Back to Journals » Journal of Pain Research » Volume 19
Comparing Efficacy of Oxycodone versus Sufentanil for Postoperative Recovery in Patients Receiving Bilateral Modified Thoracoabdominal Nerves Block Through Perichondrial Approach (M-TAPA) Following Laparoscopic Radical Distal Gastrectomy: A Study Protocol for a Prospective, Blinded, Randomized Controlled Trial
Authors Tong J ![]() , Cui L
, Cui L ![]() , Wei Y, Zhu X, Ma D
, Wei Y, Zhu X, Ma D
Received 5 March 2026
Accepted for publication 4 June 2026
Published 12 June 2026 Volume 2026:19 606601
DOI https://doi.org/10.2147/JPR.S606601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Jiaqi Tong, Lingli Cui, Yueting Wei, Xinyan Zhu, Danxu Ma
Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
Correspondence: Danxu Ma, Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, No. 95 Yong’an Road, Beijing, 100050, People’s Republic of China, Email [email protected]
Introduction: While laparoscopic radical distal gastrectomy (LRDG) has been widely adopted for its minimally invasive benefits in the treatment of gastric cancer, acute postoperative pain, comprising both somatic incisional pain and visceral discomfort, remains a clinical challenge that can affect patients’ perioperative comfort and the rehabilitation process. Consequently, optimizing postoperative analgesic strategies remains essential for enhanced recovery. The modified thoracoabdominal nerves block through a perichondrial approach (M-TAPA) has been introduced as an emerging regional analgesic technique for upper abdominal incisions. In the regard of effective management of visceral pain, oxycodone is a unique agonist at κ-opioid receptors and potentially influences inhibiting visceral nociceptive transmission better than sufentanil. Therefore, this study aims to evaluate whether the combination of M-TAPA with oxycodone-based patient-controlled intravenous analgesia (PCIA) is more effective to provide analgesia efficacy and facilitate gastrointestinal recovery compared to a sufentanil-based analgesic regimen.
Methods/Analysis: This single-center, prospective, double-blind, randomized controlled trial will enroll 96 patients scheduled for elective laparoscopic radical distal gastrectomy. Eligible patients will be randomly assigned at a 1:1 ratio to receive either Oxycodone PCIA (Group O) or Sufentanil PCIA (Group S). Both groups will receive bilateral ultrasound-guided M-TAPA before surgical incision. The primary outcome is the Quality of Recovery-15 (QoR-15) score assessed at 24 hours postoperatively. Secondary outcomes include static and dynamic numeric rating scale (NRS) pain scores, cumulative opioid consumption (converted to intravenous morphine equivalents), clinical recovery milestones, and the incidence of adverse events such as postoperative nausea and vomiting (PONV) and respiratory depression.
Ethics and Dissemination: This trial was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University on August 28, 2025. The trial started recruiting patients after being registered on the Chinese Clinical Trial Registry.
Trial Registration Number: ChiCTR2600119394.
Keywords: abdominal surgery, ultrasound-guided nerve block, oxycodone, sufentanil, multimodal analgesia, visceral pain
Introduction
In Asia (particularly in high-incidence regions such as China, Japan, and South Korea), more than 50% of gastric adenocarcinomas are located in the gastric antrum and the lower third of the gastric body, radical distal gastrectomy is often considered the preferred standard surgical approach.1 With the development of minimally invasive techniques, laparoscopic radical distal gastrectomy (LRDG) has become a primary surgical intervention due to its minimally invasive characteristics, rapid recovery, and lower infection rates.2 Despite these advantages, acute postoperative pain remains a big challenge to patient recovery. Compared with lower abdominal procedures such as colorectal surgery, radical gastrectomy routinely induces a higher intensity of acute postoperative pain and greater analgesic demand due to the extensive dissection of the upper abdominal visceral nerve network (T5–T9) and consistent respiratory-related wound motion.3 Accumulating neurobiological evidence clarifies that severe visceral pain secondary to LRDG induces intensive sympathetic nerve hyperactivation, which clinically culminates in reflex ileus and delayed gastroduodenal motility.4,5 According to Enhanced Recovery After Surgery (ERAS) guidelines, multimodal analgesic regimens that combine regional nerve blocks with Patient-Controlled Intravenous Analgesia (PCIA) are currently recommended. This approach integrates different analgesic mechanisms to achieve synergistic pain relief, thereby reducing opioid consumption and minimizing opioid-related complications such as respiratory depression and ileus. These benefits provide essential support for rapid postoperative recovery of patients undergoing LRDG.
