Back to Journals » Journal of Pain Research » Volume 19
Effects of Oxycodone versus Sufentanil-Based Intravenous Patient-Controlled Multimodal Analgesia on Early Gastrointestinal Recovery and Pain After Laparoscopic Colorectal Cancer Surgery: A Randomized Double-Blind Trial
Authors Jia W, Wang Z, Lin Y, Yao X, Sheng X, Zhou Y, Xu C, Liu Y, Jiao H
Received 26 December 2025
Accepted for publication 1 April 2026
Published 14 April 2026 Volume 2026:19 591268
DOI https://doi.org/10.2147/JPR.S591268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rushna Ali
Wensen Jia,1,2,* Zeyang Wang,3,* Yulian Lin,1,2,* Xiangyu Yao,2 Xinfang Sheng,2 Ye Zhou,2 Chun Xu,2 Yangming Liu,2 Hao Jiao1,2,4
1Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2School of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Anesthesiology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 4Department of Anesthesiology, Jiangsu Cancer Hospital, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Jiao, Department of Anesthesiology, Jiangsu Cancer Hospital, Nanjing, Jiangsu, People’s Republic of China, Tel +86 13512560960, Email [email protected]
Purpose: Oxycodone is a dual μ/κ-opioid receptor agonist effective in managing both somatic and visceral pain. We compared the effect of oxycodone-based versus sufentanil-based multimodal regimens on early gastrointestinal recovery and pain control following laparoscopic colorectal cancer surgery.
Methods: In this single-center, prospective, randomized, double-blind trial, 76 patients undergoing elective laparoscopic colorectal cancer surgery were allocated to the oxycodone group (Group O) or the sufentanil group (Group S). Both groups received standardized multimodal analgesia with preoperative TAP block, postoperative PCIA, and flurbiprofen axetil for rescue. The primary endpoint was time to first flatus; secondary outcomes included other recovery indicators, pain and sedation scores, opioid and PCIA use, adverse effects, PACU stay, and hospital length of stay.
Results: Group O shortened time to first flatus (43.7± 7.9 h vs 48.4± 8.7 h, mean difference − 4.8 h; 95% CI − 8.6 to − 1.0; P = 0.015) and time to ambulation (47.3± 5.1 h vs 50.0± 3.8 h, mean difference − 2.7 h; 95% CI − 4.8 to − 0.7; P = 0.010). Group O reduced PCIA demands (median 0 vs 2), rescue analgesia (7.9% vs 26.3%), PONV (7.9% vs 31.6%), PACU stay (median 55 vs 60 min), and remifentanil use (2.8± 0.4 vs 3.1± 0.5 mg) (all P < 0.05). Postoperative sedation at 4 h was better in group O. Visceral pain scores at 12 h and 48 h were lower with oxycodone, whereas incisional pain and solid-food tolerance did not differ; length of stay was similar.
Conclusion: Oxycodone-based multimodal analgesia was associated with improved early gastrointestinal recovery indicators, better visceral pain control, and fewer opioid-related adverse effects than the sufentanil-based regimen, but did not reduce hospital length of stay.
Trial Registration: Chinese Clinical Trial Registry (ChiCTR2500100676).
Keywords: oxycodone, laparoscopic colorectal surgery, gastrointestinal recovery, multimodal analgesia, enhanced recovery after surgery, ERAS
Introduction
Colorectal cancer is among the most common gastrointestinal malignancies, and surgical resection remains the mainstay of treatment. With the increasing adoption of minimally invasive techniques, laparoscopic surgery has become widely used because it reduces surgical trauma and facilitates postoperative recovery.1,2 Nevertheless, postoperative gastrointestinal dysfunction (PGID), manifested as delayed first flatus, abdominal distension, nausea, and vomiting, remains common after laparoscopic colorectal surgery and is associated with prolonged recovery and increased healthcare resource use.3,4 Within enhanced recovery after surgery (ERAS) pathways, optimizing perioperative analgesia represents a potentially modifiable strategy to mitigate PGID and support early recovery.5
Pain itself may contribute to PGID. Post-laparoscopic pain consists mainly of incisional pain and visceral pain. Incisional pain is restricted to the abdominal wall incision site, whereas visceral pain is typically deep, dull, and poorly localized.6–8 After laparoscopic procedures, visceral pain often predominates over somatic incisional pain and is more difficult to assess and treat. Persistent visceral pain may trigger sympathetic activation and reflex ileus, thereby contributing to delayed gastrointestinal recovery.6–9 Accordingly, analgesic strategies that more effectively target visceral nociception may be particularly relevant in ERAS-oriented care for laparoscopic colorectal surgery.
Current postoperative analgesia commonly relies on μ-opioid receptor agonists such as sufentanil. Although effective for analgesia, μ-agonists may suppress enteric motility and increase postoperative nausea and vomiting (PONV), which may limit their suitability in gastrointestinal surgery.10,11 Oxycodone, a dual μ/κ opioid receptor agonist, provides analgesia for both somatic and visceral pain, and its κ-receptor activity relevant to visceral pain suggests a potentially more gut-friendly profile.12–17 Previous oxycodone-related studies in postoperative analgesia have included both intravenous and oral regimens, but have varied in surgical population, comparator strategy, and outcome focus, limiting direct comparison across studies. Oral oxycodone has demonstrated postoperative analgesic efficacy in diverse surgical populations, whereas ERAS pathways for colorectal surgery remain heterogeneous in their multimodal analgesic composition and opioid-sparing approaches.18,19 Because opioid-related gastrointestinal dysfunction may delay recovery, reducing gastrointestinal adverse effects remains a clinically relevant objective in ERAS-oriented perioperative management.20 Therefore, in laparoscopic colorectal surgery, an important unmet clinical need remains the identification of analgesic regimens that better target visceral pain while minimizing gastrointestinal side effects and supporting early postoperative recovery.
In the present study, postoperative recovery was defined primarily in terms of early ERAS-relevant clinical dimensions, including gastrointestinal function, pain control, early mobilization, and opioid-related adverse effects, rather than broader patient-reported recovery scales or long-term outcomes.5 Therefore, we conducted this prospective, randomized, double-blind trial to compare oxycodone-based versus sufentanil-based multimodal analgesia in patients undergoing laparoscopic colorectal cancer surgery, with a particular focus on early postoperative gastrointestinal recovery, pain outcomes, and short-term recovery indicators during the first 48 hours after surgery. We hypothesized that the oxycodone-based regimen would be associated with improved early gastrointestinal recovery and visceral pain control compared with the sufentanil-based regimen, while recognizing that broader ERAS outcomes, such as hospital length of stay, may be influenced by multiple perioperative factors beyond analgesic strategy alone.21
Methods
Study Design
This was a single-center, prospective, randomized, double-blind controlled trial approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (Approval No. XYFY2024-KL577-01). The enrollment started in April 2025, and all follow-ups were completed by July 2025. The study was registered in the Chinese Clinical Trial Registry (ChiCTR2500100676). Written informed consent was obtained from all participants.
Patient Selection
Eligible patients were adults aged 18 to 70 years, with American Society of Anesthesiologists (ASA) physical status I–III and a body mass index (BMI) ≤ 30 kg/m², who were scheduled to undergo laparoscopic surgery for colorectal cancer. Exclusion criteria included: (1) active or clinically significant functional gastrointestinal diseases (eg, Crohn’s disease, ulcerative colitis); (2) chronic opioid therapy or a history of opioid or alcohol dependence; (3) allergy to drugs in the study; (4) severe cardiac, respiratory, hepatic, or renal impairment that may affect anesthesia or postoperative recovery; (5) major postoperative complications, such as severe infection, uncontrolled bleeding, or analgesic device failure; (6) recent involvement in another clinical trial (within 3 months); (7) unwillingness or inability to complete follow-up assessments.
