")
Back to Journals » Infection and Drug Resistance » Volume 16
Efficacy and Safety of Add-On Plant-Based Drugs for COVID-19 Patients: A Review of the Randomized Control Trials
Authors Diantini A , Febriyanti RM, Levita J
Received 18 April 2023
Accepted for publication 13 June 2023
Published 19 June 2023 Volume 2023:16 Pages 3879—3891
DOI https://doi.org/10.2147/IDR.S417727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Ajeng Diantini,1,* R Maya Febriyanti,2,* Jutti Levita1,*
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, West Java, 46363, Indonesia; 2Department of Biology Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, West Java, 46363, Indonesia
*These authors contributed equally to this work
Correspondence: Jutti Levita, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, West Java, 46363, Indonesia, Tel +6222-84288888 Ext 3510, Email [email protected]
Abstract: COVID‐19 caused by the infection of SARS‐CoV‐2 is still a global concern. WHO reported that from 13 March to 9 April 2023, there were 3 million new cases and approximately 23,000 deaths, mostly occurring in the South-East Asia and Eastern Mediterranean regions, which is predicted due to the new Omicron variant, Arcturus XBB.1.16. Many studies have reported the potency of medicinal plants in enhancing the function of the immune system to combat virus infection. The literature review aimed to describe the efficacy and safety of add-on plant-based drugs for COVID-19 patients. The articles were explored on the PubMed and Cochrane Library databases, and published during 2020– 2023. Twenty-two varieties of plants were used as add-on therapy for COVID-19 patients. These plants were Andrographis paniculata, Viola odorata, Withania somnifera, Zingiber officinale, Curcuma longa, Ferula foetida, Centella asiatica, Thymus vulgaris, Citrus sinensis, Eugenia caryophyllus, Boswellia carterii, Elettaria cardamomum, Salvia rosmarinus, Piper nigrum, Alstonia scholaris, Picrorhiza kurroa, Swertia chirata, Caesalpinia crista, Cucurbita maxima, Tinospora cordifolia, Ocimum sanctum, and Allium sativum. The best efficacy of an add-on therapy for COVID-19 patients was found in A. paniculata herbs as a single component in pharmaceutical dosage form or in combination with other plants. The safety of the plant has been confirmed. A. paniculata does not show interaction with remdesivir or favipiravir, however, caution and therapy drug monitoring is needed if A. paniculata is used in combination with lopinavir or ritonavir because a strong noncompetitive inhibition of CYP3A4 may occur.
Keywords: adjunctive therapy, flavonoids, plant-based therapy, immunomodulatory activity, clinical studies
Introduction
The outbreak of COVID-19 has been a global concern for more than three years. This pandemic has deeply affected the health sector. It is a highly contagious severe acute respiratory syndrome that eventually attacks and damages many organs. It was reported in the last 28 days (13 March to 9 April 2023) the incidence of 3 million new cases and approximately 23,000 deaths, mostly in the South-East Asia and Eastern Mediterranean regions. 1 The new Omicron variant, which is called Arcturus XBB.1.16, migrates from infecting mainly lungs and nervous tissue to the upper airways.2
COVID-19 patients show diverse clinical presentations ranging from asymptomatic, and mild to severe symptoms. Accumulating evidence suggests that comorbidities in SARS-CoV-2-infected individuals contribute to exacerbated outcomes, heightened symptom severity, and potentially elevated mortality risk.3–5
The virus, SARS-CoV-2, is an enveloped virus of spherical shape with a single-stranded RNA genome in the nucleus. It uses ACE2 to invade the human body (Figure 1) and the cellular protease TMPRSS2 for its spike (S) protein priming (proteolytic separation of the S1 and S2 subunits).6
 |
Figure 1 The cell cycle of SARS‐CoV‐2 in humans. |
Infections are instigated by the attachment of transmembrane S glycoprotein to the peptidase domain of human ACE2.7,8 The virus enters the target cells by binding the surface unit of the S protein (S1) to ACE 2. Viral fusion is primed by TMPRSS2 and the active S protein of SARS‐CoV‐2. The pH-dependent cysteine protease cathepsin L activates the S protein for fusion within the endosomal membrane. Mpro is a non-structural cysteine protease of SARS-CoV-2 that plays a role in the replication and transcription of the virus. RdRp (RNA-dependent RNA polymerase) is a non-structural protein of SARS-CoV-2 that works as a catalyst in the translation of viral RNA. SARS-CoV-2 uses an RdRp complex for the replication of their genome and for the transcription of their genes.9,10
