")
Back to Journals » Journal of Pain Research » Volume 15
Effects of Music Therapy on Quality of Life in Adults with Sickle Cell Disease (MUSIQOLS): A Mixed Methods Feasibility Study
Authors Rodgers-Melnick SN , Lin L, Gam K, Souza de Santana Carvalho E, Jenerette C, Rowland DY , Little JA, Dusek JA , Bakshi N, Krishnamurti L
Received 9 October 2021
Accepted for publication 21 December 2021
Published 11 January 2022 Volume 2022:15 Pages 71—91
DOI https://doi.org/10.2147/JPR.S337390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Video abstract presented by Samuel N Rodgers-Melnick.
Views: 232
Samuel N Rodgers-Melnick,1,2 Lucas Lin,3 Kristina Gam,4 Evanilda Souza de Santana Carvalho,5 Coretta Jenerette,6 Douglas Y Rowland,2 Jane A Little,7 Jeffery A Dusek,1,8 Nitya Bakshi,9,10 Lakshmanan Krishnamurti9,10
1Connor Whole Health, University Hospitals of Cleveland, Cleveland, OH, USA; 2Department of Population and Quantitative Health Sciences, School of Medicine, Case Western Reserve University, Cleveland, OH, USA; 3School of Medicine, Case Western Reserve University, Cleveland, OH, USA; 4Department of Surgery, University of Chicago Medical Center, Chicago, IL, USA; 5Department of Health, Universidade Estadual de Feira de Santana, Feira de Santana, Brazil; 6College of Nursing, University of South Carolina, Columbia, SC, USA; 7Department of Medicine, University of North Carolina, Chapel Hill, NC, USA; 8Department of Family Medicine and Community Health, School of Medicine, Case Western Reserve University, Cleveland, OH, USA; 9Division of Pediatric Hematology-Oncology-BMT, Department of Pediatrics, Emory University, Atlanta, GA, USA; 10Aflac Cancer and Blood Disorders Center of Children’s Healthcare of Atlanta, Atlanta, GA, USA
Correspondence: Samuel N Rodgers-Melnick
University Hospitals Connor Whole Health, 11100 Euclid Avenue, Cleveland, OH, 44106, USA
Tel +1 216 844 7727
Fax +216 201 6220
Email [email protected]
Purpose: To investigate the feasibility, acceptability, and preliminary efficacy of a 6-session music therapy protocol on self-efficacy, quality of life, and coping skills in adults with sickle cell disease (SCD).
Patients and Methods: Using a mixed-methods intervention design, adults with SCD (ages 21– 57; mean age 32.33) were randomized (1:1) to either 1) a 6-session music therapy (MT) intervention (n = 12) or 2) waitlist control (WLC) (n = 12) using stratified randomization where factors were age in years (≤ 30 vs > 30), and sex (male, female). All participants completed two weeks of daily electronic pain diary entries and self-efficacy, quality of life, and coping skills measures before and after their assigned study condition to explore preliminary efficacy. MT participants were taught music exercises accessed via smartphone and subsequently interviewed to determine feasibility and acceptability.
Results: The enrollment rate was 89%. All study measures were completed, with high rates of electronic pain diary completion at baseline (70%) and 2-week follow-up (66%). Interviews revealed two overall themes related to MT participants’ experience: 1) participants learned new self-management skills and 2) MT improved participants’ ability to cope with pain. MT participants demonstrated 100% attendance. In preliminary analyses, MT participants demonstrated significant improvements (means ± SD) in self-efficacy (5.42 ± 5.43, p = 0.008, d = 1.20), PROMIS sleep disturbance (− 1.49 ± 6.68, p = 0.023, d = − 0.99), PROMIS pain interference (− 2.10 ± 4.68, p = 0.016, d = − 1.06), and ASCQ-Me social functioning impact scores (2.97 ± 6.91, p = 0.018, d = 1.05) compared to WLC participants.
Conclusion: Preliminary findings support the feasibility and acceptability of music therapy for home use in adults with SCD. While music therapy may assist adults with SCD in improving self-efficacy and quality of life, subsequent, fully-powered clinical research is needed to determine its efficacy.
Keywords: quality of life, chronic pain, integrative health, self-efficacy
Erratum for this paper has been published
Plain Language Summary
In this study, we examined whether a 6-part music therapy intervention was feasible, acceptable, and beneficial among adults (ages 21–57; mean age 32.33) with sickle cell disease and chronic pain. Participants were randomized to either 1) a 6-part in-person music therapy intervention involving education and music exercises (ie music-based breathing exercises, progressive muscle relaxation, imagery, and active music making) personalized to participants’ preferred music genres or 2) a waitlist control group. Participants completed daily electronic pain diary entries as well as quality of life measures before and after study conditions. We found that the study and intervention were feasible, with high rates of enrollment, attendance, and measure completion. Interviews revealed two overall themes related to participants’ experience of music therapy: 1) participants learned new self-management skills and 2) music therapy improved participants’ ability to cope with pain. When comparing participants in music therapy versus participants in waitlist control, we found large effect sizes for self-efficacy (1.20), pain interference (−1.06), social functioning impact (1.05), and sleep disturbance (−0.99). These findings support the feasibility and acceptability of music therapy for home use in adults with sickle cell disease. Music therapy may assist adults with sickle cell disease in improving self-efficacy and quality of life.
Introduction
Adults with sickle cell disease (SCD) often have to manage several comorbid painful conditions contributing to psychosocial challenges and impaired quality of life. In addition to enduring unpredictable acute vaso-occlusive pain crises throughout their lives, many adults with SCD also suffer from chronic pain syndromes that emerge from physiological complications, including chronic sickle cell vaso-occlusion, central sensitization, and opioid-induced hyperalgesia.1 In the Pain in Sickle Cell Epidemiology Study (PiSCES), which was a longitudinal etiologic study of 232 adults with SCD, 54% reported having pain, pain crises, or utilization on more than half (51%) of 31,017 analyzed patient-days. Twenty-nine percent of these patients had pain nearly every day, while only 15% rarely had pain.1
Mental health challenges further complicate chronic pain in many adults with SCD. There are several sources for depressive symptoms in patients with SCD, including the chronic nature of the disease, unpredictability of crises, chronic pain, and a significant number of complications such as anemia, fatigue, growth retardation, leg ulcers, renal failure, strokes, and reduced life expectancy.2,3 In PiSCES, 27.6% of patients were depressed at baseline, a much higher rate than that reported in African-Americans’ general adult population. Patients with SCD and depression had pain on significantly more days than patients with SCD who did not have depression. On days when patients with SCD and depression had pain without a sickle cell crisis, they had higher mean pain, distress from pain, and pain interference than patients with SCD who did not have depression.2
These physical and psychological challenges contribute to impairments in the quality of life of adults with SCD. In PiSCES, patients with SCD scored significantly worse than national norms on all subscales of health-related quality of life (HRQoL) except mental health.4 Specifically, HRQoL was equal to or worse than patients with other significant chronic conditions in many domains, and the more pain patients with SCD experienced, the worse their reported HRQoL.4 A recent systematic review found depression and anxiety occurrence to be 21–33% and 7–36%, respectively, in adults with SCD.5 Higher pain is also strongly associated with decreased work and school activity, social activity, and household chores.6 Thus, new interventions are needed to improve the overall quality of life of patients with SCD in addition to pain outcomes.
One intervention that may effectively address both pain and quality of life for adults with SCD is music therapy. Music therapy is the clinical and evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship by a credentialed professional who has completed an approved music therapy program.7 Music therapy is known to be effective for managing pain in several populations, including patients with cancer,8,9 patients with chronic pain,10–12 and patients receiving palliative care.13,14 Studies have also supported the positive effects of music therapy on quality of life, especially in patients with cancer.15 Recent multi-session interventions with urban African-Americans with chronic pain have revealed positive effects of vocal music therapy on pain self-efficacy and participants’ ability to participate in social activities.16,17 Music therapy has been shown to be effective in improving sleep quality among cancer patients undergoing treatment18 and hospitalized adults.19 Importantly, music therapy can also be tailored to the unique cultural preferences of adults with SCD. Given the positive effects of music therapy on pain, mood, and quality of life in other populations, adult patients with SCD may experience similar benefits from incorporating music therapy interventions into their daily lives.
In our prior three-arm randomized controlled trial comparing 1) music therapy, 2) music listening, and 3) no music (control),20 we found that participants with SCD who received a single 20-minute electronic music improvisation session with a music therapist reported significant improvements in pain intensity and mood compared to a control group, whereas participants who received music listening only reported improvements in mood. Qualitative data from this study supported the acceptability and feasibility of a single music therapy intervention for addressing acute pain during an acute care clinic visit. Given that SCD is a chronic disease, we felt that a more comprehensive music therapy intervention was needed to address the health challenges that individuals with SCD face in their daily lives.
Such a comprehensive music therapy intervention should be grounded in a theoretical framework that has been effective for addressing pain in this population. Currently, cognitive-behavioral therapy (CBT) has strong supporting evidence for managing pain in individuals with SCD,21–23 though several barriers (eg lack of access, cost, and stigma associated with seeking mental health services) remain that prevent individuals with SCD from receiving quality CBT pain services.24 CBT interventions contain elements that can serve as the foundation for music therapy interventions for SCD pain relief. These elements include pain psycho-education, breathing exercises, imagery, reinterpreting pain sensations, calming self-statements, and relaxation training.25–27 When deployed within the context of patients’ routine clinical care, music therapy may be a more accessible and culturally relevant option than CBT for individuals with SCD and chronic pain. Music therapy may also offer additional benefits for addressing patients’ self-efficacy and quality of life.
This intervention required novel music intervention delivery strategies and research methods. At present, it is unknown whether a 6-session music intervention would be feasible to conduct with a SCD population, or whether the intervention would be acceptable. Thus, as recommended by the National Center for Complementary and Integrative Health (NCCIH),28 it was prudent for us to conduct a feasibility study prior to a larger trial to determine 1) feasibility (eg rates of recruitment, enrollment, randomization, retention, and data collection), 2) acceptability (eg session attendance and participants' feedback), and 3) preliminary efficacy (eg effect sizes for changes in patient-reported outcomes). Here, we report the results of a study designed to determine the feasibility, acceptability, and preliminary efficacy of a 6-session music therapy intervention as compared to waitlist control for adults with SCD and chronic pain.
Materials and Methods
Design
This study utilized a mixed-methods intervention design in which qualitative data were embedded in the framework of a randomized controlled trial.29 We chose a mixed-methods intervention design to enhance our understanding of participants’ daily pain, experience with the music therapy exercises, and perceived acceptability of the music therapy intervention. This qualitative data was also used to provide context for any potential changes in quantitative outcomes. A total of 24 adults with SCD and chronic pain were randomized to either 1) a 6-session music therapy intervention (MT) or 2) a waitlist control group (WLC). See Figure 1 for a flow diagram of the study design. Given that this was a feasibility study, an a priori power calculation was not conducted nor would such a calculation have been warranted. Indeed, per the recommendations from the NCCIH,28 our sample size of 24 was based on how many participants we could practically recruit, engage in the intervention, and evaluate given our time and budgetary constraints.
