Back to Journals » International Journal of Women's Health » Volume 15
Effects of Education and Guided Imagery Program on Stress Level and Coping Behaviors Among Pregnant Women at Risk of Preterm Birth
Authors Ukhawounam U ![]() , Limruangrong P
, Limruangrong P ![]() , Pungbangkadee R
, Pungbangkadee R ![]() , Vongsirimas N
, Vongsirimas N
Received 25 April 2023
Accepted for publication 26 September 2023
Published 19 October 2023 Volume 2023:15 Pages 1581—1591
DOI https://doi.org/10.2147/IJWH.S418693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Uraiwan Ukhawounam,1 Piyanun Limruangrong,2 Rudee Pungbangkadee,2 Nopporn Vongsirimas3
1Master of Nursing Science Program in Midwifery, Faculty of Nursing, Mahidol University, Nakhonpathom, Thailand; 2Department of Obstetrics and Gynaecology Nursing, Faculty of Nursing, Mahidol University, Bangkok, Thailand; 3Department of Mental Health and Psychiatric Nursing, Faculty of Nursing, Mahidol University, Nakhonpathom, Thailand
Correspondence: Piyanun Limruangrong, Department of Obstetrics and Gynaecology Nursing, Faculty of Nursing, Mahidol University, 2 Wang Lang Road, Siriraj, Bangkoknoi, Bangkok, 10700, Thailand, Tel +66 2419 7466 80 ext. 1808, Fax +66 2412 8415, Email [email protected]
Purpose: The rate of preterm birth continues to increase worldwide. Pregnant women at risk of preterm birth experience more stress during pregnancy, which directly impacts their mental well-being and preterm birth situation. Stress management can significantly reduce stress and promote appropriate coping behaviors in pregnant women at risk of preterm birth. The purpose of this study was to determine the effects of education and guided imagery program on stress level and coping behaviors among pregnant women at risk of preterm birth.
Patients and Methods: Forty-eight pregnant women who visited the antenatal care unit at Ramathibodi Hospital and were at risk of preterm birth with moderate stress score were included. They were divided into two groups, each comprising 24 participants. The control group received standard nursing care, whereas the experimental group received an education and guided imagery program in addition to standard nursing care. The Perceived Stress Scale-10 and Coping Behavior Questionnaire were used to collect data.
Results: The results revealed that the mean stress score in the experimental group after receiving the program was lower than before with statistical significance (t = 7.14, p < 0.001). Moreover, the experimental group had lower stress score (F1,45 = 16.92, p < 0.001) and greater coping behavior score (F1,45 = 7.85, p < 0.01) compared with the control group after receiving the program, and the differences were statistically significant.
Conclusion: This research highlights the importance of preventing mental health problems in pregnant women at risk of preterm birth by using an education and guided imagery program to decrease stress and promote appropriate coping behaviors.
Keywords: stress management, mental health, preterm labor, prevention, pathophysiology, coping mechanism
Introduction
The preterm birth rate continues to increase by 15 million cases annually, which is equivalent to 10.6% of all newborns worldwide.1 In Thailand, the ratio of preterm births is 12% of 838,300 newborns, which exceeds the established indicator criteria of 9.5% per year.2 Once pregnant women undergo preterm labor, they are usually admitted immediately, placed on absolute bed rest, and provided with long-term treatment, which may lead to multiple side effects from the administered drugs.3,4 In addition, their mental well-being is affected by emotional instability, stress, anxiety regarding themselves and the fetus, and treatment costs.5,6 Furthermore, failure to inhibit uterine contractions will impact preterm birth, leading to low birth weight, birth asphyxia,7 respiratory distress syndrome,8 and neurodevelopmental delay.9
Several complex biological and biomedical risk factors may affect preterm labor and birth, including infection, hypertension, gestational diabetes mellitus, thyroid disease, placenta previa, and heart disease. These risk factors are caused by complications that occur during pregnancy, the treatment of which is curative rather than preventive. Stress is a major risk factor for preterm birth, and research has indicated that other risk factors for preterm birth are also linked to stress.10 Thus, this study examined the stress levels of pregnant women with risk factors for preterm birth, including age, body mass index, previous preterm birth, short cervix, and previous abortion.
