")
Back to Journals » International Journal of General Medicine » Volume 16
Effects of (In)Congruency in Fertility Motivation on Fertility Desire and Intention Among Couples Living with HIV: A Dyadic Approach
Authors Guo Y , Liu J, Du Y , Chongsuvivatwong V
Received 26 April 2023
Accepted for publication 19 July 2023
Published 23 August 2023 Volume 2023:16 Pages 3721—3734
DOI https://doi.org/10.2147/IJGM.S418792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yingwu Guo,1,2,* Jun Liu,1,* Yingrong Du,1,* Virasakdi Chongsuvivatwong2,*
1Department of Infectious Diseases, Third People’s Hospital of Kunming City, Kunming, People’s Republic of China; 2Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
*These authors contributed equally to this work
Correspondence: Virasakdi Chongsuvivatwong, Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, 15 Kanjanavanich Road, Hat Yai, Songkhla, 90110, Thailand, Tel +66897350098, Email [email protected]
Background: Fertility decision-making plays a negligible role in completing fertility goals among couples living with HIV (CLWH). Being commonly matched concerning fertility motivation seems essential for fertility desire/intention. Few studies report on intra-couple congruences or incongruences in fertility motivation on desire/intention. This study aims to assess the effects of (in)congruency in fertility motivation on fertility desire and intention among couples living with HIV.
Methods: This study uses the actor-partner interdependence model (APIM) to assess the independent direct and indirect effect of fertility motivation on intention, and dyadic response surface analysis with congruency/incongruent effect (DRSA) of fertility motivation on intention using fertility desire as mediator variable among CLWH. CLWH were selected from a clinic in Kunming, China, between October and December 2020. Cross-sectional research included 314 CLWH.
Results: APIM revealed that the wife’s fertility motivation had an indirect influence on fertility intention of couples mediated by her fertility desire (R2 = 0.42). There was a significant effect on fertility intention by interaction of (in)congruency in fertility motivation among couples. DRSA shows that linear congruency in fertility motivation of both husband and wife increased fertility desire and intention of couples. However, if there was an incongruent in fertility motivation among husband and wife, husband’s domination in fertility motivation was common and negatively affect the wife’s fertility desire to have a child. Overall, couples who were matched on fertility motivation reported a significant greater relationship with fertility intention than couples who were mismatched.
Conclusion: Counseling could help both the husband and wife achieve a greater positive fertility intention by addressing comparable fertility goals.
Keywords: (in)congruency, dyadic data analysis, Traits-Desires-Intentions-Behavior model, couples living with HIV
Introduction
Fertility decision-making is likely to change in the human immunodeficiency virus (HIV) context which is marked by psychosocial adjustment for both the husbands and wives. A systematic review found that 42.0% of people living with HIV wanted to have children.1 Fertility desires/intentions ranged widely from 8% to 84% in low- and middle-income countries and 32% to 58% in high-income countries based on HIV status of their partners.2–6 During the course of life until the end of an individual’s reproductive phase, the established childbearing motivations find expression in conscious desires and intentions, in behavior, and ultimately in the occurrence of fertility events.7 A previous study in China revealed that one-fifth of CLWH had the intention to have a child.8 Among CLWH, there were interpersonal and social factors such as gender expectations for women to bear child and the desires of partners for the women to have a child influence women’s desire to conceive.9 A systematic review revealed that dominance of women incongruency, women empowerment, was positively associated with the ability to make fertility decisions and increase spousal communication.10 Previous research that examined the fertility of expectant couples found that positive fertility motivations were the most often reported reason for positive fertility desire under antiretroviral treatment (ART), as well as prevention of mother-to-child HIV transmission efficacy.11,12
Toward the comprehensive understanding on fertility, our study was based on the Traits-Desires-Intentions-Behavior (TDIB) model,13 which can be integrated into a dyadic approach which evaluates the gender influence on fertility. TDIB model states that the four main steps of fertility decision-making are fertility motivation, desire, intention, and behavior. Based on the TDIB model, the actor-partner interdependence model (APIM) was developed to assess the effects of fertility motivation on intention mediated by desire.14 The actor-partner refers to the wife and husband, respectively. Fertility motivation is the feeling or faith of happiness, wellbeing, identity, social control, and continuity of offspring in the family.15 Fertility desire has been defined as the desire/willingness to have a child or another child at the present. Fertility desire reflects a wish to achieve a childbearing goal by a sort of action. Fertility intention consists of a particular choice to seek a reproductive objective and a plan for putting that fertility decision into action.16 Stable motivational dispositions affect reproductive behavior by influencing the desire and intention to have a child.16 HIV-positive Canadian women supported the TDIB model.17 Higher desire and intentions lead to more child-bearing. Knowing the relationship between the objectives of HIV-positive couples, such as happiness, well-being, identity, and continuity, fertility desire, and intention, might help enhance the bearing of a child. This complex phenomenon was assessed by dyadic response surface analysis (DRSA) by regression analysis and illustrated three-dimensional relationships between combinations of the actor’s (x-axis) and partner’s (y-axis) fertility motivation, while the wives’ and husbands’ fertility desires and intentions were the z-axis.18 Understanding the process from stable motivational dispositions to fertility intention enhances the knowledge of HIV-positive women’s reproductive decision-making. This evidence-based information is useful for planning public health policies and reproductive health services for HIV couples to complete their desires/intentions to have a child.19