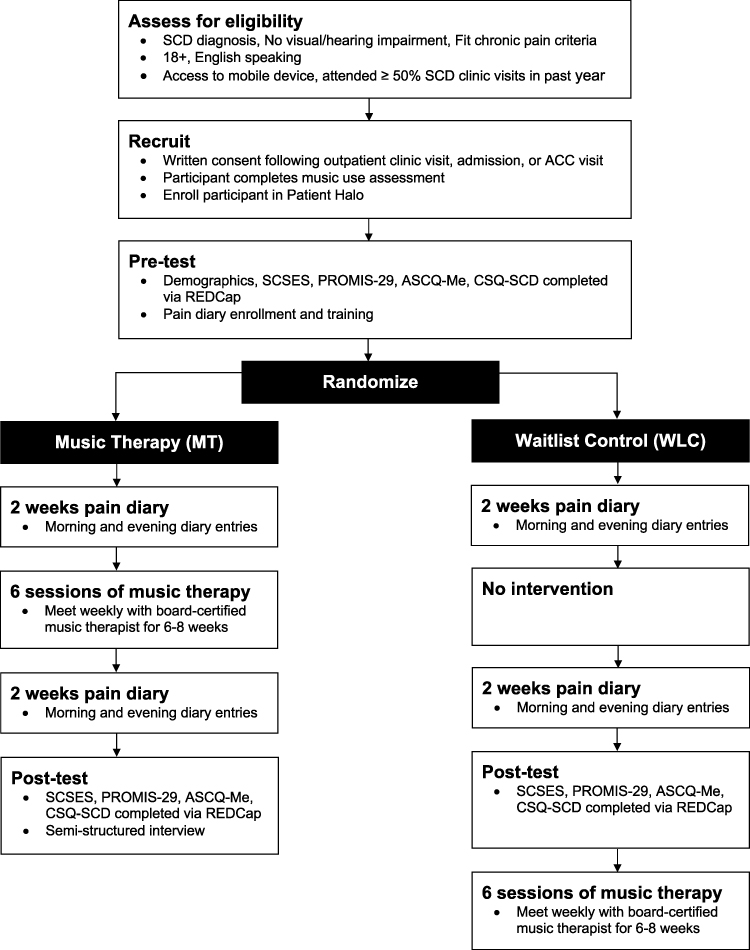 |
Figure 1 Flow diagram of MUSIQOLS study. Abbreviations: ACC, Acute Care Clinic; ASCQ-Me, Adult Sickle Cell Quality of Life Measurement System; CSQ-SCD, Coping Skills Questionnaire for Sickle Cell Disease; MT, music therapy; PROMIS-29, Patient Reported Outcomes Measurement Information System – 29; REDCap, Research Electronic Data Capture; SCD, sickle cell disease; SCSES, Sickle Cell Self-Efficacy Scale; WLC, waitlist control. |
Participants and Setting
This study was conducted between June 2018 and January 2019 at a large Midwestern hospital in the United States. Twenty-four subjects (ages 21–57; mean age 32.33) diagnosed with SCD, who were at least 18 years old, able to speak and understand English, had a working email address, had access to a mobile device with email capabilities, fit the criteria for SCD chronic pain,30 and had attended at least 50% of their scheduled outpatient visits to the adult SCD clinic in the last 12 months were recruited to participate in the study. We included the criteria pertaining to adult SCD clinic attendance to ensure we enrolled participants with demonstrated commitment to participating in treatment at the study site as this study also required a commitment to attending weekly in-person treatment. Patients who had significant hearing, visual, or cognitive impairment were excluded.
Ethics and Consent
At the time of informed consent, the investigators met with potential participants in a private treatment room or consult room out of the earshot of others to maintain privacy. To maintain confidentiality, we used several strategies including 1) storing patient identifiers, demographics, clinical characteristics, and patient-reported outcomes in REDCap, a secure, web-based application designed to support data capture for research studies;31 2) identifying participants by the number assigned to them at the beginning of the study rather than by name; 3) storing electronic pain diary data on a secure password-protected server; 4) storing de-identified audio recordings of the participants’ interviews and music therapy interventions on a password-protected encrypted hard drive; and 5) storing paper research documents in a double-locked secure cabinet in the PI’s locked office.
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board. Written, informed consent was obtained from all participants. The study is registered in clinicaltrials.gov (NCT03556657).
Procedure
Screening and Enrollment
Following a referral from the patient’s hematology provider, the principal investigator (PI), who was also the music therapist for the study, reviewed the patient’s medical record to ensure eligibility. The patient’s hematology provider also examined the patient before recruitment to determine if the patient met the chronic pain criteria.30 Participants were recruited from one of three settings: 1) following regularly scheduled visits to the adult SCD clinic, 2) during visits to the acute care clinic, or 3) before discharge from an inpatient unit. In these settings, the PI approached the patient to obtain written consent, authorization to record the patient, and contact information. The PI also enrolled the patient in Patient Halo®, a communication service that would allow each participant to communicate with the study team via secure text messages. After obtaining contact information, the PI conducted a music use assessment to determine the participant’s music preferences and resources.
Pre-Test Assessment and Pain Diary Training
Following informed consent and the music use assessment, a research assistant (RA) contacted participants to schedule a time for them to come to the hospital for individual pre-test assessment and pain diary training. Assessments were conducted in a private consult room or treatment area. Individuals completed a demographics questionnaire and pre-test measures of coping skills, quality of life, and self-efficacy on a desktop computer or a laptop provided by the RA. Details regarding these measures can be found in the preliminary efficacy subsection of our data collection procedures below. All outcome measures were assessed using REDCap.31 Individuals were allowed to skip any questions that they did not feel comfortable answering. Following the pre-test assessment, the RA trained each participant to access and use the electronic pain diary.
Randomization
Immediately following the pre-test assessment and pain diary training, the PI randomly assigned the participant into one of the two groups (1:1). The study employed stratified randomization where the stratification factors were age in years (≤30 vs >30), and sex (male, female). Before the study, the study biostatistician prepared the randomization list using a random number generator. For each stratum, as defined above, sealed and sequentially numbered opaque envelopes were prepared by the statistician, and cards within them indicated the treatment allocation for successively enrolled participants. Within each stratum, randomization was blocked with random block sizes of 4 or 6 to prevent the PI from predicting the next assignment. The RA who administered the study measures via REDCap was blinded to the participants’ group assignment, but the PI was not. Randomization continued until 24 subjects were enrolled and randomized into their respective groups.
Baseline Pain Diary
After the pre-test assessment and randomization, all participants were asked to complete daily pain diary entries two times per day (once in the morning and once in the evening) for two consecutive weeks (28 entries in total). Participants accessed the pain diary from their own mobile devices. Throughout the study, the RA remotely monitored the completion of the electronic pain diary entries. The pain diary was not a means of communication with healthcare staff, and pain diary scores were not reported to the adult SCD medical team. The RA contacted participants, who failed to complete pain diaries for three or more days, to remind them to complete their entries, troubleshoot barriers to adherence, and/or record reasons for non-completion.
Intervention
Following the 2-week baseline pain diary period, participants would engage in the intervention to which they were assigned (ie MT or WLC). More details on these interventions can be found in the music therapy (MT) intervention and waitlist control (WLC) group sections below.
Follow-Up Pain Diary
After participants completed their assigned interventions, they again completed daily pain diary entries two times per day for two consecutive weeks, as detailed in the baseline pain diary description above.
Post-Test Assessment and Semi-Structured Interview
After the follow-up pain diary period, a post-test assessment was scheduled. Excluding the demographics questionnaire, participants completed the same measures that were administered in the pre-test. A different RA then conducted a semi-structured interview with participants in the MT condition to assess the MT intervention’s delivery, acceptability, and usefulness. Details on the contents of the semi-structured interview can be found in the acceptability subsection of our data collection procedures described below.
Music Therapy for WLC Group
Following the post-test assessment, the PI promptly contacted participants randomized to WLC to schedule their music therapy sessions. To minimize burden, WLC participants were not asked to complete additional questionnaires.
Music Therapy (MT) Intervention
Development
The 6-session MT intervention created for this study was informed by 1) the PI’s clinical experience working with adults with SCD; 2) prior music therapy interventions conducted with the SCD population;20 3) a survey on the music preferences, music resources, music-based pain strategies, and needs of 100 adults with SCD;32 4) a CBT manual for chronic pain;33 and 5) feedback from patients and members of a multidisciplinary team specializing in the care of adults with SCD. The intervention was designed to provide patient education and practical music therapy exercises for adults with SCD to easily access and practice every day via their own mobile devices to manage pain and quality of life. Elements of CBT for chronic pain including 1) pain education; 2) goal setting; 3) the connection between situations, thoughts, emotions, and behaviors; 4) relaxation techniques; 5) anticipating obstacles; and 6) discharge planning were integrated into the MT session plans. A CBT orientation was chosen based on the strong supporting evidence for its use in managing pain in individuals with SCD.21,22 The first author, a board-certified music therapist (MT-BC) trained in CBT with over 6 years of experience working with adults with SCD, provided all of the music therapy interventions using the same standardized session plans.
Overview
During the study, most MT sessions were prescheduled on an outpatient basis, coordinated with provider visits when possible, and provided in private consult rooms. If a participant was admitted to the hospital or the acute care clinic on the scheduled day of an MT session, the participant had the option of participating in the MT session in their treatment room. However, no MT sessions were provided in the emergency department. Over the course of the study 59/72 (81.9%) sessions were conducted in an outpatient private consult room, 11/72 (15.3%) sessions were provided inpatient, and 2/72 (2.8%) sessions were provided in the acute care clinic. Sessions were rescheduled as needed, and each MT session lasted between 30–60 minutes.
As part of a clinical assessment, participants completed the well-being, pain, anxiety, depression, and tiredness subscales of the Edmonton Symptom Assessment Scale (ESAS) at the beginning and end of each MT session in the presence of the PI. The ESAS was used to clinically measure patients’ symptoms pre- and post-session. Each MT session included 1) setting an agenda, 2) an explanation of the music exercise, 3) a demonstration of the music exercise in which the PI engaged the participant in practicing the music exercise (eg breathing, progressive muscle relaxation, imagery), 4) time to process the participant’s response to the exercise, 5) time for the PI to electronically deliver the music exercise to the participant and ensure that the participant had all materials necessary to use the exercise at home, and 6) a homework assignment for the participant to practice the music exercise taught in that session at least once per day until the following MT session. The genres of each music exercise (ie music-based breathing exercise, progressive muscle relaxation, imagery, and active music making) were personalized to participants’ preferences (eg hip-hop, gospel, R&B, jazz, rock, and/or soul). Each music exercise lasted an average of 10.9 minutes. As the music exercises were being demonstrated, the PI simultaneously recorded the exercise. These recordings were created in a high-quality mobile recording studio developed by the first author. This studio could be moved to wherever the MT sessions were held and enabled the recording of music exercises for participants to practice at home.
