Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Effects of Nutritional Interventions in Individuals with Chronic Obstructive Lung Disease: A Systematic Review of Randomized Controlled Trials
Authors Furulund E, Bemanian M, Berggren N, Madebo T, Rivedal SH, Lid TG ![]() , Fadnes LT
, Fadnes LT ![]()
Received 11 June 2021
Accepted for publication 27 September 2021
Published 17 November 2021 Volume 2021:16 Pages 3145—3156
DOI https://doi.org/10.2147/COPD.S323736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Einar Furulund,1– 3 Mitra Bemanian,2,3 Nina Berggren,3 Tesfaye Madebo,2,4 Sara Hydle Rivedal,3 Torgeir Gilje Lid,1,5 Lars Thore Fadnes2,3
1Centre for Alcohol and Drug Research, Stavanger University Hospital, Stavanger, Norway; 2Bergen Addiction Research, Department of Addiction Medicine, Haukeland University Hospital, Bergen, Norway; 3Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway; 4Department of Respiratory Medicine, Stavanger University Hospital, Stavanger, Norway; 5Department of Public Health, University of Stavanger, Stavanger, Norway
Correspondence: Einar Furulund
Centre for Alcohol and Drug Research, Stavanger University Hospital, Stavanger, Norway
Tel +4751518000
Email [email protected]
Background: The role of nutrition and dietary patterns has been widely investigated in cancer, cardiovascular disease, and diabetes, but there are limited data on nutritional impact on COPD. This systematic review (PROSPERO-reg. no: CRD42020172712) aimed to investigate the effect of nutritional interventions on pulmonary and physical function, inflammation, and health-related quality of life among individuals with COPD.
Methods: Systematic searches were conducted in Medline, Embase, and Cochrane, resulting in 3861 references. Studies focusing exclusively on inpatient-stays, underweight or obese patients were excluded. Double screening, extraction and bias assessment were conducted. Bias was assessed according to the Cochrane risk of bias tool for randomized controlled trials. Thirteen randomized controlled trials with 916 participants were included.
Results: These trials investigated effects of protein supplementation, beetroot juice, increased fruit and vegetable intake, black seed oil, Tualang honey, Chlorella vulgaris-extract, whey-peptide containing nutritional drink, and increased macronutrient intake. The durations of the interventions were from weeks to a few months, and only one with duration > 1 year (investigating increased fruit/vegetable intake). The intervention increasing fruit/vegetables found improvement in pulmonary function tests. Some interventions observed effects on systemic inflammation, health-related quality of life and physical function, although with some mixed results. Five were classified as poor, five as fair, and three as good in terms of risk of bias and quality.
Conclusion: Increasing intake of fruits and vegetables over prolonged periods might have positive effects on lung function in individuals with COPD. Some nutritional interventions also observed effects on systemic inflammation, health-related quality of life, and physical function, although with some mixed results. Many of the trials were underpowered, had high dropout rates, or had a high risk of bias. Further research should investigate effect of prolonged dietary interventions.
Keywords: nutrition, lung function, inflammation, physical function, health-related quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) currently affects 250 million people worldwide, and the numbers are rising.1,2 COPD is a disease that progressively reduces daily functioning and quality of life, and is associated with frequent hospitalizations and high costs to healthcare systems.2 There is research supporting the concept that body composition can influence disease progression and outcomes in COPD, and it is known that both underweight and obesity impact pulmonary function negatively.3,4 COPD is associated with the development of malnutrition and muscle wasting, which in turn affects exercise capacity and quality of life negatively, and increases mortality.5,6 Overweight and obesity are also associated with worse outcomes in COPD, including more severe dyspnea, reduced daily functioning, and more severe exacerbations.3 This bi-faceted association of COPD with body composition raises the question of whether diet and nutrition play a role in the development, progression – and treatment – of the disease.
The role of nutrition and diet in relation to cancer, cardiovascular disease, and diabetes has been widely investigated, but less is known about the role of nutrition in the development, progression, and treatment of COPD.7 Observational studies have shown favorable associations of antioxidant-rich diets high in fruits, vegetables, and nuts reducing the risk of developing COPD.8–10 In contrast, a Western diet rich in processed foods, red meat and sugared soft drinks, has been associated with increased risk of developing COPD.10–12 Two meta-analyses published in 2012 presented evidence on the beneficial effect of nutritional interventions for increasing dietary intake and reducing wasting of muscles in people with COPD, especially for those already malnourished.13,14 The evidence on pulmonary function, physical capacity, inflammation and related health aspects at that point, was less consistent. Moreover, the evidence on nutritional interventions aimed at non-malnourished COPD patients is less studied systematically. Except for a recent systematic review focusing mainly on nutritional interventions during pulmonary rehabilitation15 and a systematic review and meta-analysis on vitamin D supplementation for reducing exacerbation rates,16 no updated systematic reviews have been published.13 This review will investigate the effect of oral nutritional interventions beyond single micronutrients on pulmonary function, physical function, and lung-related inflammation of individuals with stable COPD.
Materials and Methods
This article aimed to identify all relevant randomized controlled trials on nutritional interventions in individuals living with COPD. Before conducting this literature search, a review protocol was developed according to PRISMA guidelines,17 and registered in PROSPERO (registration number: CRD42020172712).
Information Sources and Search Strategy
The articles were identified using a systematic search strategy in the database Medline (via PubMed), Embase (via Ovid) and Cochrane. Free-text terms, as well as MeSH-terms, were used in both databases. No study design, data, or language limits were imposed on the search. Exposure search terms were combined with population/outcome search terms. Search terms used in Medline were as follows:
- Exposure terms: food, phytochemicals, antioxidants, vegetable, fruit, nuts, protein, amino acid, fatty acid, micronutrient, vitamins, minerals, carbohydrate, diet, nutrition, nutrition therapy, fiber, omega and probiotic.