Regional nerve block techniques are a vital component of multimodal analgesia, significantly reducing postoperative pain intensity and opioid requirements via blocking the transmission of pain signal pathways.6 The Modified Thoraco-Abdominal Nerves Block through the Perichondrial Approach (M-TAPA) has emerged as an efficient regional technique, which provides extensive dermatomal coverage for upper abdominal incisions by targeting the anterior and lateral cutaneous branches of the T5–T12 spinal nerves.7 To date, M-TAPA has been successfully applied in various laparoscopic procedures, such as sleeve gastrectomy, hernia repair, and cholecystectomy.8–10 While previous data demonstrate that M-TAPA effectively mitigates somatic incisional pain in various laparoscopic procedures, isolated regional blocks often provide incomplete relief for the visceral pain associated with intraoperative ligamentous traction and postoperative intestinal spasms.11 Consequently, the combination of M-TAPA with PCIA is frequently employed to address the gaps in visceral analgesia and support early mobilization. In current clinical practice, sufentanil-based PCIA is widely used in postoperative IV-PCA practice due to its rapid onset and high analgesic efficacy, and represents a conventional opioid regimen in many Chinese institutions. While it efficiently manages peripheral incisional inputs, its efficacy against deep visceral nociceptive arcs is limited and frequently associated with dose-dependent adverse reactions, such as nausea, vomiting, excessive sedation, and ileus, which can delay gastrointestinal functional recovery.12
In contrast, oxycodone is known to act on opioid receptors, with experimental and clinical evidence suggesting it may offer a relevant analgesic profile in visceral pain models, potentially through pathways associated with κ-opioid receptor modulation.13,14 K-opioid receptors are widely distributed throughout the gastrointestinal axis, the myenteric plexus, as well as the vagus nerve and mesenteric nerve pathways. The ligamentous traction, lymph node dissection, and local ischemia caused by radical gastrectomy can induce severe smooth muscle spasms and visceral pain. By binding to the κ-receptors in these regions, oxycodone may directly inhibit the hypersensitivity of visceral receptors, which might help impede the transmission of visceral nociceptive signals to the spinal dorsal horn.15–18
Although preliminary evidence suggests oxycodone may improve clinical recovery milestones, its comparative efficacy against sufentanil-based PCIA in patients undergoing LRDG remains unclear. Therefore, this design standardizes M-TAPA in both groups to minimize variability in somatic abdominal wall analgesia, allowing the trial to focus on whether the choice of systemic opioid (oxycodone versus sufentanil) affects residual visceral pain and overall quality of recovery.
Materials and Methods
Trial Design
This is a single-center, prospective, randomized, double-blind, controlled clinical trial. The study will be conducted at Beijing Friendship Hospital, Capital Medical University. The protocol follows the SPIRIT guidelines and has been approved by the Institutional Review Board of Beijing Friendship Hospital (Approval No. 2025-P2-373-01). All participants will provide written informed consent and will be randomly assigned to either the sufentanil-based patient-controlled intravenous analgesia (Group S) or the oxycodone-based patient-controlled intravenous analgesia (Group O). The study design is outlined in the trial flowchart (Figure 1).
