Back to Journals » Drug Design, Development and Therapy » Volume 16
Effects of Intravenous Analgesia Using Tramadol on Postoperative Depression State and Sleep Quality in Women Undergoing Abdominal Endoscopic Surgery: A Randomized Controlled Trial
Authors Fu M ![]() , Chen S
, Chen S ![]() , Xu R
, Xu R ![]() , Chen J, Chen X, Gan W, Huang H
, Chen J, Chen X, Gan W, Huang H ![]() , Duan G
, Duan G ![]()
Received 17 January 2022
Accepted for publication 20 April 2022
Published 2 May 2022 Volume 2022:16 Pages 1289—1300
DOI https://doi.org/10.2147/DDDT.S357773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Mengyue Fu,1,* Shi Chen,2,* Rui Xu,1 Jie Chen,1 Xuehan Chen,1 Wanxia Gan,1 He Huang,1 Guangyou Duan1
1Department of Anesthesiology, The Second Affiliated Hospital, Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Anesthesiology, Chongqing Beibu Maternity Hospital, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangyou Duan; He Huang, Department of Anesthesiology, The Second Affiliated Hospital, Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected]; [email protected]
Purpose: This study aimed to explore the effects of intravenous analgesia using tramadol on postoperative depression, anxiety, and sleep in women undergoing abdominal endoscopic surgery.
Patients and Methods: Two hundred female patients (100 in each group) who underwent abdominal endoscopic surgery were recruited to randomly receive intravenous analgesia with sufentanil combined with tramadol (tramadol group) or sufentanil (control group). The primary outcome was the incidence of postoperative depression, which was assessed at 1, 2, and 3 days after surgery using the 13-item Beck Depression Inventory. The secondary outcomes were the incidence of anxiety and sleep quality, which were assessed using the 20-item Self-Rating Anxiety Scale and Richards–Campbell Sleep Questionnaire.
Results: The incidence of depression (Beck depression scale≥ 4) during the 3-day follow-up in the control group was 51%, which was significantly higher than that in the tramadol group of 28% (relative risk [RR]=0.55; 95% confidence interval [CI], 0.38– 0.79; P=0.001). No difference was found in the incidence of anxiety state (Self-Rating Anxiety Scale≥ 40) between the tramadol and control groups (7%vs 5%; RR=1.40; 95% CI, 0.46– 4.25; P=0.552). All of the Richards–Campbell sleep scales of patients in the tramadol group at 1 (77.4± 15.2 vs 64.2± 20.1, P< 0.001), 2 (84.1± 14.9 vs 71.8± 18.8, P< 0.001), and 3 days (87.0± 12.2 vs 70.3± 21.0, P< 0.001) after surgery were higher than those in the control group.
Conclusion: Intravenous analgesia using tramadol can effectively improve the postoperative depression and sleep status of women undergoing abdominal endoscopic surgery. Tramadol is recommended for use in postoperative analgesia when improving postoperative mood, and sleep is needed in clinical practice.
Keywords: women, depression, anxiety, sleep, abdominal surgery
Introduction
For patients undergoing elective surgery, psychological and emotional disorders are the mental and emotional disorders with high incidence rates during the perioperative period, especially depression and anxiety. The incidence rate of depression during the perioperative period is approximately 60%,1,2 and the incidence rate of anxiety is approximately 15%.3,4 Postoperative depression and anxiety not only directly reduce the patient’s emotional level but also significantly affect the patient’s sleep quality and rehabilitation status and even prolong the hospital stay.5–7 However, the existing epidemiological studies have confirmed that women are at high risk for postoperative anxiety and depression8,9 and have a significantly higher risk of developing new depression and anxiety after surgery.10 Therefore, for women undergoing elective surgery, exploring how to relieve postoperative depression and anxiety is important to improve their satisfaction and prognosis during the perioperative period.
Currently, patient-controlled intravenous analgesia (PCIA) is one of the most commonly used methods for postoperative analgesia in surgical patients.11,12 Tramadol mainly acts by inhibiting the reuptake of norepinephrine and serotonin and is widely considered a safe and effective intravenous analgesic.13–15 Currently, the most commonly used first-line antidepressants for the treatment of depression are norepinephrine reuptake inhibitor and serotonin reuptake inhibitor,16–18 and these are the choices for the treatment of anxiety disorder.19 Therefore, it is significantly likely that tramadol can relieve depression and anxiety in women undergoing elective surgery under general anesthesia while providing postoperative analgesic effects.
Recent clinical studies have shown that a comparative study of tramadol and hydromorphone on postoperative analgesia in patients undergoing cesarean section unexpectedly found that tramadol can significantly reduce the depression and anxiety scores of patients undergoing cesarean section.20 In addition, the latest studies have also shown that tramadol can significantly reduce the incidence of postpartum depression in parturients undergoing cesarean section,21 which further supports the possibility of using tramadol to relieve depression and anxiety in women undergoing surgery, thus possibly improving their postoperative recovery. Therefore, this study included women undergoing abdominal endoscopic surgery to explore the role of tramadol intravenous analgesia in the improvement of perioperative emotional state through preoperative and postoperative depression and anxiety assessments.
Materials and Methods
Study Design
This randomized controlled study aimed to determine whether intravenous analgesia using tramadol has anti-depression and anti-anxiety effects in women undergoing abdominal endoscopic surgery under general anesthesia. This study was conducted according to the Consolidated Standards of Reporting Trials 2010 statement guidelines. This study was conducted according to the Declaration of Helsinki World Medical Association. And the study protocol was approved by the Hospital Ethics Committee of the Second Affiliated Hospital, Chongqing Medical University (Approval ID: 2021–37), and all patients provided written informed consent prior to the study. This study was registered in the Chinese Clinical Trial Registry (ID: ChiCTR2100045898). The full protocol and study data can be acquired from the corresponding author HH or GD.
Patients
The study was performed from April 26, 2021 to September 15, 2021. We screened potential female participants in surgical wards of the gynecology, hepatological surgery, and gastrointestinal surgery departments after they were scheduled to undergo laparoscopic surgery. Female patients aged 18–65 years, undergoing elective laparoscopic surgery, with American Society of Anesthesiology (ASA) physical status I–III, and voluntarily receiving PCIA were included for screening. The exclusion criteria were as follows: patients who had been diagnosed with depressive or anxiety disorder before; with a history of chronic pain; with long-term use of analgesics and psychotropic drugs; with serious diseases, such as cardiac diseases, nausea, and liver, kidney, and blood system disorders; with a history of allergies to opioids or tramadol; taking monoamine oxidase inhibitor drugs within 15 days; with a history of alcohol or opioid abuse, who were currently included in another clinical study; who were pregnant or lactating; and who were unable to communicate.
Randomization and Masking
Simple randomization was performed, and the computer-generated randomization sequence was stratified with a 1:1 allocation. An independent epidemiologist prepared the allocation sequence and hid it in an opaque, numbered them in sequence, and sealed envelopes. Subsequently, the patients were randomly assigned to the tramadol or control group according to the envelope with a random number before surgery. The envelopes were then sealed again before the end of surgery and stored at the site of investigation until the end of the study. In the study, all participants and researchers, including those involved in surgery, were blinded of their group allocation during treatment. Anesthesiologists who were responsible for performing PCIA were not involved in the data collection, input, or analysis. In addition, psychological assessment and related postoperative data collection were performed by trained professionals who did not participate in patient care, and they were blinded to the group allocations.
