")
Back to Journals » International Journal of General Medicine » Volume 16
Effects of Mind-Regulation Acupuncture Therapy on Serum Ghrelin, Gastric Inhibitory Polypeptide, Leptin, and Insulin Levels in Breast Cancer Survivors with Cancer-Related Fatigue: A Randomized Controlled Trial
Authors Li J, Xie J , Guo X, Fu R, Wang Y, Guan X
Received 26 January 2023
Accepted for publication 14 March 2023
Published 21 March 2023 Volume 2023:16 Pages 1017—1027
DOI https://doi.org/10.2147/IJGM.S405977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jinxia Li,1 Jingjun Xie,2 Xiaoqing Guo,1 Ruiyang Fu,1 Yaling Wang,1 Xinjun Guan1
1Huzhou Hospital of Traditional Chinese Medicine, Affiliated to Zhejiang Chinese Medical University, Huzhou, Zhejiang, 313000, People’s Republic of China; 2The First People’s Hospital of Huzhou, Huzhou, Zhejiang, 313000, People’s Republic of China
Correspondence: Jingjun Xie, Email [email protected]
Aim: The aim of this research is to analyze the effects of mind-regulation acupuncture on serum ghrelin, gastric inhibitory polypeptide, leptin, and insulin levels, fatigue, quality of sleep, depression, and quality of life in survivors of breast cancer with cancer-related fatigue.
Methods: Total 136 breast cancer survivors with cancer-related fatigue were randomly allocated to the mind-regulation acupuncture group and the control group in a 1:1 ratio, with 68 cases in each group. Finally, 57 cases each in both groups completed the study. The serum ghrelin, gastric inhibitory polypeptide, leptin, and insulin levels were measured in pre-treatment and post-treatment. The 20-item Multidimensional Fatigue Symptom Inventory, Pittsburgh Sleep Quality Index, Hamilton Depression Scale, and Karnofsky Performance Status were used to evaluate patients’ fatigue, quality of sleep, symptoms of depression, and quality of life, respectively.
Results: In post-treatment, the serum ghrelin, gastric inhibitory polypeptide, leptin, and insulin levels significantly reduced, 20-item Multidimensional Fatigue Symptom Inventory, Pittsburgh Sleep Quality Index, and Hamilton Depression scores were remarkably decreased, whereas the Karnofsky Performance Status scores were significantly increased in mind-regulation acupuncture group and control group comparing to those pre-treatment, while those in mind-regulation acupuncture group changed more significantly. The 20-item Multidimensional Fatigue Symptom Inventory, Pittsburgh Sleep Quality Index, and Hamilton Depression scores were remarkably lower, and remarkably higher Karnofsky Performance Status scores in the mind-regulation acupuncture group were seen than those in the control group.
Conclusion: Mind-regulation acupuncture could reduce serum ghrelin, gastric inhibitory polypeptide, leptin, and insulin levels of breast cancer survivors with cancer-related fatigue. In addition, it alleviates cancer-related fatigue, sleep disturbance, and depression in these survivors and improves their quality of life. Therefore, mind-regulation acupuncture may have potential as an alternative and complementary therapy for breast cancer survivors with cancer-related fatigue.
Keywords: mind-regulation acupuncture, traditional Chinese medicine, cancer-related fatigue, breast cancer, metabolites
Introduction
The age-standardized incidence rate in the world standard population for all cancer cases combined was 186.5/100,000. Cancer cases were reported newly in a crude incidence rate of 293.9/100,000 approximately in China,1 it means that incidence of cancer has increased in recent years. A comprehensive strategy is urgently needed to address the changing cancer burden because of a high mortality rate in China. The number of cancer survivors has risen gradually with the remarkable advances made in the field of medical technology. Cancer-related fatigue (CRF), a subjective feeling caused by the tumor and related treatment, exists throughout the process of tumor onset, progression, treatment, and prognosis evaluation, and is among the most prevalent symptoms in cancer survivors,2 the definition of which will be discussed soon in diagnostic criteria. In recent years, the overall combined prevalence of CRF was 52%,3 inviting increasing attention.
Breast cancer (BRCA), one of the most prevalent malignancies in clinical settings, significantly affects women’s physical and mental health and even endangers their lives. The incidence of BRCA has been on the rise in recent years and ranks among the top malignant tumors in women,4 even BRCA has overtaken lung cancer to become the leading cancer diagnosed globally in 2020.5 According to the 2015 Chinese cancer statistics, among patients diagnosed with cancer and survived in the past five years in China, the number of female BRCA patients took first place.6 According to statistics, 90% of breast cancer survivors develop CRF during or after radiotherapy, chemotherapy, or endocrine therapy.7,8 Therefore, how to alleviate CRF for breast cancer survivors to improve their quality of survival has become a critical issue. Current treatment options for BRCA with CRF include primarily pharmacological and non-pharmacological schemes.9 Most patients choose non-pharmacological treatments due to the fear of pharmacological treatment-related side effects. Acupuncture therapy has an improving effect on fatigue and sleeping quality in patients with BRCA and is easily accepted by them.10,11 The mind-regulation acupuncture (MRA) therapy, which is based on the traditional Chinese medicine (TCM) concept of “mind regulation”, focuses primarily on the acupuncture points in the governor meridian, along with those in the heart meridian of hand-Taiyin and the pericardium meridian of hand-Jueyin, thus exerting mind-regulation and feeling-ease effects. This research analyzed the intervention effects of MRA on CRF in BRCA survivors.
