Back to Journals » Journal of Pain Research » Volume 18
Effectiveness of Isokinetic Muscle Strength Training on Knee Osteoarthritis Patients: A Systematic Review with Meta-Analysis
Authors Chang BY, Chen L, Xu HC, Hao JH, Wang HJ ![]()
Received 23 September 2025
Accepted for publication 18 December 2025
Published 28 December 2025 Volume 2025:18 Pages 7179—7193
DOI https://doi.org/10.2147/JPR.S566838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Alaa Abd-Elsayed
Bo-Ya Chang,1 Long Chen,1 Hui-Chao Xu,1 Jian-Heng Hao,2,* Hai-Jun Wang1,*
1The Second Clinical College, Shanxi University of Chinese Medicine, Jinzhong, Shanxi Province, 030619, People’s Republic of China; 2Department of Clinical Medicine, Shanxi University of Medicine, Lvliang, Shanxi Province, 032200, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hai-Jun Wang, The Second Clinical College, Shanxi University of Chinese Medicine, Jinzhong, Shanxi Province, 030619, People’s Republic of China, Email [email protected] Jian-Heng Hao, Department of Optometry, Shanxi University of Medicine, Lvliang, Shanxi Province, 032200, People’s Republic of China, Email [email protected]
Purpose: This study systematically evaluated the effects of isokinetic muscle strength training (IMST) on pain, function, and muscle performance in patients with knee osteoarthritis (KOA).
Patients and Methods: Randomized controlled trials comparing IMST with other interventions for KOA were searched across multiple international and Chinese databases up to January 2025. Two investigators independently screened literature, extracted data, and assessed risk of bias according to the Cochrane Handbook Version 6.1.0. The RevMan 5.4 software was used to perform the meta-analysis. Overall quality of evidence was rated using GRADE approach.
Results: Nineteen RCTs involving 1386 patients were finally included. Three of which had high risk bias. Compared with other treatments, IMST showed a borderline improvement in Lysholm score (MD = 1.21, 95% CI: [− 0.62, 3.04], I2= 95%, very low certainty), and tended to enhance extensor peak torque (MD = 4.12, 95% CI: [− 0.17, 8.41], I2= 74%, very low certainty) while significantly increasing flexor peak torque (MD = 7.94, 95% CI: [4.23, 11.66], I2= 71%, low certainty). Besides, IMST also significantly reduced VAS scores (MD = − 0.64, 95% CI: [− 1.19, − 0.10], I2= 95%, Moderate certainty) and showed a trend toward lower (MD = − 6.96, 95% CI: [− 15.85, 1.92], I2= 98%, Moderate certainty), indicating overall improvements in knee function, pain, and stiffness.
Conclusion: IMST appears to improve pain and function in patients with KOA, but the overall certainty of evidence is limited. Further high-quality RCTs are needed to confirm these benefits and guide clinical practice.
Keywords: Isokinetic exercise, knee osteoarthritis, randomized controlled trials, meta-analysis, GRADE
Introduction
Osteoarthritis (OA) is a chronic degenerative joint disorder characterized by progressive cartilage destruction, subchondral bone sclerosis and osteophyte formation.1,2 Globally, the prevalence of knee osteoarthritis (KOA) was estimated at approximately 375 million cases in 2021, representing about 22.9% of individuals aged 40 and over. In China, the prevalence of radiographic KOA is around 2.79%, affecting nearly 39 million individuals based on recent national surveys, underscoring a substantial public-health burden.3
KOA is a multifactorial and complex disorder characterized by pathological alterations in joint structures and surrounding musculoskeletal tissues.4 The primary risk factors for KOA include advanced age, female sex, obesity, prior joint injuries, genetic predisposition, and occupational activities involving prolonged repetitive knee loading. From a biomechanical perspective, KOA is commonly associated with increased varus or valgus knee deformities, reduced knee flexion during the stance phase, and other gait deviations, which contribute to elevated joint contact stress and accelerated cartilage degeneration. From a kinetic standpoint, patients often demonstrate decreased peak torque in the quadriceps and hamstring muscle groups, altered muscle activation patterns, and impaired proprioception, all of which compromise joint stability.5 Research indicates that the functional status of the muscles surrounding the knee joint is closely linked to its pathogenesis. These muscles not only contribute to locomotion but also play a critical role in attenuating mechanical loads, preserving proprioceptive feedback, and ensuring joint stability, all of which are essential for protecting the integrity of the joint structure.6 Therefore, muscle strength training is an essential, noninvasive approach to restore function and stability.7 Recent studies have compared different isokinetic training modes, showing that eccentric and concentric contractions may yield distinct neuromuscular adaptations, and that variations in isokinetic angular velocity (eg, 60°/s vs 120°/s) can influence torque production and pain relief outcomes.8,9
During isokinetic muscle strength training (IMST), physiological adaptations in the osteoarthritic knee include improved neuromuscular activation, enhanced motor unit recruitment, and muscle hypertrophy. These changes promote better synovial fluid circulation and nutrient exchange, reduce joint effusion, and may downregulate pro-inflammatory cytokines. IMST can also alleviate pain through endorphin release and improve joint stability by balancing agonist–antagonist muscle groups, ultimately slowing disease progression.10 Clinically, improvements in key indicators such as the Visual Analogue Scale (VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and peak torque are directly related to pain reduction, functional mobility, and independent living in KOA patients. Importantly, IMST provides a safe and quantifiable exercise modality, particularly suitable for older adults11 or patients with comorbid conditions such as hypertension and diabetes.12
However, previous systematic reviews investigating IMST were published several years ago and often combined it with other interventions, making it difficult to isolate its independent effects.13,14 Consequently, evidence guiding whether IMST should be prioritized over other exercise modalities remains unclear. To address these gaps, this study aimed to conduct a focused and comprehensive meta-analysis evaluating the independent effects of IMST on muscle function, pain, and joint performance in patients with KOA, thereby providing updated and clinically relevant evidence for rehabilitation decision-making.
Materials and Methods
Search Strategy
The Cochrane Handbook for Systematic Reviews of Interventions9 and PRISMA Statement10 were used to guide the conduct and reporting of this review. Six databases PubMed, Cochrane Library, Web of Science, CNKI, CBM and WanFang were searched from their respective inception dates up to January 1, 2025, with no language restrictions. The inception date refers to the first year each database was indexed (PubMed: 1966; Cochrane Library: 1996; Web of Science: 1990; CNKI, CBM, and WanFang: 1998–2000). The same search strategy was applied across all databases. In addition, we conducted supplementary searches through the WHO International Clinical Trials Registry Platform (ICTRP) Search Portal and grey literature. The main search strategies were as follows: (“knee osteoarthritis” OR “osteoarthritis” OR “knee joint osteoarthritis” OR “osteoarthritis of knee” OR “osteoarthritis of knee joint” OR “OA”) AND (“isokinetic exercise” OR “isokinetic training” OR “isokinetic muscle strengthen” OR “isokinetic muscle strength training”). We have register our study protocol in the PROSPERO (CRD42024600498). Since all data and analyses were derived from an existing database, this study did not require ethical review.