- Population/outcome terms: pulmonary disease, chronic obstructive, respiratory function, obstructive lung disease, COPD, exacerbations, spirometry, lung function and inflammatory markers.
A detailed search string is available in the Supplementary File. The search was conducted on August 31st, 2021 (see further details in Supplementary Text S1–S4). A university librarian from University of Bergen with special knowledge on search strategy contributed to the search.
Study Eligibility and Selection Process
Two authors (EF & MB) independently screened the titles and abstracts for eligible studies. Articles were considered eligible for this review if they were randomized controlled trials on individuals with COPD. Only orally administered and non-micronutrient based nutritional interventions were included. As a recent systematic review and meta-analysis on vitamin D supplementation has been published, data on vitamin D and other micronutrients were not included in our review.16 Outcomes assessed included measures of pulmonary function, physical function, health-related quality of life, and inflammatory markers (see Table 1). We excluded studies taking place exclusively in hospital settings, with a duration of less than 7 days, or exclusively presenting data for malnourished or obese subjects (body mass index [BMI] < 18.5 or > 30 kg/m2). After importing eligible full-text references to Endnote, the two authors (EF & MB) continued the selection process individually if articles satisfied the inclusion criteria. Finally, discrepancies in selecting articles were discussed and agreed upon through consensus between the authors.
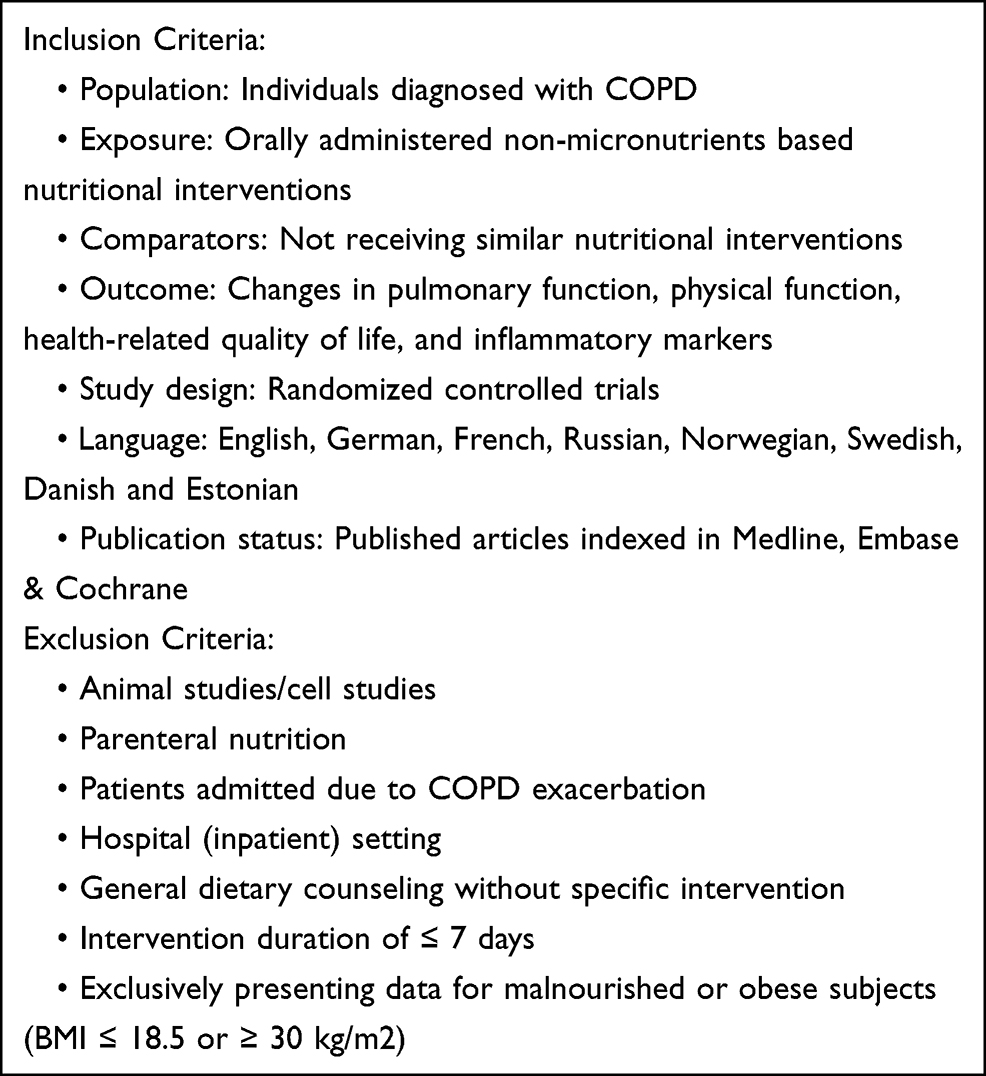 |
Table 1 Inclusion and Exclusion Criteria |
Data Extraction, Risk of Bias Assessment, and Data Synthesis
Information regarding design, population, exposure, duration, outcome measures, and results were extracted based on the established criteria (see Table 1) from the included articles. Table 1 shows the PICO criteria structure for the inclusion of studies. Both absolute and relative effect measures were of interest. Absolute values are presented in an extended table (Supplementary Table S2), whereas relative measures are presented in-text. For the in-text presentation, MB & EF calculated percentage change in outcomes whenever possible and practical, and not already presented in original papers. Approximations (~) were given whenever the extraction was based on graphical presentations.
The data extraction from the search was performed individually by EF & MB. The complete summarized data extraction presented in this article was completed by EF & MB. According to the Cochrane risk of bias tool for randomized controlled trials, all articles were evaluated with a risk of bias assessment from EF & MB.18 In short, this assessed whether sequence generation was random, concealment of allocation, risk of selective reporting, other bias, blinding of participants and personnel, blinding of outcome assessment, risk of incomplete outcome data, and evaluated overall quality. In case of uncertainty in the assessment, articles were discussed in detail with senior co-authors until reaching consensus. This review aimed to summarize and report the current evidence on nutritional intervention in individuals with COPD. There was an insufficient number of studies with overlapping exposures, outcomes, and population groups, thus, a meta-analysis could not be performed. Thirteen articles met the inclusion criteria from the search strategy. Our discussion focuses on all articles, not only articles with low bias assessment when the nature of nutritional intervention may cause difficulties in randomization and or blinding, and therefore receive a higher risk of bias.
