Back to Journals » Journal of Pain Research » Volume 19
Effectiveness of Pre-Emptive Incision-Site Infiltration with Ropivacaine Combined with Triamcinolone Acetonide versus Ropivacaine for Post-Craniotomy Pain in Adults: A Prospective Randomized Controlled Trial
Authors Liu Q ![]() , Tu S, Zhao C
, Tu S, Zhao C ![]() , Ji N
, Ji N ![]() , Luo F
, Luo F ![]()
Received 1 January 2026
Accepted for publication 14 April 2026
Published 21 April 2026 Volume 2026:19 593180
DOI https://doi.org/10.2147/JPR.S593180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Qiang Liu,1,* Shaohua Tu,2,* Chunmei Zhao,3 Nan Ji,2 Fang Luo3
1Department of Day Surgery Center, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Luo, Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, No. 119, Nansihuan Xilu, Fengtai District, Beijing, 100070, People’s Republic of China, Tel +86 010 59976664, Email [email protected]
Background: Local anesthetic incision-site infiltration (ISI) effectively eases post-craniotomy pain; however, its short duration limits sustained analgesia. This study aimed to assess the efficacy and safety of ropivacaine combined with triamcinolone acetonide along with ropivacaine alone via ISI to manage postoperative pain in adult craniotomy patients.
Methods: This prospective, randomized, open-label, controlled trial enrolled 110 patients (aged 18~65 years; American Society of Anesthesiologists Physical Status, I~III) scheduled for elective craniotomies. Patients were randomly allocated to two distinct groups: the treatment group received 0.5% ropivacaine combined with triamcinolone acetonide for ISI (n = 55) and the control group received 0.5% ropivacaine alone (n = 55). The primary outcome was sufentanil consumption (μg) via patient-controlled analgesia (PCA) within 48 h post-surgery using the intention-to-treat (ITT) principle and per-protocol (PP) analyses.
Results: Within 48 hours post-surgery, the treatment group showed significantly lower cumulative sufentanil consumption than control group (8.4 ± 5.2 μg vs 32.7 ± 12.2 μg; mean difference: − 24.3, 95% confidence interval − 27.8 to − 20.7; p < 0.001). The estimated median time to the first PCA-administered administration was 30 h in the treatment group versus 12 h in the control group (hazard ratio: 0.11, 95% CI: 0.07 to 0.18; log-rank p < 0.0001). A statistically significant decrease in numerical rating scale (NRS) pain scores was observed in the treatment group compared with the control group at all postoperative time points (2h to 1 month; p < 0.001 for all comparisons). No adverse events (AEs) occurred in either group during the study period.
Conclusion: Compared with ropivacaine alone, the addition of triamcinolone acetonide for ISI was associated with improved postoperative analgesia and reduced sufentanil consumption in adults who underwent craniotomy. Moreover, the combination was linked to a lower incidence of postoperative nausea and vomiting (PONV), with no reported severe AEs.
Keywords: postoperative pain, craniotomy, incision-site infiltration, ropivacaine
Introduction
Contrary to earlier assumptions that intracranial surgery causes minimal pain, recent evidence indicates that over half of patients endure moderate-to-severe pain following craniotomy, primarily within the first 48 hours.1 Severe postoperative pain can induce sympathetically mediated hypertension and increase the risk of complications, such as cerebral edema, hemorrhage, prolonged hospitalization, and mortality.2,3 Furthermore, the site of craniotomy may influence postoperative pain and analgesic response.4 Some patients may also develop chronic pain, which significantly diminishes their quality of life.2,5 Nevertheless, the management of pain following craniotomy remains challenging, and a consensus on effective treatment strategies has yet to be established.
Systemic analgesics, especially opioids, are frequently administered for postoperative analgesia; however, their use is associated with unavoidable side effects such as sedation, respiratory depression, interference with neurological assessments, and nausea and vomiting.6 In response, non-opioid analgesics, including nonsteroidal anti-inflammatory drugs (NSAIDs), have gained prominence in post-craniotomy pain management owing to their opioid-sparing benefits.7 However, caution is warranted in neurosurgical patients because concerns regarding NSAIDs increase the risk of intracranial hemorrhage (ICH) due to impaired platelet aggregation, and their analgesic efficacy may sometimes be insufficient.8,9 The heightened risk of thrombosis and cardiovascular events has also diminished enthusiasm for selective cyclooxygenase-2 (COX-2) inhibitors as a secure substitute.10 Therefore, developing an optimal pain management strategy that minimizes reliance on systemic analgesics is crucial.
ISI with local anesthetics is recognized as a straightforward, safe, and essential component of multimodal analgesia in craniotomies. However, the analgesic effect of local anesthetics is short-lived and insufficient for sustained post-craniotomy pain relief.11–13 Thus, there is an urgent need to explore adjuncts that can prolong postoperative analgesia. Post-craniotomy pain manifests as somatic discomfort arising from scalp, pericranial musculature, and soft tissue injuries. These injuries trigger the release of inflammatory mediators that activate peripheral nociceptors, generating pain through abnormal action potentials transmitted via afferent A-δ and C-fibers.14,15 Consequently, reducing incisional inflammation, for instance through glucocorticoid infiltration at the incision site, could be an effective strategy for managing incisional pain.13,16–18 Previous research demonstrated that preemptive ISI using dexamethasone-ropivacaine reduced post-craniotomy sufentanil consumption to 29.0 μg (vs 38.3 μg with ropivacaine alone).19 Another study reported that adding Diprospan further decreased consumption to 5 μg (vs 38 μg). As a composite glucocorticoid, Diprospan provides analgesia with effects lasting 3~4 weeks.20 Given that post-craniotomy pain typically peaks within 48 hours after surgery. Therefore, further investigation of the optimal combination of local anesthetics and mid-acting glucocorticoids with slow regional absorption is warranted to devise a more rational and effective strategy for preventing incisional pain.
As a synthetic glucocorticoid, triamcinolone acetonide exerts its effects by binding to and activating intracellular glucocorticoid receptors, prompting their translocation to the nucleus, which initiates a wide range of anti-inflammatory actions, including downregulating pro-inflammatory cytokine expression, inhibiting the synthesis and release of prostaglandins and leukotrienes from arachidonic acid, and triggering anti-inflammatory transcription elements such as lipocortin, with a median half-life spanning 18 to 36 hours.21,22 However, the effectiveness of triamcinolone acetonide infiltration, when used as an adjunct to a local anesthetic, in prolonging pain relief after craniotomy remains uncertain. To address this, we conducted prospective randomized controlled trials to evaluate the impact of preemptive in situ incision infiltration with ropivacaine combined with triamcinolone acetonide compared to ropivacaine alone on postoperative pain in patients undergoing craniotomy.