At a time of worldwide anxiety, it is imperative to find long-term solutions to prevent the transmission of such pandemics, therefore, many studies have been focused on how to enhance the role of the immune system. The immune system can be classified into two functional categories: (1) the innate (non-specific) immune system and (2) the adaptive (specific or acquired) immune system. The immune system’s architecture is organized into multiple layers, providing defenses at several levels. The skin serves as the primary and most evident barrier against infection. Physiological factors, such as body temperature and pH, also contribute to creating inhospitable environments for foreign organisms. Upon successful pathogen entry, the innate and/or adaptive immune systems become active. Both systems encompass a diverse array of cells and molecules that engage in intricate interactions to detect and eliminate pathogens. Detection and elimination rely on chemical bonding, where immune cell surfaces are adorned with various receptors. Some of these receptors bind to pathogens, while others interact with other immune cells or molecules, facilitating the complex signaling networks that underlie immune responses.11,12 In a healthy organism, the immune system preserves internal homeostasis. The functionality and efficiency of the immune system are modulated by diverse exogenous and endogenous factors, leading to either immunosuppression or immunostimulant. Agents capable of normalizing or modulating pathophysiological processes are classified as immunomodulators.12,13
Many studies have reported the potency of medicinal plants in enhancing the function of the immune system to combat virus infection, however, no study reported on the safety of randomized control trials of plant extracts for patients with COVID-19. In this review, the efficacy and safety of add-on plant-based drugs for COVID-19 patients are discussed. Randomized controlled trials or clinical trials were chosen because they are prospective studies that evaluate the effectiveness of therapy. Before performing the trials, the researchers have to attentively choose the population, what interventions to be compared, and the outcomes of interest. Through this review, readers will get insights into the results, outcomes, and benefits of using add-on plant-based therapy particularly plants with immunomodulatory activity for COVID-19 patients.
Materials and Methods
This review was based on the articles indexed in the PubMed and Cochrane Library databases, published during 2020–2023. The search was done using the keywords: (immune system AND flavonoids OR plants AND covid19 patients) AND (controlled trial” OR “randomized controlled trial” OR “randomized controlled trial” OR RCT[filter]). Inclusion criteria were limited to original articles written in English, plant-based drugs, accessible full texts, and randomized control trials or human studies. In vivo/in vitro/in silico studies, non-plant-based, or incomplete studies, were excluded. The titles and the abstracts of the articles included were further screened for their relevance to the topic of this study. Additional relevant studies were obtained from the citations in the selected articles. The detailed flowchart of the article searches and the results obtained are depicted in Figure 2.
 |
Figure 2 Flow chart diagram of the review process. |
Results
Of the 163 articles identified, 12 studies were reckoned to meet the eligibility criteria and these articles were included for analysis (depicted in Figure 2). Out of 12 studies, 11 studies are conducted in COVID-19 patients14–24 and 1 study is conducted in post-COVID-19 patients.25 There are 22 varieties of plants involved as add-on therapy for COVID-19 patients. These plants were Andrographis paniculata (Acanthaceae) in the dosage form of 150 mg extract in methylcellulose coated tablets (300 mg 3 times/day), Viola odorata (Violaceae) 1.5 g dried flower extract in 10 mL syrup (1.5 g 3 times/day), Withania somnifera (Solanaceae), Zingiber officinale (Zingiberaceae), Curcuma longa (Zingiberaceae), Ferula foetida (Apiaceae) 260 mg oleo‐gum in tablets (260 mg twice/day), Centella asiatica (Apiaceae), Thymus vulgaris (Lamiaceae), Citrus sinensis (Rutaceae), Eugenia caryophyllus (Myrtaceae), Boswellia carterii (Burseraceae), Elettaria cardamomum (Zingiberaceae), Salvia rosmarinus (Lamiaceae), Piper nigrum (Piperaceae), Alstonia scholaris (Apocynaceae), Picrorhiza kurroa (Plantaginaceae), Swertia chirata (Gentianaceae), Caesalpinia crista (Fabaceae or Leguminosae), Cucurbita maxima (Cucurbitaceae) 5 mg squalene in microemulsion injection (5 mg twice/day), Tinospora cordifolia (Menispermaceae), Ocimum sanctum (Lamiaceae), and Allium sativum (Amaryllidaceae) 90 mg (three times/day). The number of trials, sample sizes, standard drugs used, clinical outcomes, and the adverse events for each included plant are tabulated in Table 1.