Materials and Methods
Sample Sources
The study approved by the Medical Ethics Committee, Huzhou Hospital of Traditional Chinese Medicine (Approval No.2019-077-A), in compliance with the principles of the Declaration of Helsinki, and all participants provided written informed consent. It was registered in the Chinese Clinical Trial Registry (Registration No. ChiCTR1900028543) and conducted in Huzhou Hospital of Traditional Chinese Medicine of Huzhou from January 2020 to December 2021, and 1 month follow-up. The data of participants were collected in the inpatient department.
Study Design
A random number table was used to generate the random assignment sequence. Clinical participants’ random numbers and grouping information were managed by the research team. Random numbers and grouping information were placed in consecutively numbered envelopes prior to clinical treatment, and subjects were given envelopes in chronological order of inclusion in the study observations and were given the corresponding random numbers and grouping information at the same time. It was difficult to blind to the applicators and patients for the MRA treatment, but this trial was blinded to care providers and scale assessors.
Sample Size Estimation
Sample size was estimated according to the early small sample effective rate, by two-sided hypothesis testing, with the test criterion a = 0.05 (two-sided) and test efficacy β=0.10. Based on the initial evaluation of 86% efficiency in the MRA group and 60% in the control group, the minimum sample required for each group was calculated as 56 cases. Adding 20% of cases to prevent loss, 68 cases in each group, the total sample size was 136 cases. In total, 136 patients with CRF were recruited, which were divided into the MRA and control groups with a 1:1 ratio to show a statistical difference and see how generalizable it was, and 114 patients completed the study. During the course of the study, 4 cases in the MRA group were excluded due to receiving other treatment that may affect the outcomes, 7 cases drop-out due to inadequate treatment; 1 case was excluded due to pregnancy, 6 cases withdrew due to receiving sleeping pills, and 4 cases drop-out due to insufficient treatment in the control group. Finally, the data of these 114 patients was analyzed statistically. The CONSORT flow diagram is shown in Figure 1. No significant difference in pre-treatment general information, including BRCA Stages, age, career, education background, type of treatment and Karnofsky Performance Status (KPS), was seen among the two groups (P > 0.05) (Table 1).