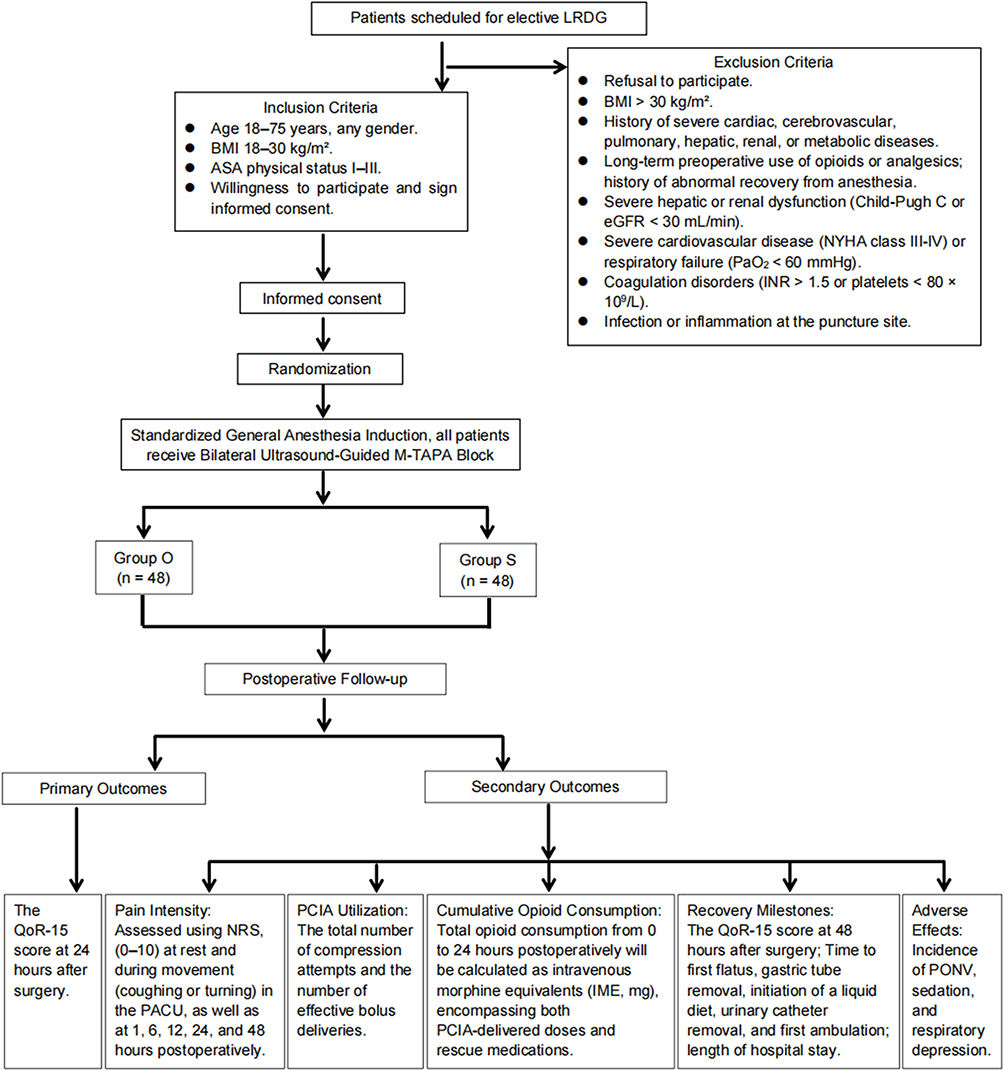 |
Figure 1 Flow-chart of study design. Abbreviations: LRDG, laparoscopic radical distal gastrectomy; BMI, body mass index; eGFR, estimated glomerular filtration rate; INR, international normalized ratio; M-TAPA, the modified thoracoabdominal nerves block through perichondrial approach; QoR-15, the Quality of Recovery-15 scale; NRS, numeric rating scale; PACU, post-anesthesia care unit; PCIA, patient-controlled intravenous analgesia; PONV, postoperative nausea and vomiting. |
Eligibility Criteria
Participants Inclusion Criteria
- Patients scheduled for elective laparoscopic radical distal gastrectomy for gastric malignancy.
- Age 18–75 years, any gender.
- Body Mass Index (BMI) 18–30 kg/m2.
- American Society of Anesthesiologists (ASA) physical status I–III.
- Willingness to participate and sign informed consent.
Exclusion Criteria
- Refusal to participate.
- BMI > 30 kg/m2.
- History of severe cardiac, cerebrovascular, pulmonary, hepatic, renal, or metabolic diseases.
- Long-term preoperative use of opioids or analgesics; history of abnormal recovery from anesthesia.
- Severe hepatic or renal dysfunction (Child-Pugh C or eGFR < 30 mL/min).
- Severe cardiovascular disease (NYHA class III–IV) or respiratory failure (PaO2 < 60 mmHg).
- Coagulation disorders (INR > 1.5 or platelets < 80 × 109/L).
- Infection or inflammation at the puncture site.
Subjects Will Be Withdrawn from the Research if
- They withdraw informed consent for any reason.
- Clinical adverse events or laboratory abnormalities occur that preclude further treatment.
- The subject is found to be ineligible after randomization.
- The patient is lost to follow-up.
- The investigator determines that continuing the trial is not in the patient’s best interest for other medical reasons.
Randomization and Blinding
Eligible patients will be randomly allocated to either the Group O or the Group S in a 1:1 ratio via a computer-generated randomization table. Patients with odd random numbers will be assigned to Group O, while those with even numbers will enter Group S. Allocation concealment will be strictly maintained using sealed, opaque envelopes. On the day of surgery, an independent anesthesia nurse, who is not involved in the subsequent study phases, will open the envelopes and prepare the PCIA pumps. The patients, postoperative follow-up researchers, outcome assessors, and data analysts will all remain blinded to the treatment allocation until the conclusion of the study.
Interventions
Following an 8-hour period of routine fasting, patients will be transferred to the operating room. Standard monitoring will be established immediately upon arrival, including electrocardiography (ECG), non-invasive blood pressure (NIBP), and pulse oximetry (SpO2). Subsequently, under local anesthesia with lidocaine, radial arterial cannulation will be performed to facilitate continuous invasive arterial blood pressure monitoring.
Anesthesia Induction and Maintenance
Anesthesia induction will comprise intravenous administration of midazolam (0.02 mg/kg), etomidate (0.3 mg/kg), sufentanil (0.5 μg/kg), and cisatracurium (0.15 mg/kg). Once tracheal intubation is secured and verified, the patient will be connected to the ventilator for mechanical ventilation. We will employ a lung-protective ventilation regimen by a tidal volume (VT) of 6–8 mL/kg and a fraction of inspired oxygen (FiO2) of 60%. Ventilatory parameters will be adjusted to maintain end-tidal carbon dioxide (EtCO2) within a range of 35–45 mmHg.
