Back to Journals » International Journal of General Medicine » Volume 19
Effects of High-Intensity Interval Training on Cardiopulmonary Function in Patients with Acute Myocardial Infarction with and without Cardiac Arrest: A Retrospective Study
Authors Zeng Y, Zhang Z, Wu J, Ge P, Xu J, Liu H, Geng J ![]()
Received 7 April 2026
Accepted for publication 27 May 2026
Published 10 June 2026 Volume 2026:19 610633
DOI https://doi.org/10.2147/IJGM.S610633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Yang Zeng,1,* Zequn Zhang,2,* Jiajia Wu,1,* Peibing Ge,2 Jie Xu,2 Hailang Liu,2 Jin Geng1,2
1Department of Cardiology, the Huaian Clinical College of Xuzhou Medical University, Huai’an, People’s Republic of China; 2Department of Cardiology, the Affiliated Huai’an NO.1 People’s Hospital of Nanjing Medical University, Huai’an, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jin Geng, Email [email protected] Hailang Liu, Email [email protected]
Objective: This study aims to explore the efficacy and safety of high-intensity interval training (HIIT) in patients with acute myocardial infarction (AMI) with or without cardiac arrest (CA).
Methods: A retrospective analysis of 100 patients with AMI who underwent primary percutaneous coronary intervention was conducted. Fifty patients experienced CA, whereas the other fifty did not. A HIIT program was performed three times per week for a 12-week duration. The target heart rate (THR) method was used to guide the intensity of exercise. The cardiopulmonary function indices include maximum oxygen uptake (VO2 max), anaerobic threshold (AT), ventilatory efficiency (E/CO2 slope), oxygen uptake efficiency slope (OUES), metabolic equivalents (METs), oxygen pulse (VO2/HR), and heart rate recovery at 1 minute (HRR1).
Results: After HIIT, VO2max in the CA group increased from 21.96± 4.40 to 23.85± 3.28 mL/kg/min (95% CI: 1.31 to 2.47; P < 0.001). AT increased from 15.01± 3.09 to 15.97± 2.09 mL/kg/min (95% CI: 0.41 to 1.51; P =0.001), while the VE/VCO2 slope decreased from 29.26± 3.14 to 27.56± 4.42 L/l (95% CI: − 3.01 to − 0.39; P =0.047). OUES increased from 1762.49± 653.77 to 1960.08± 527.43 (95% CI: 55.00 to 340.18; P =0.0078). METs increased from 6.27± 1.25 to 6.81± 0.93 (95% CI: 0.37 to 0.71; P < 0.001). Additionally, oxygen pulse (O2/HR) increased from 12.32± 2.08 to 13.74± 0.90 mL (95% CI: 0.87 to 1.97; P < 0.001), and HRR1 improved from 16.65± 7.75 to 20.1± 6.64 (95% CI: 0.87 to 6.03; P =0.010); similar improvements were also observed in the non-CA group. The adverse events during rehabilitation were comparable between the two groups.
Conclusion: Overall, HIIT-based rehabilitation was associated with significant improvements in cardiopulmonary function, with comparable outcomes in AMI patients with and without CA.
Keywords: high-intensity interval training, myocardial infarction, cardiac arrest, cardiac rehabilitation, exercise prescription
Introduction
Acute myocardial infarction (AMI) remains a major cause of cardiovascular morbidity and mortality worldwide despite substantial advances in reperfusion therapy and contemporary pharmacological managements.1 Cardiac arrest (CA), one of the most severe complications of AMI, is strongly associated with poor short- and long-term outcomes.2 Previous registry studies have demonstrated that patients experiencing CA during AMI exhibit significantly higher mortality and worse functional recovery even after successful primary percutaneous coronary intervention (PPCI).3 Although improvements in CA care have increased survival rates, many CA survivors continue to experience impaired cardiopulmonary function, autonomic dysfunction, reduced exercise tolerance, and decreased quality of life.4,5 Therefore, optimizing post-AMI rehabilitation strategies for this vulnerable population remains an important clinical challenge.
As a cornerstone of secondary prevention after AMI, cardiac rehabilitation (CR) has been demonstrated by multiple major clinical guidelines and reviews to effectively reduce cardiovascular mortality, recurrent ischemic events, and rehospitalization rates.6–8 Exercise-based CR also improves exercise capacity, endothelial function, ventricular remodeling, and overall functional status.9 In recent years, high-intensity interval training (HIIT) has gained increasing attention as a potentially effective alternative to traditional moderate-intensity continuous training (MICT).10,11 Several randomized controlled trials and recent meta-analyses have suggested that HIIT may produce greater improvements in peak oxygen uptake (VO2peak), exercise tolerance, and cardiopulmonary fitness compared with MICT in patients with coronary artery disease and heart failure.10–12 Furthermore, HIIT may enhance exercise engagement and adherence because of its intermittent structure and shorter training duration.
