Back to Journals » Open Access Emergency Medicine » Volume 15
Effects of the Hazardous Area Response Team Training Program on the Knowledge and Confidence in Operational Skills of Prehospital Emergency Medical Personnel in Thailand: A Quasi-Experimental Study
Authors Huabbangyang T ![]() , Nomrabporn T, Chiraratchawarich W, Rojsaengroeng R
, Nomrabporn T, Chiraratchawarich W, Rojsaengroeng R ![]()
Received 18 August 2023
Accepted for publication 9 December 2023
Published 14 December 2023 Volume 2023:15 Pages 447—456
DOI https://doi.org/10.2147/OAEM.S436054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Thongpitak Huabbangyang,1 Thanidtha Nomrabporn,2 Watcharan Chiraratchawarich,2 Rapeeporn Rojsaengroeng3
1Department of Disaster and Emergency Medical Operation, Faculty of Science and Health Technology, Navamindradhiraj University, Bangkok, Thailand; 2Division of Emergency Medical Service and Disaster, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 3Department of Emergency Medicine, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand
Correspondence: Rapeeporn Rojsaengroeng, Tel +66 2443000, Email [email protected]
Background: Hazardous areas are places emitting hazardous materials, terrorist- or war-related, which lead to public health risks in developed and developing countries globally. Hence, prehospital emergency medical personnel who work as frontliners should be trained.
Patients and Methods: Data via pretest, posttest, and questionnaire surveys regarding the HART’s knowledge of and confidence in operational skills were collected using the 5-point Likert scale. The cohort included prehospital emergency medical personnel aged > 18 years. The training program comprised lectures, practicals, and examinations and included three subcourses: emergency medicine in the chemical, biological, radiation, and nuclear hazardous area (EM-CBRN) course; Thailand Tactical Emergency Medical Service (TTEMS) course; and cooperation and preparation for disaster (CPD) course.
Results: The HART’s mean multiple choice question (MCQ) posttest knowledge score (12.80± 3.11) was significantly higher (p< 0.001) than the mean pretest knowledge score (7.74± 3.71) for the EM-CBRN course. The HART’s mean MCQ posttest knowledge score (24.04± 2.79) was significantly higher (p< 0.001) than the mean pretest knowledge score (14.34± 3.92) for the TTEMS course. Further, the HART’s mean MCQ posttest knowledge score (21.03± 3.49) was significantly higher (p< 0.001) than the mean pretest knowledge score (14.40± 5.08) for the CPD course. The HART’s mean confidence in operational skill score for the EM-CBRN course was significantly higher (p< 0.001) after training (4.45± 0.59) than before training (2.77± 0.90). The HART’s mean confidence in operational skill score for the TTEMS course was significantly higher (p< 0.001) after training (4.55± 0.59) than before training (2.78± 0.98). The HART’s mean confidence in operational skill score for the CPD course was significantly higher (p< 0.001) after training (4.70± 0.41) than before training (3.03± 0.90).
Conclusion: The HART training program significantly affected the HART’s knowledge development and confidence in operational skills, particularly the frontline prehospital emergency medical personnel. Therefore, prehospital emergency medical personnel should undergo training, and learning activities must be developed to reinforce capacity and improve knowledge and confidence.
Keywords: education, emergency medical service, hazardous substances, knowledge, prehospital emergency care
Introduction
The World Health Organization defines hazardous areas as any place emitting or producing hazardous materials, pathogens, chemicals, biochemicals, radiation, and nuclear energy, or causing terroristic threats or war-related situations probably leading to public health risks requiring harmonized international response.1 HAZMAT is an abbreviation for high-risk materials causing danger to humans and the environment. These materials include chemicals, radioactive substances, fire, and intentionally emitted toxins, which are likely to negatively affect human health and the ecosystem and environment. Further, they may cause danger if handled incorrectly, starting from usage, storage, and transportation to disposal.2 The effects of HAZMAT to the body are based on its amount and concentration.3 Prehospital emergency medical personnel commonly encounter unpredictable situations involving HAZMAT. The prevalence of these incidents are low, or they occur rapidly without preparation. Thus, each incident leads to a significant loss.4 The 9/11 event is among the International HAZMAT incidents affecting developed countries worldwide. On September 11, 2001, al-Qaeda terrorists hijacked airplanes, which were then crashed into the World Trade Center in New York. This event is well-known globally. After 22 years, it still has effects. Based on a previous systematic review, the first responders and emergency medical personnel of such disaster developed different types of cancer. Several studies have found that the incidence of prostate and thyroid cancer among first responders and emergency medical personnel increased compared with that in the general population. Moreover, some studies have revealed an increase in cancer incidence after several years.5
On March 11, 2011, an earthquake in Japan caused a tsunami leading to radiation emission from the Fukushima Daiichi nuclear power plant. This incident affected public health worldwide due to the large amount of radioactivity leak. This was then considered the worst nuclear disaster globally since the Chernobyl tragedy in 1986. More than 300,000 people who had lived near the nuclear power plant needed to temporarily migrate. Moreover, several areas were declared as an exclusion zone for 10 years.6 Then, the World Health Organization reported the risk of cancer development in the long term among the populations who were in the Fukushima Daiichi nuclear power plant incident. In particular, migrant female infants are at high risk of thyroid cancer (0.75–1.25%) due to contact with radioactive iodine.7 In developing countries, particularly Thailand, 24 kindergarten students and 2 homeroom teachers were killed in a nursery school shooting on October 6, 2022, in Nong Bua Lamphu. This was considered a significant tragedy.8 On December 18, 2022, the HTMS Sukhothai sank in the ocean of Thailand. In total, 24 people died, and five were missing.9 The Information Technology for Emergency Medical System in Thailand has evaluated the prevalence of public disaster and incidence of mass casualties (n=7753) requiring supportive emergency medical ambulances during 2022. In addition, there was an increased incidence of mass casualties during the long holidays in various places in Thailand, such as Songkran, and on New Year’s day.10
Earlier when there were insurgent or public disaster incidents in Thailand, relevant national organizations including ministries and provincial ones provided assistance in relief operations and addressed specific issues. The missions in disaster assistance and mitigation in responsible areas are under law defining power and duty in disaster prevention and mitigation according to the Disaster Prevention and Mitigation Act B.E. 2550.11 The National Institute for Emergency Medicine plays a role in emergency medical management based on the Emergency Medical Act B.E.2551.12 Moreover, it has a mission in not only the management of critical/emergency patients but also the provision of education and training among prehospital emergency medical personnel and for preparing for situations in hazardous areas in Thailand. That is, it facilitated the Hazardous Area Response Team (HART) training program for prehospital emergency medical personnel in the hazardous area response team in Bangkok, Thailand. The program was divided into three subcourses, which were as follows: emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course; the Thailand tactical emergency medical service (TTEMS); and the cooperation and preparation for disaster course. To appropriately improve training courses in the future and to evaluate achievements after the training program, the current study aimed to evaluate the knowledge and confidence in operational skill scores of prehospital emergency medical personnel who participated in the 8-day HART training in Thailand.