Randomization and Blinding
Patients were randomized in a 1:1 ratio into the oxycodone group (Group O) or sufentanil group (Group S). Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared and kept by an independent investigator. The envelopes were opened in sequence only after the patient had been enrolled. Both drugs were prepared as colorless solutions in normal saline and administered via identical syringes and Patient-Controlled Intravenous Analgesia (PCIA) pumps. The anesthesiologist strictly adhered to a standardized anesthesia protocol. Patients, anesthesiologists, surgical team, postoperative nursing staff and outcome assessors were blinded to group allocation. All assessors were trained to proficiency in applying the assessment scales and passed consistency tests prior to trial commencement.
Anesthesia
Preoperative fasting, bowel preparation, and perioperative thromboprophylaxis were managed according to the routine standardized protocol in all patients. Upon operating room arrival, standard monitoring was applied, including electrocardiography (ECG), blood pressure (BP), pulse oximetry (SpO2). Baseline vital signs were documented. Subsequently, general anesthesia was induced using etomidate 0.3 mg kg−1, sufentanil 0.5 μg kg−1, rocuronium 0.9 mg kg−1, and tropisetron 2 mg. Following endotracheal intubation, mechanical ventilation was initiated with EtCO2 maintained at 35–45 mmHg. Patients then received group-specific opioids: Group O (oxycodone 0.1 mg kg−1) and Group S (sufentanil 0.1 μg kg−1).
After anesthesia induction, all patients received a preoperative bilateral ultrasound-guided transversus abdominis plane (TAP) block. The block was performed by an attending anesthesiologist on the lateral abdominal wall, between the lower costal margin and the iliac crest. Under real-time ultrasound guidance, 20 mL of 0.375% ropivacaine was injected on each side, with confirmation of adequate hydrodissection and spread within the fascial plane. Anesthesia was maintained with remifentanil 0.1–0.3 μg kg−1 min−1, propofol 1–3 mg kg−1 h−1, rocuronium 5–10 μg kg−1 min−1, and sevoflurane (1–2%). BIS values were kept between 40–60, and normothermia was maintained. Sevoflurane was discontinued at skin closure, and rocuronium infusion was stopped 30 minutes before the end of surgery. Before completion, each group received a second loading dose of their assigned opioid: Group O (oxycodone 0.1 mg kg−1) and Group S (sufentanil 0.1 μg kg−1).
After surgery, patients were transferred to the PACU, and residual neuromuscular blockade was reversed with sugammadex 2 mg kg−1. Extubation criteria included adequate spontaneous breathing, consciousness, cough reflex, SpO2 > 95%, hemodynamic stability. PCIA was then started with group-specific solutions: oxycodone 2 mg kg−1 or sufentanil 2 μg kg−1 (adjusted for Boer Lean Body Mass equation),22 each with tropisetron 6 mg in 100 mL saline. Tropisetron was added to the PCIA solution in both groups at the same dose as a standardized prophylactic antiemetic measure. Consistent with literature, oxycodone clearance correlates significantly with lean body mass.23,24 Individualized PCIA dosing using Boer formula-adjusted body weight better aligns with its pharmacokinetics. PCIA was set with a 2 mL/h basal rate, 0.5 mL bolus, 15-min lockout, and continued for 48 h. Rescue analgesia (flurbiprofen axetil 50 mg IV) was provided for VAS ≥ 4. Published studies suggest that the equianalgesic ratio of intravenous morphine to oxycodone ranges from 0.65 to 1.5.25,26 Opioid doses were selected for regimen design based on available perioperative clinical literature: intravenous oxycodone 1 mg ≈ sufentanil 1 μg ≈ morphine 1 mg.27–30 This ratio was applied uniformly throughout the entire perioperative period. The conversion ratio was an approximate regimen-design assumption based on perioperative clinical literature rather than a universally established equianalgesic standard.
Patients were discharged from the PACU according to standardized criteria, including stable vital signs, adequate recovery of consciousness, satisfactory spontaneous respiration and oxygenation, and acceptable control of pain and nausea.
Postoperative Care
All patients were managed according to the same standardized postoperative care protocol to ensure consistent care between the two study groups: (1) early oral fluids within 4 hours; (2) early chewing gum; (3) unified ambulation protocol led by the surgical nursing team; (4) Tropisetron was incorporated into the PCIA solution for standardized antiemetic prophylaxis. If obvious nausea or vomiting occurred, 10 mg of Metoclopramide was intravenously injected for antiemesis; (5) standardized criteria for progression to oral food intake.
Outcome Measures
Primary outcome: time to first flatus (Time to first flatus was recorded immediately after patient report according to a standardized postoperative instruction process. For patients with an ostomy, visible inflation of the ostomy bag was used as the corresponding indicator). Secondary outcomes: time to first unaided ambulation (≥10 m with assistance permitted for safety), time to solid-food tolerance (first intake of chewable diet without emesis and nausea during the following 4 h), incisional pain scores (pain at the abdominal wall incision site) and visceral pain scores (deep, dull, and poorly localized abdominal pain) (VAS 0–10; rest vs cough) at 4, 12, 24 and 48 hours postoperatively, Ramsay Sedation Scale (RSS 1–6) at 4, 12, 24 and 48 hours postoperatively, PCIA use, rescue flurbiprofen use, intraoperative remifentanil use, PONV (any nausea requiring antiemetic or any vomiting), extubation time, respiratory depression (Respiratory rate < 8 min−1 or SpO2 < 90% despite O2), PACU stay, patient satisfaction (5-point Likert scale), and hospital length of stay.
Statistical Analysis
Sample size estimation was based on the primary outcome—time to first postoperative flatus. Pilot data from 10 patients in each group showed a mean difference of 6.2 hours, with standard deviations of 8.0 hours and 8.3 hours in the oxycodone and sufentanil groups, respectively. Using a two-sided α of 0.05 and β of 0.20 (power = 80%), the required sample size was calculated with PASS 21.0 software based on a two-sample means test model. Accounting for an estimated 20% dropout rate, a total of 76 patients were ultimately enrolled.
All statistical analyses were performed using SPSS version 25.0. Normality was assessed by Shapiro–Wilk. Between-group comparisons used Welch’s t-test or Mann–Whitney U as appropriate; categorical variables used χ²-test or Fisher’s exact test. Repeated measures (pain and sedation) were analyzed with GEE (exchangeable correlation, identity link) including group, time, and group × time, with Bonferroni for post-hoc time-point contrasts. The primary outcome was compared using a general linear model (GLM) adjusted for age, sex, surgical site, and ostomy (pre-specified). Analyses followed the intention-to-treat principle; there were no missing data. A two-sided α of 0.05 was considered statistically significant.
Results
Patient Enrollment and Baseline Characteristics
Of 88 screened patients, 76 met the eligibility criteria and consented to participate in the study, subsequently randomized into two equal groups (38 per group, Figure 1). All randomized patients completed the study and were included in the final intention-to-treat analysis, with no dropouts or losses to follow-up.
