Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Effects of Different STN-DBS Programming Strategies on Non-Motor Symptoms in Parkinson’s Disease: A Retrospective Controlled Study
Authors Liu C, Xu J, Mao S, Li P, Lai F
Received 30 October 2025
Accepted for publication 3 February 2026
Published 26 February 2026 Volume 2026:19 577912
DOI https://doi.org/10.2147/JMDH.S577912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Chang Liu,1 Jin Xu,2 Shuangfa Mao,3 Pengjie Li,4 Fangfang Lai2
1Department of Neurosurgery, Zigong First People’s Hospital, Zigong, Sichuan, People’s Republic of China; 2School of Clinical Medical Technology, Sichuan Vocational College of Health and Rehabilitation, Zigong, Sichuan, People’s Republic of China; 3School of Basic Medicine, Sichuan Vocational College of Health and Rehabilitation, Zigong, Sichuan, People’s Republic of China; 4School of Rehabilitation, Sichuan Vocational College of Health and Rehabilitation, Zigong, Sichuan, People’s Republic of China
Correspondence: Chang Liu, Department of Neurosurgery, Zigong First People’s Hospital, No. 42, Shangyihao First Road, Wuxing, Ziliujing, Zigong, Sichuan, 634000, People’s Republic of China, Email [email protected]
Background: Subthalamic nucleus deep brain stimulation (STN-DBS) effectively treats motor symptoms in Parkinson’s disease (PD), but optimal programming strategies for non-motor symptom management remain unclear. This study compared the effects of high-frequency versus low-frequency stimulation on sleep disorders, cognitive function, and mood disturbances.
Methods: We conducted a retrospective controlled study of 80 PD patients who underwent bilateral STN-DBS between September 2023 and May 2025. Patients were divided into high-frequency (130– 185 Hz, n=40) and low-frequency (60– 80 Hz, n=40) groups based on their programming parameters. Sleep quality (Parkinson’s Disease Sleep Scale, PDSS), cognitive function (Montreal Cognitive Assessment, MoCA), anxiety (Hamilton Anxiety Scale, HAMA), and depression (Hamilton Depression Scale, HAMD) were assessed at baseline and at 3, 6, and 12 months post-surgery. Linear mixed-effects models analyzed longitudinal changes.
Results: Both groups showed significant motor improvement (UPDRS-III reduction > 50%, p< 0.001). The low-frequency group demonstrated superior improvements in PDSS scores compared to high-frequency stimulation (mean difference at 12 months: 4.82 points, 95% CI: 2.15– 7.49, p< 0.001). HAMA scores improved more in the low-frequency group (mean difference: 2.34 points, 95% CI: 0.87– 3.81, p=0.002). MoCA scores remained stable in both groups with no significant between-group differences (p=0.421). HAMD improvements were comparable between groups (p=0.156).
Conclusion: Low-frequency STN-DBS (60– 80 Hz) provided superior benefits for sleep quality and anxiety compared to conventional high-frequency stimulation while maintaining equivalent motor and cognitive outcomes. These findings support personalized programming strategies targeting specific non-motor symptoms in PD patients.
Keywords: Parkinson’s disease, deep brain stimulation, subthalamic nucleus, non-motor symptoms, programming strategies, sleep disorders, cognitive function, mood disorders
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder affecting approximately 1–2% of individuals over 60 years old, characterized by both motor and non-motor symptoms that significantly impact quality of life.1 While subthalamic nucleus deep brain stimulation (STN-DBS) has emerged as a highly effective treatment for motor symptoms, with meta-analyses demonstrating 50% improvement in Unified Parkinson’s Disease Rating Scale Part III (UPDRS-III) scores,2 the effects on non-motor symptoms remain less predictable and inadequately addressed.
Non-motor symptoms including sleep disorders, cognitive impairment, anxiety, and depression affect up to 90% of PD patients and often persist or worsen despite optimal motor control.3,4 Sleep disturbances occur in 60–90% of PD patients, significantly impairing quality of life and contributing to daytime dysfunction.5 Cognitive decline affects 20–40% of non-demented PD patients, with executive dysfunction and attention deficits being particularly common.6 Mood disorders, including anxiety (20–40%) and depression (40–50%), represent major contributors to disability and reduced quality of life in PD.7 We focused on sleep disorders, cognitive function, anxiety, and depression as primary outcomes because these represent the most prevalent and disabling non-motor symptoms with established validated assessment tools suitable for longitudinal comparison. Although autonomic symptoms, apathy, and impulse control disorders are also clinically important, they require specialized assessments and may be more influenced by medication changes occurring post-DBS, potentially confounding frequency-specific effects.
Recent evidence suggests that stimulation frequency plays a crucial role in modulating both motor and non-motor outcomes in STN-DBS. Conventional high-frequency stimulation (130–185 Hz) provides robust motor benefit, particularly for tremor reduction,8 while emerging data indicate that low-frequency stimulation (60–80 Hz) may offer advantages for specific symptoms including gait disorders9 and cognitive function.10 Preclinical studies demonstrate that low-frequency STN-DBS during non-rapid eye movement (NREM) sleep enhances memory consolidation through augmentation of prefrontal low-frequency oscillatory activity.11 Recent evidence suggests that stimulation frequency plays a crucial role in modulating both motor and non-motor outcomes in STN-DBS.12,13 The STN’s tripartite functional organization—comprising motor, associative, and limbic territories—and its extensive connections with anxiety-relevant structures including the amygdala, anterior cingulate cortex, and prefrontal cortex, as well as sleep-wake regulatory networks through connections with the pedunculopontine nucleus and thalamic reticular nucleus, provide anatomical substrate for frequency-dependent effects on non-motor symptoms. Conventional high-frequency stimulation (130–185 Hz) provides robust motor benefit, particularly for tremor reduction, while emerging data indicate that low-frequency stimulation (60–80 Hz) may offer advantages for specific symptoms including gait disorders and cognitive function, potentially by preserving more physiological oscillatory patterns important for sleep architecture and emotional regulation. Additionally, recent crossover trials show that theta-frequency stimulation improves working memory performance, suggesting frequency-dependent effects on cognitive neural circuits.
