Back to Journals » Journal of Pain Research » Volume 16
Effects of False Feedback on Pain Tolerability Among Young Healthy Adults: Predictive Roles of Intentional Effort Investment and Perceived Pain Intensity
Authors Chen S, Jackson T, He Y
Received 17 March 2023
Accepted for publication 13 June 2023
Published 4 July 2023 Volume 2023:16 Pages 2257—2268
DOI https://doi.org/10.2147/JPR.S412994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Shuanghong Chen,1,2 Todd Jackson,3 Ying He1
1Xinqiao Hospital and the Second Affiliated Hospital, Army Medical University, Chongqing, People’s Republic of China; 2Faculty of Psychology, Southwest University, Chongqing, People’s Republic of China; 3Department of Psychology, University of Macau, Taipa, Macau, People’s Republic of China
Correspondence: Ying He, Xinqiao Hospital and the Second Affiliated Hospital, Army Medical University, Chongqing, 400715, People’s Republic of China, Email [email protected]
Purpose: Expectations and modification gained through critical learning influence pain perception. We tested how pain tolerability was influenced by the effects of orally delivered false feedback and participant status immediately prior to performing tasks.
Patients and Methods: A total of 125 healthy college students (69 females and 56 males) were randomly assigned to 3 groups (positive, negative, and control) to participate in two formal cold pressor tests (CPTs). Participants completed the same series of task-related questionnaires (perceived importance, intended effort, current affect, and self-efficacy) before each CPT. False performance feedback was delivered after completion of the baseline level CPT. After completion of each CPT, both pain intensity and pain tolerability (duration in ice water) were recorded.
Results: The results of linear mixed models revealed significant condition × time interactions on pain tolerability and task self-efficacy after controlling for individual variance as a random effect. Participants who received negative feedback exhibited increased pain tolerability without decreasing their self-efficacy, whereas participants who received positive feedback showed increased self-efficacy with no change in pain tolerability. A longer pain tolerance duration was also predicted by a more intentional investment of effort and a lower intensity of experienced pain as well as the effect of false feedback.
Conclusion: The research highlights the effect of powerful situational influences on laboratory-induced pain tolerance.
Keywords: cold pressor test, pain, false feedback, effort, self-efficacy, social norms
Introduction
Human beings, as social animals, tend to evaluate their own attitudes, intentions, abilities or behaviors with others (eg, social models) to gain self-knowledge and discover their individual realities in ambiguous circumstances.1 Individuals are expected to act in accordance with social norms (eg, in accordance with how a social model is performed), especially when behaviors are viewed positively in a given culture and context.2,3 Norms are cultural phenomena that prescribe and forbid behavior under specific circumstances.4 Despite their regulatory role, the attention given to social norms varied notably across a series of social and psychological experiments. Classic social modeling experiments that apply pain-tolerance/intolerance models using noxious stimuli found that people are more pain tolerant, report less pain, and show reduced physiological arousal following exposure to pain-tolerant role models.5,6 Thereafter, rather than having patients observe role models, a laboratory-induced cold pressor test (CPT) experiment found that participants reported less pain following exposure to a hand-written list of the bogus low pain ratings of confederates.7 More recently, studies have found that participants exhibit a greater level of pain tolerability in CPT tasks after exposure to verbal presentations offering positive reviews of social norms or to those offered through computer-delivered messages.8,9 However, they ignore the potential influence of baseline pain tolerance duration.
The abovementioned experimental studies directly present the means by which a social model is performed (ie, positive behavior truly being encouraged through social feedback); the situation that arises in pain studies as a result of fictitious performance feedback is less studied.10–12 Initially, participants were engaged in CPT trials and received fake feedback (either very good or not) on former CPT trials sequentially, resulting in the finding that positive feedback causes better pain tolerability and negative feedback causes worse pain tolerability.10 Researchers have incorporated peer pressure into fake feedback, making the self-evaluation process more complex.11,12 Specifically, participants who were engaged in a task where they had to tolerate painful stimulation were then provided with fake feedback comparing their level of pain tolerance with that of peers who had completed the same task.11,12 Participants receiving low-tolerance feedback or high-tolerance feedback improved their pain tolerance duration more than participants receiving average-tolerance feedback (control condition).11 More recently, the study investigated the effects of false performance feedback on the basic components of cognitive control.12 They found that participants who had received low-tolerance feedback performed poorly at inhibiting their response in a speeded go/no-go task compared to those who had received high-tolerance feedback.12
Negative feedback from inner experience in a dysfunctional self-schema leads to affect-biased attention at both the sensory-perceptual and cognitive levels, which results in depressive symptoms.13 The maintenance of self-esteem and/or self-efficacy is an essential element in treating psychopathology and other physical illnesses, such as clinical pain conditions.14 Patients with pain conditions exhibited a stronger implicit self-illness association and higher levels of self-pity than those in the healthy control.15 Individuals’ beliefs concerning their capacity for pain management could be challenged by false feedback on task performance.10,12 However, no consistent findings were observed regarding the ways in which self-efficacy influences task performance.10,16 An increased level of self-efficacy and increased tolerability was observed, which was consistent with traditional self-efficacy theory.10 Related evidence of negative associations between self-efficacy and task performance was also supported through an analytic game study, in which high levels of self-efficacy led to overconfidence and increased the likelihood of committing logic errors during the game.16
Except for task-related self-efficacy, Bandura’s contention is that verbal persuasion and building awareness of physiological and affective states both before and after enacting desired activities are alternative means of influencing task performance.17 In addition, the importance of doing well in a given task and the level of intended investment effort are common psychological factors that need to be assessed in such tasks.9,18 A motivational perspective built around the organizing powers of goal setting and self-regulatory processes has been adopted to account for the escape behavior aimed at avoiding pain experiences and (re)injury.19–21 The motivational perspective may provide further insights into the processes of automatically raised avoidance behaviors in situations that arise from goal competition. Accumulating evidence supports the motivational view of pain with competing goals in laboratory-induced pain settings. For example, the formation of conscious intentions reduces escape-avoidance behavior during tasks that incorporate painful stimuli and fosters no-pain goal pursuit, turning pain into cues for goal-directed behavior.22 In summary, it is not clear how task-related status would be influenced by fake feedback or how it influences pain tolerability.
