Back to Journals » Clinical Ophthalmology » Volume 20
Efficacy and Safety of Ab-externo Approach versus Ab-interno Approach of XEN45 Gel Stent Implantation: A Systematic Review and Meta-Analysis
Authors Hubayni R ![]() , Qedair J
, Qedair J ![]() , Aljahdali FF
, Aljahdali FF ![]() , Alotaibi N, Almuzaini YS, Almuntashri MM, Alhazzaa B
, Alotaibi N, Almuzaini YS, Almuntashri MM, Alhazzaa B
Received 13 November 2025
Accepted for publication 30 January 2026
Published 24 February 2026 Volume 2026:20 575562
DOI https://doi.org/10.2147/OPTH.S575562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rahaf Hubayni,1,2 Jumanah Qedair,1,2 Faisal F Aljahdali,2,3 Nawaf Alotaibi,2,3 Yasser Saleh Almuzaini,2,3 Manar M Almuntashri,2,4 Bader Alhazzaa3
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Ophthalmology Department, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 4College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Correspondence: Rahaf Hubayni, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia, Tel +966536382653, Email [email protected]
Purpose: The XEN45 Gel Stent is a microinvasive glaucoma surgery (MIGS) device designed to lower intraocular pressure (IOP) by enhancing aqueous humor outflow. This systematic review and meta-analysis aimed to compare efficacy and safety of the ab externo and ab interno approaches for XEN45 Gel Stent implantation.
Methods: A comprehensive literature search was conducted using PubMed, Web of Science, the Cochrane Library, the Registry of Controlled Trials, and the Directory of Open Access Journals. Of 216 screened articles, six retrospective studies met inclusion criteria. Primary outcomes included reduction in mean baseline IOP and number of IOP-lowering medications required postoperatively. Statistical analysis was performed using Stata (StataCorp, 2025).
Results: A total of 614 eyes were analyzed. Three hundred and eighteen treated with the ab externo approach and 278 with the ab interno approach. Mean patient age was comparable between groups, although proportion of female patients was higher in the ab externo cohort. Both techniques achieved significant IOP reduction: pooled standardized mean difference (SMD) was − 12.8 (95% CI: − 19.4 to − 6.2) for ab externo group and − 10.1 (95% CI: − 16.3 to − 3.8) for ab interno group. Reduction in IOP-lowering medications was also significant and similar between groups [ab externo: SMD − 2.2 (95% CI: − 2.6 to − 1.9); ab interno: SMD − 2.1 (95% CI: − 2.5 to − 1.7)]. Needling rates were significantly lower with ab externo approach compared to ab interno approach (12.1% vs 18.1%, p = 0.04). Although rate of secondary glaucoma surgeries was higher in ab interno group (19.8% vs 11.6%), this difference did not reach statistical significance (p = 0.28).
Conclusion: Both ab externo and ab interno XEN45 Gel Stent implantation techniques demonstrated comparable efficacy and safety in lowering IOP and reducing dependence on IOP-lowering medications. However, ab externo approach was associated with a lower needling rate, suggesting a potential procedural advantage.
Keywords: glaucoma, intraocular pressure, XEN 45 Gel stent, Ab externo, Ab interno
Introduction
Glaucoma is defined as a group of progressive optic neuropathies that have characteristic morphological changes at the optic nerve head, together with loss of retinal ganglion cells and their axons, leading to visual field loss.1 It is the second leading cause of blindness worldwide.2 To date, the main modifiable risk factor to prevent glaucomatous damage is lowering intraocular pressure.1 The first line of treatment is commonly topical antiglaucoma medications; however, patient compliance and side effects of these medications may lead to failure of medical treatment.3,4 For these reasons, glaucoma filtration surgeries remain the gold standard in glaucoma management. However, they are associated with well-known complications such as bleb-related endophthalmitis, choroidal effusion, leak, and hypotony.5
Micro Invasive Glaucoma Surgery (MIGS) is a term used to describe a range of newer surgical procedures used to treat mild-to-moderate glaucoma.6 They enhance aqueous outflow with minimal disruption of normal anatomy as well as high safety and rapid recovery time compared to traditional filtering surgery.6,7 Recently, various MIGS procedures have been described depending on their mechanisms of action. For instance, iStent and Hydrus work by enhancing aqueous outflow through trabecular meshwork. XEN Gel Stent decreases intraocular pressure by draining aqueous from anterior chamber to the subconjunctival space.8
The XEN Gel Stent can be implanted either via an ab interno approach (from within the anterior chamber) or an ab externo approach (through the conjunctiva). However, comparative evidence regarding the safety and efficacy of these two techniques remains limited. Therefore, the present study aims to compare the efficacy and safety of ab externo versus ab interno XEN 45 Gel Stent implantation in the management of glaucoma.