Materials and Methods
The study was conducted in strict compliance with CONSORT guidelines and adhered to the latest edition of the Declaration of Helsinki. This study was supported by the Research Ethics Committee of the Beijing Tiantan Hospital, Capital Medical University (reference no. KY 2018–034-02-4) and registered at ClinicalTrials.gov (NCT 06069804; Principal Investigator Fang Luo; Date of Registration: September 29, 2023) before patient enrollment. Data collection took place at Beijing Tiantan Hospital, Capital Medical University, Beijing, China. Patient recruitment extended from October 7, 2023, to December 31, 2023. The final follow-up was completed on February 1, 2024.
Study Design and Participants
This study was a prospective, single-center, open-label, randomized controlled clinical investigation. Following approval from the institutional review board, comprehensive written informed consent was obtained from all participating patients scheduled to undergo supratentorial craniotomy during preoperative anesthesia consultations. Patients received comprehensive instructions on utilizing a NRS to evaluate pain and underwent thorough training in the operation of the PCA device.
Eligible participants were adults (18~65 years) with an American Society of Anesthesiologists (ASA) (Schaumburg, Illinois) Physical Status classification of I to III. The inclusion criteria also required patients to be expected to fully awaken and cooperate within 2 h postoperatively, with an anticipated surgical duration not exceeding 6 h.
The exclusion criteria included patients unable to comprehend or utilize NRS; declining participation; patients with contraindications to ISI, such as documented allergies to study medications or local infection; patients with a Glasgow coma scale score ˂15, obesity (body mass index >35 kg·m−2); coagulopathy; pregnancy or lactation; prior craniotomy; chronic pain (persistent or recurrent pain lasting >3 months); drug addiction (including regular opioid or illicit substance use); chronic alcohol abuse; prolonged corticosteroid treatment (>6 months); uncontrolled systemic arterial hypertension; severe renal or hepatic diseases; mental disorders; serious neurological conditions; cardiomyopathies; arrhythmias; elevated intracranial pressure (ICP); or a history of brain trauma.
Withdrawal criteria included surgical complications, such as surgical aphasia, unconsciousness persisting beyond 2 h postoperatively, surgical duration exceeding 6 h, or postoperative mechanical ventilation need.
Randomization and Blinding
The allocation sequence was formed through randomization using SPSS version 25.0 (International Corp., Armonk, NY, USA). Eligible participants were assigned in a 1:1 ratio in random to the treatment or control groups. To ensure allocation concealment, opaque, sealed envelopes numbered in sequential order were employed, which displayed the sequential order of participants’ screening on the outside, as well as the assigned group on the inside. Prior to surgery, the envelope was disclosed by the investigator, overseeing the procedure, and the patient was allocated to receive ISI. A specialized researcher, deliberately excluded from the outcome data collection, handled participant enrollment. Patients, statisticians, and independent researchers tasked with conducting postoperative follow-up were deliberately unaware of group assignments. The blinding of neurosurgeons and anesthesiologists was not feasible in this study because of visible differences (suspension vs clear solution) in the preparation of local infiltration mixtures. However, neurosurgeons and anesthesiologists were given clear instructions to avoid disclosing the allocation while interviewing the participants.
Medications intended for ISI were prepared by an impartial investigator for each group, in which 10 mg of triamcinolone acetonide and 150 mg of ropivacaine were diluted to a final volume of 30 mL with 0.9% saline. In the control group, 150 mg of ropivacaine was similarly diluted to 30 mL with 0.9% saline. Ropivacaine concentration was maintained at 0.5% in both groups.
Procedures
Upon arrival in the operating room, all patients underwent standardized monitoring and anesthetic protocols. Continuous monitoring was conducted, including blood pressure (BP), heart rate (HR), 5-lead electrocardiography (ECG), peripheral oxygen saturation (SpO2), and the Bispectral Index (BIS). Before surgery, patients were sedated with intravenous (IV) midazolam at a dose of 0.05 mg/kg. Anesthesia was then induced using sufentanil (0.3 to 0.5 μg/kg), propofol (1.5 to 2.5 mg/kg), as well as cisatracurium (0.2 mg/kg). Following tracheal intubation, patients were ventilated to maintain end-tidal carbon dioxide at 35–40 mmHg. A combination of propofol (6 to 8 mg·kg−1·hour−1) as well as remifentanil (0.1 to 0.3 μg·kg−1·min−1) was administered to maintain a BIS, ranging from 40 to 50. Additionally, cisatracurium (0.01mg/kg was administered intravenously every 40 min for muscle relaxation maintenance. To ensure hemodynamic stability, vasoactive drugs were administered as required to preserve mean arterial pressure (MAP) as well as HR fluctuations within 20% of baseline values. Both propofol and remifentanil infusions were discontinued at the conclusion of the surgery.
After general anesthesia induction and tracheal intubation, and once all necessary equipment and catheters were in place, as well as under stable anesthetic conditions just before making the skin incision, the neurosurgeon performed local infiltration of the study solution. Using a 22-gauge needle inserted at an angle of 45, neurosurgeon infiltrated solution through full thickness of scalp along planned incision line as well as at head-holder attachment sites, and the same neurosurgeon carried out this procedure for all patients.23 Aggregate volume of investigational solution administered to every patient was ascertained by neurosurgeon, primarily according to incision length, as well as was meticulously recorded by investigator.
Patients underwent extubation once they demonstrated satisfactory hemodynamic stability, respiratory function, and neurological status. To curb PONV, patients received an intravenous dose of ondansetron (8 mg), after which they were shifted to the post-anesthesia care unit (PACU). The PCA solution was composed of 150 μg sufentanil and 16 mg ondansetron diluted in 100 mL normal saline. The PCA device was programmed to deliver a 2 μg bolus of sufentanil, with a 10-minute lockout interval between doses and a maximum hourly limit of 8 μg. Initial loading dose and background infusion rate of the PCA pump were set to 0. Patients were instructed to activate the PCA demand button when their NRS score reached ≥ 4, and they could repeat this action until their pain experienced clinically meaningful alleviation. Inadequate postoperative analgesia was defined as an NRS score greater than 4 despite receiving the maximum allowable sufentanil dose via the PCA device. If a patient experienced insufficient analgesia after five consecutive sufentanil boluses, the bolus dose was increased to 3 μg, and the maximum hourly dose was raised to 12 μg. All other factors of the postoperative rehabilitation process were kept consistent between groups.