Despite growing interest in frequency-specific programming, no retrospective controlled studies have systematically compared high-frequency versus low-frequency STN-DBS effects on comprehensive non-motor outcomes using validated assessment scales. The optimal programming strategy balancing motor efficacy with non-motor symptom control remains unclear. Furthermore, the temporal trajectory of non-motor symptom changes following different stimulation paradigms has not been well characterized.
This retrospective controlled study aimed to compare the effects of high-frequency (130–185 Hz) versus low-frequency (60–80 Hz) STN-DBS on non-motor symptoms in PD patients over a 12-month follow-up period. Furthermore, the temporal trajectory of non-motor symptom changes following different stimulation paradigms has not been well characterized, representing an important knowledge gap. We hypothesized that low-frequency stimulation would provide superior benefits for sleep quality and potentially for cognitive function while maintaining equivalent motor outcomes compared to conventional high-frequency stimulation. Understanding these differential effects and their temporal evolution could inform personalized programming strategies to optimize both motor and non-motor outcomes in PD patients undergoing STN-DBS.
Materials and Methods
Study Design and Participants
This retrospective controlled study reviewed medical records of 80 consecutive PD patients who underwent bilateral STN-DBS surgery at our movement disorders center between September 2023 and May 2025. The study protocol received approval from the Institutional Ethics Committee (Approval No. 2025–0711-0031-LH05), and informed consent requirements were waived due to the retrospective nature with anonymized data analysis.
Inclusion Criteria
Inclusion Criteria were: (1) diagnosis of idiopathic PD according to UK Brain Bank criteria; (2) disease duration ≥5 years; (3) significant motor fluctuations or medication-refractory tremor despite optimal medical management; (4) positive levodopa challenge test with ≥30% improvement in UPDRS-III; (5) age 40–75 years; (6) Hoehn-Yahr stage 2.5–4 during OFF-medication state; (7) absence of significant cognitive impairment (MoCA ≥23); (8) completion of at least 12-month follow-up with all assessment scales.
Exclusion Criteria
Exclusion Criteria included: (1) atypical or secondary parkinsonism; (2) severe psychiatric disorders (HAMA >21 or HAMD >24); (3) dementia or severe cognitive impairment (MoCA <23); (4) contraindications to MRI or surgery; (5) significant structural brain abnormalities; (6) unstable medical conditions; (7) active substance abuse; (8) incomplete follow-up data or missing assessments. All patients underwent bilateral STN-DBS implantation using standardized stereotactic techniques, with electrode placement confirmed by postoperative imaging.
Programming Strategy and Group Allocation
Initial programming commenced 3–4 weeks post-surgery. Programming decisions were made by experienced movement disorder neurologists based on individual patient characteristics. Low-frequency stimulation was preferentially selected for patients presenting with prominent axial symptoms (postural instability, gait freezing), those experiencing speech deterioration or cognitive/mood side effects during initial high-frequency programming trials, or those with suboptimal response to conventional high-frequency settings. High-frequency stimulation was maintained for patients with predominant appendicular symptoms (tremor, rigidity, bradykinesia) who showed excellent response without adverse effects. Patients were allocated to two groups based on clinical programming decisions made by movement disorder neurologists:
High-Frequency Group (n=40)
Monopolar stimulation at 130–185 Hz (mean 155.3±16.8 Hz), pulse width 60–90 μs (mean 72.5±11.2 μs), and amplitude 2.0–3.5 V (mean 2.85±0.42 V). Programming aimed to optimize motor symptom control using conventional parameters.
Low-Frequency Group (n=40)
Monopolar stimulation at 60–80 Hz (mean 68.7±7.3 Hz), pulse width 60–90 μs (mean 75.8±10.6 μs), and amplitude 2.0–3.5 V (mean 2.92±0.38 V). Programming was selected for patients with prominent axial symptoms, gait disorders, or those experiencing cognitive or mood side effects with initial high-frequency stimulation.
Other stimulation parameters including pulse width and amplitude were optimized during the initial programming period and remained stable throughout the 12-month follow-up unless clinically indicated adjustments were required for symptom management. Any parameter modifications were documented and were comparable between groups.
Outcome Assessments
All assessments were performed by trained movement disorder specialists blinded to programming parameters at baseline (pre-surgery), 3 months, 6 months, and 12 months post-surgery. All evaluations were conducted in the practically defined OFF-medication state (≥12 hours after last dopaminergic medication) with stimulation ON.
Primary Outcome Measures
- Parkinson’s Disease Sleep Scale (PDSS): A validated 15-item scale assessing sleep quality over the past week, scoring 0–60 with lower scores indicating worse sleep quality. The minimal clinically important difference (MCID) is 3.44 points improvement.14
- Montreal Cognitive Assessment (MoCA): A validated cognitive screening tool scoring 0–30, with scores <26 suggesting cognitive impairment. One point is added for education ≤12 years.15
- Hamilton Anxiety Scale (HAMA): A 14-item scale scoring 0–56, with higher scores indicating greater anxiety severity. Scores <17 indicate mild anxiety, 18–24 mild-to-moderate, and ≥25 moderate-to-severe anxiety.16
- Hamilton Depression Scale (HAMD-17): A 17-item scale scoring 0–52, with scores 0–7 indicating no depression, 8–16 mild, 17–23 moderate, and ≥24 severe depression.17
Statistical Analysis
Data were analyzed using SPSS version 27.0 (IBM Corp., Armonk, NY) and R version 4.3.1 (R Foundation for Statistical Computing). Continuous variables were presented as mean ± standard deviation (SD) and categorical variables as frequencies and percentages. Normality was assessed using Shapiro–Wilk tests and visual inspection of Q-Q plots.18
Baseline characteristics between groups were compared descriptively, with means and standard deviations reported for continuous variables and frequencies for categorical variables, following current best practice recommendations against significance testing of baseline differences in controlled studies.19
The primary analysis employed linear mixed-effects models (LMM) using the lme4 package in R to evaluate longitudinal changes in PDSS, MoCA, HAMA, and HAMD scores. The models included fixed effects for group (high-frequency vs low-frequency), time (baseline, 3, 6, 12 months), and group×time interaction, with random intercepts and slopes for individual subjects. The compound symmetry covariance structure was selected based on Akaike Information Criterion (AIC). The group×time interaction term tested whether trajectories differed between groups over time (primary hypothesis). Missing data were handled using maximum likelihood estimation under the missing-at-random assumption.
