")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Effects of Different Injection Rates of Propofol on Postoperative Cognition in Elderly Patients Undergoing Laparoscopic Inguinal Hernia Repair
Authors Li T, Han W, Yang X , Wang Y, Peng L, He L, Hu L, Liu J, Xia M, Wang S
Received 22 February 2023
Accepted for publication 6 June 2023
Published 13 June 2023 Volume 2023:17 Pages 1741—1752
DOI https://doi.org/10.2147/DDDT.S407905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Tingting Li,1,2 Wenjing Han,1,2 Xinlu Yang,1 Yu Wang,1 Li Peng,1 Lingwei He,1 Lianjia Hu,1 Jiayuan Liu,1 Min Xia,1 Sheng Wang1,2
1Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 2Department of Anesthesiology, Anhui Provincial Hospital Affiliated to Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Sheng Wang, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, No. 17 Lujiang Road, Luyang District, Hefei, Anhui Province, People’s Republic of China, Tel +86 191 5600 7726, Email [email protected]
Purpose: This study aimed to explore the effects of different injection rates of propofol on postoperative cognition in elderly patients undergoing laparoscopic inguinal hernia repair.
Methods: A total of 180 elderly patients who planned to undergo laparoscopic inguinal hernia repair were randomly divided into three groups: slow injection of propofol (VS-Group, 30 mg kg− 1 h− 1); medium injection of propofol (VM-Group, 100 mg kg− 1 h− 1) or fast injection of propofol (VF-Group, 300 mg kg− 1 h− 1). Propofol was induced by microinfusion pump, and the depth of anesthesia was monitored by bispectral index (BIS). Propofol and remifentanil were continuously infused during anesthesia maintenance and adjusted according to BIS. The primary outcome was the use of the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) to measure the incidence of postoperative cognitive decline (POCD) in elderly patients on the first and seventh postoperative day. Secondary outcomes included induced dose of propofol, incidence of burst suppression and maximum electroencephalographic (EEG) effect of propofol (BIS-min) during induction.
Results: The incidence of POCD on the first and seventh day postoperatively was similar among the three groups (P > 0.05). However, with the increase of propofol injection rate, induced dose of propofol, incidence of burst suppression and BIS-min during induction, the number of patients requiring vasoactive agents were significantly increased (P < 0.001). Multivariate regression analysis showed that the brief duration of burst suppression during induction did not affect the occurrence of POCD, while age and duration of hospitalization were risk factors for POCD.
Conclusion: For elderly patients undergoing laparoscopic inguinal hernia repair, lowering the injection rate of propofol (such as 30 mg kg− 1 h− 1) cannot decrease the incidence of early POCD, but reduces induction dose of propofol and use of vasoactive drugs, making the patient’s hemodynamics more stable.
Keywords: propofol, injection rate, bispectral index, burst suppression, elderly, postoperative cognitive decline
Introduction
As the world ages, the number of surgical procedures performed in elderly patients has rapidly increased. POCD is a common complication after anesthesia in elderly patients.1 POCD is characterized by acute or persistent impairment of attention, concentration, learning, and memory after surgery.2 The occurrence of POCD is associated with decreased quality of life, increased the long-term mortality, and significantly increased use of medical resources.3–5 This prompted us to explore anesthetic interventions that could help reduce the incidence of POCD.
Despite extensive research in recent years, the causes and pathophysiological mechanisms underlying postoperative cognitive decline remain unclear. The underlying mechanism of POCD may involve a combination of surgical, patient, and anesthetic factors.6,7 Traumatic stimuli after major surgery may activate the release of nuclear factor (NF)-κB and cytokines, thereby impairing the integrity of the blood–brain barrier. Age is an independent risk factor for POCD.8,9 Intraoperative EEG monitoring in high-risk patients with cognitive impairment can promote early postoperative cognitive recovery.10 BIS has been widely used in clinical practice as the earliest tool for monitoring the depth of anesthesia. Propofol is a commonly used intravenous anesthetic owing to its rapid onset and recovery time. Studies have shown that BIS is closely related to propofol and can accurately reflect the depth of sedation.11,12 The maximum EEG effect of propofol in patients increased with increasing rate of propofol injection.13 This may also lead to differences in the incidence of burst suppression. However, the incidence and duration of intraoperative EEG burst suppression are associated with early postoperative cognitive decline.14,15 A dose-dependent decrease in systemic vascular resistance with propofol causes hypotension and cerebral hypoperfusion.16,17 These factors may affect the early POCD in patients.
In clinical practice, the anesthesiologist can freely choose the rate of anesthesia injection for the patient. However, there is currently no relevant research on the effect of propofol injection rates on the early postoperative cognition in elderly patients. Therefore, we conducted a randomized controlled trial to compare the effect of propofol injection rate on early postoperative cognition in elderly patients undergoing laparoscopic inguinal hernia repair.
