Back to Journals » Journal of Pain Research » Volume 15
Effects of Preoperative Electroacupuncture on Remifentanil-Induced Post-Infusion Hyperalgesia in Patients Undergoing Thyroidectomy: A Double-Blind Randomized Controlled Trial
Authors Li S, Hu C, Zhu J, Zhou Y, Cui Y, Xu Q, Tian W
Received 8 March 2022
Accepted for publication 11 May 2022
Published 20 May 2022 Volume 2022:15 Pages 1465—1474
DOI https://doi.org/10.2147/JPR.S365587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Sha Li, Cheng Hu, Juan Zhu, Yudi Zhou, Yaomei Cui, Qian Xu, Weiqian Tian
Department of Anesthesiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Weiqian Tian, Department of Anesthesiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Hanzhong Road 155, Nanjing, Jiangsu, 210029, People’s Republic of China, Tel +86 139 14764426, Email [email protected]
Objective: Electroacupuncture (EA) delivered one day before surgery could reduce postoperative pain. Remifentanil-induced post-infusion hyperalgesia (RPH) was occurred after exposure to high-dose remifentanil. This study aimed to investigate the effects of preoperative EA on RPH in patients undergoing thyroidectomy.
Methods: A total of 80 patients who were scheduled to undergo elective thyroidectomy were randomly assigned to two groups: an EA group and a sham EA (SEA) group. EA was delivered at the Zusanli (ST36) and Neiguan (PC6) acupoints 24 h before the surgery. To ensure uniformity across all patients, remifentanil was administered at the same set rate (0.3 μg/kg/min) to all patients. Mechanical pain thresholds were recorded by an electronic von Frey device around the skin incision and on the arm before surgery as well as at 30 min and 6, 24, and 48 h after surgery.
Results: At 30 min and 6 h after surgery, the EA group showed considerably greater mechanical pain thresholds surrounding the surgical site compared with the SEA group. At 30 min and 6 h after surgery, the patients in the SEA group showed a greater incidence of postoperative hyperalgesia surrounding the surgical site than those in the EA group. At 24 and 48 h after surgery, no significant differences were found between the two groups, although the pain intensity of the EA group was less than that of the SEA group. There were also no substantial differences between the two groups in the frequency of postoperative adverse reactions and rescue analgesia needed.
Conclusion: EA administered 24 h before surgery could alleviate RPH in patients undergoing thyroidectomy.
Keywords: electroacupuncture, remifentanil-induced, post-infusion hyperalgesia, thyroidectomy, Zusanli acupoint, Neiguan acupoint
Introduction
Opioids are the standard drug intervention for moderate and severe pain, with remifentanil (a short-acting opioid) being frequently used for general anesthesia.1 However, experimental and clinical studies have reported a paradoxical phenomenon termed remifentanil-induced post-infusion hyperalgesia (RPH), in which pain sensitivity increases after the administration of high doses of remifentanil during surgery.2–4 The proposed mechanism for this condition is associated with the N-methyl-D-aspartate (NMDA) receptors activated by remifentanil.5 RPH is also believed to be related to central sensitization and belongs to the category of secondary hyperalgesia.6,7 Recently, some studies have reported that a continuous infusion of remifentanil at a dosage of 0.3 μg/kg/min during general anesthesia leads to RPH.4,8 Several drugs (eg, dexmedetomidine, low-dose buprenorphine, and intraoperative naloxone) and transcutaneous electric acupoint stimulation have been used to mitigate RPH.6,8–10
A quantitative sensory test (QST) is a reliable method of quantifying hyperalgesia and evaluating the magnitude of changes in pain sensation in surgical patients. Furthermore, it can adequately distinguish between hyperalgesia and pain intensity.11 Clinical trials have reported the use of QST in patients undergoing thyroidectomy who experienced RPH (9, 10). Von Frey monofilament (VFM) testing is also used as a QST to explore mechanical hyperalgesia,12 and an electronic von Frey monofilament (EvF) device has been found to be more dependable and less time consuming in the measurement of mechanical pain levels than traditional VFM devices.12
Electroacupuncture (EA), also called acupuncture analgesia, is a type of non-pharmacological therapy that has multiple therapeutic effects, including the alleviation of various types of pain. This makes it an attractive technique for assessing pain threshold. Although animal experiments have suggested that EA attenuates morphine tolerance,13,14 a few clinical trials have shown that it can help treat RPH. Furthermore, although previous studies have shown that EA delivered one day before surgery can reduce postoperative pain,15,16 the best time to administer EA to relieve RPH remains unclear, and the effect of preoperative EA on RPH in patients who have undergone thyroidectomy has not been explored. The present study therefore utilized an EvF device to examine the effects of preoperative EA on RPH in patients undergoing thyroidectomy. We hypothesized that EA delivered at the Zusanli (ST36) and Neiguan (PC6) acupoints 24 h before surgery could alleviate RPH, relieve postoperative pain in patients undergoing thyroidectomy.
Materials and Methods
Study Design
Randomization and double-blinding methods were used in this prospective single-center trial. Approval of the research was granted by the Human Research Ethics Committee of the Affiliated Hospital of Nanjing University of Traditional Chinese Medicine, Nanjing, China (2021NL-198-02), and it was registered at the Chinese Clinical Trial Registry (ChiCTR2100050235) before patient enrollment. All patients were briefed on the procedures and methodologies used in the research before it began, regardless of whether they were in the EA group or sham EA (SEA) group. Written informed consent was obtained from each patient before participation in the study.