Anesthesia maintenance will be achieved through the continuous infusion of propofol (4–5 mg/kg/h) and remifentanil (0.2 μg/kg/h), with supplemental boluses of cisatracurium administered as needed. Dosage adjustments will be titrated to target a BIS value of 45–55 and ensure hemodynamic fluctuations remain within 20% of the pre-anesthetic baseline.
Intraoperative Analgesia: Ultrasound-Guided M-TAPA Block
Following induction, all patients will receive bilateral ultrasound-guided M-TAPA blocks. A high-frequency (8–13MHz) linear transducer, protected by a sterile sleeve, will be placed in the sagittal direction between the 9th and the 10th costal margins to identify the external oblique, internal oblique and transversus abdominis muscles. Using an in-plane technique, the needle will be advanced toward the target space between the undersurface of the costal cartilage and the transversus abdominis muscle.19 After confirming needle tip placement via hydro-dissection with 2 mL of normal saline, 30 mL of 0.25% ropivacaine will be injected on each side.
Postoperative Analgesia
Approximately 30 minutes before the end of surgery, 50 mg flurbiprofen axetil will be administered intravenously, accompanied by 5 mg tropisetron for postoperative nausea and vomiting (PONV) prophylaxis. Upon completion of the procedure, residual neuromuscular blockade will be reversed with neostigmine (0.05 mg/kg) and atropine (0.01 mg/kg). Tracheal extubation will be performed once the patient is fully awake with adequate spontaneous respiration. Before leaving the operating room, the PCIA pump will be connected:
- Group O: Oxycodone 0.8 mg/kg and ondansetron 8 mg in 0.9% sodium chloride of 100 mL.
- Group S: Sufentanil 2 μg/kg and ondansetron 8 mg in 0.9% sodium chloride of 100 mL.
Pump Settings (Both Groups): Background infusion 0 mL/h, bolus dose 2 mL, lockout interval 10 min.
Upon transfer to the post-anesthesia care unit (PACU), patients’ NRS scores will be monitored by anesthesia nurse at 10-minute intervals. If the NRS score remain ≥ 4 despite PCIA, rescue analgesia will be initiated: 5 mg oxycodone for Group O or 5 μg sufentanil for Group S. Discharge from the PACU will be permitted only when the NRS < 4 and the Aldrete score > 9.
Following return to the ward, routine analgesia will consist of PCIA supplemented by flurbiprofen axetil (50 mg, twice daily). If the resting pain remains moderate-to-severe (NRS > 3) after an effective PCIA bolus, 10 mg of morphine will be administered as remedial analgesia.
Relevant Complications of Management During Anesthesia
Vasoactive medications will be administered as needed to maintain hemodynamic stability. If the intraoperative mean arterial pressure (MAP) drops below 60 mmHg or decreases by > 20% of the baseline value (defined as an MAP 5 minutes prior to induction), 6 mg of ephedrine or 10 μg of norepinephrine will be given while maintaining adequate anesthetic depth. If the MAP exceeds the baseline by > 20%, 10 mg of urapidil will be injected intravenously. 0.5 mg of atropine will be administered for bradycardia (HR < 50 bpm), while 0.5 mg/kg of esmolol will be utilized for tachycardia (HR > 100 bpm). These doses may be repeated as clinically necessary.
Outcome Measures
Primary Outcome Measure
The 15-item recovery quality scale at 24 hours after surgery (global score Quality of Recovery-15 scale, QoR-15).20
Secondary Outcomes Measures
- Pain Intensity: Assessed using the Numeric Rating Scale (NRS, 0–10) at rest and during movement (coughing or turning) in the PACU, as well as at 1, 6, 12, 24, and 48 hours postoperatively;
- PCIA Utilization: The total number of compressions attempts and the number of effective bolus deliveries;
- Cumulative Opioid Consumption: Total opioid consumption from 0 to 24 hours postoperatively will be calculated as intravenous morphine equivalents (IME, mg), encompassing both PCIA-delivered doses and rescue medications.
- Recovery Milestones: QoR-15 score at 48 hours post-surgery; Time to first flatus, gastric tube removal, initiation of a liquid diet, urinary catheter removal, and first ambulation; length of hospital stay.
- Adverse Effects: Incidence of PONV, sedation, and respiratory depression.