Materials and Methods
Study Design and Study Population
The trial was approved by the Ethics Committee of the Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital) (Ethics Approval Number: 2021 KY-081 Anhui, China), and was registered in the Chinese Clinical Trial Registry (ChiCTR2000040005) on November 18, 2020. The inclusion criteria were as follows: age 60–90 years, American Society of Anesthesiologists (ASA) physical status II–III, education level sufficient to complete neuropsychological tests, voluntary participation in this study and signed informed consent. The exclusion criteria were obesity (body mass index >28 kg m−2), allergy to the anesthetics used, history of cerebrovascular disease in the last 3 months, liver and kidney dysfunction, history of mental illness or taking psychotropic drugs, recent alcohol abuse, language communication difficulties, significant hearing or visual impairment, and preoperative Mini-Mental State Examination score <24. Patients who required more than the standard dose of propofol (2.5 mg kg−1) during anesthesia induction, experienced burst suppression during anesthesia maintenance and declined postoperative follow-up were not included in the final statistical analysis.
Randomization
Elderly patients who underwent laparoscopic inguinal hernia repair in our hospital from May to November 2021 were enrolled in this prospective randomized single-blind clinical trial. The patients were randomly divided into three groups at a 1:1:1 proportion using random number table: Vs-Group (the induction rate of propofol was 30 mg kg−1 h−1); VM-Group (the induction rate of propofol was 100 mg kg−1 h−1) or VF-Group (the induction rate of propofol was 300 mg kg−1 h−1). The assigned numbers are wrapped in opaque envelopes that can only be seen by the anesthesiologist in charge of the patient’s anesthesia. Patients, outcome evaluators, and data information analysts were blinded to trial intervention.
Anesthesia and Perioperative Care
None of the patients had received premedication. After entering the operating room, routine continuous monitoring was performed (Mindray, Shenzhen, China), including blood pressure, electrocardiography, pulse oxygen saturation (SpO2), and bispectral index (BIS Covidien IIC, USA). The direction of electroencephalogram electrode sticking was determined by tossing a coin. Before anesthesia, the peripheral veins of the upper extremities were opened and balanced crystalloid solutions (5–7 mL kg−1) were infused at a rate of 5–7 mL kg−1 h−1 until anesthesia induction. Anesthesia was induced after preoxygenation for at least 3 minutes. Anesthesia induction with propofol was accomplished by an anesthesiologist responsible for the patient’s anesthesia using a microinfusion pump. Propofol was stopped when BIS value dropped to 60. If the dose of propofol exceeds 2.5 mL kg−1 and BIS value is still greater than 60, propofol was stopped. Within 2 min, if BIS value did not decrease but increased, additional propofol of 0.5 mg kg−1 time−1 was administered for remediation until the BIS value was ≤60. Then, sufentanil 0.4 µg kg−1 and rocuronium 0.6 mL kg−1 were administered. Endotracheal intubation and mechanical ventilation were performed after muscle relaxation was satisfactory. and BIS value was less than 50. During the operation, the end-tidal carbon dioxide pressure (PetCO2) was maintained at 35–45 mmHg.
Intraoperative anesthesia was maintained with propofol 4–8 mL kg−1 h−1, remifentanil 0.1–0.3 μg kg−1 min−1 continuous intravenous pumping. BIS value was maintained between 40 and 60. At the end of pneumoperitoneum, all anesthetics were stopped and all patients in all three groups were given intravenous flurbiprofen axetil 100 mg and ondansetron 4 mg and then sent to the post-anesthesia unit (PACU). The tracheal tube was removed after spontaneous breathing resumed. If the Steward score (mainly from the degree of consciousness, respiratory tract patency, and limb activity of the three indicators; each index is 0–2 points, with the highest score of 6 points) is greater than 4, patients can be sent back to the ward. During the postoperative period, flurbiprofen axetil (50 mg) was given intravenously when the VAS score was above 3.
Perioperative heart rate (HR) was maintained at 50–100 beats min−1; If HR < 50 beats min−1, atropine (0.3–0.5 mg) was administered; If HR > 100 beats min−1, esmolol (0.3–0.6 mg kg−1) is given. If systolic blood pressure increases or decreases by 10% from baseline, nicardipine (5–10 μg kg−1) and norepinephrine (0.1–0.2 μg kg−1 min−1) are given. Ephedrine (3–6 mg) should be given if blood pressure and heart rate are low. Intraoperative midazolam, dexmedetomidine, and inhalation anesthetics were avoided, and there were no restrictions on the use of muscle relaxants and vasoactive drugs. As propofol is widely used in clinical practice, this study did not establish a clinical data safety monitor.