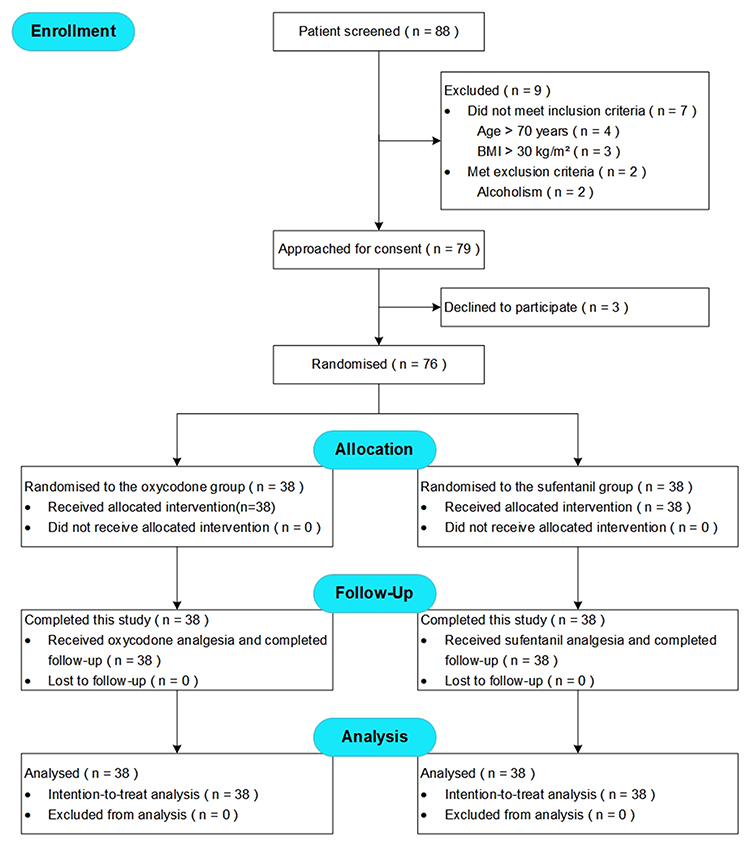 |
Figure 1 Trial flow diagram. |
Baseline demographic and clinical characteristics, including age, gender, BMI, ASA status, surgical site, comorbidities, and education level, were comparable between the oxycodone and sufentanil groups, showing no statistically significant differences (Table 1).
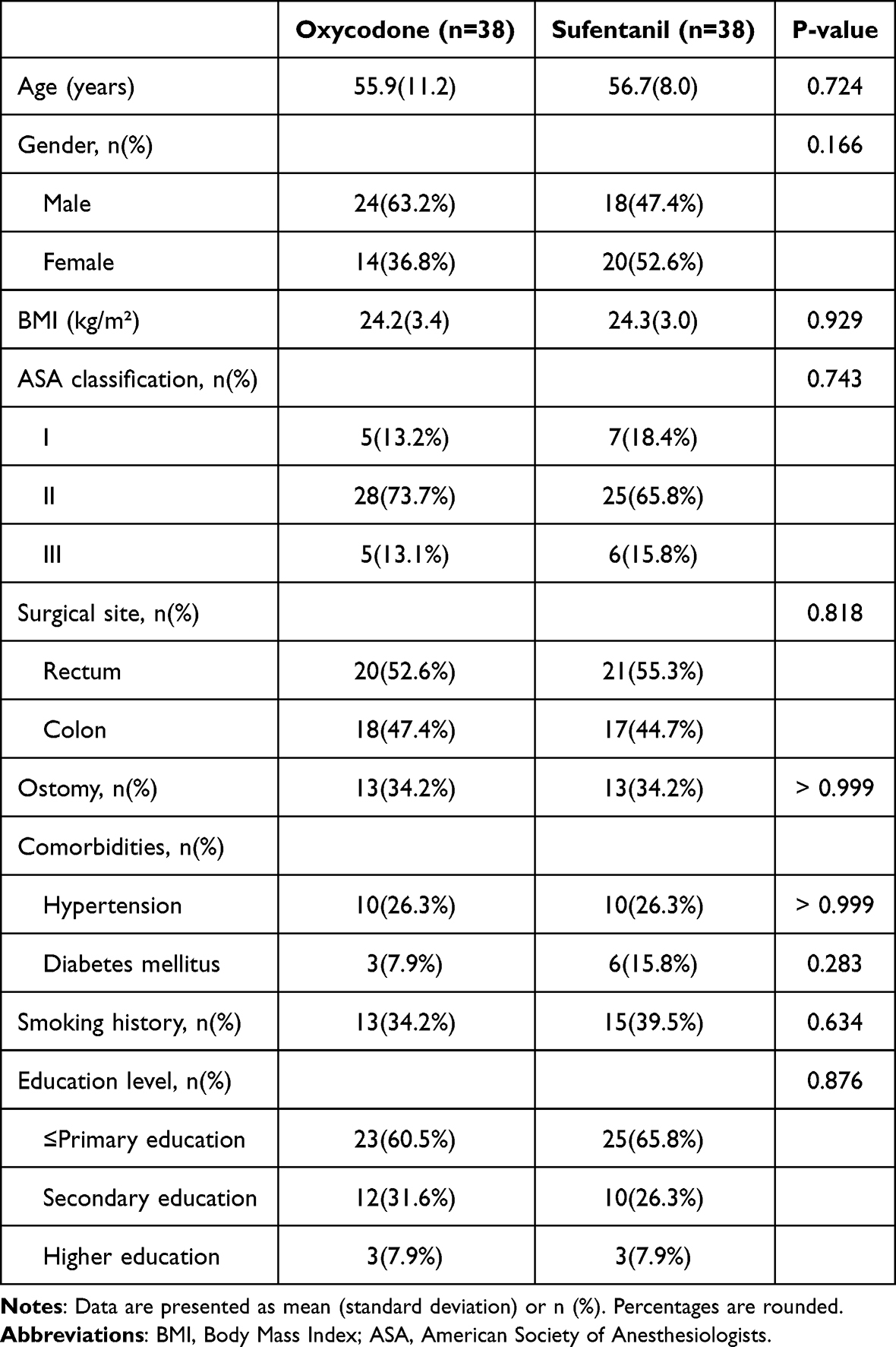 |
Table 1 Baseline Data |
Perioperative Data
There were no statistically significant differences between groups regarding surgical duration, anesthesia time, electrolyte levels, hemoglobin levels, intraoperative hemodynamic parameters, or vasoactive drug usage (Table 2).
