Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Effects of Pilates Exercises on Core Stability After Recovery from COVID-19: A Randomized Controlled Trial
Authors Amin WM ![]() , Ali OI
, Ali OI ![]() , Malik S
, Malik S ![]() , Draj SAI
, Draj SAI ![]() , Masoud FAM
, Masoud FAM ![]() , Sohel AMI
, Sohel AMI ![]() , Al Amer AM
, Al Amer AM ![]() , Khurayzi RHH, Ahmed MM
, Khurayzi RHH, Ahmed MM ![]()
Received 3 December 2023
Accepted for publication 8 February 2024
Published 20 February 2024 Volume 2024:17 Pages 753—763
DOI https://doi.org/10.2147/JMDH.S453050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wafaa Mahmoud Amin,1,2,* Olfat Ibrahim Ali,3,4,* Shazia Malik,1,* Suhair Asous I Draj,1,* Fatima Ahmed M Masoud,1,* Amal Mohammed I Sohel,1,* Asayil Mari Al Amer,1,* Rasmiah Hassan H Khurayzi,1,* Mohamed M Ahmed1,5,*
1Department of Physical Therapy, College of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 2Basic Science for Physical Therapy Department, Faculty of Physical Therapy, Cairo University, Giza, Egypt; 3Physical Therapy Program, Batterjee Medical College, Jeddah, 21442, Saudi Arabia; 4Basic Science Department, Faculty of Physical Therapy, Cairo University, Giza, Egypt; 5Basic Science Department, Faculty of Physical Therapy, Beni-Suef University, Beni-Suef, Egypt
*These authors contributed equally to this work
Correspondence: Wafaa Mahmoud Amin, Department of Physical Therapy, College of Applied Medical Sciences, Jazan University, P.O. Box. 114, Jazan, Gizan, 45142, Saudi Arabia, Email [email protected]
Purpose: The primary objective was to investigate the effects of Pilates exercises on CS, and the secondary objective was to assess static trunk balance after recovery from COVID-19.
Patients and Methods: 145 recovered COVID-19 university students between the ages of 19 and 25 participated in this single-blinded, randomized controlled trial study. The participants were divided into a Pilates group and a control group, each of which received a home exercise program. Core muscle endurance was measured using the five basic endurance tests and static balance using the Prokin system with open eyes (OE) and closed eyes (CE) at baseline and after three months of treatment.
Results: All measured parameters showed improvement within the groups after treatment. Group comparison revealed a significant increase in the Pilates group in all core endurance tests (P< 0.001). The Prokin system results showed improvement in the Pilates group after treatment, while perimeter with OE, CE, and ellipse area with EC decreased (P< 0.001), but there was no significant difference in ellipse with OE between the groups.
Conclusion: Pilates exercises positively improved core muscle endurance and trunk balance in people infected with COVID-19, which will be reflected in their quality of movement patterns and quality of life.
Keywords: pilates, core endurance, postural balance, COVID-19
Introduction
Despite the respiratory nature of COVID-19, it affects other systems: cardiovascular, gastrointestinal, neurological, and musculoskeletal.1,2 Post-COVID-19, or “long COVID”, refers to the enduring symptoms of a COVID-19 infection, impacting various organs and bodily systems, including skeletal muscle.3 COVID-19 is a health problem that limits participation in physical activity because it creates many barriers to it, including physiological, psychological, behavioral, and reduced physical activity that adversely affect quality of life (QoL) and the musculoskeletal system. The practice of physical activity is essential for promoting overall wellness and maintaining a healthy lifestyle.4 COVID-19 survivors without preexisting musculoskeletal conditions experience skeletal muscle weakness, diminished performance, decreased physical fitness, respiratory impairment, psychiatric conditions such as post-traumatic stress disorder, reduced QoL, abnormal movement patterns, and musculoskeletal complications.2,3
Muscle atrophy after COVID-19 is one of the musculoskeletal system affections, and it was hypothesized that this atrophy might be attributed to inflammation, angiotensin converting enzyme 2, muscle catabolism, hypoxia, and medication received during COVID-19 treatment side effects.1 Studies have shown that individuals experience reduced muscle function even 12 months after discharge from the hospital due to prolonged COVID-19. The collective data suggests that prolonged COVID-19 adversely affects muscle mass, function, and QoL.5 Individuals with pulmonary disease and COVID-19 experience core muscle weakness and decreased static and dynamic balance, leading to fatigue and falls.6 Accordingly, it affects core stability.