Participants were provided with all necessary materials needed to practice the music exercises at home, including handouts and personalized audio recordings of music exercises delivered via a secure Box® folder, email, and/or Airdrop® depending on the functions of the participant’s mobile device. The PI encouraged each participant to contact him via email, phone, or Patient Halo® with any questions about using the music exercises.
Participants were contacted by the PI weekly to monitor their use of MT exercises at home. Each MT session followed a standardized format over six weeks. This 6-week treatment period was extended to up to eight weeks if a scheduling conflict prevented a participant from receiving the six MT sessions over six consecutive weeks. On average, there were 10.5 days between each MT session. See the Supplementary Data for an overview of the goals, structure, and narrative description of each of the six MT sessions.
Waitlist Control (WLC) Group
Participants randomized to WLC did not receive any music therapy sessions during the 10-week study period. It is important to note that music therapy services are clinically offered in the hospital. Accordingly, the investigative team agreed that if participants randomized to WLC were referred for music therapy services as part of their clinical inpatient care during the study period, they would not receive music therapy services at that time. Nothing else about participants’ health care treatment (ie standard medication management as prescribed by the participant’s primary team) changed due to participating in this study.
Remuneration
Participants received $10.00 at the conclusion of each MT session and study assessment, $1.00 per completed pain diary entry, and one daily bus pass prior to each study assessment or MT session.
Data Collection
Demographics and Clinical Characteristics
The following information was extracted from the participant’s medical record: age, sex, race, comorbid medical conditions, chronic pain classification, type of SCD, and current treatment for SCD. We used the following three diagnostic modifiers proposed by Dampier et al to describe participants’ chronic SCD pain subtypes: 1) chronic SCD pain without contributory disease complications, 2) chronic SCD pain with contributory disease complications, or 3) chronic pain with mixed pain types. Participants’ current pain medicine prescriptions were obtained from the Ohio Automated Rx Reporting System (OARRS). Participants entered their responses to questions assessing income, marital status, religious background, employment status, and education level directly into REDCap. Health care utilization was determined through monitoring participants’ 1) visits to the emergency department, 2) visits to the acute care clinic, and 3) admissions to the hospital for any reason pre-study (ie 12 weeks before randomization) and during the study (ie between randomization and 12-weeks after randomization). Healthcare utilization data was obtained retrospectively via medical record review following participants’ completion of study measures.
Daily Pain
Participants’ daily pain scores were measured using a validated, multidimensional pain diary with evidence for content validity that has undergone user review in the adolescent SCD population.34 This pain diary measured the following every morning: 1) pain intensity (0 = no pain, 10 = worst pain), 2) pain location, 3) pain description (eg burning, stinging, shooting), 4) pain causation (eg stress, over-exertion), and 5) effects of pain on sleep (0 = did not affect my sleep, 10 = totally affected my sleep). Every evening, the pain diary measured the following: 1) pain intensity, 2) pain location, 3) pain description, 4) pain causation, 5) how much pain got in the way of things the participant wanted to do that day (0 = did not get in the way at all, 10 = totally got in the way), 6) effects of pain on interactions with family and friends, 7) effects of pain on mood (0 = did not affect my mood at all, 10 = totally affected my mood), 8) how much pain got in the way of schoolwork (if applicable), 9) how much pain got in the way of work (if applicable), 10) pain medication use, and 11) use of pain management strategies (eg heat, music, massage).34
Feasibility
The following data were collected to determine the feasibility of the MUSIQOLS protocol and intervention: 1) the number of patients who were screened, enrolled, and randomized, 2) participants’ attendance to MT sessions, 3) the number of completed pain diary entries, 4) how often participants reported using music exercises at home (ie never, once or twice a week, almost every day, every day, or more than once per day), and 5) the number of completed study assessments (eg PROMIS-29, ASCQ-Me) across the various timepoints.
Acceptability
Feasibility and acceptability were further assessed using a semi-structured interview. All interviews were conducted and recorded by one trained RA. Interview questions focused on participants’ current pain, their experience of the MT sessions (eg suitability of schedule, length, location, and impacts on pain, mood, and quality of life), and whether anything could have been done differently to improve the MT sessions. A sample of initial interviews was reviewed for consistency, and any necessary re-training (ie guidance on formatting probing questions) was implemented.
Preliminary Efficacy
Valid and reliable patient-reported outcome questionnaires were administered to determine the effects of MT relative to WLC on self-efficacy, quality of life, and use of coping skills. Details regarding when these measures were assessed are provided in Figure 2. All patient-reported outcome measures were made into electronic survey instruments in REDCap.
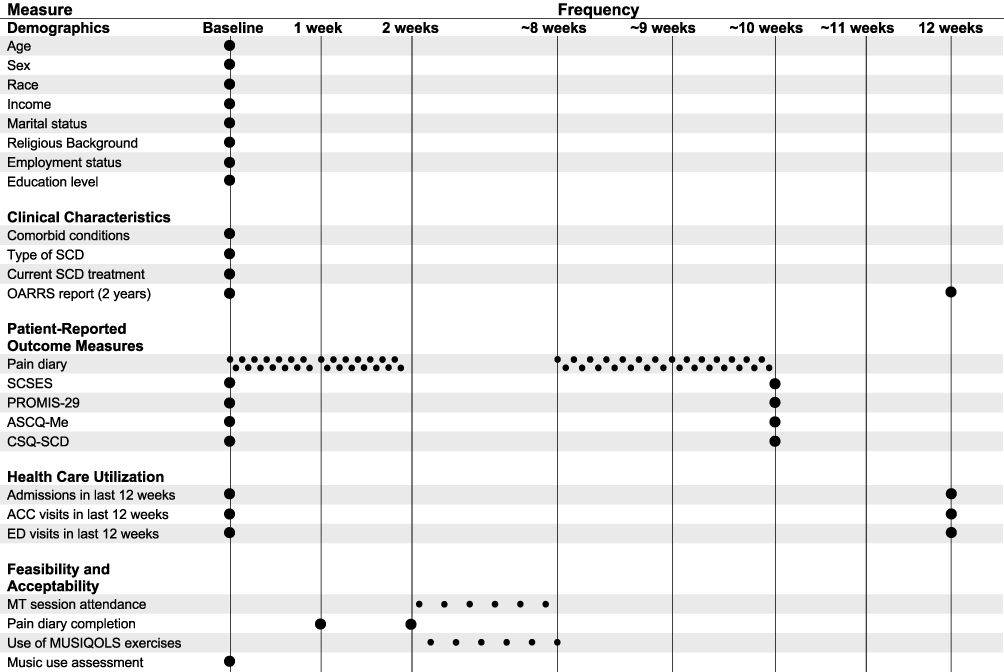 |
Figure 2 Outcome measures utilized in MUSIQOLS. Abbreviations: ACC, Acute Care Clinic; CSQ-SCD, Coping Skills Questionnaire for Sickle Cell Disease; ED, emergency department; MT, music therapy; MUSIQOLS, MUSic therapy to Improve Quality Of Life in Sickle cell disease; OARRS, Ohio Automated Rx Reporting System; PROMIS-29, Patient Reported Outcomes Measurement Information System – 29; SCD, sickle cell disease; SCSES, Sickle Cell Self-Efficacy Scale. |
Self-efficacy was measured using the Sickle Cell Self-Efficacy Scale (SCSES). The SCSES is a nine-item Likert scale developed initially for adults with SCD.35 Clay and Telfair36 reported a Cronbach’s alpha of 0.87 for the nine items, indicating adequate internal consistency and a significant association with personal health care items showing convergent validity.
Quality of life was measured using the Patient-Reported Outcomes Measurement Information System (PROMIS)-29.37 PROMIS measures are scored on a general population-based T-score metric with a mean (M) of 50 and a standard deviation (SD) of 10.37,38 We used the PROMIS-29, which included 4-item subscales of anxiety, depression, fatigue, sleep disturbance, and pain interference, where higher scores indicate greater severity of the specific symptom. The PROMIS-29 also included 4-item subscales measuring the ability to participate in social roles and activities and physical function. Higher scores indicate a greater ability to participate in social roles and activities and less severity for physical function impairment. Different PROMIS measures have been validated in the adult and pediatric populations and have been evaluated in patients with SCD.39–41
Quality of life was further assessed using the Adult Sickle Cell Quality of Life Measurement Information System (ASCQ-Me).42 This study utilized the ASCQ-Me 5-item short forms for emotional impact, pain impact, social functioning impact, and sleep impact. ASCQ-Me is a valid measure and highly reliable for use with adults with SCD.42 ASCQ-Me scores are calculated in the direction of overall health, with higher ASCQ-Me scores indicating better health.
Participants’ use of coping skills was measured using the Coping Skills Questionnaire – Sickle Cell Disease (CSQ-SCD).43 The CSQ-SCD is a modified version of the Coping Strategies Questionnaire developed by Rosenstiel and Keefe.44 Gil et al43 added items to assess coping strategies relevant to SCD (ie taking fluids, heat/cold, massage). The measure consists of 80 items; individuals rate the degree to which they use each strategy to cope with SCD pain on a scale of 0 (never do that) to 6 (always do that). This measure has high internal consistency (subscale alpha coefficients 0.69–0.91) and is commonly used to investigate coping in adults with SCD.45–47
Data Analysis
Demographics and Clinical Characteristics
For the categorical variables, counts and percentages were calculated. To make comparisons between the MT and WLC groups for categorical variables, Fisher’s exact test and the chi-square test of contingency table data were used, as appropriate. To compare the treatment groups for continuous variables (ie age), the “Student” t-test for independent groups was utilized.
To analyze participants’ opioid prescriptions at baseline, the morphine milligram equivalents per day (MME/D) data were extracted from the OARRS report for each participant’s opioid medication prescribed by the outpatient adult SCD team immediately before their randomization date. These data were extracted for all opioid medications prescribed to the participant on the same date before the randomization date, including long-acting and short-acting opioid medications. The sum of all MME/D for all of the participant’s prescribed opioid medications (eg MME/D for oxycodone + MME/D for oxycontin) was calculated. Median, ranges, and frequencies of MME/D dosages at <50 MME/D, 50–100 MME/D, and >100 MME/D were calculated.