Pregnant women at risk of preterm birth most likely feel stressed during pregnancy. Stress is a condition where a person is aware of the threat and danger from a situation or problem after primary appraisal assessment.11 Previous studies have showed that stress levels are directly linked to preterm births.12,13 Psychosocial and biological processes related to stress result in premature birth; therefore, guidelines for stress management need to be developed.14
In pregnant women at risk of preterm birth, primary appraisal is first conducted to find the risk factors causing stress; then, secondary appraisal is performed to find the resources to manage stress.11 Examples of coping resources for pregnant women at risk of preterm birth include providing information and support to promote appropriate coping behavior.10,15 There are two types of coping behaviors: problem-focused coping involves finding a strategy for solving the problem directly according to the factors that cause stress, and emotional-focused coping focuses on providing distraction from the problems or situations through activities that alleviate negative feelings resulting in relaxation.11 Pregnant women at risk of preterm birth should use both coping behaviors because emotional-focused coping mechanism alone cannot directly eliminate the risks. Therefore, pregnant women at risk of preterm birth should learn problem-focused coping techniques to ensure appropriate behavior during stressful situations. Effective coping mechanisms should lead to three desired outcomes: good adaptation of social roles (social functioning), positive adaptation of emotions and feelings (morale), and good adaptation of physical health (somatic health).11
Stress management techniques that are effective for managing stress in pregnant women include yoga,16 progressive muscle relaxation,17,18 social support,19 music therapy,20 and guided imagery.21–24
Some previous studies have used guided imagery to manage stress in pregnant women with preterm labor. Jallo et al23 studied stress levels in pregnant women with preterm labor. They found that the stress levels of pregnant women decreased after receiving education and guided imagery, and the differences were statistically significant (p < 0.05). In Thailand, Tantra et al24 studied stress levels in pregnant women with preterm labor. They found that the experimental group had lower stress levels than the control group after receiving the guided imagery program, and the differences were statistically significant (p < 0.001). Another study examined the impact of stress management education and relaxation exercises on stress in pregnant women for 5 weeks. The results showed that the experimental group had lower stress levels and higher coping behavior scores compared with the control group, and the differences were statistically significant (both p < 0.05).17
The present study explored the effects of a 5-week stress management education and guided imagery program as a mechanism for managing stress in pregnant women at risk of preterm birth. Stress management education and guided imagery have many advantages, including simple operation, convenience of monitoring pregnant women’s activities through modern technology,23 and the ability to gain knowledge about stress and the risk of preterm birth. Pregnant women will show negative emotions when they are confronted with risky situations.25 Therefore, before they receive the education and guided imagery program, they must acquire positive thoughts through the ABC technique, which aims to manage a person’s beliefs or thoughts to become a positive way for having reasonable behaviors, including A) Activating events that assess the person’s understanding regarding facing some situations or problems, B) Beliefs that assess the person’s beliefs or thoughts in that situation or problem, C) Consequences of emotions that assess the person’s emotions and behaviors to that situation or problem.26 This technique will enable the researcher to understand the beliefs or thoughts concerning the risks that pregnant women may face. Subsequently, the researcher will adjust the beliefs or thoughts so that they are reasonable and positive, which should lead to appropriate emotions and behaviors when dealing with stressful situations.
Materials and Methods
Design and Study Sites
A quasi-experimental design (pretest–posttest design with a comparison group) was applied to select pregnant women who received antenatal care at Ramathibodi Hospital between April and December 2022.
Population and Samples
The samples were selected using purposive sampling based on the following inclusion criteria: gestational age between 24 and 32 weeks, depending on the gestational of preterm birth’s definition by The Royal Thai College of Obstetricians and Gynecologists;27 at least one risk factor for preterm birth (eg age ≤19 or ≥35 years, body mass index <18.5 or ≥30 kg/m2, previous preterm birth, cervix length <25 mm, or previous abortion); moderate stress score (stress score, 14–26 points); ability to communicate in Thai; and availability of an Internet connection and smartphone. Simultaneously, pregnant women were excluded based on the following criteria: complications during pregnancy (eg heart disease, hypertension, and gestational diabetes mellitus), mental and behavioral disorders (eg schizophrenia, bipolar disorder, and depressive illness), substance abuse, and presence of fetal abnormality in the ultrasound.
The sample size was calculated using G* Power, with a 5% significance level, 80% power, and medium effect size (d = 0.73), using data from a previous study in Switzerland.28 They found the medium effect size of their outcome that the stress score of pregnant women in the experimental group, applying the guided imagery technique, after receiving the program was lower than that in the control group with statistical significance (p < 0.001). Adding 10% for allowing dropout, bringing the total to 54 cases divided into two groups with 27 cases each. Unfortunately, during the data collection period, six participants dropped out (three from the control group [one had preterm birth and two did not respond after being contacted three times] and three from the experimental group [who did not respond after being contacted three times]). Therefore, 48 cases remained at the end of data collection, with 24 cases in each group (Figure 1).
 |
Figure 1 Study flowchart. |
Research Instrument
Instruments for Implementation
The Risk Assessment Form for Preterm Birth was developed by a researcher based on a literature review.4,29 It was used as a criterion for research cases by selecting pregnant women who had moderate stress level (stress score 14–26 points) according to the Perceived Stress Scale-10 (PSS-10) and at least one of the following risk factors: age ≤19 years or ≥35 years, body mass index <18.5 or ≥30 kg/m2, previous preterm birth, cervix length <25 mm, or previous abortion.