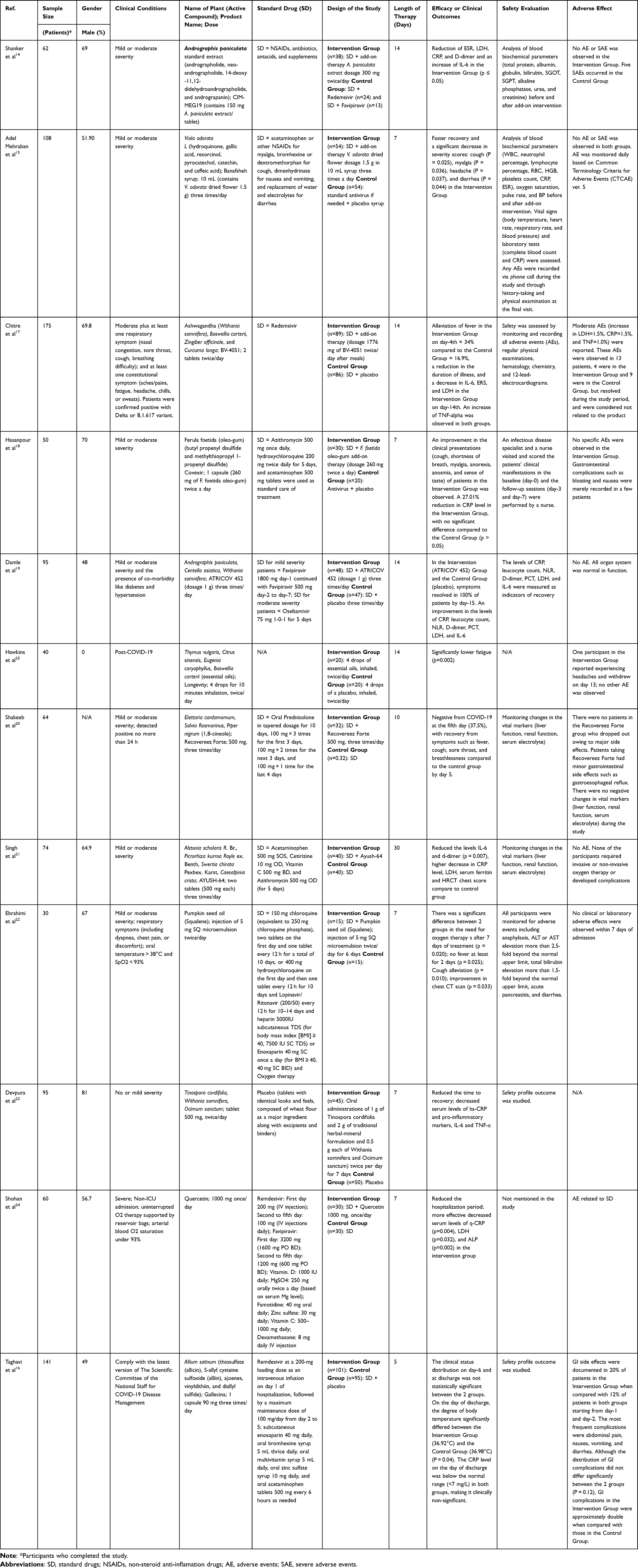 |
Table 1 Characteristics of the Study |
The articles analyzed were published from 2020 to 2023. The total number of participants involved was 1042 COVID-19 patients, with the majority of the patients being male gender (56.83%). The duration of the studies ranged from 5 to 30 days. However, one study included in this review was performed on 40 post-COVID-19 female patients.
The studies used standard-of-care drugs, eg, a combination of NSAIDs (acetaminophen 500 mg)14–16,18,21 or SAIDs (prednisolone),20 antibiotics (azithromycin 500 mg),18,21 chloroquine or hydroxychloroquine,18,22 H1R antagonists (cetirizine 10 mg for allergy or dimenhydrinate for nausea),15,21 anticoagulants (enoxaparin 40 mg),16,22 antitussive (bromhexine or dextromethorphan),15,16 antacids or H2R antagonists (famotidine),24 and supplements (Vitamin C 500 mg). The antiviral drugs used were remdesivir (in general) or favipiravir (for mild severity symptoms) or oseltamivir (for moderate severity symptoms) or a combination of lopinavir/ritonavir. Most of the studies reported a reduction of symptoms or faster recovery and a decrease in inflammatory responses (IL-6, C-reactive protein, and D-dimer) in the Intervention Group (plant-based add-on therapy) compared to the Control Group. Moreover, 6 studies indicated the safety of the add-on plant-based therapy as proven by no AEs observed in the Intervention Group patients.