Materials and Methods
Study Design and Setting
This quasi-experimental study collected data via pretest and posttest from November 2, 2022, to November 11, 2022. The training program provided by the National Institute for Emergency Medicine, Thailand, comprised lectures with practice. Further, it had three subcourses, which were as follows: emergency medicine in the chemical, biological, and radiation hazardous area course from November 2, 2022, to November 4, 2022, at Directorate of Air Medical Services; the TTEMS course from November 7, 2022, to November 9, 2022, at Medical Battalion, Marine Service Support Regiment, Sattahip, Chonburi; and cooperation and preparation for disaster course from November 10, 2022, to November 11, 2022, at National Institute for Emergency Medicine, Nonthaburi. Supplementary Table 1 shows the details about the training schedule in each course.
The training program aimed to ensure the safety of the operating staff and emergency patients in the hazardous areas. Small operation teams, including advanced life support and basic life support teams with capability in danger evaluation, coordination, self-defense, and emergency patient management in hazardous areas, were established. The training program was a pilot project. The participants were from 14 emergency medical units in Bangkok, Thailand. The study was conducted in accordance with the Standards for the Reporting of Observation Studies in Epidemiology.13
Participants
Prehospital emergency medical personnel (including emergency medical technicians, nurses/emergency nurses, advanced emergency medical technicians, paramedics, and physicians/emergency physicians) who participated in the HART training program from November 2, 2022, to November 11, 2022, were included in the study.
Eligibility Criteria
The eligibility criteria included prehospital emergency medical personnel aged > 18 years, those who provided consent for the HART training program, and those who attended the 8-day training program.
Exclusion Criteria
The exclusion criteria included patients with incomplete data, including the knowledge test or questionnaire survey results.
Data Collection
In the pretest and posttest, each course had four multiple choice questions (MCQs), which were developed by the assigned lecturers of each topic. The content validity index (CVI) was used to validate the knowledge tests by three prehospital emergency medical scholars. Then, the item objective congruence (IOC) was evaluated. The OIC of each test question was 1. The pretest and posttest were divided into the following: (1) emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course (20 questions); (2) the TTEMS course (30 questions); and (3) the cooperation and preparation for disaster course (30 questions). The exam duration was 60 min.
Questionnaires on confidence in operational skills before and after the training were similar to those developed by the authors and were validated using the CVI by three prehospital emergency medical scholars. The OIC of each questionnaire was 1. The questions were divided into two parts. The first part comprised closed-ended questions with choices about personal data including sex, age, educational level, job title, working experience in emergency operations in hazardous areas, and working experience in emergencies in hazardous areas and common emergency in hazardous areas. The second part included closed questions on confidence in operational skills before and after the HART program in all three courses. The questionnaire was divided before and after the training with five questions each. Then, the responder was instructed to select only one option per question. The questions used rating scales in accordance with the 5-point Likert scale. For the scoring criteria, 5 is the highest score; 4, high score; 3, neutral score; 2, low score; and 1, lowest score. For the mean score, the authors used the criteria in a previous study,12 which included the following: 4.21–5.00, the highest level; 3.41–4.20, high level; 2.61–3.40, neutral level; 1.81–2.60, low level; and 1.00–1.80, the lowest level. The principal investigator (TH) collected data via pretest, posttest, and questionnaire survey on confidence in operational skills before and after the training using google forms and Microsoft excel.
Outcome Measures
The primary objective was to compare knowledge scores before and after (MCQ pretest–posttest) participation in the HART training. The secondary objective was to compare confidence in operational skill scores before and after training.
Sample Size Determination
The primary objective was to compare knowledge scores before and after (MCQ pretest–posttest) the HART training. Due to the lack of previous studies, there was no statistical value for reference in sample size calculation using the sample size estimation method with the sample size calculation formula. Therefore, the sample size was determined using sample size estimation with G power version 3.1.9.4 for paired samples t-test to test differences between two dependent means. The power of test of 95% (α=0.05) and the medium effect size (d of 0.5) were defined.14 There was no reference study on statistical values in the sample size calculation of effect size. The calculated sample size from the program was at least 54. Next, 20% of the sample size was added using the sample size adjustment formula to prevent incomplete response and withdrawal from the study, and the final sample size was at least 68. Hence, the sample size of the current study was 70.
