Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 17
Effectiveness of HIV Status Disclosure Interventions Among Children and Adolescents in Low and Middle-Income Countries: A Systematic Review
Authors Kirabira J ![]() , Atim LM, Spencer A
, Atim LM, Spencer A
Received 4 March 2025
Accepted for publication 22 May 2026
Published 29 May 2026 Volume 2026:17 526169
DOI https://doi.org/10.2147/PHMT.S526169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Joseph Kirabira,1,2 Letizia Maria Atim,3 Angela Spencer1
1Division of Population Health, Health Services Research and Primary Care, Division of Population Health, University of Manchester, Manchester, UK; 2Department of Psychiatry, Busitema University, Mbale, Uganda; 3Department of Psychiatry, Soroti University, Soroti, Uganda
Correspondence: Joseph Kirabira, Email [email protected]
Background: Appropriate pediatric HIV status disclosure remains a public health challenge in low- and middle-income countries (LMICs). This review aims to describe the existing pediatric HIV disclosure interventions in LMICs and their efficacy.
Methods: Literature search was conducted in Medline, Embase, PsychInfo, Cochrane Central Register of Controlled Trials databases, and Google Scholar following PICOS framework to identify interventional studies aimed at improving HIV status disclosure among children and adolescents. Retrieved studies were screened, data were extracted using a piloted tool, and a narrative synthesis and methodological quality assessment were conducted.
Results: A total of 260 studies were retrieved and after the screening, 6 studies fulfilled the eligibility criteria, three of which were randomized clinical trials (RCTs) while others were quasi-experimental designs. Only two interventions were based on pre-existing theory. Four interventions were delivered by Health Care Workers (HCWs) only, one by HCWs and peer supporters and one by trained research assistants. The main components of the interventions included education/training, media/videos, books, disclosure counseling, and disclosure support and half of the studies applied multiple components. The commonly assessed disclosure-related intervention outcomes were safety, acceptability, prevalence of disclosure, perceptions, and experiences. Only two studies reported significant changes in outcome (prevalence of disclosure) between control and intervention groups. However, there was marked variation in the methods used to assess outcomes across studies.
Conclusion and Recommendations: This review highlights that there are limited interventions addressing pediatric HIV status disclosure in LMICs, targeting different stakeholders in the disclosure process and assessing different outcomes. Additionally, most studies were not grounded pre-existing theories, frameworks and models. There is a need to develop standardized tools to assess disclosure and related outcomes in different contexts, compare the effectiveness of single-component and multi-component pediatric disclosure interventions.
Keywords: pediatric HIV, disclosure, child, adolescent, intervention
Background
In 2024 about 2.42 million children and adolescents aged 0–19 years globally were living with HIV with the majority residing in low- and middle-income countries (LMICs) mainly sub-Saharan Africa (SSA).1 Other than sub-Saharan Africa, high prevalence of HIV among this population have also been reported in Asia and Latin America.2 The commonest mode of transmission of HIV among children is from the mother to child (vertical transmission), also known as perinatal HIV infection which accounts for 90% of the new infections.3 Following the “universal test and treat” policy by the World Health Organisation (WHO), these children are initiated on HIV treatment without knowing their HIV status to benefit from the well-documented effects of early initiation of anti-retral viral therapy (ART).4–6 However, as they mature it becomes paramount that they are informed of their HIV status, a process known as “HIV status disclosure”.7 WHO recommends that children of school-going age should be informed about their HIV status while preschool children should receive age-appropriate information about their diagnosis incrementally according to their cognitive capabilities.8 Disclosure is known to improve HIV treatment adherence, viral suppression, and mental health outcomes in children.7,9,10 Additionally, WHO recommends that pediatric HIV status disclosure should be undertaken primarily by parents or caregivers of the children living with HIV. These caregivers should be supported by healthcare workers (HCWs) throughout the disclosure process.8 Unfortunately, existing literature has indicated low prevalence of HIV status disclosure in different settings with caregivers citing several barriers to disclosure including fear of inter-personal conflicts with children, HIV-related stigma, fear of disclosure to others, and negative emotional reactions.11,12 Additionally, pediatric HIV disclosure raises various ethical challenges including respecting the child’s right to information about his/her diagnosis, who should disclose between the caregiver and healthcare worker (HCW), and at what exact age should disclosure be conducted.13
