Back to Journals » Nature and Science of Sleep » Volume 12
Effects of Mobile Use on Subjective Sleep Quality
Authors Rafique N ![]() , Al-Asoom LI
, Al-Asoom LI ![]() , Alsunni AA
, Alsunni AA ![]() , Saudagar FN
, Saudagar FN ![]() , Almulhim L, Alkaltham G
, Almulhim L, Alkaltham G
Received 11 March 2020
Accepted for publication 27 May 2020
Published 23 June 2020 Volume 2020:12 Pages 357—364
DOI https://doi.org/10.2147/NSS.S253375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sutapa Mukherjee
Nazish Rafique,1 Lubna Ibrahim Al-Asoom,1 Ahmed Abdulrahman Alsunni,1 Farhat Nadeem Saudagar,1 Latifah Almulhim,2 Gaeda Alkaltham2
1Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Ahmed Abdulrahman Alsunni Tel +966 53 525 5577
Fax +966 13 3857 8048
Email [email protected]
Purpose: The objective of this study was to find out the association between mobile use and physiological parameters of poor sleep quality. It also aimed to find out the prevalence of mobile-related sleep risk factors (MRSRF) and their effects on sleep in mobile users.
Materials and Methods: This cross-sectional study was conducted on 1925 students (aged 17– 23yrs) from multiple Colleges of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. The study tools used were Pittsburgh sleep quality index (PSQI) and MRSRF online questionnaires.
Results: The mean age (±SD) of participants was 19.91 ± 2.55 years. Average mobile screen usage time was 8.57± 4.59/24 hours, whereas average mobile screen usage time in the bed after the lights have been turned off was 38.17± 11.7 minutes. Only 19.7% of subjects used airplane mode, while 70% kept the mobile near the pillow while sleeping. The blue light filter feature was used by only 4.2% of the participants. “Screen usage time of ≥ 8 hours” was positively correlated with sleep disturbances and decrease in the length of actual sleeping time (p =0.023 and 0.022). “Using the mobile for at least 30 minutes (without blue light filter) after the lights have been turned off” showed positive correlation with poor sleep quality, daytime sleepiness, sleep disturbances and increased sleep latency (p= 0.003, 0.004 and 0.001). “Keeping the mobile near the pillow while sleeping” was also positively correlated with daytime sleepiness, sleep disturbances and increased sleep latency (p =0.003, 0.004 and 0.001).
Conclusion: This study concludes that using mobile screen ≥ 8 hours/24 hours, using the mobile for at least 30 minutes before sleeping after the lights have been turned off and keeping the mobile near the pillow are positively associated with poor sleep quality. Moreover, we observed that MRSRF were highly prevalent amongst the mobile users.
Keywords: mobile use, sleep quality, mobile-related sleep risk factors
Introduction
Sleep is a physiological state of unawareness which is regulated homeostatically.1 Almost one-third of our lives are spent while sleeping.2 Sleep plays an important role in cognitive and physical functions, cellular toxin removal, disease prevention and restoration of both mind and body.3–5 A major decline in the sleep hours and its strong correlation with obesity, diabetes, and other chronic debilitating diseases have been documented in the past 20–30 years.5,6
Proper sleep is especially important for children and adolescents.6 Lack of sleep in adolescents is becoming an important health issue worldwide.7 Many factors can affect sleep hygiene8 but the role of mobile use in causing sleep problems in adolescence has gained huge attention in the past few years.9 A recent review by Sohn et al reported that one in every four children and young people are suffering from Problematic cell phone use (PSU), which is linked to depression, anxiety and poor sleep quality.10 Current metaanalysis by Carter et al showed that bedtime use of media devices was positively associated with poor sleep quality and excessive daytime sleepiness.11
Mobile use at bedtime (after the lights have been turned off), can cause poor sleep quality (PSQ) by various mechanisms.12 Due to technology revolution, most of the mobile phone users now have smartphones which enable them to access internet and social networks, watching videos, online chatting and playing games.13 This results in exposure to stimulating content, mobile phone overuse and phone addiction thus contributing to hyper arousal in pre bedtime period and poor sleep quality.14
A major factor which can contribute to PSQ is the blue light emitted by screens of mobile phones.15 This blue light can decrease the production of melatonin, the hormone which controls the sleep/wake cycle or circadian rhythm. Reduction in melatonin makes it difficult to fall and stay asleep.16 Some studies have found that exposure to blue light increases brain alertness17 and can stimulate cognitive functions, which in turn can lead to PSQ.18
Moreover, the mobile phones receive and transmit the signals through radiofrequency electromagnetic fields (RF-EMFs).19 It is well documented that RF-EMFs can pass through the skull, and reach the brain.20 Therefore, this technology may pose dangers for human health, of particular interest are its effects on sleep parameters and sleep electroencephalogram (EEG).21 Some studies have reported that RF-EMFs exposure can result in changes in EEG during rapid eye movement (REM) sleep, non-REM sleep, and sleep latency.22–24 All these findings further strengthen the role of mobile in causing PSQ.