Statistical Analyses
A descriptive analysis was performed to examine variable distribution. Continuous variables were presented as mean ± standard deviation (SD) or median and interquartile range (IQR). Categorical variables were expressed as frequencies and proportions. If two groups were compared, differences were evaluated using the independent t-test or the Mann–Whitney U-test for numeric variables and the chi-square test or the Fisher’s exact test for categorical variables.
To compare knowledge scores between the MCQ pretest–posttest during the HART training and confidence in operational skill score before and after the HART training, the paired sample t-test or the Wilcoxon signed-rank test was used to evaluate data appropriateness. The Statistical Package for the Social Sciences software for Windows version 28.0 (IBM Corp., Armonk, NY, the USA) was used. A p-value of<0.05 was considered statistically significant.
Results
General Characteristics of the Participants
The prehospital emergency medical personnel (n=70, 82.9%) were men, with a mean age of 34.7±7.69 years. Approximately 45.7% of participants attained high school or vocational education, 64.3% were emergency medical technicians. The median working experience period was 7 (IQR: 4–10) years. Approximately 32.9% of the participants had training in emergency operations in hazardous areas. Further, the participants had working experience in emergency situations in hazardous areas (45.7%) and common emergencies in hazardous areas including fire (87.1%), flood (41.4%), chemical leak (18.6%), terrorist attack/homicide (10%), and protest (1.4%), as shown in (Table 1).
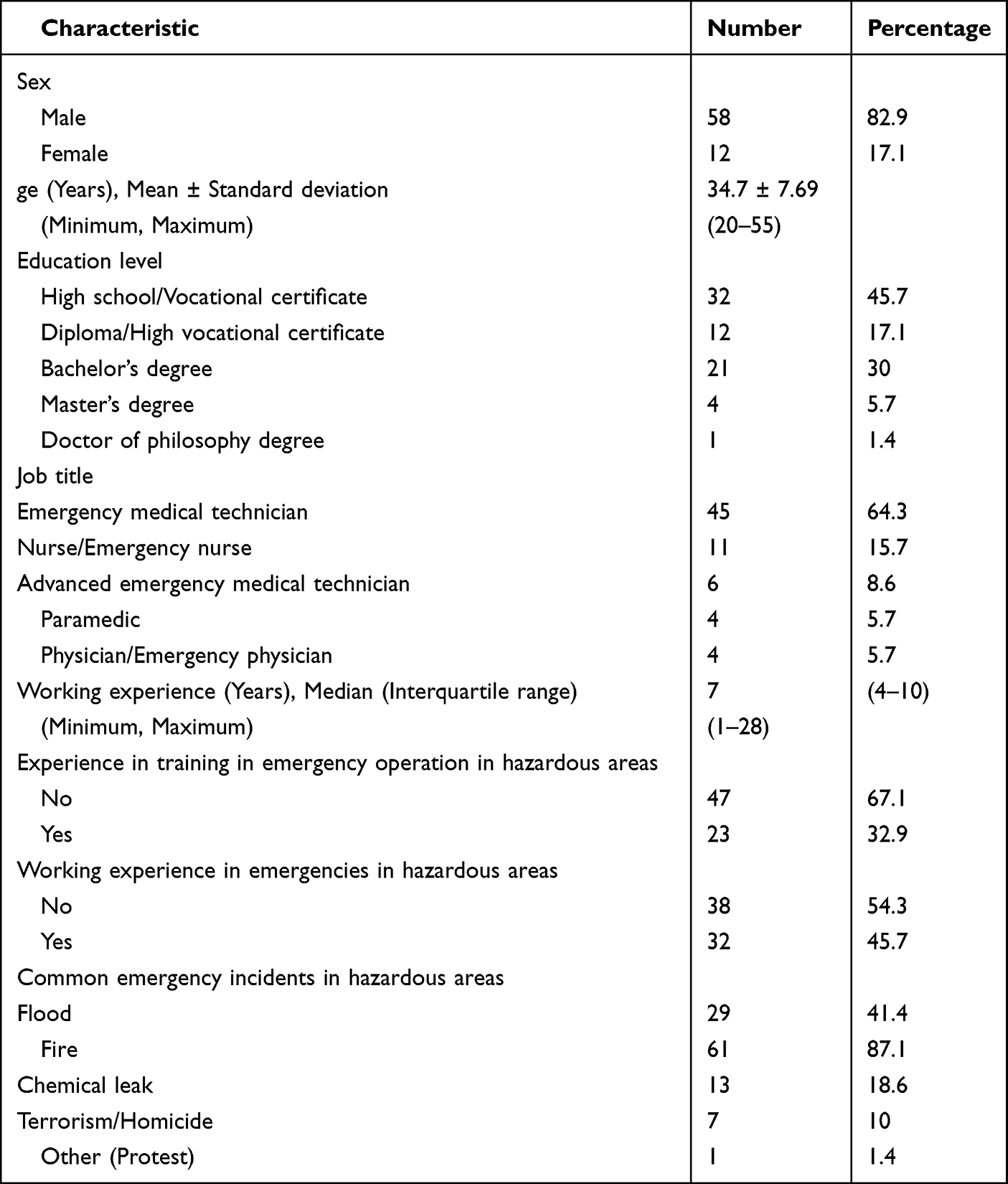 |
Table 1 General Characteristic Data of Sample (n = 70) |
MCQ Pretest and Posttest Knowledge Scores
The mean pretest and posttest knowledge scores for emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course were 7.74±3.71 and 12.80±3.11, respectively. The average posttest knowledge score was significantly higher than the pretest score. The mean pretest and posttest knowledge scores in the TTEMS course were 14.34±3.92 and 24.04±2.79, respectively. The average posttest knowledge score was significantly higher than the pretest score. The mean pretest and posttest knowledge scores for the cooperation and preparation for disaster course were 14.40±5.08 and 21.03±3.49, respectively. The average posttest knowledge score was significantly higher than the pretest score, as depicted in (Table 2).