Outcome Measures
The primary outcome measure was cumulative sufentanil consumption (μg) delivered through the PCA pump over 48-hour postoperative period. Secondary outcomes included several key elements: timing of the first analgesic request, as denoted by participants pressing the PCA demand button; the cumulative amount of sufentanil consumption by PCA at 2, 4, 8, and 24h postoperatively, NRS scores for pain (spanning a scale from 0, which denotes the absence of pain, to 10, signifying the most excruciating pain imaginable) at 2, 4, 8, 24, 48, and 72 h, as well as at 1 week, 2 weeks, and 1 month postoperatively; PONV scores (categorized as 0 for absent; 1 for nausea not requiring treatment; 2 for nausea requiring treatment; along with 3 for vomiting) at 2, 4, 8, 24, and 48 hours postoperatively; length of stay (LOS), denoted hospitalization duration following surgery; and wound healing scores (with a total score of 3 indicating optimal wound healing, a score of 4–5 suggesting good wound healing, and a score of 6 or higher indicating suboptimal wound healing) assessed at 1 month postoperatively. Additionally, the frequency of emergency BP reduction and instances of respiratory depression within the 8-hour postoperative period were recorded. Safety evaluations focused on steroid-induced complications, including wound infection, hematoma, impaired wound healing, chest infection, and gastric ulcers, during hospitalization. All AEs were closely monitored and promptly addressed. The study team validated suspected AEs whenever possible, and only AEs deemed related to the study were recorded. The follow-up assessments were performed by experienced research personnel who were blinded to the study. Data on the outcomes following discharge were collected during in-person follow-up visits or through video calls.
Sample Size
The sample size was determined based on data sourced from previously published studies.19 Power Analysis and Sample Size (PASS) V.15 software (NCSS). Drawing on insights from prior research as well as our clinical experience, we found that participants receiving preemptive scalp infiltration with 0.5% ropivacaine would require approximately 40±20 μg of sufentanil postoperatively, and postoperative pain intensity or analgesic requirements would decline by approximately 30% to 40% with the addition of triamcinolone acetonide. Consequently, we projected that the sufentanil dose in the triamcinolone acetonide group would be 26±20 μg within the first 48 hours after surgery. To achieve 90% power to detect a statistically significant difference (two-sided α = 0.05; 2-sided), an initial sample size of 44 participants per group was deemed necessary. Considering a 20% withdrawal rate, the sample size in each group was 55 patients.
Statistical Analysis
All analyses adhered to both the ITT and PP principles. Normality and homogeneity of data distribution were assessed using the Kolmogorov–Smirnov test. Normally distributed data are summarized as means with standard deviation (SD), while skewed data are described as medians with interquartile ranges (IQRs). Categorical data were expressed as frequencies and percentages (%). When dealing with continuously distributed variables, repeated-measures ANOVA was used for analysis, including NRS data, whereas the Wilcoxon rank-sum test was used for skewed data. Nominal variables were compared using the χ2 test or Fisher’s exact test. Given the potential influence of craniotomy location on postoperative pain, surgical site (categorized as infratentorial vs supratentorial) was included as a pre-specified covariate in the primary mixed-effects model. Additionally, exploratory subgroup analyses were conducted to assess the consistency of treatment effects across craniotomy sites. Subgroup analyses were performed across five predefined categories: age (< 45 and ≥ 45 years), sex (male and female), length of incision (< 20 and ≥ 20 cm), duration of surgery (<4.0 h and ≥ 4.0 h) and surgical site (supratentorial and infratentorial). To compare the time to the first rescue medication consumption, a univariate Cox proportional hazards model was used. Treatment effects are reported as mean differences along with their respective 95% CIs. All analyses were two-tailed, and statistical significance was set as a p-value of <0.05. Safety analyses were performed within the safety dataset, comparing the incidence of AEs using the χ2-test or Fisher’s exact test based on the actual treatment received. All statistical analyses were conducted by statisticians who were blinded to the allocation and the intervention process. Multiple imputations were used to handle missing data on outcomes at one month. Data analysis was performed using SPSS version 25.0.
Results
Study Population
Out of the 149 individuals screened, 110 met the inclusion criteria, provided informed consent, and were randomly assigned to groups (Figure 1). The 39 excluded participants did not meet the criteria (n=15), declined to participate (n=2), or were unavailable because of study personnel constraints (n=22). The participants were equally divided into a treatment group (n=55) and a control group (n=55). All randomized patients were analyzed using the ITT approach, while 99 patients (50 in the treatment group and 49 in the control group) completed the study and were included in the PP analyses (Figure 1).
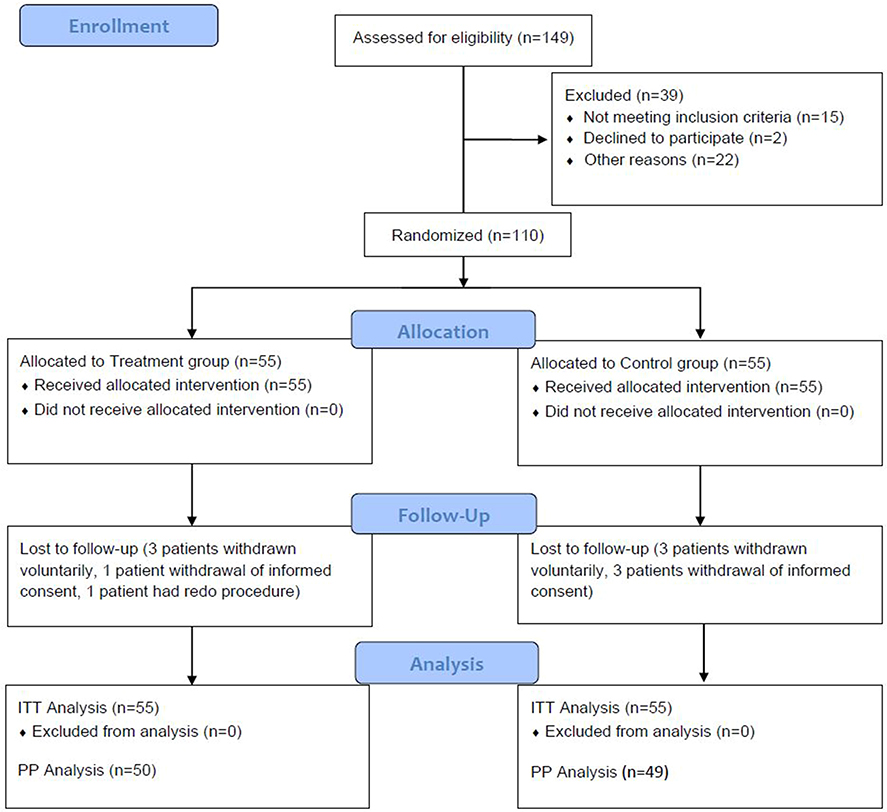 |
Figure 1 CONSORT Patient Flow Diagram Illustrating Numbers Analyzed in Each Group. Notes: Treatment group: ropivacaine plus triamcinolone acetonide group; control group: ropivacaine alone group. |
Baseline Characteristics and Intraoperative Outcomes
At baseline, all demographic and clinical characteristics of both groups were similar, with no statistically significant differences found in factors such as surgical site distribution, volume of local anesthetic used, intraoperative remifentanil dosage, operative duration, or anesthesia duration. (Table 1).