Social norms often arise spontaneously rather than being deliberately planned, and they are nested in cultural backgrounds. For example, modesty is a typical norm in China. Chinese individuals are expected to manifest low levels of explicit self-esteem while manifesting high levels of implicit self-esteem, whereas American participants linked modesty to explicit self-esteem but perceived no associations between modesty and implicit self-esteem.23 However, the way that social comparison information affects task performance as well as the self-evaluation process in laboratory settings is less addressed in the Chinese context.
In the present study, we assessed the effects of false feedback on first task performance (pain tolerance levels compared to peers who had completed the same task) on the upcoming performance of the second task via the CPT among Chinese university participants. We also measured task-related status (ie, self-efficacy, perceived task importance, intended effort, state affect) both before and after provisioning false feedback. To help clarify, Table 1 shows the definition of each essential outcome measured in the present study. We hypothesized that (1) participants in the positive or negative condition (ie, more or less tolerant than others) could maintain longer pain tolerance duration in ice water than those in the control (ie, average tolerance compared to others) and (2) those group differences remain after controlling for task-related measures that are significant predictors of pain tolerability.
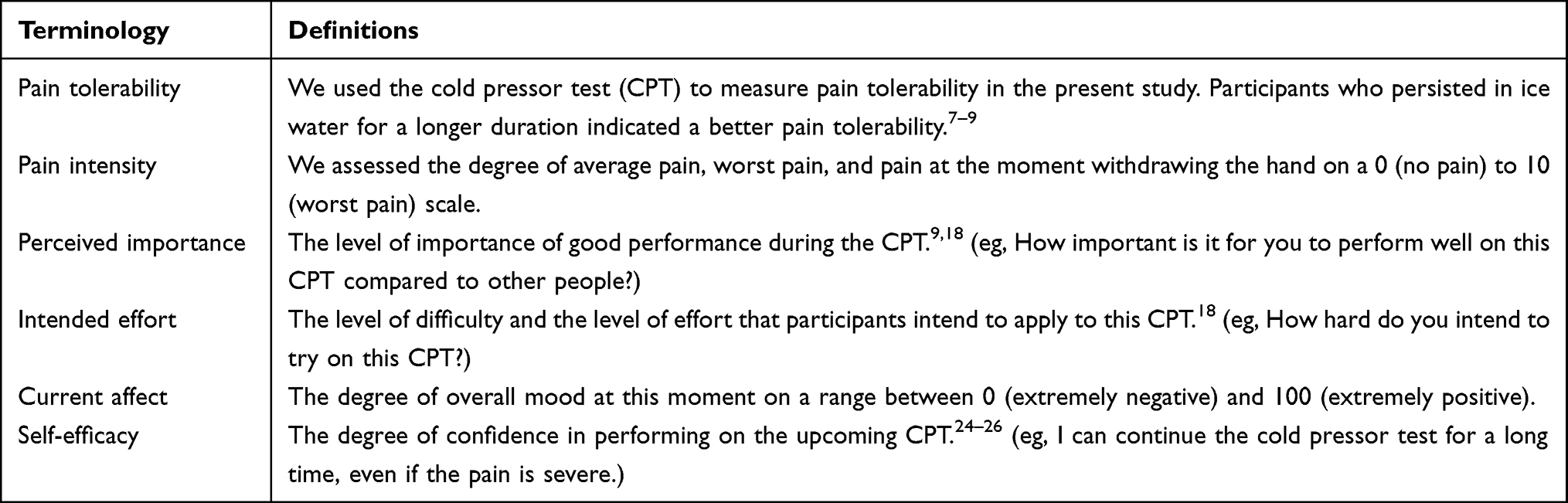 |
Table 1 Definitions Table |
Methods
Participants
The final sample comprised 125 young adults (69 women, 56 men) from Southwest University, China. Participants were 18 to 25 years of age (M = 19.61 years, SD = 1.56 years), typically in their first or second year of study (68.0%), and predominantly of Han ethnicity (83.2%), with others identifying as one of 10 ethnic minorities. The sample had an average body mass index (BMI) of 20.68 (SD = 2.76, range: 15.24 to 30.67). Four participants (1 female in the negative feedback condition, 2 females in the positive feedback condition, and 1 male in the positive feedback condition) chose the wrong manipulation check item, so their data were excluded from the analyses.
Apparatus
A cold water bath unit (Model DX-208), 25 cm wide, 25 cm long, 20 cm deep and filled with 12.5 L of circulating water was used to induce pain. A thermostat-controlled electric pump maintained the water temperature (± 0.1 degrees) via heat exchange. Previous studies have demonstrated that a cold water bath is safe and useful to assess cold pressor pain tolerance duration with water temperature ranges from 0 to 5 degree Celsius.27,28 For this experiment, the water temperature was maintained at 3 degree Celsius.
Procedure
The study was approved by the Institutional Review Board of Faculty of Psychology, Southwest University (H19015). This study complies with the Declaration of Helsinki. On the campus of Southwest University, potential volunteers were recruited via internet-based advertisements soliciting volunteers for a laboratory experiment on the factors influencing cold water pain. Interested participants were asked to complete a checklist of exclusion criteria. Please refer to the Supplementary Material for a detailed description. Appointments were made with those who remained interested, were available and claimed none of the exclusion criteria. The main procedure is depicted in Figure 1.