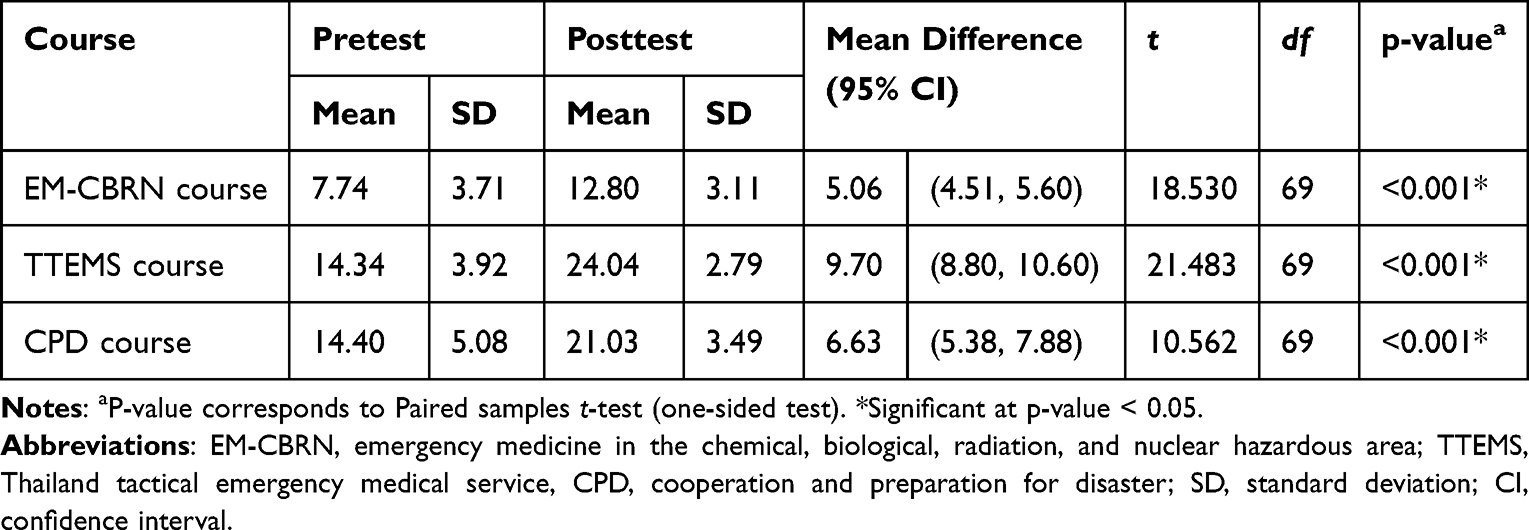 |
Table 2 Results of Comparison of Mean HART Knowledge Score Level Between Pretest and Posttest of the Training |
Confidence in Operational Skill Score Before and After the HART Training
For HART operating skills in emergency medicine in chemical, biological, radiation and nuclear hazardous area course, sample had mean confidence score of operating skills regarding management principle of chemical, biological, radiation and nuclear accidents in overall image before and after HART training participation in neutral ( =2.89, SD=0.93) and the highest levels (
=2.89, SD=0.93) and the highest levels ( =4.30, SD=0.73), respectively, skills in classification of chemicals, lives and nuclear radiation before and after HART training participation in neutral (
=4.30, SD=0.73), respectively, skills in classification of chemicals, lives and nuclear radiation before and after HART training participation in neutral ( =2.76, SD=0.94) and the highest levels (
=2.76, SD=0.94) and the highest levels ( =4.44, SD=0.65), respectively, skills in risk analysis of chemical, biological, radiation and nuclear accidents before and after HART training participation in neutral (
=4.44, SD=0.65), respectively, skills in risk analysis of chemical, biological, radiation and nuclear accidents before and after HART training participation in neutral ( =2.70, SD=1.04) and the highest levels (
=2.70, SD=1.04) and the highest levels ( =4.47, SD=0.65), respectively, skills in evaluation of impacts from chemical, biological, radiation and nuclear accidents before and after HART training participation in neutral (
=4.47, SD=0.65), respectively, skills in evaluation of impacts from chemical, biological, radiation and nuclear accidents before and after HART training participation in neutral ( =2.74, SD=1.07) and the highest levels (
=2.74, SD=1.07) and the highest levels ( =4.51, SD=0.72), respectively and if chemical, biological, radiation and nuclear accidents happen in the future, resuscitation and emergency medical system administration can be performed before and after HART training participation in neutral (
=4.51, SD=0.72), respectively and if chemical, biological, radiation and nuclear accidents happen in the future, resuscitation and emergency medical system administration can be performed before and after HART training participation in neutral ( =2.79, SD=1.10) and the highest levels (
=2.79, SD=1.10) and the highest levels ( =4.54, SD=0.70), respectively as demonstrated in (Table 3).
=4.54, SD=0.70), respectively as demonstrated in (Table 3).
