have contributed to the observed efficacy results in the China subset.
The rate of pathogen isolation was low in the China subset and in the overall study;21 however, the identified typical CAP pathogens were in line with the overall study, and with recent epidemiological findings from China.1,2,4,5 In the overall study, causative pathogen(s) were identified by culture or serology in 42–45% of patients in the MITT population.21 Equivalent values in the China subset were slightly lower (35–41%), but similar to pathogen identification rates in FOCUS 1 and 219,20 and to epidemiological data from hospitalized CAP patients in China and other countries in the Asia-Pacific region.30–32 The proportion of patients infected with C. pneumoniae (11.0%) was similar to observational data from 36 hospitals in China (11.4%)33 and close to average values for 38 Asian studies (6.9%).8 The proportion of patients infected with M. pneumoniae (2.0%) was low considering CAP clinical practice guidelines in China2 and substantially lower than reported in the observational study in 36 hospitals in China (38.9%)33 and in 38 Asian studies (8.0%).8 Other studies have identified M. pneumoniae as the most common aetiological agent of CAP in China.10,30 The low rates of M. pneumoniae and L. pneumophila identification in the current analysis might reflect differences in sample sizes and serology/diagnostic testing between this study and others.8 Of note, during the study, an independent review found that the rate of positive IgM serologies for M. pneumoniae based on the IFA IgM was considerably higher than that expected based on the literature; accordingly, the ELISA test was recommended as the default method (along with paired IgG serologies) to identify patients with M. pneumoniae. L. pneumophila testing was done by UAT only, and no cases of L. pneumophila were identified in the overall ASIA CAP study.21
Clinical response rates by pathogen for ceftaroline fosamil in the China subset varied from 66.7% to 100% for common typical CAP pathogens (ME population). The small number of isolates collected preclude meaningful comparisons between treatment groups; similarly, susceptibility data for the isolated pathogens should be interpreted with caution. The most common Gram-positive pathogen (mMITT population) was S. pneumoniae, identified in six patients (22.2%) in the ceftaroline fosamil group and eight patients (19.5%) in the ceftriaxone group. Most S. pneumoniae were identified by UAT with susceptibility data therefore unavailable. Among five respiratory S. pneumoniae isolates tested for in vitro susceptibility, all five were multidrug-resistant S. pneumoniae (ceftaroline fosamil, n = 2; ceftriaxone, n = 3), and one (ceftaroline fosamil group) was also recorded as penicillin-resistant S. pneumoniae (PRSP). Recent data suggest that the proportion of PRSP among patients with CAP in China could be as high as 55%, with UATs likely to be responsible for increased detection of non-bacteraemic pneumococcal pathogens.5 Global antimicrobial surveillance data of clinical isolates from patients with CAP in 2015–16 indicate that differences in in vitro susceptibility of PRSP to ceftaroline and ceftriaxone can be considerable: 77.6% of 93 PRSP isolates from Asian countries were susceptible to ceftaroline, compared to 2.2% susceptible to ceftriaxone.34 Patients with solely atypical causative pathogens were excluded from the mMITT population; however, clinical response at TOC by atypical pathogen status (positive, negative or indeterminate) was evaluated in the MITT population. These results showed a large treatment difference favouring ceftaroline fosamil with lower 95% CI >0% for patients without atypical pathogens (21.6%; 95% CI 8.8, 33.6) reflecting the overall study and China subset results, which was not evident in those with confirmed atypical infections (16.7%; 95% CI –15.6, 46.7). In contrast, results for patients with indeterminate atypical pathogen status were similar to those without atypical pathogens (difference in clinical cure rates 26.4%; 95% CI –12.3, 58.5). This is consistent with the hypothesis that the patients classified with indeterminate serology had false-positive Mycoplasma IgM IFA serology.