Core stability (CS) is the lumbopelvic-hip complex’s core box and has the ability to maintain vertebral column balance and stability within normal motion, minimizing external displacement, and preserving core structural integrity.7 The core box is a three-dimensional structure with the transversus abdominis muscle in front, the paraspinal and gluteal muscles in back, the diaphragm in the top, and pelvic floor muscles in the bottom.8,9 A factor that complicates the contribution of these muscles to trunk control is their essential roles in respiration and continence. In chronic respiratory disease and during induced hypercapnia, postural activation of these muscles is impaired.10
A recent systematic review found that there is not much research on non-drug treatments for post-viral syndromes and COVID-19. The reviewers found randomized clinical trials that were done in 2021 that looked at music therapy, telerehabilitation, resistance therapy, and neuromodulation, but they did not look at all the symptoms experienced in these cases, focusing only on dyspnea, arthralgia, general pain, and quality of life.11 In this study, we addressed the effect of COVID-19 on core stability and introduced treatment exercises. Randomized control trials (RCTs) show Pilates offers significant benefits to enhance core muscle strength and alleviate discomfort compared to a lack of exercise.12 Pilates exercises have been shown to improve core muscle strength and have a positive effect on pain reduction. Moreover, it enhances the vital capacity and tidal volume of the lungs.13
Most physical therapy interventions during and after COVID-19 focused on respiratory and general fitness rehabilitation in severely infected elderly individuals rather than balance and endurance training, as reported in the following studies: Mayer et al demonstrated an 8-week program of aerobic exercise, strengthening exercises, diaphragmatic breathing techniques, and mindfulness training for the post-COVID-19 case and assessed the patient’s cognitive and emotional state.14 Cevei et al conducted robotic gait training, occupational therapy, and messages on six elderly individuals post-COVID-19, evaluating their activity and participation by the Barthel index and functional independence measure.15 Ponce-Campos et al looked at an indoor program of aerobic exercises for 4 weeks for people who had COVID.16 Mashhadi et al found that 8 weeks of respiratory exercises and core stabilization tele-exercise improved quality of life and functional capacity.17 A 10-week program using instrumental Pilates exercises with slow and controlled breathing exercises significantly improved heart rate variability (HRV) and respiratory parameters.13 So, the most important feature that distinguishes this study from other research is that it aimed to treat mild-to-moderately recovered infected cases in younger adults using Pilates exercises to improve core muscle endurance and balance.
Pilates is a comprehensive exercise technique that integrates mind and body, strengthens core muscles, and focuses on the posterior pelvic tilt, which is the conventional method of Pilates.18 It was developed by Joseph Pilates into contemporary Pilates and has evolved with modern scientific advancements to render it more suitable, effective, and secure for the involved individuals.19 There are six fundamental principles for Pilates training: centering, focus, control, precision, breath, and flow.20 They maintain neutral spinal alignment and engage deep abdominal and pelvic floor muscles through co-contraction.21 It was found that core muscle endurance, depression, and quality of life improved after pilates in online and face-to-face settings in healthy individuals during the COVID-19 pandemic.22
The scientific literature has focused primarily on severe COVID-19 cases, with limited understanding of patients with mild to moderate infections who have persistent musculoskeletal symptoms.23 Similarly, they have focused on physical therapy programs to improve quality of life, respiratory and pulmonary function, and functional capacity.24,25 There is no research and exercise program evaluating core stability and the effect of Pilates on core endurance and postural stability after COVID-19. Therefore, the purpose of this study was to evaluate the effect of Pilates exercises on core endurance and static balance of the trunk; accordingly, we hypothesized that there would be no effect of Pilates exercises on core endurance and static balance in participants recovering from COVID-19.
Materials and Methods
Study Design
This is a single randomized controlled trial conducted from December 26, 2021, to February 23, 2023, and it met the reporting requirements for randomized controlled trials.26 An independent assessor accompanied the randomization process. Computer-generated randomization was used to assign participants to two groups: the study group (Pilates) (41 females + 33 males) and the control group (43 females + 28 males). Allocation was performed using a sealed, opaque envelope.
Participants
A study was conducted on 145 COVID-19-infected students (both sexes) aged 19 to 26 from Jazan University. Participants were selected based on the following criteria: mild to moderate COVID-19 symptoms, a body mass index <25 kg/m2, and non-athletic. Participants were recruited through advertisements in social media groups and student bulletin boards, and we verified their medical status through the records of COVID-19 within the unified platform of the Ministry of Health (Sehhaty) in Saudi Arabia.
Any subject was excluded if they had severe COVID-19, chest pain or symptoms of heart failure, or cardiopulmonary, visual, vestibular, or central nervous system disorders;27 previous back or abdominal surgery; evidence of systemic or musculoskeletal disease within the previous six months;28 pregnancy and lower limb asymmetries; enrollment in another treatment program. Participants were informed of the potential risks and benefits of the study and signed a written informed consent form before the study began. The study was conducted according to the tenets of the Declaration of Helsinki, and the clinical trial registration number was NCT04871672. The ethical approval reference number (REC-43/03/036) was obtained from the Standing Committee for Scientific Research at Jazan University. The sample size was determined using G-Power software (Universities, Düsseldorf, Germany) with a power of 80%, a p-value of 0.05, and an effect size of 0.5. A sample size of 126 subjects was included in the study, and to compensate for the dropout rate, the sample was increased to 75 subjects in each group (Figure 1).