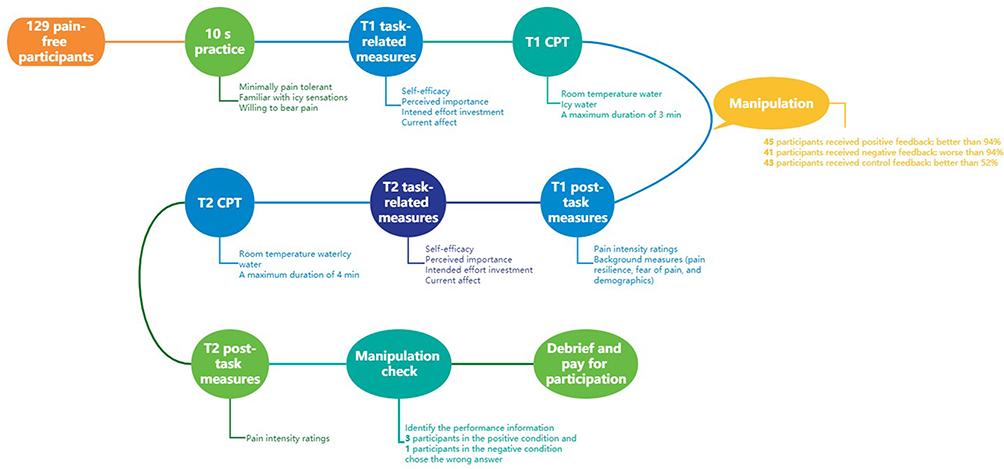 |
Figure 1 Study procedure. Abbreviation: CPT, cold pressor test. Notes: A total of 125 healthy college students were randomly assigned to 3 groups (positive, negative, and control) to participate in two formal CPTs. False performance feedback was delivered after completion of the baseline level CPT. Participants completed a series of task-related and post-task questionnaires before and after each CPT, respectively. |
After arriving at their scheduled appointments, participants read and signed a written informed consent form that reiterated the general research purpose and described the main research tasks of the study (via completion of self-report questionnaires and CPTs), the time involved (approximately 30–40 minutes), and the compensation (20 Chinese yuan). Participants then completed the exclusion criteria checklist a second time. The Supplementary Material shows the exclusion criteria checklist and all the questionnaires used in the present study with both Chinese and English versions. Then, a standardized 10-s premanipulation practice CPT was undertaken to ensure that all participants (1) were minimally pain tolerant, (2) had passing familiarity with task-related sensations prior to potentially prolonged exposure, and (3) were willing to bear pain related to an actual CPT. Specifically, the experimenter asked participants to immerse their nonwriting hands in a container of room temperature water for approximately 30 seconds to ensure that their hand temperature was the same as that of other participants. Next, participants were told to keep the same hand in the cold water for 10s after being told that nearly everyone had been able to do so in past experiments. Indeed, all participants in this study successfully completed the practice CPT.
Following this task, participants completed T1 task-related measures regarding levels of self-efficacy, importance and intended effort in the upcoming CPT and in a general current affect item. Subsequently, they completed the T1 CPT as a baseline. After immersing their non-writing hand in a container of room temperature water to ensure that hand temperatures were similar across participants just prior to the initial immersion, participants were instructed to leave their hand in the cold water for as long as possible but to remove it whenever they wanted, particularly if sensations became too uncomfortable. Participants were instructed to face forward during the task, perform any mental activities they wanted to cope with their hand being immersed in cold water, and to not talk to the experimenter, who was busy recording their times. The timer was stopped either when the hand was withdrawn or following 3 minutes of immersion.
Immediately after completing the T1 CPT, participants provided pain intensity ratings. The experimenter noted how well they performed on the CPT compared to the other participants who had completed this task and were willing to provide feedback. Specifically, participants who had been randomly assigned to a positive performance feedback condition were given false feedback indicating that they had lasted longer than 94% of participants who completed the CPT and showed a noticeably better-than-average ability to withstand pain compared to that of others. Conversely, those randomly assigned to the negative performance feedback condition were given false feedback indicating that they had lasted for less time than 94% of participants who completed the task and showed a noticeably worse than average ability to withstand pain compared to that of others. Finally, participants who had been randomly assigned to the control group were given false feedback indicating that they had lasted for more time than just over 52% of participants who completed the task and showed an average ability to withstand pain compared to that of others.
During this period, participants were instructed to rest and to complete the T1 post-task measures, which included assessments of pain resilience, pain-related fear, and demographics.
Next, T2 task-related measures with items identical to T1 measures were re-administered. Then, participants engaged in the T2 CPT following instructions and parameters from the T1 CPT. The timer was stopped either when the hand was withdrawn or after 4 minutes of immersion. Immediately after the T2 CPT, participants completed T2 post-task measures (ie, pain intensity ratings). Participants were also asked to guess the specific research hypothesis. Then, a manipulation check item comprising the correct answer and two “false distractors” was given, and participants were required to correctly identify the performance information they were given regarding the first CPT by the experimenter. Participants who chose the wrong answer indicated the manipulation failed and the data of these participants were excluded from analysis. Finally, they were debriefed on the main research focus and paid for their participation.
Measures
Pain Resilience Scale (PRS)
The 14-item PRS assesses an individual’s specific capacity to successfully manage or adapt to pain.29 Items are rated on a scale ranging between 0 (never) and 4 (all the time), with a higher total score indicating a higher level of pain resilience. The original PRS factor structure was replicated and exhibited internal consistency and a good two-week test–retest reliability in Chinese adults with temporomandibular disorder pain.30 In this sample, the PRS alpha was α = 0.90.
Fear of Pain Questionnaire – Chinese (FPQ-C)
The 25-item FPQ-C was derived from the 30-item FPQ-III and assesses fear of severe pain, minor pain, and medical pain.31,32 Each item is rated from 1 (not at all) to 5 (extreme). A higher total score indicates a higher level of fear of pain. The original FPQ structure was replicated in a Chinese sample, although five low- or double-loading items were excluded.32 In this study, the FPQ-C alpha was α = 0.91.
Task Specific Self-Efficacy Scale (SES)
A five-item SES was used to assess perceived confidence in tolerating pain during the CPT on the basis of a longer 10-item version.24 Selected items assessed the levels of confidence in being able to “leave your hand in the icy water for at least a short amount of time”, “bear mild pain for a short period of time”, “withstand a moderate amount of discomfort during the CPT”, “handle a moderate amount of pain from cold water for quite a long time” and “continue the CPT even while experiencing severe pain”. Following previously published work, the degree of confidence for each statement was evaluated between 0 (not at all confident) and 100 (completely confident).25,26 A higher mean score indicates a higher task-related self-efficacy. SES alphas were α = 0.85 and α = 0.83 for the pre- and postexposure assessments, respectively.
Cold Pressor Importance, Intended Effort, and Current Affect Scales
Three importance items, 2 intended effort items, and one single current affect item to evaluate overall mood during testing were adapted from Rhodewalt and Fairpjeld’s self-handicapping and effort study.18 The importance subscale assesses the level of importance of good performance during the CPT as “compared to other people”, “a positive way of maintaining a positive view of one’s strength and grit” and “displeasure of poor performance in comparison with that of other people”. The intended effort subscale assesses the level of difficulty and the level of effort that participants intend to apply to this CPT. The degree of importance and intended effort was assessed on a range between 0 (not at all) to 100 (extremely), and the degree of state was assessed on a range between 0 (extremely negative) and 100 (extremely positive). Higher mean scores indicate higher levels of importance and intended effort. The importance subscale alphas were α = 0.82 and α = 0.89 for the pre- and postexposure assessments, respectively, and the intended effort alphas were α = 0.60 and α = 0.83 for the pre- and postexposure assessments, respectively.