Limited availability of the data regarding the “Prevalence of mobile use and its association with sleep quality in the Saudi population” compelled us to design this project. To our knowledge, the current study recruited the largest number of samples of young Saudi population for investigating the link between mobile phone use and sleep quality. We hypothesize that a positive association exists between mobile use and poor sleep quality. We also aimed to find out the prevalence of mobile-related sleep risk factors (MRSRF) in mobile users and their effects on sleep, ie, using mobile before sleeping after the lights have been turned off, not enabling airplane mode on mobiles, putting the mobiles near or below the pillows and bedside while sleeping. As no previous studies are available to highlight these important findings.
Materials and Methods
This cross-sectional study was conducted from January 2018 till August 2019 on 1925 students (aged 17–23yrs) from multiple colleges of Imam AbdulRahman Bin Faisal University, Dammam (IAU).
Sample size calculation was done by using open source epidemiologic statistics for public health tools software (accessed at: http://epitools.ausvet.com.au/content.php?page=1Proportion&Proportion). The calculation was based on estimated prevalence of poor sleep quality in mobile users in a target population of 5000 students and desired precision as 0.02 (2%), confidence interval as 0.95 (95%). The calculated sample size was 2017.
The study tool included two questionnaires: mobile-related sleep risk factors Questionnaire (MRSRF) and Pittsburg sleep quality index (PSQI) (Supplementary material).
Identification of Mobile-Related Sleep Risk Factors (MRSRF)
This online questionnaire (generated by using Google forms) was designed by the authors based on relevant required information, extracted from few previous studies.8,13,14,21 The face validity of the questionnaire was confirmed by professors of physiology and respiratory therapy at IAU, whereas test retest technique was used to verify the reliability (interval of three weeks) with a group of 30 students (P = 0.002; r = 0.84).
MRSRF Questionnaire includes seven items which focus on the following areas: Total duration of mobile use/day, using mobile while in the bed when the lights have been turned off, using blue light filters on mobile, keeping the mobile under pillow, keeping the mobile 2 meters away from the bed and putting the mobile on airplane mode while sleeping.
Identification of Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI)
Various questionnaires are used to identify the sleep quality. But PSQI has been found to be most effective in terms of reliability and validity. It includes 19 self-rated items, which focus on seven main areas including: subjective sleep quality, sleep latency (time taken to fall asleep), sleep duration, habitual sleep efficiency (the ratio of total sleep time to time in bed), sleep disturbances, the use of sleep-inducing medicines and daytime dysfunction.25
PSQI Scoring
The PSQI includes a scoring key for calculating a patient’s seven subscores, each of which ranges from 0 to 3.
- A score of 0 indicates no difficulty.
- A score of 3 indicates severe difficulty.
The 7 component scores are then added to make a global score with a range of 0–21.
- A score of 0 means no difficulty.
- A score of 5 or more indicates poor sleep quality.