Intervention
After entering the operating room, blood pressure, electrocardiogram, end-expiratory carbon dioxide oxygen, hemoglobin saturation, and bispectral index (BIS) were continuously monitored for all included patients. Standardized anesthesia induction was performed by intravenous anesthesia of propofol (2–3 mg/kg), sufentanil (0.5–2 μg/kg), midazolam (0.05–0.2 mg/kg), and rocuronium (0.6–1.2 mg/kg). Endotracheal intubation was performed when the index BIS of the patient dropped to 40–50. Anesthesia was maintained using sevoflurane (1.0–1.5%) combined with propofol (4–12 mg/kg/h) and remifentanil (0.2–0.3 μg/kg/min). The depth of anesthesia was maintained according to the BIS index 40–60, and effort was made to maintain blood pressure and heart rate within ±20% of baseline values. The patients in the control group were intravenously injected with 8 μg of sufentanil 10–20 min before the end of surgery, and those in the tramadol group were intravenously injected with 40 mg of tramadol. To prevent postoperative nausea and vomiting (PONV), ondansetron (4 mg) and dexamethasone (10 mg) were administered after the surgery.
Postoperative pain control was provided using a PCIA pump (100 mL) at the end of the surgery. Pain treatment was divided into two types according to the random number strategy. For the patients in the control group, 3 μg/kg sufentanil (Humanwell Healthcare Co., Ltd. China) and ondansetron (16 mg) were mixed with 0.9% saline to a volume of 100 mL. In the tramadol group, tramadol (Grunenthal Co., Ltd., Aachen, Germany) (7.5 mg/kg) and sufentanil (1.5 μg/kg) and ondansetron (16 mg) mixed with 0.9% saline to a volume of 100 mL were placed in a PCIA pump. The PCIA pump was programmed to have a background infusion of 2.0 mL/h, a PCIA dose of 1 mL, and a lockout period of 15 min.
Outcomes
The primary outcome of the study was the incidence of depression during the 3-day follow-up after surgery. Depression was assessed at 1, 2, and 3 days after surgery using the 13-item Beck Depression Inventory, a commonly used self-reported scale in previous studies of the Chinese population, of which a score of 4 or above indicates possible depression.22,23 The secondary outcomes were postoperative anxiety state and sleep quality at 1, 2, and 3 days after surgery. Anxiety was assessed using a 20-item Self-Rating Anxiety Scale, including 20 items assessing symptoms of anxiety, of which a score of 40 or above indicates possible depression.24,25 Sleep quality was evaluated using the Richards–Campbell Sleep Questionnaire, which includes six items assessing quality of sleep, with higher scores indicating better sleep quality.26,27 The area under the curve (AUC) of the scores of depression, anxiety, and sleep quality during the 3-day follow-up compared to the scores before surgery was also calculated. In the study, all psychological tests were performed by an investigator who was trained by a professional psychologist, and only patients and investigators were present.
Other outcomes included length of hospital stay and time to walk out of bed. The numeric rating scale (NRS) of pain at 1, 2, and 3 days after the surgery were assessed, and the pressing frequency of the PCIA pump at 1 and 2 days and total PCIA consumption after surgery were also recorded. In addition, the patients’ degree of satisfaction during the time after surgery was assessed according to unsatisfaction, average, or satisfaction.
Adverse reactions, such as nausea, vomiting, pruritus, urinary retention, and abnormalities of the cardiovascular system after the surgery, were monitored for 48 h after surgery. Bradycardia was defined as a heart rate ≤55 bpm or a decrease of ≥20% compared to the baseline. Tachycardia was defined as a heart rate ≥100 bpm or an increase of ≥20% from the baseline. Hypotension was defined as systolic blood pressure ≤95 mmHg or a decrease of ≥20% from the baseline. Hypertension was defined as systolic blood pressure ≥160 mmHg or an increase of ≥20% from the baseline. Hypoxemia was defined as a pulse oxygen saturation ≤95%.
Sample Size Calculation
According to the pilot observations in our hospital, the incidence rate of depression, the primary outcome of the study, which was assessed using the 13-item Beck Depression Inventory, was approximately 50%. We hypothesized that intravenous analgesia tramadol accounts for 40% of the incidence, that is, 20%. Based on a significance level of 0.05 and a power of 0.8, the sample size was calculated according to a 1:1 parallel control study using the sample size calculation software PASS version 11.0 (NCSS, Kaysville, UT). The estimated sample size was 94 for each group. Considering that the missing follow-up rate was approximately 5%, the total required sample size was approximately 200 cases, with 100 cases in each group.
Statistical Analyses
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software version 22.0 (SPSS, Chicago, IL, USA). Data are presented as number (%), mean (standard deviation), or median (interquartile range). Data were analyzed according to the intention-to-treat principle, following a pre-established analysis plan. The chi-squared test was used to compare the discontinuous variables between the two groups, and an independent-samples t-test was used to compare normally distributed continuous variables. For the comparison of non-normally distributed data, the Mann–Whitney U-test was performed. Relative risk (RR) with 95% confidence interval (CI) was calculated, when appropriate. Subgroup analysis was performed to compare the incidence of depression and Richards–Campbell sleep scale between the tramadol and control groups in patients undergoing gynecological surgery and hepatobiliary or gastrointestinal surgery, respectively. In addition, stepwise logistic regression analysis was performed to determine the effect of intravenous analgesia using tramadol in predicting postoperative depression. Age, ASA classification, patient classification, surgery type, preoperative depression state, and anxiety state were included in the logistic model. Odds ratios (ORs) with 95% CIs for these factors were calculated. Differences were considered statistically significant at P < 0.05.
Results
As shown in Figure 1, none of the patient was lost to follow-up, and 200 women (100 in each group) were included in the final analysis. The baseline demographic characteristics and preoperative and intraoperative data of all patients are listed in Table 1. The depression score in the tramadol group was significantly higher than that in the control group (3.0 [1.0–5.0] vs 2.0 [1.0–3.0], P=0.046), and the incidence of depression was defined as a depression score≥4 (27% vs 15%, P=0.037). There was no difference in other basal data between the patients in the control and tramadol groups (P>0.05).