Inclusion and Exclusion Criteria
Studies were selected based on the PICO (Population, Intervention, Comparison, Outcome) framework to ensure alignment with the review’s objectives. The population of interest comprised patients diagnosed with KOA. The intervention focused on IMST, defined as exercises conducted at a constant angular velocity to assess and enhance knee flexor and extensor strength. Comparators included other forms of treatment, such as isometric or isotonic exercises, traditional Chinese medicine interventions, or no active treatment. Outcomes prioritized for inclusion were measures of pain, knee function, and muscle performance, with predefined primary endpoints encompassing the Lysholm knee function score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total and subscale scores (pain, stiffness, and function), visual analogue scale (VAS) for pain, and peak torque (PT) values for knee flexors and extensors.
To maintain methodological rigor and minimize heterogeneity, we applied strict exclusion criteria. Studies involving mixed interventions (eg, IMST combined with neuromuscular electrical stimulation or other adjunctive therapies) or mixed populations (eg, patients with concurrent knee and hip osteoarthritis without stratified outcomes for KOA) were excluded, as their incorporation could confound the isolated effects of IMST and inflate variability in pooled estimates. Additionally, trials lacking extractable numerical data for effect size calculations, those published only as conference abstracts or letters without full methodological details, or investigations failing to report at least one primary outcome were not included in the quantitative synthesis.
Study Selection, Data Extraction and Risk of Bias Assessment
Eligible studies were screened in their entirety and developed a data extraction form, and the information including authors and year of publication, publication type, sample size, gender, type of treatment was recorded in an Excel spreadsheet. We pre-tested it on five studies and subsequently adapted the final version. Two reviewers independently conducted trial screening and data extraction, when the disagreement existed, conflicts were resolved by the third reviewer. Study authors contacted to request additional information if a study was eligible based on the inclusion criteria, but not all required data could be retrieved from the full-text. Overall, we adopted a conservative procedure in that we excluded studies for which ambiguity about the primary data source could not be resolved or the information necessary for effect size calculation could not be acquired. Two study investigators (Jian-Heng Hao, Hai-jun Wang) independently rated the quality of included trials using the Cochrane Risk of Bias Tool.
Heterogeneity, Sensitivity, and Publication Bias
According to the Cochrane Handbook Version 6.1.0, we evaluated statistical heterogeneity using the I2 statistic, with values over 50% suggesting substantial heterogeneity.15 The “Leave-one-out” method is used in sensitivity analyses to check for outliers that potentially influence the results of the meta-analysis disproportionately. All analyses were performed repeatedly with each study removed once to detect whether overall results depend on a single study. Publication bias was assessed by funnel plot.16 If any bias could be assumed based on these analyses, we planned to apply the trim-and-fill procedure to estimate the unbiased overall effect.