Materials and Methods
Literature Search Strategy
A systematic review and meta-analysis, registered with PROSPERO (ID: CRD42025648982), was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9 The study screening process for this meta-analysis is illustrated in Figure 1. The following electronic databases were comprehensively searched: PubMed Central, Cochrane Library, Registry of Controlled Trials, Web of Science, and Directory of Open Access Journals, using the relevant keywords “Glaucoma,” “IOP,” “Intraocular Pressure,” “XEN Gel Stent,” “ab externo,” and “ab interno,” from inception until 10 February 2025. All published articles were considered, with no restrictions on language or publication period. Additionally, the reference lists of retrieved articles were manually screened to identify further relevant studies.
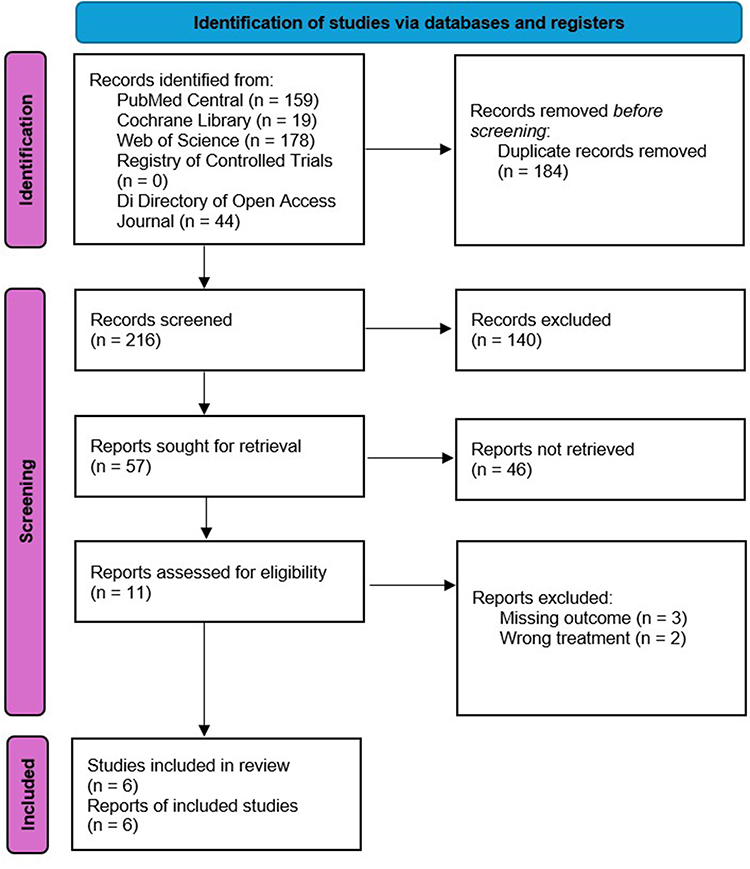 |
Figure 1 PRISMA flowchart for articles screening process. |
Eligibility Criteria and Study Selection
Studies were included if they met the following criteria: (a) clinical trials or observational studies comparing the ab externo approach with the ab interno approach for XEN Gel Stent implantation; (b) patients aged >18 years; (c) patients diagnosed with any type of primary open-angle glaucoma (POAG) or secondary open angle glaucoma (SOAG); and (d) studies reporting data on any of the following outcomes: mean baseline intraocular pressure (IOP) and the number of IOP-lowering medications at various time points.
Articles were excluded if they met any of the following criteria: (1) studies with missing results or incomplete data; (2) studies comparing either the ab externo or ab interno approach of XEN Gel Stent implantation with a different intervention; (3) studies including patients with any type of glaucoma other than POAG or SOAG; or (4) studies involving patients with a history of prior filtering glaucoma surgery. Duplicates were removed using Mendeley software. References were screened in a two-step process: first, titles and abstracts were reviewed against the inclusion criteria, followed by a full-text appraisal of relevant articles for eligibility in the meta-analysis. Each step was conducted independently by two reviewers.