Daily Pain
For the purposes of this analysis, the following quantitative items (ie scored 0–10) from the electronic pain diary were analyzed: 1) pain intensity (combining all morning and evening pain intensity values), 2) maximum daily pain intensity (the highest pain score reported on any given day), 3) how much pain got in the way of things the participant wanted to do on a given day, 4) effects of pain on sleep, and 5) effects of pain on mood. Means and standard deviations were initially calculated across all participant scores in a given study period (ie baseline or follow-up). These quantitative variables were chosen for analysis as they were conducive for summarizing trends in participants’ daily pain, pain interference, sleep disturbance, and mood between the baseline and follow-up period. Means and standard deviations were subsequently summarized by study group (ie MT or WLC) based upon the mean values per participant. The mean values of the number of scores provided were also calculated. Further statistical tests to determine differences between groups were not performed.
Feasibility
Number and percent were used to summarize quantitative measures of feasibility, including enrollment, randomization, assessment completion, self-reported use of MT exercises at home, and MT session attendance.
Acceptability
For the qualitative data, all interviews were audiotaped, professionally transcribed, and checked for accuracy. The fourth and fifth authors independently analyzed the interviews using conventional qualitative content analysis.48 In all cases, each assigned transcript was reviewed line-by-line and independently coded using a constant, comparative method of qualitative data analysis.48 All data from the interviews that appeared to be directly related to the study aims were extracted. The coded data were then organized into categories to identify themes. Findings from the independent analyses were consolidated and presented to the study team. The fourth and fifth authors have more than 20 years of experience working with individuals with SCD and have expertise in qualitative methods. Members of the research team reviewed findings for accuracy of generated themes, interpretations of the data, and conclusions.
Preliminary Efficacy
ASCQ-Me and PROMIS scores were converted to t-scores using the Health Measures scoring service.49 To compare the treatment groups for differences in changes in SCSES, PROMIS-29, ASCQ-Me, and CSQ-SCD scores, the “Student” t-test for independent groups was utilized. Statistical significance was defined as p < 0.05. Effect sizes were quantified by Cohen’s d statistic and its 95% confidence interval (95% CI). As this was a feasibility study, no adjustments were made for multiple comparisons and no a priori power analysis was conducted.
Results
Demographics and Clinical Characteristics
The demographics of the study population are described in Table 1. The mean age of all participants was 32.33 years (range 21–57 years), with the majority being female, and 17/24 (70.8%) having HbSS disease. The mean age of MT participants was higher by about 4.5 years, but this was not significantly different from the WLC group. Of the 18 participants who reported household income, 17 (94%) reported earning less than $25,000 a year. The clinical characteristics of the study population are presented in Table 2. The majority (13/24, 54%) of our study population had chronic pain that was not directly attributable to disease complications such as leg ulcers or avascular necrosis (AVN).30 The median MME/D prescribed to participants at baseline was 63.2 MME/D, with prescriptions ranging from 0 MME/D to 216 MME/D. There were no statistically significant differences in demographic or clinical characteristics between the two groups. Additionally, there were no significant differences in changes in healthcare utilization between study groups with respect to ED visits (p = 0.57), hospital admissions (p = 0.86), or acute care clinic visits (p > 0.99).
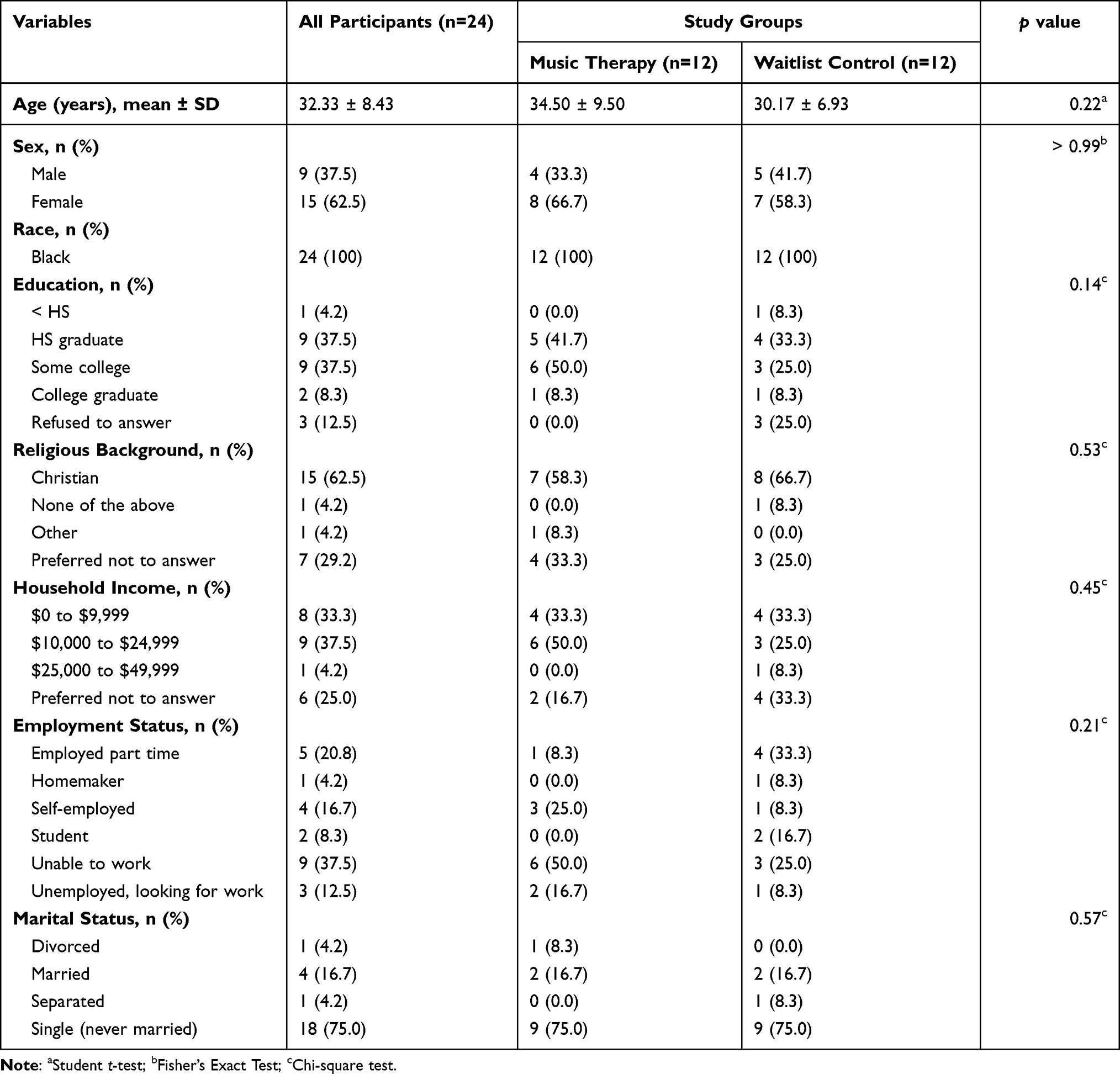 |
Table 1 Demographic Characteristics of the Study Participants |
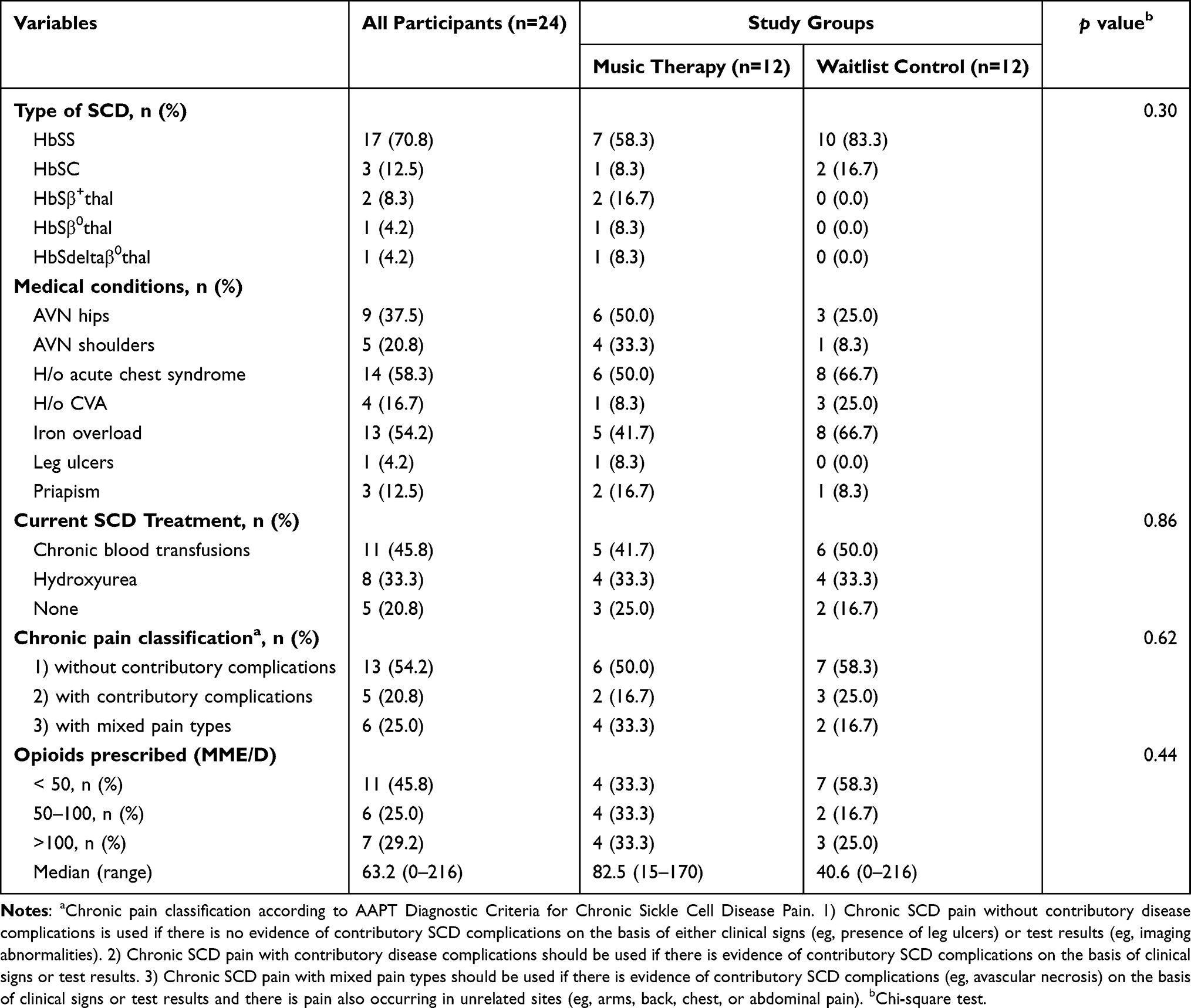 |
Table 2 Clinical Characteristics of the Study Participants |
Daily Pain
Table 3 summarizes the quantitative measures of daily pain by study group. The MT group demonstrated small reductions in pain intensity (baseline M = 5.35, follow-up M = 4.78), maximum daily pain intensity (baseline M = 5.72, follow-up M = 5.08), how much pain got in the way of things the participant wanted to do on a given day (baseline M = 5.23, follow-up M = 4.19), effects of pain on sleep (baseline M = 5.87, follow-up M = 4.77), and effects of pain on mood (baseline M = 5.13, follow-up M = 4.33). By contrast, the WLC group only demonstrated reductions in how much pain got in the way of things the participant wanted to do on a given day (baseline M = 4.81, follow-up M = 4.09) and effects of pain on mood (baseline M = 5.74, follow-up M = 4.71).