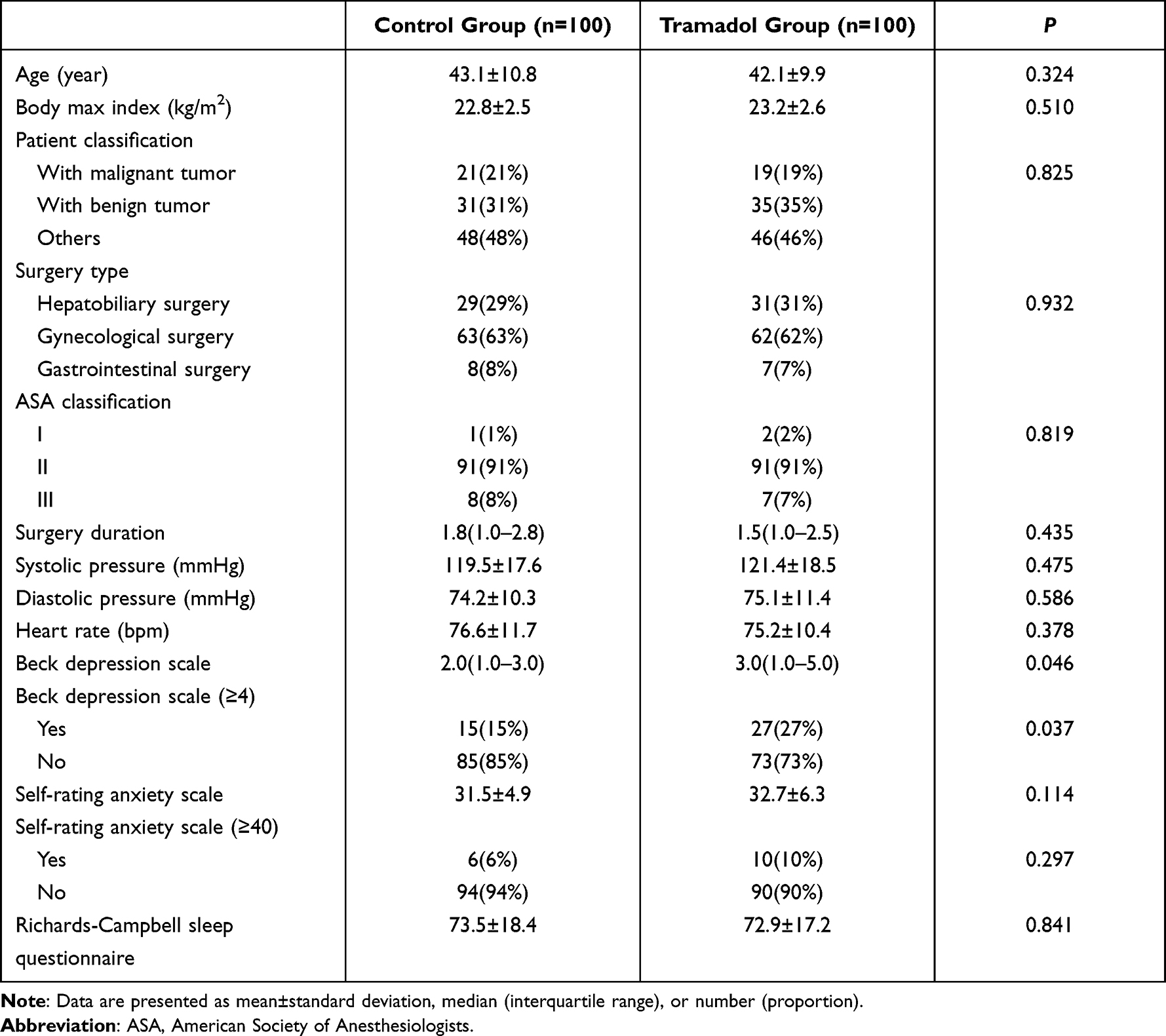 |
Table 1 Baseline Demographic Characteristics and Preoperative and Intraoperative Data Between Patients in the Control and Tramadol Groups |
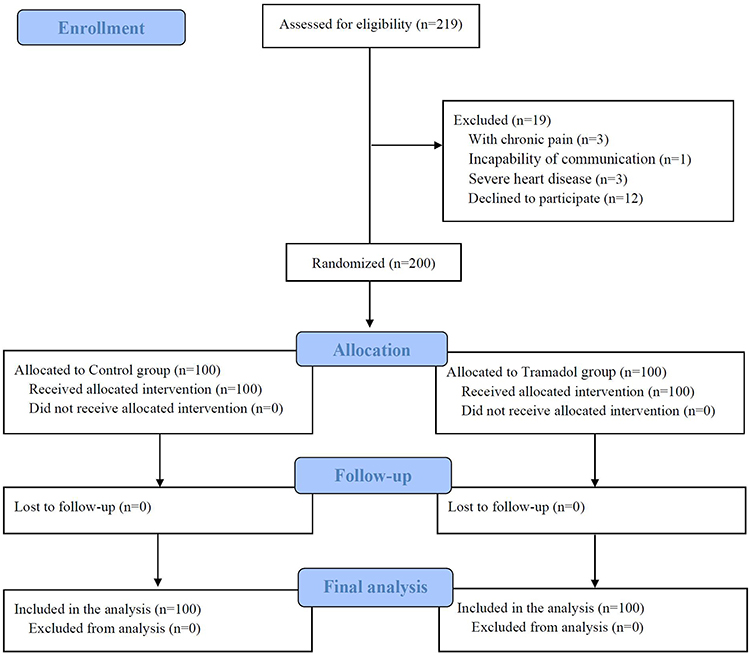 |
Figure 1 Flowchart of the study. |
The results of the postoperative evaluation of depression, anxiety, and sleep are shown in Table 2. The Beck depression scale scores of patients in the tramadol group at 1 (2.0 [1.0–4.0] vs 3.5 [2.0–5.0], P<0.001), 2 (2.0 [0.0–3.0] vs 4.0 [2.0–5.0], P<0.001), and 3 (0.0 [0.0–3.0] vs 2.0 [1.0–4.0], P<0.001) days after surgery were lower than those in the control group. The incidence rate of depression (Beck depression scale≥4) during the 3-day follow-up in the control group was 51%, which was significantly higher than that in the tramadol group (28%) (RR=0.55; 95% CI, 0.38–0.79; P=0.001).
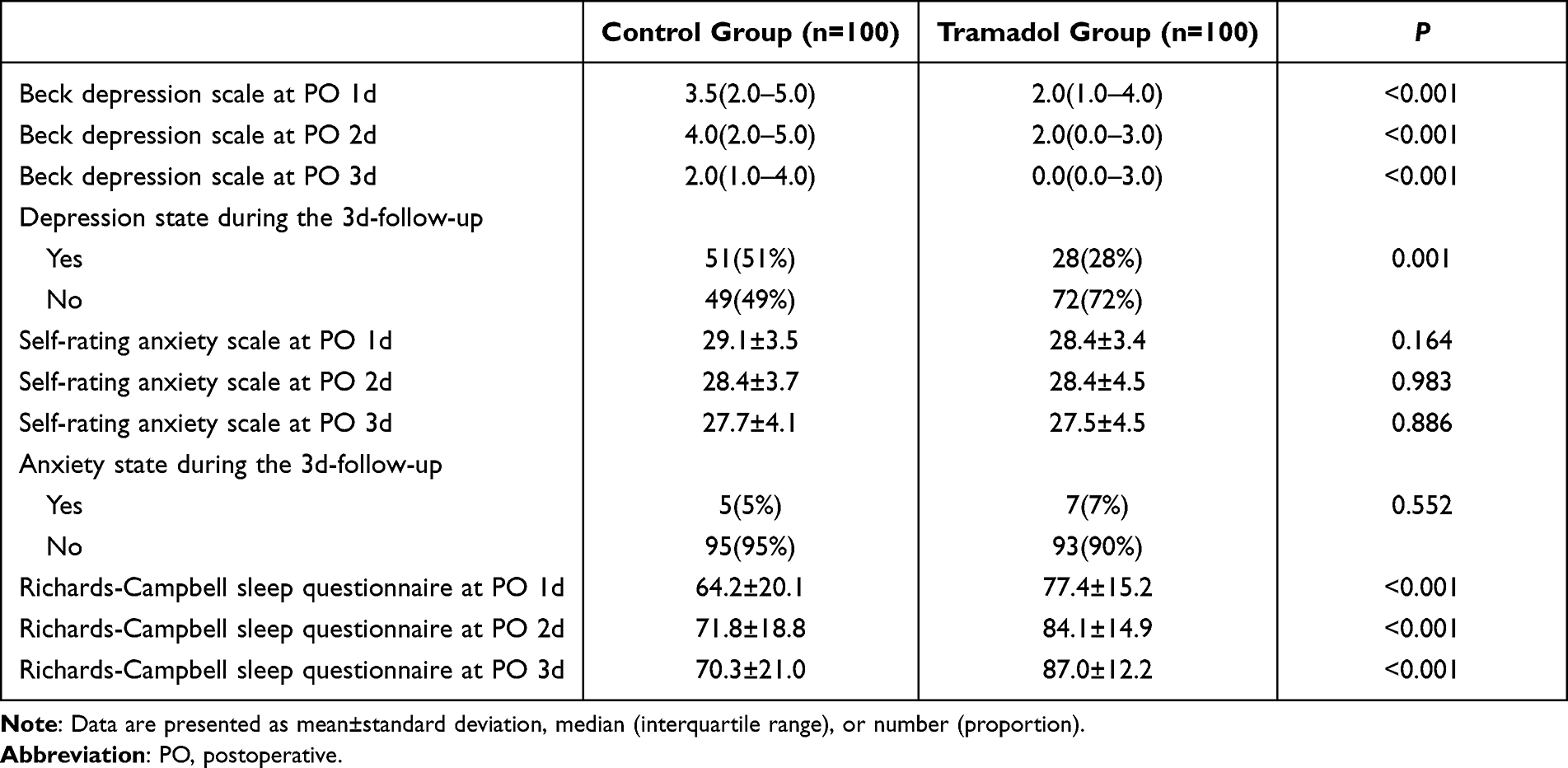 |
Table 2 Postoperative Status of Depression, Anxiety, and Sleep Between Patients in the Control and Tramadol Groups |
There was no difference in the Self-Rating Anxiety Scale between the two groups at all 3 days after surgery (P>0.05), and no difference was found in the incidence of anxiety between the tramadol and control groups (7% vs 5%; RR=1.40; 95% CI, 0.46–4.25; P=0.552). The Richards–Campbell sleep scale scores of patients in the tramadol group at 1 (77.4±15.2 vs 64.2±20.1, P<0.001), 2 (84.1±14.9 vs 71.8±18.8, P<0.001), and 3 (87.0±12.2 vs 70.3±21.0, P<0.001) days after surgery were higher than those in the control group.