Efficacy
All twelve reviewed studies reported the efficacy of the plant-based add-on therapy (Table 1). Efficacy was evaluated by measuring the levels of inflammatory responses, either IL-6 or C-reactive protein or D-dimer or all (10 articles), and/or the hospitalization period (5 articles), and/or the severity of the symptoms, eg, cough, myalgia, fever, sore throat, fatigue (7 articles). Not all studies showed their data, some of them only reported general qualitative statements, eg, an improvement in inflammatory responses or a significant decrease in inflammatory markers.
The efficacy data of the plant-based add-on therapy for COVID-19 patients in this review were obtained by comparing the changes (calculated in %) in IL-6, CRP, and D-dimer levels (Table 2) before and after the intervention.
 |
Table 2 Efficacy of the Plant-Based Add-On Therapy on the Inflammatory Responses in Patients with COVID-19 |
It is interesting to find out that the aerial part of Andrographis paniculata plants (CIM-MEG19 tablet) has shown the best efficacy as an add-on therapy for COVID-19 patients.14,19 This drug showed a statistically significant (p < 0.05) reduction in CRP (53.58%) and D-dimer (22.04%) levels as well as the ESR (erythrocyte sedimentation rate). However, an increase in IL-6 (21.88%) was observed, although in general, the patients in the Intervention Group showed no AEs or SAEs.14 A. paniculata was also studied in a combination with other plants (ATRICOV 452 capsule) and resulted in a decrease of IL-6, CRP, and D-dimer levels.19
Moreover, the bulb of garlic (Allium sativum) was studied as an add-on therapy in reducing CRP in mild-severity hospitalized patients with COVID-19. Although the result was not clinically significant compared to that of the placebo group, the add-on therapy using A. sativum could reduce 62.55% CRP level compared to the baseline. However, this plant has caused GI discomfort in 20% of the patients.16
A study in post-COVID-19 patients was included in this review because the term post-COVID-19 syndrome has recently procured global recognition among scientific communities. The pathogenesis of post-COVID syndrome involves multiple mechanisms that result in various clinical manifestations.26 The post-COVID-19 patients were given 10 minutes of inhalation of essential oils containing a mixture of Thymus vulgaris, Citrus sinensis, Eugenia caryophyllus, and Boswellia carterii (essential oils) twice per day for 14 days, which resulted in a significant decrease in fatigue in the Intervention Group. Nevertheless, one participant in the Intervention Group reported experiencing headaches and withdrew on day-13. No other AE was observed.25
Safety
The safety of the add-on therapy was evaluated in 10 of the 12 studies, by analyzing the hematologic parameters (WBC, neutrophil percentage, lymphocyte percentage, RBC, hemoglobin, platelets count) and/or blood biochemical parameters (total protein, albumin, globulin, bilirubin, SGOT, SGPT, alkaline phosphatase, urea, and creatinine), and/or inflammatory biomarkers (ESR, LDH, CRP, and D-dimer), and/or physical examination (oxygen saturation, pulse rate, and BP), and/or by monitoring the AEs, before and after add-on intervention. The most frequently reported side effects are mild GI discomfort (bloating and nausea) and headache. None of the studies reported severe side effects. All studies confirmed the safety of the add-on therapy.