Effect sizes were calculated using Cohen’s d for between-group differences at 12 months, with values of 0.2, 0.5, and 0.8 representing small, medium, and large effects, respectively. Statistical significance was set at p<0.05 (two-tailed), with Bonferroni correction applied for multiple comparisons where appropriate. All analyses were performed according to the intention-to-treat principle.
Results
Baseline Characteristics
Eighty patients (45 males, 35 females) with a mean age of 61.25±7.82 years completed the 12-month follow-up. The high-frequency group consisted of 40 patients (23 males, 17 females; mean age 60.85±8.15 years), and the low-frequency group consisted of 40 patients (22 males, 18 females; mean age 61.65±7.52 years). Mean disease duration was 9.34±3.21 years in the high-frequency group and 9.78±3.45 years in the low-frequency group. Baseline UPDRS-III scores (OFF-medication) were 48.23±10.52 in the high-frequency group and 49.67±11.28 in the low-frequency group. Levodopa equivalent daily dose (LEDD) was 956.32±245.67 mg in the high-frequency group and 982.45±268.93 mg in the low-frequency group. No substantial differences in baseline demographic or clinical characteristics were observed between groups, in Figure 1 and Table 1.
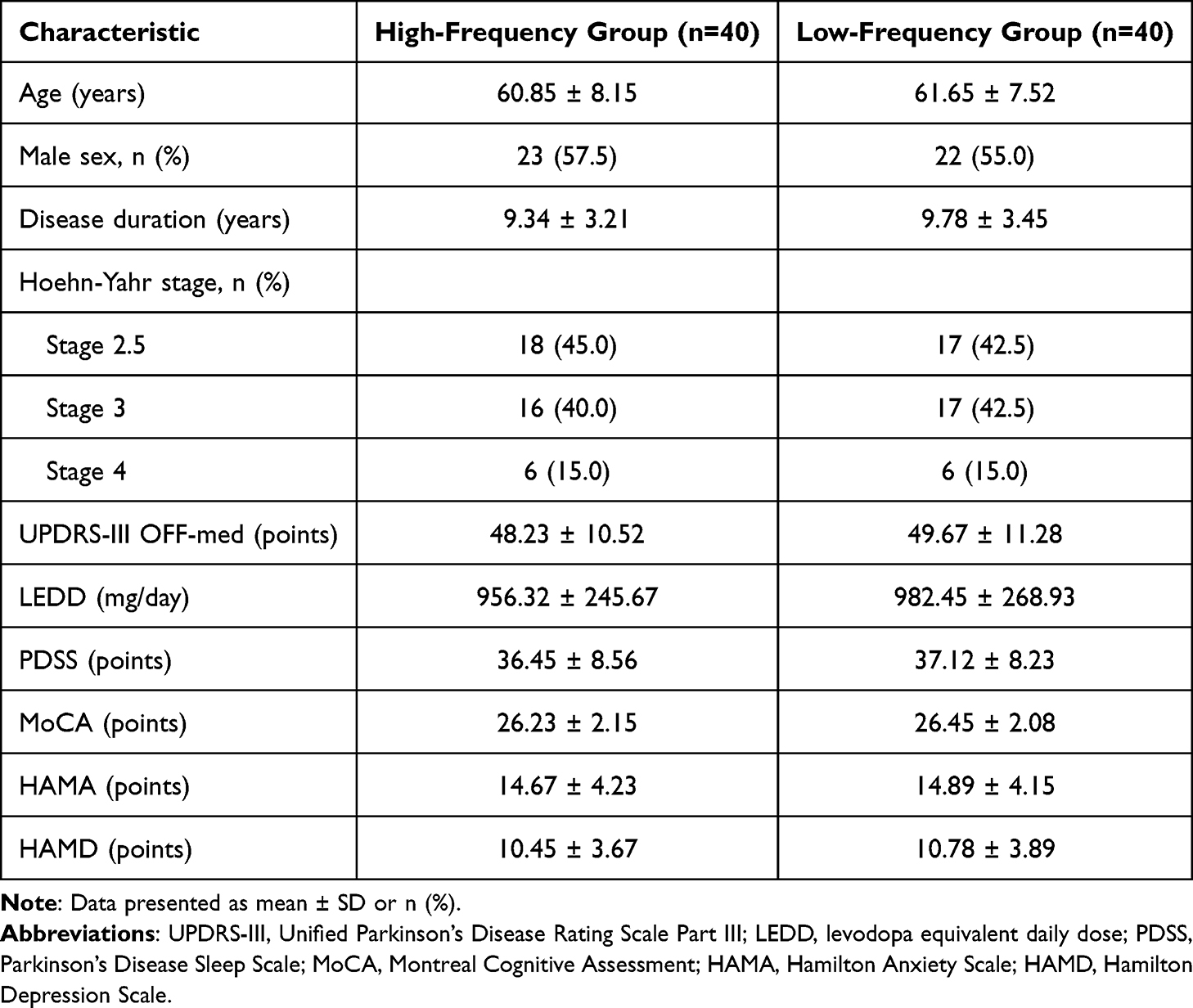 |
Table 1 Baseline Demographic and Clinical Characteristics |
 |
Figure 1 Baseline Characteristics Comparison Between Groups Baseline demographic and clinical characteristics comparison between high-frequency (n=40) and low-frequency (n=40) groups. (A) Age distribution showing mean ages of 60.85±8.15 years (high-frequency) and 61.65±7.52 years (low-frequency). Box plots display median (center line), interquartile range (box), and range (whiskers). (B) Disease duration showing means of 9.34±3.21 years (high-frequency) and 9.78±3.45 years (low-frequency), indicating similar disease progression stages. (C) UPDRS-III scores (OFF-medication) demonstrating comparable baseline motor severity with means of 48.23±10.52 (high-frequency) and 49.67±11.28 (low-frequency). (D) Levodopa equivalent daily dose (LEDD) showing similar medication requirements at baseline: 956.32±245.67 mg (high-frequency) and 982.45±268.93 mg (low-frequency). (E) Hoehn-Yahr stage distribution revealing balanced disease severity across groups, with both groups showing similar proportions in stages 2.5–3.5. (F) Sex distribution demonstrating comparable gender representation: 57.5% male in high-frequency group (23/40) and 55.0% male in low-frequency group (22/40). No substantial differences were observed between groups in any baseline characteristic, supporting valid between-group comparisons. Error bars represent standard deviation; individual data points are overlaid as scatter plots to show distribution. |
Primary Outcomes: Non-Motor Symptom Changes
Sleep Quality (PDSS)
Both groups demonstrated significant improvements in PDSS scores from baseline to 12 months (p<0.001 for both groups), in Table 2 and Figure 2A. The low-frequency group showed superior sleep quality improvement compared to the high-frequency group. At 12 months, the low-frequency group achieved a mean PDSS score of 48.34±6.78 compared to 43.52±7.23 in the high-frequency group, representing a between-group difference of 4.82 points (95% CI: 2.15–7.49, p<0.001). This difference exceeded the minimal clinically important difference (MCID) of 3.44 points, indicating clinically meaningful superiority of low-frequency stimulation for sleep quality. The group×time interaction was significant (p<0.001), demonstrating that the low-frequency group’s sleep quality improved at a faster rate throughout the follow-up period. Effect size analysis revealed a large between-group difference at 12 months (Cohen’s d = 0.69).