Data Synthesis and Statistical Analysis
In analyzing continuous data, we calculated MDs and 95% CIs. To account for clinical and methodological heterogeneity. To aid in interpretation of MDs, we used the approach from Bliddal and Christensen. The fixed-effects model and the random-effects model are based on different assumptions. The results of meta-analysis using fixed-effect models are limited to specific populations.17 As we cannot expect these studies included in the research to show the same widespread impact; the fact that the studies were conducted under different conditions (ie, days of treatment, etc.) could indispensably cause differences among the results. Thus, in the identification of effect sizes during the present meta-analytical processes, analyses were conducted according to the random effects model.18 The whole process of data analysis was performed in Review Manager 5.4.
Certainty Assessment
We utilized the GRADE approach to assess the confidence in estimates derived from meta-analysis of efficacy outcomes.19 In this methodology, initial high confidence is assigned to direct evidence from RCTs, which may be subsequently downgraded based on factors such as bias risk, indirectness, imprecision, inconsistency, and/or publication bias, resulting in moderate, low, or very low levels of confidence. The rating for indirect estimates commences at the lowest rating among the two pairwise estimates that contribute as first-order loops to the indirect estimate but can be further downgraded due to imprecision or intransitivity (differences between studies regarding clinical or methodological characteristics). If direct and indirect estimates were similar, then the higher of their rating can be assigned to the meta-analysis estimates.
Results
Selection and Characteristics of Studies
A flow diagram showed in Figure 1. From a total 786 unique studies identified using our search strategy, 201 trials were removed because of duplication. Five hundred and two trials were removed according to titles and abstracts. After excluded 64 unsuitable full-text RCTs, 19 full-text publications met the requirements for the final inclusion.8,20–37 As shown in Table 1, a total of 19 trials involving 1386 KOA were included, the duration of intervention was range from 10 days to 20 weeks. Twelve RCTs (63.16%) were published in China, four of them was published in English language and others were in Chinese. Among the results of interventions, seven trials made a comparison between the IMST and non-intervention. Six trials made a comparison between the IMST and isometric exercise. Three trials made a comparison between the IMST with traditional Chinese medicine treatment (acupuncture, warm moxibustion and Tuina).
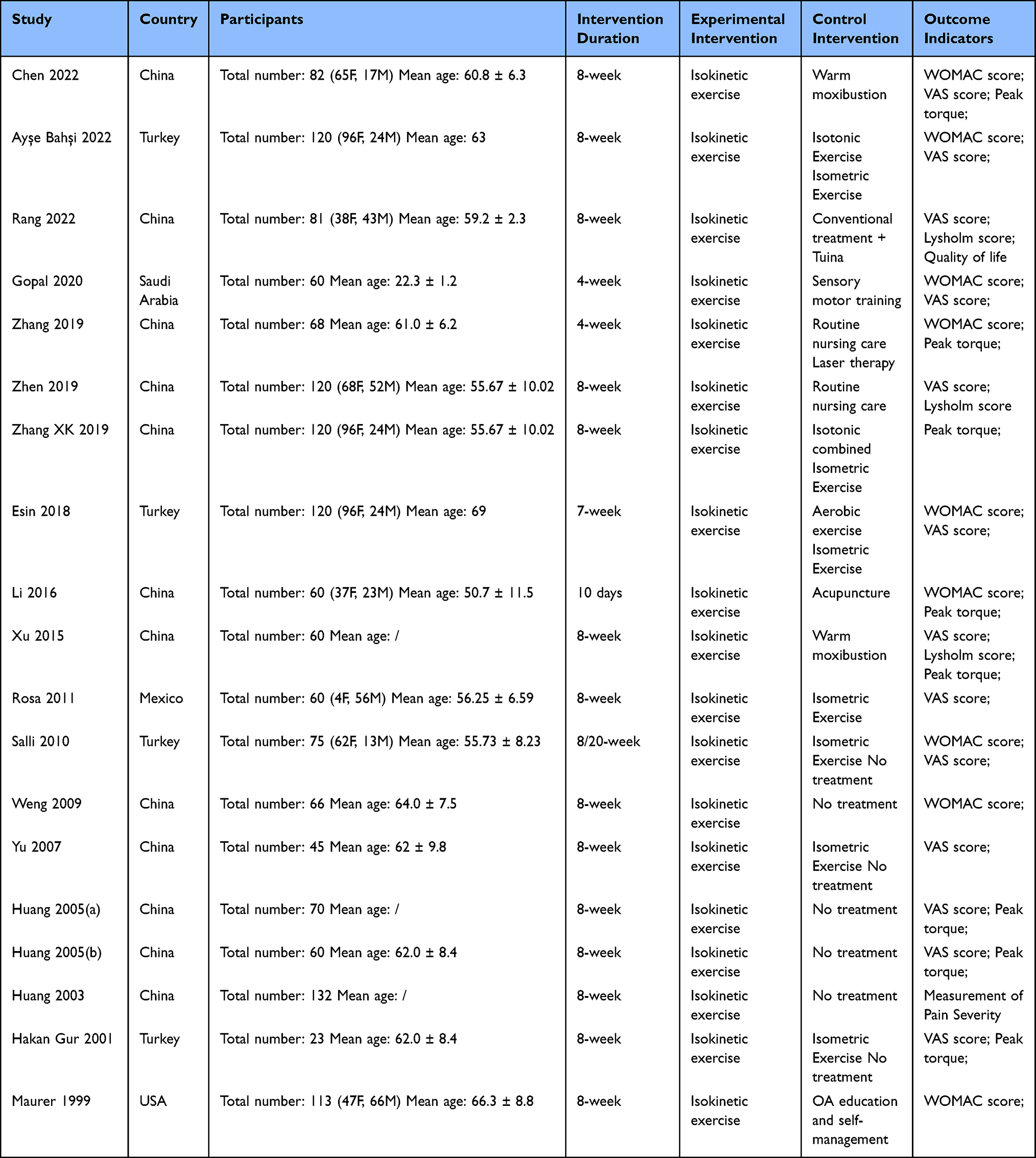 |
Table 1 Characteristic of the Studies Included in the Meta-Analysis |
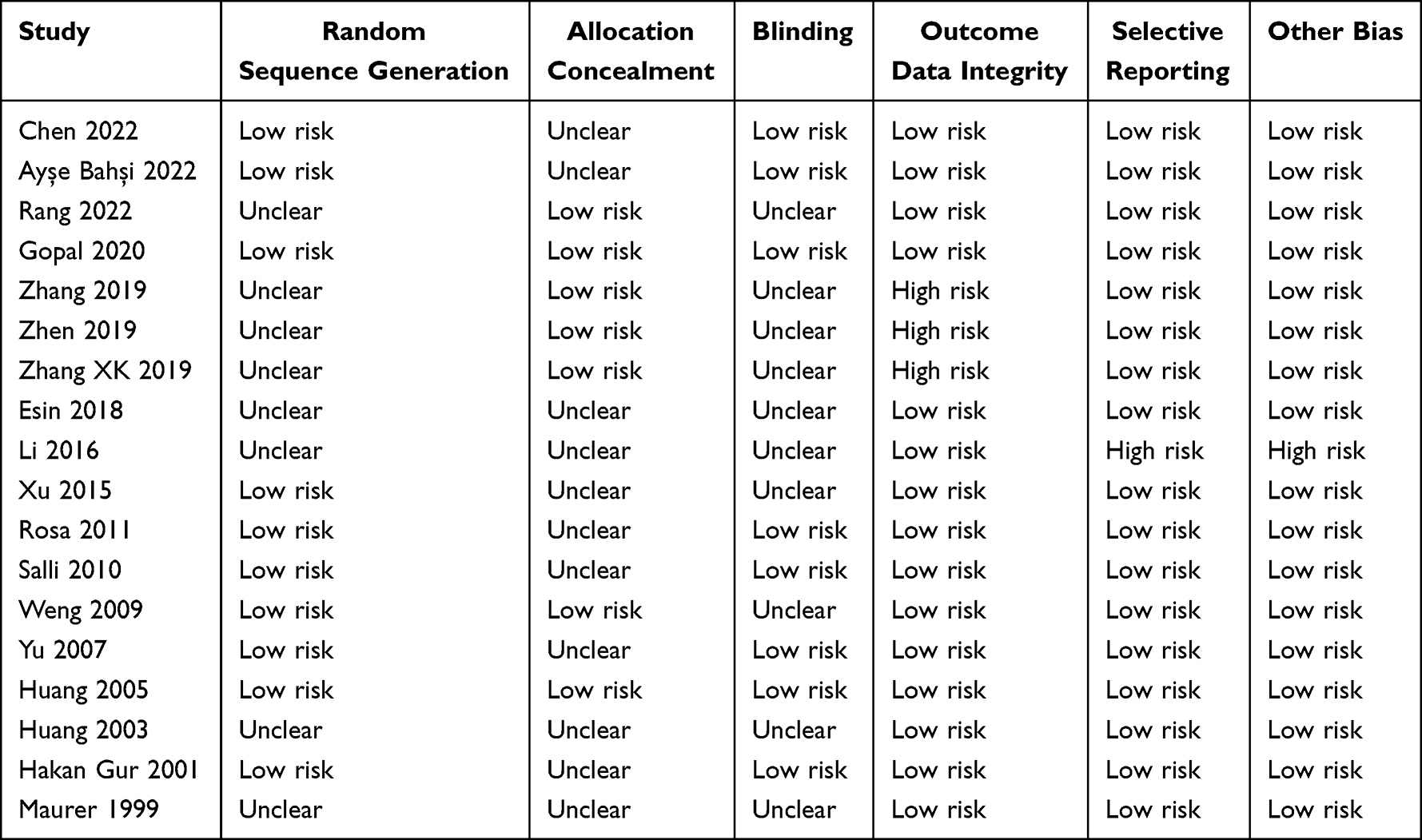 |
Table 2 Risk of Bias Assessment of Included Studies |
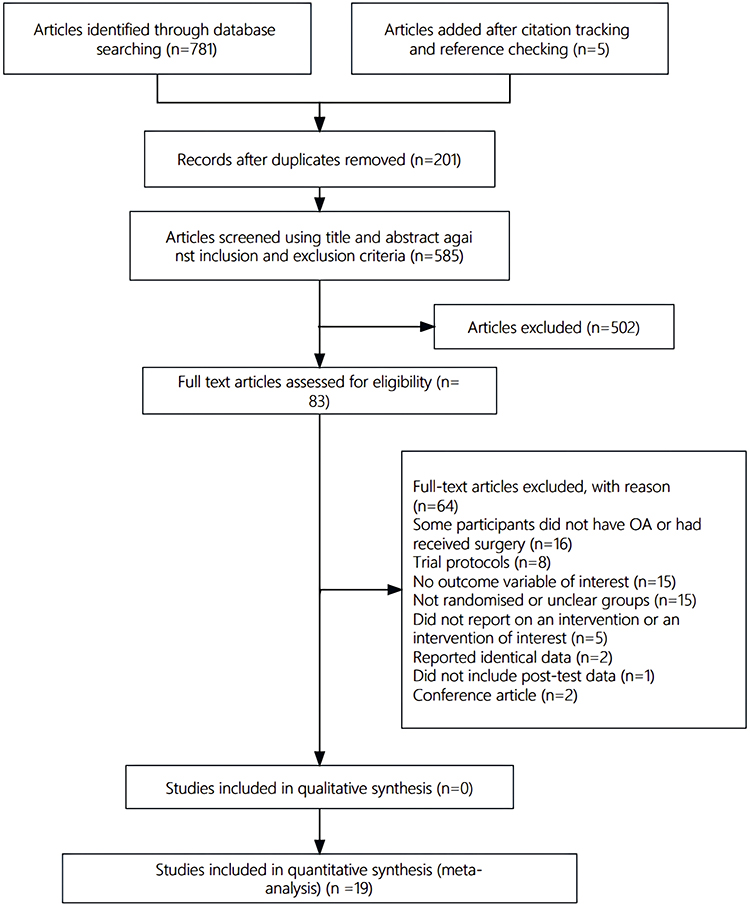 |
Figure 1 Flow diagram of the literature screening. |
Risk of Bias
As shown in Figure 2, 47.3% trials (n = 9) were judged as “low risk of bias” in the random sequence generation analysis. About 73.68% (n = 14) were judged as “unclear risk of bias” in the blinding of outcome assessment and blinding of participants because of unclear reports. About 89.47% (n = 17) were judged as “low risk bias” in the analysis of incomplete outcome data and selective reports (Table 2).