Data Extraction
Data were extracted independently by two authors. Discrepancies were resolved through discussion and consensus among the reviewers. The extracted data included study ID (name of the first author and year of publication), study location, study design, sample size, sex and age distribution of participants in each intervention arm, type of glaucoma, implantation approach, procedural techniques (standard vs pneumotrabeculoplasty), treatment outcome measures, and adverse events between treatment arms. The terms “standard” and “pneumotrabeculoplasty” techniques reflect the nomenclature used in the original included studies, and detailed procedural descriptions were therefore derived directly from the respective source articles.10–15 No data were estimated from figures; only explicitly reported information or data obtained directly from the authors were included.
Data Synthesis and Quality Assessment
The primary outcomes of interest were changes in IOP from baseline and changes in the number of IOP-lowering medications from baseline. Adverse events were considered secondary outcomes. Two independent authors assessed the risk of bias and certainty of evidence, with conflicts resolved by a third reviewer. The risk of bias and certainty of evidence of the included studies were evaluated using Cochrane’s Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool (Supplementary Figure 1).16
Results
Statistical Analysis
Stata (StataCorp. 2025) was used for all statistical analyses. Continuous variables were presented as weighted means (effect size of means) with 95% confidence intervals (CIs), while categorical variables were presented as logit-transformed proportions (effect size of proportions) with 95% CIs. All meta-analyses were conducted using a random-effects model.17,18 Subgroup meta-analyses of weighted means with 95% CIs and logit-transformed proportions with 95% CIs were performed to