Study Population
Between December 2021 and January 2022, a total of 83 patients of either sex were considered for enrollment in the study, with 80 finally being included.
Inclusion criteria: (1) aged 18–80 years; (2) American Society of Anesthesiologists physical status class I or II; (3) receiving elective thyroidectomy under general anesthesia.
Exclusion criteria: (1) history of operative treatment; (2) history of severe pain, including current pain treatment; (3) pregnant or breastfeeding; (4) mental or neurological disorder or intellectual disabilities; (5) implanted cardiac defibrillator, cardioverter, or pacemaker; (6) a rash or local infection on the stimulated skin area; (7) unexpected development of intraoperative drug allergies or requirement for surgical intervention associated with postoperative complications during the study.
Randomization and Blinding
Randomization was performed at a 1:1 ratio using a computer-generated list. The 80 patients were assigned at random to one of two groups using a sealed envelope: an EA group and an SEA group (n = 40 each).
All study personnel, including patients, the anesthetist, the investigator, the surgeons, and the recovery ward nurses who collected the data, were blinded to the group assignments.
Interventional Procedures
EA Group
Patients in the EA group were administered EA at the bilateral Zusanli (ST36) and Neiguan (PC6) acupoints within 24 h before surgery in the general surgical ward. Stainless steel needles (0.30 × 40 mm; Suzhou Medical Supplies Factory Co. Ltd, China) were used for the acupuncture. A stimulator (XS-998B, Nanjing Xiaosong Medical Instrument Research Institute, Nanjing, China) was then used to provide electrical stimulation in the dense-disperse stimulation mode (20–100 Hz) for 30 min, after which a registered acupuncturist delivered EA. Although the intensity of the EA stimulation was high, the patients judged it to be both safe and comfortable; if any patient had reported discomfort or dizziness, the treatment would have been stopped.
SEA Group
Patients in the SEA group were administered a non-invasive SEA method reported by Zheng et al.17 To begin, an empty plastic guiding tube was used to produce discernible sensation, after which the tube was pressed onto the non-acupoint close to the real point but not along any meridians. Then, bent needles (the same as those used in the EA group) with adhesive bandages were placed on each acupoint’s dermal surface. The needles were attached by means of an EA stimulator that did not provide electrical stimulation. The stimulator, which displayed a continually flashing light, was positioned within the subject’s line of sight. The acupuncturist repositioned the stimulator twice and applied the bent needles to the skin three times during the procedure to ensure that there was a distinct feeling and not merely a Deqi sensation.
Anesthesia Protocol
All patients underwent a standardized anesthetic protocol on the day of surgery and were asked to fast for at least 8 h before anesthesia. A single anesthetist, who was not aware of the group division, administered the anesthetic (lidocaine 1 mg/kg intravenous (i.v.), midazolam 0.05 mg/kg i.v., propofol 2–3 mg/kg i.v., and sufentanil 0.2–0.4 µg/kg i.v.) and endotracheal intubation to all patients, followed by vecuronium 0.1 mg/kg i.v. To avoid postsurgical nausea and vomiting (PONV), both groups received granisetron 3 mg i.v. following induction. To maintain general anesthesia and a bispectral (BIS) index of 40–60, all patients were given a steady intravenous injection of propofol with the rate of 3–5 mg/kg/h, vecuronium, and remifentanil at a constant rate of 0.3 μg/kg/min. All patients received standard monitoring protocols, consisting of a BIS index, end-tidal CO2, pulse oximetry, non-invasive blood pressure, and electrocardiography. Ringer’s lactate solution was obtained through the peripheral intravenous line predicated on presurgical deficiencies, surgical technique, and anticipated intraoperative hemorrhage. Volume-controlled mechanical ventilation was used to keep the patient’s tidal volume and respiratory rate within acceptable normocapnia limits (35–45 mmHg end-tidal CO2). As a last resort for postoperative pain relief, patients were given 50 mg of flurbiprofen i.v. Atropine 0–2.5 mg and neostigmine 0–5 mg were used to counteract remaining muscle relaxant impacts preceding tracheal extubation.
Outcome Measures
In the 30 min after surgery, the primary outcome measure was the mechanical pain threshold surrounding the skin incision.
A QST was conducted by a professional investigator blinded to the group division, utilizing an EvF device (IITC Life Science, Woodland Hills, CA, USA). The presence of QST was identified the day before surgery and confirmed at 30 min and 6, 24, and 48 h after surgery. The EvF device was composed of an 800 g probe with a stiff tip, the diameter of which was 0.8 mm. In a regulated and right-angle motion, the probe was pushed against the surface of the skin with increasing force at a controlled pace. When the subject felt pain, the data was recorded and presented in grams. Afterward, the probe was removed (see Figure 1). Mechanical pain tolerance was then determined as the mean of six findings obtained 2 cm vertically above and below the center and bilateral borders of the skin incision. Subsequently, the average of three measures taken at 3, 6, and 9 cm from the midpoint of the antecubital crease on the non-dominant inner forearm was calculated. The time interval for each measurement was 30 seconds. Postoperative hyperalgesia was determined and characterized as a significant reduction in the postoperative mechanical level of pain when compared with the preoperative value.