Within husband and wife, there is a dyadic process in the content of reproduction. One partner has an influence upon the other partner’s desire/intention to have a child.20 HIV-positive couples have the unusual challenge of managing their fertility within the HIV setting. The combination of both partners’ desire/intention to have children, as opposed to the influence of each partner’s unique fertility motivation, may thus be crucial in understanding both partners’ fertility desire/intention. However, little is known regarding the possible link between a couple’s concordance or discordance on fertility motivation, such as happiness, well-being, and identity, and the consequences for childbearing desire/intention. Partners in fertility were likely to have comparable fertility desires.21 A prior study posited that similarity between partners has advantages for both individuals and their fertility behavior among CLWH.22 Joint fertility decision-making in couples is good since it enables them to support each other better.23 Individuals with similar motivations are more likely to exhibit similar desires and intentions in response to a reproductive event,11 such as the commencement of HIV transmission worries associated with the pregnancy if they have identical motivations. Indeed, factors such as increased dyadic motivation have been observed to influence the reproductive intentions of couples in early ART among HIV-positive East Africans.24 If there is a lack of motivation to have a child reflected in either partner, it results in a lack of intention by the couple to bear a child.25 The previous studies used a dyadic approach to assess the fertility desire and intention by other factors such as stigma, HIV status, HIV-related worriers and living children.26,27
The objective of the current study was to document the effects of (in)congruency in fertility motivation linked to intention via desire among CLWH using the APIM and DRSA. To achieve this objective, we divided the analysis into three parts: the causal pathway; degree of husband-wife congruence of fertility motivations; and congruency effect of fertility motivation between wives and husbands on fertility desire/intention.
Methods
Study Design and Setting
This was a cross-sectional study conducted in China between October and December 2020 in an ART clinic of Department of Infectious Diseases, the Third People’s Hospital in Kunming City, Yunnan Province, South Region of People’s Republic of China. Kunming City is the site of an ongoing HIV epidemic and the biggest tertiary care center serving HIV patients. The hospital’s infectious disease antiretroviral treatment (ART) clinic is one of the pilot sites for a prevention of mother to child transmission program in South Region of China.
Our study involved 314 couples to determine childbearing motivation. Couples who met the following criteria were invited to participate in this study: aged 18–45 years for females, 18–50 years for males, and able to read and write in Chinese. Couples who consented were requested to fill out the questionnaire separately in a quiet place, which took about 15–30 minutes to complete.
Study Variables
Demographic Characteristics (Descriptive Variables)
The questionnaire assessed ethnicity, age, educational attainment, occupation, religion, income, and registered residence of the subjects.
Fertility Motivation (Independent Latent Variables)
Fertility motivation was measured by the Parenthood Subscale of the People Living With HIV Scale.28 The scale is widely used as a self-report instrument. It consists of 11 items designed to measure HIV-related fertility motivation. Items are rated on a 5-point Likert scale ranging from 1 (definitely disagree) to 5 (definitely agree). Total subscale scores range from 11 to 55. Higher scores indicate greater levels of fertility motivation. The Chinese version of this scale was validated and is widely used among people living with HIV in China. For this study, Cronbach’s alpha coefficients of the motivation for husband and wife were 0.84 and 0.87, respectively.
Fertility Desire (Independent Mediator Variable) and Intention (Dependent Variable)
Similar to previous studies regarding fertility intentions, all respondents were asked, “Looking to the future, do you intend to have (another) baby at some time?” (response options “yes”, “not sure”, or “no”).29 All respondents who gave positive answers were also asked, “In your case, how likely are you going to have another child within the next three years?” on a five-point scale that ranged from “definitely not” to “definitely yes”.30
Sample Size Estimation
A sample size within this range can ensure that the difference between the estimated sample and the population parameter remains stable and modest. To determine the required sample size for our research, which involved using a structural equation model (SEM) with 26 observable variables and 10 latent variables, we utilized the Structural Equation Model Sample Size Calculator.31 Our calculation considered an expected effect size of 0.3, a type I error rate of 0.05, and a desired statistical power level of 0.8. According to the calculator, a minimum sample size of 268 couples was necessary to detect the specified effect.
Data Collection
One of the investigators, who was employed at the study hospital, prepared a sampling framework using the list of current patients from the ART clinic in the ART database. The sampling frame data consisted of the patient’s clinic-specific identification number, gender, and the date of their next appointment. To select participants, the investigators utilized a computer program to randomly sample patients, stratifying them by sex.
On the day of the appointment, the investigators personally approached each patient, introduced themselves, evaluated the patient’s eligibility, provided study information, and inquired about their interest in participating. Each potential participant was given approximately 10 minutes to decide regarding their participation in the study interview. Subsequently, the investigators obtained verbal informed consent from the patients before commencing the study interview. Additionally, patients were asked for permission to contact their partner, seeking to provide information and request verbal informed consent. To this study, a “couple” refers to the patient and their partner as a unit.
The study instrument was a structured interview questionnaire. The data collection process involved four skilled research assistants who were part of a team associated with the ART clinic in Kunming City. Following the provision of study details and acquisition of verbal informed consent, each participant was interviewed individually, separate from their spouse. Face-to-face interviews were conducted with both the patient and their spouse, while telephone interviews were conducted with the spouse if they resided at a distant location. These interviews typically lasted between 15 and 30 minutes. It is noteworthy that all questionnaires were completed and returned without any missing information.