The latest evidence further underscores the importance of personalized rehabilitation strategies following myocardial infarction. A recent study demonstrated that multiple clinical factors, including age, ventricular function, cardiovascular risk burden, and baseline exercise capacity, significantly influence rehabilitation outcomes in post-myocardial infarction patients.13 These findings emphasize the need for tailored exercise prescription and careful physiological assessment during rehabilitation, particularly in higher-risk populations. Cardiopulmonary exercise testing (CPX) provides a reliable and objective method for evaluating cardiopulmonary reserve and determining safe exercise intensity, thereby playing an important role in individualized rehabilitation programs.
Despite growing evidence supporting HIIT in cardiovascular rehabilitation, data regarding its application in AMI patients complicated by CA remain limited. Compared with other AMI populations, CA survivors are less likely to receive comprehensive rehabilitation services, including supervised exercise training and structured follow-up.14 In addition, concerns regarding arrhythmia risk, hemodynamic instability, impaired myocardial reserve, and exercise safety often limit the implementation of higher-intensity exercise protocols in this subgroup. Consequently, evidence regarding the feasibility and safety of HIIT in CA survivors remains insufficient, and comparative studies evaluating cardiopulmonary recovery between AMI patients with and without CA are scarce.
Importantly, most previous studies have focused on general AMI or heart failure populations, while CPX-based assessments of HIIT outcomes specifically in CA survivors remain poorly characterized. Therefore, the present retrospective study aimed to evaluate the efficacy and safety of HIIT-based cardiac rehabilitation on cardiopulmonary function in AMI patients with and without CA using CPX-derived parameters. By comparing the functional recovery between the two groups, this study aims to further elucidate the feasibility and potential clinical value of HIIT in high-risk AMI patients complicated with CA.
Materials and Methods
Participants and Group Assignment
This retrospective study collected data from 50 AMI patients who experienced CA before admission and were successfully resuscitated before receiving PPCI treatment from January 1, 2020, to January 1, 2024. All participants underwent cardiopulmonary exercise testing (CPX) one week after discharge, followed by a 12-week HIIT program. AMI patients who received PPCI treatment without experiencing CA were 1:1 matched and were classified as the non-CA group. Ventricular fibrillation, pulseless electrical activity, or asystole were defined as cardiac arrest. The inclusion criteria for this study were as follows: 1) All patients fulfilled the diagnostic criteria for AMI and have been confirmed by coronary angiography; 2) PPCI has been performed on the culprit vessels, and elective PCI has been conducted on the non-culprit vessels; 3) Individuals capable of independent living (with a score of 100 on the Activities of Daily Living Assessment) are eligible for exercise rehabilitation. The exclusion criteria for this study were as follows: 1) Residual stenosis ≥50% in the left main coronary artery after PCI; 2) Chronic heart failure with left ventricular ejection fraction (LVEF) ≤45%; 3) History of cardiac surgery; (4) Musculoskeletal or neurological disorders; (5) Permanent atrial fibrillation; (6) Other comorbidities that may interfere with participation in or safety of rehabilitation training.
This study was approved by the Ethics Committee of Huai’an First People’s Hospital, and all enrolled patients signed informed consent forms. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Intervention
All patients were treated with regular CAD secondary prevention medication, disease-related knowledge dissemination, rational nutrition and diet, correction of unhealthy lifestyle habits, and treatment of underlying diseases. A cardiopulmonary exercise test will be performed during the follow-up visit one week after discharge.
Cardiopulmonary Exercise Testing
Before cardiopulmonary exercise testing (CPX), all participants provided written informed consent. CPX was performed using a German Jaeger cardiopulmonary exercise testing system with continuous electrocardiographic and blood pressure monitoring throughout the procedure. A symptom-limited incremental exercise protocol was conducted on an electronically braked cycle ergometer.
The testing protocol consisted of a 3-minute resting phase, followed by a 3-minute unloaded warm-up period. Exercise intensity was subsequently increased by 10–25 W/min according to the patient’s exercise tolerance and predicted functional capacity, with the goal of achieving peak exercise within approximately 6–12 minutes. A 5-minute recovery phase was performed after peak exercise.
Respiratory gas exchange variables were collected breath-by-breath and averaged every 10 seconds for analysis. Before each test, the gas analyzers and flow sensors were calibrated according to the manufacturer’s recommendations using standard reference gases and volume calibration procedures to ensure measurement accuracy and reproducibility.