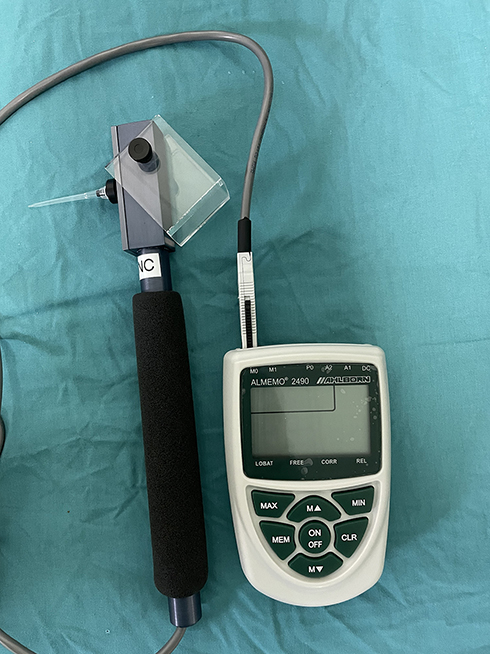 |
Figure 1 Electronic von Frey (EvF) device. |
Secondary Outcome Measures
At 30 min after surgery, the forearm’s mechanical pain threshold was measured as the secondary outcome. The mechanical pain thresholds in the forearm and surrounding the skin incision were also measured at 6, 24, and 48 h after surgery, and the occurrence of postoperative hyperalgesia in the forearm and surrounding the skin incision, postoperative pain scores (numerical rating scale, NRS), and the need for rescue analgesics were recorded.
Demographic data and baseline data, such as body mass index (BMI), gender, age, and perioperative indexes (including surgical type, surgery time, the dosage of anesthetic drug (propofol and remifentanil), extubation time, and side effects) were documented. All outcome measures were evaluated by an independent research nurse who was blinded to the group division and not engaged in the care of the patients.
Statistical Analysis
The data were analyzed using the Statistical Package for Social Sciences for Windows version 22.0. For the purpose of comparing the explanatory data across the two groups, Bonferroni-corrected independent sample t-tests were carried out. To contrast categorical data, specified as frequency (f) and numbers (%), Fisher’s exact test or a χ2 test were performed. P < 0.05 was considered statistically significant.
Using the data of our pilot study, the mean ± SD mechanical pain threshold was 99.5 ±13.8g around the skin incision 30 minutes after surgery in patients treated with sham EA, the result in group EA was 89.3 ±14.2g. We calculated the sample size needed is 29 per group to detect a significant difference with 90% power (α=0.05). Considering a 35% potential drop out rate, 40 subjects per group, or a total of 80 patients, should be reasonable for our study.
Results
Patient Features, Surgery, and Anesthesia
All 83 eligible subjects were included in the study, with 80 being hospitalized and randomly assigned to one of the two groups. One patient dropped out of the EA group after declining to undergo the procedure. The records of the remaining 79 patients were analyzed. Figure 2 depicts the study’s flow diagram.
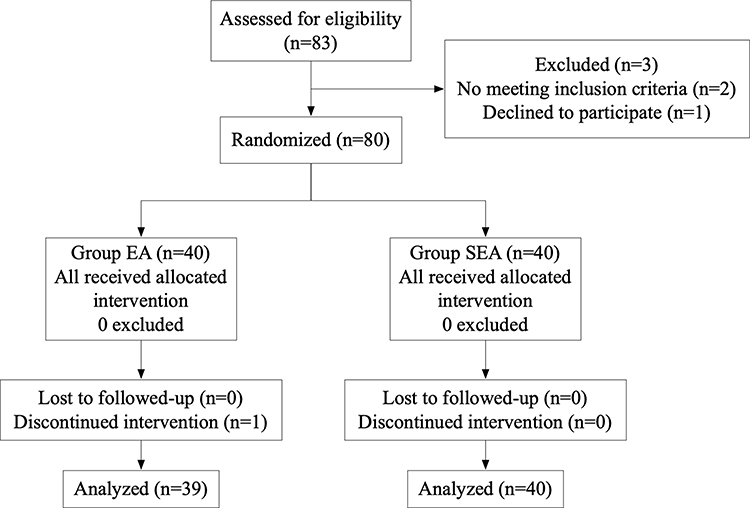 |
Figure 2 Consolidated standards of reporting trials (CONSORT) diagram of patient recruitment. Abbreviations: EA, electroacupuncture; SEA, sham electroacupuncture. |
Table 1 summarizes the perioperative features of the patients, including age, gender, BMI, type of surgery, and anesthesia-related data. Baseline features and surgical and anesthetic variables did not differ significantly between the two groups.