The AUCs of the mean Beck Depression Scale, Self-Rating Anxiety Scale, and Richards–Campbell Sleep Questionnaire at 3-day follow-up compared to those before surgery are shown in Figure 2. The AUC of the Beck depression scale in the tramadol group was significantly decreased, whereas it increased in the control group (−3.0 [−8.0–2.0] vs 3.0 [0.0–7.0], P<0.001). The AUC of the Self-Rating Anxiety Scale in the tramadol group was −11.3 (−20.0 to −5.0), whereas in the control group, it was −10.0 (−15.0–0.9). Moreover, the P value between the two groups was 0.061. In addition, the AUC of the Richards–Campbell sleep scale in the tramadol group was significantly increased, whereas it decreased in the control group (21.4 [−3.1–57.6] vs −13.0 [−50.5–19.5], P<0.001).
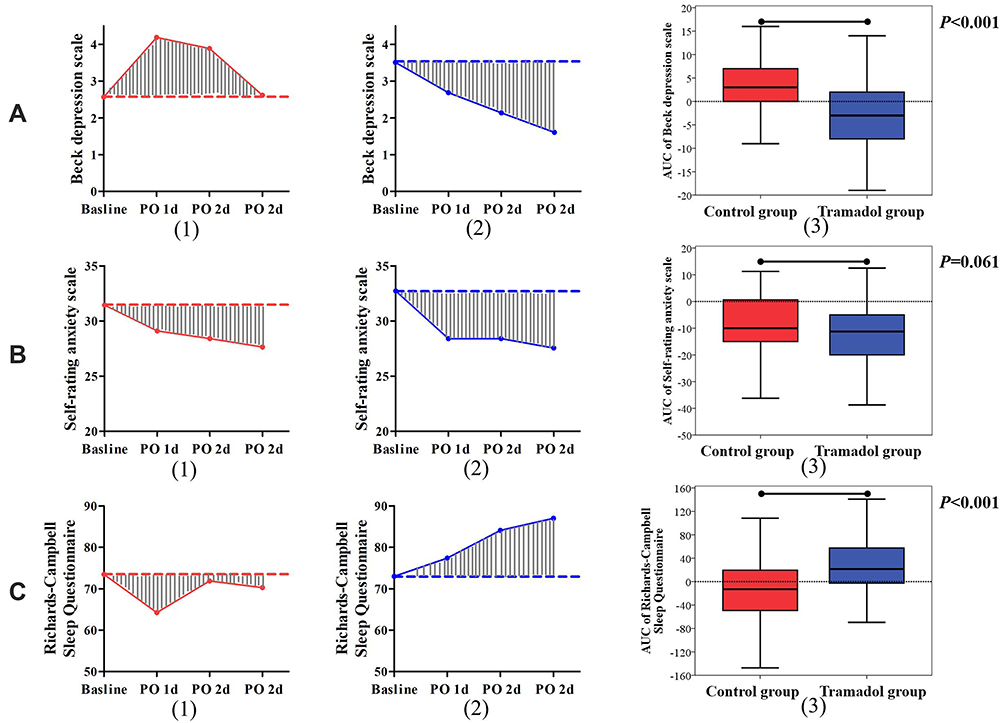 |
Figure 2 The area under the curve (AUC) of mean Beck depression scale (A), Self-Rating Anxiety Scale (B), and Richards–Campbell Sleep Questionnaire (C). (1) represents AUC in the control group, (2) represents AUC in the tramadol group, and (3) represents the comparison between the control and tramadol groups. Abbreviation: PO, postoperative. |
Subgroup analysis showed that the incidence rate of depression in the tramadol group was significantly lower than that in the control group for patients undergoing gynecological surgery (33.9% vs 52.4%; RR=0.67; 95% CI, 0.46–0.99; P=0.037; Figure 3A-1) and hepatobiliary or gastrointestinal surgery (18.4% vs 48.6%; RR=0.45; 95% CI, 0.23–0.88; P=0.005; Figure 3B-1). The Richards–Campbell sleep scale in the tramadol group was significantly higher than that in the control group for patients undergoing gynecological surgery and hepatobiliary or gastrointestinal surgery at all three time points (Figure 3A-2 and B-2). In addition, a logistic analysis considering the potential confounding factors was performed, and the model was statistically significant (P<0.001). As shown in Table 3, intravenous analgesia using tramadol (OR=3.62; 95% CI, 1.88–6.98; P<0.001) was identified as a protective factor, whereas preoperative depression status (OR=0.26; 95% CI, 0.12–0.56; P=0.001) and patients with malignant tumors (OR=0.31; 95% CI, 0.14–0.71; P=0.005) were identified as hazardous factors.