The exercise test was terminated according to the standard symptom-limited cardiopulmonary exercise testing termination criteria and institutional safety protocols. Indications for test termination included: (1) achieving target submaximal heart rate; (2) significant ischemic ECG changes; (3) excessive blood pressure elevation during exercise (systolic BP >210 mmHg in males or >190 mmHg in females); (4) clinically significant arrhythmias including frequent ventricular premature contractions, nonsustained ventricular tachycardia, or uncontrolled atrial fibrillation; (5) severe dizziness, profuse sweating, presyncope, lower extremity weakness or pain; (6) pulse oximetry desaturation exceeding 5%; (7) severe dyspnea, chest tightness, chest discomfort, or patient request to stop due to intolerable symptoms.
Determination of Exercise Intensity
According to CPX data, exercise intensity is determined by heart rate reserve. The target heart rate for high-intensity exercise is calculated as (maximum heart rate - resting heart rate) * (80%-90%) + resting heart rate, while for moderate-to-low intensity exercise, it is (maximum heart rate - resting heart rate) * (40%-50%) + resting heart rate. Considering the relatively limited tolerance and adherence of some Chinese cardiac patients to conventional long-interval HIIT protocols, a short-duration HIIT model was adopted in the present study to improve feasibility and compliance.15 Each session consists of 8 sets of 2-minute high-intensity exercise intervals, interspersed with 7 sets of 2-minute low-to-moderate intensity recovery periods. This training program lasts for 12 weeks.
Implementation of the Exercise Program
The exercise program was conducted under ECG monitoring at our hospital’s CR center. The first step involved a 5 to 10-minute warm-up on a stationary bike with no resistance. This was followed by a 30-minute HIIT session on the bike. The final step was a cool-down exercise, the duration of which was at the patient’s discretion and not included in the total exercise program time.
Exercise Safety and Symptom Monitoring
If chest pain, dizziness, significant shortness of breath, nausea and vomiting, lower limb cramps, severe fatigue, or abnormal blood pressure changes (a decrease in systolic blood pressure ≥10 mmHg or an increase ≥50 mmHg), significant ventricular or atrial arrhythmias, occurrence of second- or third-degree atrioventricular block, or significant ischemic ECG changes occur during exercise, the exercises were immediately stopped. If necessary, administer isosorbide dinitrate sublingually and provide oxygen therapy. Record the heart rate at the onset of symptoms, and aim for a target heart rate of 15 beats per minute below the symptomatic heart rate for the next session. If the patient can tolerate it, gradually increase the target heart rate again.
Definition of Certain Adverse Events During the Rehabilitation Period
New-onset atrial fibrillation: atrial fibrillation occurring during the rehabilitation period in patients with no prior history of atrial fibrillation, lasting less than 1 day, and capable of converting to sinus rhythm.
Frequent ventricular premature beats or non-sustained ventricular tachycardia: frequent ventricular premature beats are defined as more than 3 ventricular premature beats per minute observed during monitoring in the rehabilitation period.
Non-sustained ventricular tachycardia is defined as 3 consecutive ventricular premature beats lasting less than 30 seconds during monitoring in the rehabilitation period, with hemodynamic stability, requiring medication adjustment but no ICD implantation.
Exercise-related injuries: knee and ligament injuries, falls from treadmills, and other falls.
Acute heart failure episodes: heart failure episodes occurring during rehabilitation exercises that affect subsequent rehabilitation or require hospitalization.
Atrioventricular block: second-degree or higher atrioventricular block occurring during rehabilitation exercises.
Ventricular aneurysm: Post-recovery cardiac ultrasound revealed the formation of a ventricular aneurysm.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD). Normality was assessed using the Shapiro–Wilk test. In this study, all continuous variables were normally distributed. Comparisons between groups were performed using the independent samples t-test, while within-group comparisons before and after rehabilitation were analyzed using the paired t-test. Categorical variables were presented as frequencies and percentages, and comparisons were made using the chi-square test. Due to the retrospective nature of the study, no a priori sample size calculation was performed. There were no missing data in the final analysis.
Results
Baseline Characteristics
We first collected baseline data and medication regimens from both the CA group and the non-CA group. Statistically significant differences were observed in age and NT-proBNP levels (P<0.001 and P=0.003). There were no difference of the remaining data between the two groups (Table 1).