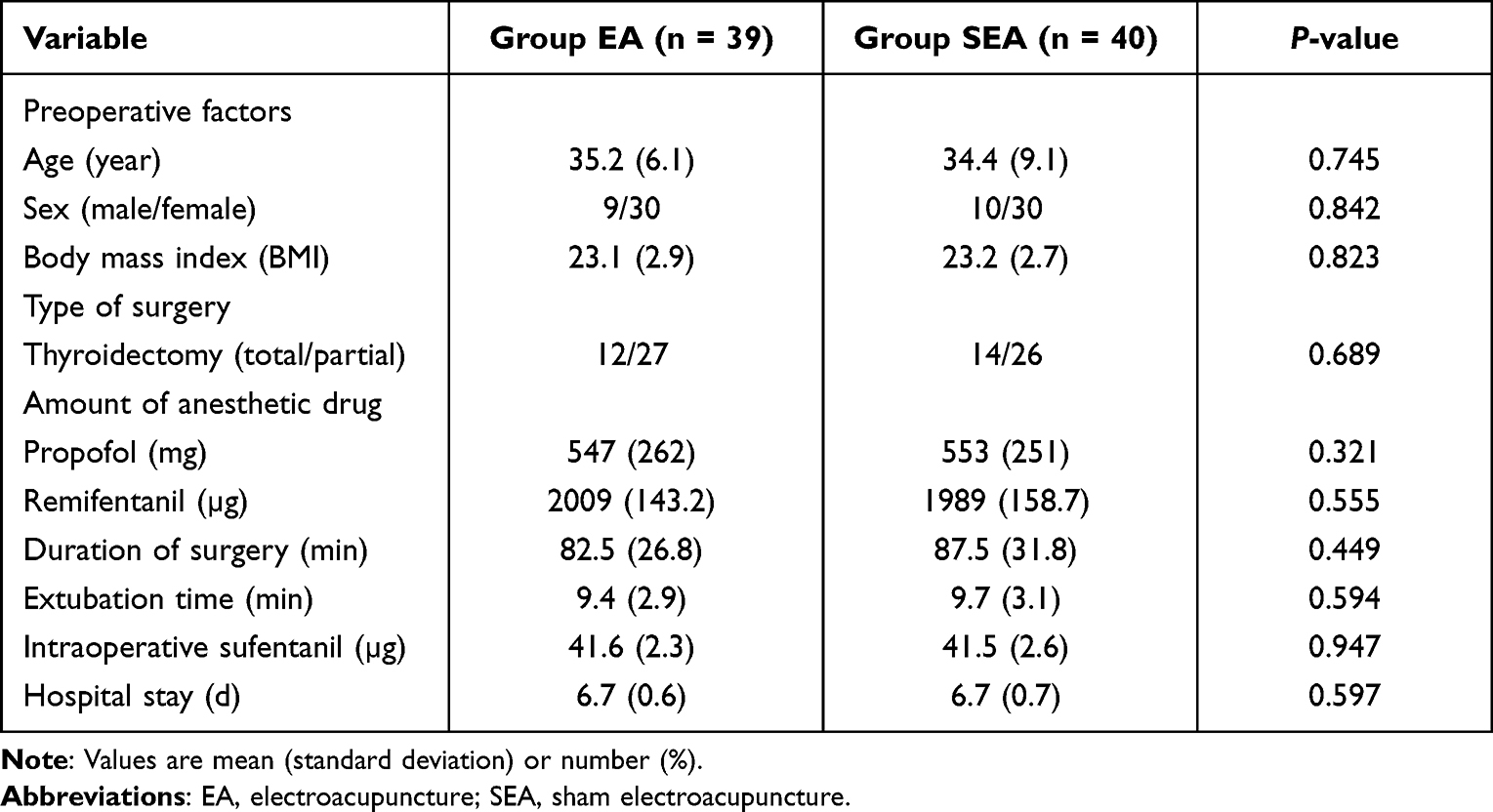 |
Table 1 Patient Age and Perioperative Variables (Mean [SD]) or n (%) |
Mechanical Pain Thresholds
Prior to surgery, there was no significant difference between the two groups in preoperative mechanical pain threshold. At 30 min and 6 h after surgery, the mechanical pain thresholds of patients in the EA group were higher than those of patients in the SEA group. No difference between the two groups was found at 24 and 48 h after surgery (see Table 2 and Figure 3).
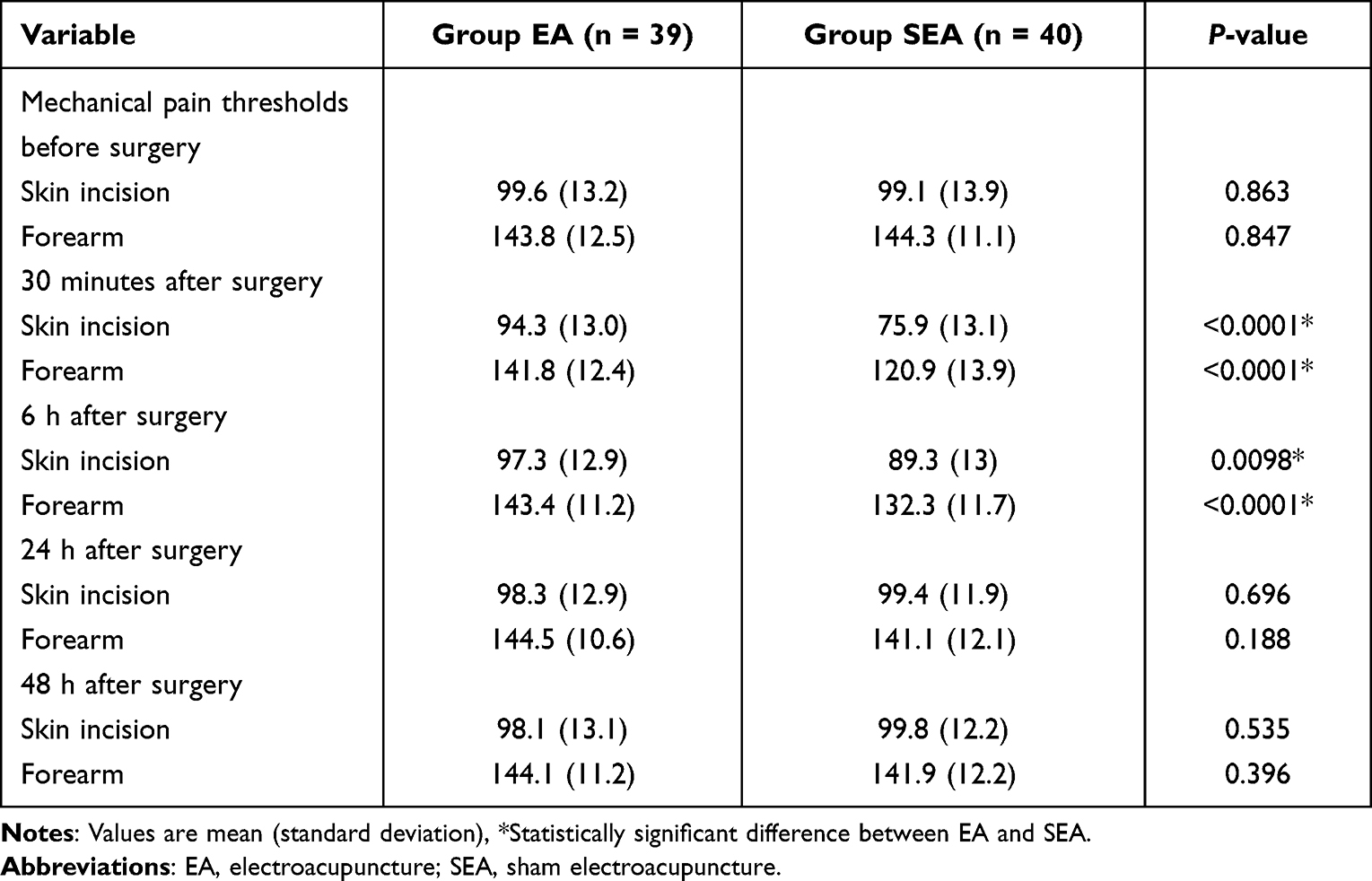 |
Table 2 Mechanical Pain Thresholds Around the Skin Incision and on the Forearm Before the Surgery, at 30 min, 6 h, 24 h, and 48 h After the Surgery (g, Mean [SD]) |
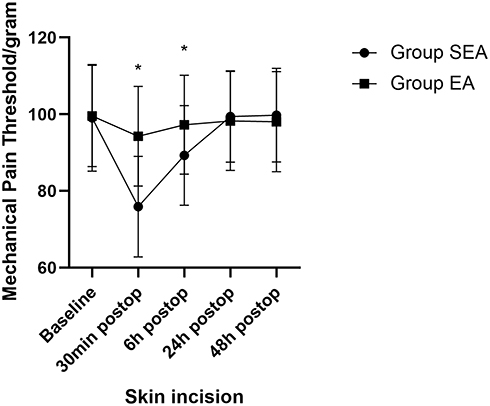 |
Figure 3 Mechanical pain thresholds around the skin incision. Mechanical pain thresholds are presented as mean and standard deviation (SD) and analyzed using Bonferroni-corrected independent sample t-tests. *Statistically significant difference between EA and SEA. Abbreviations: EA, electroacupuncture; SEA, sham electroacupuncture. |
There was no significant difference between the two groups in the baseline data of the forearm’s mechanical pain threshold. However, the EA group had greater mechanical pain tolerance at 30 min and 6 h after surgery than the SEA group. No differences between the two groups were reported in mechanical pain thresholds at 24 and 48 h after surgery (see Table 2 and Figure 4).