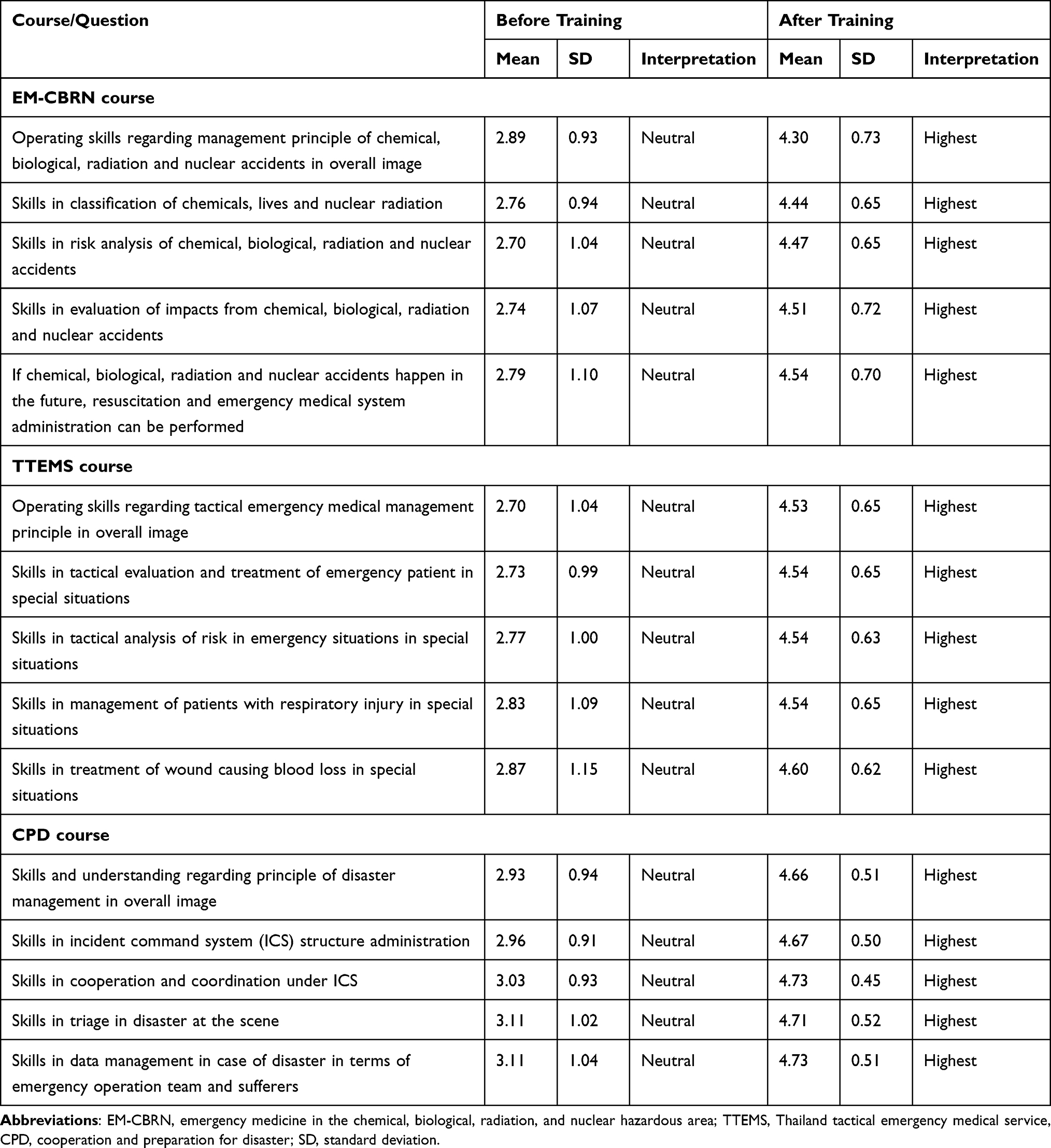 |
Table 3 Mean and Standard Deviation of Confidence Score in HART Skills Before and After Training Participation, Classified into Individual Item |
For TTEMS course, sample had mean confidence score of operating skills regarding tactical emergency medical management principle in overall image before and after HART training participation in neutral ( =2.70, SD=1.04) and the highest levels (
=2.70, SD=1.04) and the highest levels ( =4.53, SD=0.65), respectively, skills in tactical evaluation and treatment of emergency patient in special situations before and after HART training participation in neutral (
=4.53, SD=0.65), respectively, skills in tactical evaluation and treatment of emergency patient in special situations before and after HART training participation in neutral ( =2.73, SD=0.99) and the highest levels (
=2.73, SD=0.99) and the highest levels ( =4.54, SD=0.65), respectively, skills in tactical analysis of risk in emergency situations in special situations before and after HART training participation in neutral (
=4.54, SD=0.65), respectively, skills in tactical analysis of risk in emergency situations in special situations before and after HART training participation in neutral ( =2.77, SD=1.00) and the highest levels (
=2.77, SD=1.00) and the highest levels ( =4.54, SD=0.63), respectively, skills in management of patients with respiratory injury in special situations before and after HART training participation in neutral (
=4.54, SD=0.63), respectively, skills in management of patients with respiratory injury in special situations before and after HART training participation in neutral ( =2.83, SD=1.09) and the highest levels (
=2.83, SD=1.09) and the highest levels ( =4.54, SD=0.65), respectively and skills in treatment of wound causing blood loss in special situations before and after HART training participation in neutral (
=4.54, SD=0.65), respectively and skills in treatment of wound causing blood loss in special situations before and after HART training participation in neutral ( =2.87, SD=1.15) and the highest levels (
=2.87, SD=1.15) and the highest levels ( =4.60, SD=0.62), respectively as demonstrated in (Table 3).
=4.60, SD=0.62), respectively as demonstrated in (Table 3).