assess differences in demographics, type of glaucoma, techniques, second glaucoma surgery, additional interventions, and adverse events among the groups.19,20 For primary outcomes, standardized mean differences were pooled into a single standardized mean difference, representing the overall outcome value for each group from baseline to last follow-up (12 months). Heterogeneity among studies was evaluated using the Chi-square (χ2) test and the Higgins I2 test.21 A two-tailed p-value of <0.05 was considered statistically significant for all statistical analyses. Egger’s test in addition to funnel plots was used to assess publication bias among the included trials, and no bias was detected (Supplementary Figure 2).22
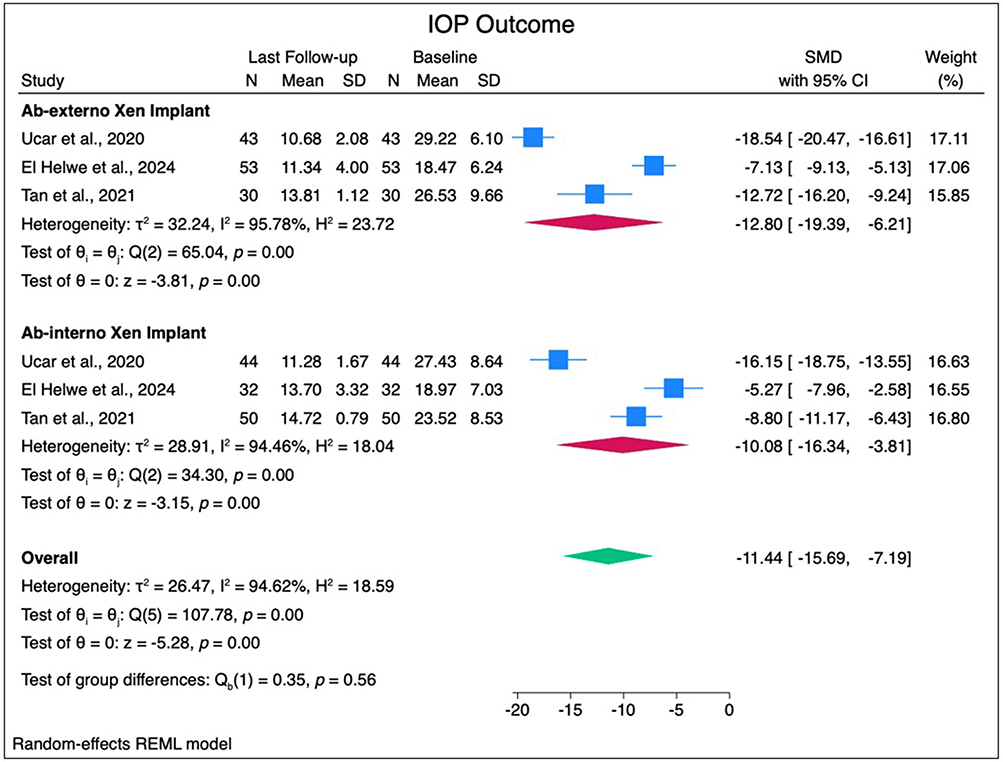 |
Figure 2 Forest plots of standardized mean difference (SMD) for intraocular pressure (IOP) outcome. Abbreviations: SD, standard deviation; CI, confidence interval. |
Study Selection
Initially, 216 articles were yielded during databases search. After duplicate removal, 184 articles left. Through title and abstract screening, 197 articles were excluded. Eleven studies were assessed in full text. Ultimately, six retrospective studies were included in the meta-analysis (Figure 1).10–15
Demographic and Clinical Characteristics
We included a total of 596 patients (614 eyes) undergoing Xen gel Stent implantation, comprising 318 patients in the ab-externo group and 278 patients in the ab-interno group (Table 1). The weighted mean age was comparable between the ab-externo (68.2 years [95% CI: 59.3–77.1]) and ab-interno (70.2 years [95% CI: 62.2–78.3]) groups (p = 0.74). Sex distribution differed significantly, with a higher proportion of females in the ab-externo group (29.9% [95% CI: (26.4–33.7%]) compared to the ab-interno group (22.3% [95% CI: 17.6–27.9%]), p = 0.02; Table 1).
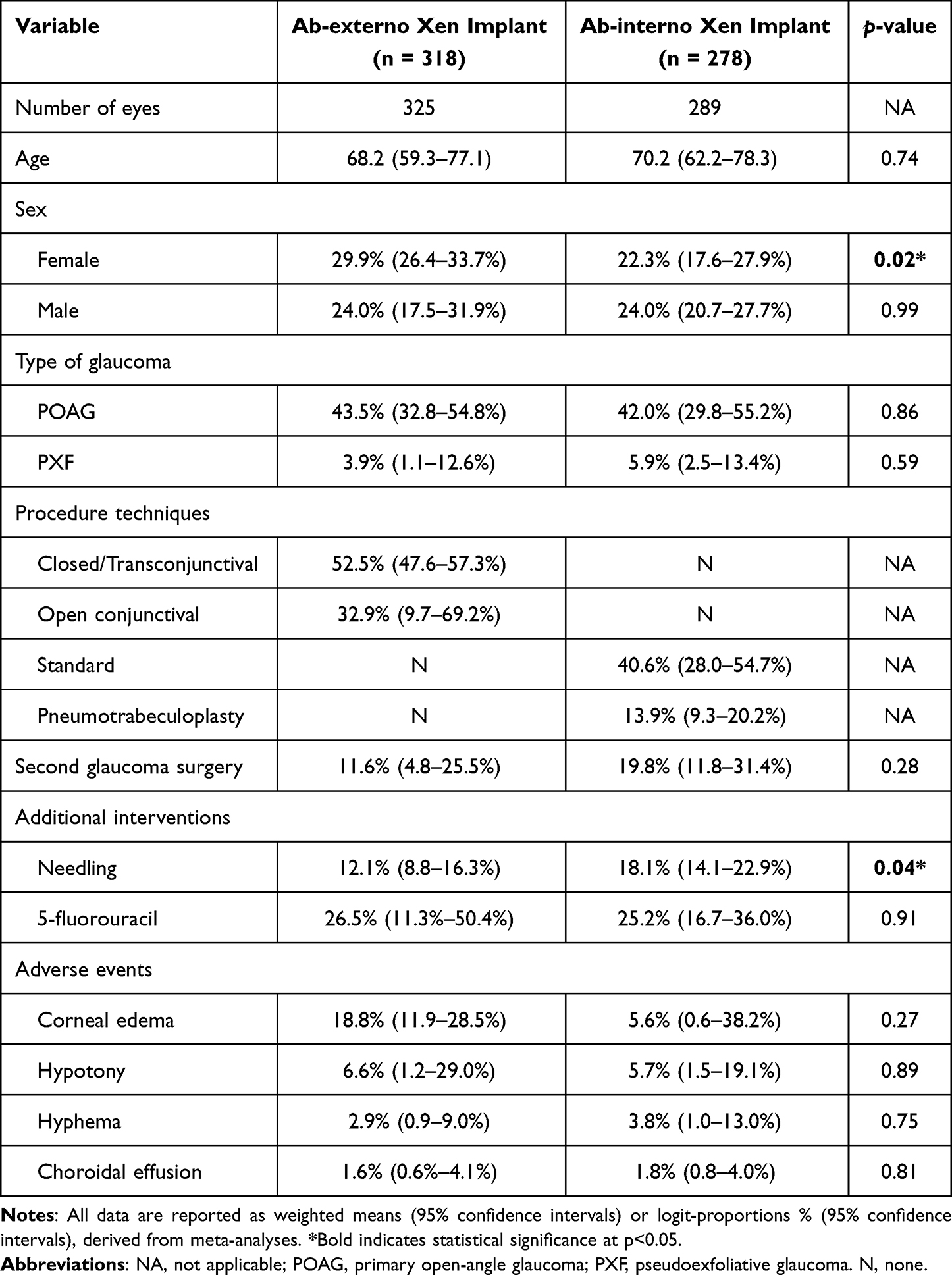 |