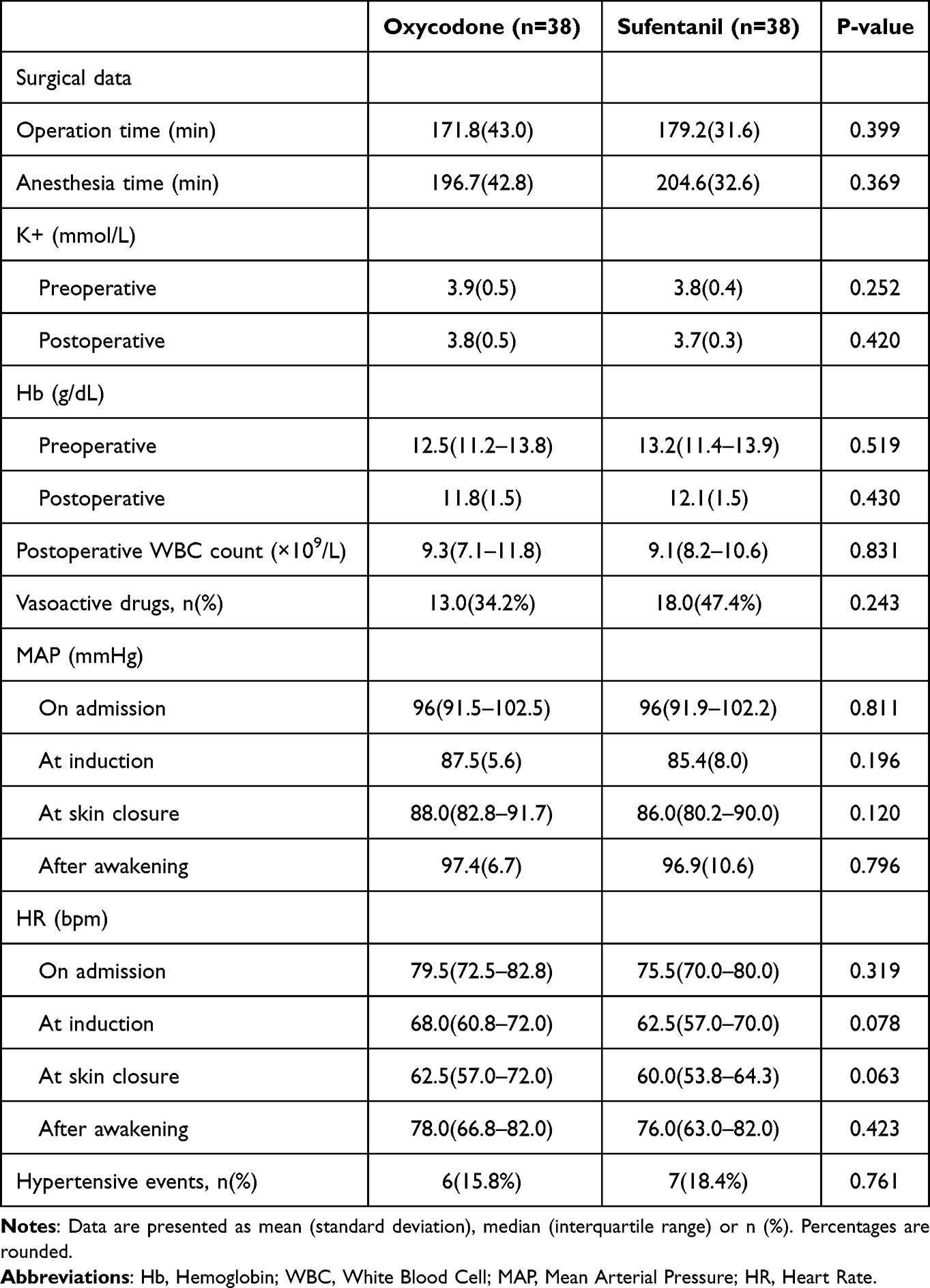 |
Table 2 Perioperative Data |
Gastrointestinal Recovery
Patients in the oxycodone group experienced significantly earlier recovery of gastrointestinal function compared with those in the sufentanil group. The oxycodone group demonstrated a shorter time to first flatus (43.7±7.9 h vs 48.4±8.7 h; mean difference −4.8; 95% CI, −8.6 to −1.0; P = 0.015; Table 3 and Figure 2). Subgroup analysis further indicated this advantage was consistent across age, gender, surgical site, and ostomy status, with no significant subgroup interactions observed (all P > 0.05; Figure 3). Early ambulation was also accelerated in the oxycodone group compared to the sufentanil group (47.3±5.1 h vs 50.0±3.8 h; mean difference −2.7; 95% CI, −4.8 to −0.7; P = 0.010; Table 3).
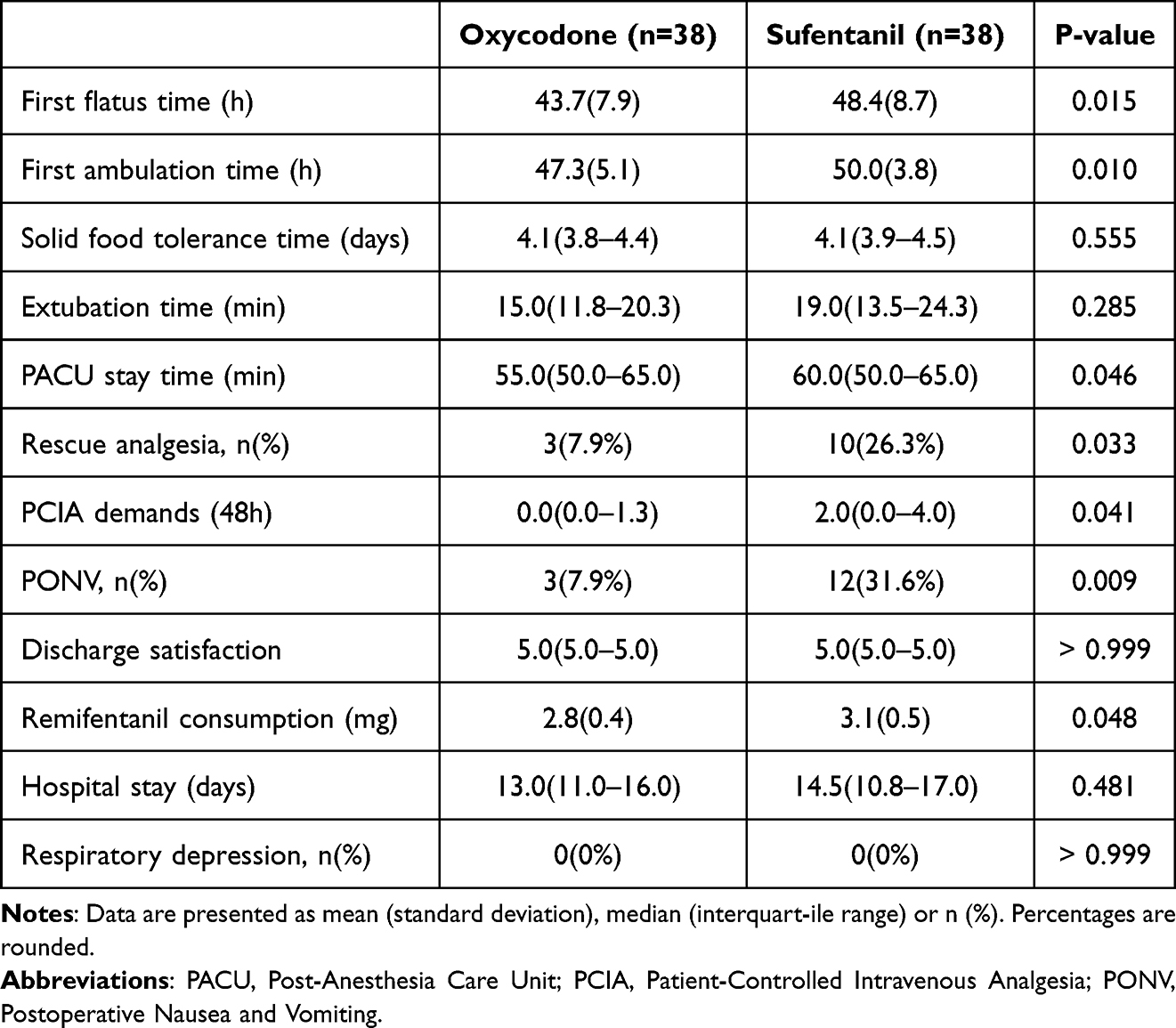 |
Table 3 Study Outcomes Data |
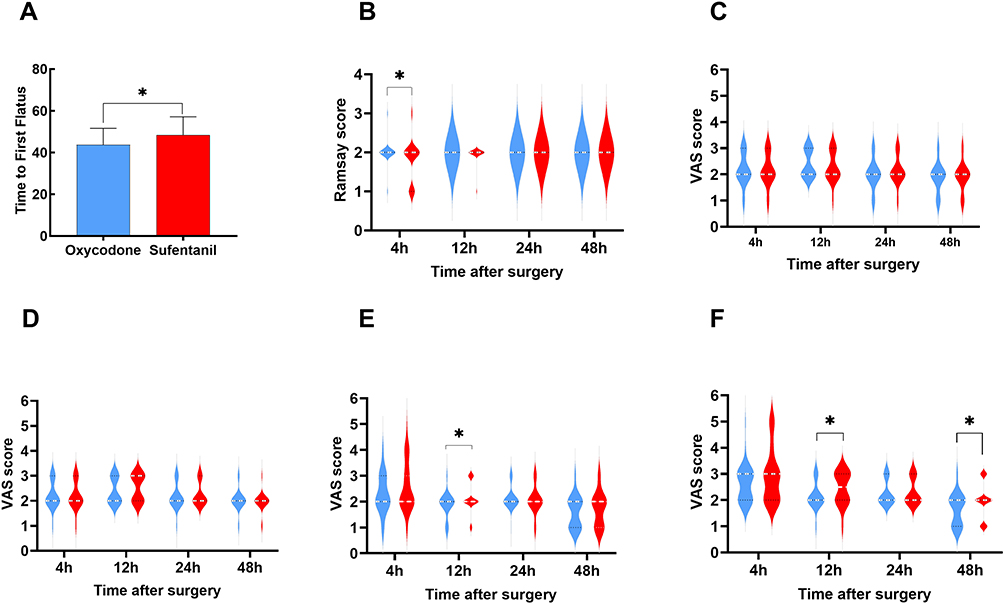 |
Figure 2 (A) Time to First Flatus; (B) Ramsay sedation scores; (C–F) Postoperative pain during the first 48 hours assessed using a Visual Analog Scale (VAS): (C) Incisional pain at rest; (D) Incisional pain at coughing; (E) Visceral pain at rest; (F) Visceral pain at coughing. The data for the oxycodone and sufentanil groups are shown in blue and red, respectively. Pointwise between-group comparisons used Welch’s t-test (A) or Mann–Whitney U-test (B–F), while longitudinal repeated-measures effects were analyzed using generalized estimating equations (GEE) and are summarized in Table 4. *P < 0.05. |
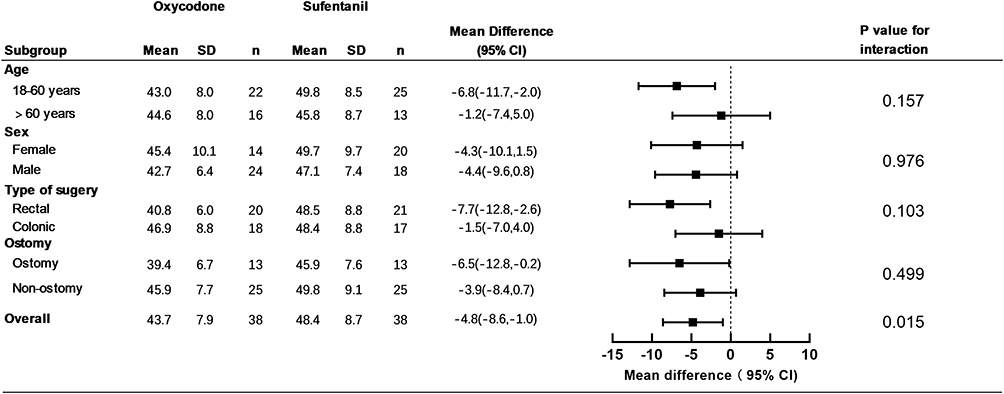 |