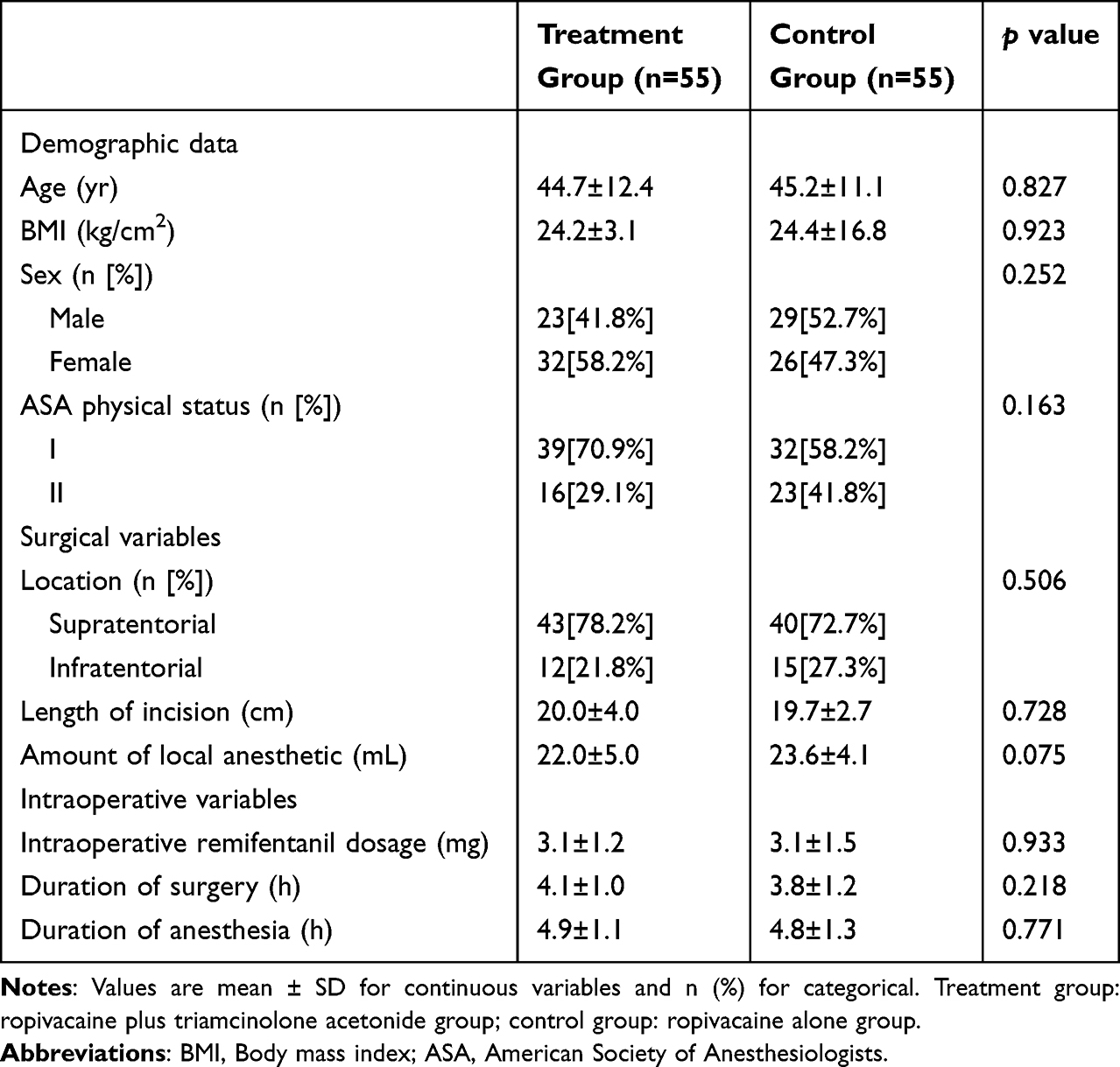 |
Table 1 Patient Baseline and Perioperative Characteristics |
Hemodynamic parameters, including HR (Figure 2A) and MAP (Figure 2B), remained stable and comparable throughout the procedure.
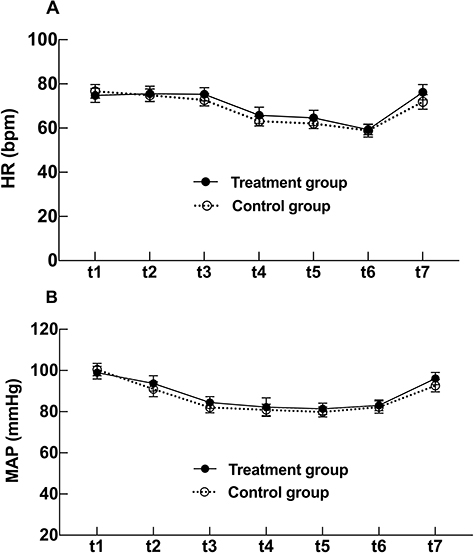 |
Figure 2 Intraoperative HR (A) as well as MAP (B) at each time point. Abbreviations: HR, heart rate; MAP, mean arterial pressure. Notes: Data are presented as mean with 95% CI throughout the study period. There were no statistically significant differences in the perioperative HR and MAP. t1, before anesthetic induction; t2, after anesthetic induction; t3, during scalp infiltration; t4, during skull drilling; t5, during dural incision; t6, during skin closure; t7, at the end of surgery. Treatment group: ropivacaine plus triamcinolone acetonide group; control group: ropivacaine alone group. |
Primary Efficacy Outcome
The treatment group demonstrated a statistically significant reduction in 48-hour cumulative sufentanil consumption compared to the control group (8.4 ± 5.2 μg vs 32.7 ± 12.2 μg; mean difference: −24.3, 95% CI: −27.8 to −20.7; p < 0.001) (Table 2). This finding was consistent with the PP analysis (mean difference: −24.1, 95% CI: −27.8 to −20.5; p < 0.001) (Table S1). The subgroup analysis results indicated trends consistent with the primary outcome measures across the five subgroups: age (< 45 years and ≥ 45 years), sex (male and female), length of incision (< 20 cm and ≥ 20 cm), duration of surgery (< 4.0 hours and ≥ 4.0 hours) and surgical site (supratentorial and infratentorial), with no significant interaction (Figure 3).