Discussion
SARS-CoV-2 infection rapidly stimulates CD4+T lymphocyte cells to become pathogenic T helper (Th)1 cells and produces granulocyte-macrophage colony-stimulating factor (GM-CSF) and IL-6. Eventually, it invigorates inflammatory factors engendering a cascade of interactions and cytokine storm.3 C-reactive protein (CRP) and IL-6 were appointed as markers to determine the severity of COVID-19. An elevation of IL-6 indicated the worsening of the disease, while a decrease indicated the effectiveness of therapy.27
IL-6, a cytokine featuring pleiotropic activity, works by stimulating the production of acute-phase proteins, eg, CRP, and blocking the production of albumin. IL-6 also contributes a part to the acquired immune response by activating immunoglobulin production and T-cells generation. IL-6 stimulates the differentiation or proliferation of various non-immune cells; thus, discontinued production of IL-6 governs the instigation of various diseases.28
CRP is a pentameric protein produced in the mitochondria of hepatocytes. The level of this protein increases in correlation with inflammation. CRP is released when oxidative stress due to the presence of reactive oxygen species which opens the mitochondrial permeability transition pore. CRP is primarily induced by the IL-6 action on the gene controlling the CRP transcription process.29 The normal level of CRP is < 10 mg/L; however, it elevates rapidly within 6–8 hours and reaches its maximum in 48 hours from the onset of inflammation.30 The level of blood CRP has been reported to range from 20 to 50 mg/L in patients with COVID‐19.31,32
Immunomodulator Activity of the Plants
Several studies reported that most of the medicinal plants used in the treatment of COVID-19 have similar mechanisms, including the regulation of apoptosis and immune response.33–35 For example, a clinical study proposed that standardized A. paniculata extract had increased both T and T helper cells, and significantly increased IFN-γ, IL-4, and decreased IL-2 at day-30 in participants with absolute lymphocyte counts of 1000–3000 cells/mm3. There were no treatment-related adverse effects following standardized A. paniculata extract intake for 30 days.35 In a multicenter randomized open‐label trial involving adult patients hospitalized with mild to moderate COVID‐19, an injection containing 9‐dehydro‐17‐hydro‐andrographolide and sodium 9‐dehydro‐17‐hydro‐andrographolide‐19‐yl sulfate (popularly known as Xiyanping injection) was proven a safe and effective in accelerating symptom resolution (eg, fever and cough) and rapid SARS‐CoV‐2 clearance.36
Andrographolide, the main active compound A. paniculate, are reported to exhibit various pharmacological activities including immunostimulator, antiviral, antibacterial, and anti-inflammation.37,38 Andrographolide was proven could inhibit the function of hepatitis C virus NS3-4A serine protease, a protein essential for RNA replication and signal transduction.39,40 In addition, an in silico study concluded that andrographolide, a major diterpenoid lactone of Andrographis paniculata, was confirmed to effectively prevent the fusion of SARS-CoV-2 to hACE2 by breaking the salt bridge in hotspot-353 and occupying the site where the virus binds (Lys353 and Asp38).7 Moreover, andrographolide could inhibit the inflammatory cytokines in LPS-induced RAW264.7 cells by blocking the NF-kappaB/MAPK signaling pathway,41 thus this diterpenoid lactone may reduce the occurrence of cytokine storms in COVID-19 patients.
A previous study investigated the immunomodulatory effect of W. somnifera (Ashwagandha) extract, revealed that after the 30-day period, participants in the intervention group showed a significant increase (p < 0.05) in immunoglobulins (IgA, IgM, IgG, IgG2, IgG3, and IgG4), cytokines (IFN-γ, IL4), and T-helper 1 (Th1) cytokines, CD4+ and CD8+ T cell counts, and natural killer NK cells, whereas, in the placebo group, these cells showed a significant decrease (p < 0.05) and no alteration in the levels of immunoglobulins and cytokines (p > 0.05).42
Herbal-Drug Interactions
Herbal-drug interactions are frequently observed, particularly in patients with chronic conditions, such as diabetes, hypertension, and psychiatric or neurological disorders, and therapy using medications with narrow therapeutic index, including anticonvulsants, anticoagulants, antiplatelet agents, antiarrhythmics, immunosuppressants, neuroleptics, antidiabetic drugs, and specific antibiotics like vancomycin.43,44
Standard-of-Care in the management of COVID-19 comprises various antiviral agents, such as remdesivir, favipiravir, and oseltamivir, alongside the extensive employment of antibacterial medications, antitussives, expectorants, and supportive care, which increase the potential of herbal-drug interactions. Although the clinical study review in this article assessed the safety profile of herbal therapies, none addressed the potential interactions between the herbal compounds and other drugs employed in the studies.