The education and guided imagery program was developed by a researcher based on the concept of stress, as portrayed by Lazarus et al.11 Guidelines were applied to reduce stress levels and promote appropriate coping behaviors among pregnant women at risk of preterm birth. The procedure consisted of problem-focused coping training activities, including education about stress and the risk of preterm birth, critical thinking practice in solving problems by conducting tests about situations at risk of preterm birth and discussion through LINE or telephone, monitoring participants through LINE or telephone to follow-up on their stress management, practicing coping techniques, inquiring about obstacles, and finding solutions together. Emotional-focused coping training activities included adjusting positive thinking with the ABC technique, relaxation training with guided imagery, monitoring with positive thinking adjustment, and practicing guided imagery, which were administered via Google form or telephone.
Instruments for Data Collection
The personal data form was developed by a researcher based on existing literature.13,17,23,29 It consists of 21 items divided into two sections: general information and gestational information of pregnant women.
The Thai version of PSS-10, developed by Wongpakaran et al,30 was used to measure perceived stress in the past month. It comprises 10 items assessed using a rating scale of five levels. The total score ranges from 0 to 40, with higher scores indicating higher stress levels and lower scores indicating lower stress levels.
The Coping Behavior Questionnaire was requested from Chunpradab31 and adapted based on the stress concept of Lazarus et al,11 who used this tool in high-risk pregnant women. The questionnaire was adapted to pregnant women at risk of preterm birth. It comprises 30 items assessed using a rating scale of four levels. The total score ranges from 30 to 120, with higher scores indicating higher coping behaviors and lower scores indicating lower coping behaviors.
The Risk Assessment Form for Preterm Birth, education and guided imagery program, personal data form and Coping Behavior Questionnaire were reviewed and approved by three experts, including an obstetrician, psychiatric nurse teacher, and professional nurse. The content validity index was calculated as 1. The risk assessment form and education and guided imagery program were tested on two pregnant women with similar situations to the samples, and the results showed that they were appropriate in terms of activity details, implementation, and duration. Moreover, PSS-10 and the Coping Behavior Questionnaire were tested on 20 pregnant women with similar situations to the samples, and they had Cronbach’s alpha coefficients equal to 0.71 and 0.84, respectively.
Ethical Considerations
This research was evaluated and certified by the Institutional Review Board of the Faculty of Nursing (NSIRB) and the Faculty of Medicine at Ramathibodi Hospital (RAMAIRB), Mahidol University (MU-MOU CoA No. IRB-NS2022/673.1503). Furthermore, the research was conducted in accordance with the Declaration of Helsinki. All participants were treated ethically in view of the Human Research Protection, whereby the researcher conducted data collection under the international standard procedures of the Human Research Ethics Committee. This study recognized the right of participants to refuse participation once they received all information regarding the study from the researcher.
Methods of Data Collection
Data were first collected from the control group and then the experimental group to prevent data contamination. The researcher contacted each group, asking the participants to fill out the personal data form and made an appointment to contact them, during conducting of this study for 5 weeks, through the LINE application, Google form, and telephone, after they consented to participate in the study. All participants in both groups received standard nursing care, which included a preliminary risk screening by the antenatal unit nurses and a more detailed screening for risks of preterm birth, including physical and antenatal examination by the obstetric team. If risk factors were found, the participants would be documented as having a high-risk pregnancy in the antenatal document and receive individual advice from the obstetricians and the nurses regarding the practice and prevention of preterm birth (without the use of media) to educate and practice preterm birth prevention skills. However, the experimental group received an education and guided imagery program in addition to standard nursing care.
Education and Guided Imagery Program for the Experimental Group
The intervention group was informed that the period of the education and guided imagery program was 5 weeks and conducted through LINE application, Google form, and telephone. The intervention consisted of a 15-min video clip on Stress in Pregnant Women at Risk of Preterm Birth and Information on Stress Management through Education with Guided Imagery through a LINE video call. Subsequently, the researcher distributed the video clip and electronic manual through the LINE application so that the participants could review the resources whenever they wished. Subsequently, the researcher sent the Google form’s link of the Critical Thinking Practice in Solving Problems Form, wherein the participants could apply their knowledge from the educational program to complete practice tests with questions regarding situations at risk of preterm birth.