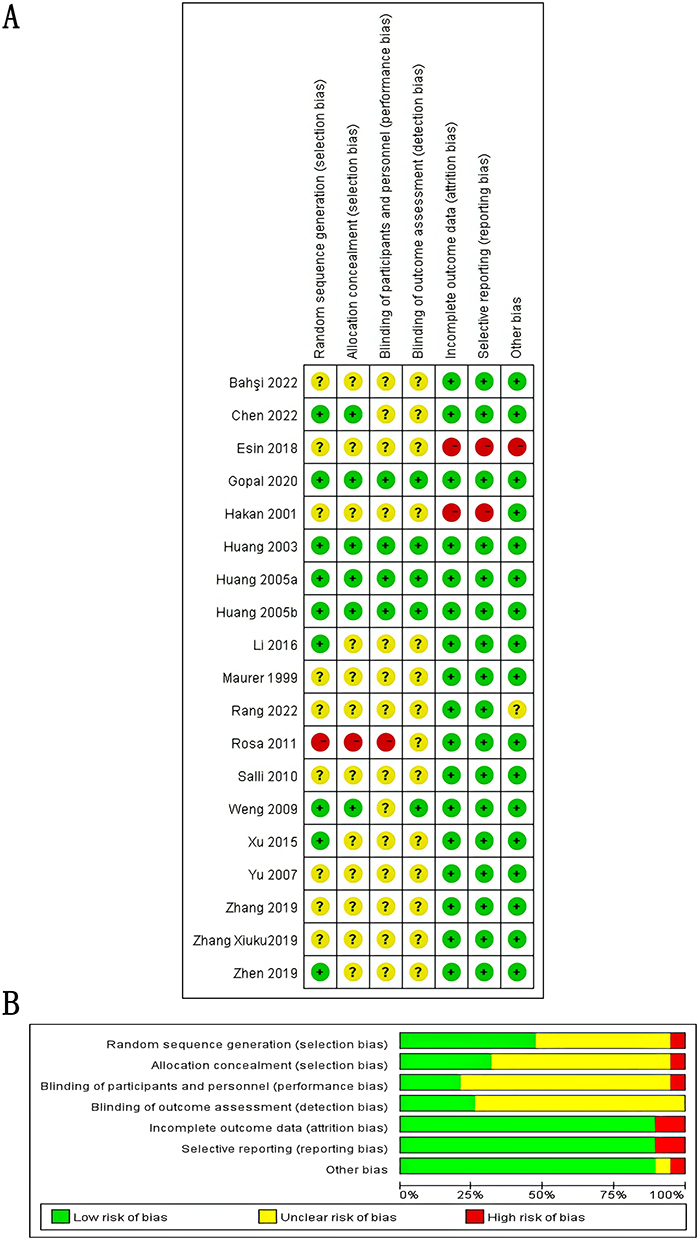 |
Figure 2 Risk of bias assessments. Notes: (A) risk of bias for each included study.“+”: low risk of bias; “-”: high risk of bias; “?”: unclear risk of bias. (B) overall risk of bias of included studies. |
Quality of Included Trials
According to the Cochrane Risk of Bias assessment, the methodological quality of the included studies ranged from low to moderate. Table 3 provides a detailed summary of the risk of bias for each included trial. Overall, random sequence generation was adequately described in nine studies, whereas allocation concealment and blinding were frequently unclear. Only a few studies fully reported both randomization and blinding procedures, raising concerns about potential performance bias. In contrast, outcome data completeness and the risk of selective reporting were generally rated as low. The high proportion of “unclear” judgments across multiple domains indicates that many studies suffered from inadequate methodological reporting, which may compromise the reliability of pooled effect estimates.
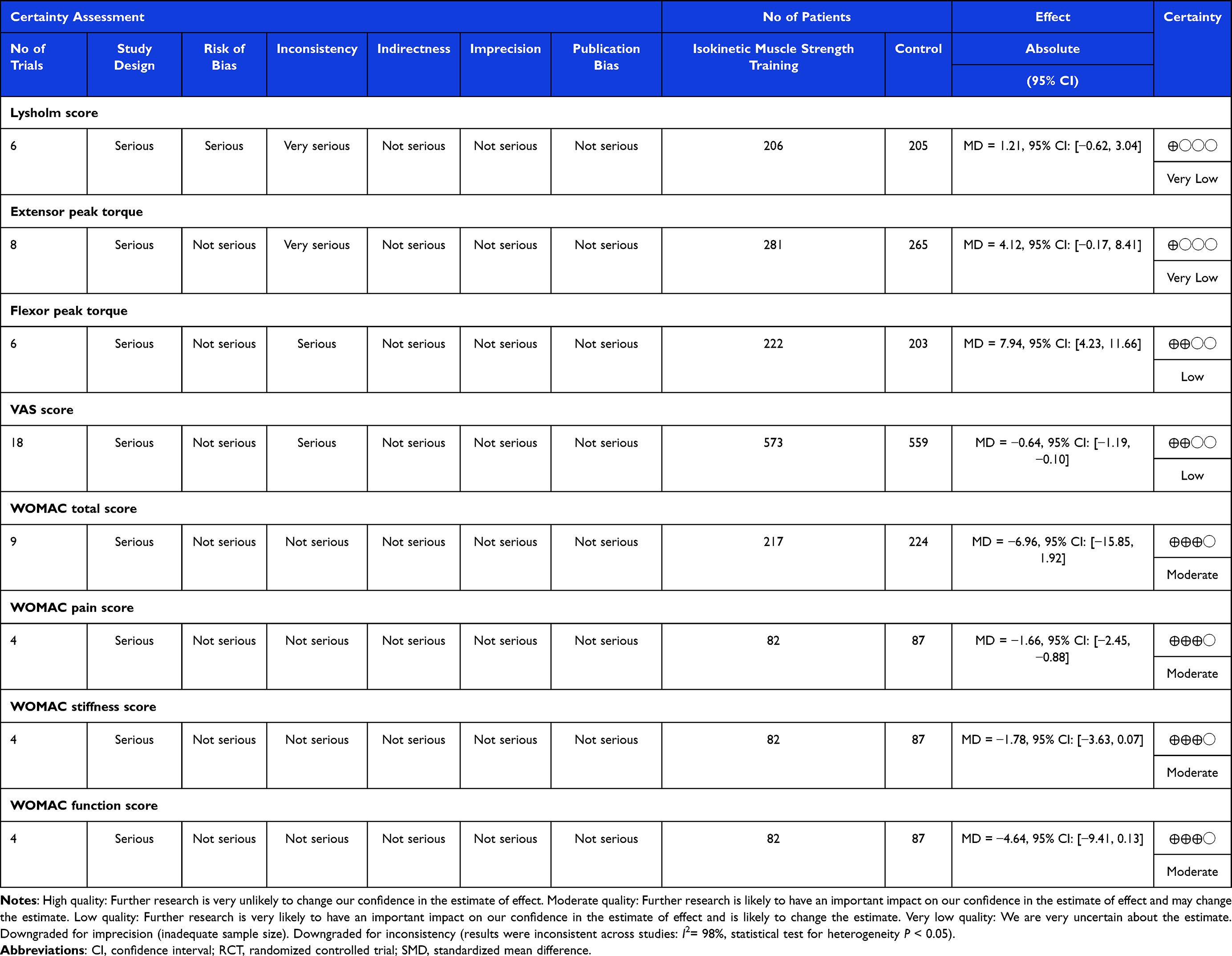 |
Table 3 Summary of Finding |
Synthesis Analysis
Lysholm Score
Six trials involving 411 patients evaluated the effectiveness of IMST for KOA patients. The random effect meta-analysis showed that, compared with other treatments, IMST showed a borderline improvement in the Lysholm score of KOA patients (MD = 1.21, 95% CI: [−0.62, 3.04], I2= 95%, P < 0.05). The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 3).