It is widely acknowledged that pharmacokinetic and pharmacodynamic interactions represent the two fundamental categories of drug interactions observed in clinical settings. Most of these interactions are associated with the role of principal drug-metabolizing enzymes or/and drug transporters, including cytochrome P450 (CYP450) enzymes and/or P-glycoprotein (P-gp). An in vitro CYP450 study in human liver microsomes indicated that remdesivir possesses a moderate inhibition towards CYP3A4, CYP2C8, and CYP2D6, while W. somnifera had no inhibitory effect alone or in combination with remdesivir. Thus, W. somnifera was considered safe to be co-administered with the substrates of CYP3A4, CYP2C8, and CYP2D6. However, caution is warranted in prescribing AYUSH-64, a polyherbal formulation, along with CYP2C8 substrate drugs.45
Although we cannot find other studies reporting the herbal-drug interaction related to those employed in the clinical study, several studies had reported justifiable findings. A recent study disclosed that an injection prepared from andrographolides, the major active components of A. paniculata (Burm. f.) had affected the pharmacokinetics of lopinavir/ritonavir through strong noncompetitive inhibition of CYP3A4 in a time-dependent manner.46 Hence, extreme caution needs to be taken when A. paniculata, as a parenteral dosage form, is co-administrated with lopinavir/ritonavir for COVID-19 treatment.
Taken together, we propose an add-on phytotherapy algorithm for COVID-19 patients using A. paniculata as a single add-on therapy or in combination with other plants possessing antioxidant or immunomodulatory activity (depicted in Figure 3).
 |
Figure 3 Proposed add-on phytotherapy algorithm for COVID-19 patients. |
Conclusion
The efficacy of plant-based add-on therapy for patients with COVID-19, in general, was evaluated by measuring the levels of inflammatory responses, and/or the hospitalization period, and/or the severity of the symptoms, eg, cough, myalgia, fever, sore throat, fatigue. The most effective and safest plant-based drugs for COVID-19 patients are A. paniculata as a single component in pharmaceutical dosage form or in combination with W. somnifera and C. asiatica or with T. cordifolia and O. sanctum. The safety of the plant-based add-on therapy has been confirmed and proven by no occurrence of AEs or mild GI discomfort. Caution and therapy drug monitoring is needed if A. paniculata is to be administered in combination with lopinavir/ritonavir because a strong noncompetitive inhibition of CYP3A4 may occur thus altering the pharmacokinetics of the antivirals.
Acknowledgments
The authors thank the Rector of Universitas Padjadjaran for funding the APC via the Directorate of Research and Community Engagement.
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. World Health Organization. Weekly epidemiological update on COVID-19 - 13 April 2023. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---13-april-2023.
2. Looi M-K. How are covid-19 symptoms changing? BMJ. 2023;380:3. doi:10.1136/bmj.p3
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
4. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020. doi:10.1016/j.ijid.2020.03.017
5. Wang T, Du Z, Zhu F, et al. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet. 2020;395(10228):e52. doi:10.1016/S0140-6736(20)30558-4
6. Hoffmann M, Hofmann-Winkler H, Pöhlmann S. Priming Time: how Cellular Proteases Arm Coronavirus Spike Proteins. Act Viruses by Host Proteases. 2018;71–98. doi:10.1007/978-3-319-75474-1_4
7. Megantara S, Levita J, Ibrahim S, Nguyen BP. Andrographolide, a diterpenoid lactone compound of andrographis paniculata, binds to lys353 and asp38 in the peptidase domain of human angiotensin-converting enzyme 2. Rasayan J Chem. 2021;14(1):241–247. doi:10.31788/RJC.2021.1416070
8. Lestari K, Sitorus T, Instiaty I, Megantara S, Levita J. Molecular Docking of Quinine, Chloroquine and Hydroxychloroquine to Angiotensin Converting Enzyme 2 (ACE2) Receptor for Discovering New Potential COVID-19 Antidote. J Adv Pharm Educ Res. 2020;10(2):1–4.
9. Hillen HS, Kokic G, Farnung L, Dienemann C, Tegunov D, Cramer P. Structure of replicating SARS-CoV-2 polymerase. Nature. 2020;584(7819):154–156. doi:10.1038/s41586-020-2368-8
10. Aftab SO, Ghouri MZ, Masood MU, et al. Analysis of SARS-CoV-2 RNA-dependent RNA polymerase as a potential therapeutic drug target using a computational approach. J Transl Med. 2020;18(1):275. doi:10.1186/s12967-020-02439-0
11. Hofmeyr SA. An interpretative introduction to the immune system. Des Princ Immune Syst Other Distrib Auton Syst. 2000;3:3–26.