Data Collection
The main outcome measure of this study was the incidence of early POCD in the three groups of patients. We simultaneously collected data at the following time points: the time from propofol injection to the declining of BIS value, the time for BIS value dropped to 60, the induction dose of propofol, the BIS-min and the incidence of burst suppression during induction of anesthesia, the number of patients with hypotension, anesthesia and surgery duration, and duration of hospitalization. In this study, burst suppression was defined if the burst suppression ratio (SR) was greater than zero and was observed 15 minutes after induction of anesthesia. The mean arterial pressure (MAP) and heart rate (HR) were recorded at baseline, 5 minutes after anesthesia induction, 5 min after surgery begin and 5 min after surgery end. Blood samples were collected at baseline, 5 min after anesthesia induction, 30 min and 24 h after surgery to determine the concentrations of interleukin (IL)-6, IL-10, S100β, and tumor necrosis factor (TNF)-α.
Cognitive Function Measurement
Cognitive function was assessed by a trained investigator on the day before surgery and on the first and seventh days after surgery. Cognitive tests were performed in a quiet room with only the patient and the investigator. The same investigator performed the tests for each patient. The researchers were unaware of the patient grouping. We used the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) to assess changes in cognitive function in elderly patients. These two scales were chosen for practical reasons owing to their relative simplicity, short time consumption, high patient compliance, and members of the research group were familiar with the MMSE and MoCA. A patient was considered to have POCD if the scores on both scales decreased by 1 SD (standard deviation) from the preoperative level.
Cognitive test scales included the following: (1) the MMSE scale, which is the most commonly used rapid screening tool for clinical cognitive dysfunction, with a high sensitivity of 88% and specificity of 86% for clinical screening.18–20 Because of its ease of completion and reliability, it remains valuable for tracking postoperative cognitive changes. This scale evaluates cognitive function in the following five parts: orientation, memory, attention, calculation, recall, and language. The higher the score, the better is the cognitive performance. (2) the MoCA Scale is a sensitive and widely used screening assessment test for detecting mild cognitive impairment, with a sensitivity and specificity of 90% and 87%, respectively.21,22 The cognitive function of the patients was assessed mainly by visuospatial and executive function, naming, memory, attention, calculation, language, abstraction, delayed recall, and orientation. For patients with a high school education and below and a total score of less than 30, the scale score adds one more point to the total score.
Enzyme-Linked Immunosorbent Assay
Blood samples were collected before anesthesia induction, 5 min after anesthesia induction, 30 min and 24 h after surgery to determine the plasma concentrations of IL-6, IL-10, S-100β, and TNFα. Blood samples were centrifuged at 3000g for 15 min at 4°C, and the centrifuged serum was stored at −80°C until analysis. The serum concentrations of IL-6, IL-10, S-100β, and TNFα were analyzed using an ELISA kit (Jianglai, Shanghai, China) according to the manufacturer’s instructions.
Sample Size and Statistical Analysis
The primary outcome of this study was the incidence of POCD. We calculated the number of patients required for each group based on the cognitive scores of the first 15 patients (5 patients in each group) recorded in the pre-experiment. In this small sample, cognitive scores decreased by 2.3 ± 3.8 (mean ± SD) immediately after surgery in the immediate postoperative period. We hypothesized that cognitive scores would not decline in the slow injection group compared with the rapid injection anesthesia group. Therefore, assuming a mean difference in groups of 2.3 and a pooled standard deviation of 3.8. Set bilateral α=0.05, 1-β=0.85. According to PASS 15.0, the sample size in each group was 50. Considering the 20% loss to follow-up rate, the final sample size in this study was 60 patients per group.
IBM SPSS Statistics software (version 25.0) was used for data analysis. Numerical variables are expressed as mean ± SD or median [IQR]. The differences among the groups were analyzed using a one-way ANOVA test or Kruskal–Wallis test, as appropriate. Categorical variables were presented as frequencies (percentages), and X2 or Fisher’s exact test was used for analysis. Repeated measures ANOVA was used to compare different time points within the groups. Univariate logistic regression analysis was used as the first step to identify the possible prognostic factors for POCD. Variables with P < 0.05 in these analyses were included in the multivariate regression analysis to exclude the influence of confounding factors. Multicollinearity among independent variables was evaluated using the variance inflation factor (VIF). The Hosmer–Lemeshow test was used to test the goodness of fit of the model. The accuracy of the model was estimated by analyzing the area under the ROC curve. Statistical significance was set at P < 0.05.