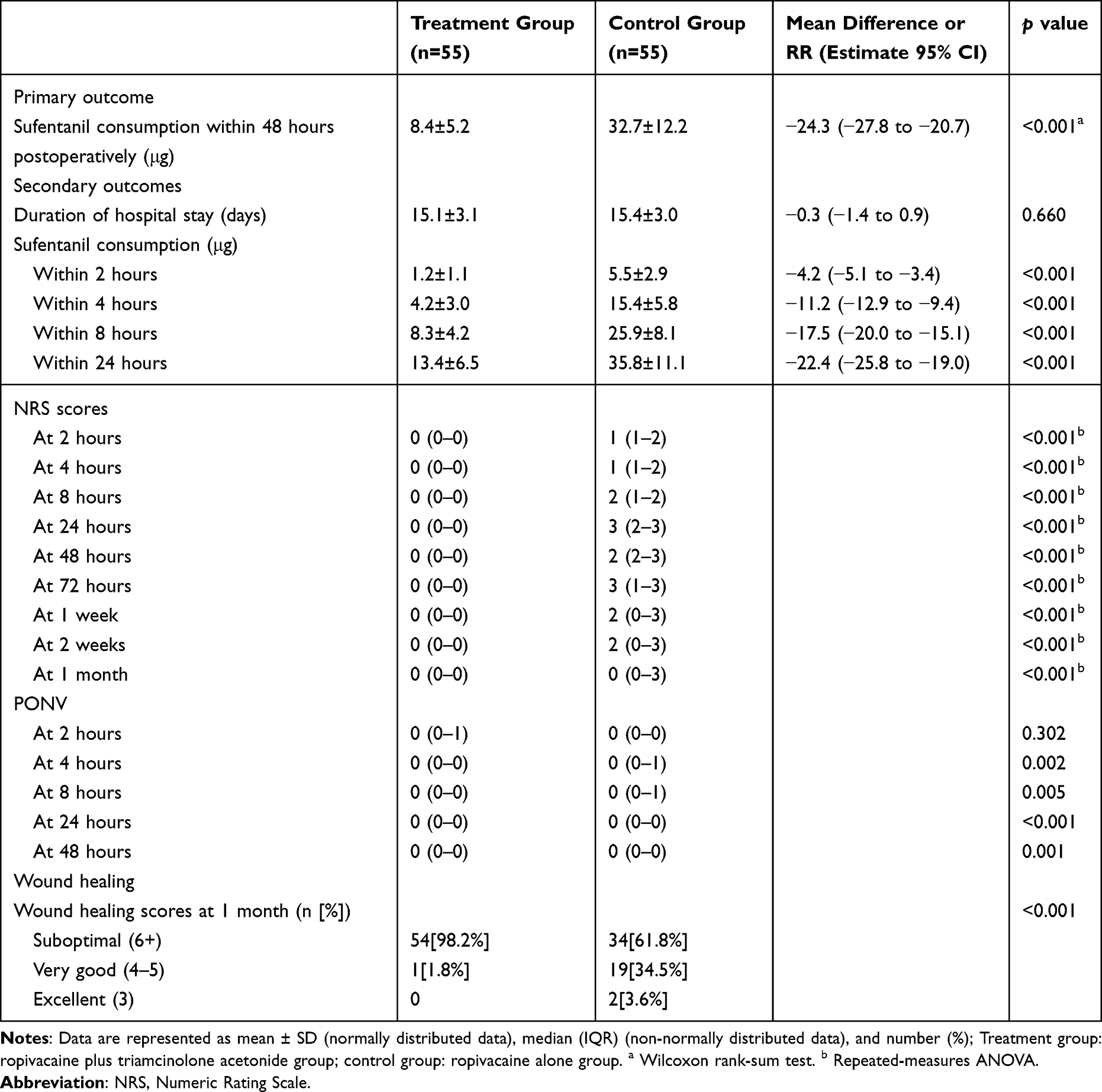 |
Table 2 Primary as Well as Secondary Outcomes |
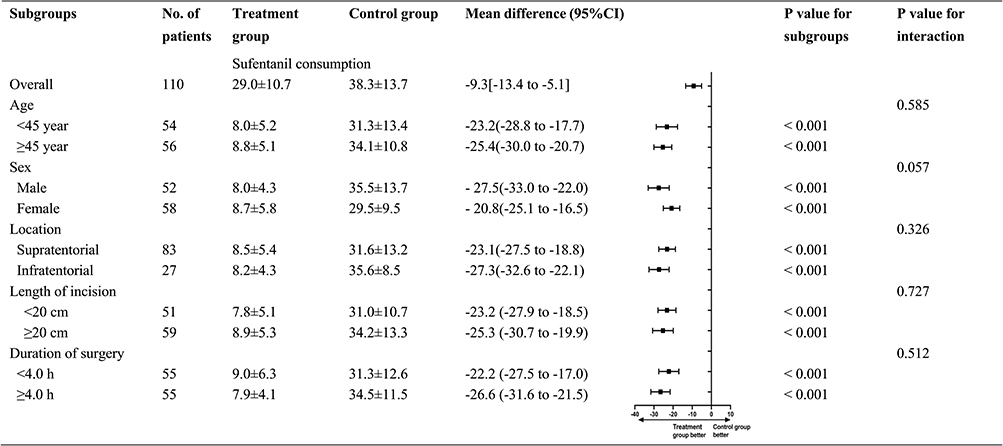 |
Figure 3 Outcomes of Subgroup Analysis for Primary Outcome Measures. Abbreviation: CIs, confidence intervals. Notes: Treatment group: ropivacaine plus triamcinolone acetonide group; control group: ropivacaine alone group. |
Secondary Outcomes
The time to the first PCA request was notably prolonged in the treatment group (median: 30 h vs 12 h; hazard ratio: 0.11, 95% CI: 0.07 to 0.18; log-rank p < 0.0001) (Figure 4). Sufentanil consumption was significantly lower in the treatment group compared with the control group at 2, 4, 8, and 24 h after craniotomy surgery (p < 0.001) (Table 2). A statistically significant decrease in NRS pain scores was observed in the treatment group compared with the control group at all postoperative time points (2h to 1 month; p < 0.001 for all comparisons) (Table 2). While no difference was observed at 2 h (p = 0.302), the treatment group exhibited a significantly lower PONV incidence at 4, 8, 24, and 48 h postoperatively (p < 0.05) (Table 2). At the 1-month follow-up, the wound healing scores did not differ significantly between the groups (p = 0.097), although a greater proportion of patients in the treatment group achieved “excellent” healing (45 [81.8%] vs 37 [67.3%] in the controls) (Table 2). The LOS was comparable between the groups (Table 2).