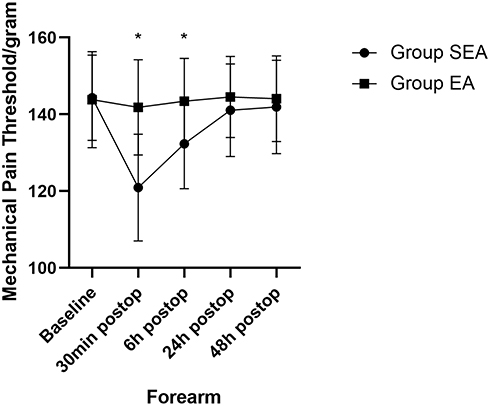 |
Figure 4 Mechanical pain thresholds on the forearm. Mechanical pain thresholds are presented as mean and standard deviation (SD) and analyzed using Bonferroni-corrected independent sample t-tests. *Statistically significant difference between EA and SEA. Abbreviations: EA, electroacupuncture; SEA, sham electroacupuncture. |
Hyperalgesia Incidence and Pain Intensity
A lower occurrence rate of hyperalgesia was seen in the forearm and surrounding the skin incision 30 min after surgery in the EA group than in the SEA group. At 6 h after surgery, the incidence of hyperalgesia surrounding the skin incision was lower in the EA group than in the SEA group, but there was no significant difference between the two groups in the incidence of hyperalgesia in the forearm. Furthermore, no statistically significant differences were found between the two groups 24 and 48 h after surgery (see Table 3). Although the numerical rating scale for both groups was low, EA treatment reduced it at 30 min and 6 h after surgery (see Table 3). Moreover, no differences were found between the two groups in terms of the proportion of patients who needed rescue analgesics (see Table 3).