Results
A total of 180 patients were enrolled in this study. Among these patients, two patients in the VS group were excluded, one of whom required additional propofol beyond the prescribed maximum dose and the other was lost to follow-up. In the VM and VF groups, one patient each refused postoperative follow-up. None of the three groups experienced burst suppression during the maintenance period of anesthesia. Thus, 58 patients in the VS group, 59 patients in the VM group and 59 patients in the VF group completed the study according to the protocol, and finally included in the data analysis (Figure 1). The baseline characteristics of patients in the experimental group are shown in Table 1. No statistically significant differences were observed among the three groups.
 |
Table 1 Basic Characteristics |
 |
Figure 1 Consolidated standards of reporting trial diagram. |
There were no statistically significant differences in the incidence of POCD in the three groups of patients at 1 day (8.6% VS 11.9% VS 16.9%; P = 0.389, Table 2) and 7 days after surgery (3.4% VS 5.1% VS 8.5%; P = 0.493). With the increase in anesthesia injection rate, the induction time of patients were significantly shortened [224 (203–249) seconds (s) vs 116 (104–135) s vs 73 (61–89) s, P < 0.001, Table 3), the induction doses of propofol [11.2 (10.4–13.7) mL vs 14.1 (12.1–15.4) mL vs 16 (14.5–17.8) mL, P < 0.001], and the maximum EEG effect of propofol [47 (42–51) vs 44 (35–47) vs 42 (37–46), P < 0.001] and the incidence of burst suppression during anesthesia induction [7 patients (12.1%) vs 11 patients (18.6%) vs 18 patients (30.5%), P < 0.001] were significantly increased. Similarly, rapid induction is not conducive to the stability of perioperative hemodynamics and increases the incidence of hypotension [15 patients (25.9%) vs 25 patients (42.4%) vs 39 patients (66.1%), P < 0.001], Table 3) in patients.
 |
Table 2 Incidence of Postoperative Cognitive Decline in Patients Who Received Different Injection Rate of General Anesthetics |
 |
Table 3 Variables During Induction of Anesthesia |
We also conducted a statistical analysis of perioperative hemodynamic in the three groups of patients. We found that mean arterial pressure (F = 0.823, P = 0.441) and heart rate (F = 0.753, P = 0.472) of patients with three anesthesia injection rates were not statistically significant (Figure 2). We planned to take blood samples were collected from all enrolled patients. However, some patients refused to draw blood or missed some points in the blood sample, and some samples showed hemolysis. Therefore, for each biomarker, 38–73 patients had a complete set of blood samples available for the analysis. Although these blood indicators (IL-6, IL-10, S100-β, and TNFα) had time-dependent changes, there were no differences in these indicators between patients with and without POCD at various times (Figure 3).
 |
Figure 2 Comparison of MAP and HR at different time points in the three groups. (A) MAP at different time points in the three groups; (B) HR at different time points in the three groups. |
 |
Figure 3 Comparison of S-100β, IL-6, IL-10 and TNFα between patients with or without POCD. (A) S-100β concentration between patients with or without POCD; (B) IL-6 concentration between patients with or without POCD; (C) IL-10 concentration between patients with or without POCD; (D) TNFα concentration between patients with or without POCD. |
Prognostic Factors for POCD
Univariate logistic regression analysis showed that the risk factors for POCD included age, cardiopathy, cerebral infarction, ASA physical status classification, educational level, preoperative MMSE and MoCA scores, and the duration of hospitalization (Supplementary Table 1). With increasing age, history of previous cerebral infarction and cardiopathy, ASA of Anesthesiologists physical status classification III, and a long hospitalization time, the incidence of POCD after surgery increased. Higher preoperative MMSE and MoCA scores and a higher educational level were associated with a lower incidence of POCD.
Variables such as age, cerebral infarction, and education level have also been reported as risk factors for POCD in previous studies.9,23,24 In this study’s univariate logistic regression analysis, the P value was also <0.05. Therefore, we selected variables with P < 0.05 in this analysis to be included in multiple regression analysis to correct for the effects of confounding factors. Multicollinearity between independent variables was evaluated using the variance inflation factor (VIF). We found that the VIFs were all less than 2.1 (1.034–2.069), indicating less collinearity between predictors in the regression analysis. The Hosmer–Lemeshow test method was used to test the goodness of fit of the model. The results showed P = 0.813, indicating that our model predictions matched the observed data well. The models were identified by analyzing the area under the curve. The area under the curve for our model was 0.833 (95% CI, 0.733–0.934). Finally, we found that age (OR, 1.11; 95% CI, 1.01–1.23; P = 0.043) and duration of hospitalization (OR, 1.71; 95% CI, 1.29–2.27; P < 0.001, Table 4) were risk factors for POCD.