Pain Tolerance and Pain Intensity
Pain tolerance was measured by the total time that the participant’s hand was immersed in ice water, using a 3-minute maximum in the first CPT (T1) and a 4-minute maximum in second CPT (T2). Pain intensity was assessed immediately after each CPT with a widely used three-item composite measuring the (1) average pain intensity during the CPT, (2) worst pain intensity during the CPT and (3) pain intensity during tolerance; each item was assessed on a 0 (no pain) to 10 (worst pain) scale. In this sample, the pain intensity used the average scores of a three-item composite and had an alpha of α = 0.82 at the first CPT and an alpha of α = 0.92 at the second CPT.
Data Analyses
The main analyses were performed with RStudio (Version 1.2.5.001; RStudio Team, 2019) in the R programming environment (Version 4.0.3; R Core Team, 2020). Initial univariate analyses of variance (ANOVAs) and chi-square tests assessed the feedback condition differences in demographics and traits (ie, pain resilience and fear of pain). Subsequently, the linear mixed effects model (using the “lmerTest” package in R) was employed to test the relationship between feedback condition (Positive vs Negative vs Control) and time (T1 vs T2) on pain tolerance (Model 1). Next, another linear mixed effects model (Model 2) was conducted to test whether task-related measures (ie, self-efficacy, importance, intended effort, and state affect) and pain intensity significantly contributed to pain tolerance. Finally, a third linear mixed model (Model 3) was adopted to test the relationship between feedback condition and time after controlling for significant covariates.
Models were represented in R as follows:
Model 1 = lmer(Tolerance~ Condition*Time+ (1 | Subject))
Model 2 = lmer(Tolerance~ Self-efficacy+Importance+Effort+Affect+Intensity + (1 | Subject))
Model 3 = lmer(Tolerance~ Condition*Time + Covariates + (1 | Subject)).
Results
Feedback Condition Differences in Background Characteristics
Feedback conditions did not differ by participant gender χ2 (2) = 0.001, p = 0.995 or ethnicity χ2 (2) = 0.42, p = 0.813. ANOVAs showed no feedback group differences by age, year in university, BMI, pain resilience, or fear of pain (see Table 2).
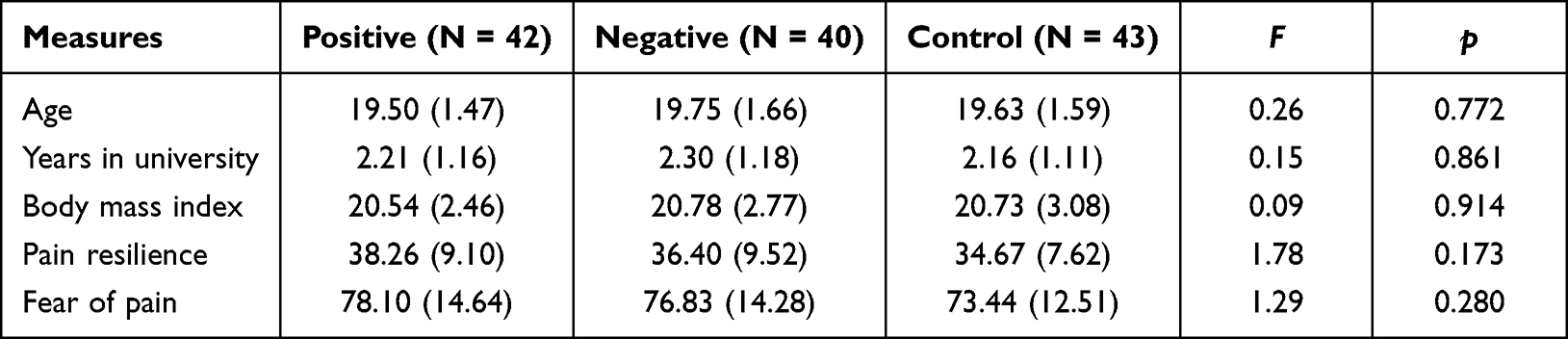 |
Table 2 False Feedback Condition Differences in Background Characteristics |
Effects of False Feedback on Pain Perception and Task-Related Measures
Descriptive statistics (mean and standard deviations) for pain tolerance and task-related measures and for the effects of false performance feedback on those measures are presented in Table 3. The results of linear mixed models showed a significant Condition*Time interaction on pain tolerance and task self-efficacy. As depicted in Figure 2, compared with T1 task performance, participants receiving negative feedback exhibited a higher pain tolerance duration than those receiving control feedback or those receiving positive feedback at the second CPT, whereas the pain tolerance levels of the subsequent two groups did not differ from each other at the second CPT. For task-related self-efficacy (see Figure 3), compared with T1 task performance, participants receiving positive feedback had improved levels of self-efficacy compared to those receiving negative feedback and those receiving control feedback at the second CPT, whereas the task self-efficacy levels of the subsequent two groups did not differ from each other at the second CPT.