 |
Figure 3 Meta-analysis for Lysholm score of KOA patients. |
Extensor Peak Torque
Eight trials involving 546 patients evaluated the effectiveness of IMST for KOA patients. The random effect meta-analysis showed that, compared with other treatments, IMST tended to improve extensor peak torque (MD = 4.12, 95% CI: [−0.17, 8.41], I2= 74%, P < 0.05). The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 4).
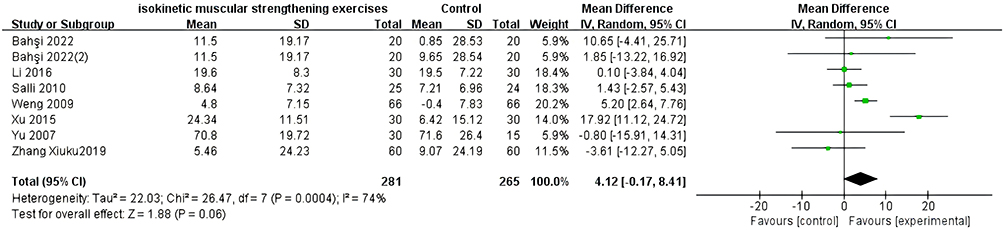 |
Figure 4 Meta-analysis for extensor peak torque of KOA patients. |
Flexor Peak Torque
Six trials involving 425 patients evaluated the effectiveness of IMST for KOA patients. The random effect meta-analysis showed that, compared with other treatments, IMST can significantly increase the flexor peak torque of KOA patients (MD = 7.94, 95% CI: [4.23, 11.66], I2= 71%, P < 0.05). The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 5).
 |
Figure 5 Meta-analysis for the flexor peak torque of KOA patients. |
VAS Score
Eighteen trials involving 1132 patients evaluated the effectiveness of IMST for KOA patients. The random effect meta-analysis showed that, compared with other treatments, IMST can decrease the VAS score of KOA patients (MD = −0.64, 95% CI: [−1.19, −0.10], I2= 95%, P < 0.05). The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 6).
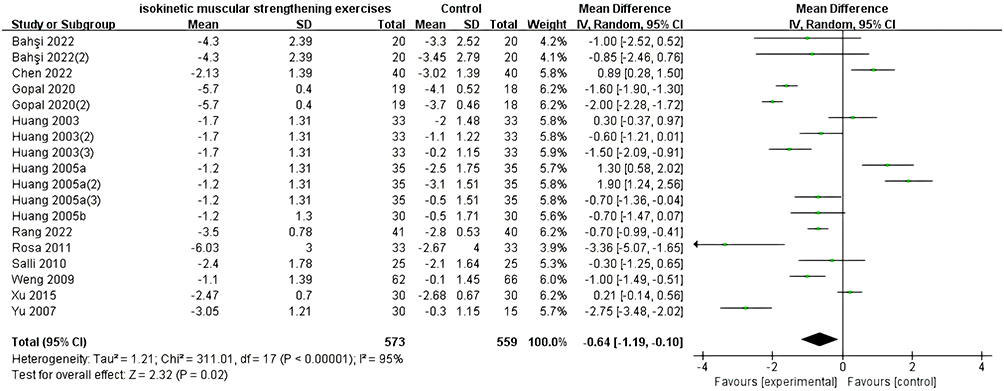 |
Figure 6 Meta-analysis for VAS score of KOA patients. |
WOMAC Total Score
The efficacy of IMST in treating patients with KOA was evaluated in 9 trials involving 441 patients. The random effect meta-analysis showed that, compared with other treatments, IMST showed a non-significant trend toward lower WOMAC total score of KOA patients (MD = −6.96, 95% CI: [−15.85, 1.92], I2= 98%, P < 0.05), indicating a possible functional improvement. The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 7).
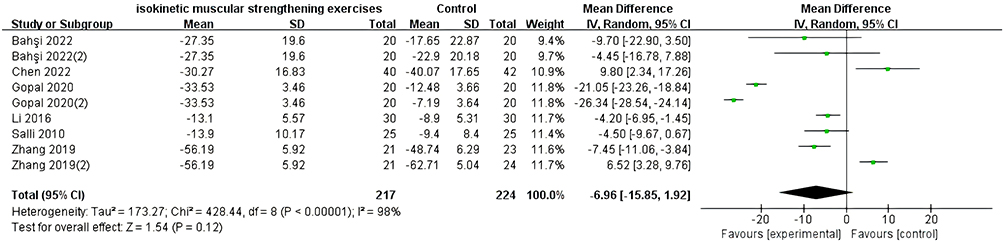 |
Figure 7 Meta-analysis for WOMAC total score of KOA patients. |
WOMAC Sub-Score
Four trials involving 169 patients showed that IMST significantly reduced WOMAC pain score (MD = −1.66, 95% CI: [−2.45, −0.88], I2= 0%, P > 0.91); whereas improvements in stiffness (MD = −1.78, 95% CI: [−3.63, 0.07], I2= 34%, P > 0.21) and function subscales (MD = −4.64, 95% CI: [−9.41, 0.13], I2= 0%, P > 0.40) showed non-significant trends. The sensitivity analysis showed that no single study significantly affected overall heterogeneity (Figure 8).