12. Jantan I, Ahmad W, Bukhari SNA. Plant-derived immunomodulators: an insight on their preclinical evaluation and clinical trials. Front Plant Sci. 2015;6:655. doi:10.3389/fpls.2015.00655
13. Yuandani JI, Rohani AS, Sumantri IB. Immunomodulatory Effects and Mechanisms of Curcuma Species and Their Bioactive Compounds: a Review. Front Pharmacol. 2021;12(April):1–26. doi:10.3389/fphar.2021.643119
14. Shanker K, Rangnekar H, Wele A, et al. A randomized controlled pilot study of add-on therapy of CIM-MEG19 (standardized Andrographis paniculata formulation) in mild to moderate COVID-19. Phytomedicine Plus Int J Phyther Phytopharm. 2023;3(1):100398. doi:10.1016/j.phyplu.2022.100398
15. Adel Mehraban MS, Shirzad M, Taghizadeh Kashani L M, et al. Efficacy and safety of add-on Viola odorata L. in the treatment of COVID-19: a randomized double-blind controlled trial. J Ethnopharmacol. 2023;304:116058. doi:10.1016/j.jep.2022.116058
16. Taghavi MR, Tavanaei Tamanaei T, Oghazian MB, et al. Effectiveness of Fortified Garlic Extract Oral Capsules as Adjuvant Therapy in Hospitalized Patients with Coronavirus Disease 2019: a Triple-Blind Randomized Controlled Clinical Trial. Curr Ther Res Clin Exp. 2023;98:100699. doi:10.1016/j.curtheres.2023.100699
17. Chitre D, Nadkarni S, Jagtap N, et al. Phase III randomized clinical trial of BV-4051, an Ayurvedic polyherbal formulation in moderate SARS-CoV-2 infections and its impact on inflammatory biomarkers. Phytother Res. 2023;37(4):1232–1241. doi:10.1002/ptr.7683
18. Hasanpour M, Safari H, Mohammadpour AH, et al. Efficacy of Covexir® (Ferula foetida oleo-gum) treatment in symptomatic improvement of patients with mild to moderate COVID-19: a randomized, double-blind, placebo-controlled trial. Phytother Res. 2022;36(12):4504–4515. doi:10.1002/ptr.7567
19. Damle L, Damle H, Br B. Plant formulation ATRICOV 452 in improving the level of COVID-19 specific inflammatory markers in patients. Contemp Clin Trials Commun. 2022;28:100961. doi:10.1016/j.conctc.2022.100961
20. Shakeeb N, Varkey P, Hynse A, Mandlecha A. Anti-inflammatory response of cardamom extract and prediction of therapeutic window in COVID-19 patients by assessing inflammatory markers using RT-PCR. Inflammopharmacology. 2022;30(3):883–894. doi:10.1007/s10787-022-00951-x
21. Singh H, Srivastava S, Yadav B, et al. AYUSH-64 as an adjunct to standard care in mild to moderate COVID-19: an open-label randomized controlled trial in Chandigarh, India. Complement Ther Med. 2022;66:102814. doi:10.1016/j.ctim.2022.102814
22. Ebrahimi M, Farhadian N, Amiri AR, Hataminia F, Soflaei SS, Karimi M. Evaluating the efficacy of extracted squalene from seed oil in the form of microemulsion for the treatment of COVID-19: a clinical study. J Med Virol. 2022;94(1):119–130. doi:10.1002/jmv.27273
23. Devpura G, Tomar BS, Nathiya D, et al. Randomized placebo-controlled pilot clinical trial on the efficacy of ayurvedic treatment regime on COVID-19 positive patients. Phytomedicine. 2021;84:153494. doi:10.1016/j.phymed.2021.153494
24. Shohan M, Nashibi R, Mahmoudian-Sani M-R, et al. The therapeutic efficacy of quercetin in combination with antiviral drugs in hospitalized COVID-19 patients: a randomized controlled trial. Eur J Pharmacol. 2022;914:174615. doi:10.1016/j.ejphar.2021.174615
25. Hawkins J, Hires C, Keenan L, Dunne E. Aromatherapy blend of thyme, Orange, clove bud, and frankincense boosts energy levels in post-COVID-19 female patients: a randomized, double-blinded, placebo controlled clinical trial. Complement Ther Med. 2022;67:102823. doi:10.1016/j.ctim.2022.102823
26. Mahmoud N, Radwan N, Alkattan A, et al. Post-COVID-19 syndrome: nature of symptoms and associated factors. J Public Health (Bangkok). 2023. doi:10.1007/s10389-022-01802-3
27. Liu T, Zhang J, Yang Y, et al. The role of interleukin-6 in monitoring severe case of coronavirus disease 2019. EMBO Mol Med. 2020;12(7):e12421. doi:10.15252/emmm.202012421
28. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
29. Nehring SM, Goyal A, Patel BC. C Reactive Protein. Treasure Island (FL); 2023.
30. Young B, Gleeson M, Cripps AW. C-reactive protein: a critical review. Pathology. 1991;23(2):118–124. doi:10.3109/00313029109060809
31. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
32. Gao Y, Li T, Han M, et al. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J Med Virol. 2020;92(7):791–796. doi:10.1002/jmv.25770
33. Soleymani S, Naghizadeh A, Karimi M, et al. COVID-19: general Strategies for Herbal Therapies. J Evidence-Based Integr Med. 2022;27:2515690X211053641. doi:10.1177/2515690X211053641
34. Alhazmi HA, Najmi A, Javed SA, et al. Medicinal Plants and Isolated Molecules Demonstrating Immunomodulation Activity as Potential Alternative Therapies for Viral Diseases Including COVID-19. Front Immunol. 2021;12:1–24. doi:10.3389/fimmu.2021.637553
35. Rajanna M, Bharathi B, Shivakumar BR, et al. Immunomodulatory effects of Andrographis paniculata extract in healthy adults - An open-label study. J Ayurveda Integr Med. 2021;12(3):529–534. doi:10.1016/j.jaim.2021.06.004
36. Zhang X-Y, Lv L, Zhou Y-L, et al. Efficacy and safety of Xiyanping injection in the treatment of COVID-19: a multicenter, prospective, open-label and randomized controlled trial. Phytother Res. 2021;35(8):4401–4410. doi:10.1002/ptr.7141
37. Discovery C-D. A Comprehensive Review of Andrographis paniculata (Burm. f.) Nees and Its Constituents as Potential Lead Compounds for COVID-19 Drug Discovery. Molecules. 2022;27:4479.
38. Jayakumar T, Hsieh CY, Lee JJ, Sheu JR. Experimental and clinical pharmacology of andrographis paniculata and its major bioactive phytoconstituent andrographolide. Evidence-Based Complement Altern Med. 2013;2013. doi:10.1155/2013/846740
39. Enmozhi SK, Raja K, Sebastine I, Joseph J. Andrographolide as a potential inhibitor of SARS-CoV-2 main protease: an in silico approach. J Biomol Struct Dyn. 2021;39(9):3092–3098. doi:10.1080/07391102.2020.1760136
40. Chandramohan V, Kaphle A, Chekuri M, Gangarudraiah S, Bychapur Siddaiah G. Evaluating Andrographolide as a Potent Inhibitor of NS3-4A Protease and Its Drug-Resistant Mutants Using In Silico Approaches. Adv Virol. 2015;2015:972067. doi:10.1155/2015/972067
41. Li Y, He S, Tang J, et al. Andrographolide Inhibits Inflammatory Cytokines Secretion in LPS-Stimulated RAW264.7 Cells through Suppression of NF-κB/MAPK Signaling Pathway. Evid Based Complement Alternat Med. 2017;2017:8248142. doi:10.1155/2017/8248142
42. Tharakan A, Shukla H, Benny IR, Tharakan M, George L, Koshy S. Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract-A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants. J Clin Med. 2021;10(16). doi:10.3390/jcm10163644
43. Albassam AA, Alanazi A, Alhaqbani N, et al. The potential of drug-herbal interaction among patients with chronic diseases in Saudi Arabia. Complement Ther Clin Pract. 2021;43:101324. doi:10.1016/j.ctcp.2021.101324
44. Chen X-W, Serag ES, Sneed KB, et al. Clinical herbal interactions with conventional drugs: from molecules to maladies. Curr Med Chem. 2011;18(31):4836–4850. doi:10.2174/092986711797535317
45. Kasarla SS, Borse SP, Kumar Y, Sharma N, Dikshit M. In vitro effect of Withania somnifera, AYUSH-64, and remdesivir on the activity of CYP-450 enzymes: implications for possible herb-drug interactions in the management of COVID-19. Front Pharmacol. 2022;13:973768. doi:10.3389/fphar.2022.973768
46. Ye L, Cheng L, Deng Y, et al. Herb-Drug Interaction Between Xiyanping Injection and Lopinavir/Ritonavir, Two Agents Used in COVID-19 Pharmacotherapy. Front Pharmacol. 2021;12:773126. doi:10.3389/fphar.2021.773126
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.