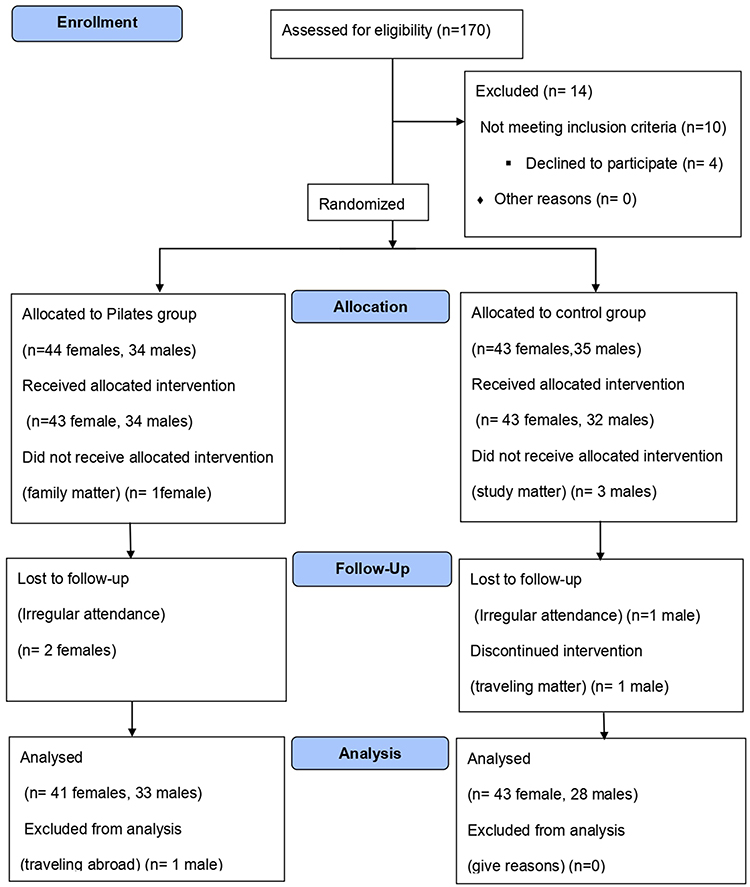 |
Figure 1 Consort flowchart. |
Outcome Measures
Primary Outcome Measures
Core Endurance Test
Five core endurance tests were performed, in which the subject maintained a static position for as long as possible. The endurance tests are the abdominal fatigue test, the Sorensen back extension test, the prone plank test, and the right and left side plank tests.29 The investigator used a handheld digital stopwatch to time the trials in seconds, with the subjects receiving verbal instructions and visual examples.28 Participants were encouraged to give their best effort, and the order of the tests was randomized to eliminate order effects. In addition, an interval of approximately 10 seconds was maintained between consecutive tests to reduce the influence of fatigue on performance.30
Abdominal fatigue test (trunk flexor test): was performed with a 60° angle of flexion, a 90° knee and hip flexion, arms crossed over the chest, and the position was maintained as long as possible. The Sorensen test (trunk extensor test) was performed in a semi-prone position with the pelvis, hips, and knees fixed on a treatment table, the arms crossed over the chest, and a horizontal body position maintained for as long as possible. Side plank test: The participant assumed a sideways position on a mat, supporting the body weight with the lower elbows and feet while lifting the hips. The test was stopped when the side-lying position was lost or the hips returned to the mat.31 The Prone Plank Test: Participants assume a prone position on an elbow-supported mat, lifting their hips and torso on their forearms and toes while maintaining a straight position with their elbows under their shoulders.31
Secondary Outcome Measures
Static Balance Measurement
It is valid and accurate to use the Prokin System (Prokin-PK 212–252-TechnoBody-Italy) to check both static and dynamic balance by moving the force platform from the center of pressure (COP) movements to measure postural sway.32 A 5-minute warm-up of walking at a moderate speed (2.5–3 miles per hour) on the treadmill was performed prior to measurement. Participants using a Prokin device were instructed to look straight ahead at a screen with their arms at their sides and to focus on a stationary target. They performed two standing trials with eyes open and closed, each lasting 30 seconds. Four outcome variables were calculated in two conditions: perimeter (mm) and ellipse area (mm2) with eyes open (OE) and eyes closed (CE). The test was repeated twice, and the mean value was recorded.33
Perimeter (mm): measures chaotic lines during body sway, with good postural balance observed with shorter lines.34 Ellipse area (mm2): represents the area of body sway, elliptical in shape, covering at least 90% or 95% of the chaotic sway lines, with smaller areas resulting in better balance performance.35 Measurements were taken before and after three months of treatment.
Both outcomes were collected in the laboratories of the Physical Therapy Department, College of Applied Medical Sciences, Jizan University. An independent assessor collected data for the core endurance testing and static balance data. Both outcomes were measured in two separate, consecutive sessions to avoid participant fatigue.
Intervention
- The home exercise program included daily 15-minute breathing exercises, self-stretching activities targeting various muscles (pectoralis major, shoulder extensors, back muscles, hip flexors, hip adductors, and hamstring muscles), and 15 minutes of daily walking to improve overall physical health.
- Pilates exercise program: The Pilates exercise program lasted for three months and consisted of three weekly sessions. Each session lasted one hour. Each session began with 10 minutes of simple stretching movements to warm up, followed by 40 minutes of the main exercise routine, followed by 10 minutes of cool-down stretching. Participants were trained by a qualified practitioner, given step-by-step instructions, and taught the proper breathing techniques and spinal neutrality prior to the intervention. The program included five basic intermediate Pilates exercises: the mat hundred, roll-up, one-leg circle, rolling like a ball, and spine stretch. These exercises are suggested by Thompson et al and focus on voluntary activation of the deep abdominal muscles by pulling the navel toward the spine and combining the movement with breathing.36 CS was assessed by endurance testing after 12 sessions.37,38
The following are the descriptions of the Pilates exercises:
Mat-Hundred: The exercise involved lying on a mat with legs bent and feet flat on the floor. The participant inhales to engage the abdominal muscles, then lifts the head and shoulders off the mat with the eyes between the legs. Arms pump vigorously, lifting up and down no higher than the hips. The exercise was repeated 10 times with 5 inhales and 5 exhales for a total of 100.
Mat-Roll-Up: The participant positioned the legs parallel to the ground, flexed the legs, and extended the arms above the head. Focus on the gaze and position of the arms for a thorough examination. The action includes taking a deep breath, then rolling the body upward. Maintain the C-curve by exhaling forward and lifting the abdomen inward. Rolling shoulder blades down the back ensures the shoulders are relaxed and broad. Inhaling and maintaining the curvature of the spine by lowering the lower back towards the mat.