Initially, a total of 325 couples were invited to participate in the study. Eleven couples had at least one spouse who did not complete the consent form. Finally, 314 couples (96.6% of all recruited couples) were included in this analysis.
Statistical Analysis
The descriptive statistics and bivariate correlations for all psychometric variables were computed. Normal distributions were evaluated by assessing estimates of skewness and kurtosis, and acceptable normality was determined using cutoffs of −3/+3.32 We applied two dyadic models to explore the congruency effect of fertility motivation and desire/intention, which included the APIM and DRSA based on the TDIB model.
Actor-Partner Interdependence Model (APIM)
The first part of the analysis was to assess the individual effects of the husbands’ and wives’ fertility motivations on intention mediated by desire using the APIM.14 Figure 1 summarizes our APIM according to the TDIB model. Actor causation pathway for the wives is represented in the upper part and for the husbands in the lower part. Fertility motivation is a latent variable loaded with four latent variables: happiness; well-being; identity; and continuity. Each of these variable loads refers to its own observed variable (3 items for happiness (“h”), 2 items for well-being (“b”), 3 items for identity (“i”), and 3 items for continuity (“c”) in which h denotes the husband and w denotes the wife). Fertility motivation influences fertility intention directly and through fertility desire. The crossing arrows between upper and lower parts indicate cross-influences of each partner on fertility desire and intention. Finally, the errors from predicting fertility intention of the wife and husband are correlated. The first part of the analysis did not test for the similarity effect of the husbands’ and wives’ motivations on fertility desire and intention.
 |
Figure 1 Actor-partner interdependence model to assess the effects of the husbands’ and wives’ motivations on fertility desire and intention. |
Frequencies of Fertility Motivation Discrepancies and Congruence Between Husbands and Wives
The second section determined whether the husband or wife has similarity (congruence) in fertility motivation. For each couple, the difference in the motivation factor scores was determined, and the standard deviation (SD) in the difference was obtained. The wives’ ratings were deducted from the husbands’ ratings. The couple’s fertility motivation was dominated by the husband if the husband-wife score difference was larger or smaller than the SD of −0.5. If the difference was larger than the SD of 0.5, fertility motivation was dominated by the wife. Otherwise, there was congruence in fertility motivation.
Effects of Congruency
The third section tested the effects of dyadic congruency in fertility motivation on fertility desire/intention using the DRSA.18 We examined polynomial regression route models with our dyadic data. Four equations independently predict husband and wife fertility desire and intention. The equations share variables that include his/her own and the spouse’s fertility motivation, their interaction, and the quadratic terms of the motivation in case the response was curvilinear.




Each equation assessed two linear (fertility motivation) coefficients, one linear–linear interaction, and two quadratic coefficients.
For each equation, the line of congruence and line of incongruence with the interaction/quadratic terms of outcomes are defined as follows:
Slope of linear congruence = β1 wife’s motivation + β2 husband’s motivation
Slope of curvature congruence = β4 wife’s motivation2 + β5 husband’s motivation2 +
β3 interaction of the wife’s and husband’s motivations
Slope of linear incongruence of wife = β1 wife’s motivation − β2 husband’s motivation
Slope of linear incongruence of husband = β2 husband’s motivation − β1 wife’s motivation
Slope of curvature incongruence of wife = β4 wife’s motivation2 – β5 husband’s motivation2 +
β3 interaction of the wife’s and husband’s motivations
Slope of curvature incongruence of husband = Β5 husband’s motivation2 − β4 wife’s motivation2 +
β3 interaction of the wife’s and husband’s motivations
Our major concern in the present research was the relationship between the degree of disagreement between the wife’s own level of fertility motivation and her husband’s level of fertility motivation (curvature incongruence of wife and husband) and the direction of disagreement (linear incongruence of wife and husband) and each partner’s fertility desire and intention. The analysis also examined how the degree of agreement between a wife’s own level of fertility motivation and her husband’s level of motivation (linear congruence) was associated with fertility desire and intention—that is, when partners have high agreement, is it better to agree on higher versus lower fertility desire and intention?—and whether linear congruence is best described by a nonlinear relationship (curvature congruence)—that is whether the association between agreement and deliberation is linear or nonlinear.
Statistical Software and Model Fit
All APIM and DRSA models were tested in two steps. First, we set up an unconstrained model in which all parameters were estimated freely. Second, we forced all of the actor and partner effects to be equal for wives and husbands in the constrained model. Subsequently, we evaluated the saturated model between the constrained and unconstrained model via the χ2 difference test. All models were analyzed using the lavaan package for R.33 The APIM used the maximum likelihood robust estimator. The overall model fit was evaluated using multiple fit indices as suggested in the literature. Specifically, five goodness-of-fit indices were used that included the chi-square/degree of freedom (χ2/df), Tucker-Lewis Index (TLI), comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Values of χ2/df <3, TLI and CFI >0.90, and RMSEA and SRMR <0.08 are indicative of a good fit with the data. We generated confidence intervals using bootstrapped percentile samples in the DRSA. Percentile bootstrapping was done using 10,000 bootstrapped samples.