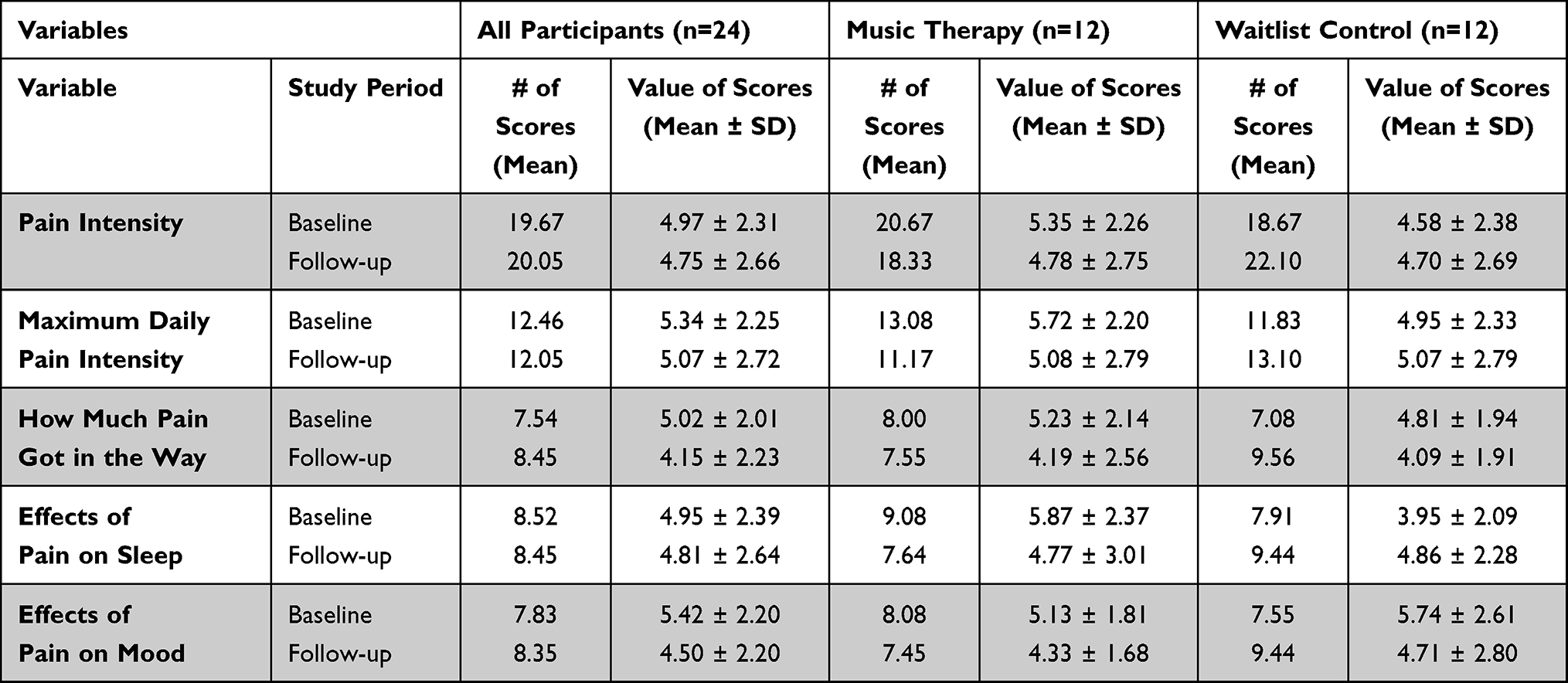 |
Table 3 Daily Pain Scores of the Study Participants |
Feasibility
Initially, 28 patients were invited to participate in this study. Of those, 25 (89%) enrolled, and one (4%) withdrew from participation before randomization (see Figure 3 for the study flow chart). The remaining 24 participants were randomized, with 12 being assigned to each group.
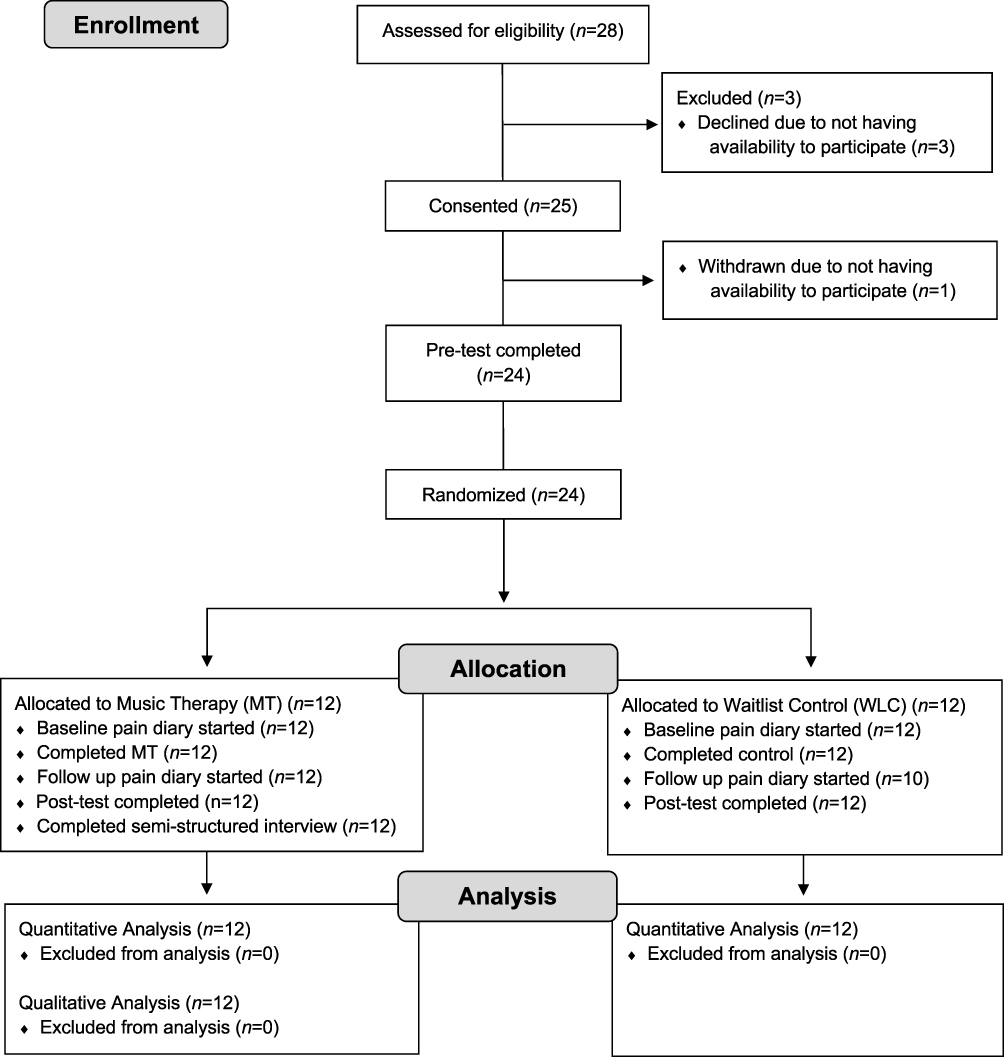 |
Figure 3 Participant flow chart. Abbreviations: MT, music therapy; WLC, waitlist control. |
All pre- and post-test study measures and interviews were completed. There was a high rate of completed pain diary entries, with an average of 19.6/28 (70%) completed entries during the baseline period and 18.4/28 (66%) completed entries during the follow-up period. Nine participants reported technical difficulties related to accessing the pain diary at the start of the follow-up period. The RA was able to assist these participants in regaining access to the pain diary. MT participants completed all six MT sessions. Since all music exercises deployed during the study were accessible via participants’ own devices, we found across all six MT sessions that most MT participants reported using music exercises at home almost every day (40%) or every day (35%). Fewer MT participants reporting using music exercises once or twice per week (12%), never (10%), or more than once per day (3%).
Acceptability
Analysis of the qualitative data identified two overall themes directly related to the MT intervention: 1) participants learned new self-management skills, and 2) MT improved participants’ ability to cope with pain. Table 4 presents themes and representative quotes from the MT participants. Quotes from theme one are presented with participants’ corresponding self-efficacy scores, and quotes from theme two are presented with participants’ corresponding pain interference scores.