Mat-one-leg circle: The participant assumed supine, extended one leg vertically towards the ceiling, aligned both legs along the centerline, and secured arms, shoulder blades, pelvis, and head onto the mat. Create a circular shape with the toe, then cross a leg over the body and execute a circular motion below, around, and above. Roll down the shoulder blades while maintaining contact with the mat. Inhale during one cycle and exhale during the next.
Mat-Rolling Like a Ball: The participant demonstrated it by placing his hands crossed, keeping his heels firmly on the floor, and performing a forward curling motion. Then lifts his feet off the mat, keeping his heels close together and his toes slightly apart. Engaging the abdominal muscles, keep the chin lowered toward the chest, and inhale to initiate a backward rolling motion. Maintain a state of equilibrium while rolling up and looking down.
Mat-Spine Stretch: The student sat on his back, chin to chest, and extended his leg while imprinting his spine on the mat. He pressed his shoulder blade tips into the mat, drawing his belly in and up. He then lowered his leg to the ground, touching the calf three times. He inhaled to switch, and he exhaled to lower and touch.
Statistical Analysis
A histogram, drawing box plot, mean, standard deviation, and Shapiro–Wilk test were employed to examine the homogeneity of the observed results. The distribution of all assessed variables (core endurance tests, Prokin indices) showed a parametric distribution. In order to distinguish between and within the measured outcomes, a two-way mixed model MANOVA was employed. The demographic information of the individuals was compared using the unpaired t–test, and the nominal data were compared using the chi-square test. Mean and standard deviation were used to represent quantitative data, and numbers and percentages were used for nominal data. An alpha level of 0.05 or less was set as a significance level. SPSS version 20 was used for all statistical computations.
Results