Statistical Analysis and Sample Size Calculation
Statistical analyses will be performed using SPSS (Version 26.0). We will strictly adhere to the Intent-to-Treat (ITT) principle; all randomized participants will be analyzed according to their original group assignment to provide an unbiased estimate of the treatment effect. For the primary outcome, missing data will be primarily addressed using multiple imputation to minimize potential bias. The normality of continuous data will be assessed using the Shapiro–Wilk test. Normally distributed data will be presented as mean (standard deviation, SD) and analyzed using the independent samples t-test. Non-normally distributed data will be expressed as medians (interquartile range, IQR) and compared using the Mann–Whitney U-test. The primary outcome (QoR-15 score) will be analyzed using the appropriate test based on its distribution, as described above. Categorical Variables such as the incidence of adverse events presented as frequencies and percentages and comparisons between groups will be conducted using the Chi-square test or Fisher’s exact test, as appropriate. For longitudinal data, such as NRS pain scores recorded at multiple postoperative intervals, a mixed-effects model for repeated measures (MMRM) or a generalized estimating equation (GEE) will be employed to account for the correlation between time points. A two-tailed P < 0.05 will be considered statistically significant for all tests.
The primary outcome of this study will be the QoR-15 score at 24 hours postoperatively. Based on prior literature and our pilot study results, the minimal clinically important difference (MCID) for the QoR-15 is approximately 8 points; thus, a difference of Δ=8 will be defined as the minimum meaningful difference between the two groups.21 Although pilot studies calculated a standard deviation (SD) of roughly 8, the SD for major surgery typically ranges from 10 to 16. To ensure adequate power, a conservative SD of 13 will be utilized for our calculation. Using an online statistical tool (https://www.trialstats.com/statbox/), with a two-sided significance level (α) of 0.05 and a power of 80% (β= 0.20), a sample size of 43 patients per group is required. Accounting for a 10% dropout rate, we will enroll 48 patients per group, resulting in a total sample size of 96.
Ethical Considerations, Amendments and Dissemination
The study will be conducted in strict accordance with the Declaration of Helsinki. All pharmacological agents utilized in this protocol, including oxycodone and sufentanil, are administered within their approved clinical indications for postoperative analgesia.22,23 Furthermore, the M-TAPA block is an established regional anesthetic technique documented in similar surgical populations.8–10 Written informed consent will be obtained from all eligible participants by a trained investigator after a comprehensive explanation of this study. Participants will be explicitly informed of their right to withdraw from the trial at any stage without providing a justification and without any influence in their subsequent medical care. Patient confidentiality will be rigorously maintained; all personal identifiers will be removed, and data will be stored in a password-protected database accessible only to the primary research team.
Any modifications to the study protocol will be formally submitted to the Ethics Committee of Beijing Friendship Hospital for review and approval. Once approved, these amendments will be updated in the Chinese Clinical Trial Registry and communicated to all investigators involved in the trial. All changes will be documented and reported in the final study report. The findings of this clinical trial will be disseminated through publication in peer-reviewed journals. Following the primary publication, de-identified individual participant data and the full study protocol may be shared upon reasonable request to promote scientific transparency and collaborative research.
Trial Status
The trial protocol has been approved by the Beijing Friendship Hospital Ethics Committee (No. 2025-P2-373-01; August 28, 2025). The study has been registered in the Chinese Clinical Trial Registry (ChiCTR2600119394) before the start of patient recruitment. Patient recruitment is scheduled to commence in March 2026 and is projected to conclude in March 2027. Written informed consent will be obtained from all participants before enrollment.
Discussion
Within the framework of ERAS, the goal of postoperative analgesia is no longer confined to achieving “resting painlessness”. Modern perioperative management attaches great importance to minimal sedation, early mobilization, accelerated resumption of oral intake, and the prevention of postoperative ileus. For patients undergoing gastric surgery, selecting an optimal analgesic strategy is essential, as the quality of recovery directly influences the incidence of perioperative complications.
Epidural analgesia has long served as a traditional first-line adjunct for abdominal surgery, but its application is often limited by a high incidence of side effects and contraindications, such as the anticoagulants use or coagulation disorders.24 Regional nerve blocks are now a cornerstone of multimodal strategies, becoming increasingly popular across various surgical disciplines.6 For LRDG, subcostal or oblique subcostal transversus abdominis plane blocks (TAPB) are frequently employed. TAPB, however, primarily targets the anterior cutaneous branches and often fails to provide adequate coverage for the lateral cutaneous branches, which may result in inadequate analgesia at lateral trocar sites.25 By contrast, the M-TAPA effectively infiltrates the anterior and lateral cutaneous branches of the T5–T12 spinal nerves, requiring only a single-point injection beneath the costal cartilage to enable sufficient cephalad spread of the given anesthetic volume. This comprehensive “hemispherical” abdominal wall analgesia covers both the midline incision and lateral trocar ports, thereby mitigating somatic incisional pain.26 Compared to the complex four-point injection of subcostal TAPB, M-TAPA offers a standardized, ultrasound-visible landmark (the costal cartilage), making it a simpler and more efficient option for upper abdominal surgery.