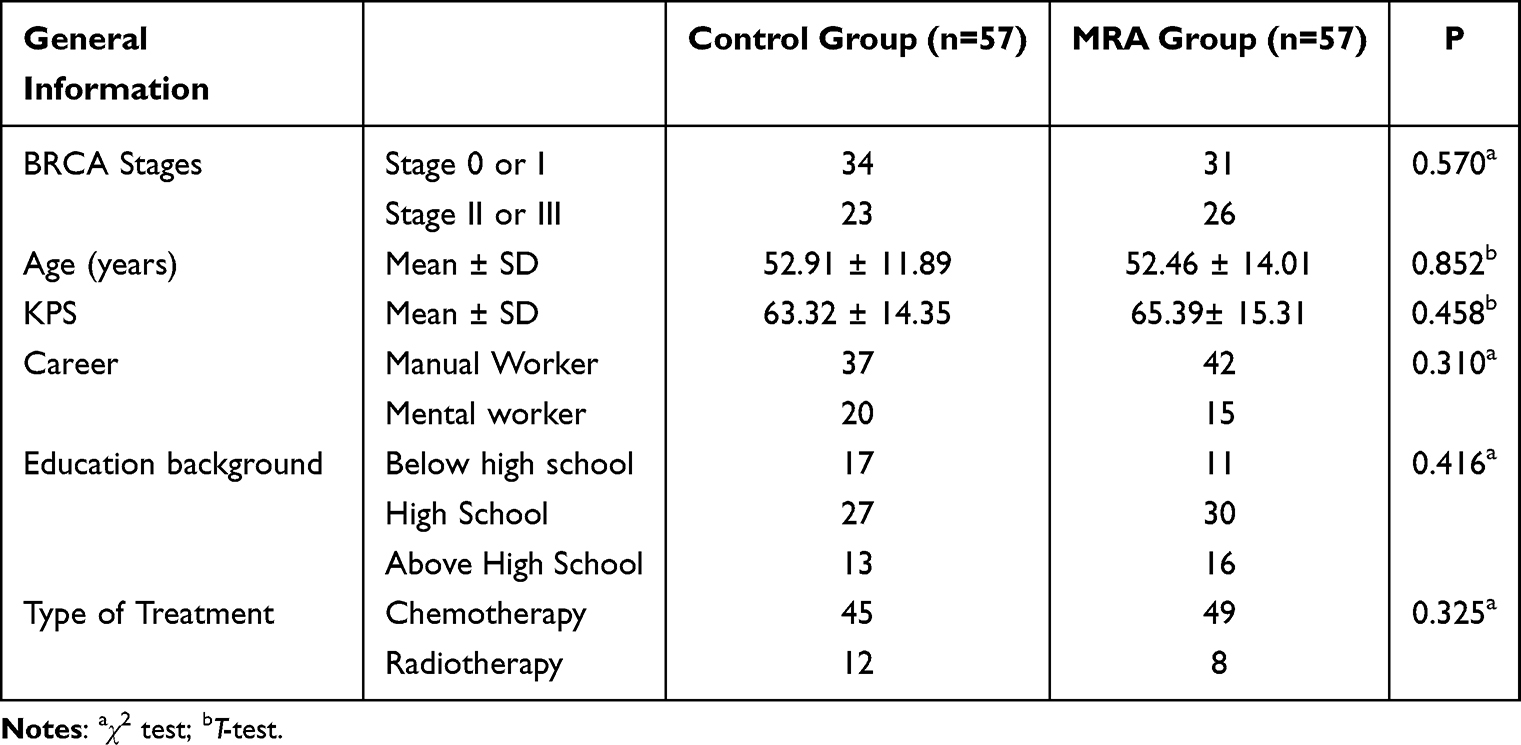 |
Table 1 Pre-Treatment General Information |
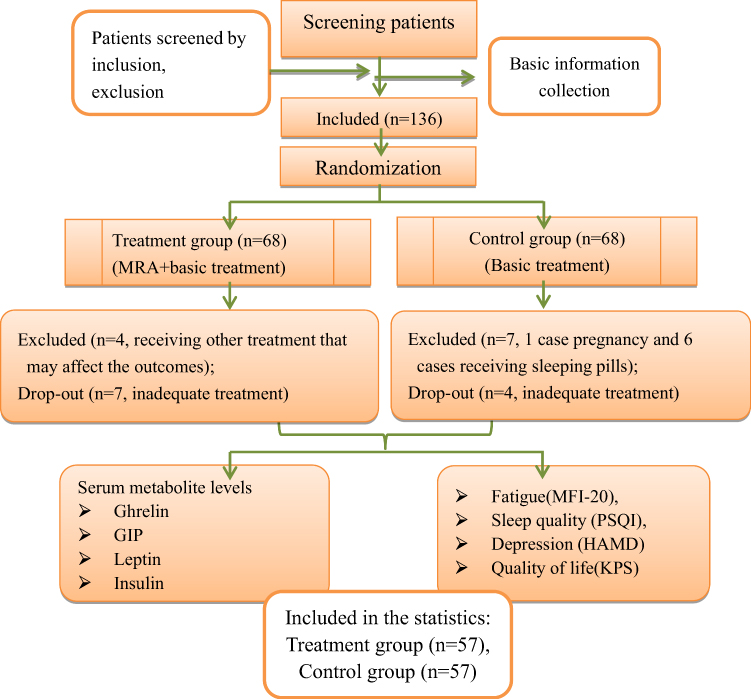 |
Figure 1 CONSORT flow diagram. |
Diagnostic Criteria
Diagnostic Criteria for BRCA
The BRCA patients who were included in this research were selected according to the following diagnostic criteria: (1) the patients were 18 years of age or older female postoperative patients with BRCA (Stage 0–III); (2) they had completed radiotherapy or chemotherapy for cancer; and (3) they were free of cancer metastasis and recurrence at the time of inclusion.
Diagnostic Criteria for CRF
As per the International Classification of Diseases (ICD, 10th edition), CRF is defined as recurrent symptoms of fatigue that persist for more than 2 weeks, accompanied by five or more of the following symptoms: (1) lack of concentration; (2) weakness of the limbs; (3) insomnia or somnolence; (4) lack of enthusiasm, low mood, and energy; (5) failure to recover energy after sleep; (6) short-term memory loss; (4) inability to complete daily activities that were previously competent; (8) emotional reactions such as frustration, irritability, and sadness; (9) difficulty in activities; (10) failure to relieve fatigue within a few hours after resting from activities.
Inclusion, Exclusion, and Drop-Out Criteria
Inclusion Criteria
The inclusion criteria for selecting patients were as follows: (1) patients who met the above diagnostic criteria for BRCA and CRF; (2) patients who had BRCA surgery a year before and were not under chemotherapy or radiotherapy during this study; (3) patients aged 18 to 75 years; (4) patients with a KPS score greater than or equal to 60; and (5) patients who agreed to participate in this study, understood, and signed the informed consent form. Individuals who were not meeting any of the above-mentioned criteria were not included in this study.
Exclusion Criteria
Following were the patient exclusion criteria for this research: (1) patients suffering from grade-IV BRCA; (2) patients with any psychoactive substance or hypnotic sedative administered within 24 hours; (3) patients having concurrent severe chronic diseases of the heart, liver, and kidney or other cancers; (4) patients having a severe cognitive impairment or psychiatric disorders that prevent from cooperation; (5) patients with other physical or pathological fatigue such as chronic fatigue syndrome; (6) patients who have received acupuncture within the past six months; (7) pregnant or lactating women.