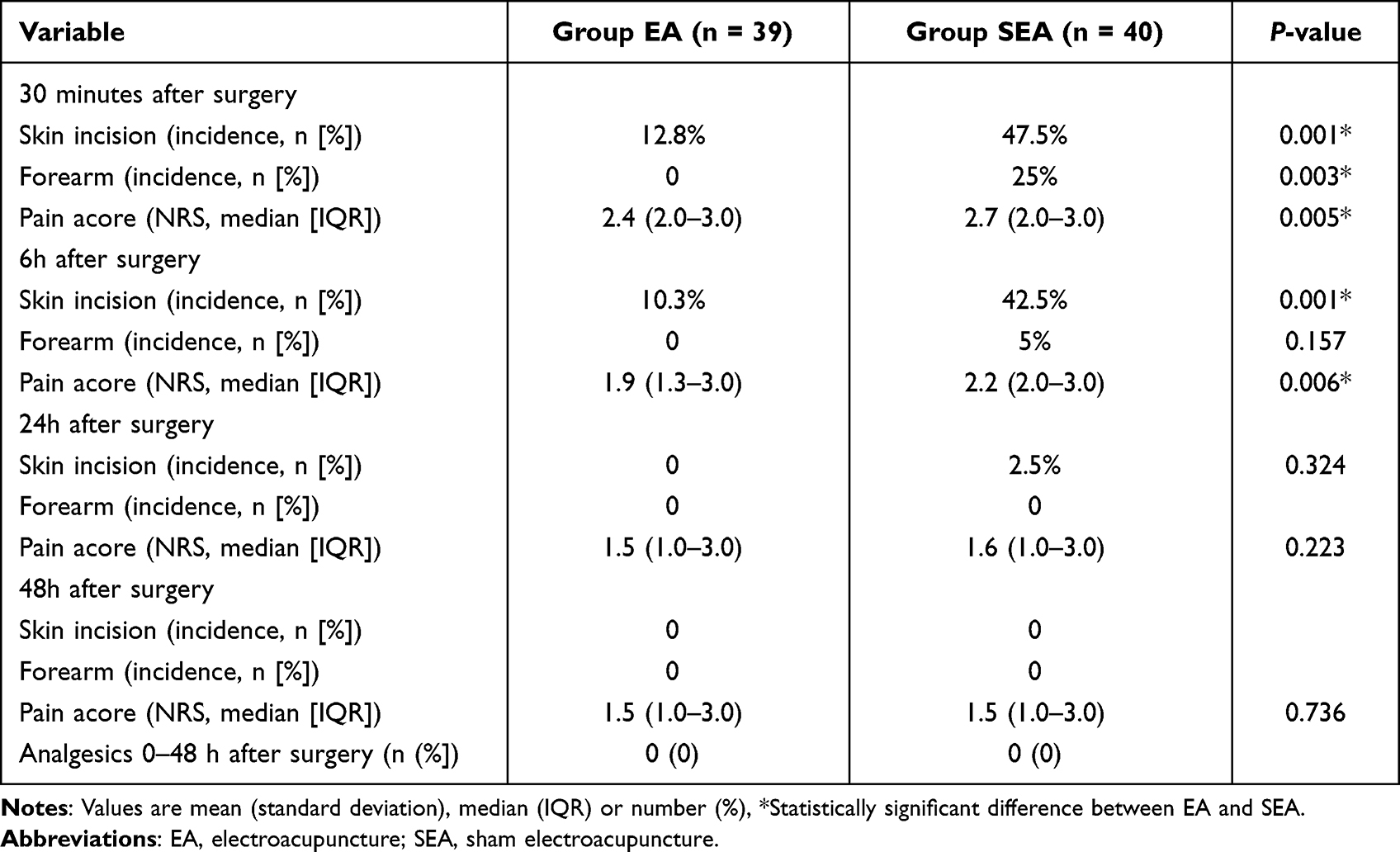 |
Table 3 Incidence of Hyperalgesia Around the Skin Incision and on the Forearm at 30 Min, 6 h, 24 h, and 48 h After the Surgery, and Pain Score Around the Skin Incision (Mean [SD]) |
Postoperative Side Effects
Two patients (one in the EA group and one in the SEA group) complained of pain at the needle sites. As the complaints were mild, however, medical attention was not required. The EA and SEA treatments were well tolerated by all patients.
Discussion
The findings of this clinical trial suggest that patients undergoing thyroidectomy can exhibit postoperative hyperalgesia after the administration of 0.3 μg/kg/min intraoperative remifentanil. EA treatment delivered one day prior to surgery not only increases mechanical pain thresholds but also decreases the incidence of hyperalgesia in the forearm and surrounding the skin incision, lowering the patient’s pain score.
The present study found that mechanical pain thresholds decreased in the forearm and surrounding the skin incision at 30 min and 6 h after surgery in the SEA group, suggesting the occurrence of postoperative hyperalgesia. This finding is similar to those reported previously.18 As previously reported, RPH may be linked to central sensitization, which activates and upregulates the spinal NMDA receptors.5,19 The synergistic effects of intraoperative opioids and surgery could contribute to postoperative hyperalgesia.20 Because of the low relativity between subjective pain intensity and objective pain thresholds in a QST,20 an EvF device can assess a QST rapidly with good reproducibility.12 The present study found that the results obtained using an EvF device and by subjective pain intensity were identical. In addition, compared with subjective pain intensity, an EvF device is more sensitive and objective for when performing a QST.