In SSA countries including Ethiopia, South Africa, Ghana, Kenya, Ivory Coast, and Uganda, among others, the prevalence of HIV status disclosure among children and adolescents living with HIV (CALH) varies widely from 9% to 72%.9 Regrettably, there are no universally accepted interventions for pediatric HIV status disclosure, which leaves a significant gap in the evidence base regarding how the process should be handled. As a result of this public health challenge, various studies have been conducted to address this gap in different contexts by designing pediatric HIV status disclosure interventions.14,15 However, these studies differ in the methodological approach to the problem and assessment of disclosure outcomes among other aspects. Some of these interventions are primarily education focusing on HCWs while others target caregivers and CALH.16,17 At present, no review has been conducted to describe the existing pediatric HIV status disclosure interventions and their efficacy, especially in LMICs where HIV is most prevalent. Therefore, this review aims at describing existing pediatric HIV status disclosure interventions and assessing their efficacy or effectiveness among children and adolescents living (CALH) with HIV in LMICs. Findings from this review will be key in informing decision-makers about the available options regarding pediatric HIV status disclosure interventions to inform related health decisions or choices. It will also highlight the existing strengths and weaknesses in the existing interventions for both health policy and decision-making and inform future research in this field. Finally, the review will be a direct positive contribution in the direction of achieving sustainable development goal 3 and an indirect contribution to all other goals.18
This review aimed at answering mainly two research questions that are critical to pediatric HIV status disclosure which are;
- What are the existing interventions for pediatric HIV status disclosure for CALH in LMICs?
- What is the efficacy or effectiveness of pediatric HIV status disclosure interventions among CALH in LMICs?
Methods
Definition of Intervention and Study Population
This review considered Pediatric HIV status disclosure intervention as any biological, psychological, or social intervention that is designed and implemented to improve the rate of HIV status disclosure among children or adolescents living with HIV as one of the outcomes. This intervention should focus on children with perinatally acquired HIV who start taking ART without knowing that they have HIV and hence later need to be informed of their status either by parents, other caregivers, HCWs, or any other persons. The main study population consists of children and adolescents aged less than 19 years living with HIV residing within any LMIC.
Outcomes of the Review Outcomes
Primary Outcome
Pediatric HIV status disclosure intervention.
Secondary Outcome
Efficacy or effectiveness of the existing pediatric HIV status disclosure interventions.
Search Strategy and Sources of Literature/Information
All literature searches were made via the Ovid platform by JK following the PICOS (Population Intervention Outcome Study Design) framework indicated in Table 1. Searched databases included Medline, Embase, PsychInfo, and Cochrane Central Register of Controlled Trials. All databases were searched from inception (Medline, 1946; Embase, 1947, PsychInfo 1967; and Cochrane Central Register of Controlled Trials, 1996) up to February 02, 2024. Appropriate MeSH terms for each database were identified via the advanced search option while several free texts were used to increase the yield of the searches. Several search terms such as Human Immunodeficiency Virus and others were focused to include only those articles where these were the main subjects while others like child, were expanded to increase the sensitivity of the search. Free texts were searched via the title, abstract, and keyword fields. We also searched grey literature through Google Scholar. For the relevant retrieved articles, forward and backward searches were conducted to obtain any additional articles. Boolean operators like “AND” and “OR” were used during all database searches.