Results
Selection Process and Characteristics of Included Studies
The search included 3861 references from Embase, Medline, and Cochrane. Twenty-seven articles were assessed in full-text, and of these, thirteen were considered eligible for review. The selection process and reasons for exclusion are presented in Figure 1, PRISMA flow-diagram.
 |
Figure 1 PRISMA flow diagram. Notes: PRISMA figure adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta- Analyses: The PRISMA Statement. PLoS Med 6(7):e1000097. Creative Commons.17 For more information, visit www.prisma-statement.org. |
In total, 916 participants in the 13 articles were included in this review. Extracted data are summarized in Table 2 (and an extended version is included as a Supplementary File: Table S2). The following interventions were studied in the included trials: protein supplementation,19 beetroot juice,20–22 increased fruit and vegetable intake,23,24 black seed oil,25 Tualang honey,26 Chlorella vulgaris extract,27 whey-peptide containing nutritional drink,28 and finally increased macronutrient intake.29–31 All participants were adults with COPD, mostly aged 40 years and above. Five studies included physical activity interventions, although participants in the intervention groups and control groups were treated equally except differences in nutritional interventions.19,22,28,29,31 Using the Cochrane risk of bias tool, in terms of risk of bias and quality, five studies were classified as poor,19,21,25,27,28 five were classified as fair,23,24,26,29,31 and three were classified as good20,22,30 (Supplementary Table S1). Examining all thirteen articles with bias assessment, nutritional interventions often have inherent challenges related to blinding. Five studies scored high on the assessment category of blinding of participants and personnel. This impacts on the quality grade within the Cochrane risk of bias assessment.
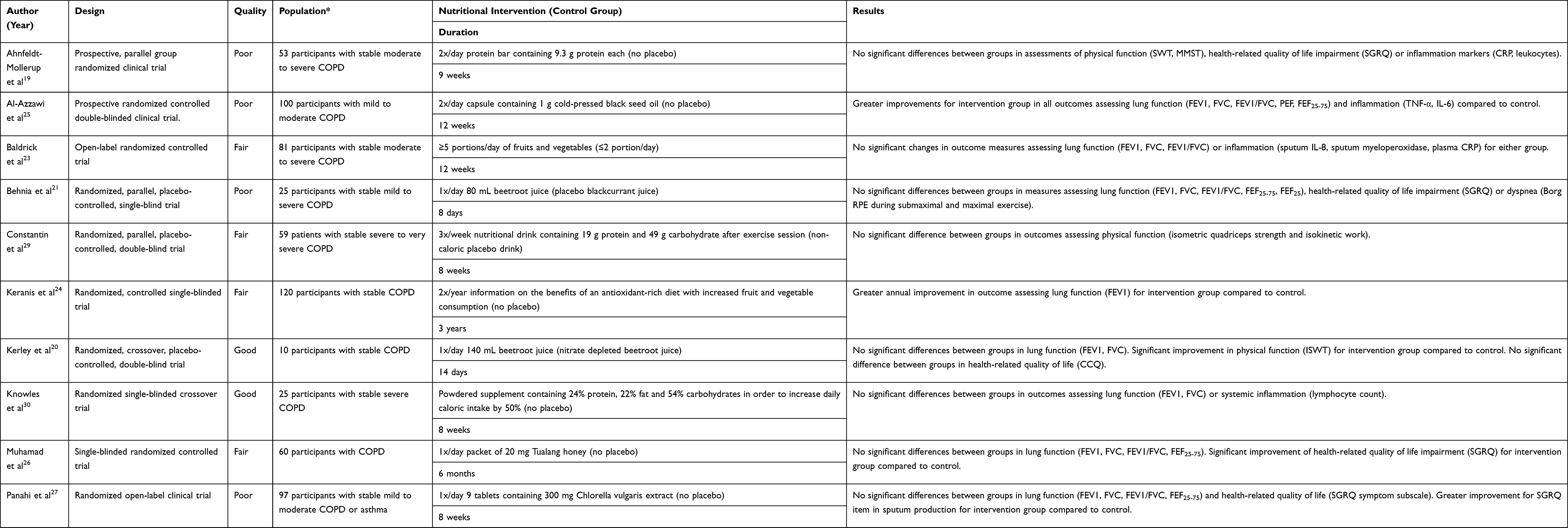 |
Table 2 Design, Population, Intervention, and Results of Included Studies |
Pulmonary Function
Eight trials investigated the impact on pulmonary function assessed through spirometry. Only two of the trials found significant effects of nutritional interventions on pulmonary function parameters. In a three-year duration open-label trial by Keranis et al, the intervention (I) group received bi-annual specific counseling on increasing fruit and vegetable consumption. They found a significant improvement on forced expiratory volume within one second (FEV1, % of predicted) compared to the control group (C), (I: ~+8%, C: ~−15%, p=0.03).24 A study on daily supplementation with 2-gram cold-pressed black seed oil by Al-Azzawi et al also found significant improvements in predicted values of FEV1 (I: +11%, C: +5%, p<0.001), forced vital capacity (FVC, I: +10%, C: +3%, p=0.002) and FEV1/FVC (I: +12%, C: +6%, p=0.001) after twelve weeks.25 Six trials found no significant effect of nutritional interventions on pulmonary function parameters; two of which focused on nitrate-rich beetroot juice for one and two weeks,20,21 one on Chlorella Vulgaris extract for eight weeks,27 one on Tualang honey for 6 months,26 one on increased fruit and vegetable consumption for twelve weeks,23 and finally one on powdered nutritional supplement for eight weeks.30
Physical Function
Six trials investigated outcomes related to physical function, including muscle performance and aerobic capacity. Of these, three trials found significant differences between intervention and control groups.20,22,28 In a twelve-week trial, Sugawara et al found improvements in the quadriceps muscle function and the 6-minute walk test (6MWT) for the intervention group receiving a nutritional drink containing whey peptide daily (I: +20%, C: −7%, p=0.014).28 In a two-week double-blinded crossover trial by Kerley et al, the intervention group consuming nitrate-rich beetroot juice daily showed significantly increased distance walked on the incremental shuttle walk test (ISWT) compared to the placebo group (I: +15%, C: +3%, p<0.001).20 Another trial on nitrate-rich beetroot juice by Pavitt et al found a significantly greater improvement in the ISWT for the intervention group compared to the control group after eight weeks (I: + 22%, C: +11%, p=0.027).22 Lastly, Steiner et al did not find significant differences between groups in physical function measures in their seven-week trial on the effect of carbohydrate-rich nutritional drink. However, when performing a sensitivity analysis on those with BMI > 19, a small significant improvement was seen in the ISWT for the intervention group compared to the placebo group (difference between I and C: 27 m, p=0.041).31 Of the trials that did not find significant differences in outcomes related to physical function, one studied the effect of protein bars for nine weeks and one studied the effect of a protein-carbohydrate supplement post-exercise for eight weeks.19,29