Figure 3 The estimated mean difference (MD) and 95% confidence interval (CI) between the sufentanil and oxycodone groups are displayed for each subgroup, derived from a general linear model (GLM). The squares represent the point estimate of the MD for each subgroup, with the horizontal lines spanning the 95% CI. The vertical dashed line (MD = 0) indicates no difference between groups. Subgroups are based on age, sex, type of surgery, and presence of an ostomy. Abbreviation: SD, standard deviation. |
Postoperative Pain and Sedation
Analgesic outcomes favored the oxycodone group. The incidence of rescue analgesia was lower (7.9% vs 26.3%; odds ratio [OR] 4.17; 95% CI, 1.05 to 16.60; P = 0.033), and patients in this group had fewer PCIA demands within 48 hours postoperatively (median: 0 vs 2, P = 0.041). Additionally, intraoperative remifentanil consumption was reduced in the oxycodone group (2.8±0.4 mg vs 3.1±0.5 mg; mean difference −0.2 mg; 95% CI −0.4 to −0.0; P = 0.048; Table 3). Patients receiving oxycodone reported better sedation at 4 hours postoperatively (Ramsay scores, P < 0.05; Figure 2). Furthermore, postoperative visceral pain control was superior in the oxycodone group, with lower VAS scores observed at rest (12 hours postoperatively, P < 0.05; Figure 2) and during coughing (12 and 48 hours postoperatively, all P < 0.05; Figure 2). However, incisional pain scores did not differ significantly between groups at any timepoint (Figures 2). The VAS scores for visceral and incisional pain demonstrated a statistically significant decrease over time (all P < 0.05), with no significant difference observed in the temporal trends between the two groups. Sedation scores did not change significantly over time, although an overall group effect was observed (Table 4).