For cooperation and preparation for disaster course, sample had mean confidence score of skills and understanding regarding principle of disaster management in overall image before and after HART training participation in neutral ( =2.93, SD=0.94) and the highest levels (
=2.93, SD=0.94) and the highest levels ( =4.66, SD=0.51), respectively, skills in incident command system (ICS) structure administration before and after HART training participation in neutral (
=4.66, SD=0.51), respectively, skills in incident command system (ICS) structure administration before and after HART training participation in neutral ( =2.96, SD=0.91) and the highest levels (
=2.96, SD=0.91) and the highest levels ( =4.67, SD=0.50), respectively, skills in cooperation and coordination under ICS before and after HART training participation in neutral (
=4.67, SD=0.50), respectively, skills in cooperation and coordination under ICS before and after HART training participation in neutral ( =3.03, SD=0.93) and the highest levels (
=3.03, SD=0.93) and the highest levels ( =4.73, SD=0.45), respectively, skills in triage in disaster at the scene before and after HART training participation in neutral (
=4.73, SD=0.45), respectively, skills in triage in disaster at the scene before and after HART training participation in neutral ( =3.11, SD=1.02) and the highest levels (
=3.11, SD=1.02) and the highest levels ( =4.71, SD=0.52), respectively and skills in data management in case of disaster in terms of emergency operation team and sufferers before and after HART training participation in neutral (
=4.71, SD=0.52), respectively and skills in data management in case of disaster in terms of emergency operation team and sufferers before and after HART training participation in neutral ( =3.10, SD=1.04) and the highest levels (
=3.10, SD=1.04) and the highest levels ( =4.73, SD=0.51), respectively as demonstrated in (Table 3).
=4.73, SD=0.51), respectively as demonstrated in (Table 3).
The mean confidence in operational skill scores of emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course before and after the HART training were 2.77±0.90 and 4.45±0.59, respectively. The mean score after training was significantly higher than that before training (vs 1.68, 95% CI: 1.51–1.85) (p-value<0.001). The mean confidence in operational skill scores of the TTEMS course before and after the HART training were 2.78±0.98 and 4.55±0.59, respectively. The mean score after training was significantly higher than that before training (vs 1.77, 95% CI: 1.57–1.97) (p-value<0.001). The mean confidence in operational skill scores of the cooperation and preparation for disaster course before and after the HART training were 3.03±0.90 and 4.70±0.41, respectively. The mean score after training was significantly higher than that before training (vs 1.67, 95% CI: 1.48–1.86) (p-value<0.001), as shown in (Table 4).
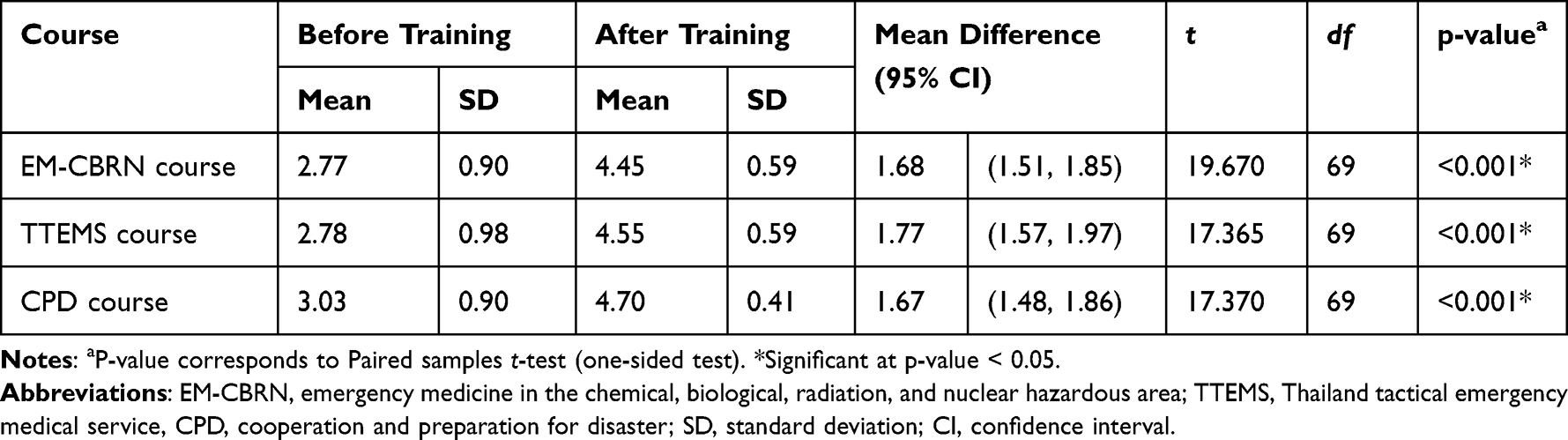 |
Table 4 Results of Mean Confidence Score in HART Skills Before and After Training Participation |
Discussion
The mean knowledge scores of the posttest score in all three courses was higher than that of the pretest score (mean difference 5.06, 95% CI: 4.51–5.60). The posttest score in the TTEMS course was higher than the pretest score (mean difference 9.70, 95% CI: 8.80–10.60). The posttest score for the cooperation and preparation in the disaster course was higher than the pretest score (mean difference 6.63, 95% CI: 5.38–7.88). This finding was consistent with that of a previous study on the training of prehospital emergency personnel in United States Armed Forces, such as physicians and physician assistants. After the completion of training on tactical combat casualty care (TCCC) course, the knowledge score increased.15 This result was comparable to that of a previous study reporting knowledge score in the clinical competency of nurses and medics who passed the TCCC, disaster management, and advanced cardiac life support courses. Their knowledge increased after they have passed the training.16 These findings were also consistent with those of a previous study conducted in Ethiopia. That is, after the nurses passed the training in the preparation of emergency and disaster management course, their mean knowledge scores significantly increased.17 A previous study showed that the emergency medical staff of Thailand had high occupational risks, particularly risks for infection and poison and chemical exposure because they worked as frontliners. In addition, this study found that prehospital emergency medical personnel did not participate in trainings, and they lacked skill support in operations involving chemicals and HAZMAT.18 The three training courses in the HART training program included emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course, TTEMS course, and cooperation and preparation for disaster course, which were set as a pilot in prehospital emergency medical staff in Bangkok, Thailand. In this training, each course focused on interactive lecture and practices in simulated settings, which were helpful in the integrated education in hazardous area management systematically among prehospital emergency medical staff. Moreover, the course provided a step-by-step information on the cognitive, skill, and affective domains, which provided confidence to prehospital emergency medical staff in the management of danger in hazardous areas from their own capacity from applying knowledge and skills obtained from the HART training program. The development of knowledge among prehospital emergency medical personnel was important. A previous study showed that knowledge was a determining factor of readiness for handling disaster management and that appropriate knowledge is associated with confidence in skill application during operations.19