In the guided imagery therapy, the participants were allowed to listen to 8–15-min sessions by the researcher, selected from the five video sets sent to them through the LINE, for at least two times per week. After each set, the participants recorded what they heard in the Follow-up Guided Imagery Form, which enabled the researcher to monitor the results using the forms or inquiring through the telephone.
Moreover, the participants were assessed and adjusted their beliefs and thoughts using the ABC technique at least once per week by the researcher. First, the researcher used the following question: “Do you know what risk factors you have for the risk of preterm birth?” to assess the participants’ understanding that they were at risk of preterm birth with the help of the researcher (A: Activating Event). In addition, the researcher used the following question: “What are your beliefs or thoughts on the situations you may face that risk preterm birth?” to assess the beliefs or thoughts of participants (B: Beliefs). Finally, the researcher used the following question: “What are your beliefs or thoughts about the risky situation that you may face, and how do they affect your mood?” to assess the emotions and behaviors (C: Emotional consequences) of participants by observing their facial expressions and posture for signs of concern or stress. After analyzing their beliefs and emotions, the researcher gave advice and adjusted their thoughts positively in two ways. First, the researcher adjusted their negative beliefs or thoughts (B), which helped to adjust the participants’ mood and reduce stress levels, leading to appropriate behaviors. Second, the researcher praised and highlighted positive beliefs or thoughts that the participants already had (B), which would further promote appropriate coping behaviors.
The researcher followed up the participants via telephone once a week for 10–15 min. The activities included positive thought assessment regarding the risky situation of preterm birth and inquiry on some problems or obstacles that might occur during the activities that the researcher would encourage them to find solutions together. Five weeks after the intervention, a posttest, the PSS-10 (10 items) and Coping Behavior Questionnaire (30 items), were obtained from all participants in both groups through Google form.
Data Analysis
The data were analyzed by using the PASW Statistics version 18.0 (SPSS Inc., Chicago, USA),32 wherein the significance level was set at.05. The personal data were analyzed using descriptive statistics, and comparisons were made between the experimental group and the control group by using the chi-square test or Fisher’s exact test.
The stress levels in the experimental group, comparing between before and after receiving the program, were analyzed using the paired sample t-test, based on the interval scale of the variable and normal distribution that was verified using the Kolmogorov–Smirnov test (p > 0.05), and had two related groups.
Moreover, the stress levels and coping behaviors between the groups were analyzed using the analysis of covariance (ANCOVA), in which the covariate (pretest stress score) was controlled. ANCOVA was based on 1) the normal distribution of posttest stress score and posttest coping behavior score that was verified using the Kolmogorov–Smirnov test (p > 0.05), 2) the homogeneity of variance of posttest stress score and posttest coping behavior score that had no statistically significant difference based on the Levene’s test (p > 0.05), 3) the independent of covariate and treatment effect of pretest stress score between the two groups that had no statistically significant difference (p > 0.05), 4) the homogeneity of regression slope between pretest stress score and posttest stress score and posttest coping behavior score that had no statistically significant difference (p > 0.05).33
Results
The demographic characteristics between the experimental group and the control group were compared using the chi-square test or Fisher’s exact test. The results showed that the demographic characteristics of both groups were not significantly different (p > 0.05) in terms of age, marital status, education level, occupation, nature of work, income, and income sufficiency (Table 1). Similarly, the obstetric characteristics of both groups were not significantly different (p > 0.05) in terms of gestational age, gestational age of first antenatal visit, parity, and prepregnancy body mass index (Table 2).