Results
Characteristics of CLWH
A total of 314 couples were identified, and verbal commitments were obtained to participate in the research with their spouses and be included in the data analysis. The mean (SD) ages of wives and husbands were 33.8 (5.2) and 36.9 (5.8) years, respectively. In the husband group, the most frequent educational level was senior high school or less. In the wife group, the most common educational level was junior high school or less. The percentage of husbands with a graduate degree or higher was 26.4%, which was more than the proportion of wives with a graduate degree or higher (17.8%). When questioned about their job status, the majority of wives in the study said they were unemployed. Many respondents were of Han ethnicity and dwelled in rural areas. The majority of couples (63.2%) indicated New Rural Cooperative Medical Insurance as their supplier of medical insurance. Table 1 displays the sociodemographic and HIV serostatus characteristics of the HIV-positive couples. As a variable at the couple level, more than half of the couples had a low household monthly income of less than CNY 9999. HIV positive on the wife’s side was somewhat more prevalent than on the husband’s side among the HIV discordant couples. The socio-economic and HIV status characteristics are summarized in Table 1.
 |
Table 1 Socio-Demographic Characteristics |
Descriptive Statistics and Bivariate Correlation in Husband-Wife Dyads
Table 2 shows Pearson’s correlation coefficients between fertility motivation and fertility desire/intention in both the husbands and their wives. Despite the high mean values of the variables, the correlations between husband and wife in the observed and latent variables of fertility motivation and desire/intention were within the range of 0.3 to 0.74. In this study, all scales had good Cronbach’s alpha reliability (CR = 0.73–0.96) and good average variance extracted discriminant validity coefficients (0.51–0.93).
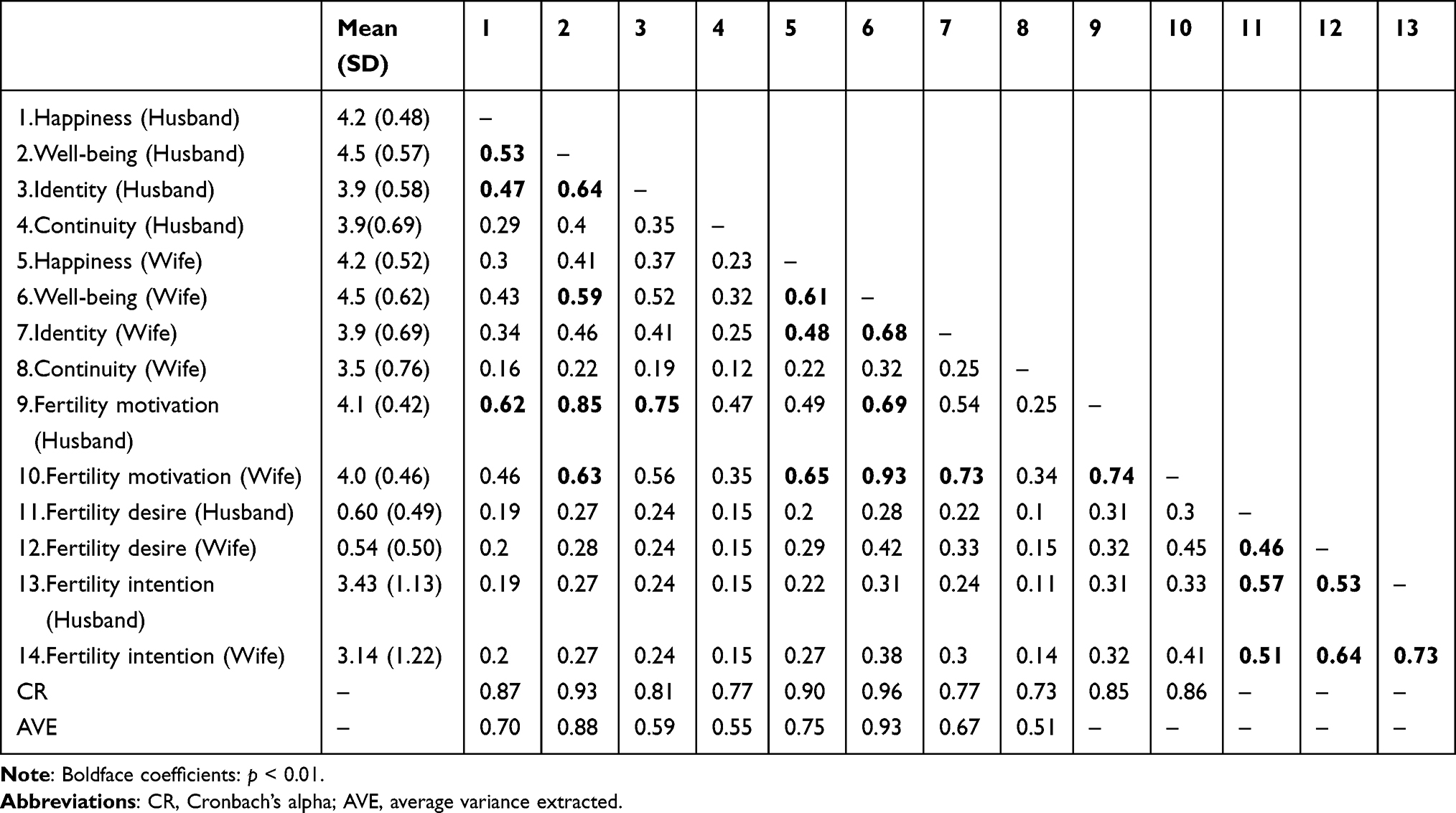 |
Table 2 Means, Standard Deviations, Correlations, and Average Variance Extracted Among the Study Variables |
Actor-Partner Interdependence Modeling (APIM)
Figure 2 summarizes the results of the APIM analysis. The latent variable fertility motivation had a high load level on the observed variable. The wife’s fertility motivation had an indirect influence on fertility intention mediated by fertility desire (R2 = 0.42). Consistent with results from both the husband-and-wife correlation matrix for all variables summarized in Table 2, APIM showed significant influence of the husband’s fertility desire on both the wife’s fertility desire and intention and vice versa (R2 = 0.48). This model fit the data well: χ2/df = 2.5; CFI = 0.920; TLI = 0.906; RMSEA = 0.069; and SRMR = 0.074. There was no significant cross-influence of fertility motivation of either the husband or wife on their fertility desires and intentions. The model was not adjusted for the congruency and incongruency effect of the husbands’ and wives’ motivations on their fertility desire and intention.