- A score of 21 means severe difficulties in all areas.
- (The higher the score, the worse the quality).
Data Collection
Data were collected by convenience sampling technique, and response rate was 38.5%, as 1925 out of 5000 students volunteered and completed the questionnaire. A five minutes briefing session was given in the class to explain the rational of study and terminologies used in the questionnaire (Average strength of students/class was 50). The online questionnaire was shared with each class on their WhatsApp groups, and a time of 8 minutes was provided to the students to fill the questionnaire. The students were assured about the confidentiality of their personal information.
Inclusion Criteria
- The students between 17 and 26 years who were willing to participate in the study.
- The students who use mobile phone daily, even if they use it for a brief moment.
Exclusion Criteria
The students suffering from
- Any diagnosed sleep disorder.
- Any diagnosed chronic respiratory problem (including nasal congestion, chest infections, asthma, adenoids, allergic rhinitis)
- Any chronic physical or mental illness, affecting their sleep.
- Using any prescription medication for at least last 3 months.
Finally, 156 students were excluded, and 1925 were selected.
Ethical approval of the study was taken by Deanship of Scientific Research College of Medicine (IAU).
Statistical Analysis
The data were analyzed using Statistical Package for Social Sciences (SPSS) for Windows, Version 20.0. Descriptive statistics were used to determine the demographic data.
Comparison of sleep quality and sleep parameters in the participants with various “Mobile-related sleep risk factors” (MRSRF) was done by using Cross tab Chi square test for nominal variables, and independent t test for qualitative data. A p value of <0.05 was considered statistically significant.
Correlation of Poor sleep quality and various sleep parameters with MRSRF was done by using Pearson and Spearman tests.
Binary regression analysis test was run using the quality of sleep (poor PSQI>5 versus good PSQI<5) as the dependent variable and the following variables were the independent factors: age, gender, screen usage time >8 hours, using the mobile phone during two hours before sleep, using mobile in bed after lights are turned off, duration of cell phone use after the lights are turned off (minutes), keeping the mobile phone near the pillow while sleeping.
A shapiro-Wilk’s test (p>0.05) and visual inspection of histogram showed that the data were approximately normally distributed.
Results
The mean age (±SD) of participants was 19.91 ± 2.55 years. Number of female participants was 1502 (77%), whereas the number of male participants was 423 (21%). 98% of the participants owned smart phones. Average screen usage time was 8.57±4.59/24 hours, and 38% of the participants reported of using mobile for more than 8/24 hours. Almost 88.7%of the subjects were using the mobile after the lights have been turned off with an average screen usage time of 38.17±11.7 minutes. Out of these 88.7% subjects, 84.5% were not using the blue light filters on their mobiles. Average time spent on watching videos was 1.8±1.74 hours. Poor sleep quality was seen in 33% of males and 37% of females. Comparison of these parameters between male and female subjects is given in Table 1.
 |
Table 1 Comparison of Screen and Sleep-Related Parameters, Between Male and Female Subjects |
Prevalence of mobile usage, and various MRSRF are shown in Table 2. Only 19.7% of subjects used airplane mode, while 70% kept the mobile near the pillow while sleeping. The blue light filter feature was used by only 4.2% of the participants. It was observed that the greater number of females as compared to males keep the mobiles near their pillow while sleeping (p = 0.029). Whereas the number of females who use airplane mode on their mobiles while sleeping was greater than the number of males using this function (p = 0.021).