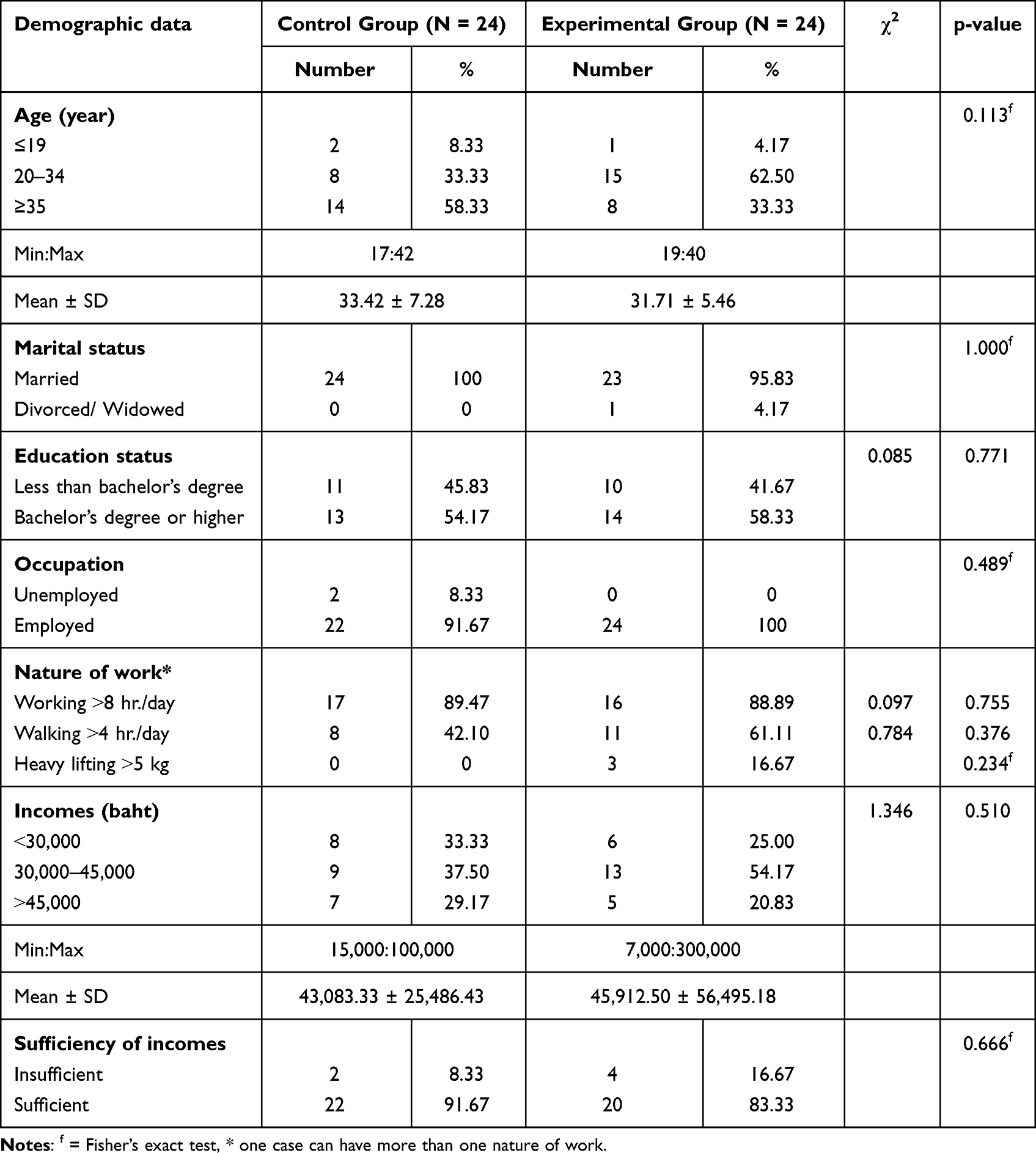 |
Table 1 Characteristics of Participants Classified According to Personal Characteristics |
 |
Table 2 Characteristics of Participants Classified According to Obstetric Characteristics |
A comparison of the characteristics of risk factors of preterm birth between the control group and the experimental group was conducted. The results showed that the characteristics of participants in both groups were not significantly different (p > 0.05) (Table 3).
 |
Table 3 Characteristics of Participants Classified According to Risk Factors for Preterm Birth |
According to the data, the mean stress scores were 17.79 points (standard deviation [SD] = 3.48) and 10.83 points (SD = 4.69) before starting and after receiving the program, respectively. When these stress scores were compared using the paired t-test, the results showed that the mean stress scores of the experimental group after receiving the program were lower than those before receiving the program, and the differences were statistically significant (t = 7.14, p < 0.001) (Table 4).
 |
Table 4 Comparison of Mean Stress Scores Before and After Receiving the Program in the Experimental Group |
The results showed that the control and experimental groups had mean stress scores of 16.08 points (SD = 5.18) and 10.83 points (SD = 4.69), respectively, after receiving the program. Moreover, the stress scores in the experimental group were lower than those in the control group when analyzed by ANCOVA, which controlled for the influence of the covariate (pretest stress score), and the differences were statistically significant (F1,45 = 16.92, p < 0.001) (Table 5).