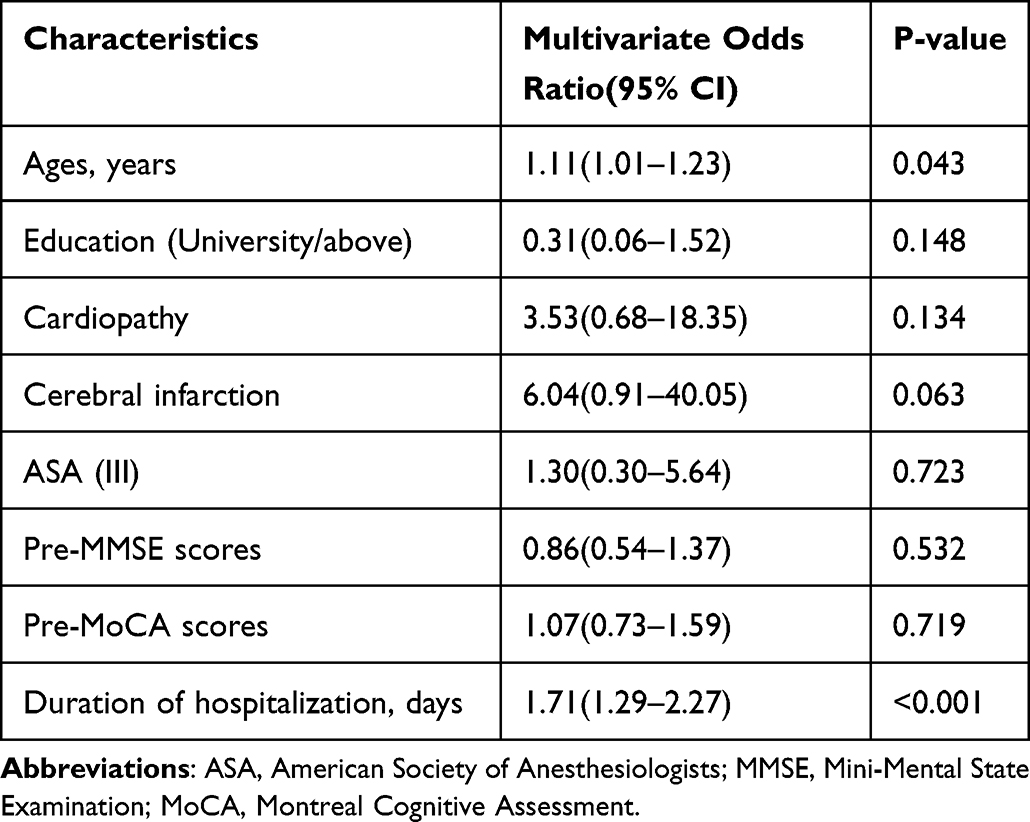 |
Table 4 Multiple Logistic Regression Analysis of Potential Risk Factors for Postoperative Cognitive Decline |
Discussion
We observed no correlation between the injection rate of propofol and the incidence of early postoperative cognitive decline. However, with the decrease in the induction rate of propofol, the incidence of burst suppression and the induction dose of propofol decreased significantly, and the hemodynamics of patients became more stable.
In this study, with the increase in the propofol injection rate, the time to anesthesia was significantly shortened, but the induction dose of propofol was significantly increased. Of course, the dosage was all within the reasonable range of the recommended dosage.25 Studies have shown that owing to the special physicochemical properties of propofol, “biological phase delay” is a rate-limiting process that regulates the concentration of propofol at its action site.26 A slower infusion rate can easily reach the necessary concentration at the action site. Therefore, the total induction dose was lower than that required for rapid injection. This finding implies that a higher infusion rate may result in excess propofol, which is the price for achieving the rapid induction of propofol. During anesthesia induction with propofol at 300 mg kg−1 h−1, we stopped the infusion of lactated Ringer’s solution to avoid drug reflux. Previous studies have shown that the infusion rate of the equilibrium solution had no effect on the induction time, propofol dosage, and plasma propofol concentration.27
In our study, the increase in propofol injection rate was associated with a decrease in BIS value, which was consistent with previous studies.28,29 The incidence of burst suppression during induction of anesthesia in patients increased significantly with an increase in anesthesia injection rate. However, no correlation was found between burst suppression during induction of anesthesia and early postoperative cognitive decline in regression analysis. This suggests that further attention should be paid to the maintenance phase of anesthesia. A recently published multicenter clinical study also found that the occurrence and duration of intraoperative burst suppression were associated with POCD.14,30 This is why we excluded patients with intraoperative burst suppression in order to accurately observe the effects of different induction rates of propofol on burst suppression during induction and postoperative cognition. Previous studies have suggested that intraoperative hypotension is a risk factor for postoperative cognitive dysfunction.31,32 Therefore, in this study, we took immediate intervention measures for hypotension that appeared during the induction to avoid its influence on the study results. We found that the number of patients requiring vasoactive drugs increased with injection rate. This also prompts us to choose a slower rate of anesthesia induction (at least 30 mg kg−1 h−1) to stabilize the hemodynamics of patients in clinical practice.