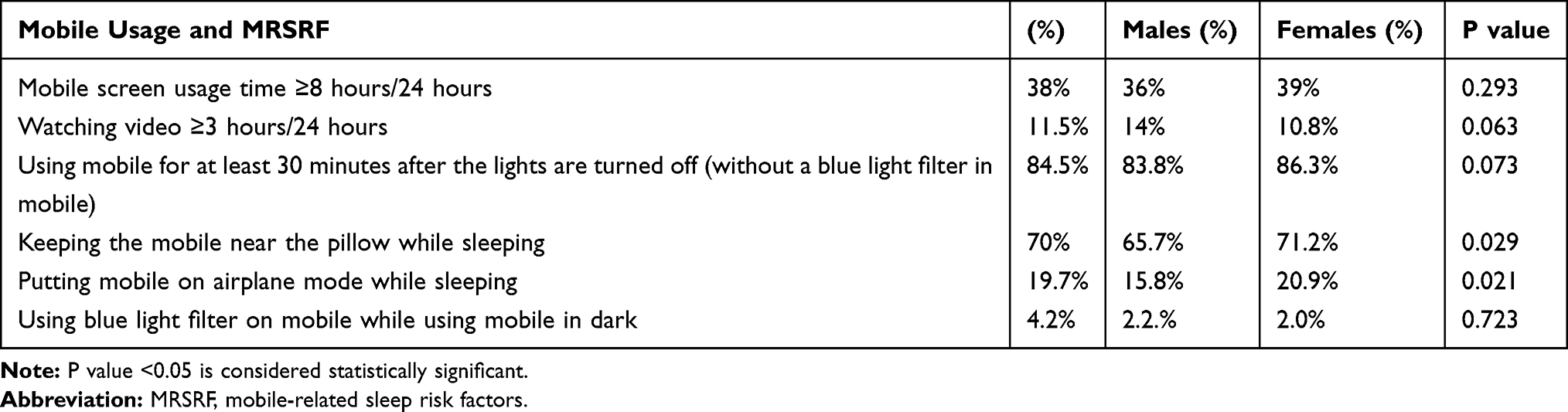 |
Table 2 Prevalence of Mobile Usage and “Mobile-Related Sleep Risk Factors” in Study Participants |
Comparison of sleep quality in the participants with various MRSRF is shown in Table 3. Data indicated that the subjects who use the mobile after the lights have been turned off for at least 30 minutes (without a blue light filter in mobile), and who put the mobile near their pillow while sleeping have a statistically significant poor sleep quality (P=0.001, 0.001) respectively.
 |
Table 3 Comparison of Sleep Quality in the Participants with Various “Mobile-Related Sleep Risk Factors” |
Further analysis revealed a strong positive correlation of poor sleep quality with Using Mobile for at least 30 minutes after the lights are turned off (without a blue light filter in mobile) (p=0.018) Table 4.
 |
Table 4 Correlation of Poor Sleep Quality with Various “Mobile-Related Sleep Risk Factors” |
Correlation of various sleep parameters with MRSRF is highlighted in Table 5. Screen usage time of >8 hours was positively but weakly correlated with sleep disturbances and decrease in the length of actual sleeping time (P value 0.023 and 0.022, respectively). Using the mobile after the lights have been turned off for at least 30 minutes (without a blue light filter in mobile) showed positive but weak correlation with daytime sleepiness, sleep disturbances and increased sleep latency (p= 0.003, 0.004 and 0.001). Keeping the mobile near the pillow while sleeping was also positively but weakly correlated with daytime sleepiness, sleep disturbances and increased sleep latency (p =0.003, 0.004 and 0.001).