Health-Related Quality of Life
Lung-related quality of life impairment was assessed in seven of the thirteen included studies. Four studies used St. George's respiratory questionnaire, one used the chronic respiratory questionnaire, one used the clinical COPD questionnaire, and one used the COPD assessment test. Two trials found significant effects on lung-related quality of life impairment, one from Tualang honey for six months26 and a nutritional drink containing whey peptide for six weeks.28 A reduction of COPD symptoms is one of the factors for the significant increase in quality of life. Five trials did not find significant differences between intervention and control groups in lung-related quality of life impairment; three of which studied the effect of beetroot juice for one, two and eight weeks,20–22 one studied Chlorella vulgaris extract’s effect after eight weeks,27 and one the effect of protein bars after nine weeks.19
Inflammation
Five trials investigated the effect of nutritional interventions on markers of systemic inflammation among people with COPD, including C-reactive protein (CRP), interleukin 6 and 8 (IL-6/8), tumor necrosis factor-alpha (TNF-α) and lymphocyte count. Daily supplementation with a nutritional drink containing whey peptide for six weeks reduced plasma levels of high-sensitivity CRP (Δ ratio % + standard deviation (SD), I: −23±42, C: +29±101, p=0.05), TNF-α (Δ ratio + SD, I: −13±15, C: +4.4±21, p=0.01), IL-6 (Δ ratio % + SD, I: −11±34, C: +17±29p=0.03), and IL-8 (Δ ratio % + SD, I: −33±101, C: +1.5±2.3, p =0.002) significantly.28 Ingestion of cold-pressed black seed oil daily for twelve weeks significantly reduced plasma levels of TNF-α (I: −35%, C: −22%, p <0.001) and IL-6 (I: 38%, C: 28%, p = nr).25 Daily supplementation with protein bars for nine weeks showed a tendency toward treatment effect on plasma CRP (Δ mean: 3.9, p=0.14).19 No significant effect was found on blood lymphocyte count after eight weeks of daily nutritional supplementation.30 High intake of fruits and vegetables did not show effects on plasma CRP, sputum IL-8, and sputum myeloperoxidase after twelve weeks.23
Discussion
This systematic review aimed to provide an overview of the existing evidence on nutritional intervention as an addition to standard COPD management or pulmonary rehabilitation for non-malnourished individuals outside a hospital setting. All included participants in the included articles were adults and mostly 40 years and above. The outcomes of interest were pulmonary and physical function, lung-related quality of life impairment, and systemic inflammation. The literature presented in this review is highly heterogeneous. Many of the thirteen trials included in this review were underpowered due to small sample sizes, and the trials were not similar enough for a meta-analysis to be performed. There was particularly high heterogeneity in regards to type of intervention and reporting of outcome measures. Moreover, several reviewed trials were considered to have a moderate to high risk of bias, mostly due to lack of blinding of participants, personnel and outcome assessment, or unclear reporting of study design.
Pulmonary Function
The effect of nutritional intervention on pulmonary function was assessed in eight trials.20,21,23–27,30 The majority of these did not show statistically significant or clinically relevant effects on these measures. The trial by Keranis et al, with a fair risk of bias, found significant improvements in FEV1 after three years of bi-annual specific dietary counseling focused on the benefits of an antioxidant-rich diet.24 Importantly, nutritional assessment showed that participants in the intervention group increased their intake of fruits and vegetables in line with the recommendation they received, and that they thereby increased their intake of antioxidants from food. In contrast, the control group did not alter their diet or antioxidant intake, and exhibited a decline in FEV1 parallel to what would be expected without interventions.24 Interestingly, this was by far the longest-spanning study presented in this review. In contrast, the trials that did not find changes in pulmonary function had a mean duration of nine weeks – including a trial on high fruit and vegetable intake for twelve weeks.23
One could argue that a time perspective of weeks to a few months is too short for producing measurable changes in FEV1 and other pulmonary function markers. COPD is a progressive disease where airway inflammation and structural changes in lung parenchyma gradually alter pulmonary function, including FEV1.32 FEV1 usually declines slowly over the course of many years, although the rate of decline is highly variable between individuals.33,34 It seems unlikely that FEV1, or other pulmonary function parameters, would improve substantially in trials lasting just a few weeks or months.