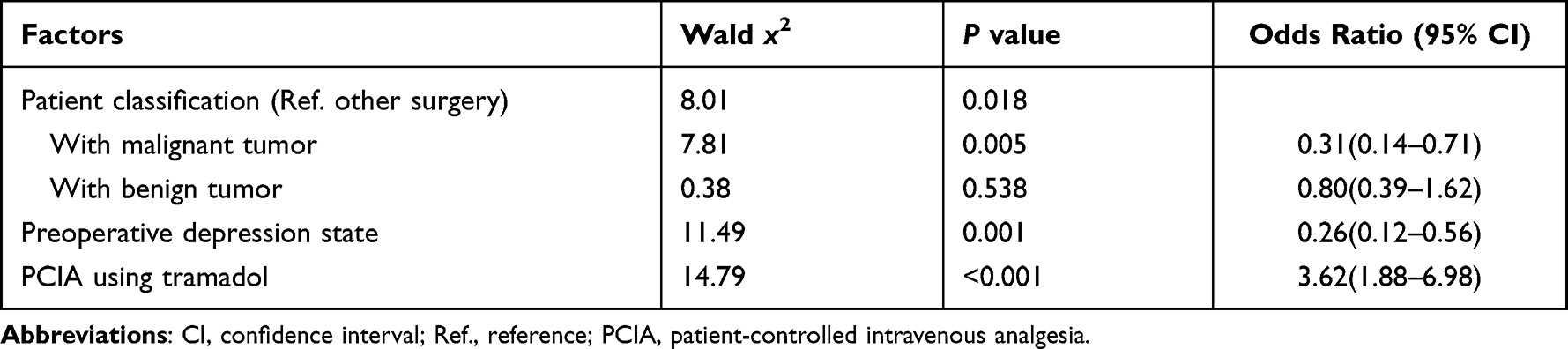 |
Table 3 Stepwise Logistic Regression Model Based on Patients’ Characteristics for Predicting Postoperative Depression |
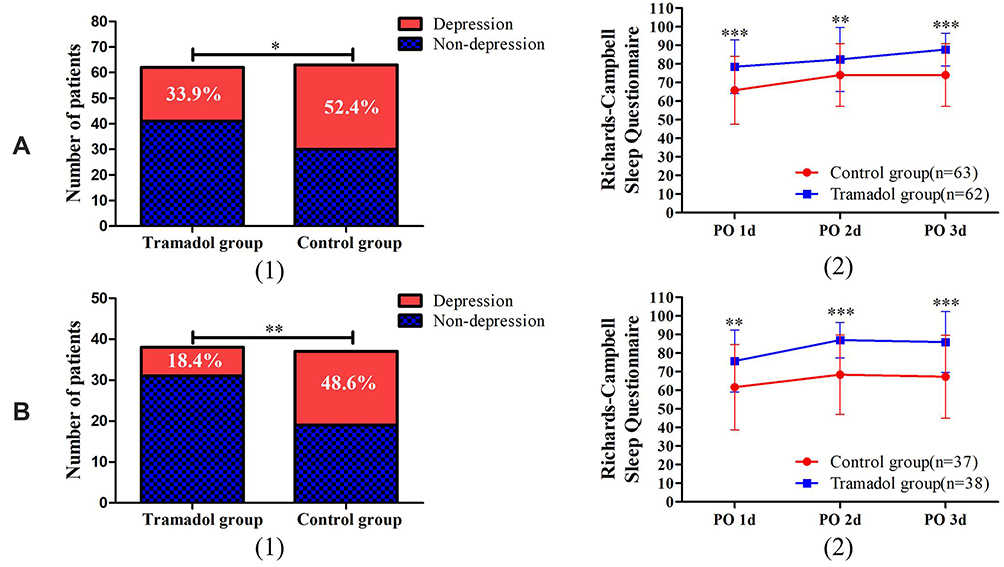 |
Figure 3 Subgroup analysis of comparisons of patients undergoing gynecological surgery (A) and hepatobiliary or gastrointestinal surgery (B) in the incidence of depression (1) and Richards–Campbell sleep scale (2) between the tramadol and control groups. *P<0.05, **P<0.01, ***P<0.001. Abbreviation: PO, postoperative. |
As listed in Table 4, no significant difference was found in pain NRS, PCIA pressing frequency or consumption, time to off-bed activity, or hospital stay between the tramadol and control groups (P>0.05). The incidence rate of satisfaction after surgery in the tramadol group was significantly higher than that in the control group (84% vs 72%; OR=1.17; 95% CI, 1.01–1.36; P=0.041).
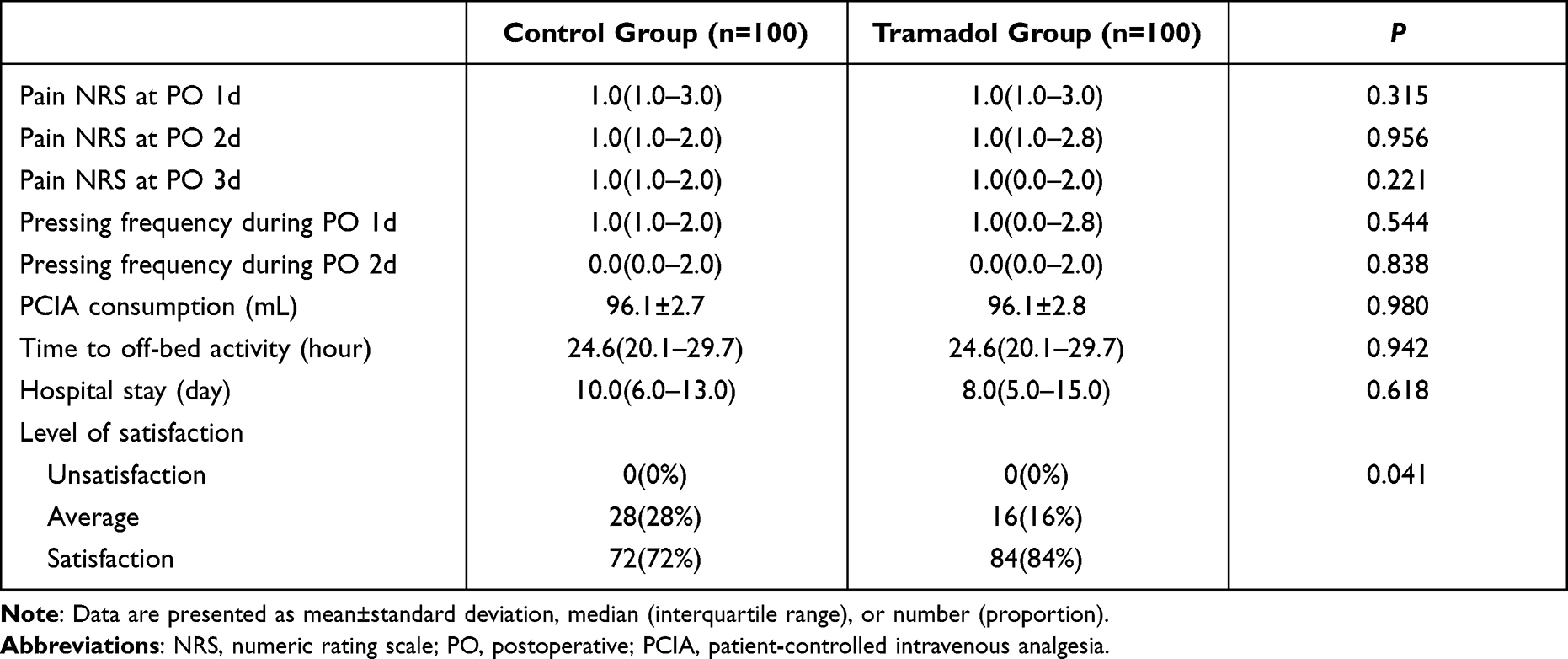 |
Table 4 Postoperative Outcomes Related to Pain Between Patients in the Control and Tramadol Groups |
Postoperative adverse events during analgesia for patients in the control and tramadol groups are shown in Table 5. No significant difference was found in the incidence of hypoxemia, bradycardia, tachycardia, hypotension, or hypertension between the tramadol and control groups. In addition, the incidence rate of PONV after surgery in the tramadol group was lower than that in the control group (19% vs 33%; OR=0.83; 95% CI, 0.70–0.98; P=0.024).