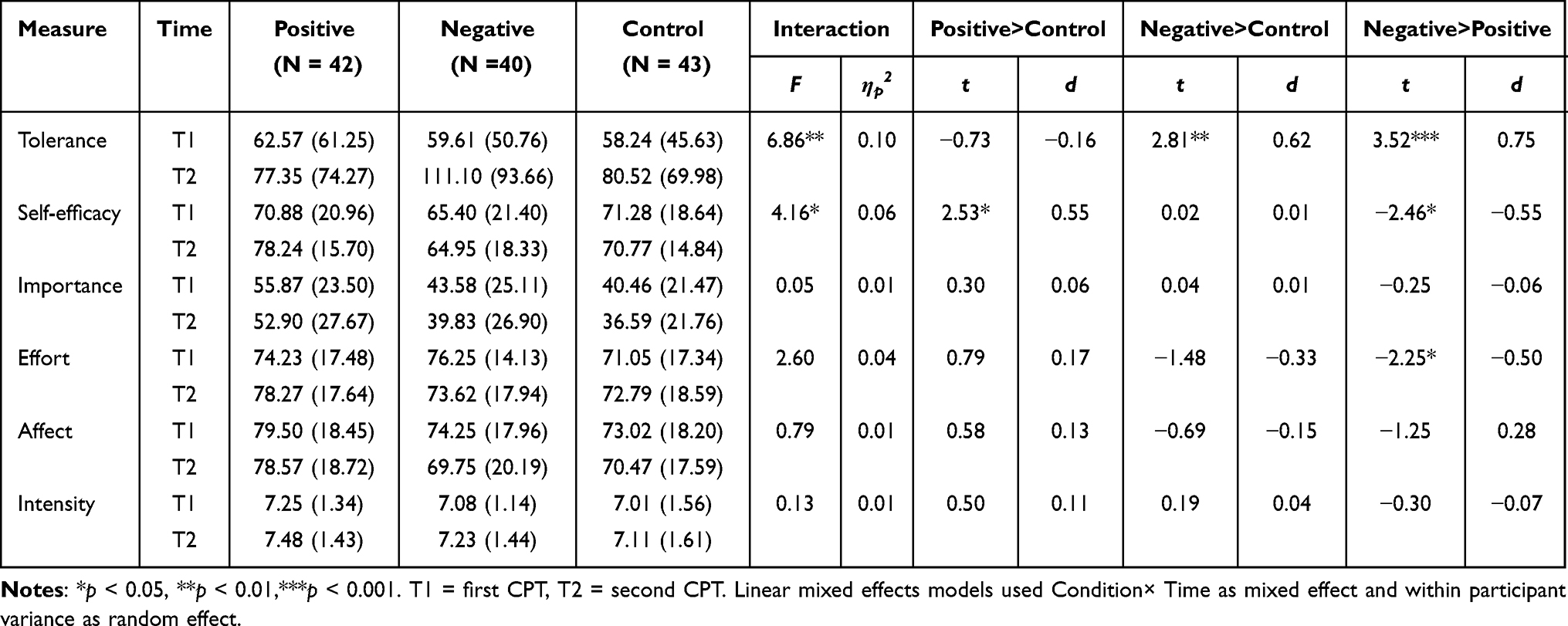 |
Table 3 Mean and Standard Deviation for Pain Tolerance and Task-Related Measures |
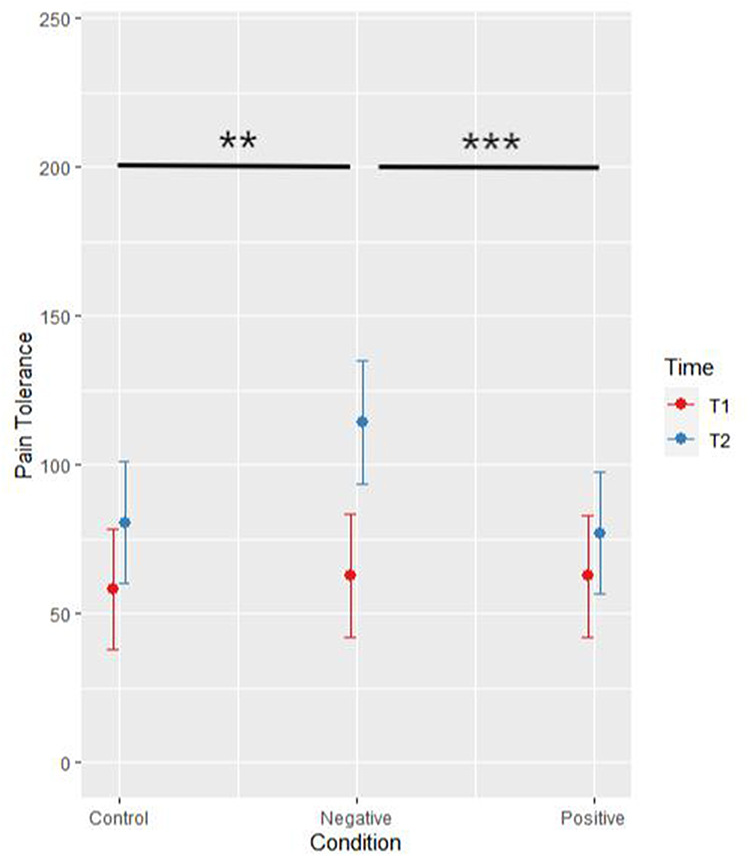 |
Figure 2 Interaction of feedback condition by time on pain tolerance (N = 125). Notes: T1 = first CPT, T2 = second CPT. Compared with T1 task performance, participants receiving negative feedback exhibited a higher pain tolerance duration than those receiving control feedback or those receiving positive feedback at the second CPT, whereas the pain tolerance levels of the positive and control feedback groups did not differ from each other at the second CPT. Error bar represents the standard error. |
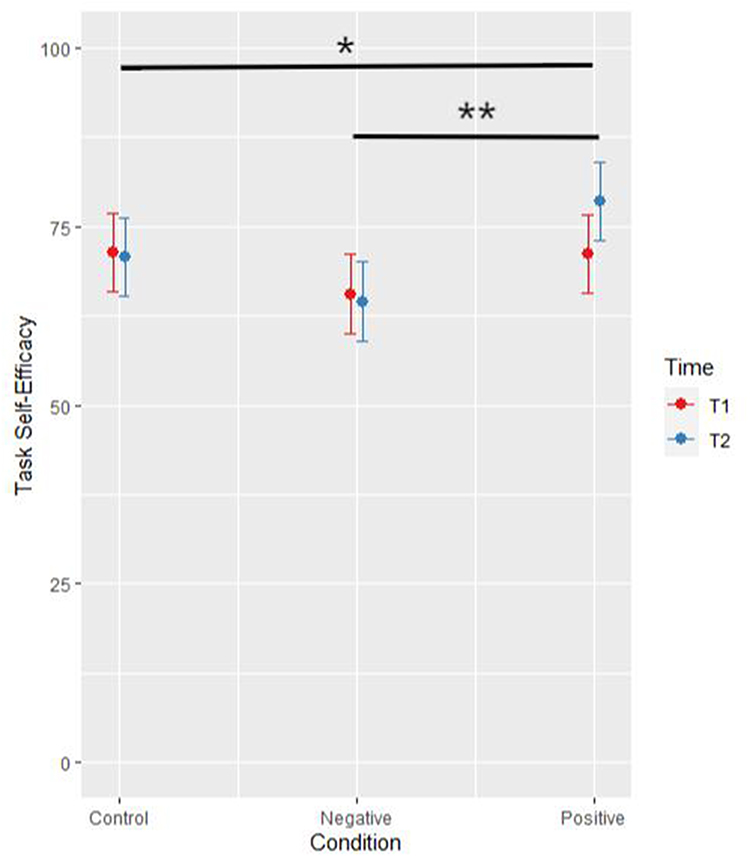 |
Figure 3 Interaction of feedback condition by time on task-related self-efficacy (N = 125). Notes: T1 = first battery of questionnaires measured before CPT, T2 = second battery of questionnaires measured before CPT. Compared with T1 task performance, participants receiving positive feedback had improved levels of self-efficacy compared to those receiving negative feedback and those receiving control feedback at the second CPT, whereas the task self-efficacy levels of the negative and control feedback groups did not differ from each other at the second CPT. Error bar represents the standard error. |
The Condition*Time interaction was marginally significant on intended effort (p = 0.078), though Positive condition showed larger intended effort investment compared to Negative condition at the second CPT. Finally, Condition*Time interaction was not significant on task-related measures of importance, current affect, or pain intensity.