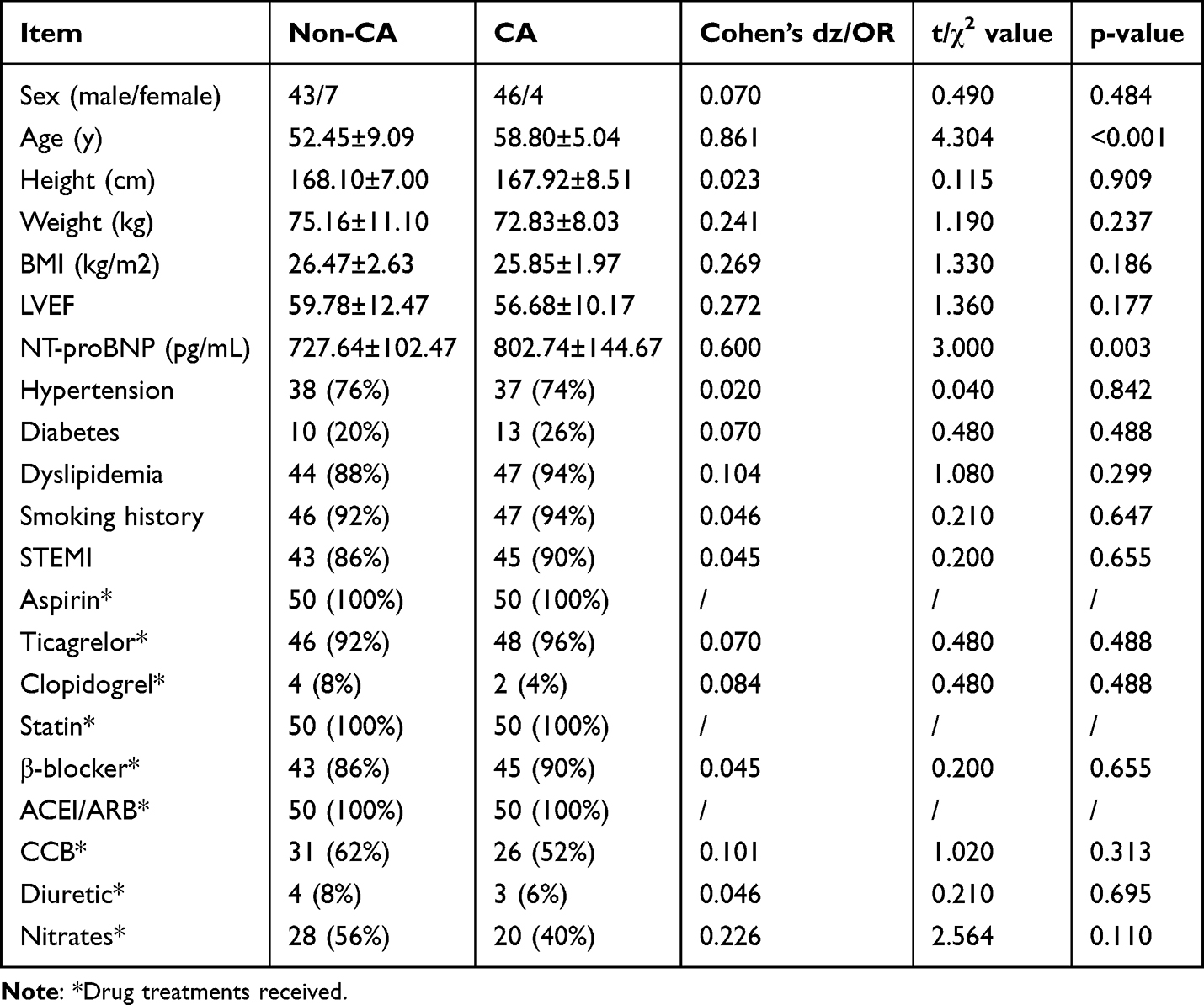 |
Table 1 General Clinical Data Comparison |
Cardiopulmonary Function Before Rehabilitation
Before rehabilitation, there were no statistically significant differences in VO2max, AT, VE/VCO2 slope, OUES, METs, O2/HR, and HRR1 between the CA group and the non-CA group (P > 0.05, Table 2). This may be related to the timeliness of cardiopulmonary resuscitation and the subsequent systematic comprehensive treatment.