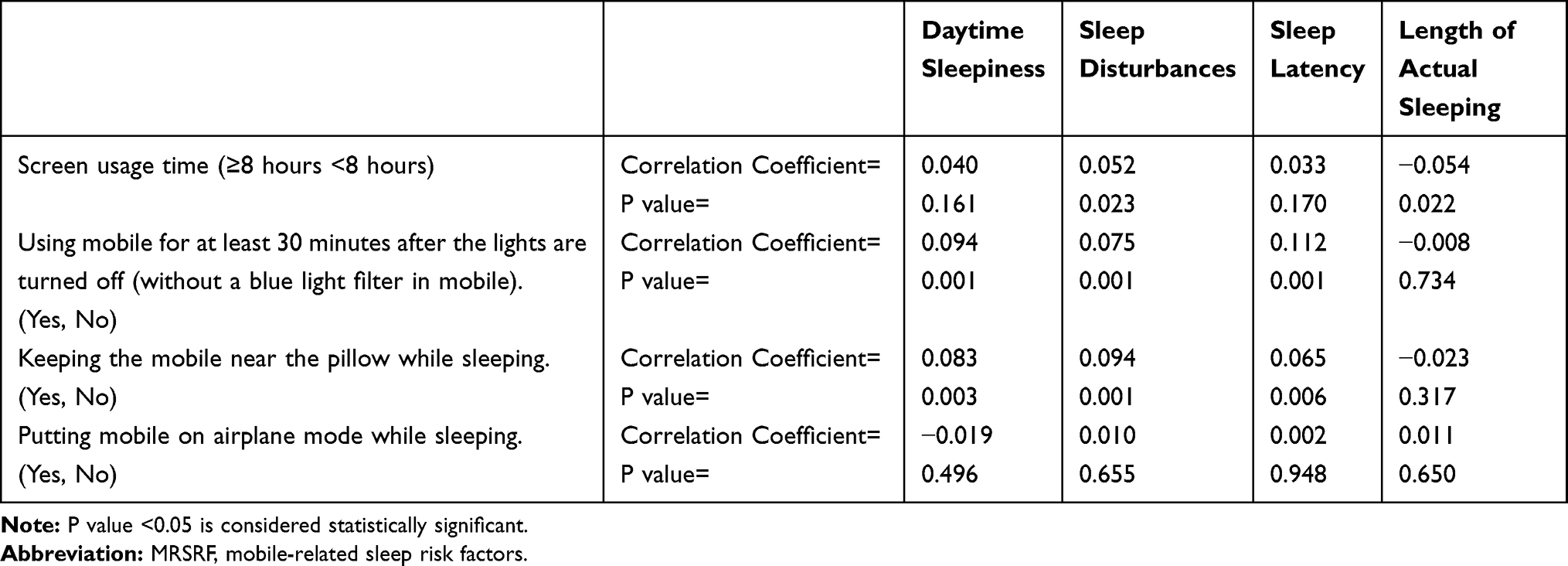 |
Table 5 Correlation of Various Sleep Parameters with “Mobile-Related Sleep Risk Factors” |
Discussion
Our study showed a high prevalence and prolonged duration of mobile use in young adults. Average mobile screen usage time was 8.57±4.59/24 hours, and 38% of the participants reported of using mobile for more than 8/24 hours. Almost similar results have been demonstrated by other authors, Rideout et al and Strasburger found that school-aged children and adolescents spend almost a 7 hours/day in front of a screen.26,27 Moreover, a recent review of literature reported that one in every four children and young people are suffering from (PSU).28
Using Mobile after the lights have been turned off was reported by 88.7% of the subjects (average duration 38 minutes). About 75% of study participants of Munezawa et al reported of using mobile after lights out. Whereas a large study conducted on 90,000 young participants showed that only 17% of their subject use mobile after the lights have been turned off. This difference may be due to the reason that their study population included younger subjects from grades 7 to 12 only, who are under strict supervision of their parents as compared to the older adults.29
One supreme finding of this study was that using mobile for at least 30 minutes after the lights have been turned off (without a blue light filter in mobile) correlates with poor sleep quality, daytime sleepiness, sleep disturbances and increased sleep latency. A study on 844 Flemish subjects (18–94 years old) also revealed that using mobile after lights out negatively affects PSQI scores, sleep latency, sleep efficiency and causes more sleep disturbance and daytime dysfunction.30 Almost similar results were reported by a Japanese study on younger subjects (aged 13 to 19 years).29 But these studies did not mention the exact duration of mobile use; moreover, they have not specified that either or not their subjects were using a blue light filter mode on their mobiles. The data regarding the use of blue light filers on mobile screens are scarce, but our study indicated that only 4.4% of the subjects are using this filter. So we can assume that most of the participants in the above-mentioned studies were also using their mobiles without a blue light filter.