The postoperative pain of LRDG is complex, consisting of both somatic incisional pain and visceral pain. Specifically, the surgical incisions and trocar sites of LRDG are mostly located in the subxiphoid and upper abdominal regions. Because these anatomical areas are closely related to respiratory movement, patients often suffer from high-frequency, dynamic pain caused by incisional traction during breathing and coughing. Furthermore, LRDG also causes intense visceral pain due to extensive internal surgical trauma. The stomach, along with its surrounding omentum and ligamentous attachments, is densely innervated by vagal afferents and greater splanchnic nerves (T5–T9). Surgical maneuvers integral to LRDG including comprehensive D2 lymphadenectomy, major vascular skeletonization, and gastrointestinal reconstruction (eg, Roux-en-Y or Billroth anastomoses), can cause widespread nerve injury and mechanical injury. After surgery, local tissue ischemia, edema, and frequent smooth muscle spasms at the anastomosis site continuously stimulate the mechanoreceptors in the visceral wall.27
Although the M-TAPA block provides extensive dermatomal coverage for the abdominal wall, its capacity to alleviate deeper visceral components remains limited. Therefore, it is necessary to incorporate a systemic analgesic strategy via PCIA to provide comprehensive pain management. Sufentanil is a pure μ-opioid receptor agonist and is widely used for PCIA. However, it exhibits limited efficacy in modulating visceral pain and frequently associated with dose-dependent adverse events, delaying bowel function.
In contrast, oxycodone is a dual μ- and κ-opioid receptor agonist, has been proposed as a theoretically advantageous alternative for visceral pain management.13 It not only interacts with central μ-opioid receptors to reduce somatic pain but also is suggested to activate κ-opioid receptors widely distributed in the gastrointestinal axis, myenteric plexus, and visceral afferent nerve endings.28 By potentially limiting calcium influx via κ-receptors, the drug might lessen the deep discomfort caused by gastrointestinal spasms and mesenteric traction.14,28 Reducing this visceral input could also help decrease the sympathetic hyperactivity associated with surgical trauma.29,30 Furthermore, surgical tissue damage typically triggers a local inflammatory response, releasing factors like PGE2 and TNF-α that contribute to peripheral sensitization. Oxycodone may lower the expression levels of serum substance P and related pro-inflammatory cytokines, which might help lower the sensitivity of peripheral nociceptors and manage inflammation-associated pain.31 Following intravenous administration, oxycodone can cross the blood–brain barrier relatively quickly without depending on active transport proteins like P-glycoprotein, which is associated with a steady and rapid onset of action in the central nervous system.32 Beyond physiological analgesia, oxycodone has been shown to modulate the limbic system, specifically the amygdala, to reduce anxiety behaviors.33 Consequently, we hypothesize that oxycodone may present more suitable pharmacological profile for patients undergoing gastric surgery, potentially reducing both the physical and emotional distress caused by visceral stimulation.
The QoR-15 scale, which assesses physical comfort, pain, independence, psychological support, and emotional state, is a validated and reliable tool for evaluating whether the choice between these two systemic opioid regimens translates into differences in the overall quality of recovery.20,34,35 While prior research in other surgical models suggests that oxycodone may be associated with a lower incidence of severe respiratory depression and faster gastrointestinal rehabilitation, its specific impact when combined with an M-TAPA block for LRDG remains to be rigorously evaluated.36
By targeting different pain transmission pathways, the results of this trial are intended to clarify whether refining the choice of systemic opioid within a multimodal framework can further optimize the postoperative recovery process for patients undergoing LRDG.
Abbreviations
LRDG, laparoscopic radical distal gastrectomy; M-TAPA, the modified thoracoabdominal nerves block through perichondrial approach; PCIA, patient-controlled intravenous analgesia; GI, gastrointestinal; QoR-15, the Quality of Recovery-15; NRS, Numeric Rating Scale; PONV, postoperative nausea and vomiting; ERAS, enhanced recovery after surgery; BMI, body mass index; ASA, American Society of Anesthesiologists; ECG, electrocardiography; NIBP, non-invasive blood pressure; SpO2, pulse oximetry; VT, tidal volume; FiO2, fraction of inspired oxygen; EtCO2, end-tidal carbon dioxide; PACU, post-anesthesia care unit; MAP, mean arterial pressure; IME, intravenous morphine equivalents; ITT, Intent-to-Treat.
Data Sharing Statement
All data used or analyzed in this study can be obtained from the corresponding author (Email: [email protected]).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Wutong Ankang – Medical Research Program for Pain Comfortable Care of the Bethune Charitable Foundation (BCF) (J202502E054-A02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Japanese Gastric Cancer Association jgca@ koto. kpu-m. ac. jp. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. 2021;24(1):1–10. doi:10.1007/s10120-020-01042-y
2. Duda M, Dusek L, Jinek T, Adamcik L, Skrovina M. Stav chirurgicke lecby karcinomu zaludku a gastroezofagealni junkce v Ceske republice [Current state of surgical treatment of cancer of the stomach and gastro-esophageal junction in the Czech Republic]. Rozhl Chir. 2018;97(7):309–319.