 |
Table 2 Baseline Cardiopulmonary Function Parameters |
Cardiopulmonary Function After Rehabilitation
After a 12-week HIIT program, VO2max in the CA group increased from 21.96±4.40 to 23.85±3.28 mL/kg/min (95% CI: 1.31 to 2.47; P<0.001; dz = 0.92). AT increased from 15.01±3.09 to 15.97±2.09 mL/kg/min (95% CI: 0.41 to 1.51; P =0.001; dz = 0.49), while the VE/VCO2 slope decreased from 29.26±3.14 to 27.56±4.42 L/l (95% CI: −3.01 to −0.39; P=0.047; dz = 0.42). OUES increased from 1762.49±653.77 to 1960.08±527.43 (95% CI: 55.00 to 340.18; P=0.0078; dz = 0.39). METs increased from 6.27±1.25 to 6.81±0.93 (95% CI: 0.37 to 0.71; P <0.001; dz = 0.92). Additionally, oxygen pulse (O2/HR) increased from 12.32±2.08 to 13.74±0.90 mL (95% CI: 0.87 to 1.97; P <0.001; dz = 0.73), and HRR1 improved from 16.65±7.75 to 20.1±6.64 (95% CI: 0.87 to 6.03; P =0.010; dz = 0.38) (Table 3; Figure 1A–G); similar improvements were also observed in the non-CA group (Table 4; Figure 1A–G). This demonstrates the powerful improvement effect of HIIT on the cardiopulmonary function in AMI population. Subsequently, we compared the VO2max, AT, VE/VCO2 slope, OUES, METs, O2/HR, and HRR1 between the non-CA group and the CA group after 12 weeks of HIIT, and no differences were observed. (P > 0.05) (Table 5).
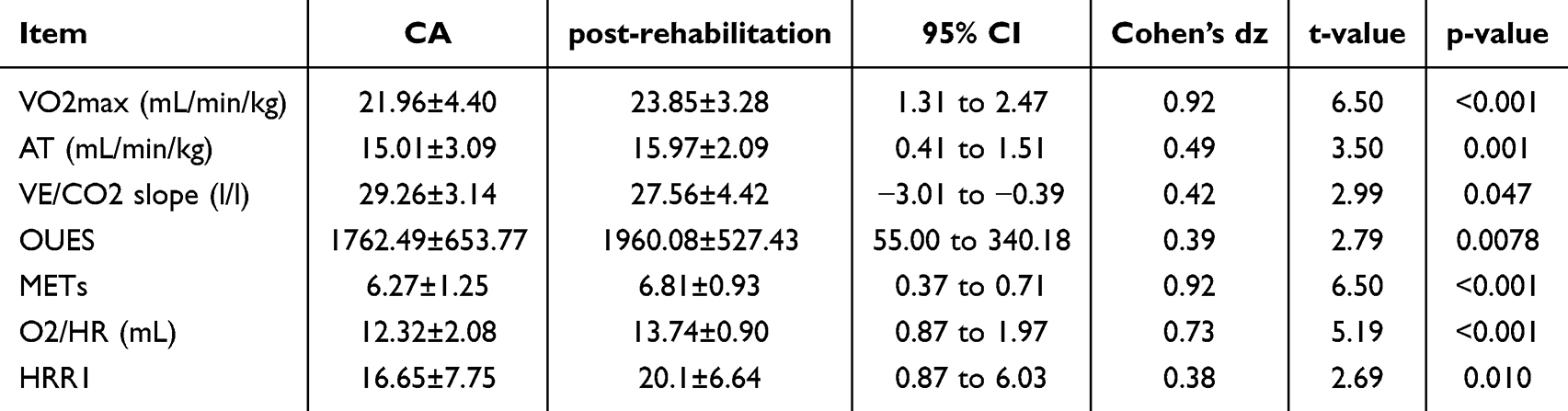 |
Table 3 Cardiopulmonary Function Before and After HIIT in the CA Group |
 |
Table 4 Cardiopulmonary Function Before and After HIIT in the Non-CA Group |
 |
Table 5 Post-Rehabilitation Comparison Between Groups |
 |
Figure 1 Changes in cardiopulmonary function parameters before and after cardiac rehabilitation in the CA and non-CA groups. (A) Changes in VO2max before and after cardiac rehabilitation in the CA group and non-CA group. (B) Changes in AT before and after cardiac rehabilitation in the CA group and non-CA group. (C) Changes in VE/VCO2 slope before and after cardiac rehabilitation in the CA group and non-CA group. (D) Changes in OUES before and after cardiac rehabilitation in the CA group and non-CA group. (E) Changes in METs before and after cardiac rehabilitation in the CA group and non-CA group. (F) Changes in heart oxygen pulse before and after cardiac rehabilitation in the CA group and non-CA group. (G) Changes in HRR1 before and after cardiac rehabilitation in the CA group and non-CA group. *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001, ****P ≤ 0.0001. |
Adverse Events During Rehabilitation
During the rehabilitation training period, there were 2 cases of new-onset atrial fibrillation and 2 cases of frequent ventricular premature beats or non-sustained ventricular tachycardia in the non-CA group. In the CA group, there were 3 cases of new-onset atrial fibrillation and 4 cases of frequent ventricular premature beats or non-sustained ventricular tachycardia. Neither group experienced adverse events such as ventricular tachycardia or fibrillation, sudden death, exercise-related injuries, acute heart failure episodes, bradycardia, ventricular aneurysm formation, or atrioventricular block. (Table 6).