Observational studies have shown favorable associations between fruit and vegetable consumption and pulmonary health outcomes,10 and the trial by Keranis et al strengthens this evidence.24 High fruit and vegetable consumption is associated with a lower risk of developing COPD,9 slower deterioration of FEV1, and reduced symptom severity.35–37 These findings could be related to the high antioxidant content of fruits and vegetables and the anti-inflammatory effects of antioxidants,38 and there is also some evidence from observational studies of a beneficial association of different antioxidants with pulmonary function.39 Interestingly, several of the nutritional interventions included in this review were high in antioxidant content, including cold-pressed black seed oil,25 and Chlorella Vulgaris extract.27 Only the former trial showed beneficial effects on pulmonary function, in addition to a significant reduction in markers of systemic inflammation – although it is worth noting that this trial has a high risk of bias due to unclear reporting on several aspects.
In addition to the limited time perspective of many studies, one could also question whether narrowed nutritional interventions can feasibly generate powerful enough biological responses for changes to occur at the tissue and organ level within the time span of the studies. For one, the pathogenesis of COPD is multifactorial and dependent on a vast array of biological processes and tissue responses, and changes in one pathway alone are unlikely to have a substantial influence on the overall disease progression.32 The progression and exacerbations of COPD are intimately associated with tobacco smoke or biomass fuel-induced oxidative and aldehyde/carbonyl stress, alterations in signaling of pro-inflammatory factors, steroid resistance, unfolded protein response, mucus hypersecretion, extracellular matrix remodeling, autophagy/apoptosis, epigenetic changes, cellular senescence/aging, endothelial dysfunction, autoimmunity, and skeletal muscle dysfunction.40 Secondly, it is unclear whether antioxidants, or other compounds from food, are transported to and concentrated in lung tissue at the quantities needed to evoke biological responses. Another systematic review on supplementation with vitamin D found a reduced exacerbation rate among COPD patients with a vitamin D deficiency and no effects among non-deficient patients.16 This could suggest an advantage of nutritional interventions targeting specific deficiencies and it could suggest that broader interventions containing a larger array of nutrients could be of a greater benefit at a group level than narrowed interventions aimed at a few macro- or micronutrients.
Physical Function
Among the most common disease-related consequences for individuals with COPD are reduced physical function and reduced exercise capacity.41 Both oxygen uptake (Vo2) and the distance walked in a six-minute walking test (6MWT) have been described as predictors of mortality.42 Even for COPD patients with a BMI within the ideal range, both abnormal body composition and micronutrient deficiencies are common. This leads to a range of experienced disabilities that affect the individuals´ well-being and the ability to perform daily activities.43,44 In our review, one out of four trials with a macronutrient or protein-related intervention showed a significant effect on 6MWT.28 This was also seen in two trials on beetroot juice where the subjects improved in the incremental shuttle walk test (ISWT).20,22 Interestingly, a trial from Steiner et al showed that nutritional intervention with macronutrient supplementation. A carbohydrate-rich drink enhanced the performance in the ISWT but only for individuals with a BMI over 19.31 This could indicate a potential for improvement in physical function for non-malnourished individuals with COPD.31
For individuals with COPD, a high protein diet has often been recommended to restore respiratory muscle force and promote immune function improvement (with protein intake of 1–1.5 g/kg of body weight/day).45 Besides, there is a need to correct common micronutrient deficiencies within this group, such as vitamin D, suggesting that dietary factors may contribute to the observed low muscle mass.46 The article from Keranis et al, with a promising effect on pulmonary function from increasing fruit and vegetable intake, and Kerley et al on increasing exercise capacity with nitrate rich beetroot juice, could indicate that there could be a concerted action of numerous active phytochemicals. Thus, it could be reasons to recommend increasing fruit and vegetable intake during physical or pulmonary rehabilitation programs, but also through dietary recommendations given to patients. This strategy matches the European respiratory society’s statement on future research; to determine whether targeting exacerbations with intensive nutritional therapy (perhaps combined with exercise and anabolic drugs) would improve outcomes.47
This research field uses a large variety of different physical function tests, and this was also noted in another systematic review on the COPD population.15 There is a need to coordinate a standard in this research field to better allow for comparison across studies. Both the 6MWT and the ISWT are good semi-objective tests, and both are achievable within this population when considering time length and intensity.
Inflammation
COPD is characterized by chronic inflammation of the lung and is associated with systemic inflammation.48,49 Therefore, this review included outcomes related to markers of airway, as well as systemic inflammation. Only one trial, by Baldrick et al on high fruit and vegetable intake, examined airway inflammation using sputum markers interleukin-8 and myeloperoxidase – and found no significant differences in these markers.23 No significant difference in plasma C-reactive protein, a marker of systemic inflammation, was seen either. This was attributed partly to high intra- and inter individual variation in these measures. Another systematic review on the effect of fruit and vegetable consumption on inflammation overwhelmingly found beneficial effects on different markers of systemic inflammation in both epidemiological and experimental studies.50
The trial on supplementation with cold-pressed black seed oil found a significant reduction in systemic inflammation markers after twelve weeks.25 Black seed oil is derived from the plant Nigella sativa and contains many bioactive compounds, including antioxidants.51 There is promising research emerging on the anti-inflammatory and immunomodulatory effect of Nigella sativa derivatives in animal models, and their potential use in the treatment of pulmonary diseases.51 Supplementation with a nutritional drink containing whey peptide for six weeks also significantly lowered systemic inflammation markers.28 Whey peptide is a protein complex derived from milk, and contains components with proposed anti-inflammatory properties.52 Lastly, supplementation with protein bars had a non-significant tendency toward effect on CRP after nine weeks. This was partly attributed to the addition of omega-3 fatty acids to the protein bars which are known for their anti-inflammatory properties – but the amount added might have been too small and the duration of the study too short for significant effects to occur.19
The observed discrepancies seen in the effects of nutritional intervention on inflammation status could be related to the many factors that influence inflammation status in COPD, such as individual differences in how inflammation or inflammatory stimuli are modulated, genetic factors, COPD severity, smoking status, and the effects of other medications such as steroids or statins.53,54
Based on studies on other health outcomes, in addition to fruits and vegetables, interventions increasing intake of nuts, legumes, whole grains and olive oil, seem to be particularly promising.55–62 Similarly, a traditional Mediterranean diet pattern also including many of these components show positive effects for a range of outcomes that could be relevant also for people with COPD. For future research, assessing potential pulmonary effects of such interventions could be relevant. Additionally, factors related to trial design, and in particular low study samples, may not allow for multivariable adjustment of many potential confounders. Moreover, specific and narrowed nutritional interventions may not be effective alone, compared to broader interventions aimed at overall healthy dietary patterns. Future studies, including RCTs, on the role of nutrition for inflammation status in COPD are needed.