A Greater Investment of Effort and Less Pain Intensity Predicted Longer Pain Tolerance
The results of Model 2 indicate that effort and pain intensity were significant predictors of pain tolerance after controlling for individual variance as random effects. Participants who invested more effort (β = 0.64, t(243.78) = 2.21, p = 0.028) and experienced less pain intensity (β = −12.76, t(243.89) = −4.22, p < 0.001) persisted longer with their hand in ice water. Task-related measures of importance, current affect, and self-efficacy were not significant covariates for pain tolerance (|t|s < 1.25, ps >0.213).
The results of the linear mixed Model 3 with individual variance as a random effect and the addition of effort and pain intensity as covariates still revealed a significant Condition*Time interaction on pain tolerance (F(2, 118.29) = 8.90, p < 0.001, partial η2 = 0.13). After controlling for variance in intentional effort investment (t(237.16) = 2.44, p = 0.015) and pain intensity (t(228.30) = −5.50, p < 0.001), participants receiving negative feedback showed improved pain tolerance duration compared to those receiving control feedback (t(118.11) = 3.31, p = 0.001) and those receiving positive feedback (t(119.44) = 3.96, p < 0.001) during the second CPT, whereas the level of pain tolerance of the positive feedback and control feedback groups did not differ at the second CPT (t(117.40) = −0.72, p = 0.476).
Discussion
The present study investigated how the fake feedback entailing false social comparison information (ie, task performance compared with peers who completed the same task) and delivered orally influenced the task-related status and pain tolerability for ice water in a sample of Chinese university students. Both pain tolerability and task-related self-efficacy were significantly influenced by this false feedback. A longer pain tolerance duration was also predicted by a more intentional investment of effort and a lower intensity of experienced pain in addition to the effect of false feedback. The results of the present study shed light on the situational influences on pain perception via social comparison and motivational perspectives with competing goals.
Consistent with past studies, pain tolerance duration in ice water was significantly impacted by fake feedback on former task performance.10,11 Past studies found that participants receiving high-tolerance feedback had longer pain tolerance duration and better speeded go/no-go task performance compared to control conditions.10–12 However, we did not observe the superiority of positive feedback over negative and control feedbacks in the present study. Specifically, we found that participants receiving negative feedback (ie, worse than average) regarding their performance in the first CPT had better pain tolerance duration in ice water at the second CPT than those receiving control feedback (ie, at the average) and those receiving positive feedback (ie, better than average). Negative feedback prompted the longest increased pain tolerance duration, which might be explained by the face-negotiation theory, which claims that when one’s face or self-image is threatened (eg, my task performance is worse than average), the person tends to strive to save or restore his or her face.33 To defend against the unfavorable impressions and to save face, people tend to invest more effort into self-improvement behaviors.18,34 This is globally true, while the degree is severe in East Asian cultures, particularly in China. Chinese people prefer to compare themselves to the average cultural persona and attempt to position themselves as slightly higher than average.35,36 Whereas in Western cultures, low-tolerance feedback or social models resulted in poor pain tolerability and poor performance in speeded go/no-go task.8,12
Task-related self-efficacy was significantly impacted by fake feedback, which is partially consistent with previous findings.10–12 More specifically, a larger increase in self-efficacy was observed in the positive feedback group than in the other two groups. However, participants who received negative feedback did experience a decrease in their task-related self-efficacy. This observation reveals that healthy participants are more sensitive to positive feedback than to negative feedback, while patients with clinical pain are more vulnerable to threatening information than those in healthy controls.15 Deficiency in the capacity to obtain, communicate, process and understand basic health information and services was one of the barriers to self-efficacy among patients with chronic disease experience.37 Evidence from neuropsychology also demonstrates that fibromyalgia patients showed significant cognitive impairment in all components of executive function (eg, set shifting, inhibition control) compared to age-matched healthy control groups.38
Therefore, we assumed that young healthy participants educated with a university background in the present study had pretty healthy self-efficacy and the capacity to decenter from threatening information regarding self-image (eg, better than average).39
Furthermore, we found that higher pain tolerance duration in ice water was influenced by feedback manipulation, greater intentional effort investment, and a lower intensity of experienced pain. In addition to the effects of false feedback on pain tolerance, we verified the predictive role of intended effort investment in expected behavior (ie, persisting in ice water as long as possible), as previous studies found similar results regarding the completion of environmentally friendly requests and the economics of information.40,41 Naturally, when no specific instruction on how to cope with pain was provided, a negative association between the levels of experienced pain intensity and pain tolerability was confirmed in a laboratory-induced pain setting.42 However, instructions on strategies (eg, acceptance) for coping with experimentally induced pain lead to a reduction in pain ratings and an increase in pain tolerance among healthy participants.43,44 The results of the present study provide empirical evidence to support the planned behavior theory, which claims that intentions serve as predictors of goal-directed behavior.45
Lower than expected levels of perceived importance regarding upcoming tasks, the current state of affect, or task-related self-efficacy were not found to be predictors of pain tolerability. Self-efficacy has been identified as exerting a robust influence on a variety of health outcomes, including the capacity to maintain daily activities despite ongoing pain.14 However, Powers predicted a negative relationship between self-efficacy and performance on the basis of perceptual control theory.46 Consistent with perceptual control theory, Vancouver et al also found that self-efficacy leads to overconfidence and increases the likelihood of committing logic errors during the game.16 In the present study, the association between changes in self-efficacy and changes in pain tolerance was marginally significant (r = −0.15, p = 0.091), showing the tendency to support the perceptual control theory. For the state of affect, one study also found that individual mood differences could not account for the observed group differences in task performance.12 Finally, the level of investment of intentional effort, rather than the perceived importance of the task, was found to be essential to task performance.18 Whether and under what conditions we can further learn from negative or positive feedback has always been a matter of debate.47,48