 |
Table 5 Comparison of Mean Stress Scores Between the Control and Experimental Groups by Controlling the Influence of Pretest Stress Scores Using ANCOVA (N = 48) |
Based on the results, the control and experimental groups had mean coping behavior scores of 87.13 points (SD = 10.13) and 95.33 points (SD = 9.82), respectively, after receiving the program. Moreover, the coping behavior scores in the experimental group were higher than those in the control group when analyzed by ANCOVA, which controlled for the influence of the covariate (pretest stress score), and the differences were statistically significant (F1,45 = 7.85, p < 0.01) (Table 6).
 |
Table 6 Comparison of Mean Coping Behavior Scores Between the Control and Experimental Groups by Controlling the Influence of Pretest Stress Scores Using ANCOVA (N = 48) |
Discussion
This study aimed to determine the effects of education and guided imagery program on stress level and coping behaviors among pregnant women at risk of preterm birth, based on the conceptual stress framework of Lazarus et al11 to reduce the stress level and promote appropriate behavior during stressful situations. The results showed that education and guided imagery programs effectively reduce stress levels and promote coping behaviors in pregnant women at risk of preterm birth.
These findings are consistent with the conceptual stress framework of Lazarus et al11 When pregnant women at risk of preterm birth were aged ≤19 or ≥35 years and had a body mass index <18.5 or ≥30 kg/m2, previous preterm birth, or previous abortion, they underwent primary appraisal to determine whether the risk factors cause stress. If the participants were found to have risk factors that cause stress, they would undergo secondary appraisal to find coping resources to manage stress. The necessary coping resources for pregnant women at risk of preterm birth include providing substantial information on how to behave appropriately in situations of risk and support from other medical personnel.10,15 The results of the present study indicate that pregnant women at risk of preterm birth would benefit from having problem-focused and emotional-focused coping behaviors. This would ensure appropriate and successful coping in all three aspects: social functioning where the adaptation of social roles is good, morale where adaptation to emotions and feelings is positive, and somatic health where adaptation is manifested in good physical health.11
This study consisted of problem-focused coping training activities, including education on stress and the risk of preterm birth, critical thinking practice in solving problems by conducting practice tests with questions on risky situations for preterm birth, and monitoring participants through LINE or telephone. The results showed that the participants displayed better self-care skills after receiving information and knowledge. Furthermore, regular weekly follow-up visits proved to be beneficial because some participants, when faced with actual situations, were unsure whether or not they were facing a situation of risk. For instance, in labor pain situations, some participants still doubted whether they were in preterm labor, and when they had more vaginal discharge than usual, some participants were uncertain whether it was caused by an infection or a symptom of leakage. Therefore, follow-up visits by the researcher were beneficial because they allowed the participants to make inquiries and receive clearer explanations.
The emotional-focused coping training activities included listening to guided imagery therapy, which made the participants feel relaxed. Furthermore, positive thinking adjustment activity through telephone once a week with the ABC technique helped the participants to consistently have positive thoughts toward the risk of preterm birth, affecting their emotions and appropriate coping behaviors.26 The results indicated that all participants had positive thoughts about the risk of preterm birth and believed that they could prevent preterm birth if they behaved properly.
The results of this study are consistent with those of previous research, confirming that education and guided imagery programs can reduce stress levels in pregnant women facing stressful situations. This was consistent with the study of Chuang et al34 and Jallo et al23 investigated stress levels in pregnant women with preterm labor by providing education programs on stress management and listening to guided imagery therapy. The results showed that the experimental group had lower stress levels than the control group, and the differences were statistically significant (p < 0.001, p< 0.05 respectively). In Thailand, Tantra et al24 studied stress levels in pregnant women with preterm labor by providing knowledge about guided imagery practice together with listening to guided imagery therapy. They discovered that the experimental group had lower stress levels compared with the control group after receiving the program, and the differences were statistically significant (p < 0.001). Moreover, this study, having the programs for 5 weeks, effectively reduced stress and promoted coping behavior among pregnant women exposed to stressful situations. Similarly, Ertekin Pinar et al17 studied stress education and relaxation training in general pregnant women for 5 weeks. They found that the experimental group had lower stress levels and higher coping behavior scores than the control group at the end of the program, and the differences were statistically significant (both p < 0.05).