Strengths and Limitations
Our study adhered to PRISMA guidelines and was registered in PROSPERO in advance. To minimize the risk of bias, two pairs of reviewers separately screened databases for eligible studies. The bias assessment was performed by two reviewers and discussed in detail until consensus was met. Two reviewers extracted data from the included studies. A limitation is that we only included published articles indexed in Medline, Embase, and Cochrane, and that it only included randomized controlled trials. Grey literature, basic research such as animal and cell studies, and observational studies were not included in this review. Therefore, this review does not provide detailed evidence regarding the mechanisms of nutritional factors in COPD, but rather systematic empirical evidence from interventions on humans.
An important limitation of this review was related to the substantial heterogeneity of the included trials, characterized by high variability in outcome measures, type of nutritional intervention, and trial duration. As a result of this variability, a meta-analysis was not possible. Several studies might have had too short duration to find relevant effects. Many of the included trials had small samples, which may explain some non-significant and mixed results. Only three out of thirteen articles were graded as good in terms of quality when using the Cochrane risk of bias assessment tool (see Supplementary Table S1). Still, many of the other articles were categorized as fair or poor quality due to the lack of blinding, even though the risk of bias was low related to many or all other aspects in the assessment. We acknowledge that blinding was not feasible due to the nature of the interventions studied in the said trials.
Conclusion
This systematic review revealed relatively few trials on nutritional interventions and effects on lung function tests for non-malnourished and non-obese individuals with COPD. Many of the trials were underpowered with small sample sizes or high dropout rates, often relatively short timespan, and there was substantial heterogeneity in the outcome measures reported between the studies, making meta-analyses difficult. The only study with more prolonged follow-up indicated that increasing intake of antioxidant-rich fruits and vegetables over prolonged periods have positive effects on lung function tests in individuals with COPD. Further, some nutritional interventions in people with COPD also observed effects on systemic inflammation, lung-related quality of life, and physical function tests, although with some mixed results. Further research should investigate effect of prolonged dietary interventions and should preferably report several functional outcomes to enable future meta-analysis.
Acknowledgments
We received important contribution to search strategy from a librarian, Randi Bolstad. We also received useful comments from Dr. Rune Nielsen, associate professor in Respiratory Medicine at the Department of Clinical Science, University of Bergen.
Funding
This research received no external funding except from author salaries.
Disclosure
The authors declare no conflict of interest.
References
1. Soriano JB, Abajobir AA, Abate KH; Collaborators GCRD. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X
2. López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
3. Lambert AA, Putcha N, Drummond MB, et al. Obesity is associated with increased morbidity in moderate to severe COPD. Chest. 2017;151(1):68–77. doi:10.1016/j.chest.2016.08.1432
4. Dixon AE, Peters U. The effect of obesity on lung function. Expert Rev Respir Med. 2018;12(9):755–767. doi:10.1080/17476348.2018.1506331
5. Mostert R, Goris A, Weling-Scheepers C, Wouters EF, Schols AM. Tissue depletion and health related quality of life in patients with chronic obstructive pulmonary disease. Respir Med. 2000;94(9):859–867. doi:10.1053/rmed.2000.0829
6. Schols AM, Broekhuizen R, Weling-Scheepers CA, Wouters EF. Body composition and mortality in chronic obstructive pulmonary disease. Am J Clin Nutr. 2005;82(1):53–59. doi:10.1093/ajcn/82.1.53
7. Schulze MB, Martínez-González MA, Fung TT, Lichtenstein AH, Forouhi NG. Food based dietary patterns and chronic disease prevention. BMJ. 2018;361:k2396. doi:10.1136/bmj.k2396
8. Kaluza J, Harris HR, Linden A, Wolk A. Long-term consumption of fruits and vegetables and risk of chronic obstructive pulmonary disease: a prospective cohort study of women. Int J Epidemiol. 2018;47(6):1897–1909.
9. Kaluza J, Larsson SC, Orsini N, Linden A, Wolk A. Fruit and vegetable consumption and risk of COPD: a prospective cohort study of men. Thorax. 2017;72(6):500–509. doi:10.1136/thoraxjnl-2015-207851
10. Scoditti E, Massaro M, Garbarino S, Toraldo DM. Role of diet in chronic obstructive pulmonary disease prevention and treatment. Nutrients. 2019;11(6):1357. doi:10.3390/nu11061357
11. Salari-Moghaddam A, Milajerdi A, Larijani B, Esmaillzadeh A. Processed red meat intake and risk of COPD: a systematic review and dose-response meta-analysis of prospective cohort studies. Clin Nutr. 2019;38(3):1109–1116. doi:10.1016/j.clnu.2018.05.020
12. Varraso R, Fung TT, Hu FB, Willett W, Camargo CA. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax. 2007;62(9):786–791. doi:10.1136/thx.2006.074534
13. Collins PF, Stratton RJ, Elia M. Nutritional support in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1385–1395. doi:10.3945/ajcn.111.023499
14. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:Cd000998.