This study included a total of 145 undergraduate students, consisting of 84 females and 61 males. Figure 1 presents the study flowchart. Table 1 displays the demographic characteristics of the participants. Findings revealed no statistically significant difference between the two groups regarding age, weight, height, BMI, or sex, and the baseline values of the measured outcomes (p ˃ 0.05), as displayed in Tables 1–3.
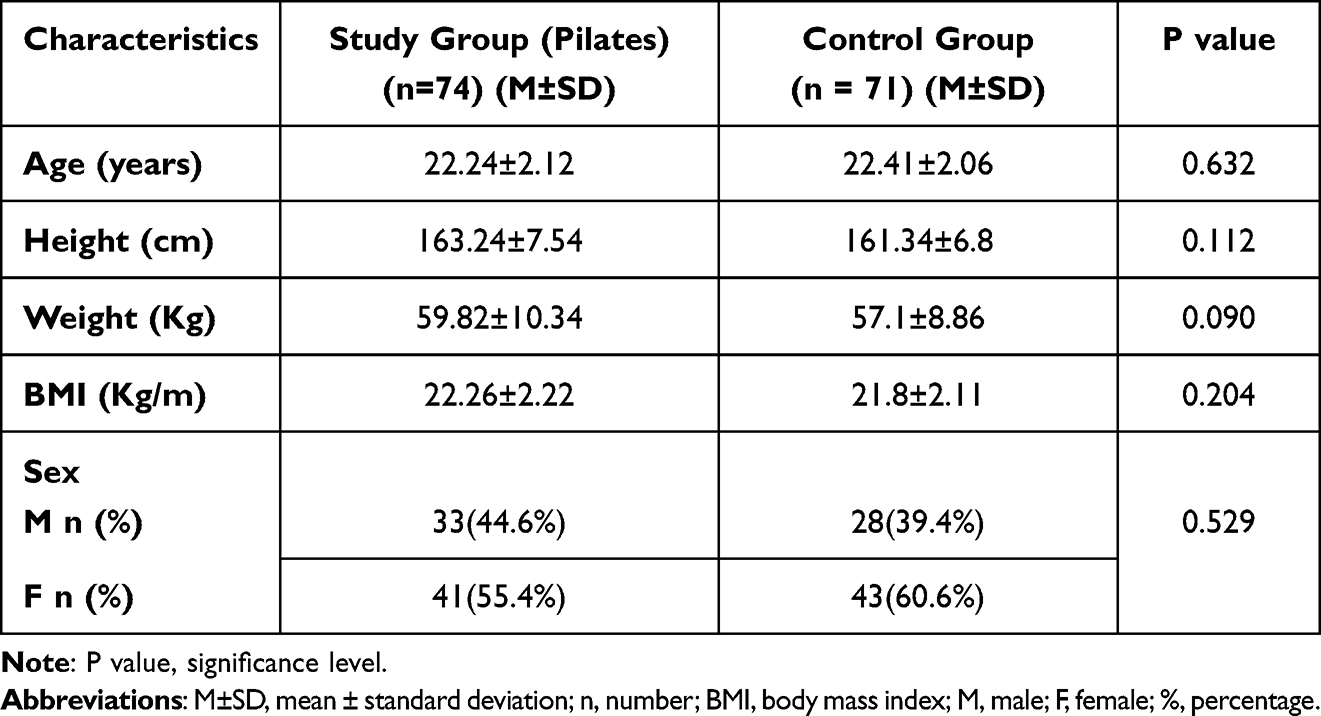 |
Table 1 Demographic and Clinical Characteristics of Both Groups |
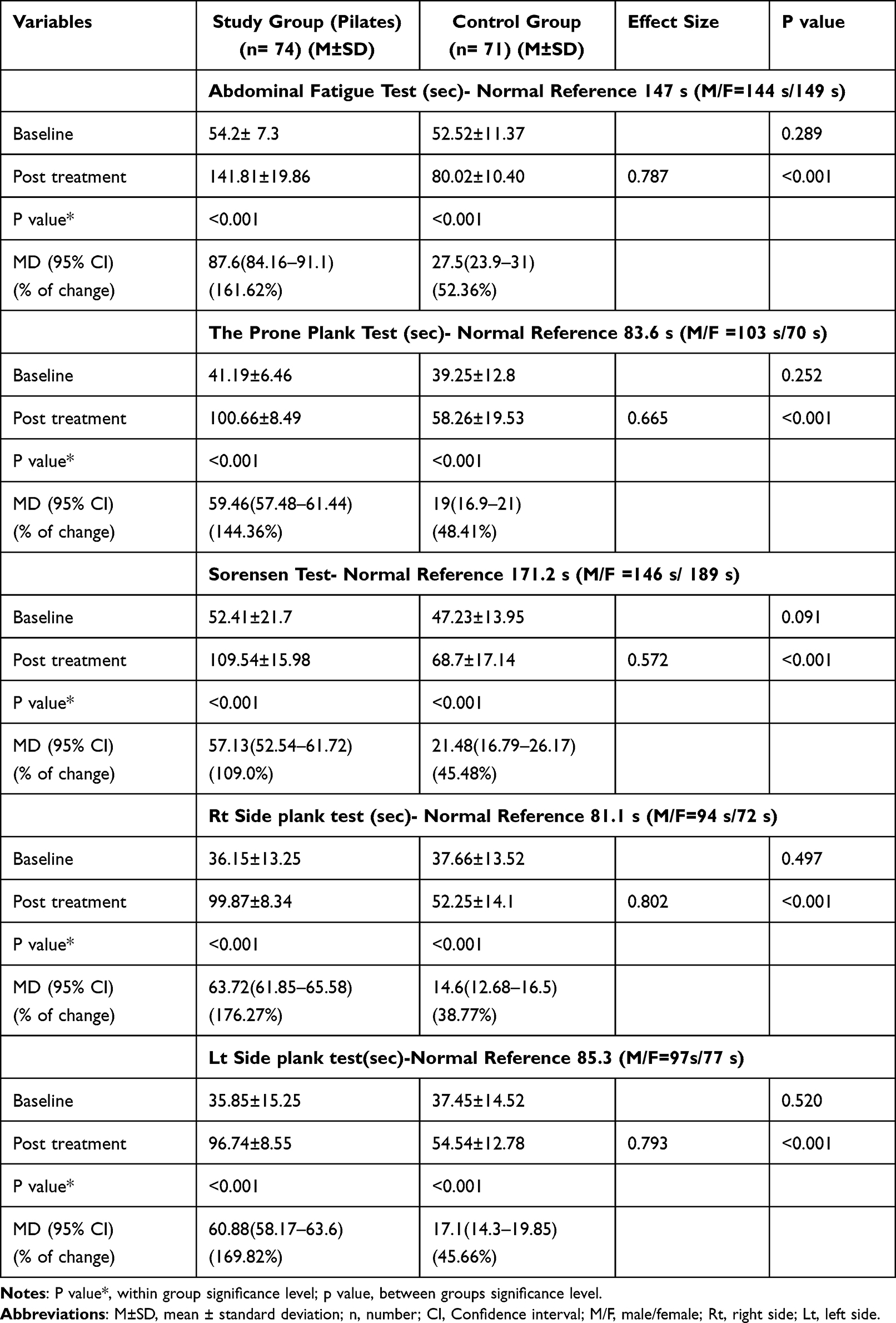 |
Table 2 Within and Between Groups, Comparisons of the Primary Outcome Measures (Core Endurance Tests) |
 |
Table 3 Within and Between Groups, Comparisons of the Secondary Outcome Measures (Prokin System Variables) |
After 3 months of exercise, the within-group comparison revealed a significant difference in both the Pilates and control groups in all the tested outcomes (p<0.001). Comparison between groups exhibited an improvement that favored the Pilates group regarding the core endurance tests (p < 0.05), Prokin balance indices OE_Perimeter, OE_Perimeter, and OE_ Ellipse area (p < 0.001); however, there is no difference regarding CE_ Ellipse area (p = 0.062), as shown in Tables 2 and 3.
Discussion
To the best of our knowledge, this is the first study that has been conducted to investigate the effect of pilates exercise on core endurance and static balance after recovery from COVID-19. A 12-week Pilates exercise program showed positive results for core endurance and static balance; therefore, we rejected our null hypothesis regarding the effects of Pilates exercises on core endurance and static balance. For all participants, the baseline scores of the five core endurance tests performed were well below the normal average means, indicating the weakness of the core muscles of the participants included in the study. We used the normal average means from McGill et al for the trunk flexor, trunk extensor, and right and left side plank tests as guides in our study because the characteristics of their sample were similar to ours.29 For the prone plank test, we used the normal values from Strand et al.39 In the Pilates group, the post-scores on the core endurance tests increased by almost twice the pre-training score compared to the control group.