Second, to compare confidence in operational skill score before and after the HART training, the participants had increased mean operating skill confidence scores in each course after training. The mean score level for emergency medicine in the chemical, biological, radiation, and nuclear hazardous area course after training was higher than that before the training (vs 1.68, 95% CI: 1.51–1.85). The mean score for the TTEMS course after training was higher than that before training (vs 1.77, 95% CI: 1.57–1.97). Further, the mean score for cooperation and preparation in the disaster course after training was higher than that before training (vs 1.67, 95% CI: 1.48–1.86). This finding was consistent with that of a previous study on the training of prehospital emergency medical personnel in the United States Armed Forces. After the completion of training with the TCCC course, the confidence in operational skill score of the participants increased.15 This result was comparable to that of a previous study showing that after completing the training with the Combat Lifesaver course, prehospital emergency medical personnel who were not physicians had increased confidence in entering the scenes and performing resuscitation and other procedures.20 This is also consistent with a study reporting that after passing advanced life support training, nursing students had a higher confidence skill score in resuscitating patients in emergency/critical settings.21 Confidence skills are extremely important in emergency medical operations, particularly those in hazardous areas because confidence can lead to good and accurate practice, especially in emergency/critical situations faced by prehospital emergency medical staff. This is comparable to the individual self-efficacy concept, which indicates improvement in individual self-efficacy. An efficient method is associated with performance accomplishment. This can help build confidence, thereby perceiving their capability and trying to use skills to succeed goals.22 In all three courses, prehospital emergency medical staff perceived their abilities more, and they had increased confidence skills during operations because they had more procedural education than theory learning in classroom, practical education, including working experience exchange and reciprocating knowledge between teachers and learners. These factors can increase learners’ skills, knowledge, and confidence.
Study Limitations
The current study had several limitations. First, only emergency medical personnel in the Bangkok area were included, and this could have led to selection bias. Second, the training programs in the courses were determined by the National Institute for Emergency Medicine. The training period of each course differed. The authors could not intervene in the training period of each course. Third, the pretest and posttest of each course were similar, which might have caused a learning curve of knowledge measurement. Hence, the pretest and posttest should have different examinations. Fourth, although the CVI was used in the confidence questionnaires by three prehospital emergency medical scholars, there was no reliability test for the developed confidence questionnaire tools. Fifth, the study is using the same questions for pretest and posttests. Six, currently the post test is conducted immediately after the training. However, there are no insights regarding if the knowledge gain is longitudinal, knowledge outcome was immediately evaluated after training which might lead to bias from learning curve. Finally, there was no practicing skill measurement. Only the MCQ examination was used to measure knowledge, and the questionnaire was utilized to assess confidence skills during operations. Therefore, future research must be conducted to appropriately identify knowledge and skills in actual practice.
Conclusion
The HART training program significantly affected the development of knowledge and confidence in operational skills of frontline prehospital emergency medical personnel. Therefore, to address knowledge gap, prehospital emergency medical personnel should undergo trainings, and learning activities must be developed to reinforce capacity and improve knowledge and confidence.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The ethical consideration of the study protocol was granted by at the Institutional Review Board of the Faculty of Medicine, Vajira Hospital, Navamindradhiraj University (COA no. 089/2566). The committee reviewed the study protocol, methodology, and potential ethical implications to ensure participant protection, privacy, and compliance with ethical guidelines. A written informed consent was obtained from each participant before research participation. The study data were kept under confidentiality to ensure the privacy of the study participants. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors were grateful to the National Institute for Emergency Medicine and Erawan Center, Bangkok for supporting funds in provision of the hazardous area response team’s (HART) training program and Navamindradhiraj University Research Fund for supporting funds in development of the present research. We would like to thank Mr Chanathip Wanphen and Mr Thanakorn Faikhao, paramedic students at Faculty of Medicine Vajira Hospital, Navamindradhiraj University, for data collection in the present study.
Author Contributions
All authors made a significant contribution to the study conception, design, execution, acquisition of data, analysis or interpretation of data, or in all these areas. All authors took part in drafting, revising, or critically reviewing the article. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The study was funded by Navamindradhiraj University who played no role in study design, data collection, data analysis, or writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Exposure to hazardous area [Internet]; 2023. Available from: https://www.who.int/tools/occupational-hazards-in-health-sector/exposure-to-hazardous-chemicals.