 |
Figure 2 Actor-partner interdependence mediation model of fertility intention. Note: **pvalue<0.01. |
Dyadic Response Surface Analysis
Frequencies of Fertility Motivation Discrepancies and Congruence
More than half (165, 52.5%) of the 314 couples had congruence in fertility motivation. Ninety-nine (31.5%) and 50 (15.9%) had husband and wife dominance, respectively (see Supplemental Appendix Table 1). The frequencies of discrepancy between the wives’ and husbands’ motivations were larger than 10%, which indicated that DRSA was warranted for analyzing the level of congruence in the data.
Congruency and Incongruency in Fertility Motivation and Fertility Desire/Intention
Table 3 summarizes the DRSA model analysis results to determine the congruency effect of fertility motivation by the husbands’ and wives’ intentions and fertility desires. Figures 3 and 4 are the corresponding surface plots for fertility intention and desire of the wife (a) and husband (b) (z-axis), which was influenced by both the wife’s (x-axis) and husband’s (y-axis) motivations. There was a significant effect on the husbands’ fertility intention by interaction of motivation by the husbands and wives, which indicated influence of congruence and incongruence of the husbands’ and wives’ motivations to fertility intention.
 |
Table 3 Dyadic Polynomial Regression Coefficients and Response Surface Parameters of Fertility Motivation and Fertility Desire of Both Husbands and Wives (N = 314 Couples) |
 |
Figure 3 (a and b) Dyadic response surface plots for congruence of husband-wife fertility motivation to predict fertility intention. |
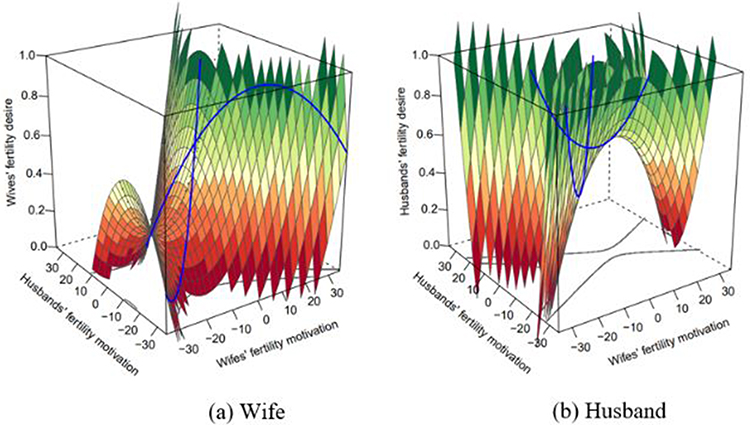 |
Figure 4 (a and b) Dyadic response surface plots for the association between the wives’ own and their husbands’ fertility motivation and desire. |
Surface analysis showed that the linear congruence of husbands’ and wives’ motivations (α1 = β1 + β2) significantly enhanced fertility desire and intention of both the husband and wife. Figures 3a, b, 4a and b show that the peaks of fertility desire and intention reached higher levels with an increase in value of the husbands’ and wives’ motivations. More specifically, the curvature congruence (α2 = β4 + β5 + β3) indicated that the husbands’ fertility intentions increased more sharply when both the husbands’ and wives’ motivations corresponded to increasingly high levels (Figure 3b).
Incongruence of fertility motivation, on the other hand, affects only the fertility desire rather than fertility intention. When the wife’s motivation was higher than the husband’s motivation (linear incongruence of wife (α3) = β1 − β2 > 0), it increased her fertility desire. In the reverse condition, it means that when the husband’s motivation was higher than the wife’s motivation (linear incongruence of wife = β1 − β2 < 0) in incongruent couples, it would lead to a lower fertility desire in the wife. Figure 4a reveals the lowest peak of the wives’ fertility desire with an increase in the husbands’ motivation over the wives’ motivation. In addition, if there was a higher discrepancy between the motivations of the wives and husbands (curvature incongruence of husband (α4) = β4 − β5+ β3), ie, stronger husband motivation in incongruent couples, it would result in a positive desire of the husband to have a child (Figure 4b). However, the degree of motivation discrepancy was not associated with fertility intention for either the husband or wife; that is, overall, couples who were matched on fertility motivation reported a significantly greater relationship with fertility intention than couples who were mismatched.