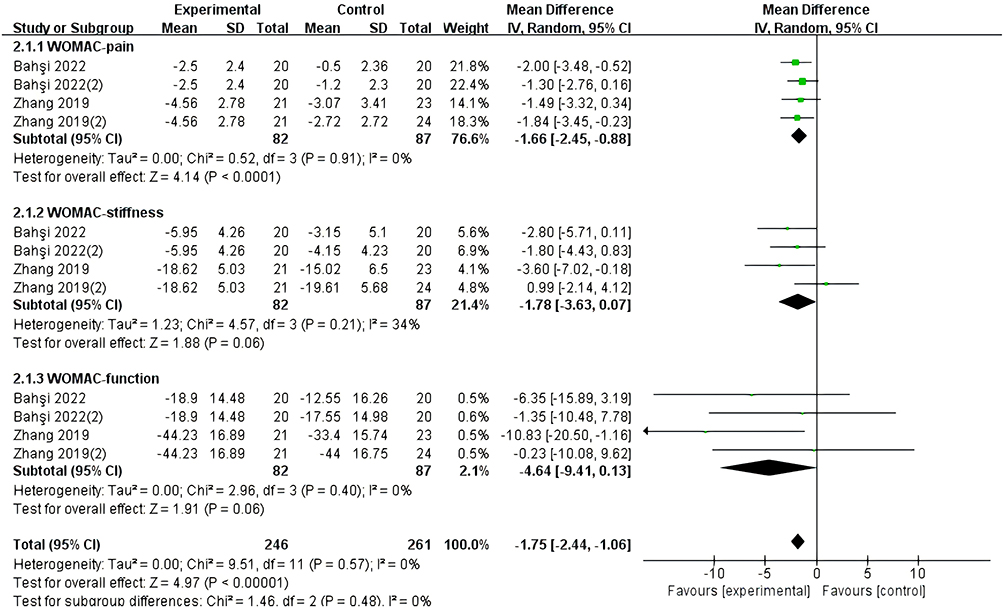 |
Figure 8 Meta-analysis for WOMAC sub-score of KOA patients. |
Sensitivity and Publication Bias
According to the “leave-one-out” strategy, 18 effect sizes of VAS score estimated values from −0.39 to −0.31 were got, indicated that there were no particularly prominent sensitivity issues in the included literature. Funnel plot shown a certain publication bias, and there was no obvious change in the results after the trim-and-fill estimate (Figure 9).
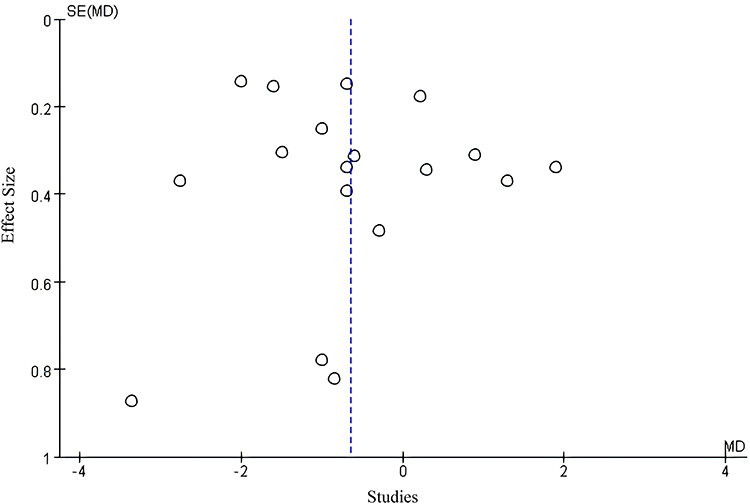 |
Figure 9 Publication bias of included studies. |
Evidence Certainty
As shown in Table 3, the certainty of the evidence from very low to moderate according to the assessments of inconsistency (high heterogeneity between studies), study design (methodology, such as trial design), and other considerations (such as risk of bias or small effect sizes). Among all the outcomes, outcomes of Lysholm score and extensor peak torque were rated as very low-quality evidence. Flexor peak torque was rated as low evidence. VAS score, WOMAC relevant scores were rated as moderate level.
Discussion
This study focused on the clinical effect of IMST on improving muscle function in knee osteoarthritis. A total of 19 RCTs were included, involving 1386 patients. Through a meta-analysis of the main clinical indicators reflecting muscle function, the results showed that IMST could improve Lysholm’s knee function score, increase the both flexor and extensor peak torque value, and reduce VAS and WOMAC scores. It showed that muscle strength training is effective in improving muscle function, relieving pain and improving peak torque.
At present, the management of KOA primarily involves surgical intervention, medication therapy, and rehabilitation. Rehabilitation treatment, particularly muscle strength training, offers a safe, efficient, and adaptable approach to breaking the cycle of muscle atrophy, mechanical instability, and pain.27 Muscle strength training encompasses isometric exercises for muscle strengthening without joint movement; isotonic exercises involving joint movement against resistance; and isokinetic exercises that control resistance throughout the range of motion.38 The goal of KOA rehabilitation is to alleviate pain, prevent muscle weakness, and preserve joint function along with peripheral muscles. Pain stands out as a prominent symptom experienced by individuals with KOA. Its origin may be linked to mechanical injury or inflammation-induced stimulation of peripheral nerves leading to increased pain intensity. IMST enhances nerve activity while improving movement coordination for more balanced mobility. The primary symptom experienced by patients with KOA is pain, which often results from mechanical stress and inflammation. IMST has been reported to enhance neuromuscular activation, improve movement coordination, and increase exercise efficiency compared with traditional training methods. Previous studies have shown that patients with KOA experienced significant reductions in pain, as measured by the VAS, after approximately five weeks of IMST training.34 In this study, both the intervention and control groups demonstrated decreased VAS scores following treatment; however, the IMST group exhibited significantly lower post-treatment scores than the controls. Although the pooled reduction in VAS reached statistical significance, its magnitude was smaller than the commonly accepted Minimal Clinically Important Difference (MCID) for pain relief in KOA, typically estimated at 1.5–2.0 points.39 Therefore, while IMST may produce measurable pain improvement, the clinical relevance of this change should be interpreted with caution. Nonetheless, even modest pain reductions may help enhance mobility, promote patient adherence, and support overall functional recovery, particularly among older adults with KOA.
The decline in muscle function of the knee joint leads to instability, resulting in both localized pain and impaired knee joint function, which is a contributing factor to KOA.15 KOA can cause disuse atrophy due to reduced muscle function and abnormal stress distribution on the articular surface, exacerbating joint imbalance and accelerating disease progression. Previous studies have shown that IMST can alleviate cartilage wear caused by excessive concentration of local stress by enhancing knee joint muscle function, thereby reducing pain.40 Furthermore, it can improve knee joint stability by alleviating abnormal muscle tension and decreasing pain associated with tissue dissociation. IMST helps maintain knee joint stability by increasing the strength and coordination of the muscles surrounding it. Additionally, it ensures stable angular velocity during movement without acceleration, thus reducing impact load on the joints and facilitating better recovery of muscle function and knee joint stability.1 These findings are generally consistent with recent randomized trials, such as that by Hammami et al, which demonstrated that isokinetic strengthening improved muscle strength and functional performance in overweight women with KOA.41
The comprehensive findings of this study indicated that compared to isometric exercise, isotonic exercise, warm acupuncture intervention, aerobic exercise, and conventional rehabilitation treatment, there were significant improvements in the Lysholm score and extensor and flexor PT. The study suggested that enhancing the muscle strength of knee joint extensors and flexors can effectively maintain knee joint stability.1 Furthermore, IMST helps maintain joint flexibility, enhances neuromuscular control of the joint, improves patellar-femoral contact area, and increases joint mobility.34
The primary objective of KOA treatment is to optimize overall well-being. Due to the limited availability of data on quality of life as an outcome measure in this study, conducting a meta-analysis is not feasible. Research has demonstrated that compared to traditional muscle strength rehabilitation training combined with massage therapy, 8 weeks of IMST significantly improve the quality of life for KOA patients. Survey findings indicate that over 80% of individuals aged 60 and above suffer from KOA.42 Considering the increasing prevalence of knee arthritis among younger populations, this study’s results also suggest that 4-week of IMST effectively alleviates pain in young individuals with KOA when compared to sensory motor training.20 These findings imply that IMST offers greater advantages in improving quality of life, thereby facilitating normal daily activities and work performance.