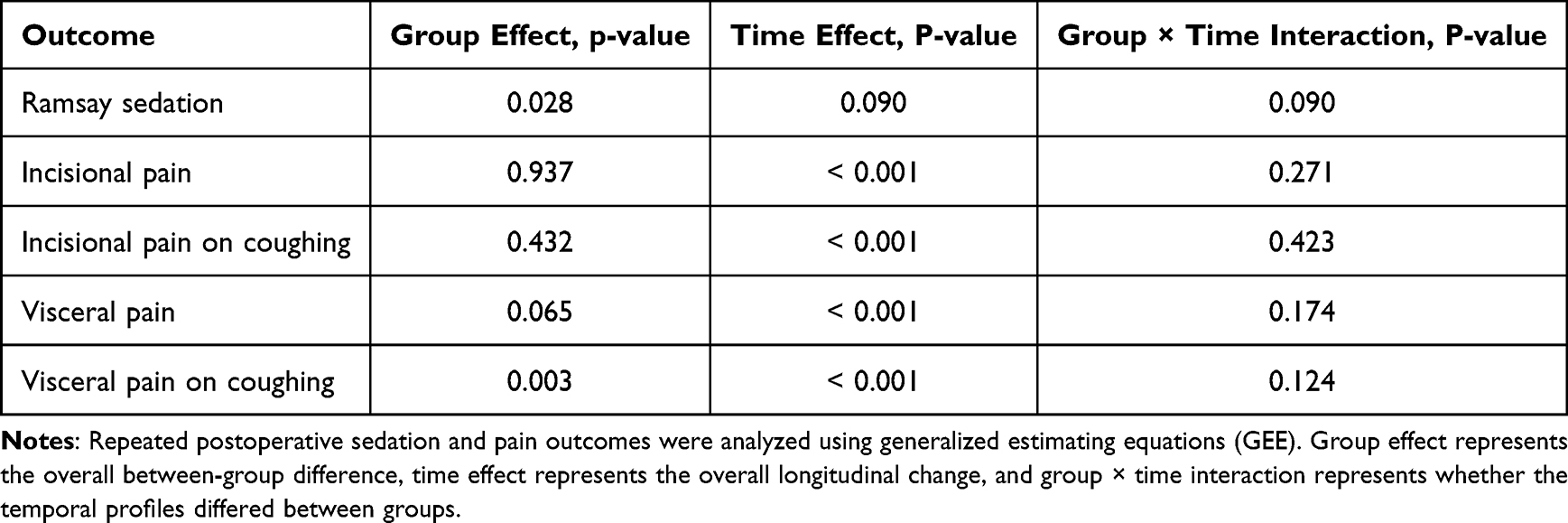 |
Table 4 Generalized Estimating Equation Analysis of Repeated Postoperative Pain and Sedation Outcomes |
Adverse Events and Other Outcomes
Postoperative nausea and vomiting (PONV) occurred significantly less frequently in the oxycodone group compared to the sufentanil group (7.9% vs 31.6%; OR, 5.4; 95% CI, 1.4 to 21.0; P = 0.009). Patients receiving oxycodone spent less time in the PACU (55 minutes [IQR: 50–65] vs 60 minutes [IQR: 50–65], P = 0.046). No episodes of respiratory depression occurred in either group, and discharge satisfaction scores and hospital stay length were comparable between groups (Table 3).
Discussion
Postoperative gastrointestinal dysfunction is common after colorectal surgery and is influenced by multiple factors, including bowel manipulation, postoperative inflammation, inadequate analgesia, and opioid exposure.31,32 In this context, the present findings suggest that an oxycodone-based multimodal regimen may better support early postoperative recovery than a sufentanil-based regimen, particularly with respect to gastrointestinal recovery indicators and visceral pain control. A possible explanation is that oxycodone may provide more favorable coverage of visceral nociception while imposing a lower gastrointestinal burden, thereby helping to reduce the interaction between pain-related stress responses and opioid-related gut dysfunction. Rather than indicating a global improvement in all recovery domains, these benefits appear to be mainly relevant to selected early postoperative recovery dimensions within ERAS-oriented care.
Our findings support the concept that analgesic strategies targeting visceral nociception may translate into tangible gastrointestinal benefits after colorectal surgery. By contrast, μ-selective opioids—while potent for somatic incisional pain—may be less suited to addressing visceral pain and can contribute to enteric hypomotility and emetogenicity.10,11,16 The lack of between-group differences in incisional pain is clinically plausible given the standardized TAP block, which likely equalized somatic pain control.33,34 The lighter early sedation and lower PONV with oxycodone are consistent with an overall opioid-sparing effect (fewer PCIA demands and less remifentanil).28,35,36
Oxycodone’s dual μ/κ-receptor profile provides broad analgesic coverage; κ-receptor activity is particularly relevant for visceral pain and may be less detrimental to gut motility than relying on μ-agonism alone.29,30,37,38 Better suppression of visceral nociceptive input could reduce sympathetic activation and reflex ileus, aligning with the observed advances in first flatus and ambulation.12–17 Additionally, lower remifentanil exposure may mitigate opioid-induced hyperalgesia, further reduce postoperative pain and decrease PCIA requirements.39,40 The reduction in PONV likely reflects both lower overall opioid burden and improved visceral analgesia.41 Because both groups received identical tropisetron prophylaxis in the PCIA solution, the between-group difference in PONV is unlikely to be explained by differential antiemetic exposure. Metoclopramide was used only as rescue treatment. Although it has prokinetic effects that could theoretically influence gastrointestinal recovery, its use was consistent across groups and thus likely represents only a minimal potential confounding factor. However, this finding should not be interpreted as being solely attributable to oxycodone itself; rather, it may reflect the overall differences between the two opioid-based analgesic regimens.
The observed reduction in PONV may be associated with enhanced gastrointestinal recovery. However, the lighter sedation observed in the oxycodone group should not be interpreted as a definitive marker of superior overall recovery. This difference is more likely attributable to the pharmacodynamic distinctions between oxycodone and sufentanil. Furthermore, the opioid-sparing effect achieved in the oxycodone regimen may have contributed to this sedation profile. It is noteworthy that the sedation difference was transient: while significant at the 4-hour assessment, the Ramsay sedation scores showed no statistically significant disparity between the two groups at 12–48 hours postoperatively. This temporally limited pattern further supports the interpretation that early divergence in sedation levels is primarily driven by pharmacodynamic factors rather than by a sustained recovery advantage.
Notably, although the oxycodone-based regimen was associated with faster time to first flatus and earlier ambulation, no significant difference was observed in hospital length of stay between the two groups. This finding is clinically relevant and should be interpreted cautiously. Length of stay is a broader and multifactorial outcome than early gastrointestinal recovery alone, and may be influenced by several factors beyond postoperative analgesic regimen, including surgical complexity, ostomy, postoperative complications, discharge criteria, and institutional perioperative pathways. Therefore, improvement in selected early recovery indicators does not necessarily translate into a shorter hospitalization, particularly in a single-center study with a relatively limited sample size. Our findings should thus be interpreted as suggesting that oxycodone-based multimodal analgesia may improve certain early recovery dimensions relevant to ERAS, rather than demonstrating a broader optimization of all ERAS-related outcomes.
The equianalgesic conversion between intravenous oxycodone and sufentanil remains uncertain in acute postoperative multimodal analgesia. Although the conversion ratio adopted in the present study was derived from available perioperative clinical literature, other literature-based interpretations suggest that intravenous oxycodone may provide relatively greater analgesic potency in some settings.25–30 For example, interpretations such as “intravenous oxycodone’s potency is approximately 1.5–2 times that of morphine” may also be reasonable, although this remains to be further validated in future studies. The present findings should be interpreted as a comparison between two clinically applied multimodal analgesic regimens. Therefore, residual nonequivalence between the two opioid regimens cannot be fully excluded and should be considered when interpreting the observed between-group differences.
From an ERAS perspective, a roughly 5-hour earlier first flatus and 3-hour earlier ambulation are operationally meaningful differences that can streamline care pathways, improve patient comfort and promote the patient’s early recovery. Given the absence of differences in incisional pain, solid-food tolerance, or hospital stay, the primary added value of an oxycodone-centered regimen appears to lie in early visceral analgesia and gastrointestinal recovery, with collateral benefits on PONV and early sedation. These data support considering oxycodone as the core opioid within a multimodal strategy (regional blocks + non-opioids), with dosing reference to lean body mass and routine monitoring for sedation and respiratory safety.