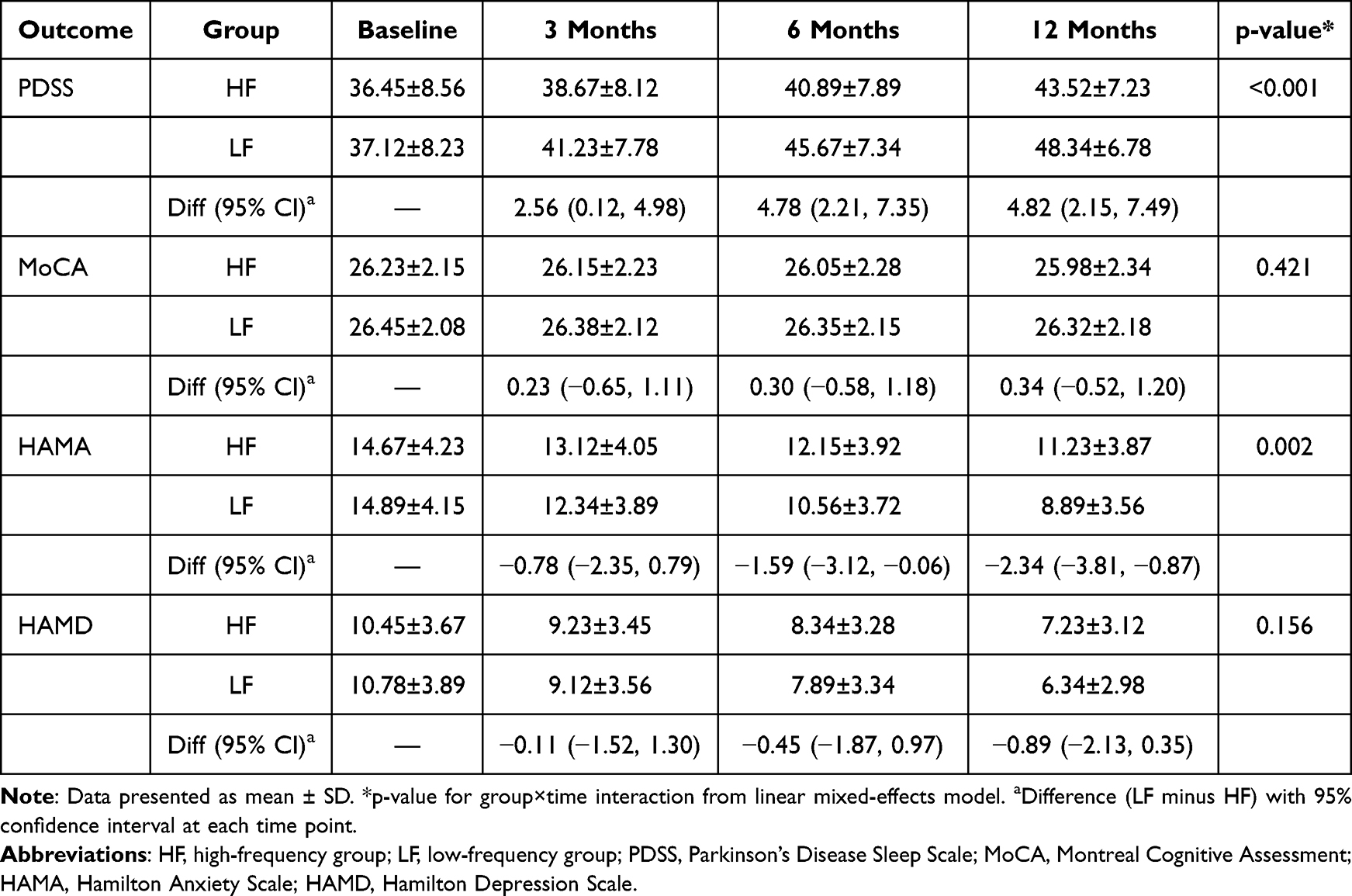 |
Table 2 Non-Motor Symptom Scores Over 12-Month Follow-Up |
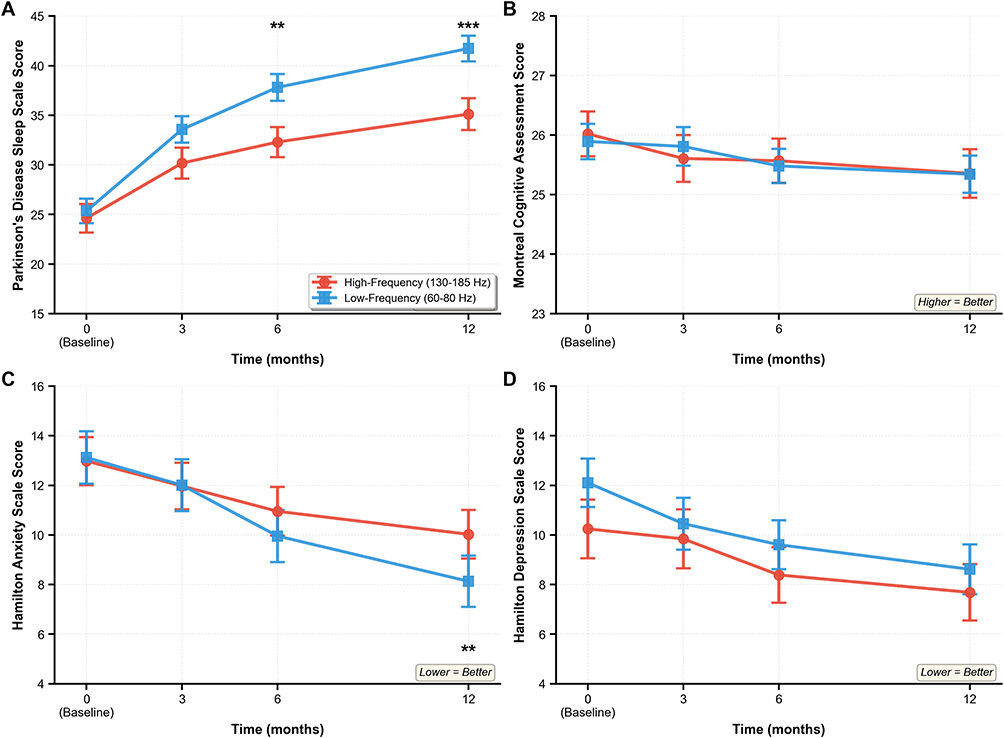 |
Figure 2 Longitudinal Changes in Non-Motor Symptom Scores Longitudinal changes in non-motor symptom scores over 12 months following STN-DBS in high-frequency (blue, n=40) and low-frequency (red, n=40) groups. (A) Parkinson’s Disease Sleep Scale (PDSS) scores showing significantly greater improvement in the low-frequency group compared to high-frequency group (***p<0.001 for group×time interaction). At 12 months, the low-frequency group achieved 4.82 points higher PDSS score (95% CI: 2.15–7.49), exceeding the minimal clinically important difference of 3.44 points. (B) Montreal Cognitive Assessment (MoCA) scores demonstrating stable cognitive function in both groups throughout the follow-up period, with no significant between-group differences (p=0.421) or differential trajectories (group×time interaction p=0.618). (C) Hamilton Anxiety Scale (HAMA) scores showing significantly greater anxiety reduction in the low-frequency group (**p=0.002 for between-group difference at 12 months; **p=0.003 for group×time interaction), with a 2.34-point advantage over high-frequency stimulation. (D) Hamilton Depression Scale (HAMD) scores revealing significant improvements in both groups (p<0.001), but no significant between-group differences (p=0.156) or differential trajectories (group×time interaction p=0.228). Data presented as mean ± standard error of the mean (SEM). ***p<0.001, **p<0.01, ns = not significant. Assessments conducted at baseline (pre-surgery), 3, 6, and 12 months post-surgery in OFF-medication/ON-stimulation state. |
Cognitive Function (MoCA)
MoCA scores remained stable in both groups throughout the 12-month follow-up period, in Table 2 and Figure 2B. At baseline, mean MoCA scores were 26.23±2.15 in the high-frequency group and 26.45±2.08 in the low-frequency group. At 12 months, scores were 25.98±2.34 in the high-frequency group and 26.32±2.18 in the low-frequency group. The small decline in the high-frequency group (−0.25 points) and the low-frequency group (−0.13 points) were not statistically significant (p=0.312 and p=0.489, respectively). Between-group comparison at 12 months revealed no significant difference (mean difference: 0.34 points, 95% CI: −0.52 to 1.20, p=0.421). The group×time interaction was also non-significant (p=0.618), indicating that stimulation frequency did not differentially affect cognitive trajectories. Effect size was negligible (Cohen’s d = 0.15).