The core endurance improvement could be attributed to that Pilates exercises improve pulmonary function and capacity by engaging the respiratory muscles,40 increasing oxygen delivery to skeletal muscles. Moreover, enhancement of trunk proprioception and trunk control give another clarification of the effect of Pilates training on core endurance, particularly the effect on the local core muscles, which play an important role in improving movement quality, postural balance,41 and neuromuscular efficiency and consequently improve proximal stability.42
Pilates exercises increase the thickness of the transverse abdominis (TrA), internal and external oblique, pelvic floor, and multifidus muscles, as confirmed through ultrasound evaluation after the application of pilates exercises.43,44 These play a key role in trunk stability. In addition, Pilates exercises increase core muscle contraction and intra-abdominal pressure, stabilizing the lumbar spine and pelvis.45,46 This finding was confirmed recently by the Tsartsapakis et al.45 They found that Pilates exercises significantly improved overall TrA thickness and activation in 44 healthy young and middle-aged women, particularly in young women aged 25–35 years. Moreover, the current results are supported by previous studies examining the greatest effects of core stability exercises and Pilates on TrA activation.47–50
Pilates exercises also improve neutral spinal alignment, co-contraction of the pelvic floor and deep abdominal muscles,21 and awareness and coordination of the TrA,45 as supported by a systematic review and meta-analysis that concluded that Pilates exercises performed for 5 to 12 weeks in healthy individuals, showing improved activation of core muscle endurance in both sexes,51 despite being conducted on healthy individuals.
The improvement in core muscle endurance was verified by the Lee study, which analyzed 16 experienced Pilates practitioners and 16 non-experienced subjects using 3D motion analysis. He found that experienced subjects had stronger abdominal and lower back core muscles and better trunk and pelvic stability, with a moderate correlation between experience and core stability.42
The Pilates group showed better static core balance than the control group, as indicated by a significant decrease in perimeter with OE and CE and ellipse area with CE compared to the control group. The decrease in perimeter and ellipse area was higher in OE than CE due to visual information improving the brain’s motor program and replacing the loss of somatosensory function.52
The Prokin system is a valid instrument that was used for evaluation of balance after balance training in people with white matter lesions,33 and stroke patients.53 Their results showed decreased parameters in perimeter and ellipse areas after 2 to 3 weeks of training.
The present results come in agreement with a study that examined the effect of Pilates mat exercise for 12 weeks on static and dynamic balance posture in 20 Korean high school archers using the Humac Norm Balance System. Dividing participants into exercise and control groups showed that only the exercise group showed improvement in both balance postures.38
Previous studies investigated the effect of Pilates mat exercises on pulmonary function and quality of life in COVID-19 patients; recently, Bagherzadeh-Rahmani et al conducted a study on the impact of Pilates and aqua Pilates training on COVID-19 patients, revealing significant improvements in pulmonary function and quality of life, attributing this effect to Pilates’ impact on core muscle endurance and balance.54 Moreover, a recent systematic review conducted on multiple sclerosis patients reported that Pilates exercise improves core stabilization, balance, gait, muscle strength, and aerobic capacity.55
The results of this study provide evidence of decreased core stability as a result of COVID-19 and support what other studies have found about the effects of Pilates. Our study is valuable and has many strengths: the sample size was sufficient to represent the study population; we used an easily clinically applicable and reliable method to assess core endurance using the five core endurance tests; and we used an objective, reliable method for static balance testing. The treatment program of this study lasted for a 12-week period, demonstrating its importance and practical implications in the evaluation and treatment of core muscle endurance and static balance in cases of post-COVID-19 infection. However, there are certain limitations to this study: first, it was not possible to blind the participants; second, it focused on examining only two aspects of core stability (endurance and balance); and third, it did not examine long-term follow-up after Pilates training was discontinued.
Conclusion
The study confirmed the decreased core muscular endurance after recovery from COVID-19 and showed that adding Pilates training to home exercises significantly improved core stability, endurance, and static balance in post-COVID-19 cases.
Data Sharing Statement
The research study’s dataset is not publicly accessible, but can be obtained from the author upon formal request.
Acknowledgments
We are grateful to the students who have recovered from COVID-19 for their participation in this study.
Funding
The study received no specific financial support from public, commercial, or non-profit funding bodies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evcik D. Musculoskeletal involvement: COVID-19 and post COVID 19. Turkish J Phys Med Rehabil. 2023;69(1):1–7
2. Novelli G, Biancolella M, Mehrian-Shai R, et al. COVID-19 update: the first 6 months of the pandemic human genomics. Human Genomics. 2020;4:1–9.
3. Akbarialiabad H, Taghrir MH, Abdollahi A, et al. Long COVID, a comprehensive systematic scoping review. Infection. 2021;49(6):1163–1186. doi:10.1007/s15010-021-01666-x
4. Yapici H, Yagin FH, Emlek B, et al. Examining barriers to participation in physical activity: a study of adults. J Exerc Sci Phys Act Rev. 2023;2023:1–11.
5. Montes-Ibarra M, Oliveira CLP, Orsso CE, Landi F, Marzetti E, Prado CM. The impact of long COVID-19 on muscle health, clinics in geriatric medicine. W B Saunders. 2022;38:545–557.
6. Giardini M, Arcolin I, Guglielmetti S, Godi M, Capelli A, Corna S. Balance performance in patients with post-acute COVID-19 compared to patients with an acute exacerbation of chronic obstructive pulmonary disease and healthy subjects. Int J Rehabil Res. 2022;45(1):47–52. doi:10.1097/MRR.0000000000000510
7. Huxel Bliven KC, Anderson BE. Core stability training for injury prevention. Sports Health. 2013;5(6):514–522. doi:10.1177/1941738113481200
8. Hibbs AE, Thompson KG, French D, Wrigley A, Spears I. Optimizing performance by improving core stability and core strength. Sports Med. 2008;38(12):995–1008. doi:10.2165/00007256-200838120-00004
9. Smith CE, Nyland J, Caudill P, Brosky J, Caborn DNM. Dynamic trunk stabilization: a conceptual back injury prevention program for volleyball athletes. J Orthop Sports Phys Ther. 2008;38(11):703–720. doi:10.2519/jospt.2008.2814
10. Rasmussen-Barr E, Nordin M, Skillgate E. Are respiratory disorders risk factors for troublesome neck/shoulder pain? A study of a general population cohort in Sweden. Eur Spine J. 2023;32(2):659–666. doi:10.1007/s00586-022-07509-z
11. Chandan JS, Brown KR, Simms-Williams N, et al. Non-pharmacological therapies for post-viral syndromes, including long COVID: a systematic review. Int J Environ Res Public Health. 2023;16(4):1.