Table 1 Demographic and Clinical Characteristics of the Cohort (n = 596) |
The majority of cases in both groups had primary open-angle glaucoma (43.5% ab-externo and 42.0% ab-interno, p = 0.86). Closed or transconjunctival (52.5% [95% CI: 47.6–57.3%]) and open conjunctival (32.9% [95% CI: 9.7–69.2%]) techniques were exclusively used in the ab-externo group, while in the ab-interno group, standard (40.6% [95% CI: 28.0–54.7%]) and pneumotrabeculoplasty (13.9% [95% CI: 9.3–20.2%]) techniques were used (Table 1).
Clinical Outcomes: Adverse Events and Intraocular Pressure (IOP)
Rates of second glaucoma surgery were 11.6% (95% CI: 4.8–25.5%) in the ab-externo group and 19.8% (95% CI: 11.8–31.4%) in the ab-interno group (p = 0.28). There was a statistically significant difference between the two interventions in terms of needling rates (ab-externo: 12.1% [95% CI: 8.8–16.3%] vs ab-interno: 18.1% [95% CI: 14.1–22.9%], p = 0.04; Table 1).
The most common adverse event in both groups was corneal edema (18.8% ab-externo and 5.6% ab-interno, p = 0.27), followed by hypotony (6.6% ab-externo and 5.7% ab-interno, p = 0.89), hyphema (2.9% ab-externo and 3.8% ab-interno, p = 0.75), and choroidal effusion (1.6% ab-externo and 1.8% ab-interno, p = 0.81; Table 1).
Our meta-analysis showed significant IOP reduction in both groups, with no statistically significant differences between the ab-externo and ab-interno approaches (p = 0.56; Figure 2). For the ab-externo group, the overall standardized mean difference (SMD) was −12.8 (95% CI: −19.4 to −6.2), while the ab-interno group’s SMD was −10.1 (95% CI: −16.3 to −3.8).
Both groups demonstrated significant reduction in the number of IOP-lowering medications use and burden, with no statistically significant differences between the two groups (p = 0.56; Figure 3). In the ab-externo group, the SMD was −2.2 (95% CI: −2.6 to −1.9), while the ab-interno group’s SMD was −2.1 (95% CI: −2.5 to −1.7).