Some recent studies have indicated that the blue light emitted by the mobile screens is the major culprit behind the PSQ in late night mobile users. As most of the mobile screens emit blue light in wave length between 400−495 nm and blue light in the range of 460–480 nm can cause a phase-shifting in human circadian clock by decreasing the production of melatonin.31,32 Reduced melatonin levels have been linked to prolonged sleep latency and sleep disturbances.16 Moreover, exposure to blue light increases brain alertness and stimulates cognitive functions, resulting in PSQ.17,18 Our study findings were also supportive of the above-mentioned facts, we observed that participants who “used the mobile for at least 30 minutes after the lights have been turned off (without a blue light filter),” showed strong positive correlation with poor sleep quality, daytime sleepiness, sleep disturbances and increased sleep latency. Moreover, a comparative study of Mortazavi et al found that using amber blue light filter in the mobiles, significantly improves the sleep quality, but this study used a small sample size of 43 participants only.33 We therefore recommend further case control and experimental studies with larger sample size to confirm these findings.
In addition to the blue light effects of mobile screen, using mobile in pre bed time, ie, surfing the web, playing a game, seeing something exciting on facebook, or reading a negative email can also cause physical and psychological hyperexcitability contributing to hyper arousal state and PSQ.13,14
Another important finding of this study was that putting the mobile near pillow while sleeping caused increased sleep latency, sleep disturbances and daytime sleepiness. These effects may be caused by; a continuous urge to see notifications and updates on the nearly placed phone,14 disturbance created by the vibrations from receiving notifications and messages, heat generated by charging phones and RF-EMF exposure from the mobile phone. RF-EMF exposure can cause changes in EEG during REM and non-REM sleep.21–24 During the sleep time, when the mobile phones are not in use, they still emit RF-EMFs; however, the levels are much lower than that of a phone call. Moreover, the smart phones are constantly scanning for signals, text updates, emails, and software updates. Even notifications that we receive through apps require a certain level of radiation to be released.34,35 These RF-EMFs can cross the skull and reach the brain20 causing neuronal hyper-excitability resulting in various sleep problems.36 The above-mentioned findings may be the underlying reason of the sleep problems (daytime sleepiness, sleep disturbances and increased sleep latency) seen in our study subjects who placed their mobiles near their pillows while sleeping. But further experimental and case control studies are required to confirm this causal relationship.
To our knowledge, this is the first study which also aimed to find out the prevalence of MRSRF in mobile users. To our surprise, there was limited awareness about the possible hazardous effects of the mobile phone on human health, especially on sleep. As 88.7% of the subjects mentioned that they used mobile for at least 30 minutes after the lights are turned off, blue light filter feature was used by only 4.2% of the participants. Only 19.7% of the subjects used airplane mode, whereas 70% kept the mobile near their pillow while sleeping. Although we consider smartphone use to be a source of PSQ, many adolescents mistakenly believe that these media facilitate them to sleep.37 It is therefore strongly recommended that health authorities should conduct seminars and awareness sessions in schools, colleges and universities. And students should be educated about the “hazardous effects of mobile phone use on sleep” and should be encouraged to implement the safety practices to prevent these effects.
This study incorporated a large sample size and showed a positive association between bedtime mobile use and poor sleep quality. It also provided an insight into the causal relationship between mobile use and poor sleep quality, ie, hazardous effects of RF-EMFs and blue light emitted from the mobiles phones on sleep. But due to study limitations, and lack of objective measures we were not able to measure these effects directly. So we recommend further experimental and case control studies to probe the role of these causal factors, especially (RF-EMF and Blue light emitted from mobile screens), in causing poor sleep quality.
Conclusions
This study concludes that
- “Using the mobile for at least 30 minutes (without blue light filter) after the lights have been turned off” results in poor sleep quality, daytime sleepiness, sleep disturbances and increased sleep latency.