Strengths of this study include the randomized, double-blind design, standardized anesthesia, regional analgesia, and PCIA parameters, as well as consistent findings across subgroups. This study also has several limitations. First, the sample size calculation was based on pilot data for the primary endpoint, time to first flatus. The treatment effect observed in the pilot study was larger than that observed in the full trial, reflecting the instability of effect-size estimates derived from small pilot samples. Although the primary endpoint remained statistically significant, the smaller observed effect implies a risk of type II error for secondary outcomes, infrequent adverse events, and other non-significant endpoints. Consequently, secondary outcomes should be regarded as preliminary and supportive. These outcomes, such as reductions in PONV and analgesic rescue requirements, require confirmation in future multicenter trials with larger patient populations. Second, gastrointestinal recovery was assessed mainly using prespecified early clinical indicators (time to first flatus, time to first ambulation), which are commonly used and ERAS-aligned, but do not fully reflect the multidimensional or mechanistic aspects of postoperative gastrointestinal dysfunction. Objective biomarkers, structured tools such as ultrasonographic peristalsis indices or the I-FEED classification were not included. Similarly, the proposed link between oxycodone’s κ-receptor-related visceral analgesia and improved gastrointestinal recovery remains biologically plausible but indirect. Because time to first flatus was based primarily on patient report, some degree of reporting bias cannot be excluded, despite the use of a standardized recording procedure. Third, this study focused on early postoperative recovery relevant to ERAS, rather than a comprehensive assessment of global recovery quality. Broader recovery domains, including patient-reported well-being, psychological recovery, and overall symptom burden, were not assessed. Long-term outcomes beyond 48 hours—such as chronic pain, bowel function recovery, persistent opioid use, and patient-reported metrics like QoR-15—were also not captured, leaving the duration of oxycodone-related benefits uncertain. Finally, generalizability to populations outside the inclusion criteria (eg, opioid-tolerant patients or those with substantially higher BMI) warrants confirmation.
Future studies should consider larger multicenter trials, broader perioperative variable collection, standardized objective recovery measures, long-term outcomes including chronic pain and quality of global recovery and life, dose-finding studies, and comparative effectiveness against other ERAS-consistent multimodal analgesic regimens.
Conclusion
In this single-center randomized double-blind trial, oxycodone-based multimodal analgesia was associated with faster early gastrointestinal recovery, improved visceral pain control, and fewer opioid-related adverse effects than the sufentanil-based regimen after laparoscopic colorectal cancer surgery. However, these benefits were observed mainly in early postoperative recovery measures within 48 hours and did not translate into a shorter hospital stay. Therefore, these findings support a potential role for oxycodone in ERAS-oriented analgesic selection, while requiring confirmation in larger multicenter studies.
Abbreviations
TAP, Transversus Abdominis Plane; PCIA, Patient-Controlled Intravenous Analgesia; RSS, Ramsay Sedation Scale; PACU, Post-Anesthesia Care Unit; ERAS, Enhanced Recovery after Surgery; PGID, Postoperative Gastrointestinal Dysfunction; PONV, Postoperative Nausea and Vomiting; BMI, Body Mass Index; ASA, American Society of Anesthesiologists; ECG, Electrocardiography; BP, Blood pressure; SpO2, Pulse Oximetry; O, Oxycodone; S, Sufentanil; Hb, Hemoglobin; WBC, White Blood Cell; MAP, Mean Arterial Pressure; HR, Heart Rate; SD, Standard Deviation; CI, Confidence Interval; OR, Odds Ratio.
Data Sharing Statement
The raw data supporting the conclusions of this article are available from the corresponding author, Hao Jiao (Email: [email protected]), upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University. This study was conducted in accordance with the Declaration of Helsinki. The participants provided their written informed consent to participate in this study.
Acknowledgments
The authors extend their sincere gratitude to all study participants for their valuable contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Qunfeng Project of Jiangsu Cancer Hospital (No. DFXK202503). The funder had no role in the study design, data collection, data analysis, interpretation, or writing of this manuscript.
Disclosure
The authors report there are no conflicts of interest in this work.
References
1. Kim SY, Kim NK, Baik SH, et al. Effects of postoperative pain management on immune function after laparoscopic resection of colorectal cancer: a randomized study. Medicine. 2016;95(19):e3602. doi:10.1097/MD.0000000000003602
2. Xu L, Xie F, Zhou H, et al. Clinical application of laparoscopy and laparotomy in the treatment of colorectal cancer and its effect on immune function. Panminerva Med. 2024;66(1):103–13. doi:10.23736/S0031-0808.22.04661-4
3. Mazzotta E, Villalobos-Hernandez EC, Fiorda-Diaz J, Harzman A, Christofi FL. Postoperative ileus and postoperative gastrointestinal tract dysfunction: pathogenic mechanisms and novel treatment strategies beyond colorectal enhanced recovery after surgery protocols. Front Pharmacol. 2020;11:583422. doi:10.3389/fphar.2020.583422
4. Guo M, Liu S, Gao J, Han C, Yang C, Liu C. The effects of fentanyl, oxycodone, and butorphanol on gastrointestinal function in patients undergoing laparoscopic hysterectomy: a prospective, double-blind, randomized controlled trial. BMC Anesthesiol. 2022;22(1):53. doi:10.1186/s12871-022-01594-9
5. Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) society recommendations: 2018. World J Surg. 2019;43(3):659–695. doi:10.1007/s00268-018-4844-y
6. Sjövall S, Kokki M, Kokki H. Laparoscopic surgery: a narrative review of pharmacotherapy in pain management. Drugs. 2015;75(16):1867–1889. doi:10.1007/s40265-015-0482-y
7. Choi GJ, Kang H, Baek CW, Jung YH, Kim DR. Effect of intraperitoneal local anesthetic on pain characteristics after laparoscopic cholecystectomy. World J Gastroenterol. 2015;21(47):13386–13395. doi:10.3748/wjg.v21.i47.13386
8. Johnson AC, Greenwood-Van Meerveld B. The pharmacology of visceral pain. Adv Pharmacol. 2016;75:273–301. doi:10.1016/bs.apha.2015.11.002
9. Stakenborg N, Gomez-Pinilla PJ, Boeckxstaens GE. Postoperative ileus: pathophysiology, current therapeutic approaches. Handb Exp Pharmacol. 2017;239:39–57. doi:10.1007/164_2016_108
10. Hughes PA, Costello SP, Bryant RV, Andrews JM. Opioidergic effects on enteric and sensory nerves in the lower GI tract: basic mechanisms and clinical implications. Am J Physiol Gastrointest Liver Physiol. 2016;311(3):G501–G513. doi:10.1152/ajpgi.00442.2015
11. Castro C, Tharmaratnam U, Brockhurst N, Tureanu L, Tam K, Windrim R. Patient-controlled analgesia with fentanyl provides effective analgesia for second trimester labour: a randomized controlled study. Can J Anaesth. 2003;50(10):1039–1046. doi:10.1007/BF03018370
12. Li Y, Dou Z, Yang L, Wang Q, Ni J, Ma J. Oxycodone versus other opioid analgesics after laparoscopic surgery: a meta-analysis. Eur J Med Res. 2021;26(1):4. doi:10.1186/s40001-020-00463-w
13. Lenz H, Sandvik L, Qvigstad E, Bjerkelund CE, Raeder J. A comparison of intravenous oxycodone and intravenous morphine in patient-controlled postoperative analgesia after laparoscopic hysterectomy. Anesth Analg. 2009;109(4):1279–1283. doi:10.1213/ane.0b013e3181b0f0bb
14. An Y, Zhao L, Wang T, et al. Preemptive oxycodone is superior to equal dose of sufentanil to reduce visceral pain and inflammatory markers after surgery: a randomized controlled trail. BMC Anesthesiol. 2019;19(1):96. doi:10.1186/s12871-019-0775-x
15. Liu X, Hu J, Hu X, et al. Preemptive intravenous nalbuphine for the treatment of post-operative visceral pain: a multicenter, double-blind, placebo-controlled, randomized clinical trial. Pain Ther. 2021;10(2):1155–1169. doi:10.1007/s40122-021-00275-8
16. De Schepper HU, Cremonini F, Park MI, Camilleri M. Opioids and the gut: pharmacology and current clinical experience. Neurogastroenterol Motil. 2004;16(4):383–394. doi:10.1111/j.1365-2982.2004.00513.x
17. Burness CB, Keating GM. Oxycodone/Naloxone prolonged-release: a review of its use in the management of chronic pain while counteracting opioid-induced constipation. Drugs. 2014;74(3):353–375. doi:10.1007/s40265-014-0177-9
18. Cheung CW, Ching Wong SS, Qiu Q, Wang X. Oral oxycodone for acute postoperative pain: a review of clinical trials. Pain Physician. 2017;20(2S):SE33–SE52.