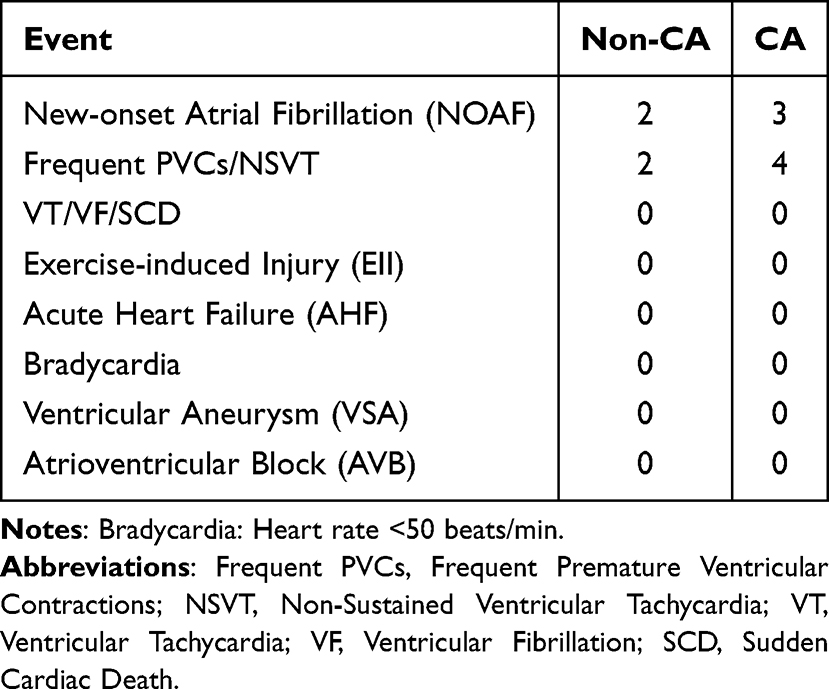 |
Table 6 Adverse Events During Rehabilitation |
Discussion
This study expands the existing evidence on exercise-based cardiac rehabilitation by evaluating the efficacy and safety of HIIT in patients with AMI complicated by CA. Cardiac rehabilitation in this population is under-represented in clinical research. Previous studies have demonstrated that exercise-based cardiac rehabilitation following PCI helps improve outcomes in AMI patients. A meta-analysis revealed that multiple exercise modalities can enhance patients’ cardiopulmonary function, with combined exercise intervention programs showing the most significant benefits.16 Additionally, it was reported that traditional exercise interventions such as Baduanjin and moderate-intensity walking can improve exercise capacity and psychological status in AMI patients.17 These findings collectively demonstrate the importance of cardiac rehabilitation for CA survivors in AMI. In this study, we compared cardiopulmonary function parameters before and after the implementation of a HIIT-based rehabilitation program in patients, including VO2max, VE/VCO2 slope, AT, OUES, METs, oxygen pulse, and HRR1. Following rehabilitation treatment, both the CA group and non-CA group showed significant improvements. These findings suggest that AMI patients with comorbid CA can achieve functional recovery comparable to those without CA when participating in a structured CPX-guided HIIT training program. However, this should be interpreted as an absence of observed differences rather than evidence of equivalence. Although baseline cardiopulmonary function, such as oxygen pulse, appeared relatively lower in the CA group, this may reflect more severe myocardial injury, as supported by higher NT-proBNP levels in this subgroup. Additionally, the CA group was older than the non-CA group, which may also contribute to the observed baseline differences. These findings are consistent with previous evidence indicating that CA is associated with greater myocardial damage and impaired functional capacity after AMI. The potential mechanisms underlying the benefits of HIIT remain incompletely understood. Experimental and clinical studies suggest that exercise training may improve cardiovascular function through modulation of endothelial function, attenuation of adverse ventricular remodeling, and regulation of neurohormonal activation, including the endothelin-1 and renin–angiotensin–aldosterone systems.18 In terms of safety, no major adverse cardiovascular events, sustained arrhythmias, or fatal incidents were observed during the rehabilitation period. Although a small number of transient arrhythmic events occurred in both groups, the overall incidence was low, suggesting that CPX-guided high-intensity interval training may be feasible for selected acute myocardial infarction patients (including those with prior CA treatment) under supervised conditions. However, given the retrospective study design and limited sample size, these findings should be considered preliminary. Compared with the previous study by Kim et al19 this research incorporated more comprehensive cardiopulmonary exercise parameters, a relatively larger sample size for this subgroup, and a structured 12-week rehabilitation program. In summary, our findings provide preliminary evidence supporting the feasibility and functional benefits of HIIT-based rehabilitation programs for AMI patients with and without CA, while highlighting the need to validate these observations through prospective controlled trials.