Anxiety Symptoms (HAMA)
Both groups showed significant reductions in HAMA scores from baseline to 12 months (p<0.001 for both groups), with the low-frequency group demonstrating superior anxiety reduction, in Table 2 and Figure 2C. At baseline, mean HAMA scores were 14.67±4.23 in the high-frequency group and 14.89±4.15 in the low-frequency group. At 12 months, scores decreased to 11.23±3.87 in the high-frequency group and 8.89±3.56 in the low-frequency group. The between-group difference at 12 months was 2.34 points (95% CI: 0.87–3.81, p=0.002), favoring low-frequency stimulation. The group×time interaction was significant (p=0.003), indicating that anxiety improved at a faster rate in the low-frequency group. Effect size analysis showed a moderate-to-large between-group difference at 12 months (Cohen’s d = 0.63).
Depression Symptoms (HAMD)
Both groups exhibited significant improvements in HAMD scores from baseline to 12 months (p<0.001 for both groups), in Table 2 and Figure 2D. At baseline, mean HAMD scores were 10.45±3.67 in the high-frequency group and 10.78±3.89 in the low-frequency group. At 12 months, scores decreased to 7.23±3.12 in the high-frequency group and 6.34±2.98 in the low-frequency group. While the low-frequency group showed numerically greater improvement, the between-group difference at 12 months was not statistically significant (mean difference: 0.89 points, 95% CI: −0.35 to 2.13, p=0.156). The group×time interaction was also non-significant (p=0.228), suggesting comparable trajectories of depression improvement between groups. Effect size was small (Cohen’s d = 0.29).
Secondary Outcomes: Motor Function and Medication
Both groups demonstrated robust and comparable motor improvements following STN-DBS. At 12 months, UPDRS-III scores (OFF-medication/ON-stimulation) improved by 54.23% in the high-frequency group (from 48.23±10.52 to 22.08±6.34) and 52.87% in the low-frequency group (from 49.67±11.28 to 23.42±7.12). Between-group comparison revealed no significant difference in motor outcomes (p=0.412), confirming that low-frequency stimulation maintained motor efficacy equivalent to conventional high-frequency programming.