Ceftaroline fosamil 600 mg every 12 h was generally well tolerated in the China subset, and safety findings were in line with those of the overall ASIA CAP study.21 The AEs reported in this study are consistent with the known safety profile of ceftaroline fosamil from previously conducted studies29 and were mostly typical cephalosporin class effects. Gastrointestinal events, particularly diarrhoea, constipation, and vomiting, appeared to be less prevalent in the China subset than in the overall study population. Conversely, of the nine AEs of abnormal hepatic function (ceftaroline fosamil, n = 6; ceftriaxone, n = 3) reported in the overall study, eight were in patients in China (ceftaroline fosamil, n = 5; ceftriaxone, n = 3). These AEs were all non-serious and of mild or moderate intensity.
There were no notable differences in laboratory values and vital signs findings between the Chinese patient subset and the overall study.21 Post-baseline seroconversion of the Coombs direct antiglobulin test from negative to positive occurred more frequently in the ceftaroline fosamil (9.8%) than in the ceftriaxone (1.5%) group; however, there were no reports of haemolytic anaemia with clinical or laboratory evidence to support the diagnosis. Coombs seroconversion is a well-documented side effect of the cephalosporin drug class and is rarely associated with development of haemolytic anaemia.35 Similar results were seen in the overall study (post-baseline seroconversion of the Coombs test from negative to positive seen in 11.5% versus 4.2% of patients in the ceftaroline fosamil and ceftriaxone groups, respectively).21 The incidence of death was low, and no deaths were related to study treatment.
Conclusions
In summary, in this subset analysis of the Phase 3 randomized controlled ASIA CAP trial, ceftaroline fosamil 600 mg every 12 h demonstrated clinical efficacy in the treatment of hospitalized patients with CAP enrolled at study sites in China that met the predefined criteria for non-inferiority and superiority for the overall study.21 The safety and tolerability profile of ceftaroline fosamil in this patient population was reflective of the cephalosporin class and with that observed in previous ceftaroline fosamil clinical studies, with no new safety signals identified.
Data Sharing Statement
Upon request, and subject to certain criteria, conditions and exceptions see (https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (1) for indications that have been approved in the US and/or EU or (2) in programs that have been terminated (ie, development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
Ethics and Study Conduct
The trial was conducted in compliance with the Declaration of Helsinki and the International Conference on Harmonisation (ICH) Good Clinical Practice (GCP) Guidelines as well as local regulatory requirements. The study protocol, any amendments, and informed consent documentation were approved by the relevant Institutional Review Boards and/or Independent Ethics Committees at each study site. All patients (or their representatives) provided written informed consent. A list of study sites is provided in the Supplementary Appendix.
Acknowledgments
The authors thank the patients, their families and all investigators involved in the ceftaroline fosamil Asia community-acquired pneumonia clinical trial programme. Medical writing support for manuscript preparation was provided by Mark Waterlow BSc of Prime, Knutsford, Cheshire, UK, funded by Pfizer. Ultimate responsibility for opinions, conclusions and data interpretation lies with the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This trial was originally sponsored by AstraZeneca and is now sponsored by Pfizer. AstraZeneca’s rights to ceftaroline fosamil were acquired by Pfizer in December 2016.
Disclosure
Chao Zhuo, Yijiang Huang, Wenyuan Liu, and Jin-Fu Xu received institutional research grant funding from AstraZeneca for the conduct of the study. Wei Yun Zhu, Gregory G. Stone, Jean Li Yan and Naglaa Mohamed are employees and share holders of Pfizer. The authors report no other conflicts of interest in this work.