15. Aldhahir AM, Rajeh AMA, Aldabayan YS, et al. Nutritional supplementation during pulmonary rehabilitation in COPD: a systematic review. Chron Respir Dis. 2020;17:1479973120904953. doi:10.1177/1479973120904953
16. Jolliffe DA, Greenberg L, Hooper RL, et al. Vitamin D to prevent exacerbations of COPD: systematic review and meta-analysis of individual participant data from randomised controlled trials. Thorax. 2019;74(4):337–345. doi:10.1136/thoraxjnl-2018-212092
17. Moher DSL, Clarke M, Ghersi D, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
18. Higgins AD, Sterne JAC. Chapter 8: assessing risk of bias in included studies. In: Higging CR, Chandler J, Cumpston MS, editors. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane; 2017.
19. Ahnfeldt-Mollerup P, Hey H, Johansen C, Kristensen S, Brix Lindskov J, Jensahnfeldt-Mollerupen C. The effect of protein supplementation on quality of life, physical function, and muscle strength in patients with chronic obstructive pulmonary disease. Eur J Phys Rehabil Med. 2015;51(4):447–456.
20. Kerley CP, James PE, McGowan A, Faul J, Cormican L. Dietary nitrate improved exercise capacity in COPD but not blood pressure or pulmonary function: a 2 week, double-blind randomised, placebo-controlled crossover trial. Int J Food Sci Nutr. 2019;70(2):222–231. doi:10.1080/09637486.2018.1492521
21. Behnia M, Wheatley CM, Avolio A, Johnson BD. Influence of dietary nitrate supplementation on lung function and exercise gas exchange in COPD patients. Nitric Oxide. 2018;76:53–61. doi:10.1016/j.niox.2018.03.009
22. Pavitt MJ, Tanner RJ, Lewis A, et al. Oral nitrate supplementation to enhance pulmonary rehabilitation in COPD: ON-EPIC a multicentre, double-blind, placebo-controlled, randomised parallel group study. Thorax. 2020;75(7):547–555. doi:10.1136/thoraxjnl-2019-214278
23. Baldrick FR, Elborn JS, Woodside JV, et al. Effect of fruit and vegetable intake on oxidative stress and inflammation in COPD: a randomised controlled trial. Eur Respir J. 2012;39(6):1377–1384. doi:10.1183/09031936.00086011
24. Keranis E, Makris D, Rodopoulou P, et al. Impact of dietary shift to higher-antioxidant foods in COPD: a randomised trial. Eur Respir J. 2010;36(4):774–780. doi:10.1183/09031936.00113809
25. Al-Azzawi MA, AboZaid MMN, Ibrahem RAL, Sakr MA. Therapeutic effects of black seed oil supplementation on chronic obstructive pulmonary disease patients: a randomized controlled double blind clinical trial. Heliyon. 2020;6(8):e04711. doi:10.1016/j.heliyon.2020.e04711
26. Muhamad R, Draman N, Aziz AA, Abdullah S, Jaeb MZM. The effect of Tualang honey on the quality of life of patients with chronic obstructive pulmonary disease: a randomized controlled trial. J Taibah Univ Med Sci. 2018;13(1):42–50. doi:10.1016/j.jtumed.2017.05.014
27. Panahi Y, Tavana S, Sahebkar A, Masoudi H, Madanchi N. Impact of adjunctive therapy with chlorellav ulgaris extract on antioxidant status, pulmonary function, and clinical symptoms of patients with obstructive pulmonary diseases. Sci. 2012;80(3):719–730.
28. Sugawara K, Takahashi H, Kashiwagura T, et al. Effect of anti-inflammatory supplementation with whey peptide and exercise therapy in patients with COPD. Respir Med. 2012;106(11):1526–1534. doi:10.1016/j.rmed.2012.07.001
29. Constantin D, Menon MK, Houchen-Wolloff L, et al. Skeletal muscle molecular responses to resistance training and dietary supplementation in COPD. Thorax. 2013;68(7):625–633. doi:10.1136/thoraxjnl-2012-202764
30. Knowles JB, Fairbarn MS, Wiggs BJ, Chan-Yan C, Pardy RL. Dietary supplementation and respiratory muscle performance in patients with COPD. Chest. 1988;93(5):977–983. doi:10.1378/chest.93.5.977
31. Steiner MC, Barton RL, Singh SJ, Morgan MD. Nutritional enhancement of exercise performance in chronic obstructive pulmonary disease: a randomised controlled trial. Thorax. 2003;58(9):745–751. doi:10.1136/thorax.58.9.745
32. Hogg JC, Timens W. The pathology of chronic obstructive pulmonary disease. Annu Rev Pathol. 2009;4:435–459. doi:10.1146/annurev.pathol.4.110807.092145
33. Kirkby J, Nenna R, McGowan A. Changes in FEV(1) over time in COPD and the importance of spirometry reference ranges: the devil is in the detail. Breathe (Sheff). 2019;15(4):337–339. doi:10.1183/20734735.0252-2019
34. Tashkin DP. Variations in FEV1 decline over time in chronic obstructive pulmonary disease and its implications. Curr Opin Pulm Med. 2013;19(2):116–124. doi:10.1097/MCP.0b013e32835d8ea4
35. Smit HA. Chronic obstructive pulmonary disease, asthma and protective effects of food intake: from hypothesis to evidence? Respir Res. 2001;2(5):261–264. doi:10.1186/rr65
36. Kelly Y, Sacker A, Marmot M. Nutrition and respiratory health in adults: findings from the health survey for Scotland. Eur Respir J. 2003;21(4):664–671. doi:10.1183/09031936.03.00055702
37. Tabak C, Smit HA, Heederik D, Ocké MC, Kromhout D. Diet and chronic obstructive pulmonary disease: independent beneficial effects of fruits, whole grains, and alcohol (the MORGEN study). Clin Exp Allergy. 2001;31(5):747–755. doi:10.1046/j.1365-2222.2001.01064.x