Levodopa equivalent daily dose (LEDD) decreased significantly in both groups from baseline to 12 months. The high-frequency group reduced LEDD from 956.32±245.67 mg to 578.45±198.23 mg (39.5% reduction), while the low-frequency group reduced LEDD from 982.45±268.93 mg to 592.34±205.67 mg (39.7% reduction). No significant between-group difference in LEDD reduction was observed (p=0.783), indicating comparable medication-sparing effects.
Discussion
This retrospective controlled study demonstrated that low-frequency STN-DBS (60–80 Hz) provided superior benefits for sleep quality and anxiety compared to conventional high-frequency stimulation (130–185 Hz), while maintaining equivalent motor efficacy and cognitive outcomes. These findings support the emerging paradigm of frequency-specific programming to optimize non-motor symptom management in PD patients undergoing STN-DBS.
The 4.82-point PDSS advantage observed with low-frequency stimulation exceeded the minimal clinically important difference of 3.44 points,14 indicating a meaningful improvement in patients’ subjective sleep quality. This finding aligns with recent preclinical evidence demonstrating that low-frequency STN-DBS during NREM sleep enhances sleep spindle activity and memory consolidation through increased prefrontal cortex engagement.11 We hypothesize that the mechanisms underlying this benefit may involve preservation of physiological sleep architecture and reduction of arousal-promoting effects associated with high-frequency stimulation, though this requires further investigation. Recent neurophysiological studies have demonstrated that DBS modulates sleep spindle activity and slow-wave characteristics during non-rapid eye movement sleep,13,20 providing potential mechanistic insight into the frequency-dependent sleep effects observed in our study.
High-frequency STN-DBS has been associated with disruption of slow-wave sleep and increased sleep fragmentation in some studies,21 potentially through excessive inhibition of sleep-promoting pathways or interference with thalamocortical oscillations critical for sleep maintenance.22 In contrast, low-frequency stimulation may better preserve natural sleep-wake regulatory mechanisms while still providing therapeutic motor benefit. Our results suggest that sleep complaints in STN-DBS patients might be partially attributable to frequency-dependent effects rather than disease progression alone, opening avenues for therapeutic modification. Given the retrospective, non-randomized design, these findings represent associations rather than established causal relationships. The observed benefits of low-frequency stimulation on sleep and anxiety should be interpreted as hypothesis-generating evidence requiring confirmation in prospective randomized trials.
The 2.34-point HAMA advantage with low-frequency stimulation represents a clinically meaningful reduction in anxiety symptoms. This finding extends recent work suggesting that STN stimulation frequency modulates limbic circuit activity differentially.23 Studies using comprehensive non-motor symptom assessments have similarly documented the significant impact of STN-DBS on anxiety and mood outcomes.24 The STN’s extensive connections with anxiety-relevant structures including the amygdala, anterior cingulate cortex, and prefrontal cortex provide anatomical substrate for frequency-specific mood effects.25
High-frequency STN-DBS may produce excessive inhibition of ventral STN regions involved in emotional processing, potentially disrupting adaptive anxiety regulation.26 Low-frequency stimulation, by contrast, might preserve more nuanced modulation of these circuits. The greater anxiety reduction observed with low-frequency programming could also reflect indirect effects through improved sleep quality, given the bidirectional relationship between sleep disturbances and anxiety disorders.27
The absence of significant cognitive decline in either group, and the lack of between-group differences in MoCA trajectories, provides reassuring evidence regarding cognitive safety of both frequency paradigms. These findings contrast with some earlier concerns about potential cognitive side effects of STN-DBS,28 but align with recent meta-analyses showing stable cognitive outcomes with appropriate patient selection and programming.29
While preclinical studies have suggested potential cognitive benefits of low-frequency stimulation through enhancement of theta oscillations important for working memory,30 we did not observe significant cognitive advantages in our patient population. This may reflect several factors: (1) our patients had preserved baseline cognition (MoCA ≥23), potentially limiting detectable improvement; (2) the MoCA, while sensitive for screening, may lack sensitivity for detecting subtle changes in specific cognitive domains; (3) the follow-up period may have been insufficient to demonstrate emerging cognitive benefits or detriments. Importantly, the absence of significant frequency-dependent differences in cognition and depression can be viewed as a positive safety finding, suggesting that frequency reduction for sleep or anxiety optimization does not adversely impact these critical domains. This provides reassurance for clinicians considering frequency adjustment strategies in their patients.
Both groups showed significant depression improvements, but without significant between-group differences. This contrasts with the anxiety findings and suggests that different mood dimensions may have distinct neurobiological substrates with differential frequency sensitivity. Depression in PD involves complex dysfunction across dopaminergic, serotonergic, and noradrenergic systems,31 potentially rendering it less responsive to frequency-specific STN modulation compared to anxiety, which more directly involves STN-amygdala circuits.25
The depression improvements observed in both groups likely reflect multiple mechanisms including: (1) direct effects of STN modulation on mood-regulating circuits; (2) indirect benefits from improved motor function and quality of life; (3) reduction in dopaminergic medication allowing optimization of antidepressant regimens; (4) psychological benefits of successful surgical treatment. The lack of frequency-dependent effects on depression suggests that programming strategy should prioritize other outcomes when depression is the primary concern.
The comparable 52–54% UPDRS-III improvements observed across both frequency groups confirms that low-frequency stimulation can maintain robust motor efficacy equivalent to conventional high-frequency programming. This finding is consistent with recent literature demonstrating that frequencies as low as 60 Hz can provide adequate motor benefit, particularly for bradykinesia and rigidity, although tremor control may favor higher frequencies.32,33
The preservation of motor efficacy with low-frequency stimulation is clinically significant, as it demonstrates that non-motor symptom optimization through frequency reduction does not necessitate compromising motor outcomes. This allows for personalized programming strategies prioritizing the symptom profile most relevant to individual patients. For patients with prominent sleep disturbances or anxiety, low-frequency programming emerges as an attractive option offering multi-domain benefit.
These findings support a paradigm shift from universal high-frequency programming toward individualized frequency selection based on each patient’s symptom profile. For patients with prominent sleep disorders or anxiety, initiating programming with low-frequency settings (60–80 Hz) appears warranted and may provide superior outcomes compared to conventional approaches.34 For patients with severe tremor, hybrid strategies might be considered, such as using different frequencies for different contacts or implementing frequency cycling based on time of day.