Strengths aside, this study also has some limitations. First, the fact that these results are derived from the laboratory-induced pain settings among pain-free university students limits their application in clinical pain samples. In clinical contexts, patients, compared with those who have been suffering from the same type of disease, can obtain new perspectives on their situation, set more realistic goals, and finally attenuate health-related dysfunctions.49,50 Therefore, future studies should test whether orally delivered falsified feedback regarding either their disease or coping capacity could attenuate health-related dysfunctions in samples comprising clinical pain patients. Second, social comparison information involving peer pressure was tested in the Chinese context, and whether the findings of the present study could be replicated in other East Asian cultures (eg, Japanese, Korean) remains to be verified. East Asian cultures share similar social norms (eg, modesty) in such a way that individuals are sensitive to the judgments and evaluations of others both explicitly and implicitly.23 We adopted self-reported measures to test the effects of false feedback in the form of social comparison information on explicit self-evaluation (eg, self-efficacy) without measures to test for implicit self-evaluation, which represents the third limitation of the present study. Chinese individuals are expected to manifest low explicit self-esteem while manifesting high implicit self-esteem.23 The discrepancy between explicit and implicit measures accounts for intention‒behavior discordance.51 Third, the experimenters who executed the present study are females, though we intended to simplify the study design and control for possible bias caused by the different genders of the experimenters. Future studies could investigate how feedback given by different genders of experimenters influences participants’ pain tolerability. Finally, although we found that more intended effort investment predicted a longer pain tolerance duration, expectations and their modification impact on pain perception through learning should be addressed in the future research.52
Conclusion
Overall, the results of the present study suggest that orally delivered false feedback concerning pain tolerability in comparison with peers in similar situations provides novel insights into self-efficacy and pain tolerance duration in icy water. Task-related self-efficacy was significantly impacted by false feedback; however, this was not linked to pain tolerance duration. Changes in self-efficacy were also not linked to changes in pain tolerance, though its negative association was marginally significant. Instead, a stable and more intentional investment of effort and a lower level of perceived pain intensity improved pain tolerance. After controlling for intentional effort investment and perceived pain intensity, the false feedback effects on pain tolerance remained significant. Most interestingly, healthy Chinese university participants improved their pain tolerability without decreasing their task-related self-efficacy scores after receiving negative feedback (low-tolerance) than those in positive and neutral conditions. This capacity of healthy individuals to align their behavior with goal-directed instruction (ie, keep one hand in icy water as long as possible) and ignore any threatening information to self-image needs to be further investigated.
Acknowledgments
This research was supported by grants from Xinqiao Hospital and The Second Affiliated Hospital of Army Medical University (2022YQB100) to the first author (SC), China National Natural Sciences Foundation (31871141) to TJ, and Army Medical University (2019R044) to the corresponding author (YH).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Festinger L. A theory of social comparison processes. Human Relat. 1954;7(2):117–140. doi:10.1177/001872675400700202
2. McCaul KD, Johnson RJ, Rothman AJ. The effects of framing and action instructions on whether older adults obtain flu shots. Health Psychol. 2002;21(6):624–628. doi:10.1037/0278-6133.21.6.624
3. Scholly K, Katz AR, Gascoigne J, et al. Using social norms theory to explain perceptions and sexual health behaviors of undergraduate college students: an exploratory study. J Am Coll Health. 2005;53(4):159–166. doi:10.3200/JACH.53.4.159-166
4. Hechter M, Opp KD. What have we learned about the emergence of social norms. In: Hechter M, Opp KD, editors. Social Norms. Russell Sage Foundation; 2001.
5. Craig KD. Social modelling determinants of pain processes. Pain. 1975;1(4):375–378. doi:10.1016/0304-3959(75)90074-3
6. Craig KD, Prkachin KM. Social modeling influences on sensory decision theory and psychophysiological indexes of pain. JPSP. 1978;36:805–815.
7. Wilson JJ, Chaplin WF, Thorn BE. The influence of different standards on the evaluation of pain: implications for assessment and treatment. Behav Ther. 1995;26(2):217–239. doi:10.1016/S0005-7894(05)80103-0
8. Jackson T, Phillips H. Social comparison performance standards, threat, and tolerance for experimentally-induced pain. Eur J Pain. 2011;15(10):1081–1086. doi:10.1016/j.ejpain.2011.04.008
9. Pulvers K, Schroeder J, Limas EF, et al. Computer-delivered social norm message increases pain tolerance. Ann Behav Med. 2014;47(3):316–324. doi:10.1007/s12160-013-9547-x
10. Litt MD. Self-efficacy and perceived control: cognitive mediators of pain tolerance. JPSP. 1988;54:149–160.
11. Liu K, Chen H, Li X, et al. Influence of social comparison on pain coping and tolerance. Chin J Pain Med. 2010;16:200–203.
12. Rigoni D, Braem S, Pourtois G, et al. Fake feedback on pain tolerance impacts proactive versus reactive control strategies. Conscious Cogn. 2016;42:366–373. doi:10.1016/j.concog.2016.04.015
13. Beck AT. The evolution of the cognitive model of depression and its neurobiological correlates. Am J Psychiat. 2008;165(8):969–977. doi:10.1176/appi.ajp.2008.08050721
14. Jackson T, Wang Y, Wang Y, et al. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. 2014;15(8):800–814. doi:10.1016/j.jpain.2014.05.002
15. Henrich JF, Gjelsvik B, Martin M. Implicit identification with illness in patients with irritable bowel syndrome (IBS). Cognit Ther Res. 2018;42(3):328–339. doi:10.1007/s10608-017-9888-z
16. Vancouver JB, Thompson CM, Tischner EC, et al. Two studies examining the negative effect of self-efficacy on performance. J Appl Psychol. 2002;87(3):506–516. doi:10.1037/0021-9010.87.3.506
17. Bandura A. Self-Efficacy: The Exercise of Control. New York: Freedom; 1997.
18. Rhodewalt F, Fairfield M. Claimed self-handicaps and the self-handicapper: the relation of reduction in intended effort to performance. J Res Pers. 1991;25(4):402–417. doi:10.1016/0092-6566(91)90030-T
19. Crombez G, Eccleston C, Van Damme S, et al. Fear-avoidance model of chronic pain: the next generation. Clin J Pain. 2012;28(6):475–483. doi:10.1097/AJP.0b013e3182385392
20. Karoly P, Crombez G. Motivational Perspectives on Chronic Pain: Theory, Research, and Practice. New York: Oxford University Press; 2018.