Drop-Out Criteria
The patients with any of the following points were considered being dropped out of this study: (1) patients who dropped out voluntarily; (2) patients who had serious adverse reactions during the study and were not suitable to continue to participate in this study; (3) patients who had serious complications or deterioration during the study and required urgent measures.
The reasons and time of drop-out were recorded in detail. In addition, exceeded treatment course was subjected to the efficacy statistics.
Interventions
Patients in the control group received psychological, health, and exercise guidance, along with nutritional support, based on their general conditions. In addition, they were administered an intravenous injection of ShenqiFuzheng (Livzon Pharmaceutical Grouping Limin Pharmaceutical factory; SFDA approval No: Z19990065) (250 mL, once a day, and 5 times a week for consecutive 4 weeks; one treatment course; basic treatment). Medical prescriptions are prescribed by subject physicians and carried out by professionally trained nurses.
Individuals in the MRA group underwent MRA on the basis of the treatment in the control group. The acupuncture points were taken with reference to Acupuncture Therapeutics, including Baihu (GV20), Yintang (GV29), Taichong (LR3), Hegu (LI4), Zusanli (ST36), Sanyinjiao (SP6), and Shenmen (HT7). After routine disinfection of the skin, disposable sterile acupuncture needles (0.30 mm × 50 mm, Dong Bang Brand) were used to stab directly or obliquely at specific acupuncture points in a mild reinforcing–attenuating manner until attaining a needling response. The acupuncture was performed once every 10 minutes, and the needles were removed after 30 minutes of retention (once a day and 5 times a week for consecutive 4 weeks; one treatment course). MRA treatment was performed by a uniformly trained attending physician in Chinese medicine.
Serum insulin, ghrelin, gastric inhibitory polypeptide (GIP), and leptin levels were collected from all participants by a professionally trained nurse on the day of treatment start and at the end of the treatment session by a testing institution not involved in the study. All scales were assessed by therapists who were not involved in the treatment process but were uniformly trained.
Primary Outcome Indicator
Fatigue Symptoms
The 20-item Multidimensional Fatigue Symptom Inventory (MFI-20) consists of 20 items in 5 dimensions: general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue, with 4 items for each dimension. The scores of each item ranged from 1 to 5. The range of the total scores was from 20 to 100, and a highly severe fatigue symptom was indicated by a high total score.
Secondary Outcome Indicator
Measurement of Serum Metabolite Levels
Blood was collected from all subjects before and after treatment and mixed with ethylene diamine tetra acetic acid (EDTA) to prevent clotting. Subsequently, blood samples were centrifuged at 2500 rpm (700 g) for 15 min within 60–90 min to minimize the risk of sample contamination and stored at −80°C. Serum ghrelin, GIP, and leptin levels were measured using ELISA kits. In addition, serum insulin levels were determined by electrochemiluminescence immunoassay.
Sleep Quality
Pittsburgh Sleep Quality Index (PSQI) involves seven dimensions: patients’ sleep latency, sleep disorder, sleep duration, sleep quality, sleep efficiency, daytime dysfunction, and hypnotic drug application. The range of the total PSQI score was from 0 to 21, and the poorest sleep quality was indicated by a higher total score.
Depression Degree
Hamilton Depression Scale (HAMD), containing 24 items, was used to evaluate the depression degree of the patients. A 5-point scale of 0–4 was used for all items: 0, no symptoms; 1, mild symptom; 2, moderate symptom; 3, severe symptom; and 4, very severe symptom. Total scores less than 8 mean normal status; scores from 8 to 20 indicate possible depression; scores from 20 to 35 indicate definite depression; scores more than 35 indicate severe depression. Generally, a higher total score indicates a more severe depressive condition.
Quality of Life
The KPS scale has 10 levels with a total score of 0–100, with higher scores indicating better health status. The initial scores of patients included in this study were all greater than or equal to 60.
Statistical Analysis
Statistical software SPSS22.0 was employed to analyze the complete data of this study. Confidence interval set to 95%, the mean ± standard deviation ( ) expressed the measurement data and data were tested for normality and homoscedasticity. The t-test was employed for the comparison of the two groups of data that conformed to a normal distribution, whereas the Mann–Whitney U-test was used for data not conforming to a normal distribution. Enumeration data were tested by the chi-square test or Fisher’s exact test. In addition, P <0.05 was used as the criterion for statistical difference.
) expressed the measurement data and data were tested for normality and homoscedasticity. The t-test was employed for the comparison of the two groups of data that conformed to a normal distribution, whereas the Mann–Whitney U-test was used for data not conforming to a normal distribution. Enumeration data were tested by the chi-square test or Fisher’s exact test. In addition, P <0.05 was used as the criterion for statistical difference.