- “Keeping the mobile near the pillow while sleeping” positively correlates with daytime sleepiness, sleep disturbances and increased sleep latency.
- Mobile-related sleep risk factors (MRSRF), ie, “using mobile before sleeping after the lights have been turned off, not using blue light filter, not using airplane mode, putting the mobile near the pillow while sleeping” were highly prevalent amongst the mobile users.
Acknowledgment
The authors are thankful to Dr. Afzal Haq Asif, Dr. Faisal Fahad Essa Alousi, Dr. Hina Khan, Saira Saeed, and Dr. Samina Bashir for their help in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown LK. Can sleep deprivation studies explain why human adults sleep? Curr Opin Pulm Med. 2012;18(6):541–545. doi:10.1097/MCP.0b013e3283596740
2. Webb WB, Friel J. Characteristics of “natural” long and short sleepers: a preliminary report. Psychol Rep. 1970;27:63–66. doi:10.2466/pr0.1970.27.1.63
3. Curcio G, Ferrara M, De Gennaro L. Sleep loss, learning capacity and academic performance. Sleep Med Rev. 2006;10:323–337. doi:10.1016/j.smrv.2005.11.001
4. Davies SK, Ang JE, Revell VL, et al. Effect of sleep deprivation on the human metabolome. Proc Natl Acad Sci. 2014;111:10761–10766. doi:10.1073/pnas.1402663111
5. Cappuccio FP, Elia L, Strazzullo P, et al. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 2010;33:585–592. doi:10.1093/sleep/33.5.585
6. Max H, Kaitlyn W, Steven MA, et al. National Sleep Foundation’s sleep time duration recommendations. Sleep Health. 2015;01:40–43.
7. Owens J. Adolescent Sleep Working Group, Committee on Adolescence. Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics. 2014;134:921–932. doi:10.1542/peds.2014-1696
8. Dagmara D, Frances LC, Patrick M. The role of environmental factors on sleep patterns and school performance in adolescents. Front Psychol. 2015;01:17–24.
9. Duygu A, Bulent A. The effect of mobile phone usage on sleep quality in adolescents. J Neuro Behav Sci. 2018;5:68–71.
10. Sohn S, Rees P, Wildridge B, et al. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: a systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry. 2019;19:356–360. doi:10.1186/s12888-019-2350-x
11. Carter B, Rees P, Hale L, Bhattacharjee D, Paradkar MS. Association between portable screen-based media device access or use and sleep outcomes: a systematic review and meta-analysis. JAMA Pediatr. 2016;170:1202–1208. doi:10.1001/jamapediatrics.2016.2341
12. Mireku M, Barker M, Mutz J, et al. Night-time screen-based media device use and adolescents’ sleep and health-related quality of life. Environ Int. 2019;124:66–78. doi:10.1016/j.envint.2018.11.069
13. Haug S, Castro RP, Kwon M, et al. Smartphone use and smartphone addiction among young people in Switzerland. J Behav Addict. 2015;4:299–307. doi:10.1556/2006.4.2015.037
14. Sahin S, Ozdemir K, Unsal A, et al. Evaluation of mobile phone addiction level and sleep quality in university students. Pak J Med Sci. 2013;29:913–918. doi:10.12669/pjms.294.3686
15. Shechter A, Kim EW, Onge MP, et al. Blocking nocturnal blue light for insomnia: a randomized controlled trial. J Psychiatr Res. 2018;96:196–202. doi:10.1016/j.jpsychires.2017.10.015
16. Chang AM, Aeschbach D, Duffy JF. Evening use of light-emitting e-Readers negatively affects sleep, circadian timing, and next-morning alertness. PNAS. 2015;112:1232–1237. doi:10.1073/pnas.1418490112
17. Lockley SW, Gooley JJ. Circadian photoreception: spotlight on the brain. Curr Biol. 2006;16:795–799. doi:10.1016/j.cub.2006.08.039