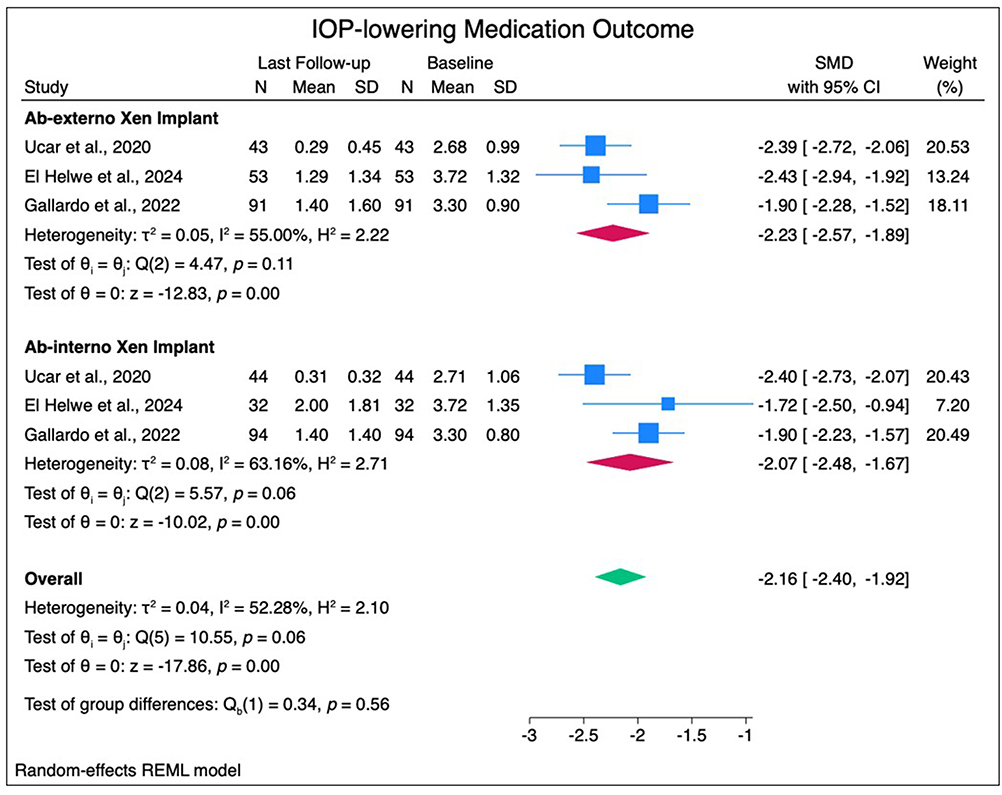 |
Figure 3 Forest plots of standardized mean difference (SMD) for number of medications lowering intraocular pressure (IOP) outcome. Abbreviations: SD, standard deviation; CI, confidence interval. |
Discussion
This systematic review and meta-analysis included six retrospective studies comprising 596 patients (614 eyes) and compared the safety profiles of ab-externo and ab-interno XEN45 gel Stent implantation.
Successful XEN implantation depends heavily on avoiding entrapment of the stent within Tenon’s capsule. Accurate placement and meticulous technique are essential, as Tenon’s involvement can obstruct aqueous outflow, compromise surgical efficacy, and predispose to fibrosis or surgical failure.23 With the ab interno approach, the injector must traverse the anterior chamber, sclera, and Tenon’s capsule. Complete penetration can be technically demanding, as the fibrous capsule tends to stretch rather than perforate cleanly, increasing the risk of the stent becoming entrapped within Tenon’s tissue. Such entrapment can restrict aqueous flow, promote localized fibrosis, and contribute to bleb failure, thereby necessitating postoperative needling. In contrast, in the ab-externo approach, the stent is inserted from the external surface toward the anterior chamber. This allows compression or direct visualization of Tenon’s tissue during insertion, facilitating its penetration and enabling placement of the stent within the supra-Tenon space, thereby reducing the risk of entanglement. However, ab-externo implantation offers less precise control of the entry site into the anterior chamber. An excessively steep scleral trajectory may result in posterior entry through the iris root or ciliary body, increasing the risk of intraoperative bleeding, hyphema, or iris occlusion of the implant. Conversely, the ab interno technique allows more controlled placement under direct gonioscopic visualization.14
Pooled analysis demonstrated comparable outcomes between the two approaches with respect to intraocular pressure (IOP) reduction and reduction in medication burden. Ruda et al reported no difference in mean postoperative IOP or in the number of medications between the two groups.14 Yuan et al similarly found no statistically significant differences at any postoperative time point.15 Tan et al observed significant reductions in both IOP and medication use with each technique, though intergroup differences were not significant.12 Helwe et al reported consistent findings.11
One statistically significant difference was identified in needling rates, which were lower in the ab externo group compared to the ab interno group. Do et al reported postoperative needling in only 11.8% of open-conjunctiva cases versus 36.1% of closed cases (p=0.001).24 Tan et al similarly observed higher needling in ab interno eyes (42.0% vs 26.7%).12 This suggests that bleb failure and fibrosis were less frequent after ab externo implantation. The more posterior and supra-Tenon stent placement achieved with ab externo insertion may create a healthier bleb environment with better exposure to antimetabolites and a reduced tendency for scarring. The need for secondary glaucoma surgery was also similar across techniques, with a slight but non-significant trend toward higher rates following ab interno implantation. These findings are consistent with previous evidence. Gallardo et al reported no significant differences in outcomes between ab interno and ab externo placement.13 Tan et al observed a higher rate of secondary procedures with ab interno, though this did not reach statistical significance, likely owing to the smaller sample size.12 A plausible explanation for this trend is Tenon’s capsule entanglement, which may be more common with the ab interno technique. Although differences in secondary glaucoma surgery and postoperative corneal edema did not reach statistical significance, the magnitude of these differences may still be clinically relevant and should be considered when selecting the surgical approach, particularly in patients at higher risk for postoperative complications.