Discussion
Our study revealed the effects of (in)congruency in fertility motivation on fertility desire and intention among CLWH to formulate the effective counselling strategy for childbearing with the psychosocial support on fertility among them. Among CLWH, we found that fertility desire and intention were highly correlated and had mutual influence between the wife and husband. Fertility motivation influenced fertility desire on the wife’s side but not on the husband’s side. Individual fertility motivation had no significant effect on the spouse. Congruence of fertility motivation was found in more than half of the couples. In the case of incongruent couples, the husband’s motivation was often stronger than the wife’s motivation. Congruence in fertility motivation enhanced the individual fertility desire/intention on both sides, whereas the husband’s stronger motivation depleted fertility desire in the wife.
Casual Pathway of Fertility Motivation-Desire-Intention
The linkage between fertility desire and intention among CLWH was reported in a previous study in Ontario, Canada.17 We confirmed this relationship in CLWH and demonstrated a strong intercorrelation within CLWH. We also found influences of individual fertility desire on the spouse’s fertility intention.
We put fertility motivation as a factor influencing fertility desire. This was confirmed on the wife’s side but not on the husband’s side. This difference was unexpected because there was a strong correlation (r = 0.74) between the husbands’ and wives’ fertility motivation. Perhaps, such a difference was due to a difference in perceived fertility responsibility in Chinese women and men. In the Chinese culture, women bear more responsibility on fertility than the husband.34,35 Chinese wives are expected to give birth to continue the blood line of the husband. Also, the mother plays more important roles in raising children. Family planning procedures are more commonly done on the wife’s side.36 With low perceived fertility responsibility among men, their fertility motivation would not have significant effect on fertility desire and intention. Globally and in China, the husband plays a passive role in fertility regulation. For CLWH without male heirs, HIV-positive women risk desertion because males may have little decision-making authority. Mothers-in-law who urge their daughters-in-law to have children do not inquire about lineage with their husbands in Vietnam or in China.21,37
Congruency and Congruency of Fertility Motivation on Fertility Desire/Intention in Wife-Husband Dyads
Our results further highlight the importance of moving beyond one-way perspectives and considering both the perspectives of the wives and husbands when examining fertility motivation.
Our findings showed that more than one-half of congruence in fertility motivation among the wives and husbands were consistent with most previous studies using a DRSA among couples.38–40 Among the incongruent couples, the husband was more likely to have stronger fertility motivation than the wife.
The positive effects of congruence on fertility motivation on both the wife’s and husband’s fertility desire and intention indicated a statistical effect. With synergism, congruent couples would be more successful in carrying out their family plan. On the other hand, a husband’s stronger motivation was not only ineffective in raising his fertility desire and intention but may also deplete the effect of an already lower motivation of the wife on fertility desire and intention. It may indicate that among women with low fertility motivation, demonstrating motivation by her husband would have a further negative effect on her own fertility desire and intention. If this causal relationship is true, the dominating husband should be counselled to be aware of this possible unwanted effect and if possibly adjust himself to fit with this incongruent setting. A previous study also revealed a similar pattern of fertility desire which was mostly dominant in male and less in female highlighting the needs of specific health strategy in the contents of fertility for PLHIV.1
Our Study Has Some Strengths and Limitations
Our study used standardized psychometric questionnaires. This dyadic analysis enabled us to gain better insight into the interrelationship within CLWH using the similarity and discrepancy of fertility motivation based on the TDIB model. More important is our finding of the negative effect of incongruence of fertility motivation of the wives with low fertility motivation. However, although this statistical analysis gave clear results, the actual causal relationship needs to be confirmed with similar studies. The fertility desire and intention can be influenced by several factors (especially socio-cultural barriers, religious beliefs, gender norms, stereotypes, attitudes towards gender equality, and women’s and men’s roles within and outside of the family). Our quantitative study could not assess those factors. It would be more answerable by conducting qualitative studies to explore these factors. Our study result had the limitation to generalize the whole country.
For public health implications, the desire and expectation of having children among CLWH carry significant consequences in terms of preventing the transmission of HIV from parent to child and within heterosexual relationships. It highlights the necessity of consideration on effects of (in)congruency in fertility motivation on fertility desire and intention among CLWH during counseling to provide the psychosocial support for well-informed decision-making regarding childbearing and safe family planning among them.
Conclusions
Despite the high level and correlation of fertility desire and motivation in the study of CLWH, incongruence in fertility motivation should not be ignored. Our findings may suggest the need to examine and compare fertility motivation within the couple before giving fertility advice. The husband’s domination in fertility motivation was common and may negatively affect the wife’s fertility desire and intention if her fertility motivation is already weak.
Abbreviations
HIV, human immunodeficiency; ART, antiretroviral therapy; CLWH, couples living with HIV; APIM, actor-partner interdependence model; DRSA, dyadic response surface analysis; TDIB, Traits-Desire-Intention-Behavior (TDIB); χ2/df, chi-square/degree of freedom; CFI, comparative fit index; TLI, Tucker-Lewis Index; SRMR, standardized root means square residual; RMSEA, root mean square error of approximation.