Univariate logistic regression analysis showed that age, coronary heart disease, cerebral infarction, ASA physical status classification, education level, preoperative MMSE and MOCA scores were predictors of POCD, which were similar to those previously reported.9,23,33,34, However, only age and duration of hospitalization were found to be independent risk factors for POCD in multivariate regression analysis. This indicated that the incidence of POCD increased with age and the duration of hospitalization increased, similar to the finding reported previously.33,34 This may be because with the increase in age, the functions of various organs in the body of elderly patients tend to degenerate, the reserve capacity decreases, and the ability to withstand trauma such as surgery and anesthesia decreases.35 The pharmacodynamics and pharmacokinetics of elderly patients may be decreased, making them more sensitive to drugs. At the same time, advanced age can reduce brain weight and volume, reduce cell bodies and myelin sheath fibers, synaptic density and DNA repair capacity of multiple brain regions (such as the hippocampus), which is not conducive to memory formation and indirectly contributes to postoperative cognitive decline in elderly patients.36
To further explore the role of neuroinflammation in the pathogenesis of POCD, we assessed the levels of S-100β, IL-6, IL-10 and TNFα according to previous studies. However, there was no significant difference between the groups. In a recent multicenter study, the serum levels of IL-6, ascertain endothelial growth factor, intercellular adhesion molecule, transforming growth factor-β1, C3α, and advanced glycation were detected. Finally, it was only found that higher blood interleukin-6 concentration after surgical incision was an independent risk factor for delayed neurocognitive recovery.37 This suggests that only selected cytokines are induced to change. The cytokines included in this study are limited, which may be the reason why we did not observe differences.
In this study, we adjusted the drugs under BIS monitoring rather than the modified observer’s assessment of alertness/sedation (MOAA/S) score. BIS is superior to MOAA/S in simplicity and provides a more continuous measurement.38 Although there may be some delayed effect of BIS. According to literature reports, there is currently no monitoring tool that can monitor or predict patients’ conscious response in real time. However, BIS is the monitoring tool with the least delay effect among these monitoring tools.39 In addition, BIS can more accurately reflect the depth of sedation of propofol compared with other anesthetics.11 BIS best detected suppressed periods, and BIS monitors might be preferable for older patients with increased sensitivity to anaesthesia.40 At the same time, we also look forward to the emergence of more real-time anesthesia depth monitoring tools to facilitate the management of clinical anesthesia.
The present study still has several limitations. First, this study was a single-center study, and the data only came from one study center, which needs further multi-center study to verify the results. Secondly, since most of the patients with inguinal hernia are elderly men, it remains to be further studied whether the results of this study can be generalized in elderly women. Finally, we did not include normal patients as control group, but we disrupted the order of cognitive correlation scales, which may mitigate the learning effects of repeated testing to some extent.
Conclusion
For elderly patients undergoing laparoscopic inguinal hernia repair, lowering the injection rate of propofol (such as 30 mg kg−1 h−1) cannot decrease the incidence of early POCD, but reduces induction dose of propofol and use of vasoactive drugs, making the patient’s hemodynamics more stable. For the induction of propofol anesthesia in elderly patients, slow induction (at least 30 mg kg−1 h−1) is recommended.
Abbreviations
POCD, postoperative cognitive decline; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; PND, perioperative neurocognitive disorder; NF, nuclear factor; EEG, electroencephalographic; BIS, bispectral index; ASA, American Society of Anesthesiologists; BMI, body mass index; SpO2, pulse oxygen saturation; PetCO2, end-tidal carbon dioxide pressure; PACU, post-anesthesia care unit; SR, suppression ratio; MAP, mean arterial pressure; HR, heart rate; SD, standard deviation; IL, interleukin; TNF, tumor necrosis factor; VIF, variance inflation factor; MOAA/S, modified observer’s assessment of alertness/sedation.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki and was registered at ClinicalTrials.gov (ID: ChiCTR2000040005). The study protocol was approved by the Research Ethics Committee for Experimental and Clinical Studies at the Anhui Provincial Hospital, China, [ethics approval number: 081, 8 May 2021].
Acknowledgments
We thank all those who supported and participated in the study, including our staff, patients and their family members. In addition, an unauthorized version of the Chinese MMSE was used by the study team without permission. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com). Therefore, we are very grateful to PAR Inc. for authorizing the use of MMSE scale in this study.