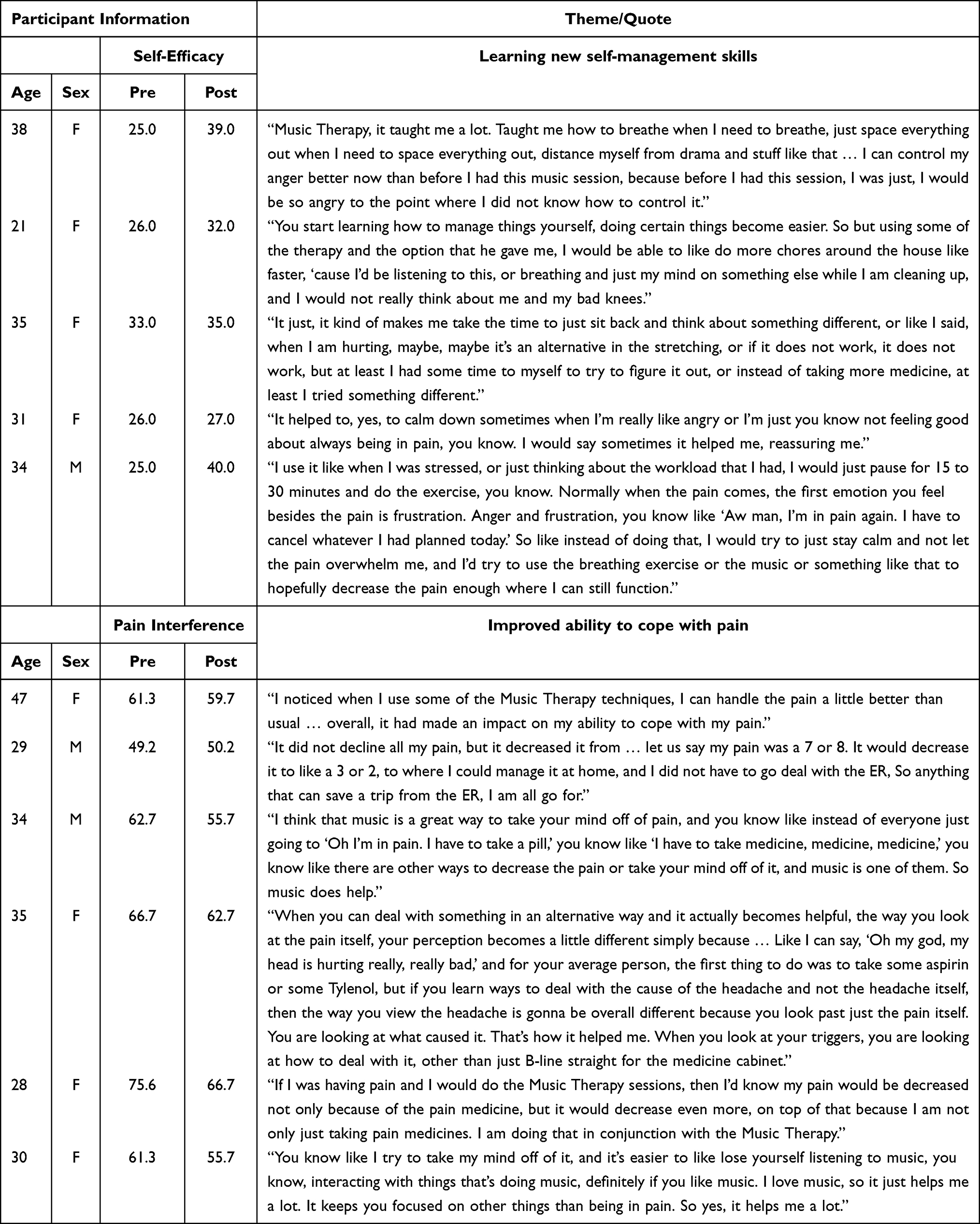 |
Table 4 Themes and Representative Quotes from Music Therapy Participants |
In theme one, participants described what they learned about living with SCD through MT and how perceptions of pain can be influenced by refocusing attention. Participants described how MT transported them to different places with imagination and creativity. While listening to music, participants reported forgetting daily problems and thinking of more positive ideas. Although participants reported listening to music before the study, the MT intervention allowed participants to figure out how music could positively influence their pain experience. Participants transitioned from merely listening to music to intentionally incorporating music into their pain management regimens to prevent/lessen other stressful situations and improve quality of life.
Participants also noted how MT provided them with the opportunity to understand relationships among SCD, the body, emotions, and what happens during stressful situations. They discussed using the MT exercises to control their breathing and reduce stress by listening to the beat of the MT exercises, feeling their respirations, and connecting with positive feelings. Additionally, breathing exercises helped participants learn to calm their respirations, gain more self-control, become more relaxed, and improve mood. Some participants even felt compelled to teach others the strategies they learned.
In theme two, participants described how they needed less external intervention, including pain medications and healthcare utilization for pain management when they used MT strategies early. Participants noted that MT reduced their perception of pain, mostly when pain levels were rated at levels of 5–6/10. They attributed this decreased pain level to the reduced stress and anxiety produced from MT exercises. Participants reported how MT reduced their stress immediately after using an MT exercise.
MT also changed how participants thought about their disease’s limitations, leading to perhaps new and more positive thoughts. Participants considered how their pain would not last forever and how some problems could be resolved. Additionally, MT allowed participants to reflect on different aspects of life while providing the opportunity to disconnect from the disease and change self-care perspectives to cope with problematic situations wherein analgesics were not the only way to manage pain. MT provided a broadening of the repertoire of strategies participants had available to cope with painful conditions and understand their pain triggers. For other participants, MT taught them to prioritize their needs by changing the way they looked at pain and managing pain without the use of medications.
Participants also described how MT gave them new insights into their pain experience. These new insights led some participants to change their behaviors for managing stressful situations and the pain crises often attributed to these situations. Moreover, MT provided participants with knowledge about their pain and skills related to breathing techniques and imagery.
Although the prominent themes reflect the positive impact of MT, an important limitation was identified. Time was perceived as a limitation of MT because applying or learning the MT exercises required time to learn and practice, even though the MT exercises could be accessed at any time via smartphone. Participants also expressed a desire for additional time to learn the MT techniques, but they saw that time commitment as part of being better able to manage their own daily activities. The time commitment was also mentioned in a positive context noting that MT resulted in fewer days with pain and the hope of having a better day.
Preliminary Efficacy
Table 5 summarizes the self-efficacy and quality of life scores of the study participants. There were significant differences in baseline scores between participants in the MT and WLC groups. In assessing change scores between the two study groups, MT participants demonstrated significant improvements in self-efficacy (M = 5.42, SD = 5.43, p = 0.008, d = 1.20, 95% CI 0.33 to 2.07), PROMIS sleep disturbance (M = −1.49, SD = 6.68, p = 0.023, d = −0.99, 95% CI −1.84 to −0.15), PROMIS pain interference (M = −2.10, SD = 4.68, p = 0.016, d = −1.06, 95% CI −1.92 to −0.21), and ASCQ-Me social functioning impact scores (M = 2.97, SD = 6.91, p = 0.018, d = 1.05, 95% CI 0.19 to 1.90) compared to WLC participants. There were no significant differences between groups in changes in the other PROMIS measures (ie physical function, anxiety, depression, ability to participate in social roles and activities), ASCQ-Me measures (ie emotional impact, pain impact, sleep impact) or CSQ-SCD measures.
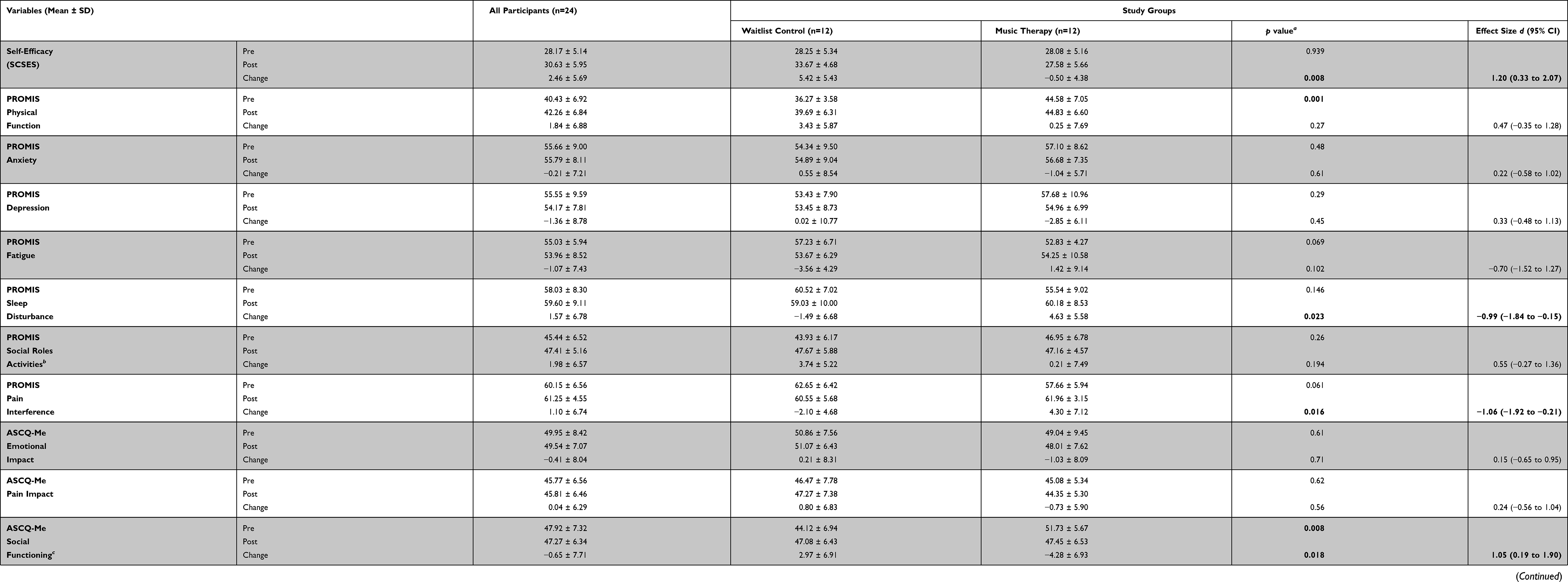 |
Table 5 Self-Efficacy and Quality of Life Scores of the Study Participants |
Discussion
MUSIQOLS was designed to determine the feasibility, acceptability, and preliminary efficacy of a 6-session MT intervention for adults with SCD and chronic pain. The baseline characteristics of our study population are similar to adults with SCD described in other studies. Specifically, our sample of African-American adults was comprised of individuals who 1) were predominantly young adults with a mean age between 30 and 35, 2) had educational attainment less than a college graduate, 3) had a household income less than $25,000 per year, 4) were mostly single, and 5) primarily had the HbSS genotype.1,2,4,50–52 Participants were receiving a wide range of opioid doses ranging from 0 to 216 MME/D, similar to reports in the literature.53 The pain diary responses indicate that study participants faced daily challenges related to the effects of pain on mood, sleep, and things they wanted to do. Further research is needed to determine if these responses are associated with changes in corresponding values on the PROMIS-29 and ASCQ-Me measures.
The high rates of enrollment (89%), retention (96%), MT session attendance (100%), and completion of study assessments (100%) and electronic pain diary entries (M = 70% at baseline, 66% at follow-up) support the feasibility of the MUSIQOLS protocol in adults with SCD and chronic pain. Our enrollment (89%) and attrition (4%) rates were superior to those reported in recent feasibility studies of music therapy interventions with urban African-Americans with chronic pain spanning 12 weeks (56% enrollment, 23% attrition)17 and 8 weeks (77% enrollment, 27% attrition),16 though these studies included larger samples. Several factors may have contributed to the feasibility of MUSIQOLS, including 1) the provision of study stipends and transportation assistance, 2) participants’ history of regular attendance at the study site, 3) frequent communications between study personnel and participants, and 4) a 6-week as opposed to 8–12-week intervention.
Even with the high rates of enrollment, retention, and attendance, there were some challenges to implementation that warrant attention for the future. Some participants had limited experience working with the applications on their mobile devices, and the music therapist often had to demonstrate how to use these applications. Some participants changed phones or lost phone service during the study, requiring the RA to use other contact methods to collect follow up data. Additionally, the music therapist had to offer flexible scheduling opportunities Monday through Friday to accommodate participants’ availability and access to transportation. Investigators in a recent feasibility study of outpatient yoga for chronic pain in SCD noted similar challenges with scheduling, transportation, and reaching participants by phone.54 Thus, it is important to address logistical and technological barriers to engagement among patients with SCD when implementing this intervention.