Data Sharing Statement
All pertinent information is contained in the text and its accompanying information files.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of Prince of Songkla University (REC-63-208-18-1) and the Research Ethics Review Committee of the Third People’s Hospital (2020072001). In this study, pseudonyms were used to protect the identity of the participants.
Acknowledgments
This study is a part of the first author’s thesis in partial fulfillment of the requirements for a Ph.D. degree in Epidemiology at Prince of Songkla University, Songkhla, Thailand. We greatly appreciate the assistance from the staff members of the HIV treatment center who supported our study at the Third People’s Hospital in Kunming, China. The opinions expressed in this viewpoint are solely those of its writers and do not necessarily reflect the opinions of the institutions with which they are connected.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was received from the Higher Education Research Promotion and Thailand’s Education Hub for the Southern Region of ASEAN Countries Project Office of the Higher Education Commission (TEH-AC:016/2018).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Guo Y, Chongsuvivatwong V, Songwathana P, Liu J, Wichaidit W. Fertility desire among HIV-positive individuals in the Chinese sociocultural context: a qualitative study. J Educ Health Promot. 2023;12(1):156. doi:10.4103/jehp.jehp_126_23
2. Martins A, Alves S, Chaves C, Canavarro MC, Pereira M. Prevalence and factors associated with fertility desires/intentions among individuals in HIV-serodiscordant relationships: a systematic review of empirical studies. J Int AIDS Soc. 2019;22(5):e25241. doi:10.1002/jia2.25241
3. Jose H, Madi D, Chowta N, et al. Fertility desires and intentions among people living with HIV/AIDS (PLWHA) in Southern India. J Clin Diagn Res. 2016;10(6):OC19–22. doi:10.7860/JCDR/2016/20282.7968
4. Kuete M, Yuan H, He Q, et al. Sexual practices, fertility intentions, and awareness to prevent mother-to-child transmission of HIV among infected pregnant women at the Yaounde central hospital. Sex Med. 2016;4(2):e95–103. doi:10.1016/j.esxm.2016.01.004
5. Muldoon KA, Kanters S, Birungi J, et al. “He said, she said”: assessing dyadic agreement of reported sexual behaviour and decision-making among an HIV sero-discordant couples cohort in Uganda. J Fam Plann Reprod Health Care. 2017;43(2):142–146. doi:10.1136/jfprhc-2015-101323
6. Mindry D, Wagner G, Lake J, et al. Fertility desires among HIV-infected men and women in Los Angeles County: client needs and provider perspectives. Matern Child Health J. 2013;17(4):593–600. doi:10.1007/s10995-012-1035-6
7. Miller WB, Rodgers JL, Pasta DJ. Fertility motivations of youth predict later fertility outcomes: a prospective analysis of national longitudinal survey of youth data. Biodemography Soc Biol. 2010;56(1):1–23. doi:10.1080/19485561003709131
8. Que M, ping JG, Du J, Li T. The fertility status of the married people living with HIV/AIDS in China. Contrast Media Mol Imaging. 2022;2022:e2938340. doi:10.1155/2022/2938340
9. Jones DL, Cook R, Potter JE, et al. Fertility desires among women living with HIV. PLoS One. 2016;11(9):e0160190. doi:10.1371/journal.pone.0160190
10. Upadhyay UD, Gipson JD, Withers M, et al. Women’s empowerment and fertility: a review of the literature. Soc Sci Med. 2014;2014:111–120. doi:10.1016/j.socscimed.2014.06.014
11. Klein J, Peña JE, Thornton MHI, Sauer MV. Understanding the motivations, concerns, and desires of human immunodeficiency virus 1–serodiscordant couples wishing to have children through assisted reproduction. Obstet Gynecol. 2003;101(5 Part 1):987–994. doi:10.1016/S0029-7844(03)00012-7
12. Rogers AJ, Achiro L, Bukusi EA, et al. Couple interdependence impacts HIV-related health behaviours among pregnant couples in southwestern Kenya: a qualitative analysis. J Int AIDS Soc. 2016;19(1):21224. doi:10.7448/IAS.19.1.21224
13. Miller WB. Childbearing motivations, desires, and intentions: a theoretical framework. Genet Soc Gen Psychol Monogr. 1994;120(2):223–258.
14. Cook WL, Kenny DA. The actor–partner interdependence model: a model of bidirectional effects in developmental studies. Int J Behav Dev. 2005;29(2):101–109. doi:10.1080/01650250444000405
15. Dyer S, Mokoena N, Maritz J, van der Spuy Z. Motives for parenthood among couples attending a level 3 infertility clinic in the public health sector in South Africa. Hum Reprod. 2008;23(2):352–357. doi:10.1093/humrep/dem279
16. Miller WB. Differences between fertility desires and intentions: implications for theory, research and policy. Vienna Yearb Popul Res. 2011;9:75–98.