References
1. Chen L, Zhou F, Li H, et al. Disease characteristics and management of hospitalised adolescents and adults with community-acquired pneumonia in China: a retrospective multicentre survey. BMJ Open. 2018;8(2):e018709. doi:10.1136/bmjopen-2017-018709
2. Cao B, Huang Y, She DY, et al. Diagnosis and treatment of community-acquired pneumonia in adults: 2016 clinical practice guidelines by the Chinese Thoracic Society, Chinese Medical Association. Clin Respir J. 2018;12(4):1320–1360. doi:10.1111/crj.12674
3. Song J-H, Thamlikitkul V, Hsueh P-R. Clinical and economic burden of community-acquired pneumonia amongst adults in the Asia-Pacific region. Int J Antimicrob Agents. 2011;38(2):108–117. doi:10.1016/j.ijantimicag.2011.02.017
4. Zhao M, Song B, Liu Y, Pu Z, Yu H. Etiological classification and clinical research on community-acquired pneumonia in Yantai, China. Biomedical Res. 2017;28(8):3501–3506.
5. Zhu YG, Tang XD, Lu YT, Zhang J, Qu JM. Contemporary situation of community-acquired pneumonia in China: a systematic review. J Transl Int Med. 2018;6(1):26–31. doi:10.2478/jtim-2018-0006
6. Marchello C, Dale AP, Thai TN, Han DS, Ebell MH. Prevalence of atypical pathogens in patients with cough and community-acquired pneumonia: a meta-analysis. Ann Fam Med. 2016;14(6):552–566. doi:10.1370/afm.1993
7. Wang H, Liu YL, Chen MJ, et al. [Antimicrobial susceptibility of community-acquired respiratory tract pathogens isolated from adults in China during 2009 and 2010]. Zhonghua Jie He He Hu Xi Za Zhi. 2012;35(2):113–119. Chinese.
8. Peto L, Nadjm B, Horby P, et al. The bacterial aetiology of adult community-acquired pneumonia in Asia: a systematic review. Trans R Soc Trop Med Hyg. 2014;108(6):326–337. doi:10.1093/trstmh/tru058
9. Zhao C, Zhang F, Wang Z, et al. [Resistance surveillance of major pathogens for adult community-acquired respiratory tract infections in China: a multicenter study 2012]. Zhonghua Jie He He Hu Xi Za Zhi. 2015;38(1):18–22. Chinese.
10. Liu Y, Chen M, Zhao T, et al. Causative agent distribution and antibiotic therapy assessment among adult patients with community acquired pneumonia in Chinese urban population. BMC Infect Dis. 2009;9:31. doi:10.1186/1471-2334-9-31
11. Zhang X, Wang R, Di X, Liu B, Liu Y. Different microbiological and clinical aspects of lower respiratory tract infections between China and European/American countries. J Thorac Dis. 2014;6(2):134–142. doi:10.3978/j.issn.2072-1439.2014.02.02
12. Woodhead M, Blasi F, Ewig S, et al. Guidelines for the management of adult lower respiratory tract infections–full version. Clin Microbiol Infect. 2011;17(Suppl 6):E1–59. doi:10.1111/j.1469-0691.2011.03672.x
13. Gupta D, Agarwal R, Aggarwal AN, et al. Guidelines for diagnosis and management of community- and hospital-acquired pneumonia in adults: joint ICS/NCCP(I) recommendations. Lung India. 2012;29(Suppl 2):S27–62. doi:10.4103/0970-2113.99248
14. Infectious Diseases Society of Taiwan, Taiwan Society of Pulmonary and Critical Medicine, Medical Foundation in Memory of Dr. Deh-Lin Cheng, Foundation of Professor Wei-Chuan Hsieh for Infectious Diseases Research and Education, C. Y. Lee’s Research Foundation for Pediatric Infectious Diseases and Vaccines. Guidelines on antimicrobial therapy of pneumonia in adults in Taiwan, revised 2006. J Microbiol Immunol Infect. 2007;40(3):279–283.
15. Committee for The Japanese Respiratory Society guidelines for the management of respiratory infections. Guidelines for the management of community acquired pneumonia in adults, revised edition. Respirology. 2006;11(Suppl 3):S79–133. doi:10.1111/j.1440-1843.2006.00937_1.x
16. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
17. Pfizer. Zinforo 600 mg powder for concentrate for solution for infusion: summary of product characteristics; 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/zinforo-epar-product-information_en.pdf.