19. Helander EM, Webb MP, Bias M, Whang EE, Kaye AD, Urman RD. A comparison of multimodal analgesic approaches in institutional enhanced recovery after surgery protocols for colorectal surgery: pharmacological agents. J Laparoendosc Adv Surg Tech A. 2017;27(9):903–908. doi:10.1089/lap.2017.0338
20. Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009;144(10):961–969. doi:10.1001/archsurg.2009.170
21. Pirie K, Traer E, Finniss D, Myles PS, Riedel B. Current approaches to acute postoperative pain management after major abdominal surgery: a narrative review and future directions. Br J Anaesth. 2022;129(3):378–393. doi:10.1016/j.bja.2022.05.029
22. Boer P. Estimated lean body mass as an index for normalization of body fluid volumes in humans. Am J Physiol. 1984;247(4 Pt 2):F632–F636. doi:10.1152/ajprenal.1984.247.4.F632
23. Saari TI, Ihmsen H, Neuvonen PJ, Olkkola KT, Schwilden H. Oxycodone clearance is markedly reduced with advancing age: a population pharmacokinetic study. Br J Anaesth. 2012;108(3):491–498. doi:10.1093/bja/aer395
24. Umukoro NN, Aruldhas BW, Rossos R, Pawale D, Renschler JS, Sadhasivam S. Pharmacogenomics of oxycodone: a narrative literature review. Pharmacogenomics. 2021;22(5):275–290. doi:10.2217/pgs-2020-0143
25. Treillet E, Laurent S, Hadjiat Y. Practical management of opioid rotation and equianalgesia. J Pain Res. 2018;11:2587–2601. doi:10.2147/JPR.S170269
26. Chang SH, Maney KM, Phillips JP, Langford RM, Mehta V. A comparison of the respiratory effects of oxycodone versus morphine: a randomised, double-blind, placebo-controlled investigation. Anaesthesia. 2010;65(10):1007–1012. doi:10.1111/j.1365-2044.2010.06498.x
27. Han L, Su Y, Xiong H, et al. Oxycodone versus sufentanil in adult patient-controlled intravenous analgesia after abdominal surgery: a prospective, randomized, double-blinded, multiple-center clinical trial. Medicine. 2018;97(31):e11552. doi:10.1097/MD.0000000000011552
28. Wang Y, Wu M, Zhao L, Yan X, Zhao L. Comparison of the analgesic effects of oxycodone vs. sufentanil on postoperative pain after laparoscopic gallbladder-preserving cholecystolithotomy: a prospective randomized controlled trial. Front Surg. 2024;11:1382759. doi:10.3389/fsurg.2024.1382759
29. Yang GW, Cheng H, Song XY, et al. Effect of oxycodone-based multimodal analgesia on visceral pain after major laparoscopic gastrointestinal surgery: a randomised, double-blind, controlled trial. Drug Des Devel Ther. 2024;18:1799–1810. doi:10.2147/DDDT.S464518
30. Dang SJ, Li RL, Wang J, et al. Oxycodone vs sufentanil in patient-controlled intravenous analgesia after gynecological tumor operation: a randomized double-blind clinical trial. J Pain Res. 2020;13:937–946. doi:10.2147/JPR.S236933
31. Mythen MG. Postoperative gastrointestinal tract dysfunction. Anesth Analg. 2005;100(1):196–204. doi:10.1213/01.ANE.0000139376.45591.17
32. Vather R, O’Grady G, Bissett IP, Dinning PG. Postoperative ileus: mechanisms and future directions for research. Clin Exp Pharmacol Physiol. 2014;41(5):358–370. doi:10.1111/1440-1681.12220
33. Grape S, Kirkham KR, Akiki L, Albrecht E. Transversus abdominis plane block versus local anesthetic wound infiltration for optimal analgesia after laparoscopic cholecystectomy: a systematic review and meta-analysis with trial sequential analysis. J Clin Anesth. 2021;75:110450. doi:10.1016/j.jclinane.2021.110450
34. Oh TK, Lee SJ, Do SH, Song IA. Transversus abdominis plane block using a short-acting local anesthetic for postoperative pain after laparoscopic colorectal surgery: a systematic review and meta-analysis. Surg Endosc. 2018;32(2):545–552. doi:10.1007/s00464-017-5871-8
35. Staahl C, Christrup LL, Andersen SD, Arendt-Nielsen L, Drewes AM. A comparative study of oxycodone and morphine in a multi-modal, tissue-differentiated experimental pain model. Pain. 2006;123(1–2):28–36. doi:10.1016/j.pain.2006.02.006
36. Riley J, Eisenberg E, Müller-Schwefe G, Drewes AM, Arendt-Nielsen L. Oxycodone: a review of its use in the management of pain. Curr Med Res Opin. 2008;24(1):175–192. doi:10.1185/030079908x253708
37. Black D, Trevethick M. The kappa opioid receptor is associated with the perception of visceral pain. Gut. 1998;43(3):312–313. doi:10.1136/gut.43.3.312
38. Kwon YS, Jang JS, Lee NR, et al. A comparison of oxycodone and alfentanil in intravenous patient-controlled analgesia with a time-scheduled decremental infusion after laparoscopic cholecystectomy. Pain Res Manag. 2016;2016:7868152. doi:10.1155/2016/7868152
39. Jin Y, Mao Y, Chen D, et al. Thalamocortical circuits drive remifentanil-induced postoperative hyperalgesia. J Clin Invest. 2022;132(24):e158742. doi:10.1172/JCI158742
40. Fletcher D, Martinez V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth. 2014;112(6):991–1004. doi:10.1093/bja/aeu137
41. Daes J, Morrell DJ, Hanssen A, et al. Paragastric autonomic neural blockade to prevent early visceral pain and associated symptoms after laparoscopic sleeve gastrectomy: a randomized clinical trial. Obes Surg. 2022;32(11):3551–3560. doi:10.1007/s11695-022-06257-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Efficacy of Oxycodone versus Sufentanil for Postoperative Recovery in Patients Receiving Bilateral Modified Thoracoabdominal Nerves Block Through Perichondrial Approach (M-TAPA) Following Laparoscopic Radical Distal Gastrectomy: A Study Protocol for a Prospective, Blinded, Randomized Controlled Trial
Tong J, Cui L, Wei Y, Zhu X, Ma D
Journal of Pain Research 2026, 19:606601
Published Date: 12 June 2026