With regard to acceptability, qualitative interviews indicated that the MT intervention was associated with cognitive behavior changes as participants integrated the music exercises into their methods of coping with SCD to gain more control of managing their disease. MT participants reported gaining skills beyond listening to music, including self-care behaviors, cognitive reframing, dealing with stress, and relaxation. MT provided a remedy that influenced participants’ feelings towards their daily lives and their pain management skills. These findings are consistent with interviews from a recent study investigating music use in adolescents and young adults with SCD. Participants in that study described music listening as being helpful for pain relief, mood regulation, and relaxation.55 Participants’ reports of increased relaxation, improved mood, and improved pain perception were also reminiscent of themes reported in our previous study of a single electronic music improvisation session in adults with SCD experiencing a pain crisis.20 Taken together, qualitative data from these studies support the use of music therapy as a beneficial self-care strategy for adults with SCD.
Although participants still reported using pain medications, they stated that MT helped decrease the pain and make them aware that pain medication was not their only choice in coping with pain. These reports of improved self-management skills, pain management, and using music exercises as an alternative to pain medication are consistent with interviews featured in recent multi-session music therapy interventions in urban African-Americans with chronic pain.16,17
Previous studies have supported the use of music interventions for reducing pain medication use among malignant hematology patients undergoing autologous stem cell transplant56 and patients hospitalized with chronic pain.10 Further analysis is planned to determine whether participants’ self-reported use of pain medication in the electronic pain diary is consistent with their qualitative reports of decreased reliance on pain medication.
In our preliminary assessment of efficacy, MT participants reported improvements in self-efficacy compared to WLC participants. According to Matthie, Jenerette, and McMillan,57 self-efficacy “may be the most important step in improving health outcomes with self-care activities” (p. 264). Self-efficacy is related positively to fewer physical and psychological symptoms36,58 and improved quality of life59,60 among individuals with SCD. Urban African-American adolescent and young adult participants with SCD in a previous study of educational music therapy interventions61 had slight improvements in self-efficacy (M = 1.73) from baseline to the end of the study, but these changes were not significant (p = 0.365). Whereas this prior study utilized interventions focused on educational goals such as medication management, understanding baseline lab values, and creating a pain action plan, MUSIQOLS provided music exercises targeted toward items in the SCSES such as reducing day-to-day pain, preventing symptoms from interfering with daily tasks, and improving sleep. Accordingly, participants’ improvements in self-efficacy may have influenced other quality of life domains.
The reported reductions in pain interference scores among MT participants are especially important given the challenges adults with SCD face in managing pain. Participants’ elevated baseline pain interference scores (M = 60.15, SD = 6.56) in this study were consistent with previous research demonstrating that adults with SCD have more pain interference than the general US population.62 These improvements are particularly meaningful, given that the MT intervention occurred during the period between September and January in the Midwestern United States, when temperature changes often trigger acute pain episodes.63 Quantitative improvements in pain interference were congruent with the content of semi-structured interviews that revealed the various ways MT changed participants’ experience with pain. However, MT participants also discussed several improvements (eg improved mood, decreased stress and anxiety, decreased pain catastrophizing) that were not demonstrated in quantitative measures of depression, anxiety, or subscales of the CSQ-SCD. This disparity between the quantitative and qualitative findings may have been due to a small sample size, respondent burden (particularly in the 80-item CSQ-SCD), or the scales’ inability to measure participants’ experiences meaningfully.
Given that this feasibility study was conducted at a single site containing multiple clinical areas for serving adults with SCD, MUSIQOLS may need to be adapted to serve multiple institutions. These adaptations could include: 1) providing the MT intervention at community sites, particularly for SCD centers serving large geographic areas; 2) implementing the MT intervention virtually and providing resources for internet access for participants with poor access to broadband; and 3) implementing strategies to provide services to patients when they are receiving care in various clinical environments (eg emergency medicine, outpatient hematology, inpatient care, and infusion centers) at different locations during the study.
All studies have limitations, and this study is no exception. The primary limitation was the small sample in that 12 participants were randomized to the MT and the WLC groups respectively. The second important limitation was the content of the control condition, as a waitlist control does not provide a control for time and attention. Third, as this was a feasibility study, our ability to examine preliminary efficacy was limited. Indeed, these scores enable us to assess whether participants would complete the measures over time. As such, the generalizability of our preliminary results is limited by the small sample size as well as lack of a more rigorous control condition. Fourth, there was a risk of bias due to some participants having previous clinical relationships with the first author before study initiation. Fifth, although we were unable to blind participants to their study condition assignments, data was collected by an RA who was blinded to participants’ assignments to help address the potential risk of bias. Finally, study personnel had access to technology and resources that may not be available at other institutions. Therefore, it is important to evaluate the feasibility of MUSIQOLS in different settings where access to resources may differ and patients have not had previous experience with music therapy.
Despite these limitations, there were numerous strengths of this study. These included the: 1) randomized design, 2) use of standardized MT interventions which incorporated participants’ individual music preferences, 3) nuanced understanding of results provided by the integration of quantitative and qualitative data, 4) the ability to measure changes in participants’ symptoms and functioning day-to-day using an electronic pain diary, and 5) the use of specific pain criteria to describe participants’ chronic pain status.
Conclusion
Preliminary findings support the feasibility and acceptability of music therapy for home use in adults with SCD and chronic pain. Music therapy may assist adults with SCD in reducing pain interference and improving their sleep, social functioning, and perceived ability to manage their symptoms. This study provides a framework for future music therapy research in adults with SCD and other chronic pain populations. More research is needed to determine the efficacy of this MT intervention. Future randomized controlled trials should include a larger sample size, feature an active control condition, and be conducted in an environment where clinical delivery of MT is not readily available. To address additional research gaps related to music therapy in SCD, investigators should examine 1) whether demonstrated improvements persist at 6 months and 1-year post-intervention; 2) whether the use of music exercises influences the use of pain medication; 3) whether early intervention with music therapy influences the development of chronic pain in youth with SCD; and 4) the comparative effectiveness of music therapy virtually versus in-person.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, SRM. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Ethics Approval and Informed Consent
This study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board (Date: 5/1/2018 No: STUDY20180101). Written, informed consent was obtained from all participants. The study is registered in clinicaltrials.gov (NCT03556657). This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Participants signed informed consent regarding publishing their data and interview content.
Acknowledgments
We thank the individuals with SCD who participated in this study. We would also like to thank the following collaborators on this study: The Adult SCD Team: Tara Alin, CNP, Santina Ciarallo, CNP, Maranda Lumpkin, Tiffany Cousino, LISW, Rene Crooker, BSN, OCN, and Brandi Griffin, BSN, RN; Research Advisors: Deforia Lane, PhD, MT-BC, Seneca Block, MA, MT-BC, and Sara Debanne, PhD; Research Assistants: Cara Smith, MT-BC, Tracey L. Baker (transcriptionist); The Emory University Pain Diary Development Team: Ashley Griffin, Kolanda Sanders. We especially appreciate the support of Nancy McCann and Anita Louise Steele, MM, MT-BC.
Funding
This work was supported by the Kulas Foundation in Cleveland, OH [Grant no. K16059M]. Nitya Bakshi is supported from a grant from the National Heart, Lung and Blood Institute of the NIH (1K23HL140142). The content is solely the authors’ responsibility and does not necessarily represent the official views of the National Institutes of Health. The funding organizations had no role in the study design or decision to submit the paper to this journal for publication.
Disclosure
The authors declare that they have no competing interests.
References
1. Smith WR, Penberthy LT, Bovbjerg VE, et al. Daily assessment of pain in adults with sickle cell disease. Ann Intern Med. 2008;148(2):94–101. doi:10.7326/0003-4819-148-2-200801150-00004
2. Levenson JL, McClish DK, Dahman BA, et al. Depression and anxiety in adults with sickle cell disease: the PiSCES project. Psychosom Med. 2008;70(2):192–196. doi:10.1097/PSY.0b013e31815ff5c5
3. Molock SD, Belgrave FZ. Depression and anxiety in patients with sickle cell disease: conceptual and methodological considerations. J Heal Soc Policy. 1994;5(3–4):39–53. doi:10.1300/J045v05n03_04
4. McClish DK, Penberthy LT, Bovbjerg VE, et al. Health related quality of life in sickle cell patients: the PiSCES project. Health Qual Life Outcomes. 2005;3:50. doi:10.1186/1477-7525-3-50
5. Lee S, Vania DK, Bhor M, Revicki D, Abogunrin S, Sarri G. Patient-reported outcomes and economic burden of adults with sickle cell disease in the United States: a systematic review. Int J Gen Med. 2020;13:361–377. doi:10.2147/IJGM.S257340
6. Gil KM, Porter L, Ready J, Workman E, Sedway J, Anthony KK. Pain in children and adolescents with sickle cell disease: an analysis of daily pain diaries. Child Heal Care. 2000;29(4):225–241. doi:10.1207/S15326888CHC2904_1
7. American Music Therapy Association. AMTA Official Definition of Music Therapy. Available from: https://www.musictherapy.org/.