21. Vlaeyen JW, Crombez G. Behavioral conceptualization and treatment of chronic pain. Annu Rev Clin Psychol. 2020;16(1):187–212. doi:10.1146/annurev-clinpsy-050718-095744
22. Karsdorp PA, Geenen R, Kroese FM, et al. Turning pain into cues for goal-directed behavior: implementation intentions reduce escape-avoidance behavior on a painful task. J Pain. 2016;17(4):499–507. doi:10.1016/j.jpain.2015.12.014
23. Cai H, Sedikides C, Gaertner L, et al. Tactical self-enhancement in China: is modesty at the service of self-enhancement in East Asian culture? Soc Psychol Pers Sci. 2011;2(1):59–64. doi:10.1177/1948550610376599
24. Jackson T, Iezzi T, Gunderson J, et al. Gender differences in pain perception: the mediating role of self-efficacy beliefs. Sex Roles. 2002;47(11/12):561–568. doi:10.1023/A:1022077922593
25. Hutchinson JC, Sherman T, Martinovic N, et al. The effect of manipulated self-efficacy on perceived and sustained effort. J Appl Sport Psychol. 2008;20(4):457–472. doi:10.1080/10413200802351151
26. O’Mara EM, Gaertner L. Does self-enhancement facilitate task performance? JEPG. 2017;146:442–455.
27. Chen S, Jackson T, Kueh YC. Causal effects of challenge and threat appraisals on pain self-efficacy, pain coping, and tolerance for laboratory pain: an experimental path analysis study. PLoS One. 2019;14(4):e0215087. doi:10.1371/journal.pone.0215087
28. Watso JC, Huang M, Belval LN, et al. Low-dose fentanyl reduces pain perception, muscle sympathetic nerve activity responses, and blood pressure responses during the cold pressor test. Am J Physiol. 2022;322(1):R64–R76. doi:10.1152/ajpregu.00218.2021
29. Slepian PM, Ankawi B, Himawan LK, et al. Development and initial validation of the pain resilience scale. J Pain. 2016;17(4):462–472. doi:10.1016/j.jpain.2015.12.010
30. He S, Wang J, Ji P. Validation of the Pain Resilience Scale in Chinese‐speaking patients with temporomandibular disorders pain. J Oral Rehabi. 2018;45(3):191–197. doi:10.1111/joor.12591
31. McNeil DW, Rainwater AJ. Development of the fear of pain questionnaire-III. J Behav Med. 1998;21(4):389–410. doi:10.1023/A:1018782831217
32. Yang Z, Todd J, Meng J, et al. The reliability and validity of the Fear of Pain Questionnaire-III. Chin J Clin Psychol. 2013;21:768–773.
33. Ting-Toomey S, Kurogi A. Facework competence in intercultural conflict: an updated face-negotiation theory. Int J Intercult Rel. 1998;22(2):187–225. doi:10.1016/S0147-1767(98)00004-2
34. Sherman DK, Hartson KA. Reconciling self-protection with self-improvement. Handbook Self Enhanc Self Protect. 2011;128:128–151.
35. Alickee MD, Sedikides C. Self-enhancement and self-protection: what they are and what they do. Eur Rev Soc Psychol. 2009;20(1):1–48. doi:10.1080/10463280802613866
36. Heine SJ, Hamamura T. In search of East Asian self-enhancement. Pers Soc Psychol Rev. 2007;11(1):4–27. doi:10.1177/1088868306294587
37. Farley H. Promoting self‐efficacy in patients with chronic disease beyond traditional education: a literature review. Nurs Open. 2020;7(1):30–41. doi:10.1002/nop2.382
38. Bell T, Trost Z, Buelow MT, et al. Meta-analysis of cognitive performance in fibromyalgia. J Clin Exp Neuropsychol. 2018;40(7):698–714. doi:10.1080/13803395.2017.1422699
39. Zell E, Strickhouser JE, Sedikides C, et al. The better-than-average effect in comparative self-evaluation: a comprehensive review and meta-analysis. Psychol Bull. 2020;146(2):118–149. doi:10.1037/bul0000218
40. Baek TH, Yoon S, Kim S. When environmental messages should be assertive: examining the moderating role of effort investment. In J Advert. 2015;34(1):135–157. doi:10.1080/02650487.2014.993513
41. Kleinberg J, Raghavan M. How do classifiers induce agents to invest effort strategically? ACM TEAC. 2020;8(4):1–23. doi:10.1145/3417742
42. Nayak S, Shiflett SC, Eshun S, et al. Culture and gender effects in pain beliefs and the prediction of pain tolerance. CCR. 2000;34:135–151.
43. Gutiérrez O, Luciano C, Rodríguez M, et al. Comparison between an acceptance-based and a cognitive-control-based protocol for coping with pain. Behav Ther. 2004;35(4):767–783. doi:10.1016/S0005-7894(04)80019-4
44. Keogh E, Bond FW, Hanmer R, et al. Comparing acceptance-and control-based coping instructions on the cold-pressor pain experiences of healthy men and women. Eur J Pain. 2005;9(5):591–598. doi:10.1016/j.ejpain.2004.12.005
45. Ajzen I, Madden TJ. Prediction of goal-directed behavior: attitudes, intentions, and perceived behavioral control. J Exp Soc Psychol. 1986;22(5):453–474. doi:10.1016/0022-1031(86)90045-4
46. Powers WT. Commentary on Bandura’s “human agency”. Am Psychol. 1991;46(2):151–153. doi:10.1037/0003-066X.46.2.151.b
47. Klein TA, Neumann J, Reuter M, et al. Genetically determined differences in learning from errors. Science. 2007;318(5856):1642–1645. doi:10.1126/science.1145044
48. Eppinger B, Kray J. To choose or to avoid: age differences in learning from positive and negative feedback. J Cognit Neurosci. 2011;23(1):41–52. doi:10.1162/jocn.2009.21364
49. Davison KP, Pennebaker JW, Dickerson SS. Who talks? The social psychology of illness support groups. Am Psychol. 2000;55(2):205–217. doi:10.1037/0003-066X.55.2.205
50. Cheng ST, Fung H, Chan A. Maintaining self-rated health through social comparison in old age. J Gerontol B Psychol. 2007;62(5):277–285. doi:10.1093/geronb/62.5.P277
51. Divine A, Berry T, Rodgers W, et al. The relationship of self-efficacy and explicit and implicit associations on the intention–behavior gap. J Phys Act Health. 2020;18(1):29–36. doi:10.1123/jpah.2019-0033
52. Wiech K. Deconstructing the sensation of pain: the influence of cognitive processes on pain perception. Science. 2016;354(6312):584–587. doi:10.1126/science.aaf8934
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.