17. Wagner AC, Ivanova EL, Hart TA, Loutfy MR. Examining the traits-desires-intentions-behavior (TDIB) model for fertility planning in women living with HIV in Ontario, Canada. AIDS Patient Care STDS. 2014;28(11):594–601. doi:10.1089/apc.2014.0075
18. Schönbrodt FD, Humberg S, Nestler S. Testing similarity effects with dyadic response surface analysis. Eur J Pers. 2018;32(6):627–641. doi:10.1002/per.2169
19. Finocchario-Kessler S, Dariotis JK, Sweat MD, et al. Do HIV-infected women want to discuss reproductive plans with providers, and are those conversations occurring? AIDS Patient Care STDS. 2010;24(5):317–323. doi:10.1089/apc.2009.0293
20. Shreffler KM, Tiemeyer S, McQuillan J, Greil AL, Spierling T. Partner congruence on fertility intentions and values: implications for birth outcomes. J Soc Pers Relat. 2019;36(8):2307–2322. doi:10.1177/0265407518787232
21. Tran BX, Duong HD, Nguyen AQ, Pham LD, Tran TT, Latkin CA. Child desire among men and women living with HIV/AIDS in the traditional culture of Vietnam. AIDS Behav. 2018;22(9):2888–2894. doi:10.1007/s10461-018-2029-1
22. Beyeza-Kashesya J, Ekstrom AM, Kaharuza F, Mirembe F, Neema S, Kulane A. My partner wants a child: a cross-sectional study of the determinants of the desire for children among mutually disclosed sero-discordant couples receiving care in Uganda. BMC Public Health. 2010;10(1):247. doi:10.1186/1471-2458-10-247
23. Miller WB, Pasta DJ. Couple disagreement: effects on the formation and implementation of fertility decisions. Pers Relatsh. 1996;3(3):307–336. doi:10.1111/j.1475-6811.1996.tb00119.x
24. Mujugira A, Heffron R, Celum C, et al. Fertility intentions and interest in early antiretroviral therapy among East African HIV-1–infected individuals in serodiscordant partnerships. J Acquir Immune Defic Syndr. 2013;63(1):e33. doi:10.1097/QAI.0b013e318288bb32
25. Mandell LN, Rodriguez VJ, Peltzer K, Weiss SM, Jones DL. Fertility intentions of women living with HIV and their male partners during the perinatal period in rural South Africa. Int J STD AIDS. 2021;32(8):740–750. doi:10.1177/0956462420987447
26. Guo Y, Wichaidit W, Du Y, Liu J, Chongsuvivatwong V. Mediation of the association between stigma and HIV status and fertility intention by fertility desire among heterosexual couples living with HIV in Kunming, China. PLoS One. 2022;17(12):e0278244. doi:10.1371/journal.pone.0278244
27. Guo Y, Du Y, Liu J, et al. Effects of HIV-related worries on fertility motivation moderated by living children among couples living with HIV: a dyadic analysis. Front Psychol. 2022;13:1000100. doi:10.3389/fpsyg.2022.1000100
28. Bell JS, Bancroft J, Philip A. Motivation for parenthood: a factor analytic study of attitudes towards having children. J Comp Fam Stud. 1985;16(1):111–119. doi:10.3138/jcfs.16.1.111
29. Bloom TL, Mosher W, Alhusen J, Lantos H, Hughes RB. Fertility desires and intentions among U.S. women by disability status: findings from the 2011–2013 national survey of family growth. Matern Child Health J. 2017;21(8):1606–1615. doi:10.1007/s10995-016-2250-3
30. Wagner GJ, Wanyenze R. Fertility desires and intentions and the relationship to consistent condom use and provider communication regarding childbearing among HIV clients in Uganda. ISRN Infect Dis. 2013;2013. doi:10.5402/2013/478192
31. A-priori sample size for structural equation models references - free statistics calculators; 2023. Available from: https://www.danielsoper.com/statcalc/references.aspx?id=89.
32. Bonett DG, Woodward JA, Randall RL. Estimating p-values for Mardia’s coefficients of multivariate skewness and kurtosis. Comput Stat. 2002;17(1):117–122. doi:10.1007/s001800200094
33. Rosseel Y. lavaan An R package for structural equation modeling. J Stat Softw. 2012;48(2):1–36. doi:10.18637/jss.v048.i02
34. Zhang J, Tian Y. Housework division and second-child fertility anxiety among couples in China: the urban and rural differences. Int J Environ Res Public Health. 2019;16(20):3910. doi:10.3390/ijerph16203910
35. Kane D, Li K. Fertility cultures and childbearing desire after the two-child policy: evidence from southwest China. J Fam Stud. 2021;29:1–19.
36. Kan MY, Hertog E. Domestic division of labour and fertility preference in China, Japan, South Korea, and Taiwan. Demogr Res. 2017;S25(18):557–588. doi:10.4054/DemRes.2017.36.18
37. Yeo TED, Chu TH. Social-cultural factors of HIV-related stigma among the Chinese general population in Hong Kong. AIDS Care. 2017;29(10):1255–1259. doi:10.1080/09540121.2017.1282601
38. Nattabi B, Li J, Thompson SC, Orach CG, Earnest J. A systematic review of factors influencing fertility desires and intentions among people living with HIV/AIDS: implications for policy and service delivery. AIDS Behav. 2009;13(5):949–968. doi:10.1007/s10461-009-9537-y
39. Hashemzadeh M, Shariati M, Mohammad Nazari A, Keramat A. Childbearing intention and its associated factors: a systematic review. Nurs Open. 2021;8(5):2354–2368. doi:10.1002/nop2.849
40. Diro CW, Afework MF. Agreement and concordance between married couples regarding family planning utilization and fertility intention in Dukem, Ethiopia. BMC Public Health. 2013;13(1):903. doi:10.1186/1471-2458-13-903
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.