Results
Primary Outcome
Fatigue Symptom Evaluation
As we see in Table 2, general fatigue scores, physical fatigue scores, reduced activity scores, reduced motivation scores, mental fatigue scores and MFI-20 total scores were observed insignificant differences (P > 0.05) in pre-treatment between the control group and MRA group. Significant differences (P < 0.05) in general fatigue scores, physical fatigue scores, reduced activity scores, reduced motivation scores, mental fatigue scores and MFI-20 total scores were seen between these two groups in post-treatment, while those in MRA group changed more significantly. In MRA group, general fatigue scores, physical fatigue scores, reduced activity scores, reduced motivation scores, mental fatigue scores and MFI-20 total scores indicated a remarkable decrease (P < 0.05), compared to those in control group at the end of the treatment course (Table 2).
 |
Table 2 Comparison of MFI-20 Between the Control Group and the MRA Group |
Secondary Outcomes
Serum Ghrelin, GIP, Leptin, and Insulin Levels
Patients’ serum ghrelin, GIP, leptin, and insulin levels were measured in pre-treatment and post-treatment. No remarkable difference was seen in the level of pre-treatment serum ghrelin, GIP, insulin, and leptin among the control group and the MRA group (P > 0.05). The level of serum ghrelin, GIP, insulin, and leptin in post-treatment was decreased remarkably (P < 0.01) as compared to those in pre-treatment, while those in MRA group changed more significantly. In the MRA group, the level of post-treatment serum ghrelin, GIP, insulin, and leptin decreased significantly as compared to those in the control group (P < 0.01) (Table 3).
 |
Table 3 Comparison of Serum Ghrelin, GIP, Leptin, and Insulin Levels Between the Control Group and the MRA Group |
Sleep Quality Evaluation
No significant differences were noted in pre-treatment sleep quality scores, sleep latency scores, sleep duration scores, sleep efficiency scores, sleep disorder scores, daytime dysfunction scores, hypnotic drug application scores, and total PSQI scores between the control and MRA group (P > 0.05). In post-treatment sleep quality scores, sleep latency scores, sleep duration scores, sleep efficiency scores, sleep disorder scores, daytime dysfunction scores, hypnotic drug application scores, and total PSQI scores decreased significantly in both groups compared with pre-treatment scores (P < 0.05 or P < 0.01). Post-treatment sleep quality scores, sleep latency scores, sleep duration scores, sleep efficiency scores, hypnotic drug application scores, and total PSQI scores were remarkably decreased in patients of the treatment group as compared to the individuals in the control group (P < 0.05 or P < 0.01). However, no remarkable variations were seen in the post-treatment sleep disorder scores and daytime dysfunction scores between both groups (P > 0.05) (Table 4).
 |
Table 4 Comparison of PSQI Between the Control Group and the MRA Group |
Depression Degree and Quality of Life Evaluation
Between the control group and MRA group, no remarkable differences were seen in HAMD scores and KPS scores before treatment (P > 0.05). A remarkable decrease was observed HAMD scores (P < 0.01), whereas KPS scores increased remarkably (P < 0.01) at the end of the treatment in both groups as compared to the pre-treatment scores, the more, those in MRA group changed more significantly. In comparison to the individuals in the control group, a remarkable decrease of HAMD scores was observed (P < 0.01), whereas KPS scores increased significantly (P < 0.01) after treatment course ending in the MRA group (Table 5).
 |
Table 5 Comparison of HAMD and KPS Between the Control Group and the MRA Group |
Discussion
CRF, also known as tumor-related fatigue, affects patients’ physical functioning during cancer treatment. The physio-pathological mechanisms of CRF are not fully understood. Available studies suggest that possible mechanisms of CRF include elevated pro-inflammatory cytokine levels, hypothalamic–pituitary–adrenal (HPA) axis dysfunction, circadian dysregulation, and muscle atrophy; these mechanisms transmit peripheral immune signals to the brain, affecting neurotransmission pathways and neurotransmitter metabolism, thus, leading to fatigue. However, evidence supporting these mechanisms is relatively limited.12,13 Broad functional alterations in brain areas and networks that modulate executive function are linked to BRCA-related fatigue.14 Fatigue has received relatively little attention and treatment compared to other cancer-related symptoms such as pain and nausea. Some cancer patients are never clinically screened and managed for CRF.15 Evidence on the effects of pharmacological agents for CRF, such as psychostimulants, corticosteroids, testosterone, and melatonin, is limited.16 In recent years, CRF received more and more attention as the prevalence of CRF increasing. As a result, non-pharmacological management strategies have become a research focus.17
CRF is classified as a “consumptive disease” in TCM theory. On the one hand, CRF is caused by the lack of positive qi and the imbalance between qi and blood in the internal organs due to cancer; on the other hand, radiotherapy and chemotherapy, which are considered “attacking methods” in TCM theory, damage the body’s positive qi and cause the deficiency of qi and blood in the internal organs.18,19 Unlike conventional Western medicine, acupuncture therapy for CRF can deal with the functional status of all systems of the human body in an integrated manner and regulate the overall functional status of the human body from multiple aspects, which is effective in CRF, a physical and mental disease with complex etiology, especially in BRCA-related fatigue.20,21 Acupuncture has therapeutic potential in cancer survivors with CRF and may improve their quality of life.22 It has been confirmed to be effective for CRF.23 In addition, female cancer patients are more likely to accept acupuncture therapy.24 The MRA therapy developed in this study, guided by the concept of “integration of form (body) and spirit”, treats patients as a whole with both form and spirit and adjusts patients’ inner balance through acupuncture, thus alleviating their physical and mental fatigue.