38. Bøhn SK, Myhrstad MC, Thoresen M, et al. Blood cell gene expression associated with cellular stress defense is modulated by antioxidant-rich food in a randomised controlled clinical trial of male smokers. BMC Med. 2010;8:54. doi:10.1186/1741-7015-8-54
39. Hu G, Cassano PA. Antioxidant nutrients and pulmonary function: the third national health and nutrition examination survey (NHANES III). Am J Epidemiol. 2000;151(10):975–981. doi:10.1093/oxfordjournals.aje.a010141
40. O’Donnell DE, Parker CM. COPD exacerbations. 3: pathophysiology. Thorax. 2006;61(4):354–361. doi:10.1136/thx.2005.041830
41. Pinto-Plata VM, Celli-Cruz RA, Vassaux C, et al. Differences in cardiopulmonary exercise test results by American Thoracic Society/European Respiratory Society-Global Initiative for Chronic Obstructive Lung Disease stage categories and gender. Chest. 2007;132(4):1204–1211. doi:10.1378/chest.07-0593
42. Cote CG, Pinto-Plata V, Kasprzyk K, Dordelly LJ, Celli BR. The 6-min walk distance, peak oxygen uptake, and mortality in COPD. Chest. 2007;132(6):1778–1785. doi:10.1378/chest.07-2050
43. Hopkinson NS, Tennant RC, Dayer MJ, et al. A prospective study of decline in fat free mass and skeletal muscle strength in chronic obstructive pulmonary disease. Respir Res. 2007;8(1):25. doi:10.1186/1465-9921-8-25
44. Engelen MP, Schols AM, Baken WC, Wesseling GJ, Wouters EF. Nutritional depletion in relation to respiratory and peripheral skeletal muscle function in out-patients with COPD. Eur Respir J. 1994;7(10):1793–1797. doi:10.1183/09031936.94.07101793
45. Collins PF, Yang IA, Chang Y-C, Vaughan A. Nutritional support in chronic obstructive pulmonary disease (COPD): an evidence update. J Thorac Dis. 2019;11(Suppl 17):S2230–S2237. doi:10.21037/jtd.2019.10.41
46. Horadagoda C, Dinihan T, Roberts M, Kairaitis K. Body composition and micronutrient deficiencies in patients with an acute exacerbation of chronic obstructive pulmonary disease. Intern Med J. 2017;47(9):1057–1063. doi:10.1111/imj.13453
47. Schols AM, Ferreira IM, Franssen FM, et al. Nutritional assessment and therapy in COPD: a European Respiratory Society statement. Eur Respir J. 2014;44(6):1504–1520. doi:10.1183/09031936.00070914
48. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
49. Gan WQ, Man SFP, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574. doi:10.1136/thx.2003.019588
50. Hosseini B, Berthon BS, Saedisomeolia A, et al. Effects of fruit and vegetable consumption on inflammatory biomarkers and immune cell populations: a systematic literature review and meta-analysis. Am J Clin Nutr. 2018;108(1):136–155. doi:10.1093/ajcn/nqy082
51. Saadat S, Aslani MR, Ghorani V, Keyhanmanesh R, Boskabady MH. The effects of Nigella sativa on respiratory, allergic and immunologic disorders, evidence from experimental and clinical studies, a comprehensive and updated review. Phytother Res. 2021;35:2968–2996. doi:10.1002/ptr.7003
52. Tsutsumi R, Tsutsumi Y. Peptides and proteins in whey and their benefits for human health. Austin J Nutri Food Sci. 2014;1(1):1002.
53. Barbu C, Iordache M, Man MG. Inflammation in COPD: pathogenesis, local and systemic effects. Rom J Morphol Embryol. 2011;52(1):21–27.
54. Su B, Liu T, Fan H, et al. Inflammatory markers and the risk of chronic obstructive pulmonary disease: a systematic review and meta-analysis. PLoS One. 2016;11(4):e0150586–e0150586. doi:10.1371/journal.pone.0150586
55. Schwingshackl L, Hoffmann G. Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids Health Dis. 2014;13. doi:10.1186/1476-511X-13-154
56. Schwingshackl L, Hoffmann G. Mediterranean dietary pattern, inflammation and endothelial function: a systematic review and meta-analysis of intervention trials. Nutr Metab Cardiovas. 2014;24(9):929–939. doi:10.1016/j.numecd.2014.03.003
57. Schwingshackl L, Hoffmann G, Iqbal K, Schwedhelm C, Boeing H. Food groups and intermediate disease markers: a systematic review and network meta-analysis of randomized trials. Am J Clin Nutr. 2018;108(3):576–586. doi:10.1093/ajcn/nqy151
58. Schwingshackl L, Hoffmann G, Missbach B, Stelmach-Mardas M, Boeing H. An umbrella review of nuts intake and risk of cardiovascular disease. Curr Pharm Design. 2017;23(7):1016–1027. doi:10.2174/1381612822666161010121356
59. Schwingshackl L, Missbach B, Konig J, Hoffmann G. Adherence to a Mediterranean diet and risk of diabetes: a systematic review and meta-analysis. Public Health Nutr. 2015;18(7):1292–1299. doi:10.1017/S1368980014001542
60. Schwingshackl L, Schwedhelm C, Hoffmann G, et al. Food groups and risk of all-cause mortality: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr. 2017;105(6):1462–1473.
61. Schwingshackl L, Strasser B, Hoffmann G. Effects of monounsaturated fatty acids on glycaemic control in patients with abnormal glucose metabolism: a systematic review and meta-analysis. Ann Nutr Metab. 2011;58(4):290–296. doi:10.1159/000331214
62. Viguiliouk E, Glenn AJ, Nishi SK, et al. Associations between dietary pulses alone or with other legumes and cardiometabolic disease outcomes: an umbrella review and updated systematic review and meta-analysis of prospective cohort studies. Adv Nutr. 2019;10(Suppl_4):S308–S319. doi:10.1093/advances/nmz113
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.