Funding
This study was funded by the National Natural Science Foundation of China (81860249).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Moller JT, Cluitmans P, Rasmussen LS, et al. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet. 1998;351(9106):857–861. doi:10.1016/S0140-6736(97)07382-0
2. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br J Anaesth. 2018;121(5):1005–1012. doi:10.1016/j.bja.2017.11.087
3. Steinmetz J, Christensen KB, Lund T, Lohse N, Rasmussen LS, Group I. Long-term consequences of postoperative cognitive dysfunction. Anesthesiology. 2009;110(3):548–555. doi:10.1097/ALN.0b013e318195b569
4. Sun Y, Feng H, Zou T, et al. Assessment of risk factors for postoperative cognitive dysfunction after coronary artery bypass surgery: a single-center retrospective cohort study. Biosci Rep. 2021;41(2). doi:10.1042/BSR20190719
5. Steinmetz J, Rasmussen LS. Peri-operative cognitive dysfunction and protection. Anaesthesia. 2016;71 Suppl 1:58–63. doi:10.1111/anae.13308
6. Terrando N, Eriksson LI, Ryu JK, et al. Resolving postoperative neuroinflammation and cognitive decline. Ann Neurol. 2011;70(6):986–995. doi:10.1002/ana.22664
7. Li Z, Zhu Y, Kang Y, Qin S, Chai J. Neuroinflammation as the underlying mechanism of postoperative cognitive dysfunction and therapeutic strategies. Front Cell Neurosci. 2022;16:843069. doi:10.3389/fncel.2022.843069
8. Corona AW, Fenn AM, Godbout JP. Cognitive and behavioral consequences of impaired immunoregulation in aging. J Neuroimmune Pharmacol. 2012;7(1):7–23. doi:10.1007/s11481-011-9313-4
9. Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008;108(1):18–30. doi:10.1097/01.anes.0000296071.19434.1e
10. Dustin Boone M, Lin HM, Liu X, et al. Processed intraoperative burst suppression and postoperative cognitive dysfunction in a cohort of older noncardiac surgery patients. J Clin Monit Comput. 2021;36:1433–1440. doi:10.1007/s10877-021-00783-0
11. Li Z, Cai J, Li J, Xu X, Zheng L. Comparative evaluation of the bispectral index (BIS) and BISpro during propofol anaesthesia. J Int Med Res. 2021;49(4):3000605211001705. doi:10.1177/03000605211001705
12. Struys MM, Vereecke H, Moerman A, et al. Ability of the bispectral index, autoregressive modelling with exogenous input-derived auditory evoked potentials, and predicted propofol concentrations to measure patient responsiveness during anesthesia with propofol and remifentanil. Anesthesiology. 2003;99(4):802–812. doi:10.1097/00000542-200310000-00010
13. Blum J, Kochs E, Forster N, Schneider G. The influence of injection rate on the hypnotic effect of propofol during anesthesia: a randomized trial. PLoS Clin Trials. 2006;1(3):e17. doi:10.1371/journal.pctr.0010017
14. Evered LA, Chan MTV, Han R, et al. Anaesthetic depth and delirium after major surgery: a randomised clinical trial. Br J Anaesth. 2021;127(5):704–712. doi:10.1016/j.bja.2021.07.021
15. Shi X, Chen X, Ni J, et al. Systematic review and meta-analysis of the prognostic value of Narcotrend monitoring of different depths of anesthesia and different Bispectral Index (BIS) values for cognitive dysfunction after tumor surgery in elderly patients. Ann Transl Med. 2022;10(4):186. doi:10.21037/atm-22-90
16. Saugel B, Bebert EJ, Briesenick L, et al. Mechanisms contributing to hypotension after anesthetic induction with sufentanil, propofol, and rocuronium: a prospective observational study. J Clin Monit Comput. 2022;36(2):341–347. doi:10.1007/s10877-021-00653-9
17. Needham MJ, Webb CE, Bryden DC. Postoperative cognitive dysfunction and dementia: what we need to know and do. Br J Anaesth. 2017;119(suppl_1):i115–i125. doi:10.1093/bja/aex354
18. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
19. Hensel A, Angermeyer MC, Riedel-Heller SG. Measuring cognitive change in older adults: reliable change indices for the Mini-Mental State Examination. J Neurol Neurosurg Psychiatry. 2007;78(12):1298–1303. doi:10.1136/jnnp.2006.109074
20. Momeni M, Meyer S, Docquier MA, et al. Predicting postoperative delirium and postoperative cognitive decline with combined intraoperative electroencephalogram monitoring and cerebral near-infrared spectroscopy in patients undergoing cardiac interventions. J Clin Monit Comput. 2019;33(6):999–1009. doi:10.1007/s10877-019-00253-8
21. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
22. Kang JM, Cho YS, Park S, et al. Montreal cognitive assessment reflects cognitive reserve. BMC Geriatr. 2018;18(1):261. doi:10.1186/s12877-018-0951-8