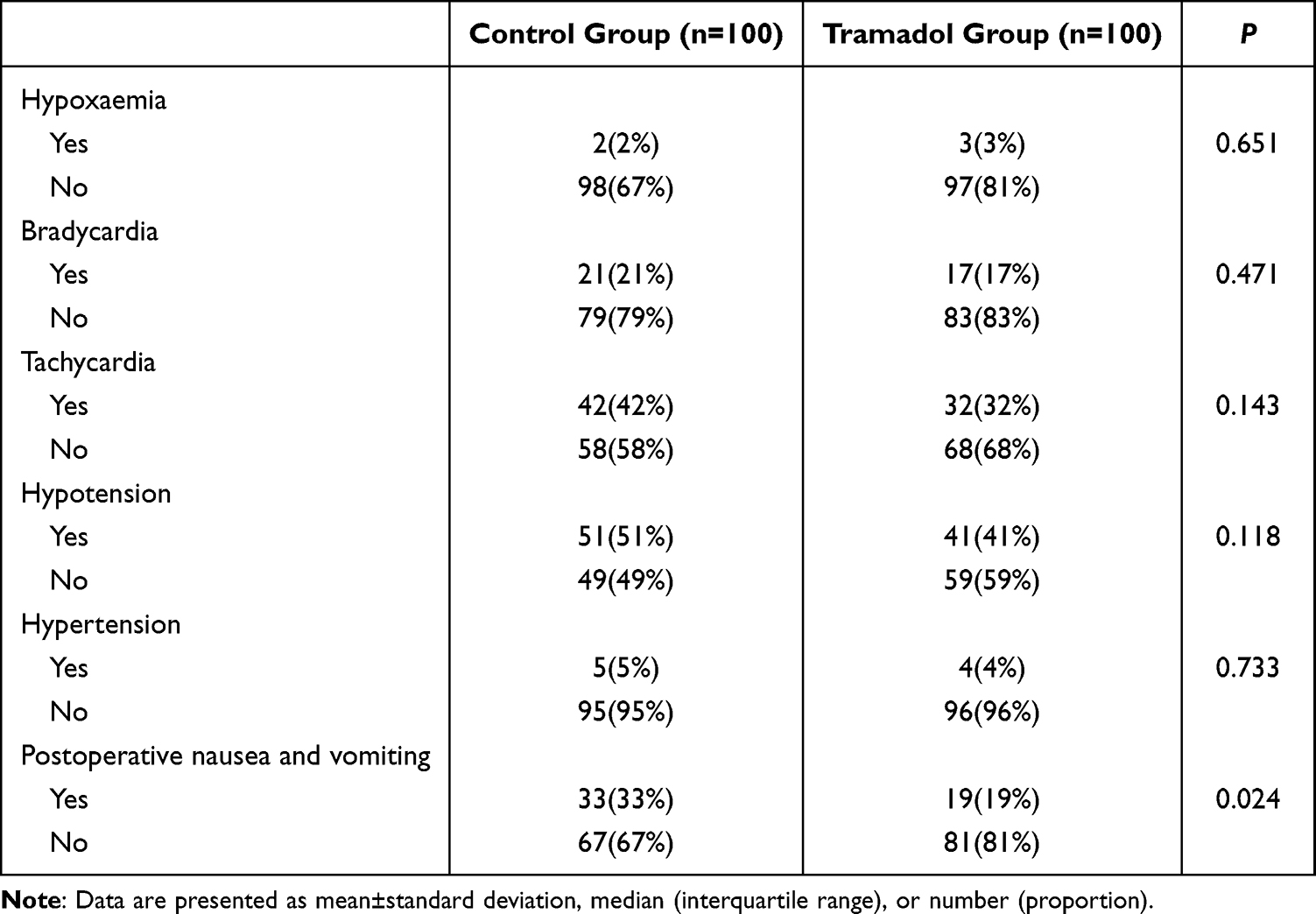 |
Table 5 Postoperative Adverse Events During the Analgesia Induction Between Patients in the Control and Tramadol Groups |
Discussion
The results of this study showed that the incidence rate of depression in the tramadol group within 3 days after abdominal endoscopic surgery was lower than that in the control group, and the Baker depression scores at 3 consecutive postoperative days were significantly lower than those in the control group. In addition, the Richards–Campbell Sleep Questionnaire scores in the tramadol group 3 days after the operation were also significantly higher than those in the control group. There was no significant difference in the incidence of anxiety and anxiety scale scores between the two groups during the days after surgery. In addition, the incidence rate of PONV in the tramadol group was lower than that in the control group, and the overall postoperative satisfaction was better in the tramadol group than in the control group.
Considering that women have a higher risk of anxiety and depression during the perioperative period,8,9 this study focused on women undergoing elective surgery. In contrast, because sex differences can affect the occurrence of emotional disorders,28–30 unifying sex could help us directly explore the role of tramadol in the emotional improvement of patients undergoing elective surgery. In addition, intravenous analgesia is a commonly used method in clinical practice; thus, emotional intervention based on this method is easy to perform. The current data showed that there was no significant difference in postoperative pain intensity between the two groups, which indicated that the analgesic effect of the tramadol group was not worse than that of the control group. In the study, to preclude the influence of differences in analgesic effects on the outcomes of depression, anxiety and sleep disorders, we chose a relative high dose of sufentanil. And as reported in previous studies, the commonly used sufentanil dose was 1.8 to 4μg/kg, and background infusion rate was 0.03 to 0.06μg/kg/h in PCIA after abdominal endoscopy surgery.31–34 In these studies, the mean NRS of pain at 24 hours after surgery were all less than 3. Thus in this study we chose to use total dose of 3μg/kg sufentanil with background infusion rate of 0.06μg/kg/h in PCIA pump in control group. Considering that tramadol alone may not have sufficient analgesia, we designed the intervention group to use single sufentanil in the control group, while tramadol combined with sufentanil in the experimental group. The results showed that mean NRS scores in this study were all less than 3 points and there was no significant difference between the two groups, precluding the influence of differences in analgesic effects on the outcomes of depression, anxiety, and sleep disorders. Although “less sufentanil” may be a potential influencing factor, through a literature search, we found that short-term exposure to opioid drugs did not affect the occurrence of emotional disorder.35 Thus, the current study is feasible to verify the improvement effect of tramadol on postoperative mood in female surgical patients.
Previously, studies on the application of tramadol for cesarean section have found that it can reduce the occurrence of postpartum depression.20,21 However, there are many differences, such as pregnancy and primary and concomitant diseases between women undergoing elective abdominal endoscopic surgery and women undergoing cesarean section. In this study, the incidence rate of postoperative depression in the control group reached 51%, which was close to those reported in previous studies.1,36 The incidence rate of postoperative depression after cesarean section is usually between 13.7% and 15.7%.37,38 Therefore, the effects of tramadol on postoperative depression in general elective surgery remain unclear. In this study, we found that intravenous analgesia tramadol significantly reduced the incidence of postoperative depression, with an RR value of 0.55. However, since the baseline depression score in the tramadol group before surgery was higher than that in the control group, we performed logistic analysis considering the potential confounding factors. Intravenous analgesia use tramadol was determined as a protective factor, whereas patients with preoperative depression and malignant tumors were identified as risk factors. In addition, we also performed subgroup analysis, and the results also showed that the incidence of depression and postoperative depression scores at different time points in the tramadol group were significantly lower than those in the control group for patients undergoing gynecological surgery and hepatobiliary or gastrointestinal surgery. The improvement effect of tramadol was slightly better for patients undergoing hepatobiliary or gastrointestinal surgery (RR=0.45) than for patients undergoing gynecological surgery (RR=0.67). Therefore, based on this study, we concluded that tramadol can significantly improve the depression of women, especially in those undergoing gastrointestinal or hepatobiliary surgery.
In this study, there was no significant difference in the incidence of postoperative anxiety and anxiety scores between the tramadol and control groups. The current results showed that the overall incidence rate of postoperative anxiety was 6%, which is lower than those reported in clinical studies of female surgical patients.36,39 We believe that two reasons may account for this result. First, the nursing department of our hospital routinely educates patients receiving elective surgery to improve their anxiety before and after surgery, which may counteract the effect of tramadol on improving anxiety. Second, the average age of the two groups in this study was not more than 45 years old, and previous studies have demonstrated that the high prevalence of anxiety disorder is often concentrated in middle-aged and elderly people.29,30 Thus, based on this study, the effect of tramadol on postoperative anxiety remains unclear and requires further study.