To our knowledge, this is the first systematic review and meta-analysis to directly compare the safety of ab externo and ab interno XEN45 implantation. Our analysis examined several clinically relevant outcomes. Our findings suggest that both ab externo and ab interno approaches are effective and safe options for XEN45 implantation. The ab externo approach may offer a modest advantage in reducing postoperative needling, likely due to better Tenon’s capsule management and bleb morphology. Meanwhile, the ab interno technique offers the advantage of direct gonioscopic visualization and avoids conjunctival dissection, which may be beneficial for eyes with limited conjunctival reserve or prior surgery. The decision between approaches should thus be guided by surgeon experience, ocular anatomy, and specific patient needs rather than a clear superiority in pressure-lowering efficacy. The relatively large aggregated sample size strengthens the generalizability of our findings and provides a clearer perspective on the relative safety of both techniques.
Several limitations should be acknowledged. First, all included studies were retrospective, limiting the ability to establish causality. Second, variability and deficiencies in follow-up duration restricted comparability of IOP outcomes at specific time points. Third, evidence regarding the relative cost-effectiveness of the two techniques remains limited. Finally, future well-designed, prospective, and controlled comparative trials are needed to validate and extend these findings.
Conclusion
To conclude, the reduction in intraocular pressure (IOP) and the reduction in the need for IOP-lowering medications was statistically significant in the two approaches of XEN 45 Gel stent implantation. Although second glaucoma surgery rates were higher in the ab-interno group, both groups demonstrated similar efficacy and safety in managing glaucoma patients. However, all included studies were retrospective studies, and this warrants more randomized controlled trials to assess the long-term safety and efficacy of Ab externo approach and Ab interno approach.
Acknowledgments
We would like to express our sincere gratitude to all those who contributed to this research project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition - Chapter 2: classification and terminologySupported by the EGS Foundation: part 1: foreword; Introduction; Glossary; Chapter 2 Classification and Terminology. Br J Ophthalmol. 2017;101(5):73–9. PMID: 28424171; PMCID: PMC5583685. doi:10.1136/bjophthalmol-2016-EGSguideline.002
2. Tielsch JM, Katz J, Singh K, et al. A population-based evaluation of glaucoma screening: the Baltimore Eye Survey. Am J Epidemiol. 1991;134(10):1102–1110. PMID: 1746520. doi:10.1093/oxfordjournals.aje.a116013
3. Schuman JS. Antiglaucoma medications: a review of safety and tolerability issues related to their use. Clin Ther. 2000;22(2):167–208. PMID: 10743979. doi:10.1016/S0149-2918(00)88478-7
4. Dreer LE, Girkin C, Mansberger SL. Determinants of medication adherence to topical glaucoma therapy. J Glaucoma. 2012;21(4):234–240. PMID: 21623223; PMCID: PMC3183317. doi:10.1097/IJG.0b013e31821dac86
5. Kirwan JF, Lockwood AJ, Shah P, et al; Trabeculectomy Outcomes Group Audit Study Group. Trabeculectomy in the 21st century: a multicenter analysis. Ophthalmology. 2013;120(12):2532–2539. PMID: 24070811. doi:10.1016/j.ophtha.2013.07.049
6. Chen DZ, Sng CCA. Safety and efficacy of microinvasive glaucoma surgery. J Ophthalmol. 2017;2017:3182935. PMID: 28512578; PMCID: PMC5420434. doi:10.1155/2017/3182935