18. Allergan. TEFLARO™ (ceftaroline fosamil) injection for intravenous (IV) use; 2020. Available from: https://www.allergan.com/assets/pdf/teflaro_pi.
19. File TM
20. Low DE, File TM
21. Zhong NS, Sun T, Zhuo C, et al. Ceftaroline fosamil versus ceftriaxone for the treatment of Asian patients with community-acquired pneumonia: a randomised, controlled, double-blind, phase 3, non-inferiority with nested superiority trial. Lancet Infect Dis. 2015;15(2):161–171. doi:10.1016/S1473-3099(14)71018-7
22. Taboada M, Melnick D, Iaconis JP, et al. Ceftaroline fosamil versus ceftriaxone for the treatment of community-acquired pneumonia: individual patient data meta-analysis of randomized controlled trials. J Antimicrob Chemother. 2016;71(4):862–870. doi:10.1093/jac/dkv415
23. Li J, Das S, Zhou D, Al-Huniti N. Population pharmacokinetic modeling and probability of target attainment analyses in Asian patients with community-acquired pneumonia treated with ceftaroline fosamil. Clin Pharmacol Drug Dev. 2019;8(5):682–694. doi:10.1002/cpdd.673
24. Das S, Li J, Iaconis J, et al. Ceftaroline fosamil doses and breakpoints for Staphylococcus aureus in complicated skin and soft tissue infections. J Antimicrob Chemother. 2019;74:425–431. doi:10.1093/jac/dky439
25. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336(4):243–250. doi:10.1056/NEJM199701233360402
26. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382. doi:10.1136/thorax.58.5.377
27. Zhang J, Hu W, Huang Y, Qu J, Infection Assembly of the Chinese Thoracic S. Blind spots of traditional microbiological tests for severe community-acquired pneumonia in adults and availability of nonculture techniques: a Nationwide Survey of Physicians in China. J Infect Dis. 2020;221(Suppl2):S198–S205. doi:10.1093/infdis/jiz636
28. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Third Informational Supplement M100-S23. Wayne, PA: CLSI; 2013.
29. Cheng K, Pypstra R, Yan JL, Hammond J. Summary of the safety and tolerability of two treatment regimens of ceftaroline fosamil: 600 mg every 8 h versus 600 mg every 12 h. J Antimicrob Chemother. 2019;74(4):1086–1091. doi:10.1093/jac/dky519
30. Lui G, Ip M, Lee N, et al. Role of ‘atypical pathogens’ among adult hospitalized patients with community-acquired pneumonia. Respirology. 2009;14(8):1098–1105. doi:10.1111/j.1440-1843.2009.01637.x
31. Huang HH, Zhang YY, Xiu QY, et al. Community-acquired pneumonia in Shanghai, China: microbial etiology and implications for empirical therapy in a prospective study of 389 patients. Eur J Clin Microbiol Infect Dis. 2006;25(6):369–374. doi:10.1007/s10096-006-0146-7
32. Yoo KH, Yoo CG, Kim SK, et al. Economic burden and epidemiology of pneumonia in Korean adults aged over 50 years. J Korean Med Sci. 2013;28(6):888–895. doi:10.3346/jkms.2013.28.6.888
33. Tao LL, Hu BJ, He LX, et al. Etiology and antimicrobial resistance of community-acquired pneumonia in adult patients in China. Chin Med J (Engl). 2012;125(17):2967–2972.
34. Bae IG, Stone GG. Activity of ceftaroline against pathogens associated with community-acquired pneumonia collected as part of the AWARE surveillance program, 2015-2016. Diagn Microbiol Infect Dis. 2019;95(3):114843. doi:10.1016/j.diagmicrobio.2019.05.015
35. Brayfield A. Martindale: The Complete Drug Reference.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.