Postoperative sleep has become the focus of perioperative medicine in recent years.40 Even if it is included in perioperative education,41 women are at a high risk for sleep disorders.42,43 One study found that patients with fibromyalgia who used tramadol for analgesia had a lower incidence of sleep disorders compared to other analgesics.44 Recent animal studies have also found that tramadol dose-dependently reduces sleep time during rapid eye movement sleep and increases the attack latency of rapid eye movement sleep.45 In this study, we found that compared with the control group, tramadol can directly improve the sleep score of patients on the first to third day after surgery. One study has indicated that opioids can affect the quality of sleep, and both acute (for sedation or postoperative analgesia) or chronic (long-term for chronic pain) can disrupt sleep patterns.46 On the contrary, some studies have shown that opioids can significantly improve the sleep structure of healthy people and increase N2 sleep.47,48 Therefore, it remains unclear whether the “less opioid application” was the reason for the improved sleep in this study. In addition to the pain induced by the operation, postoperative sleep disorders, anxiety, and depression will also increase the incidence of sleep disorders. The improvement in the depression state of tramadol observed in this study may also be one of the reasons for its improvement in sleep. Nevertheless, based on this study, we concluded that intravenous analgesia combined with tramadol can significantly improve postoperative sleep, which should be beneficial to the patients’ postoperative recovery.
One previous study found that perioperative use of 5-HT-AR reuptake inhibitors may slightly reduce acute and chronic postoperative pain and opioid consumption, and it does not increase the occurrence of adverse events, including PONV.49 In this study, compared with the control group, the incidence of PONV was lower when tramadol combined with analgesia was used. This may be related to less exposure to opioids, because opioids have been clearly associated with PONV.49 Except for adverse events, this study also performed a satisfaction evaluation, and the results showed that it was significantly better in the tramadol group than in the control group. The occurrence of adverse reactions, such as postoperative emotional state, pain, sleep, and PONV, is an important factor affecting postoperative satisfaction. In this study, we found that tramadol can significantly improve depression and sleep quality and reduce the incidence of PONV. Therefore, intravenous analgesia using tramadol may be an effective method to improve postoperative patient satisfaction.
The following limitations must be considered when interpreting the study data. First, because preoperative anxiety intervention has become the routine nursing content in our hospital, it remains to be studied whether intravenous analgesia using tramadol affects postoperative anxiety. Second, in this study, no objective devices, such as PSG, were used to test patients’ sleep parameters after surgery, and the specific sleep pattern induced by tramadol remains unclear. Thirdly, in experimental group we designed tramadol combined with sufentanil considering that tramadol alone may not have sufficient analgesia. Thus the “less sufentanil” effect could not be completely excluded, and future study remains needed.
Conclusion
In conclusion, intravenous analgesia using tramadol can effectively improve the postoperative depression and sleep status of women undergoing abdominal endoscopic surgery. Tramadol is recommended for use in postoperative analgesia when improving postoperative mood, and sleep is needed in clinical practice.
Data Sharing Statement
The datasets for this study is available from the corresponding author (email: [email protected] or [email protected]) on reasonable request.
Acknowledgments
We would like to thank all subjects’ selfless contribution to this work.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by Joint Medical Research Project of Chongqing Science and Technology Bureau and Health Commission (No. 2019QNXM022).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Smith CE, Hawkins MAW, Williams-Kerver GA, et al. Depression subtypes, binge eating, and weight loss in bariatric surgery candidates. Surg Obes Relat Dis. 2020;16(5):690–697. doi:10.1016/j.soard.2019.12.017
2. Boakye M, Sharma M, Adams S, et al. Patterns and impact of electronic health records-defined depression phenotypes in spine surgery. Neurosurgery. 2021;89(1):E19–e32. doi:10.1093/neuros/nyab096
3. De Oliveira GS Jr, Holl JL, McCarthy RJ, et al. Overestimation of mortality risk and preoperative anxiety in patients undergoing elective general surgery procedures: a propensity matched analysis. Int J Surg. 2014;12(12):1473–1477. doi:10.1016/j.ijsu.2014.11.016
4. Du J, Plas M, Absalom AR, et al. The association of preoperative anxiety and depression with neurocognitive disorder following oncological surgery. J Surg Oncol. 2020;121(4):676–687. doi:10.1002/jso.25836
5. Persson P, Wijma K, Hammar M, et al. Psychological wellbeing after laparoscopic and abdominal hysterectomy–a randomised controlled multicentre study. Bjog. 2006;113(9):1023–1030. doi:10.1111/j.1471-0528.2006.01025.x
6. Hanusch BC, O’Connor DB, Ions P, et al. Effects of psychological distress and perceptions of illness on recovery from total knee replacement. Bone Joint J. 2014;96-b(2):210–216. doi:10.1302/0301-620X.96B2.31136
7. Wilson TJ, Chang KW, Yang LJ. Depression and anxiety in traumatic brachial plexus injury patients are associated with reduced motor outcome after surgical intervention for restoration of elbow flexion. Neurosurgery. 2016;78(6):844–850. doi:10.1227/NEU.0000000000001086
8. Bekeris J, Wilson LA, Fiasconaro M, et al. New onset depression and anxiety after spinal fusion surgery: incidence and risk factors. Spine. 2020;45(16):1161–1169. doi:10.1097/BRS.0000000000003467
9. Ananthakrishnan AN, Gainer VS, Cai T, et al. Similar risk of depression and anxiety following surgery or hospitalization for Crohn’s disease and ulcerative colitis. Am J Gastroenterol. 2013;108(4):594–601. doi:10.1038/ajg.2012.471
10. Wilson L, Bekeris J, Fiasconaro M, et al. Risk factors for new-onset depression or anxiety following total joint arthroplasty: the role of chronic opioid use. Reg Anesth Pain Med. 2019;44:990–997. doi:10.1136/rapm-2019-100785
11. Morlion B, Schäfer M, Betteridge N, et al. Non-invasive patient-controlled analgesia in the management of acute postoperative pain in the hospital setting. Curr Med Res Opin. 2018;34(7):1179–1186. doi:10.1080/03007995.2018.1462785
12. Finlay JE, Leslie K. Sedation/analgesia techniques for nonoperating room anesthesia: new drugs and devices. Curr Opin Anaesthesiol. 2021;34(6):678–682. doi:10.1097/ACO.0000000000001057
13. Lehmann KA. Tramadol in acute pain. Drugs. 1997;53(Suppl 2):25–33. doi:10.2165/00003495-199700532-00007
14. Scott LJ, Perry CM. Tramadol: a review of its use in perioperative pain. Drugs. 2000;60(1):139–176. doi:10.2165/00003495-200060010-00008
15. Terracina S, Robba C, Prete A, et al. Prevention and treatment of postoperative pain after lumbar spine procedures: a systematic review. Pain Pract. 2018;18(7):925–945. doi:10.1111/papr.12684