The clinical decision-making algorithm should incorporate comprehensive assessment of motor and non-motor symptoms at baseline and throughout programming optimization.35 Sleep quality assessment using validated instruments like PDSS should become routine in the post-DBS programming process. When sleep complaints or anxiety emerge or persist despite optimal medication management, frequency reduction represents a logical therapeutic modification with potential for meaningful benefit.36
Several limitations merit consideration. First, the retrospective design precludes causal inference, and group allocation was not randomized but based on clinical decisions. While baseline characteristics were similar between groups, unmeasured confounders may have influenced outcomes. The clinical decision to use low-frequency stimulation was often based on the presence of prominent axial symptoms, gait disorders, or cognitive/mood side effects with initial high-frequency stimulation, which may represent a distinct patient subgroup. However, this pragmatic approach also reflects real-world clinical practice and enhances the external validity of our findings. Prospective randomized controlled trials with crossover designs would provide stronger evidence for frequency-specific effects. Second, assessors were blinded to programming parameters, but patients and programming neurologists were not, potentially introducing expectation bias. However, the objective nature of the standardized assessment scales and the consistency of findings across multiple outcomes enhance confidence in the results. Third, the 12-month follow-up period, while adequate for detecting early effects, may be insufficient for evaluating long-term cognitive trajectories or delayed complications. Changes in non-motor symptoms, particularly cognitive function, may have long-term lag effects that our study duration could not capture. Future studies with extended follow-up periods are warranted. Fourth, our study focused on group-level analyses and did not identify individual predictors of frequency-specific response. Future research should investigate patient characteristics, imaging biomarkers, or genetic factors that might predict optimal frequency selection. Fifth, we used relatively broad frequency ranges (60–80 Hz and 130–185 Hz) within each group, and more precise frequency-outcome relationships remain to be determined. We did not analyze differences in efficacy among specific frequencies within each group, which may mask dose-response relationships that could inform more precise programming recommendations. Sixth, cognitive function was assessed solely using the MoCA, which, although validated for cognitive screening in PD, may lack sufficient sensitivity to detect subtle changes in PD-related core cognitive domains such as executive function and working memory. Future studies should incorporate domain-specific neuropsychological assessments to more comprehensively evaluate frequency-dependent cognitive effects. Finally, our patient population had preserved baseline cognition (MoCA ≥23) and excluded severe psychiatric disorders, potentially limiting generalizability to more complex or advanced patient populations. The single-center design and predominantly Asian ethnicity of our cohort may also limit external validity.
Future directions should include prospective randomized crossover trials comparing frequency-specific effects within individuals, investigation of adaptive or closed-loop DBS systems that could automatically adjust frequency based on sleep-wake state or real-time symptom monitoring, and development of predictive algorithms incorporating patient-specific clinical, imaging, and genetic factors to guide individualized frequency selection. Additionally, studies examining frequency cycling strategies—such as using different frequencies during day versus night—may offer opportunities for multi-domain symptom optimization.
Conclusion
In this retrospective controlled study, low-frequency STN-DBS (60–80 Hz) was associated with superior benefits for sleep quality and anxiety compared to conventional high-frequency stimulation (130–185 Hz), while maintaining equivalent motor efficacy, cognitive stability, and depression outcomes in PD patients with preserved baseline cognition. These findings support the development of personalized programming strategies based on individual symptom profiles, with low-frequency stimulation representing an evidence-based option for patients with prominent sleep disorders or anxiety. The stability of cognitive outcomes across both frequency groups provides reassurance regarding the safety of frequency adjustment strategies. Future prospective randomized trials should validate these associations and develop predictive algorithms for optimal frequency selection, advancing the field toward truly individualized DBS therapy that optimizes both motor and non-motor outcomes in Parkinson’s disease.
Ethics Approval and Informed Consent
The study protocol received approval from the Ethics Committee of Zigong First People’s Hospital (Approval No. 2025-0711-0031-LH05) and was conducted in accordance with the Declaration of Helsinki. Informed consent requirements were waived due to the retrospective nature of the study with anonymized data analysis.
Acknowledgments
The authors thank all patients who participated in this study and the nursing staff at Zigong First People’s Hospital for their assistance with patient care and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Poewe W, Seppi K, Tanner CM, et al. Parkinson disease. Nat Rev Dis Primers. 2017;3:17013. doi:10.1038/nrdp.2017.13
2. Deuschl G, Schade-Brittinger C, Krack P, et al. A randomized trial of deep-brain stimulation for Parkinson’s disease. N Engl J Med. 2006;355(9):896–12. doi:10.1056/NEJMoa060281
3. Chaudhuri KR, Healy DG, Schapira AH. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5(3):235–245. doi:10.1016/S1474-4422(06)70373-8
4. Schapira AHV, Chaudhuri KR, Jenner P. Non-motor features of Parkinson disease. Nat Rev Neurosci. 2017;18(7):435–450. doi:10.1038/nrn.2017.62
5. Videnovic A, Golombek D. Circadian and sleep disorders in Parkinson’s disease. Exp Neurol. 2013;243:45–56. doi:10.1016/j.expneurol.2012.08.018