2. Ng CA, von Goetz N. The global food system as a transport pathway for hazardous chemicals: the missing link between emissions and exposure. Environ Health Perspect. 2017;125(1):1–7. doi:10.1289/EHP168
3. Murray V, Goodfellow F. Mass casualty chemical incidents--towards guidance for public health management. Public Health. 2002;116(1):2–14. doi:10.1016/S0033-3506(02)90053-3
4. Moles TM. Emergency medical services systems and HAZMAT major incidents. Resuscitation. 1999;42(2):103–116. doi:10.1016/S0300-9572(99)00096-9
5. Boffetta P, Hall CB, Todd AC, et al. Cancer risk among world trade center rescue and recovery workers: a review. CA Cancer J Clin. 2022;72(4):308–314. doi:10.3322/caac.21723
6. Law RK, Schier JG, Martin CA, et al. National surveillance for radiological exposures and intentional potassium iodide and iodine product ingestions in the United States associated with the 2011 Japan radiological incident. Clin Toxicol. 2013;51(1):41–46. doi:10.3109/15563650.2012.732701
7. World Health Organization. Despite the fear, the health risks from the Fukushima accident are minimal [Internet]; 2023. Available from: https://science.time.com/2013/03/01/meltdown-despite-The-fear-The-health-risks-from-The-fukushima-accident-are-minimal/#ixzz2MnbjhPmv.
8. BBC News. Shooting incident in Nong Bua Lamphu province, Thailand [Internet]; 2023. Available from: https://www.bbc.com/thai/articles/clm8lx797gyo.
9. BBC News. Sukhothai royal ship capsized [Internet]; 2022. Available from: https://www.bbc.com/thai/articles/cml0ydv8y00o.
10. Information Technology for Emergency Medical System. Disaster report system [Internet]; 2023. Available from: http://ws.niems.go.th/disaster/.
11. Sri-On J, Vanichkulbodee A, Sinsuwan N, Rojsaengroeng R, Kamsom A, Liu SW. Disaster preparedness among Thai elderly emergency department patients: a survey of patients’ perspective. BMC Emerg Med. 2019;19(1):58. doi:10.1186/s12873-019-0269-7
12. National Institute for Emergency Medicine. Emergency medical act B.E. 2551; 2023. Available from: https://www.niems.go.th/1/SubWebsite/?id=38.
13. Best JW, Kahn JV. Research in Education.
14. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Academic press; 2013.
15. Gurney JM, Stern CA, Kotwal RS, et al. Tactical combat casualty care training, knowledge, and utilization in the US army. Mil Med. 2020;185(Suppl 1):500–507. doi:10.1093/milmed/usz303
16. Suresh MR, Valdez-Delgado KK, Staudt AM, Trevino JD, Mann-Salinas EA, VanFosson CA. An assessment of pre-deployment training for army nurses and medics. Mil Med. 2021;186(1–2):203–211. doi:10.1093/milmed/usaa291
17. Tilahun L, Desu B, Zeleke M, Dagnaw K, Andualem A. Emergency and disaster handling preparedness among front line health service providing nurses and associated factors at emergency department, at Amhara Regional State Referral Hospitals, Ethiopia. Open Access Emerg Med. 2021;13:221–232. doi:10.2147/OAEM.S310932
18. Unahalekhaka A. Obstacles and needs of first responders in Northern Region: a Mixed Methods Study. J Emerg Med Serv Thailand. 2022;2(1):3–16.
19. Emaliyawati E, Ibrahim K, Trisyani Y, Mirwanti R, Ilhami FM, Arifin H. Determinants of nurse preparedness in disaster management: a Cross-Sectional Study among the community health nurses in coastal areas. Open Access Emerg Med. 2021;13:373–379. doi:10.2147/OAEM.S323168
20. Studer NM, Horn GT, Armstrong JH. Self-rated readiness for performance of needle decompression in combat lifesaver training. Mil Med. 2013;178(11):1218–1221. doi:10.7205/MILMED-D-13-00141
21. Kumkong M, Leejareon P, Aramrom Y, Jitviboon A. Effects of simulation-based learning on perceived self-efficacy in providing nursing care for advanced life support to patients with critical illness or emergency condition among nursing students. SCNJ. 2016;3:52–64.
22. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26. doi:10.1146/annurev.psych.52.1.1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Basic Determinants of Disease Knowledge in COPD Patients: Results from COSYCONET
Fischer C, Jörres RA, Alter P, Trudzinski FC, Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D, Behr J, Watz H, Holle R, Kahnert K
Patient Preference and Adherence 2022, 16:1759-1770
Published Date: 26 July 2022
Are We Scared of Clinical Trials if Not Sufficiently Informed and Educated?
Burnazovic-Ristic L, Todic A, Maleskic Kapo S, Kusturica J, Kulo Cesic A, Loga-Zec S, Aganovic-Musinovic I, Rakanovic-Todic M
Advances in Medical Education and Practice 2022, 13:1359-1366
Published Date: 27 October 2022
Comparing Knowledge Acquisition and Retention Between Mobile Learning and Traditional Learning in Teaching Respiratory Therapy Students: A Randomized Control Trial
Alhamad BR, Agha S
Advances in Medical Education and Practice 2023, 14:333-342
Published Date: 6 April 2023
The Effect of Family Planning Education on Knowledge, Attitude and Practice Toward Family Planning Methods Among Married Couples in Kersa and Goma Districts of Jimma Zone, South West Ethiopia
Yadassa F, Debelew GT, Birhanu Z
Risk Management and Healthcare Policy 2023, 16:2051-2062
Published Date: 2 October 2023
Assessing the Proficiency in Basic and Advanced Life Support Among Physicians in Ecuador: A Cross-Sectional Study
Izquierdo-Condoy JS, Naranjo-Lara P, Arias Rodríguez FD, Puglla-Mendoza AG, Jima-Sanmartín J, Andrade Casanova D, Duque-Sánchez EP, Alegría N N, Rojas Cadena MG, Ortiz-Prado E
Advances in Medical Education and Practice 2024, 15:25-35
Published Date: 6 January 2024