The effect of acupuncture on the body is in a multi-linked, multi-pathway, multi-target, and multi-level holistic regulatory manner, which may benignly regulate the disordered metabolic pathways in patients and improve energy metabolism, protein synthesis, and various other chemical reactions in the brain, thus restoring the normal metabolic network. The underlying mechanism of acupuncture therapy may be related to regulating mitochondrial function, coordinating nervous system activity, regulating neurotransmitter production and alleviating immune response.25 Serum ghrelin, GIP, leptin, and insulin levels are associated with both sleep quality and CRF, according to the 2018 NCCN guidelines for the condition, suggesting a potential link between such metabolic markers and CRF.26
Ghrelin is not only a growth hormone secretagogue but also plays a multi-dimensional role in regulating the body’s metabolic balance, inflammatory response, reward feeding, depression and anxiety behavior.27 Ghrelin’s neural conduction in different regions of the hypothalamus affects the appetite, indirectly affects food intake, and participates in the regulation of metabolic disorders under pathological conditions. Gastric inhibitory polypeptide (GIP), also called glucose‐dependent insulinotropic polypeptide (GIP) secreted from enteroendocrine K cells, is one of gastrointestinal peptides that play an important role in response to nutrient ingestion, the regulation of plasma glucose, potentiate glucose-stimulated insulin secretion and involving in insulin resistance. GIP exerts important effects on metabolism.28,29 Insulin is the most important anabolic hormone that promotes carbon energy deposition in the body. Its synthesis, quality control, delivery and action are carefully regulated by highly coordinated intracellular mechanisms. Insulin plays a variety of roles in peripheral tissue parenchyma, the most important of which is the regulation of glucose metabolism. The main function of insulin in muscle and adipose tissue is to increase their uptake of carbon sources and store them to meet the tissue’s energy needs.30 Leptin acts as both a hormone and a cytokine. As a hormone, it plays a key role in regulating energy homeostasis by affecting a variety of endocrine functions and bone metabolism, glucose homeostasis, insulin synthesis and secretion, regulating key functions of energy homeostasis. As a cytokine, leptin promotes inflammatory responses.31,32 It can be seen that Ghrelin, GIP, insulin, and leptin are all closely related to fatigue, poor appetite and insufficient energy intake in patients with CRF. Therefore, we not only selected fatigue degree as the primary indicator but also the serum ghrelin, GIP, insulin, leptin, sleep quality, depression degree, and quality of life as secondary outcome indicators in the study.
The effectiveness of the MRA therapy on fatigue, sleep quality, depression degree, and quality of life among BRCA survivors were evaluated according to objectively accepted assessment criteria, in the meanwhile, the patients’ serum metabolite levels including ghrelin, GIP, insulin, and leptin were measured. The MRA therapy significantly and effectively not only improved the fatigue symptoms but also the sleep quality, depression degree, and quality of life of BRCA survivors compared to the basic treatment. Meanwhile, the results indicated that the MRA therapy significantly reduced the serum ghrelin, GIP, insulin, and leptin levels in patients. The patients’ post-treatment functional status, fatigue symptoms, sleep quality, depression degree, and quality of life were significantly improved. These findings suggest that the MRA therapy can significantly alleviate CRF-related symptoms in BRCA survivors.
From our findings, we concluded that MRA therapy can improve CRF in patients with BRCA by regulating the levels of serum metabolites such as ghrelin, GIP, insulin, and leptin. In addition, it can improve sleep quality and reduce depression. Therefore, MRA can be used as an alternative option for clinical improvement of BRCA survivors’ quality of life. This is basically consistent with the results of some previous studies,11,25,33–38 but differs from them, the MRA therapy adopted in this trial has been improved in the prescription of acupuncture from the perspective of body and mind, emphasizing the importance of MRA, which is a acupuncture method to regulate the mind and spirit, calm the heart, strengthen Qi and eliminate fatigue. Some studies have found that acupuncture can effectively regulate emotional changes and cognitive dysfunction.39 In addition, this study observed the changes of metabolites closely related to CRF, and more objectively evaluated the intervention effect of MRA on CRF. The underlying mechanism of acupuncture therapy may be related to regulating mitochondrial function, coordinating nervous system activity, regulating neurotransmitter production and alleviating immune response.40 Our trial explored the effect of MRA from the perspective of metabolism, which is consistent with the overall concept of Traditional Chinese Medicine. No adverse events occurred during the trial conducting. Similar studies in the past have not found serious adverse effects associated with acupuncture.22,33
The patients in control group did get interventions for fatigue, eg injections and lifestyle advice, even though it would also have been helpful to have the blank control group. Strengths of this trial was that the interventions received by the control group would help to overcome the “Hawthorne effect” and improve patient compliance. However, some limitations still existed, such as small sample size, short observation time, short follow-up time, no blank control group or sham acupuncture group, and no multicenter established, which may induce some bias. Further research is needed to develop to enlarge sample size and establish multi-center clinical trials, so as to provide more reliable scientific research basis for clinical application. The related mechanism of MRA improving CRF in BRCA survivors also still needs to be further studied.