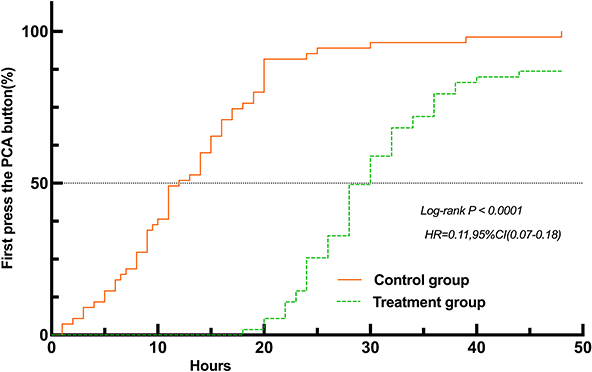 |
Figure 4 Kaplan-Meier Analysis of First Analgesia Demand Time After Preemptive ISI (Treatment group vs Control group). Abbreviations: ISI, Incision-site Infiltration; CI, indicates confidence interval; HR, hazard ratio. Notes: Treatment group: ropivacaine plus triamcinolone acetonide group; control group: ropivacaine alone group. |
Adverse Events
Neither group experienced any serious AEs during the intraoperative or postoperative period, and no additional AEs or drug reactions specifically associated with the ISI of triamcinolone acetonide were observed (Table 2).
Discussion
The main finding of this prospective, randomized, open-label clinical trial is that, compared with ropivacaine alone, preemptive ISI of ropivacaine plus triamcinolone acetonide can significantly reduce cumulative sufentanil consumption within 48h after craniotomy and improve pain control during postoperative 1month. These encouraging results provide a high level of evidence-based medical evidence for this multimodal analgesic strategy.
Although our previous study found a 30% reduction in analgesic consumption with dexamethasone as an adjuvant, this study showed that triamcinolone acetonide achieved 74% reduction. This markedly greater effect is likely due to the more potent local anti-inflammatory action of triamcinolone compared to that of water-soluble dexamethasone.19 Our findings regarding opioid reduction are inherently tied to the specific multimodal analgesic regimen employed at our institution. Consequently, the generalizability of these results is limited. Given the substantial variability in postoperative analgesia practices worldwide, the observed magnitude of the opioid-sparing effect may differ under alternative clinical protocols. The results of subgroup analysis indicated a consistent trend with sufentanil consumption among the five subgroups (age, sex, incision length, duration of surgery and surgical site), with no significant interaction. But subgroup analyses are underpowered, with sample size may not be sufficient to detect minor interactions, and therefore the results should be presented as exploratory rather than definitive.24,25 While this study excluded patients with severe systemic diseases (including uncontrolled hypertension, severe renal or hepatic impairment, mental disorders, serious neurological conditions, cardiomyopathies, arrhythmias, elevated intracranial pressure, or a history of brain trauma) and performed subgroup analyses by surgical site, the interpretation of our PCA outcomes could be further strengthened by a more comprehensive consideration of surgical site variability and underlying disease burden. Future studies should consider stratifying or adjusting for these factors to better isolate the treatment effect and enhance the clinical applicability of findings.
The median time to the first analgesic request through the PCA pump was 30 hours in the treatment group, which was significantly longer than that in the control group. It is important to note that PCA sufentanil consumption, though an objective endpoint, may reflect patient alertness in addition to pain intensity. Despite our protocol-driven exclusion of patients with major neurological complications, residual confounding from subtle differences in alertness cannot be completely ruled out. Incorporating objective measures of sedation or neurological recovery in future studies would help address this limitation.
In addition to reduced analgesic consumption, the treatment group exhibited notably lower NRS pain scores at every postoperative interval (from 2 h to 1 month) than the control group, suggesting potential clinical importance. Additional benefit of corticosteroid use is its postoperative antiemetic property. Postoperative nausea typically peaks within the first 24 h post-surgery, and IV dexamethasone administration has proven effective in preventing it.24 Moreover, periarticular corticosteroid administration exhibits an antiemetic effect following surgical procedures.26 This study showed that the preemptive ISI of triamcinolone acetonide can reduce PONV incidence at 4, 8, 24, and 48 h post-surgery. One possible reason is that the triamcinolone acetonide group had reduced cumulative sufentanil consumption, thereby lowering the incidence of opioid-related nausea and vomiting.2,6
Complications of glucocorticoid treatment such as hypertension, hyperglycemia, and peptic ulcers are frequently linked to high- and long-lasting systemic utilization.27 In this study, the average dose of triamcinolone acetonide was 7.33 mg per patient, which was lower than the clinical dose of 10–40 mg.21,27 Therefore, none of the patients experienced systemic side effects related to triamcinolone acetonide. Although no infections or wound complications were reported in this study, the use of corticosteroids in neurosurgical incisions raises theoretical concerns regarding wound healing. No adverse effects of triamcinolone acetonide on wound healing or infection rates were observed, and a higher proportion of patients in the triamcinolone acetonide group exhibited “good” wound healing. The finding that no adverse events were observed is not definitive given the limited sample size. Nevertheless, the theoretical risk of postoperative infection associated with steroid use warrants specific attention. Future research with larger sample sizes and adequate statistical power is essential to comprehensively assess the safety of pre-emptive ISI with ropivacaine combined with triamcinolone acetonide, including the potential for infection and other steroid-related AEs. Triamcinolone acetonide can minimize detrimental cascade by limiting localized edema, reducing edema at the edge of the wound, and thereby alleviating excessive tension on sutures or staples, maybe it is more conducive to promoting the healing of surgical incisions.28 It is reported that corticosteroids can reduce discomfort along the incision line after surgery. Whether it can reduce the formation of incision scars and lower the incidence of scar pain requires further studied.28
Post-craniotomy pain is superficial and attributed to surgical incision reflection of the underlying scalp muscles rather than the brain tissue itself. Prior research has elucidated a shared mechanism for incisional pain, wherein inflammatory mediators released following tissue damage activate the peripheral nociceptors. This abnormal stimulation, conveyed by Aδ and C-fibers, induces localized pain after tissue injury.17,29,30 Glucocorticoids counteract inflammatory responses by inhibiting elements, such as bradykinin, prostaglandins, and leukotrienes, thereby diminishing inflammation and its associated signs and symptoms. These results suggest that addition of triamcinolone acetonide alters the nociceptive cascade during craniotomy. Triamcinolone acetonide, which is water-insoluble, has a prolonged duration of action that extends for up to 14 days. Notably, our findings revealed sustained pain relief in the triamcinolone acetonide group even one month after craniotomy. However, whether there was a difference in chronic pain more than three months after craniotomy still requires an expanded sample size as well as an extended duration of follow-up.7,31
This study has several strengths. First, we successfully enrolled a predetermined number of patients based on our sample size calculation, and achieved high adherence and follow-up rates. Consequently, statistical inferences remained consistent across PP and ITT populations; Secondly, the trial’s pragmatic design and wide-ranging criteria enhance clinical applicability of the results to patients undergoing craniotomy; Thirdly, by closely mirroring daily clinical practices, the trial ensures high external validity for our findings; Lastly, our primary outcome (48 hours escape sufentanil use) serves as a comprehensive proxy for patients’ overall pain experience, thereby amplifying its clinical significance.