From a clinical perspective, IMST may serve as a safe and quantifiable rehabilitation modality for patients with knee osteoarthritis, particularly for those unable to perform high-load or weight-bearing exercises. It can improve muscle strength, enhance joint stability, and reduce pain, thereby supporting mobility and independence in daily life. Incorporating IMST into individualized rehabilitation programs could optimize functional outcomes and patient quality of life. Furthermore, establishing standardized IMST protocols and integrating them into multidisciplinary rehabilitation frameworks may help bridge the gap between evidence and practice.
Although this Meta-analysis demonstrated the potential benefits of IMST in the management of KOA, several limitations should be acknowledged. Firstly, variations in sample size and experimental design across different studies may impact the stability and generalizability of the results. Secondly, differences in disease severity, patient age, and gender in different studies may influence the assessment of treatment efficacy. The substantial heterogeneity observed in key outcomes such as VAS and WOMAC likely reflects these clinical and methodological differences. Although meta-regression or subgroup analyses were considered, the limited number of studies with comparable parameters made such analyses infeasible. Sensitivity analyses, however, indicated that no single study had a disproportionate influence on the pooled results, suggesting reasonable robustness.
Furthermore, the IMST protocols varied considerably across studies, including differences in angular velocity, contraction mode, training frequency, and total intervention duration. This lack of standardization limits comparability between trials and reduces the clinical applicability of the synthesized evidence. Future multicenter studies should therefore adopt unified IMST parameters and consistent reporting methods to improve reproducibility and facilitate clinical translation.
Finally, potential publication bias was identified in the funnel plot, suggesting that studies with positive results may have been more likely to be published. This bias could have slightly overestimated the effect sizes, although sensitivity analyses showed that it did not alter the overall direction of the results. Future reviews should include grey literature and unpublished registered trials to minimize publication bias and provide a more comprehensive evidence base.
Conclusion
This meta-analysis demonstrated that IMST can effectively improve knee muscle function, alleviate pain, and enhance joint stability in patients with KOA. However, the overall methodological quality of the included studies was low to moderate, and considerable heterogeneity was observed. Future clinical trials should aim to address these limitations by including more diverse participant populations, encompassing various age groups, disease severities, and comorbid conditions to enhance generalizability. Greater emphasis should be placed on standardizing intervention parameters, such as the type, intensity, frequency, and duration of IMST, to facilitate reproducibility and comparison across studies. Additionally, comprehensive outcome assessments that combine both subjective measures and objective indices are encouraged. Long-term follow-up investigations are needed to assess the durability of therapeutic benefits and potential risks. Finally, comparative effectiveness trials examining IMST versus other rehabilitation modalities, or their combined applications, would further strengthen the evidence base and guide personalized rehabilitation strategies for patients with KOA.
Highlights
- Isokinetic exercise is commonly used as an adjunctive treatment in rehabilitation of osteoarthritis.
- Isokinetic muscle strength training may provide benefits for knee osteoarthritis, but its isolated effects have not been systematically assessed.
- High-quality randomized controlled trials are needed to confirm the efficacy of isokinetic muscle strength training for knee osteoarthritis.
Abbreviations
IMST, Isokinetic muscle strength training; KOA, knee osteoarthritis; RCTs, randomized controlled trials; GRADE, Grading of Recommendations, Assessment, Development and Evaluation; OA, Osteoarthritis; CNKI, China National Knowledge Infrastructure; CBM, Chinese Biomedical Literature Database; ICTRP, International Clinical Trials Registry Platform; PICO, Population, Intervention, Comparison, Outcome; MDs, Mean Differences; CI, Confidence Intervals.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Author Contributions
Conceptualization: Jian-Heng Hao, Hai-Jun Wang; Methodology: Bo-Ya Chang, Long Chen; Data curation and analysis: Hui-Chao Xu, Long Chen; Writing—original draft preparation: Bo-Ya Chang; Writing—review and editing: Jian-Heng Hao, Hai-Jun Wang.
All authors have read and approved the final manuscript.
Funding
This work was supported by National Natural Science Foundation of China [grant numbers 82074549].
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Cui S-Y, Wang J-H, Zhao J-X, Liang J-Y, Liu G-T, Yan W. Effect of acupuncture exercise therapy synchronizing isokinetic muscle strength training for postoperative rehabilitation of meniscectomy under arthroscopy. Zhongguo Zhen Jiu. 2023;43(10):1118–1122.
2. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014;22(3):363–388. doi:10.1016/j.joca.2014.01.003
3. Xie X, Zhang K, Li Y, et al. Global, regional, and national burden of osteoarthritis from 1990 to 2021 and projections to 2035: a cross-sectional study for the global burden of disease study 2021. PLoS One. 2025;20(5):e0324296. doi:10.1371/journal.pone.0324296
4. Hyoung-Won L. Evidence-based physical therapy for anterior cruciate ligament injury: literature review. J Korean Soc Physical Therapy. 2019;31(4):161–168. doi:10.18857/jkpt.2019.31.4.161
5. Andriacchi TP, Favre J. The nature of in vivo mechanical signals that influence cartilage health and progression to knee osteoarthritis. Curr Rheumatol Rep. 2014;16(11):463. doi:10.1007/s11926-014-0463-2
6. Tang Y, Man X. Possible mediators for the positive effects of exercise therapy on symptoms of osteoarthritis. Chinese J Osteopor. 2018;24(1):111–115.
7. Xiang S, Zhang J. Effect of acupuncture at yanglingquan (GB34) combined with isokinetic muscle strength training on knee osteoarthritis patients. Chinese J Integrated Traditional Western Med. 2018;38(6):655–657.
8. Gür H, Cakin N, Akova B, Okay E, Küçükoğlu S. Concentric versus combined concentric-eccentric isokinetic training: effects on functional capacity and symptoms in patients with osteoarthrosis of the knee. Arch Phys Med Rehabil. 2002;83(3):308–316. doi:10.1053/apmr.2002.30620
9. Almosnino S, Brandon SC, Sled EA. Does choice of angular velocity affect pain level during isokinetic strength testing of knee osteoarthritis patients? Eur J Phys Rehabil Med. 2012;48(4):569–575.
10. Wang K, Cheng L, Wang B, He B. Effect of isokinetic muscle strength training on knee muscle strength, proprioception, and balance ability in athletes with anterior cruciate ligament reconstruction: a randomised control trial. Front Physiol. 2023;14:1237497. doi:10.3389/fphys.2023.1237497
11. Kucuk EB, Taskiran OO, Tokgoz N, Meray J. Effects of isokinetic, isometric, and aerobic exercises on clinical variables and knee cartilage volume using magnetic resonance imaging in patients with osteoarthritis. Turkish J Physical Med Rehabili. 2018;64(1):8–16. doi:10.5606/tftrd.2018.795
12. He X, Jin R, Tang T, et al. Effect of isokinetic training of knee flexors and extensors on walking ability in patients with knee osteoarthritis. Chin J Rehabil Theory Pract. 2018;24(4):437–441.