7. Schehlein EM, Kaleem MA, Swamy R, Saeedi OJ. Microinvasive glaucoma surgery: an evidence-based assessment. Expert Rev Ophthalmol. 2017;12:331–343. doi:10.1080/17469899.2017.1335597
8. De Gregorio A, Pedrotti E, Stevan G, Bertoncello A, Morselli S. XEN glaucoma treatment system in the management of refractory glaucomas: a short review on trial data and potential role in clinical practice. Clin Ophthalmol. 2018;12:773–782. doi:10.2147/OPTH.S146919
9. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
10. Ucar F, Cetinkaya S. Xen implantation in patients with primary open-angle glaucoma: comparison of two different techniques. Intl Ophthalmol. 2020;40(10):2487–2494. doi:10.1007/s10792-020-01427-z
11. El Helwe H, Ingram Z, Neeson CE, et al. Comparing outcomes of 45 Xen implantation ab interno with closed conjunctiva to Ab externo with open conjunctiva approaches. J Glaucoma. 2024;33(2):116–125. doi:10.1097/IJG.0000000000002320
12. Tan NE, Tracer N, Terraciano A, Parikh HA, Panarelli JF, Radcliffe NM. Comparison of safety and efficacy between ab interno and ab externo approaches to XEN gel stent placement. Clinical Ophthalmol. 2021;15:299–305. doi:10.2147/OPTH.S292007
13. Gallardo MJ, Vincent LR, Porter M. Comparison of clinical outcomes following gel stent implantation via ab-externo and ab-interno approaches in patients with refractory glaucoma. Clinical Ophthalmol. 2022;16:2187–2197. doi:10.2147/OPTH.S354038
14. Ruda RC, Yuan L, Lai GM, Raiciulescu S, Kim WI. Clinical outcomes of Ab Interno placement versus Ab Externo placement of XEN45 gel stents. Ophthalmol Glaucoma. 2023;6(1):4–10. doi:10.1016/j.ogla.2022.07.002
15. Yuan L, Rana HS, Lee I, Lai G, Raiciulescu S, Kim W. Short-term outcomes of Xen-45 gel stent Ab Interno Versus Ab Externo transconjunctival approaches. J Glaucoma. 2023;32(7):e71–e79. doi:10.1097/IJG.0000000000002208
16. Sterne JAC, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016;355(i4919). doi:10.1136/bmj.i4919
17. Riley RD, Higgins JPT, Deeks JJ. Interpretation of random effects meta-analyses. BMJ. 2011;342(7804):964–967. doi:10.1136/BMJ.D549
18. Nikolakopoulou A, Mavridis D, Salanti G. How to interpret meta-analysis models: fixed effect and random effects meta-analyses. BMJ Ment Health. 2014;17(2):64. doi:10.1136/EB-2014-101794
19. Andrade C. Mean difference, standardized mean difference (SMD), and their use in meta-analysis: as simple as it gets. J Clin Psychiatry. 2020;81(5). doi:10.4088/JCP.20F13681
20. Barker TH, Migliavaca CB, Stein C, et al. Conducting proportional meta-analysis in different types of systematic reviews: a guide for synthesisers of evidence. BMC Med Res Methodol. 2021;21(1):1–9. doi:10.1186/S12874-021-01381-Z/FIGURES/5
21. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/SIM.1186
22. Sterne JAC, Sutton AJ, Ioannidis JPA, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343(7818):d4002–d4002. doi:10.1136/BMJ.D4002
23. Gupta C, Mathews D. XEN® stent complications: a case series. BMC Ophthalmol. 2019;19(1):253. PMID: 31830935; PMCID: PMC6909486. doi:10.1186/s12886-019-1267-y
24. Do A, McGlumphy E, Shukla A, et al. Comparison of clinical outcomes with open versus closed conjunctiva implantation of the XEN45 gel stent. Ophthalmol Glaucoma. 2021;4(4):343–349. doi:10.1016/j.ogla.2020.12.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Update on Surgical Techniques Best Practices to Optimize Outcomes Following Gel Stent Implantation

Vera V, Sheybani A, Panarelli JF, Grover DS, Lee J, Craven ER, Samuelson TW, Ahmed IIK
Clinical Ophthalmology 2025, 19:325-347
Published Date: 31 January 2025