This trial had some limitations. First, as a pragmatic trial, blinding surgeons and anesthesiologists for treatment allocation is infeasible in practice. The lack of surgeons and anesthesiologists blinding could introduce potential bias due to different patient management during surgery. The absence of a protocol-specified dose per unit of incision length constitutes a limitation, as it may hinder the precise replication of this study; Secondly, our findings on opioid consumption are confined to initial 48 hours post-surgery, and pain levels were only assessed up to one month after, leaving the long-term adjuvant analgesic potential of triamcinolone uncertain based on our current data; Thirdly, since we examined the effects of triamcinolone at doses below 10 mg, we cannot generalize our conclusions to other dosages or treatment regimens of drug; Fourthly, although blood sugar levels were not evaluated as an outcome, prior studies suggest that any increase caused by triamcinolone is minimal; Fifthly, the postoperative analgesic regimen limited to sufentanil PCA with ondansetron, without adjunct non-opioid agents such as acetaminophen or NSAIDs. This may have contributed to the high opioid requirements observed in the control group. Sixth, the subgroup analyses were exploratory and underpowered, as the sample size was calculated for the primary outcome in the overall population. Furthermore, these analyses were not adjusted using a mixed-effects model. Therefore, no definitive conclusions should be drawn from these findings. Future research should delve into other potential subgroup factors, such as genetic profiles, lifestyle, and comorbidities to better understand the impact of interventions across diverse populations. Seventh, absence of pre- and postoperative inflammatory marker measurements (eg, IL-6, CRP) represents a limitation of this study. While we hypothesize that the prolonged analgesic effect observed with triamcinolone acetonide is mediated by its anti-inflammatory properties, we cannot provide direct biochemical evidence to support this mechanism. Future studies should incorporate serial measurements of relevant inflammatory cytokines to confirm the mechanistic pathway. It is important to note that PCA sufentanil consumption, though an objective endpoint, may reflect patient alertness in addition to pain intensity. Despite our protocol-driven exclusion of patients with major neurological complications, residual confounding from subtle differences in alertness cannot be completely ruled out. Incorporating objective measures of sedation or neurological recovery in future studies would help address this limitation. Finally, our trial’s findings may not be applicable to patients who do not meet the eligibility criteria, highlighting the need for further research in broader patient groups.
Conclusion
Pre-emptive ISI with triamcinolone acetonide combined with ropivacaine was associated with enhanced postoperative analgesia, reduced sufentanil consumption, and a lower incidence of PONV in craniotomy patients, with no severe AEs reported. Although these preliminary results suggest a potential role for this combination in multimodal analgesia, larger multicenter trials are warranted to validate its efficacy, generalizability, and safety.
Abbreviations
ASA, American Society of Anesthesiologists; AEs, adverse events; BMI, body mass index; ICH, intracranial hemorrhage; ICP, intracranial pressure; IRB, Institutional Review Board; ISI, incision-site infiltration; ITT, intention-to-treat; LOS, length of stay; MAP, mean arterial pressure; NRS, numerical rating scale; NSAIDs, nonsteroidal anti-inflammatory drugs; PCA, patient-controlled analgesia; PONV, postoperative nausea and vomiting; PP, per-protocol.
Data Sharing Statement
The data supporting the findings of this study are available upon request from the corresponding author (Fang Luo, email: [email protected]). The data were not publicly available due to privacy or ethical restrictions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sector.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mestdagh FP, Lavand’homme PM, Pirard G, Joshi GP, Sauter AR, Van de Velde M. Pain management after elective craniotomy A systematic review with procedure-specific postoperative pain management (PROSPECT) recommendations. Eur J Anaesthesiol. 2023;40:747–12.
2. Hanley C, Ladha KS, Clarke HA, Cuthbertson BC, Wijeysundera DN. Association of postoperative complications with persistent post-surgical pain: a multicentre prospective cohort study. Br J Anaesth. 2022;128(2):311e320.
3. Liu Y, Xiao S, Yang H, et al. Postoperative pain-related outcomes and perioperative pain management in China: a population-based study. Lancet Regional Health. 2023;39:100822. doi:10.1016/j.lanwpc.2023.100822
4. Thibault M, Girard F, Moumdjian R, Chouinard P, Boudreault D, Ruel M. Craniotomy site influences postoperative pain following neurosurgical procedures: a retrospective study. Can J Anesth. 2007;54(7):544–548.
5. Richebé P, Capdevila X, Rivat C. Persistent postsurgical pain pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129:590–607.
6. Sriganesh K, Bharadwaj S, Shanthanna H, Rao GSU, Kramer BW, Sathyaprabha TN. Opioid versus nonopioid analgesia for craniotomy: a systematic review and meta-analysis of randomized controlled trials. World Neurosurg. 2023;173:e66–e75. doi:10.1016/j.wneu.2023.01.111
7. Carley ME, Chaparro LE, Choinière M, et al. Pharmacotherapy for the prevention of chronic pain after surgery in adults: an updated systematic review and meta-analysis. Anesthesiology. 2021;135:304–325.