18. Daneault V, Hébert M, Albouy G, et al. Aging reduces the stimulating effect of blue light on cognitive brain functions. Sleep. 2014;37:85–90. doi:10.5665/sleep.3314
19. Patel N. Cell phone radiations and its effects in public health - Comparative review study. MOJ Public Health. 2018;7(2):14–17. doi:10.15406/Mojph.2018.07.00197
20. Tattersall JE, Scott IR, Wood SJ, et al. Effects of low intensity radiofrequency electromagnetic fields on electrical activity in rat hippocampal slices. Brain Res. 2001;904:43–53. doi:10.1016/S0006-8993(01)02434-9
21. Loughran SP, Wood A, Barton JM, et al. The effect of electromagnetic fields emitted by mobile phones on human sleep. NeuroReport. 2005;16:1973–1976. doi:10.1097/01.wnr.0000186593.79705.3c
22. Borbely AA, Huber R, Graf T, et al. Pulsed high-frequency electromagnetic field affects human sleep and sleep electroencephalogram. Neurosci Lett. 1999;275:207–210. doi:10.1016/S0304-3940(99)00770-3
23. Mann K, Roschke J. Effects of pulsed high-frequency electromagnetic fields on human sleep. Neuropsychobiology. 1996;33:41–47. doi:10.1159/000119247
24. Wagner P, Roschke J, Mann K, et al. Human sleep under the influence of pulsed radiofrequency electromagnetic fields: a polysomnographic study using standardized conditions. Bioelectromagnetics. 1998;19:199–202. doi:10.1002/(SICI)1521-186X(1998)19:3<199::AID-BEM8>3.0.CO;2-X
25. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
26. Rideout VJ, Foehr UG, Roberts DF. Generation M2. Media in the Lives of 8-To 18-Year-Olds. Henry J Kaiser. Family Foundation; 2010.
27. Strasburger VC. Children, adolescents, obesity, and the media. Pediatrics. 2011;128:201–208.
28. Saling LL, Haire H. Are you awake? Mobile phone use after lights out. Comput Human Behav. 2016;10:101–106.
29. Munezawa T, Kaneita Y, Osaki Y, et al. The association between use of mobile phones after lights out and sleep disturbances among Japanese adolescents: a nationwide cross-sectional survey. Sleep. 2011;34:1013–1020. doi:10.5665/SLEEP.1152
30. Exelmans L, Vanden BJ. Bedtime mobile phone use and sleep in adults. Soc Sci Med. 2016;148:93–101. doi:10.1016/j.socscimed.2015.11.037
31. Lockley SW, Brainard GC, Czeisler CA. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab. 2003;88:502–505. doi:10.1210/jc.2003-030570
32. Ruger M, Hilaire MA, Brainard GC, et al. Human phase response curve to a single 6.5 h pulse of short-wavelength light. J Physiol. 2013;591:353–356. doi:10.1113/jphysiol.2012.239046
33. Mortazavi S, Parhoodeh MA, Hosseini H, et al. Blocking short-wavelength component of the visible light emitted by smartphones’ screens improves human sleep quality. J Biomed Phys Eng. 2018;8:375–380. doi:10.31661/jbpe.v8i4Dec.647
34. Bosquillon JA, Del VF, Delanaud S, et al. Effects of co-exposure to 900 MHz radiofrequency electromagnetic fields and high-level noise on sleep, weight, and food intake parameters in juvenile rats. Environ Pollut. 2020;256:113461. doi:10.1016/j.envpol.2019.113461
35. Cell phone radio frequency radiation. Final Report from Rat Studies. National Toxicology Program, US Department of Health and Human Services; 2018.
36. Ferreri F, Curcio G, Pasqualetti P, et al. Mobile phone emissions and human brain excitability. Ann Neurol. 2006;60:188–196. doi:10.1002/ana.20906
37. Eggermont S, Van BJ. Nodding off or switching off? The use of popular media as a sleep aid in secondary-school children. J Paediatr Child Health. 2006;42:428–433. doi:10.1111/j.1440-1754.2006.00892.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.