The present study also showed that EA treatment increased mechanical pain thresholds in the forearm and surrounding the skin incision at 30 min and 6 h after surgery. Moreover, EA was found to alleviate RPH in patients undergoing thyroidectomy, further confirming its analgesic effect. The mechanisms of EA’s analgesic effects are complicated, but evidence suggests that it relieves pain by activating bioactive chemicals, triggering endogenous pathways and directly inhibiting the opioid-sensitive spinal cord interneurons.21,22
The present study selected the bilateral Zusanli (ST36) and Neiguan (PC6) acupoints for EA treatment. According to traditional Chinese medicine, PC6 is located along the hand-Jueyin in the pericardium meridian. Stimulation of PC6 is known to alleviate the symptoms of angina, lessen the incidence of PONV, and mitigate remifentanil-induced hyperalgesia.15,22,23 Traditional Chinese medicine states that ST36 belongs to the stomach meridian of the foot-Yangming, and its stimulation is known to adjust qi and blood. In a mouse cancer pain model, EA treatment at ST36 induced analgesic activity.24 A previous study also demonstrated that combined stimulation of PC6 and ST36 produced better anti-emesis and analgesic effects.15,25 The timing of acupuncture intervention has remained controversial, however. Although some studies have reported the delivery of acupuncture after surgery, the majority have reported its delivery before surgery.15,26–28 Coura et al16 reported that acupuncture produced better pain reduction when delivered one day prior to surgery compared to 30 min before surgery. Our previous study suggested that it was safe and effective to deliver EA treatment within 24h prior to surgery in patients undergoing gynecologic laparoscopic surgery.15 In the present study, EA was delivered one day before surgery, with the results indicating that preoperative EA is effective in mitigating RPH.
The present study had some limitations. First, it exclusively investigated pressure-induced pain levels, even though a QST can be utilized to assess the severity of a variety of nociceptive stimuli, such as touch pressure, vibration, and heat. Second, blood samples were not collected to study changes in EA-induced endogenous opioid peptides, so the underlying mechanism remains unclear. Last, the research was conducted at a single center with a limited sample of participants, so it is uncertain whether the findings can be extended to other centers. Further studies are required to address these issues.
Conclusion
The present study demonstrated that EA delivered at the Zusanli (ST36) and Neiguan (PC6) acupoints 24 h before surgery can effectively alleviate RPH in patients undergoing thyroidectomy. However, future research is required to explore the underlying mechanism.
Abbreviations
EA, electroacupuncture; RPH, remifentanil-induced post-infusion hyperalgesia; EvF, electronic von Frey; ST36, Zusanli; PC6, Neiguan; QST, Quantitative sensory testing; VFM, Von Frey monofilaments; ASA, American Society of Anesthesiologists; I.V, intravenous; PONV, postsurgical nausea and vomiting; BMI, body mass index.
Clinical Trial Registration Number
Approval of the research was granted by the Human Research Ethics Committee of the Affiliated Hospital of Nanjing University of Traditional Chinese Medicine, Nanjing, China (2021NL-198-02). It was registered at the Chinese Clinical Trial Registry (ChiCTR2100050235) before patient enrollment.
Data Sharing Statement
We would like to sharing all the individual participant data. The data in this study available from the corresponding author on reasonable request in two years after this article published online.
Ethics Approval and Consent to Participate
Approval of the research was granted by the Human Research Ethics Committee of the Affiliated Hospital of Nanjing University of Traditional Chinese Medicine, Nanjing, China (2021NL-198-02). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
Funding
This study was funded by a research grant from the Postgraduate Research & Practice Innovation Program of Jiangsu Province (grant numbers SJCX21_0783), China.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Komatsu R, Turan AM, Orhan-Sungur M, McGuire J, Radke OC, Apfel CC. Remifentanil for general anaesthesia: a systematic review. Anaesthesia. 2007;62:1266–1280. doi:10.1111/j.1365-2044.2007.05221.x
2. Angst MS, Koppert W, Pahl I, Clark DJ, Schmelz M. Short-term infusion of the mu-opioid agonist remifentanil in humans causes hyperalgesia during withdrawal. Pain. 2003;106:49–57. doi:10.1016/S0304-3959(03)00276-8
3. Petersen KL, Jones B, Segredo V, Dahl JB, Rowbotham MC. Effect of remifentanil on pain and secondary hyperalgesia associated with the heat–capsaicin sensitization model in healthy volunteers. Anesthesiology. 2001;94:15–20. doi:10.1097/00000542-200101000-00008
4. Zhang L, Shu R, Zhao Q, Li Y, Yu Y, Wang G. Preoperative butorphanol and flurbiprofen axetil therapy attenuates remifentanil-induced hyperalgesia after laparoscopic gynecological surgery: a randomized double-blind controlled trial. Br J Anaesth. 2016;117:504–511. doi:10.1093/bja/aew248
5. Zhao M, Joo DT. Enhancement of spinal N-methyl-D-aspartate receptor function by remifentanil action at delta-opioid receptors as a mechanism for acute opioid-induced hyperalgesia or tolerance. Anesthesiology. 2008;109:308–317. doi:10.1097/ALN.0b013e31817f4c5d
6. Mercieri M, Palmisani S, De Blasi RA, et al. Low-dose buprenorphine infusion to prevent postoperative hyperalgesia in patients undergoing major lung surgery and remifentanil infusion: a double-blind, randomized, active-controlled trial. Br J Anaesth. 2017;119:792–802. doi:10.1093/bja/aex174
7. Chu LF, Angst MS, Clark D. Opioid-induced hyperalgesia in humans: molecular mechanisms and clinical considerations. Clin J Pain. 2008;24:479–496. doi:10.1097/AJP.0b013e31816b2f43
8. Lee C, Kim YD, Kim JN. Antihyperalgesic effects of dexmedetomidine on high-dose remifentanil-induced hyperalgesia. Korean J Anesthesiol. 2013;64:301–307. doi:10.4097/kjae.2013.64.4.301
9. Koo CH, Yoon S, Kim BR, et al. Intraoperative naloxone reduces remifentanil-induced postoperative hyperalgesia but not pain: a randomized controlled trial. Br J Anaesth. 2017;119:1161–1168. doi:10.1093/bja/aex253
10. Chen Y, Yao Y, Wu Y, Dai D, Zhao Q, Qiu L. Transcutaneous electric acupoint stimulation alleviates remifentanil-induced hyperalgesia in patients undergoing thyroidectomy: a randomized controlled trial. Int J Clin Exp Med. 2015;8:5781–5787.