Conclusions
MRA could regulate serum ghrelin, GIP, leptin, and insulin levels in BRCA survivors. In addition, it alleviates CRF, sleeping disturbance, and depression symptoms in these survivors and improves their quality of life. MRA was simple to operate with high patient compliance, so the findings have external validity and applicability. It indicates that MRA may be effective in breast cancer survivors with CRF, in other words MRA may have potential as an alternative and complementary therapy for BRCA survivors with CRF.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statements
The studies involving human participants were reviewed and approved by the Medical Ethics Committee, Huzhou Hospital of Traditional Chinese Medicine (Approval No.2019-077-A).
Acknowledgments
The study was registered in the Chinese Clinical Trial Registry (registration no. ChiCTR1900028543).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Zhejiang Province (No. LGF20H270011).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Maomao C, He L, Dianqin S, et al. Current cancer burden in China: epidemiology, etiology, and prevention. Cancer Biol Med. 2022;19(8):1121–1138. doi:10.20892/j.issn.2095-3941.2022.0231
2. Ye Z, Du F, Wu Y, Yang X, Yi Z. Interpretation of NCCN clinical practice guidelines in oncology: cancer-related fatigue. J Int Transl Med. 2016;4:1–8. doi:10.11910/2227-6394.2016.04.01
3. Ma Y, He B, Jiang M, et al. Prevalence and risk factors of cancer-related fatigue: a systematic review and meta-analysis. Int J Nurs Stud. 2020;111:103707. doi:10.1016/j.ijnurstu.2020.103707
4. Shi J, Liang D, Dao-Juan LI. Epidemiological status of global female breast cancer. China Cancer. 2017;26(9):683–690.
5. Cao W, Chen HD, Yu YW, Li N, Chen WQ. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
6. Ehlers DK, DuBois K, Salerno EA. The effects of exercise on cancer-related fatigue in breast cancer patients during primary treatment: a meta-analysis and systematic review. Expert Rev Anticancer Ther. 2020;20(10):865–877. doi:10.1080/14737140.2020.1813028
7. Abrahams HJG, Gielissen MFM, Schmits IC, Verhagen C, Rovers MM, Knoop H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: a meta-analysis involving 12 327 breast cancer survivors. Ann Oncol. 2016;27:965–974. doi:10.1093/annonc/mdw099
8. Stan DL, Croghan KA, Croghan IT, et al. Randomized pilot trial of yoga versus strengthening exercises in breast cancer survivors with cancer-related fatigue. Support Care Cancer. 2016;24:4005–4015. doi:10.1007/s00520-016-3233-z
9. Thong MSY, van Noorden CJF, Steindorf K, Arndt V. Cancer-related fatigue: causes and current treatment options. Curr Treat Options Oncol. 2020;21:17. doi:10.1007/s11864-020-0707-5
10. Zhang X, Qiu H, Li C, Cai P, Qi F. The positive role of traditional Chinese medicine as an adjunctive therapy for cancer. Biosci Trends. 2021;15(5):283–298. doi:10.5582/bst.2021.01318
11. Mao JJ, Farrar JT, Bruner D, et al. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: a randomized trial. Cancer. 2014;120(23):3744–3751. doi:10.1002/cncr.28917
12. Yang S, Chu S, Gao Y, et al. A narrative review of Cancer-Related Fatigue (CRF) and its possible pathogenesis. Cells. 2019;8(7):738. doi:10.3390/cells8070738
13. Kim S, Miller BJ, Stefanek ME, Miller AH. Inflammation-induced activation of the indoleamine 2,3-dioxygenase pathway: relevance to cancer-related fatigue. Cancer. 2015;121(13):2129–2136. doi:10.1002/cncr.29302
14. Arya N, Vaish A, Zhao K, Rao H. Neural mechanisms underlying breast cancer related fatigue: a systematic review of neuroimaging studies. Front Neurosci. 2021;15:735945. doi:10.3389/fnins.2021.735945