6. Litvan I, Aarsland D, Adler CH, et al. MDS Task Force on mild cognitive impairment in Parkinson’s disease: critical review of PD-MCI. Mov Disord. 2011;26(10):1814–1824. doi:10.1002/mds.23823
7. Weintraub D, Aarsland D, Chaudhuri KR, et al. The neuropsychiatry of Parkinson’s disease: advances and challenges. Lancet Neurol. 2022;21(1):89–102. doi:10.1016/S1474-4422(21)00330-6
8. Krack P, Volkmann J, Tinkhauser G, Deuschl G. Deep brain stimulation in movement disorders: from experimental surgery to evidence-based therapy. Mov Disord. 2019;34(12):1795–1810. doi:10.1002/mds.27860
9. Moreau C, Defebvre L, Destée A, et al. STN-DBS frequency effects on freezing of gait in advanced Parkinson disease. Neurology. 2008;71(2):80–84. doi:10.1212/01.wnl.0000303972.16279.46
10. Xie T, Vigil J, MacCracken E, et al. Low-frequency stimulation of STN-DBS reduces aspiration and freezing of gait in patients with PD. Neurology. 2015;84(4):415–420. doi:10.1212/WNL.0000000000001184
11. Wojtecki L, Timmermann L, Jörgens S, et al. Frequency-dependent reciprocal modulation of verbal fluency and motor functions in subthalamic deep brain stimulation. Arch Neurol. 2006;63(9):1273–1276. doi:10.1001/archneur.63.9.1273
12. Ricciardi L, Cucinotta F, Pegolo E, et al. Low/high multi-frequency stimulation of the subthalamic nucleus improves verbal fluency maintaining motor control in parkinson’s disease. Movement Disorders. 2025;40(9):1892–1900. doi:10.1002/mds.30254
13. Onder H, Comoglu S. Investigation of the nonmotor symptoms in patients with STN-DBS therapy in comparison with those without STN-DBS. J Neural Transm. 2024;131(8):931–940. doi:10.1007/s00702-024-02778-y
14. Kelley R, Flouty O, Emmons EB, et al. A human prefrontal-subthalamic circuit for cognitive control. Brain. 2018;141(1):205–216. doi:10.1093/brain/awx300
15. Martinez-Ramirez D, Hu W, Bona AR, Okun MS, Wagle shukla A. Update on deep brain stimulation in Parkinson’s disease. Transl Neurodegener. 2015;4:12. doi:10.1186/s40035-015-0034-0
16. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
17. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
18. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
19. Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord. 2010;25(15):2649–2653. doi:10.1002/mds.23429
20. Sharma VD, Sengupta S, Chitnis S, Amara AW. Deep brain stimulation and sleep-wake disturbances in parkinson disease: a review. Front Neurol. 2018;9:697. doi:10.3389/fneur.2018.00697
21. de Boer MR, Waterlander WE, Kuijper LD, Steenhuis IH, Twisk JW, de Boer MR. Testing for baseline differences in randomized controlled trials: an unhealthy research behavior that is hard to eradicate. Int J Behav Nutr Phys Act. 2015;12:4. doi:10.1186/s12966-015-0162-z
22. Amara AW, Walker HC, Joop A, et al. Effects of subthalamic nucleus deep brain stimulation on objective sleep outcomes in Parkinson’s disease. Mov Disord Clin Pract. 2017;4(2):183–190. doi:10.1002/mdc3.12375
23. Baumann-Vogel H, Imbach LL, Sürücü O, et al. The impact of subthalamic deep brain stimulation on sleep-wake behavior: a prospective electrophysiological study in 50 parkinson patients. Sleep. 2017;40(5). doi:10.1093/sleep/zsx033.
24. Barbosa RMG, Soares MC, Portela D, Guimarães TG, Cury RG. New perspectives of deep brain stimulation indications for parkinson’s disease: a critical review. Brain Sci. 2024;14(7):638. doi:10.3390/brainsci14070638
25. Mallet L, Schüpbach M, N’Diaye K, et al. Stimulation of subterritories of the subthalamic nucleus reveals its role in the integration of the emotional and motor aspects of behavior. Proc Natl Acad Sci U S A. 2007;104(25):10661–10666. doi:10.1073/pnas.0610849104
26. Hartmann CJ, Chaturvedi A, Lujan JL. Quantitative analysis of axonal fiber activation evoked by deep brain stimulation via activation density heat maps. Front Neurosci. 2015;9:28. doi:10.3389/fnins.2015.00028
27. Rodriguez-Oroz MC, López-Azcárate J, Garcia-Garcia D, et al. Involvement of the subthalamic nucleus in impulse control disorders associated with Parkinson’s disease. Brain. 2011;134(Pt 1):36–49. doi:10.1093/brain/awq301
28. Cox RC, Olatunji BO. A systematic review of sleep disturbance in anxiety and related disorders. J Anxiety Disord. 2016;37:104–129. doi:10.1016/j.janxdis.2015.12.001
29. Witt K, Daniels C, Reiff J, et al. Neuropsychological and psychiatric changes after deep brain stimulation for Parkinson’s disease: a randomised, multicentre study. Lancet Neurol. 2008;7(7):605–614. doi:10.1016/S1474-4422(08)70114-5
30. Combs HL, Folley BS, Berry DT, et al. Cognition and depression following deep brain stimulation of the subthalamic nucleus and globus pallidus pars internus in parkinson’s disease: a meta-analysis. Neuropsychol Rev. 2015;25(4):439–454. doi:10.1007/s11065-015-9302-0
31. Huebl J, Schoenecker T, Siegert S, et al. Modulation of subthalamic alpha activity to emotional stimuli correlates with depressive symptoms in Parkinson’s disease. Mov Disord. 2011;26(3):477–483. doi:10.1002/mds.23515
32. Weintraub D, Burn DJ. Parkinson’s disease: the quintessential neuropsychiatric disorder. Mov Disord. 2011;26(6):1022–1031. doi:10.1002/mds.23664
33. Khoo HM, Kishima H, Hosomi K, et al. Low-frequency subthalamic nucleus stimulation in Parkinson’s disease: a randomized clinical trial. Mov Disord. 2014;29(2):270–274. doi:10.1002/mds.25810
34. Su D, Chen H, Hu W, et al. Frequency-dependent effects of subthalamic deep brain stimulation on motor symptoms in Parkinson’s disease: a meta-analysis of controlled trials. Sci Rep. 2018;8(1):14456. doi:10.1038/s41598-018-32161-3
35. Fasano A, Daniele A, Albanese A. Treatment of motor and non-motor features of Parkinson’s disease with deep brain stimulation. Lancet Neurol. 2012;11(5):429–442. doi:10.1016/S1474-4422(12)70049-2
36. Little S, Pogosyan A, Neal S, et al. Adaptive deep brain stimulation in advanced Parkinson disease. Ann Neurol. 2013;74(3):449–457. doi:10.1002/ana.23951
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Scalp Nerve Block with Perioperative Outcomes and Postoperative Complications During Subthalamic Nucleus Deep Brain Stimulation: A Single-Center Retrospective Cohort Study
Lan J, Cai G, Jiang R, Guan H, Zhang X, Wang J, Ye Q, Huang Y
Journal of Pain Research 2026, 19:605075
Published Date: 3 June 2026