The present and previous studies conducted on general pregnant women,17 pregnant women with preterm labor,23,24 and pregnant women at risk of preterm birth revealed that education and stress management programs could effectively reduce stress levels, which effectively promoted emotional-focused coping behaviors. Moreover, several studies found that effective coping behaviors depend on the interval of each intervention; for example, the United States study found that effective coping behaviors could not be promoted in 8 days.23 In contrast, this study and Turkey’s study found that effective coping behaviors could be promoted in 5 weeks.17 Moreover, this study was concerned with providing knowledge about the situations at risk of preterm birth among pregnant women, while other studies focused only on stress information.17,23,24 The evidence shows that, during the program, most pregnant women who were at risk of preterm birth were concerned about their health and the fetus’s health when they were in situation at risk of preterm birth. Therefore, providing pregnant women with knowledge about the situations at risk of preterm birth could promote problem-focused coping behaviors, which in turn can prevent preterm birth.
Strengths and Limitations
The strengths of this study are that the education and guided imagery program was developed for high-risk pregnant women who experience stressful situations during pregnancy. Moreover, the program has been developed according to the conceptual stress framework of Lazarus et al11 to help high-risk pregnant women reduce stress and promote coping behaviors effectively, which are both problem- and emotional-focused coping behaviors. However, the current study was limited by the selection of pregnant women from a single center and use of a purposive sampling method without random allocation of participants into groups. Therefore, future studies should be conducted in a larger sample size across multicenter and use randomized controlled trials to obtain more reliable research results.
Conclusion
The mental well-being and preterm birth situation of pregnant women at risk of preterm birth are affected when they face stressful situations. Therefore, effective stress management techniques are significant in managing stress. This study showed that education and guided imagery program could reduce stress and promote coping behaviors effectively. In addition, nurses or midwives can prevent mental health problems in pregnant women at risk of preterm birth by using this program for stress management, which can be self-implemented, leading to decreased stress levels and increased appropriate coping behaviors.
Acknowledgments
The authors would like to thank all the participants who contributed to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chawanpaiboon S, Vogel JP, Moller A-B, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Global Health. 2019;7(1):e37–e46. doi:10.1016/S2214-109X(18)30451-0
2. Ministry of Public Health. Guidelines for the Inspection of the Ministry of Public Health for the Year 2018; 2018.
3. American College of Obstetricians and Gynecologists. Practice bulletin no. 171: management of preterm labor. Obstet Gynecol. 2016;128(4):e155–164. doi:10.1097/AOG.0000000000001711
4. Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics.
5. Maloni JA. Antepartum bed rest for pregnancy complications: efficacy and safety for preventing preterm birth. Biol Res Nurs. 2010;12(2):106–124. doi:10.1177/1099800410375978
6. Rubarth LB, Schoening AM, Cosimano A, Sandhurst H. Women’s experience of hospitalized bed rest during high-risk pregnancy. J Obstetric Gynecol Neonatal Nursing. 2012;41(3):398–407. doi:10.1111/j.1552-6909.2012.01349.x
7. Tasew H, Zemicheal M, Teklay G, Mariye T, Ayele E. Risk factors of birth asphyxia among newborns in public hospitals of Central Zone, Tigray, Ethiopia 2018. BMC Res Notes. 2018;11(1):496. doi:10.1186/s13104-018-3611-3
8. Qari SA, Alsufyani AA, Muathin SH, El Margoushy NM. Prevalence of respiratory distress syndrome in neonates. Egyptian J Hospital Med. 2018;70(2):257–264. doi:10.12816/0043086
9. Bolisetty S, Dhawan A, Abdel-Latif M, Bajuk B, Stack J, Lui K. Intraventricular hemorrhage and neurodevelopmental outcomes in extreme preterm infants. Pediatrics. 2014;133(1):55–62. doi:10.1542/peds.2013-0372
10. Alderdice F, Lynn F. Stress in pregnancy: identifying and supporting women. Br J Midwifery. 2009;17(9):552–559. doi:10.12968/bjom.2009.17.9.43787
11. Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York: Springer Publishing Company; 1984.