Limitations
This study has several limitations that need to be addressed. Due to the retrospective, single-center, observational design, causal inference regarding the effects of HIIT cannot be established, and there may be potential selection bias without randomization. Given the retrospective and non-randomized design, adjustments for potential confounding variables were not made. Therefore, the observed associations should be interpreted with caution, as they may be influenced by confounders, including gender differences. Second, the lack of MICT or non-exercise control group limits the ability to directly compare the effects of different rehabilitation strategies. Third, although this study included a clinically significant subgroup of patients with AMI complicated by CA, the sample size remains relatively small, which may limit statistical power and the generalizability of the findings. Furthermore, although this subgroup has been underrepresented in previous HIIT-based cardiac rehabilitation studies and belongs to a clinically high-risk population, the novelty of this study primarily lies in its progressive innovation, focusing mainly on feasibility and preliminary functional outcomes rather than confirmatory efficacy comparisons. Lastly, while CPX was used to guide exercise prescription and assess outcomes, long-term clinical endpoints such as mortality and rehospitalization rates were not evaluated. Therefore, further large-scale prospective randomized controlled trials are needed to validate these findings and determine the long-term clinical benefits of HIIT in this high-risk population.
Conclusions
In conclusion, this study suggests that supervised HIIT can improve cardiorespiratory fitness and exercise capacity in patients with AMI, including those with concurrent CA. Although no significant difference was observed between CA and non-CA patients, the findings indicate that HIIT under appropriate medical supervision may be feasible and potentially beneficial in this high-risk subgroup. However, given the retrospective single-center design, limited sample size, and lack of a control group, the results should be interpreted with caution. Large-scale prospective randomized controlled trials are needed in the future to confirm the safety, efficacy, and long-term clinical benefits of HIIT in AMI patients complicated by CA.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Sharing Statement
The raw data supporting the conclusions of this article will be available from Yang Zeng upon reasonable request. Email: [email protected].
Acknowledgments
The author thanks Cardiology Ward 1 and the Cardiac Rehabilitation Center of Huai’an First People’s Hospital for providing rehabilitation venue support.
Funding
This research was funded by Huai’an Key Laboratory of Cardiovascular and Cerebrovascular Diseases (HAP202202), Jiangsu Province Health Commission Scientific Research Project (H2023086), Huai’an municipal Science and Technology Program Project (HAB202307),Chinese Cardiovascular Association-Natural lipid-lowering drugs fund (2023-CCA-NLD-055), Northern Jiangsu Clinical Medicine Research Institute's 2024 Key Cultivation Projects, (HAKY202400407) and The APC was funded by Postgraduate Research Fund of Xuzhou Medical University. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vallabhajosyula S, Verghese D, Henry TD, et al. Contemporary management of concomitant cardiac arrest and cardiogenic shock complicating myocardial infarction. Mayo Clin Proc. 2022;97(12):2333–10. doi:10.1016/j.mayocp.2022.06.027
2. Jortveit J, Andersen GØ, Halvorsen S. Short- and long-term outcomes of patients with acute myocardial infarction complicated by cardiac arrest: a nationwide cohort study 2013–22. Euro Heart J. 2024;13(12):828–837. doi:10.1093/ehjacc/zuae121
3. Ando H, Sawano M, Kohsaka S, et al. Cardiac arrest and post-discharge mortality in patients with myocardial infarction: a large-scale nationwide registry analysis. Resuscitation Plus. 2024;18:100647. doi:10.1016/j.resplu.2024.100647
4. Amacher SA, Sahmer C, Becker C, et al. Post-intensive care syndrome and health-related quality of life in long-term survivors of cardiac arrest: a prospective cohort study. Sci Rep. 2024;14(1):10533. doi:10.1038/s41598-024-61146-8