16. Jacobsen JPR, Krystal AD, Krishnan KRR, et al. Adjunctive 5-hydroxytryptophan slow-release for treatment-resistant depression: clinical and preclinical rationale. Trends Pharmacol Sci. 2016;37(11):933–944. doi:10.1016/j.tips.2016.09.001
17. Haenisch B, Bönisch H. Depression and antidepressants: insights from knockout of dopamine, serotonin or noradrenaline re-uptake transporters. Pharmacol Ther. 2011;129(3):352–368. doi:10.1016/j.pharmthera.2010.12.002
18. Dell’Osso B, Palazzo MC, Oldani L, et al. The noradrenergic action in antidepressant treatments: pharmacological and clinical aspects. CNS Neurosci Ther. 2011;17(6):723–732. doi:10.1111/j.1755-5949.2010.00217.x
19. Williams T, Hattingh CJ, Kariuki CM, et al. Pharmacotherapy for social anxiety disorder (SAnD). Cochrane Database Syst Rev. 2017;10(10):Cd001206. doi:10.1002/14651858.CD001206.pub3
20. Duan G, Bao X, Yang G, et al. Patient-controlled intravenous tramadol versus patient-controlled intravenous hydromorphone for analgesia after secondary cesarean delivery: a randomized controlled trial to compare analgesic, anti-anxiety and anti-depression effects. J Pain Res. 2019;12:49–59. doi:10.2147/JPR.S184782
21. Wu Z, Zhao P, Peng J, et al. A patient-controlled intravenous analgesia with tramadol ameliorates postpartum depression in high-risk woman after cesarean section: a randomized controlled trial. Front Med. 2021;8:679159. doi:10.3389/fmed.2021.679159
22. Zhang J, Su H, Tao J, et al. Relationship of impulsivity and depression during early methamphetamine withdrawal in Han Chinese population. Addict Behav. 2015;43:7–10. doi:10.1016/j.addbeh.2014.10.032
23. Li SX, Yan SY, Bao YP, et al. Depression and alterations in hypothalamic-pituitary-adrenal and hypothalamic-pituitary-thyroid axis function in male abstinent methamphetamine abusers. Hum Psychopharmacol. 2013;28(5):477–483. doi:10.1002/hup.2335
24. Yang Z, Jia H, Lu Y, et al. Prevalence and related factors of depression and anxiety in a cohort of Chinese elderly caregivers in the nursing home. J Affect Disord. 2021;295:1456–1461. doi:10.1016/j.jad.2021.09.026
25. Yue T, Li Q, Wang R, et al. Comparison of Hospital Anxiety and Depression Scale (HADS) and Zung self-rating anxiety/depression scale (SAS/SDS) in evaluating anxiety and depression in patients with psoriatic arthritis. Dermatology. 2020;236(2):170–178. doi:10.1159/000498848
26. Chen LX, Ji DH, Zhang F, et al. Richards-Campbell sleep questionnaire: psychometric properties of Chinese critically ill patients. Nurs Crit Care. 2019;24(6):362–368. doi:10.1111/nicc.12357
27. Obanor OO, McBroom MM, Elia JM, et al. The impact of earplugs and eye masks on sleep quality in surgical ICU patients at risk for frequent awakenings. Crit Care Med. 2021;49(9):e822–e832. doi:10.1097/CCM.0000000000005031
28. Jacobi F, Wittchen HU, Holting C, et al. Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German health interview and examination survey (GHS). Psychol Med. 2004;34(4):597–611. doi:10.1017/S0033291703001399
29. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):593–602. doi:10.1001/archpsyc.62.6.593
30. Andrews G, Henderson S, Hall W. Prevalence, comorbidity, disability and service utilisation. Overview of the Australian national mental health survey. Br J Psychiatry. 2001;178:145–153. doi:10.1192/bjp.178.2.145
31. Zhen L, Li X, Gao X, et al. Dose determination of sufentanil for intravenous patient-controlled analgesia with background infusion in abdominal surgeries: a random study. PLoS One. 2018;13(10):e0205959. doi:10.1371/journal.pone.0205959
32. Sun Z, Zhu Z, Yang G, et al. The 95% effective dose of nalbuphine in patient-controlled intravenous analgesia for patients undergoing laparoscopic total hysterectomy compared to equivalent sufentanil. Medicine. 2020;99(22):e20424. doi:10.1097/MD.0000000000020424
33. Oh SK, Lee IO, Lim BG, et al. Comparison of the analgesic effect of sufentanil versus fentanyl in intravenous patient-controlled analgesia after total laparoscopic hysterectomy: a randomized, double-blind, prospective study. Int J Med Sci. 2019;16(11):1439–1446. doi:10.7150/ijms.34656
34. Lee HM, Kil HK, Koo BN, et al. Comparison of sufentanil- and fentanyl-based intravenous patient-controlled analgesia on postoperative nausea and vomiting after laparoscopic nephrectomy: a prospective, double-blind, randomized-controlled trial. Int J Med Sci. 2020;17(2):207–213. doi:10.7150/ijms.39374
35. Wardle MC, Fitzgerald DA, Angstadt M, et al. Effects of oxycodone on brain responses to emotional images. Psychopharmacol. 2014;231(22):4403–4415. doi:10.1007/s00213-014-3592-4
36. Rideout A, Lindsay G, Godwin J. Patient mortality in the 12 years following enrolment into a pre-surgical cardiac rehabilitation programme. Clin Rehabil. 2012;26(7):642–647. doi:10.1177/0269215511429161
37. Wang SY, Jiang XY, Jan WC, et al. A comparative study of postnatal depression and its predictors in Taiwan and mainland China. Am J Obstet Gynecol. 2003;189(5):1407–1412. doi:10.1067/S0002-9378(03)00673-2
38. Wisner KL, Sit DK, McShea MC, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70(5):490–498. doi:10.1001/jamapsychiatry.2013.87
39. Erdoğan E, Demir S, Çalışkan BB, et al. Effect of psychological care given to the women who underwent hysterectomy before and after the surgery on depressive symptoms, anxiety and the body image levels. J Obstet Gynaecol. 2020;40(7):981–987. doi:10.1080/01443615.2019.1678574
40. Hillman DR. Sleep loss in the hospitalized patient and its influence on recovery from illness and operation. Anesth Analg. 2021;132(5):1314–1320. doi:10.1213/ANE.0000000000005323
41. Singh M, Gali B, Levine M, et al. Integrating sleep knowledge into the anesthesiology curriculum. Anesth Analg. 2021;132(5):1296–1305. doi:10.1213/ANE.0000000000005490
42. Pengo MF, Won CH, Bourjeily G. Sleep in women across the life span. Chest. 2018;154(1):196–206. doi:10.1016/j.chest.2018.04.005
43. Nevšímalová S. Sleep and sleep-related disorders in women. Cas Lek Cesk. 2019;158(7–8):321–322.
44. Perrot S. Fibromyalgia syndrome: a relevant recent construction of an ancient condition? Curr Opin Support Palliat Care. 2008;2(2):122–127. doi:10.1097/SPC.0b013e3283005479
45. Koncz S, Papp N, Menczelesz N, et al. EEG and sleep effects of tramadol suggest potential antidepressant effects with different mechanisms of action. Pharmaceuticals. 2021;14:5. doi:10.3390/ph14050431
46. Wang D, Teichtahl H. Opioids, sleep architecture and sleep-disordered breathing. Sleep Med Rev. 2007;11(1):35–46. doi:10.1016/j.smrv.2006.03.006
47. Shaw IR, Lavigne G, Mayer P, et al. Acute intravenous administration of morphine perturbs sleep architecture in healthy pain-free young adults: a preliminary study. Sleep. 2005;28(6):677–682. doi:10.1093/sleep/28.6.677
48. Dimsdale JE, Norman D, DeJardin D, et al. The effect of opioids on sleep architecture. J Clin Sleep Med. 2007;3(1):33–36.
49. Wang L, Tobe J, Au E, et al. Selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors as adjuncts for postoperative pain management: systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2022;128(1):118–134. doi:10.1016/j.bja.2021.08.032
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.