8. Yeh SJ, Tang SC, Tsai LK, Jeng JS. Effects of Non-aspirin nonsteroidal anti-inflammatory drugs on acute intracerebral hemorrhage. Ann Clin Transl Neurol. 2025;12(11):2328–2334.
9. Ungprasert P, Matteson EL, Thongprayoon C. Nonaspirin nonsteroidal anti-inflammatory drugs and risk of hemorrhagic stroke. Stroke. 2016;47(2):356–364.
10. Williams DL, Pemberton E, Leslie K. Effect of intravenous parecoxib on post-craniotomy pain. Br J Anaesth. 2011;107(3):398–403.
11. Jayaram K, Srilata M, Kulkarni D, Ramachandran G. Regional anesthesia to scalp for craniotomy: innovation with innervation. J Neurosurg Anesthesiol. 2015;28(1):32–37.
12. Vadivelu N, Kai AM, Tran D, Kodumudi G, Legler A, Ayrian E. Options for perioperative pain management in neurosurgery. J Pain Res. 2016;9:37–47. doi:10.2147/JPR.S85782
13. Skutulienė J, Banevičius G, Bilskienė D, Macas A. The effect of scalp block or local wound infiltration versus systemic analgesia on post-craniotomy pain relief. Acta Neurochirurgica. 2022;164(5):1375–1379. doi:10.1007/s00701-021-04886-0
14. Pinho-Ribeiro FA, Verri WA, Chiu IM. Nociceptor sensory neuron–immune interactions in pain and inflammation. Trends Immunol. 2017;38(1):5–19. doi:10.1016/j.it.2016.10.001
15. García-Domínguez M. Injury-driven structural and molecular modifications in nociceptors. Biology. 2025;14(7):788.
16. Akcil EF, Dilmen OK, Vehid H, Ibısoglu LS, Tunali Y. Which one is more effective for analgesia in infratentorial craniotomy? The scalp block or local anesthetic infiltration. Clin Neurol Neurosurg. 2017;154:98–103.
17. Brennan TJ, Zahn PK, Pogatzki-Zahn EM. Mechanisms of incisional pain. Anesthesiology Clin N Am. 2005;23:1–20.
18. Jia YT, Ren H, Wang T, Luo F. Pre-emptive scalp infiltration with dexamethasone plus ropivacaine for postoperative pain after craniotomy: a protocol for a prospective, randomized controlled trial. J Pain Res. 2019;12:1709–1719.
19. Zhao CM, Wang SH, Pan YS, Ji N, Luo F. Pre-emptive incision-site infiltration with ropivacaine plus dexamethasone for postoperative pain after supratentorial craniotomy: a prospective randomized controlled trial. J Pain Res. 2021;14:1071–1082. doi:10.2147/JPR.S300943
20. Han XY, Ren T, Wang Y, Ji N, Luo F. Postoperative analgesic efficacy and safety of ropivacaine plus diprospan for preemptive scalp infiltration in patients undergoing craniotomy: a prospective randomized controlled trial. Anesth Analg. 2022;135(6):1253–1261. doi:10.1213/ANE.0000000000005971
21. Bodick N, Lufkin J, Willwerth C, et al. An intra-articular, extended-release formulation of triamcinolone acetonide prolongs and amplifies analgesic effect in patients with osteoarthritis of the knee: a randomized clinical trial. J Bone Joint Surg Am. 2015;97(11):877–888. doi:10.2106/JBJS.N.00918
22. Kim B, Lee H, Chung H, et al. The efficacy of topical bupivacaine and triamcinolone acetonide injection in the relief of pain after endoscopic submucosal dissection for gastric neoplasia: a randomized double-blind, placebo-controlled trial. Surg Endosc. 2015;29(3):714–722. doi:10.1007/s00464-014-3730-4
23. Chaki T, Sugino S, Janicki PK, et al. Efficacy and safety of a lidocaine and ropivacaine mixture for scalp nerve block and local infiltration anesthesia in patients undergoing awake craniotomy. J Neurosurg Anesthesiol. 2014;28(1):1–5.
24. Gasbjerg KS, Hägi-Pedersen D, Lunn TH, et al. Effect of dexamethasone as an analgesic adjuvant to multimodal pain treatment after total knee arthroplasty: randomised clinical trial. BMJ. 2022;376:e067325. doi:10.1136/bmj-2021-067325
25. Chowdhury T, Garg R, Sheshadri V, et al. Perioperative factors contributing the post-craniotomy pain: a synthesis of concepts. Front Med. 2017;4:23. doi:10.3389/fmed.2017.00023
26. Hanson P, Kivitz A, Mehra P, et al. Safety and systemic exposure of triamcinolone acetonide following ultrasound-guided intra-articular injection of triamcinolone extended-release or standard triamcinolone acetonide in patients with shoulder osteoarthritis: an open-label, randomized study. Drugs R&D. 2021;21:285–293.
27. Wang X, Dong WF, Song Z, et al. Comparing the effectiveness of betamethasone and triamcinolone acetonide in multimodal cocktail intercostal injection for chest pain after harvesting costal cartilage: a prospective, double-blind, randomized controlled study. Aesth Plast Surg. 2023;48(6):1111–1117.
28. Wesley CK, Teo LHY, Xu T, Unger RH, Unger WP. The influence of peri-incisional triamcinolone acetonide injection on wound edge apposition. J Dermatological Treat. 2014;25(4):345–349. doi:10.3109/09546634.2012.755253
29. Gray LC, Matta BF. Acute and chronic pain following craniotomy: a review. Anaesthesia. 2005;60(7):693–704. doi:10.1111/j.1365-2044.2005.03997.x
30. Stamenkovic DM, Bezmarevic M, Bojic S, et al. Updates on wound infiltration use for postoperative pain management: a narrative review. J Clin Med. 2021;10:4659.
31. Phoowanakulchai S, Naito Y, Kawaguchi M. Persistent incisional pain at 1 year after craniotomy: a retrospective observational study. BMC Anesthesiol. 2023;23:115.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Preemptive Topical Lidocaine 5% Plaster in the Prevention of Post-Craniotomy Pain, a Randomized Clinical Trial
Han X, Yang Y, Ren T, Ji N, Luo F
Journal of Pain Research 2024, 17:4251-4261
Published Date: 13 December 2024
Comparing Liposomal Bupivacaine and Ropivacaine in Serratus Anterior Plane Block for Thoracoscopic Lobectomy: A Randomized Controlled Trial
Zhang Y, Li W, Wei A, Chen S, Wang X
Drug Design, Development and Therapy 2025, 19:4717-4726
Published Date: 4 June 2025