15. NCCN. NCCN Guidelines Version 1.2018 Cancer-Related Fatigue [EB/OL]. Fort Washington: NCCN; 2018.
16. Klasson C, Helde Frankling M, Lundh Hagelin C, Bjorkhem-Bergman L. Fatigue in cancer patients in palliative care-a review on pharmacological interventions. Cancers. 2021;13(5):985. doi:10.3390/cancers13050985
17. Strebkova R. Cancer-related fatigue in patients with oncological diseases: causes, prevalence, guidelines for assessment and management. Folia Med. 2020;62(4):679–689. doi:10.3897/folmed.62.e50517
18. Yeh MH, Chao CH, Koo M, Chen CY, Yeh CC, Li TM. Association of traditional Chinese medicine body constitution and moderate-to-severe cancer-related fatigue in cancer patients. Complement Ther Med. 2019;43:44–48. doi:10.1016/j.ctim.2019.01.004
19. Deng SM, Chiu AF, Wu SC, et al. Association between cancer-related fatigue and traditional Chinese medicine body constitution in female patients with breast cancer. J Tradit Complement Med. 2021;11:62–67. doi:10.1016/j.jtcme.2020.08.005
20. Mao H, Mao JJ, Chen J, et al. Effects of infrared laser moxibustion on cancer-related fatigue in breast cancer survivors: study protocol for a randomized controlled trial. Medicine. 2019;98(34):e16882. doi:10.1097/MD.0000000000016882
21. Li X, Wang X, Song L, et al. Effects of Qigong, Tai Chi, acupuncture, and Tuina on cancer-related fatigue for breast cancer patients: a protocol of systematic review and meta-analysis. Medicine. 2020;99(45):e23016. doi:10.1097/MD.0000000000023016
22. Jang A, Brown C, Lamoury G, et al. The effects of acupuncture on cancer-related fatigue: updated systematic review and meta-analysis. Integr Cancer Ther. 2020;19:1534735420949679. doi:10.1177/1534735420949679
23. Wu C, Zheng Y, Duan Y, et al. Nonpharmacological interventions for cancer-related fatigue: a systematic review and bayesian network meta-analysis. Worldviews Evid Based Nurs. 2019;16:102–110. doi:10.1111/wvn.12352
24. Widgren Y, Fransson P, Efverman A. Acupuncture in patients undergoing cancer therapy: their interest and belief in acupuncture is high, but few are using it. Integr Cancer Ther. 2022;21:15347354221077277. doi:10.1177/15347354221077277
25. Zhang Y, Lin L, Li H, Hu Y, Tian L. Effects of acupuncture on cancer-related fatigue: a meta-analysis. Support Care Cancer. 2018;26(2):415–425. doi:10.1007/s00520-017-3955-6
26. Lin PJ, Culakova E, Heckler CE, Janelsins MC, Mustian KM. The association of serum ghrelin, GIP, insulin, and leptin levels with sleep quality and cancer-related fatigue in cancer survivors. J Clin Oncol. 2018;36:10122. doi:10.1200/JCO.2018.36.15_suppl.10122
27. Jiao ZT, Luo Q. Molecular mechanisms and health benefits of ghrelin: a narrative review. Nutrients. 2022;14:4191. doi:10.3390/nu14194191
28. Campbell JE, Drucker DJ. Pharmacology, physiology, and mechanisms of incretin hormone action. Cell Metab. 2013;17:819–837. doi:10.1016/j.cmet.2013.04.008
29. Cho YM, Kieffer TJ. K-cells and glucose-dependent insulinotropic polypeptide in health and disease. Vitam Horm. 2010;84:111–150. doi:10.1016/B978-0-12-381517-0.00004-7
30. Tokarz VL, MacDonald PE, Klip A. The cell biology of systemic insulin function. J Cell Biol. 2018;217:2273–2289. doi:10.1083/jcb.201802095
31. Pereira S, Cline DL, Glavas MM, Covey SD, Kieffer TJ. Tissue-specific effects of leptin on glucose and lipid metabolism. Endocr Rev. 2021;42:1–28. doi:10.1210/endrev/bnaa027
32. Zhang Y, Chua S Jr. Leptin function and regulation. Compr Physiol. 2017;8:351–369. doi:10.1002/cphy.c160041
33. Choi TY, Ang L, Jun JH, et al. Acupuncture for managing cancer-related fatigue in breast cancer patients: a systematic review and meta-analysis. Cancers. 2022;14:4419. doi:10.3390/cancers14184419
34. Johnston MF, Hays RD, Subramanian SK, et al. Patient education integrated with acupuncture for relief of cancer related fatigue randomized controlled feasibility study. BMC Complement Altern Med. 2011;11:49. doi:10.1186/1472-6882-11-49
35. Molassiotis A, Bardy J, Finnegan-John J, et al. Acupuncture for cancer-related fatigue in patients with breast cancer: a pragmatic randomized controlled trial. J Clin Oncol. 2012;30:4470–4476. doi:10.1200/JCO.2012.41.6222
36. Molassiotis A, Bardy J, Finnegan-John J, et al. A randomized, controlled trial of acupuncture self-needling as maintenance therapy for cancer-related fatigue after therapist-delivered acupuncture. Ann Oncol. 2013;24:1645–1652. doi:10.1093/annonc/mdt034
37. Smith C, Carmady B, Thornton C, Perz J, Ussher JM. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: a pilot randomised controlled trial. Acupunct Med. 2013;31:9–15. doi:10.1136/acupmed-2012-010228
38. Deng G, Chan Y, Sjoberg D, et al. Acupuncture for the treatment of post-chemotherapy chronic fatigue: a randomized, blinded, sham-controlled trial. Support Care Cancer. 2013;21:1735–1741. doi:10.1007/s00520-013-1720-z
39. He Y, Yuan M, He C, Zhu D, Wang F. The effects of transcutaneous acupoint electrical stimulation on cancer-related fatigue and negative emotions in cancer patients: a systematic review and meta-analysis of randomized controlled trials. Contrast Media Mol Imaging. 2022;2022:1225253. doi:10.1155/2022/1225253
40. Han QQ, Fu Y, Le JM, et al. The therapeutic effects of acupuncture and electroacupuncture on cancer-related symptoms and side-effects. J Cancer. 2021;12:7003–7009. doi:10.7150/jca.55803
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.