5. Pek PP, Fang K, Lim SL, et al. Physical, psychological, cognitive, social health outcomes, and health-related quality of life in out-of-hospital cardiac arrest survivors and co-survivors: 3-month outcomes from the Quality Cardiac Arrest Survivorship cohort study (QualiCAS). Resusci Plus. 2026;27:101179. doi:10.1016/j.resplu.2025.101179
6. Zhang S, Lin Y. Advancements, challenges, and innovative strategies in cardiac rehabilitation for patients with acute myocardial infarction: a systematic review. Curr Problems Cardiol. 2025;50(2):102934. doi:10.1016/j.cpcardiol.2024.102934
7. Visseren FLJ, Mach F, Smulders YM, et al. ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
8. Dibben GO, Faulkner J, Oldridge N, et al. Exercise-based cardiac rehabilitation for coronary heart disease: a meta-analysis. Eur Heart J. 2023;44(6):452–469. doi:10.1093/eurheartj/ehac747
9. Gao J, Li L, Zhai S, et al. Exercise training for myocardial ischemia reperfusion injury: mechanism and clinical practice (Review). Int J Mol Med. 2025;56(5):1–12. doi:10.3892/ijmm.2025.5632
10. Gao C, Yue Y, Wu D, Zhang J, Zhu S, Coquart JB. Effects of high-intensity interval training versus moderate-intensity continuous training on cardiorespiratory and exercise capacity in patients with coronary artery disease: a systematic review and meta-analysis. PLoS One. 2025;20(2):e0314134. doi:10.1371/journal.pone.0314134
11. Gomes-Neto M, Durães AR, Conceição LSR, Silva CM, Martinez BP, Carvalho VO. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and health-related quality of life in patients with coronary artery disease: an updated systematic review and meta-analysis. Braz J Phys Ther. 2025;29(1):101137. doi:10.1016/j.bjpt.2024.101137
12. Albustami M, Hartfiel N, Charles JM, et al. Cost-effectiveness of High-Intensity Interval Training (HIIT) vs Moderate Intensity Steady-State (MISS) Training in UK cardiac rehabilitation. Arch Phys Med Rehabil. 2024;105(4):639–646. doi:10.1016/j.apmr.2023.09.005
13. Bryndal A, Glowinski S, Grochulska A. Influence of risk factors on exercise tolerance in patients after myocardial infarction—early cardiac rehabilitation in poland. J Clin Med. 2022;11(19):5597. doi:10.3390/jcm11195597
14. Sawyer KN, Camp-Rogers TR, Kotini-Shah P, et al. Sudden cardiac arrest survivorship: a scientific statement from the American heart association. Circulation. 2020;141(12):e654–e685. doi:10.1161/cir.0000000000000747
15. Chinese Medical Association, Editorial Board of Chinese Journal of Cardiology. Expert consensus on exercise rehabilitation in outpatient of cardiovascular disease. Zhonghua Xin Xue Guan Bing Za Zhi. 2025;53(10):1099–1111. doi:10.3760/cma.j.cn112148-20241011-00600
16. Álvarez-Martínez P, Alonso-Calvete A, Justo-Cousiño LA, González-González Y. Efficacy of the different therapeutic exercise modalities in cardiac rehabilitation after myocardial infarction. A review of the literature. Anales del Sistema Sanitario de Navarra. 2022;45(3). doi:10.23938/assn.1021
17. Kang L, Li Y, Chen K, et al. Effect of Baduanjin exercise on acute myocardial infarction in patients with anxiety and depression after percutaneous coronary intervention: a randomized controlled trial. Medicine. 2024;103(45):e40225. doi:10.1097/md.0000000000040225
18. Wang B, Zhou R, Wang Y, et al. Effect of high-intensity interval training on cardiac structure and function in rats with acute myocardial infarct. Biomed Pharmacother. 2020;131:110690. doi:10.1016/j.biopha.2020.110690
19. Kim C, Jung H, Choi HE, Kang SH. Cardiac rehabilitation after acute myocardial infarction resuscitated from cardiac arrest. Ann Rehabil Med. 2014;38(6):799–804. doi:10.5535/arm.2014.38.6.799
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of the COVID-19 Pandemic on Emergency Department Visits of Patients with an Emergent or Urgent Diagnosis
Yeh CC, Chien CY, Lee TY, Liu CH
International Journal of General Medicine 2022, 15:4657-4664
Published Date: 4 May 2022
Post-Myocardial Infarction Rehabilitation: The Absence in the Rehabilitation Process of the Diaphragm Muscle
Bordoni B, Mapelli L, Toccafondi A, Di Salvo F, Cannadoro G, Gonella M, Escher AR, Morici N
International Journal of General Medicine 2024, 17:3201-3210
Published Date: 22 July 2024
Factors Influencing Cardiac Rehabilitation Compliance in Elderly Myocardial Infarction Patients and the Development of a Nomogram Prediction Model
Zhou B, Yan J, Wang Q, He Q, Ao W, Yang Y, Ren Y
Patient Preference and Adherence 2025, 19:2015-2025
Published Date: 11 July 2025