13. Bartholdy C, Juhl C, Christensen R, Lund H, Zhang W, Henriksen M. The role of muscle strengthening in exercise therapy for knee osteoarthritis: a systematic review and meta-regression analysis of randomized trials. Semin Arthritis Rheumatism. 2017;47(1):9–21. doi:10.1016/j.semarthrit.2017.03.007
14. Zacharias A, Green RA, Semciw AI, Kingsley MIC, Pizzari T. Efficacy of rehabilitation programs for improving muscle strength in people with Hip or knee osteoarthritis: a systematic review with meta-analysis. Osteoarthritis Cartilage. 2014;22(11):1752–1773. doi:10.1016/j.joca.2014.07.005
15. Wu JQ, Che XC. Evaluation on curative effects of isokinetic muscle strength training for improving muscle function in patients with knee osteoarthritis: a protocol for systematic review and meta-analysis. Medicine. 2021;100(45):e27655. doi:10.1097/MD.0000000000027655
16. Parmley WW. Publication bias. J Ame College Cardiol. 1994;24(5):1424–1425. doi:10.1016/0735-1097(94)90129-5
17. Maitra S. Fixed-effect versus random-effect model in meta-analysis: how to decide? Indian J Anaesthesia. 2025;69(1):143–146. doi:10.4103/ija.ija_1203_24
18. Andrade C. Fixed effect versus random effects models in meta-analysis: as simple as it gets. Indian J Psychologic Med. 2025;02537176251390987.
19. Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126–135. doi:10.1016/j.jclinepi.2019.10.014
20. Rang M. Effect of isokinetic muscle strength training in the application of rehabilitation treatment of knee arthritis. Chinese Foreign Med Res. 2022;20(14):167–171.
21. Chen W, Li J, Liu GJ, Zhang FQ. Clinical study on warm needling moxibustion plus isokinetic muscle strength training in treating knee osteoarthritis. J Acupunc Tuina Sci. 2022;20(3):221–228. doi:10.1007/s11726-022-1316-6
22. Zhen TS, Qin YL. Observational study on the efficacy of isokinetic resistance training in the management of knee osteoarthritis. Chinese J Rural Med Pharm. 2019;26(18):30–31.
23. Zhang XK, Wang DJ. Effect of active isokinetic centripetal knee joint combined with centrifugal muscle strength training on muscle strength and knee joint performance in patients with knee osteoarthritis. Hainan Med J. 2019;30(06):731–735.
24. Zhang J, Chen SL, Wang CH, Wang YY, Zhang S, Du JG. Rehabilitation effect of isokinetic muscle training combined with semiconductor laser on acute knee osteoarthritis. Inter J Biomed Engine. 2019;42(3):216–221.
25. Xu YH, Wang JH, Xie J, Liu F, Gao F. Research on effects to the knee osteoarthritis after the treatments of warming needle moxibustion Yanglingquan point and isokinetic training. Global Traditional Chinese Med. 2015;8(08):908–912.
26. Yu XJ, Wu Y, Bai YL, Li MP. The study on concentric and eccentric isokinetic strength training in patients with knee osteoarthritis. Chin J Rehabil Med. 2007;(11):985–988.
27. Nambi G, Abdelbasset WK, Alrawail SM, Elnegamy TE, Abodonya AM, Saleh AK. Effects of isokinetic knee muscle training on bone morphogenetic proteins and inflammatory biomarkers in post-traumatic osteoarthritis after anterior cruciate ligament injury: a randomized trial. J Rehabili Med. 2020;52(9):jrm00098. doi:10.2340/16501977-2732
28. Rosa UH, Velásquez Tlapanco J, Lara Maya C, et al. Comparison of the effectiveness of isokinetic vs isometric therapeutic exercise in patients with osteoarthritis of knee. Reumatologia clinica. 2012;8(1):10–14. doi:10.1016/j.reuma.2011.08.001
29. Weng MC, Lee CL, Chen CH, et al. Effects of different stretching techniques on the outcomes of isokinetic exercise in patients with knee osteoarthritis. Kaohsiung J Med Sci. 2009;25(6):306–315. doi:10.1016/S1607-551X(09)70521-2
30. Huang MH, Yang RC, Lee CL, Chen TW, Wang MC. Preliminary results of integrated therapy for patients with knee osteoarthritis. Arthritis Rheum. 2005;53(6):812–820. doi:10.1002/art.21590
31. Huang MH, Lin YS, Lee CL, Yang RC. Use of ultrasound to increase effectiveness of isokinetic exercise for knee osteoarthritis. Arch Phys Med Rehabil. 2005;86(8):1545–1551. doi:10.1016/j.apmr.2005.02.007
32. Huang MH, Lin YS, Yang RC, Lee CL. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin Arthritis Rheumatism. 2003;32(6):398–406. doi:10.1053/sarh.2003.50021
33. Maurer BT, Stern AG, Kinossian B, Cook KD, Schumacher HR. Osteoarthritis of the knee: isokinetic quadriceps exercise versus an educational intervention. Arch Phys Med Rehabil. 1999;80(10):1293–1299. doi:10.1016/S0003-9993(99)90032-1
34. Bahşi A, Altındağ Ö, Akaltun MS, Aydeniz A, Avcı EE, Gür A. Comparison of the effects of isokinetic, isometric, and isotonic exercises on knee osteoarthritis using ultrasound. Cureus. 2022;14(8):e28324. doi:10.7759/cureus.28324
35. Salli A, Sahin N, Baskent A, Ugurlu H. The effect of two exercise programs on various functional outcome measures in patients with osteoarthritis of the knee: a randomized controlled clinical trial. Isokinetics Exercise Sci. 2010;18(4):201–209. doi:10.3233/IES-2010-0385
36. Li TJ, Li X. Acupuncture combined with isokinetic muscle strength training for the treatment of 30 cases of knee osteoarthritis. Fujian J Trad Chinese Med. 2016;47(1).
37. Benli Küçük E, Özyemişci TÖ, Tokgöz N, Meray J. Effects of isokinetic, isometric, and aerobic exercises on clinical variables and knee cartilage volume using magnetic resonance imaging in patients with osteoarthritis. Turkish J Physical Med Rehabili. 2018;64(1):8–16.
38. Rausch Osthoff AK, Juhl CB, Knittle K, et al. Effects of exercise and physical activity promotion: meta-analysis informing the 2018 EULAR recommendations for physical activity in people with rheumatoid arthritis, spondyloarthritis and Hip/knee osteoarthritis. RMD Open. 2018;4(2):e000713. doi:10.1136/rmdopen-2018-000713
39. Jeyaraman N, Jeyaraman M, Ramasubramanian S, Balaji S, Muthu S. Beyond statistical significance: embracing minimal clinically important difference for better patient care. World J Methodol. 2025;15(1):97814. doi:10.5662/wjm.v15.i1.97814
40. Lee SEK, CABd L, Nouailhetas VLA, Vancini RL, Andrade MS. Do isometric, isotonic and/or isokinetic strength trainings produce different strength outcomes? J Bodywork Movement Therap. 2018;22(2):430–437. doi:10.1016/j.jbmt.2017.08.001
41. Hammami N, Jdidi H, Khezami MA, et al. Isokinetic strengthening and neuromuscular electrical stimulation protocol impact on physical performances, functional status and quality of life in knee osteoarthritis overweight/obese women. Knee. 2022;39:106–115. doi:10.1016/j.knee.2022.09.004
42. Gezginaslan Ö, Öztürk EA, Cengiz M, Mirzaoğlu T, Çakcı FA. Effects of isokinetic muscle strengthening on balance, proprioception, and physical function in bilateral knee osteoarthritis patients with moderate fall risk. Turkish J Physical Med Rehabili. 2018;64(4):353–361. doi:10.5606/tftrd.2018.2422
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.