3. Mimica Z, Pogorelić Z, Perko Z, Srsen D, Stipić R, Dujmović D. Effect of surgical incision on pain and respiratory function after abdominal surgery: a randomized clinical trial. Hepatogastroenterology. 2007;54(80):2216–2220.
4. Rychter J, Clavé P. Intestinal inflammation in postoperative ileus: pathogenesis and therapeutic targets. Gut. 2013;62(11):1534–1535. doi:10.1136/gutjnl-2012-304176
5. Zhou Y, Yin ZH, Sun MS, et al. Global research trends in postoperative ileus from 2011 to 2023: a scientometric study. World J Gastrointest Surg. 2024;16(9):3020–3031. doi:10.4240/wjgs.v16.i9.3020
6. Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: a review. JAMA Surg. 2017;152(7):691–697. doi:10.1001/jamasurg.2017.0898
7. Tulgar S, Selvi O, Thomas DT, Deveci U, Özer Z. Modified thoracoabdominal nerves block through perichondrial approach (M-TAPA) provides effective analgesia in abdominal surgery and is a choice for opioid sparing anesthesia. J Clin Anesth. 2019;55:109. doi:10.1016/j.jclinane.2019.01.003
8. Güngör H, Ciftci B, Alver S, Gölboyu BE, Ozdenkaya Y, Tulgar S. Modified thoracoabdominal nerve block through perichondrial approach (M-TAPA) vs local infiltration for pain management after laparoscopic cholecystectomy surgery: a randomized study. J Anesth. 2023;37(2):254–260. doi:10.1007/s00540-022-03158-0
9. Alver S, Ciftci B, Güngör H, et al. Efficacy of modified thoracoabdominal nerve block through perichondrial approach following laparoscopic inguinal hernia repair surgery: a randomized controlled trial. Braz J Anesthesiol. 2023;73(5):595–602. doi:10.1016/j.bjane.2023.05.001
10. de Oliveira E, De Lima RC, Sakata RK, et al. Modified thoracoabdominal nerve block through the perichondral approach (M-TAPA) in laparoscopic sleeve gastroplasty: a case series. Obes Surg. 2022;32(1):197–201. doi:10.1007/s11695-021-05612-6
11. Lohmöller K, Carstensen V, Pogatzki-Zahn EM, Freys SM, Weibel S, Schnabel A. Regional anaesthesia for postoperative pain management following laparoscopic, visceral, non-oncological surgery a systematic review and meta-analysis. Surg Endosc. 2024;38(4):1844–1866. doi:10.1007/s00464-023-10667-w
12. Gan TJ, Robinson SB, Oderda GM, Scranton R, Pepin J, Ramamoorthy S. Impact of postsurgical opioid use and ileus on economic outcomes in gastrointestinal surgeries. Curr Med Res Opin. 2015;31(4):677–686. doi:10.1185/03007995.2015.1005833
13. Kokki H, Kokki M, Sjövall S. Oxycodone for the treatment of postoperative pain. Expert Opin Pharmacother. 2012;13(7):1045–1058. doi:10.1517/14656566.2012.677823
14. Davis MP. Drug management of visceral pain: concepts from basic research. Pain Res Treat. 2012;2012:265605. doi:10.1155/2012/265605
15. Liguori S, Gottardi M, Micheletto G, Bruno L. Pharmacological approach to chronic visceral pain. Focus on oxycodone controlled release: an open multicentric study. Eur Rev Med Pharmacol Sci. 2010;14(3):185–190.