8. Bradt J, Dileo C, Magill L, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev. 2016;2016(8). doi:10.1002/14651858.CD006911.pub3
9. Lopez G, Christie AJ, Powers-James C, et al. The effects of inpatient music therapy on self-reported symptoms at an academic cancer center: a preliminary report. Support Care Cancer. 2019;27(11):4207–4212. doi:10.1007/s00520-019-04713-4
10. Guétin S, Giniès P, Siou DKA, et al. The effects of music intervention in the management of chronic pain: a single-blind, randomized, controlled trial. Clin J Pain. 2012;28(4):329–337. doi:10.1097/AJP.0b013e31822be973
11. Kenny DT, Faunce G. The impact of group singing on mood, coping, and perceived pain in chronic pain patients attending a multidisciplinary pain clinic. J Music Ther. 2004;41(3):241–258. doi:10.1093/jmt/41.3.241
12. Lee JH. The effects of music on pain: a meta-analysis. J Music Ther. 2016;53(4):430–477. doi:10.1093/jmt/thw012
13. Gutgsell KJ, Schluchter M, Margevicius S, et al. Music therapy reduces pain in palliative care patients: a randomized controlled trial. J Pain Symptom Manage. 2013;45(5):822–831. doi:10.1016/j.jpainsymman.2012.05.008
14. Mcconnell T, Scott D, Porter S. Music therapy for end-of-life care: an updated systematic review. Palliat Med. 2016;30(9):877–883. doi:10.1177/0269216316635387
15. Li Y, Xing X, Shi X, et al. The effectiveness of music therapy for patients with cancer: a systematic review and meta-analysis. J Adv Nurs. 2020;76(5):1111–1123. doi:10.1111/jan.14313
16. Bradt J, Norris M, Shim M, Gracely EJ, Gerrity P. Vocal music therapy for chronic pain management in inner-city African Americans: a mixed methods feasibility study. J Music Ther. 2016;53(2):178–208. doi:10.1093/jmt/thw004
17. Low MY, Lacson C, Zhang F, et al. Vocal music therapy for chronic pain: a mixed methods feasibility study. J Altern Complement Med. 2020;26(2):113–122. doi:10.1089/acm.2019.0249
18. Vinayak S, Dehkhoda F, Vinayak R. The effect of music therapy on sleep quality of cancer patients undergoing chemotherapy or radiotherapy: a randomized control trial. J Soc Sci. 2017;6(4):734–743. doi:10.25255/jss.2017.6.4.734.743
19. Chang-Lit W, Loewy J, Fox J, Grabscheid E, Fogel J. The role and effect of the comprehensive music therapy in project sleep: a multi disciplinary quality improvement project. J Sleep Sleep Disord Res. 2018;1(2):26–41. doi:10.14302/issn.2574-4518.jsdr-17-1785
20. Rodgers-Melnick SN, Matthie N, Jenerette C, et al. The effects of a single electronic music improvisation session on the pain of adults with sickle cell disease: a mixed methods pilot study. J Music Ther. 2018;55(2):156–185. doi:10.1093/jmt/thy004
21. Williams H, Tanabe P. Sickle cell disease: a review of nonpharmacological approaches for pain. J Pain Symptom Manage. 2016;51(2):163–177. doi:10.1016/j.jpainsymman.2015.10.017
22. Anie KA, Green J. Psychological therapies for sickle cell disease and pain. Cochrane Database Syst Rev. 2015;2015(5). doi:10.1002/14651858.CD001916.pub3
23. Sil S, Lai K, Lee JL, et al. Preliminary evaluation of the clinical implementation of cognitive-behavioral therapy for chronic pain management in pediatric sickle cell disease. Complement Ther Med. 2020;49:102348. doi:10.1016/j.ctim.2020.102348
24. Badawy SM, Abebe KZ, Reichman CA, et al. Comparing the effectiveness of education versus digital cognitive behavioral therapy for adults with sickle cell disease: protocol for the cognitive behavioral therapy and real-time pain management intervention for sickle cell via mobile applications (CaRISMA) Study. JMIR Res Protoc. 2021;10(5):e29014. doi:10.2196/29014
25. McClellan CB, Schatz JC, Puffer E, Sanchez CE, Stancil MT, Roberts CW. Use of handheld wireless technology for a home-based sickle cell pain management protocol. J Pediatr Psychol. 2009;34(5):564–573. doi:10.1093/jpepsy/jsn121
26. Schatz J, Schlenz AM, McClellan CB, et al. Changes in coping, pain, and activity after cognitive-behavioral training: a randomized clinical trial for pediatric sickle cell disease using smartphones. Clin J Pain. 2015;31(6):536–547. doi:10.1097/AJP.0000000000000183
27. Thomas VJ, Dixon AL, Milligan P, Thomas N. Cognitive-behaviour therapy for the management of sickle cell disease pain: an evaluation of a community-based intervention. Br J Health Psychol. 1999;4(3):209–229. doi:10.1348/135910799168588
28. National Center for Complementary and Integrative Health. Pilot studies: common uses and misuses. NCCIH; 2021. Available from: https://www.nccih.nih.gov/grants/pilot-studies-common-uses-and-misuses.
29. Creswell J. A Concise Introduction to Mixed Methods Research. SAGE Publications Ltd; 2015.
30. Dampier C, Palermo TM, Darbari DS, Hassell K, Smith W, Zempsky W. AAPT diagnostic criteria for chronic sickle cell disease pain. J Pain. 2017;18(5):490–498. doi:10.1016/j.jpain.2016.12.016
31. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
32. Rodgers-Melnick SN, Gam K, Debanne S, Little JA. Music use in adult patients with sickle cell disease: a pilot survey study. Music Ther Perspect. 2021;39(1):34–41. doi:10.1093/mtp/miaa026
33. Murphy JL, McKellar JD, Raffa SD, Clark ME, Kerns RD, Karlin BE. Cognitive Behavioral Therapy for Chronic Pain Therapist Manual. Washington, DC: US Department of Veterans Affairs; 2014.
34. Bakshi N, Stinson JN, Ross D, et al. Development, content validity, and user review of a web-based multidimensional pain diary for adolescent and young adults with sickle cell disease. Clin J Pain. 2015;31(6):580–590. doi:10.1097/AJP.0000000000000195
35. Edwards R, Telfair J, Cecil H, Lenoci J. Reliability and validity of a self-efficacy instrument specific to sickle cell disease. Behav Res Ther. 2000;38(9):951–963. doi:10.1016/S0005-7967(99)00140-0
36. Clay OJ, Telfair J. Evaluation of a disease-specific self-efficacy instrument in adolescents with sickle cell disease and its relationship to adjustment. Child Neuropsychol. 2007;13(2):188–203. doi:10.1080/09297040600770746
37. Cella D, Riley W, Stone A, et al. The patient-reported outcomes measurement information system (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi:10.1016/j.jclinepi.2010.04.011
38. Irwin DE, Stucky BD, Thissen D, et al. Sampling plan and patient characteristics of the PROMIS pediatrics large-scale survey. Qual Life Res. 2010;19(4):585–594. doi:10.1007/s11136-010-9618-4
39. Badawy SM, Thompson AA, Liem RI. Beliefs about hydroxyurea in youth with sickle cell disease. Hematol Oncol Stem Cell Ther. 2018;11(3):142–148. doi:10.1016/j.hemonc.2018.01.001
40. Dampier C, Barry V, Gross HE, et al. Initial evaluation of the pediatric PROMIS®health domains in children and adolescents with sickle cell disease. Pediatr Blood Cancer. 2016;63(6):1031–1037. doi:10.1002/pbc.25944
41. Dampier C, Jaeger B, Gross HE, et al. Responsiveness of PROMIS® pediatric measures to hospitalizations for sickle pain and subsequent recovery. Pediatr Blood Cancer. 2016;63(6):1038–1045. doi:10.1002/pbc.25931
42. Keller S, Yang M, Treadwell MJ, Hassell KL. Sensitivity of alternative measures of functioning and wellbeing for adults with sickle cell disease: comparison of PROMIS®to ASCQ-MeSM. Health Qual Life Outcomes. 2017;15(1). doi:10.1186/s12955-017-0661-5
43. Gil KM, Abrams MR, Phillips G, Keefe FJ. Sickle cell disease pain: relation of coping strategies to adjustment. J Consult Clin Psychol. 1989;57(6):725–731. doi:10.1037/0022-006X.57.6.725
44. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain. 1983;17(1):33–44. doi:10.1016/0304-3959(83)90125-2
45. Anie KA, Green J, Tata P, Fotopoulos CE, Oni L, Davies Sc. Self-help manual-assisted cognitive behavioural therapy for sickle cell disease. Behav Cogn Psychother. 2002;30(4):451–458. doi:10.1017/S135246580200406X
46. Anie KA, Steptoe A, Bevan DH. Sickle cell disease: pain, coping and quality of life in a study of adults in the UK. Br J Health Psychol. 2002;7(3):331–344. doi:10.1348/135910702760213715
47. Sanders KA, Labott SM, Molokie R, Shelby SR, Desimone J. Pain, coping and health care utilization in younger and older adults with sickle cell disease. J Health Psychol. 2010;15(1):131–137. doi:10.1177/1359105309345554
48. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
49. Assessment Center. HealthMeasures scoring service; 2021. Available from: https://www.assessmentcenter.net/ac_scoringservice.
50. McClish DK, Smith WR, Dahman BA, et al. Pain site frequency and location in sickle cell disease: the PiSCES project. Pain. 2009;145(1–2):246–251. doi:10.1016/j.pain.2009.06.029
51. Aisiku IP, Penberthy LT, Smith WR, et al. Patient satisfaction in specialized versus nonspecialized adult sickle cell care centers: the PiSCES study. J Natl Med Assoc. 2007;99(8):886–890.
52. Citero de VA, Levenson JL, McClish DK, et al. The role of catastrophizing in sickle cell disease - The PiSCES project. Pain. 2007;133(1–3):39–46. doi:10.1016/j.pain.2007.02.008
53. Karafin MS, Singavi A, Hussain J, et al. Predictive factors of daily opioid use and quality of life in adults with sickle cell disease. Hematology. 2018;23(10):856–863. doi:10.1080/10245332.2018.1479997
54. Bakshi N, Cooley A, Ross D, et al. A pilot study of the acceptability, feasibility and safety of yoga for chronic pain in sickle cell disease. Complement Ther Med. 2021;59:102722. doi:10.1016/j.ctim.2021.102722
55. Solodiuk JC, Jantz B, Fuller M, et al. The use of music by adolescents and young adults with sickle cell disease. Creat Nurs. 2020;26(3):189–196. doi:10.1891/CRNR-D-19-00069
56. Bates D, Bolwell B, Majhail NS, et al. Music therapy for symptom management after autologous stem cell transplantation: results from a randomized study. Biol Blood Marrow Transplant. 2017;23(9):1567–1572. doi:10.1016/j.bbmt.2017.05.015
57. Matthie N, Jenerette C, McMillan S. Role of self-care in sickle cell disease. Pain Manag Nurs. 2015;16(3):257–266. doi:10.1016/j.pmn.2014.07.003
58. Ahmadi M, Shariati A, Jahani S, Tabesh H, Keikhaei B. The effectiveness of self-management programs on self-efficacy in patients with sickle cell disease. Jundishapur J Chronic Dis Care. 2014;3(3). doi:10.5812/jjcdc.21702
59. Adegbola M. Spirituality, self-efficacy, and quality of life among adults with sickle cell disease. South Online J Nurs Res. 2011;11(1):5.
60. Goldstein-Leever A, Peugh JL, Quinn CT, Crosby LE. Disease self-efficacy and health-related quality of life in adolescents with sickle cell disease. J Pediatr Hematol Oncol. 2020;42(2):141–144. doi:10.1097/MPH.0000000000001363
61. Rodgers-Melnick SN, Pell TJG, Lane D, et al. The effects of music therapy on transition outcomes in adolescents and young adults with sickle cell disease. Int J Adolesc Med Health. 2017;31(3):1–14. doi:10.1515/ijamh-2017-0004
62. Master S, Arnold C, Davis T, Shi R, Mansour RP. Anxiety, depression, pain intensity and interference in adult patients with sickle cell disease. Blood. 2016;128(22):1312. doi:10.1182/blood.v128.22.1312.1312
63. Tewari S, Brousse V, Piel FB, Menzel S, Rees DC. Environmental determinants of severity in sickle cell disease. Haematologica. 2015;100(9):1108–1116. doi:10.3324/haematol.2014.120030
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.