23. Wang Z, van Veluw SJ, Wong A, et al. Risk factors and cognitive relevance of cortical cerebral microinfarcts in patients with ischemic stroke or transient ischemic attack. Stroke. 2016;47(10):2450–2455. doi:10.1161/STROKEAHA.115.012278
24. Amado LA, Perrie H, Scribante J, Ben-Israel KA. Preoperative cognitive dysfunction in older elective noncardiac surgical patients in South Africa. Br J Anaesth. 2020;125(3):275–281. doi:10.1016/j.bja.2020.04.072
25. Cummings GC, Dixon J, Kay NH, et al. Dose requirements of ICI 35,868 (propofol, ‘Diprivan’) in a new formulation for induction of anaesthesia. Anaesthesia. 1984;39(12):1168–1171. doi:10.1111/j.1365-2044.1984.tb06425.x
26. Stokes DN, Hutton P. Rate-dependent induction phenomena with propofol: implications for the relative potency of intravenous anesthetics. Anesth Analg. 2014;119(2):302–310. doi:10.1213/ANE.0000000000000317
27. Kazama T, Ikeda K, Morita K, et al. Investigation of effective anesthesia induction doses using a wide range of infusion rates with undiluted and diluted propofol. Anesthesiology. 2000;92(4):1017–1028. doi:10.1097/00000542-200004000-00019
28. Gale T, Leslie K, Kluger M. Propofol anaesthesia via target controlled infusion or manually controlled infusion: effects on the bispectral index as a measure of anaesthetic depth. Anaesth Intensive Care. 2001;29(6):579–584. doi:10.1177/0310057X0102900602
29. Rudner R, Jalowiecki P, Kawecki P, Gonciarz M, Mularczyk A, Petelenz M. Conscious analgesia/sedation with remifentanil and propofol versus total intravenous anesthesia with fentanyl, midazolam, and propofol for outpatient colonoscopy. Gastrointest Endosc. 2003;57(6):657–663. doi:10.1067/mge.2003.207
30. Joosten A, Rinehart J, Bardaji A, et al. Anesthetic management using multiple closed-loop systems and delayed neurocognitive recovery: a randomized controlled trial. Anesthesiology. 2020;132(2):253–266. doi:10.1097/ALN.0000000000003014
31. Xu X, Hu X, Wu Y, et al. Effects of different BP management strategies on postoperative delirium in elderly patients undergoing Hip replacement: a single center randomized controlled trial. J Clin Anesth. 2020;62:109730. doi:10.1016/j.jclinane.2020.109730
32. Siepe M, Pfeiffer T, Gieringer A, et al. Increased systemic perfusion pressure during cardiopulmonary bypass is associated with less early postoperative cognitive dysfunction and delirium. Eur J Cardiothorac Surg. 2011;40(1):200–207. doi:10.1016/j.ejcts.2010.11.024
33. Hasan TF, Kelley RE, Cornett EM, Urman RD, Kaye AD. Cognitive impairment assessment and interventions to optimize surgical patient outcomes. Best Pract Res Clin Anaesthesiol. 2020;34(2):225–253. doi:10.1016/j.bpa.2020.05.005
34. Wei Y, Zhang C, Wang D, Wang C, Sun L, Chen P. Progress in research on the effect of melatonin on postoperative cognitive dysfunction in older patients. Front Aging Neurosci. 2022;14:782358. doi:10.3389/fnagi.2022.782358
35. Lin X, Chen Y, Zhang P, et al. The potential mechanism of postoperative cognitive dysfunction in older people [J]. Exp Gerontol. 2020;130:110791. doi:10.1016/j.exger.2019.110791
36. K SA, H TM, Pakkenberg H, et al. The effect of age and gender on the volume and size distribution of neocortical neurons [J]. Neuroscience. 2007;150:121–130. doi:10.1016/j.neuroscience.2007.06.062
37. Li Y, Chen D, Wang H, et al. Intravenous versus volatile anesthetic effects on postoperative cognition in elderly patients undergoing laparoscopic abdominal surgery. Anesthesiology. 2021;134(3):381–394. doi:10.1097/ALN.0000000000003680
38. Fan Y, Yuan L, Ji M, Yang J, Gao D. The effect of melatonin on early postoperative cognitive decline in elderly patients undergoing Hip arthroplasty: a randomized controlled trial. J Clin Anesth. 2017;39:77–81. doi:10.1016/j.jclinane.2017.03.023
39. Zanner R, Pilge S, Kochs EF, et al. Time delay of electroencephalogram index calculation: analysis of cerebral state, bispectral, and Narcotrend indices using perioperatively recorded electroencephalographic signals. Br J Anaesth. 2009;103(3):394–399. doi:10.1093/bja/aep198
40. Eagleman SL, Drover CM, Li X, et al. Offline comparison of processed electroencephalogram monitors for anaesthetic-induced electroencephalogram changes in older adults. Br J Anaesth. 2021;126(5):975–984. doi:10.1016/j.bja.2020.12.042
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.