16. Olesen AE, Staahl C, Arendt-Nielsen L, Drewes AM. Different effects of morphine and oxycodone in experimentally evoked hyperalgesia: a human translational study. Br J Clin Pharmacol. 2010;70(2):189–200. doi:10.1111/j.1365-2125.2010.03700.x
17. Ruan X, Mancuso KF, Kaye AD. Revisiting oxycodone analgesia: a review and hypothesis. Anesthesiol Clin. 2017;35(2):e163–e174. doi:10.1016/j.anclin.2017.01.022
18. Staahl C, Christrup LL, Andersen SD, Arendt-Nielsen L, Drewes AM. A comparative study of oxycodone and morphine in a multi-modal, tissue-differentiated experimental pain model. Pain. 2006;123(1–2):28–36. doi:10.1016/j.pain.2006.02.006
19. Ari DE, Ar AY, Karip CS, et al. Ultrasound-guided subcostal-posterior transversus abdominis plane block for pain control following laparoscopic sleeve gastrectomy. Saudi Med J. 2017;38(12):1224–1229. doi:10.15537/smj.2017.12.21133
20. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
21. Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, Dennis A. Minimal clinically important difference for three quality of recovery scales. Anesthesiology. 2016;125(1):39–45. doi:10.1097/aln.0000000000001158
22. Dong P, Qu X, Yang Y, Li X, Wang C. Effect of oxycodone versus fentanyl for patient-controlled intravenous analgesia after laparoscopic hysteromyomectomy: a single-blind, randomized controlled trial. Sci Rep. 2024;14(1):20478. doi:10.1038/s41598-024-71708-5
23. Zhou Y, Huang X, Chang H, et al. The optimal dose of oxycodone in PCIA after laparoscopic surgery for gastrointestinal cancer in elderly patients: a randomized controlled trial. Front Surg. 2023;10:1111376. doi:10.3389/fsurg.2023.1111376
24. Gadsden JC, Lindenmuth DM, Hadzic A, Xu D, Somasundarum L, Flisinski KA. Lumbar plexus block using high-pressure injection leads to contralateral and epidural spread. Anesthesiology. 2008;109(4):683–688. doi:10.1097/ALN.0b013e31818631a7
25. Ma N, Duncan JK, Scarfe AJ, Schuhmann S, Cameron AL. Clinical safety and effectiveness of transversus abdominis plane (TAP) block in post-operative analgesia: a systematic review and meta-analysis. J Anesth. 2017;31(3):432–452. doi:10.1007/s00540-017-2323-5
26. Turunc E, Dost B, Sarikaya Ozel E, et al. Bilateral ultrasound-guided external oblique intercostal block vs. modified thoracoabdominal nerve block through perichondrial approach for postoperative analgesia in patients undergoing laparoscopic sleeve gastrectomy surgery: a randomized controlled study. Obes Surg. 2024;34(10):3726–3734. doi:10.1007/s11695-024-07454-4
27. Sengupta JN. Visceral pain: the neurophysiological mechanism. Handb Exp Pharmacol. 2009;(194):31–74. doi:10.1007/978-3-540-79090-7_2
28. Koh JC, Kong HJ, Kim MH, et al. Comparison of analgesic and adverse effects of oxycodone- and fentanyl-based patient-controlled analgesia in patients undergoing robot-assisted laparoscopic gastrectomy using a 55:1 potency ratio of oxycodone to fentanyl: a retrospective study. J Pain Res. 2020;13:2197–2204. doi:10.2147/jpr.S264764
29. García-Domínguez M. κ-opioid receptor agonists as robust pain-modulating agents: mechanisms and therapeutic potential in pain modulation. J Clin Med. 2025;14(20). doi:10.3390/jcm14207263
30. An Y, Zhao L, Wang T, et al. Preemptive oxycodone is superior to equal dose of sufentanil to reduce visceral pain and inflammatory markers after surgery: a randomized controlled trail. BMC Anesthesiol. 2019;19(1):96. doi:10.1186/s12871-019-0775-x
31. Lao WL, Song QL, Jiang ZM, Chen WD, Zheng XH, Chen ZH. The effect of oxycodone on post-operative pain and inflammatory cytokine release in elderly patients undergoing laparoscopic gastrectomy. Front Med Lausanne. 2021;8:700025. doi:10.3389/fmed.2021.700025
32. Bällgren F, Hammarlund-Udenaes M, Loryan I. Active uptake of oxycodone at both the blood-cerebrospinal fluid barrier and the blood-brain barrier without sex differences: a rat microdialysis study. Pharm Res. 2023;40(11):2715–2730. doi:10.1007/s11095-023-03583-0
33. Bruijnzeel AW, Behnood-Rod A, Malphurs W, et al. Oxycodone decreases anxiety-like behavior in the elevated plus-maze test in male and female rats. Behav Pharmacol. 2022;33(6):418–426. doi:10.1097/fbp.0000000000000690
34. Bu XS, Zhang J, Zuo YX. Validation of the Chinese version of the quality of recovery-15 score and its comparison with the post-operative quality recovery scale. Patient. 2016;9(3):251–259. doi:10.1007/s40271-015-0148-6
35. Myles PS, Shulman MA, Reilly J, Kasza J, Romero L. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. Br J Anaesth. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
36. Hellinga M, Algera MH, Olofsen E, et al. Oral oxycodone-induced respiratory depression during normocapnia and hypercapnia: a pharmacokinetic-pharmacodynamic modeling study. Clin Pharmacol Ther. 2023;113(5):1080–1088. doi:10.1002/cpt.2863
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Oxycodone versus Sufentanil-Based Intravenous Patient-Controlled Multimodal Analgesia on Early Gastrointestinal Recovery and Pain After Laparoscopic Colorectal Cancer Surgery: A Randomized Double-Blind Trial
Jia W, Wang Z, Lin Y, Yao X, Sheng X, Zhou Y, Xu C, Liu Y, Jiao H
Journal of Pain Research 2026, 19:591268
Published Date: 14 April 2026