11. Samuelsen PJ, Nielsen CS, Wilsgaard T, Stubhaug A, Svendsen K, Eggen AE. Pain sensitivity and analgesic use among 10,486 adults: the tromsø study. BMC Pharmacol T Oxicol. 2017;18:45. doi:10.1186/s40360-017-0149-2
12. Tena B, Escobar B, Arguis MJ, Cantero C, Rios J, Gomar C. Reproducibility of electronic von Frey and von Frey monofilaments testing. Clin J Pain. 2012;28:318–323. doi:10.1097/AJP.0b013e31822f0092
13. Shi RY, Fu TF, Cai YQ, et al. Electroacupuncture intervention relieves pain possibly by promoting MOR endocytosis in locus coeruleus in bone cancer pain rats with morphine tolerance. Zhen Ci Yan Jiu. 2019;44:161–169. Chinese. doi:10.13702/j.1000-0607.180635
14. Jiang B, Zhong XM, Fang JF, et al. Electroacupuncture attenuates morphine tolerance in rats with bone cancer pain by inhibiting PI3K/Akt/JNK1/2 signaling pathway in the spinal dorsal horn. Integr Cancer Ther. 2021;20:1534735421995237. doi:10.1177/1534735421995237
15. Li S, Zheng M, Wu WZ, Guo J, Ji F, Zheng Z. Effects of electroacupuncture administered 24 hours prior to surgery on postoperative nausea and vomiting and pain in patients undergoing gynecologic laparoscopic surgery: a feasibility study. Explore. 2017;13:313–318. doi:10.1016/j.explore.2017.06.002
16. Coura LE, Manoel CH, Poffo R, Bedin A, Westphal GA. Randomised, controlled study of preoperative electroacupuncture for postoperative pain control after cardiac surgery. Acupunc Med. 2011;29:16–20. doi:10.1136/aim.2010.003251
17. Zheng Z, Bai LH, O’Loughlan M, Li CG, Xue CC. Does electroacupuncture have different effects on peripheral and central sensitization in humans: a randomized controlled study. Front Integr Neurosci. 2019;13:61. doi:10.3389/fnint.2019.00061
18. Wu ZJ, Yu JJ, Lin QH, et al. Effects of an intraoperative intravenous bolus dose of dexmedetomidine on remifentanil-induced postinfusion hyperalgesia in patients undergoing thyroidectomy: a double-blind randomized controlled trial. Anesth Analg. 2021;132:320–328. doi:10.1213/ANE.0000000000005003
19. Guntz E, Dumont H, Roussel C, et al. Effects of remifentanil on N-methyl-D-aspartate receptor: an electrophysiologic study in rat spinal cord. Anesthesiology. 2005;102:1235–1241. doi:10.1097/00000542-200506000-00025
20. Song JW, Lee YW, Yoon KB, Park SJ, Shim YH. Magnesium sulfate prevents remifentanil-induced postoperative hyperalgesia in patients undergoing thyroidectomy. Anesth Analg. 2011;113:390–397. doi:10.1213/ANE.0b013e31821d72bc
21. Liu YJ, Du JY, Fang JF, et al. Electroacupuncture inhibits the interaction between peripheral TRPV1 and P2X3 in rats with different pathological pain. Physiol Res. 2021;70:635–647. doi:10.33549/physiolres.934649
22. Zhang RX, Lao LX, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120:482–503. doi:10.1097/ALN.0000000000000101
23. Zhang HX, Liu LG, Huang GH, et al. Protective effect of electroacupuncture at the Neiguan point in a rabbit model of myocardial ischemia-reperfusion injury. Can J Cardiol. 2009;25:359–363. doi:10.1016/S0828-282X(09)70095-9
24. Lee HJ, Lee JH, Lee EO, et al. Substance P and beta endorphin mediate electroacupuncture induced analgesic activity in mouse cancer pain model. Acupunct Electrother Res. 2009;34:27–40. doi:10.3727/036012909803861095
25. Lu DX, Lu DR, Liu YY, et al. TCM basic theory and contemporary study on cancerous pain treated with acupuncture at Zusanli (ST36) and Neiguan (PC6). World J Integr Tradit Western Med. 2017;12:593–597. Chinese.
26. Yang XY, Xiao J, Chen YH, et al. Dexamethasone alone vs in combination with transcutaneous electrical acupoint stimulation or tropisetron for prevention of postoperative nausea and vomiting in gynaecological patients undergoing laparoscopic surgery. Br J Anaesth. 2015;115:883–889. doi:10.1093/bja/aev352
27. Li SS, Zhang Q, Yin X, et al. Electroacupuncture for postoperative pain after nasal endoscopic surgery: study protocol for a pilot randomized controlled trial. Trials. 2020;21:163. doi:10.1186/s13063-020-4064-2
28. Park S, Gu JH, Jang HK, Oh MS, Lee EJ, Jung IC. Electroacuncture for post-thoracotomy pain: protocol for a systematic review and meta-analysis. Medicine. 2020;99:e19312. doi:10.1097/MD.0000000000019312
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.