12. Franks J, Thwaites C, Morris ME. Pilates to improve core muscle activation in chronic low back pain: a systematic review. Healthc. 2023;11(10):1.
13. Adıgüzel S, Aras D, Gülü M, Aldhahi MI, Alqahtani AS, AL-Mhanna SB. Comparative effectiveness of 10-week equipment-based pilates and diaphragmatic breathing exercise on heart rate variability and pulmonary function in young adult healthy women with normal BMI – a quasi-experimental study. MC Sports Sci Med Rehabil. 2023;15(1):1.
14. Mayer KP, Steele AK, Soper MK, et al. Physical therapy management of an individual with post-COVID syndrome: a case report. Phys Ther. 2021;1(6):101.
15. Cevei M, Onofrei RR, Gherle A, Gug C, Stoicanescu D. Rehabilitation of post-COVID-19 musculoskeletal sequelae in geriatric patients: a case series study. Int J Environ Res Public Health. 2022;19(22):15350. doi:10.3390/ijerph192215350
16. Ponce-Campos SD, Díaz JM, Moreno-Agundis D, et al. A physiotherapy treatment plan for post-COVID-19 patients that improves the FEV1, FVC, and 6-min walk values, and reduces the sequelae in 12 sessions. Front Rehabil Sci. 2022;3:907603. doi:10.3389/fresc.2022.907603
17. Mashhadi M, Sahebozamani M, Daneshjoo A, Adeli SH. the effect of respiratory and core stability tele-exercises on pulmonary and functional status in COVID-19 survivors: a randomized clinical trial. Phys Treat - Specif Phys Ther J. 2022;12(2):85–92.
18. Patti A, Thornton JS, Giustino V, et al. Effectiveness of Pilates exercise on low back pain: a systematic review with meta-analysis. Disabil Rehabil. 2023;26:1–14. doi:10.1080/09638288.2023.2251404
19. Rydeard R, Leger A, Smith D. Pilates-based therapeutic exercise: effect on subjects with nonspecific chronic low back pain and functional disability: a randomized controlled trial. J Orthop Sports Phys Ther. 2006;36(7):472–484. doi:10.2519/jospt.2006.2144
20. Anderson BD, Spector A Introduction to pilates-based rehabilitation;2024.
21. Wells C, Kolt GS, Marshall P, Bialocerkowski A. The definition and application of pilates exercise to treat people with chronic low back pain: a delphi survey of Australian physical therapists. Phys Ther. 2014;94(6):792–805. doi:10.2522/ptj.20130030
22. Bulguroglu HI, Bulguroglu M. The effects of online pilates and face-to-face pilates in healthy individuals during the COVID-19 pandemic: a randomized controlled study. BMC Sport Sci Med Rehabil. 2023;15(1):12. doi:10.1186/s13102-023-00625-3
23. Pk DS, Sigoli E, Ljg B, As C. The musculoskeletal involvement after mild to moderate COVID-19 infection. Front Mater. 2022;13:1.
24. Yang LL, Yang T. Pulmonary rehabilitation for patients with coronavirus disease 2019 (COVID-19). Chronic Dis Tran Med. 2020;6(2):79–86. doi:10.1016/j.cdtm.2020.05.002
25. Chaves C, Filho RAF, Dutra MAB. Physical therapy rehabilitation after hospital discharge in patients affected by COVID-19: a systematic review. BMC Infect Dis. 2023;23(1):1–9. doi:10.1186/s12879-022-07947-6
26. Schulz KF, Altman DG, Moher D. Consort 2010 statement. Obstet Gynecol. 2010;115(5):1063–1070. doi:10.1097/AOG.0b013e3181d9d421
27. Löllgen H, Bachl N, Papadopoulou T, et al. Recommendations for return to sport during the SARS-CoV-2 pandemic. BMJ Open Sport Exercise Med. 2020;6(1):e000858. doi:10.1136/bmjsem-2020-000858
28. AlAbdulwahab SS, Kachanathu SJ. Effects of body mass index on foot posture alignment and core stability in a healthy adult population. J Exerc Rehabil. 2016;12(3):182–187. doi:10.12965/jer.1632600.300
29. McGill SM, Childs A, Liebenson C. Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil. 1999;80(8):941–944. doi:10.1016/S0003-9993(99)90087-4
30. Aggarwal A, Kumar S, Madan R, Kumar R. Relationship among different tests of evaluating low back core stability. J Musculoskelet Res. 2011;14(02):1250004. doi:10.1142/S0218957712500042
31. Waldhelm A, Li L. Endurance tests are the most reliable core stability related measurements. J Sport Heal Sci. 2012;1(2):121–128. doi:10.1016/j.jshs.2012.07.007
32. Wang S, Yang J, Zhu Y. Reliability and validity of static balance measures in hemiplegic patients using balance feedback training equipment. Chinese J Rehabil Med. 2011;26(11):1.