12. Pais M, Pai M. Stress among pregnant women: a systematic review. J Clin Diagnostic Res. 2018;12:LE01–LE04.
13. Tanpradit K, Kaewkiattikun K. The effect of perceived stress during pregnancy on preterm birth. Int J Womens Health. 2020;12:287–293. doi:10.2147/IJWH.S239138
14. Schetter CD. Stress processes in pregnancy and preterm birth. Curr Dir Psychol Sci. 2009;18(4):205–209. doi:10.1111/j.1467-8721.2009.01637.x
15. Giurgescu C, Penckofer S, Maurer MC, Bryant FB. Impact of uncertainty, social support, and prenatal coping on the psychological well-being of high-risk pregnant women. Nurs Res. 2006;55(5):356–365. doi:10.1097/00006199-200609000-00008
16. Chen PJ, Yang L, Chou CC, Li CC, Chang YC, Liaw JJ. Effects of prenatal yoga on women’s stress and immune function across pregnancy: a randomized controlled trial. Complement Ther Med. 2017;31:109–117. doi:10.1016/j.ctim.2017.03.003
17. Ertekin Pinar S, Duran Aksoy O, Daglar G, Yurtsal ZB, Cesur B. Effect of stress management training on depression, stress and coping strategies in pregnant women: a randomised controlled trial. J Psychosom Obstet Gynaecol. 2018;39(3):203–210. doi:10.1080/0167482X.2017.1321632
18. Jittrapirom A, Sateapongprapa J, Klunklin A. Effectiveness of relaxation training program and education provision for women with preterm labor. Nurs J (Manila). 2018;45(4):47–55.
19. Klomma C, Baosoung C, Sansiriphun N. Effect of social support on stress of pregnant women with preterm labor. Nurs J (Manila). 2017;44(3):9–18.
20. Park H-J, Sung M-H. Effects of music therapy on stress of preterm labor and uterine contraction in pregnant women with preterm labor. Korean J Women Health Nursing. 2017;23(2):109. doi:10.4069/kjwhn.2017.23.2.109
21. Jallo N, Cozens R. Effects of guided imagery on maternal stress during hospitalization for preterm labor. J Obstetric Gynecol Neonatal Nursing. 2011;40.
22. Jallo N, Ruiz RJ, Elswick RK, French E. Guided imagery for stress and symptom management in Pregnant African American Women. Evid Based Complement Alternat Med. 2014;2014:840923. doi:10.1155/2014/840923
23. Jallo N, Thacker LRI, Menzies V, Stojanovic P, Svikis DS. A stress coping app for hospitalized pregnant women at risk for preterm birth. Am J Maternal Child Nursing. 2017;42(5):257–262. doi:10.1097/NMC.0000000000000355
24. Tantra M, Supavititpatana B, Chaloumsuk N. Effect of imagery relaxation training on stress among pregnant women with preterm labor. Nurs J (Manila). 2020;47(3):61–72.
25. Rodrigues PB, Zambaldi CF, Cantilino A, Sougey EB. Special features of high-risk pregnancies as factors in development of mental distress: a review. Trends iPsychiatry Psychotherapy. 2016;38(3):136–140. doi:10.1590/2237-6089-2015-0067
26. Ellis A. Overcoming Destructive Beliefs, Feelings, and Behaviors. New York: Prometheus Books; 2001.
27. The Royal Thai College of Obstetricians and Gynecologists. The Management of Preterm Labour and Preterm Premature Rupture of Membrane; 2015.
28. Urech C, Fink NS, Hoesli I, Wilhelm FH, Bitzer J, Alder J. Effects of relaxation on psychobiological wellbeing during pregnancy: a randomized controlled trial. Psychoneuroendocrinology. 2010;35(9):1348–1355. doi:10.1016/j.psyneuen.2010.03.008
29. Chawanpaiboon S. Preterm Labour. Bangkok: P.A.LIVING CO., LTD.; 2010.
30. Wongpakaran N, Wongpakaran T. The Thai version of the PSS-10: an Investigation of its psychometric properties. Biopsychosoc Med. 2010;4(1):4. doi:10.1186/1751-0759-4-6
31. Chunpradub P. Relationship Between Self-Esteem, Social Support and Coping Behavior in High-Risk Pregnant Women. Nakhonpathom, Thailand: Mahidol University; 1995.
32. SPSS Inc. PASW Statistics for Windows, Version 18.0. Chicago: SPSS Inc; 2009.
33. Field A. Discovering Statistics Using IBM SPSS Statistics.
34. Chuang LL, Lin LC, Cheng PJ, Chen CH, Wu SC, Chang CL. Effects of a relaxation training programme on immediate and prolonged stress responses in women with preterm labour. J Adv Nurs. 2011;68(1):170–180. doi:10.1111/j.1365-2648.2011.05765.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Contrast-Induced Acute Kidney Injury: Evidence in Support of Its Existence and a Review of Its Pathogenesis and Management
Chaudhari H, Mahendrakar S, Baskin SE, Reddi AS
International Journal of Nephrology and Renovascular Disease 2022, 15:253-266
Published Date: 11 October 2022
Reimagining Mental Health with Artificial Intelligence: Early Detection, Personalized Care, and a Preventive Ecosystem
Mikaeili N, Naeim M, Narimani M
Journal of Multidisciplinary Healthcare 2025, 18:7355-7373
Published Date: 7 November 2025