33. You H, Zhang H, Liu J, et al. Effect of balance training with Pro-kin System on balance in patients with white matter lesions. Medicine. 2017;96(51):e9057. doi:10.1097/MD.0000000000009057
34. Donath L, Roth R, Zahner L, Faude O. Testing single and double limb standing balance performance: comparison of COP path length evaluation between two devices. Gait Posture. 2012;36(3):439–443. doi:10.1016/j.gaitpost.2012.04.001
35. Asseman F, Caron O, Crémieux J. Is there a transfer of postural ability from specific to unspecific postures in elite gymnasts? Neurosci Lett. 2004;358(2):83–86. doi:10.1016/j.neulet.2003.12.102
36. Thompson PD, Arena R, Riebe D, Pescatello LS. American college of sports medicine. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr Sports Med Rep. 2013;12(4):215–217. doi:10.1249/JSR.0b013e31829a68cf
37. Marandi SM, Shahnazari Z, Minacian V, Zahed A. A comparison between Pilates exercise and aquatic training effects on mascular strength in women with Mulitple sclorosis. Pak J Med Sci. 2013;29(1 suppl):1.
38. Park JM, Hyun GS, Jee YS. Effects of Pilates core stability exercises on the balance abilities of archers. J Exerc Rehabil. 2016;12(6):553–558. doi:10.12965/jer.1632836.418
39. Strand SL, Hjelm J, Shoepe TC, Fajardo MA. Norms for an isometric muscle endurance test. J Hum Kinet. 2014;40(1):93–102. doi:10.2478/hukin-2014-0011
40. Endleman I, Critchley DJ. Transversus abdominis and obliquus internus activity during pilates exercises: measurement with ultrasound scanning. Arch Phys Med Rehabil. 2008;89(11):2205–2212. doi:10.1016/j.apmr.2008.04.025
41. Suner-Keklik S, Numanoglu-Akbas A, Cobanoglu G, Kafa N, Guzel NA. An online pilates exercise program is effective on proprioception and core muscle endurance in a randomized controlled trial. Ir J Med Sci. 2022;191(5):2133–2139. doi:10.1007/s11845-021-02840-8
42. Lee K. The relationship of trunk muscle activation and core stability: a biomechanical analysis of pilates-based stabilization exercise. Int J Environ Res Public Health. 2021;18(23):12804. doi:10.3390/ijerph182312804
43. Giacomini MB, da Silva AMV, Weber LM, Monteiro MB. The pilates method increases respiratory muscle strength and performance as well as abdominal muscle thickness. J Bodyw Mov Ther. 2016;20(2):258–264. doi:10.1016/j.jbmt.2015.11.003
44. Gala-Alarcón P, Calvo-Lobo C, Serrano-Imedio A, Garrido-Marín A, Martín-Casas P, Plaza-Manzano G. Ultrasound evaluation of the abdominal wall and lumbar multifidus muscles in participants who practice pilates: a 1-year follow-up case series. J Manipulative Physiol Ther. 2018;41(5):434–444. doi:10.1016/j.jmpt.2017.10.007
45. Tsartsapakis I, Gerou M, Zafeiroudi A, Kellis E. Transversus abdominis ultrasound thickness during popular trunk-pilates exercises in young and middle-aged women. J Funct Morphol Kinesiol. 2023;8(3):250.
46. Ali OI, Abdelraouf OR, El-Gendy AM, et al. Efficacy of telehealth core exercises during COVID-19 after bariatric surgery: a randomized controlled trial. Eur J Phys Rehabil Med. 2022;58(6):845–852. doi:10.23736/S1973-9087.22.07457-3
47. Imai A, Kaneoka K, Okubo Y, et al. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J Orthop Sports Phys Ther. 2010;40(6):369–375. doi:10.2519/jospt.2010.3211
48. Okubo Y, Kaneoka K, Mai A, et al. Electromyographic analysis of transversus abdominis and lumbar multifidus using wire electrodes during lumbar stabilization exercises. J Orthop Sports Phys Ther. 2010;40(11):743–750. doi:10.2519/jospt.2010.3192
49. Emami F, Pirouzi S, Taghizadeh S. Comparison of abdominal and lumbar muscles electromyography activity during two types of stabilization exercises. Zahedan J Res Med Sci. 2015;17(4). doi:10.5812/zjrms.17(4)2015.963
50. Moghadam N, Ghaffari MS, Noormohammadpour P, et al. Comparison of the recruitment of transverse abdominis through drawing-in and bracing in different core stability training positions. J Exerc Rehabil. 2019;15(6):819–825. doi:10.12965/jer.1939064.352
51. Campos RR, Dias JM, Pereira LM, et al. Effect of the Pilates method on physical conditioning of healthy subjects: a systematic review and meta-analysis. J Sports Med Phys Fitness. 2016;56(7–8):864–873.
52. Mulder T, Hulstyn W. Sensory feedback therapy and theoretical knowledge of motor control and learning. Am J Phys Med. 1984;63(5):226–244.
53. Zhang M, You H, Zhang H, et al. Effects of visual feedback balance training with the Pro-kin system on walking and self-care abilities in stroke patients. Medicine. 2020;99(39):1.
54. Bagherzadeh-Rahmani B, Kordi N, Haghighi AH, et al. Eight weeks of pilates training improves respiratory measures in people with a history of COVID-19: a preliminary study. Sports Health. 2023;15(5):710–717. doi:10.1177/19417381221124601
55. Rodríguez-Fuentes G, Silveira-Pereira L, Ferradáns-Rodríguez P, Campo-Prieto P. Therapeutic effects of the pilates method in patients with multiple sclerosis: a systematic review. J Clin Med. 2022;11(3):683. doi:10.3390/jcm11030683
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.