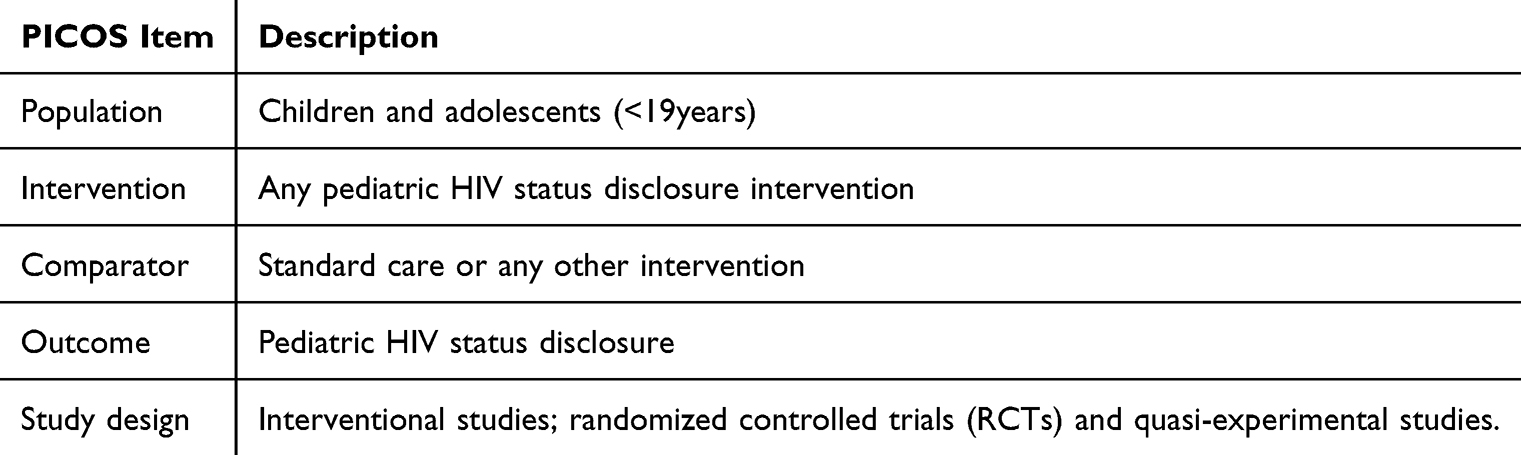 |
Table 1 PICOS Framework for Literature Search in All Databases |
Criteria for Inclusion of Studies
Considering the above PICOS framework, eligible studies included all those that were conducted within LMIC settings testing HIV disclosure interventions. We considered children and adolescents aged up to 19 years as this is the upper limit for adolescence as defined by WHO.19 In order not to leave out important interventions, we considered any studies that were interventional in nature whose activities aimed at improving pediatric HIV status disclosure. The main outcome for this review was HIV status disclosure among CALH, which would be preferably expressed as proportion/prevalence. A prior scoping literature search indicated that several studies assessed other outcomes related to the outcome such as safety, acceptability, perceptions, experiences, and knowledge hence such outcomes were considered only if they were assessed quantitatively and directly related to the intervention. Qualitative outcomes were not considered as these could not be well compared with quantitative outcomes across different interventions. Randomized and controlled studies were the preferred study design, however, due to the nature of the outcome, many studies applied quasi-experimental design hence it was also considered not to leave out important interventions. For studies that applied mixed methods, only the intervention aspect of such study that was relevant to this review was considered. No publication date restriction was considered to capture all existing studies. The study must be intervention studies focusing on either child living with HIV, their caregivers, or HCWs involved in the disclosure process. Only publications written in the English language were included.
Criteria for Exclusion of Studies
Studies that focused on other forms of HIV status disclosure other than informing the child of his or her HIV status, for example, studies focusing on self-disclosure of HIV status. Studies that lack sufficient details about the tested intervention or its outcomes and those whose full publication could not be accessed after all possible attempts to get it.
Study Selection
All the retrieved studies were uploaded into COVIDENCE application for screening, selection, and subsequent data extraction.20 For all uploaded studies, duplicates were automatically detected by COVIDENCE software and removed. The remaining studies were screened based on the inclusion and exclusion criteria using titles and abstracts by two independent persons (JK and LA). Any differences were resolved by consensus. All studies that fulfilled the above criteria were included in this review.
Assessment Risk of Bias/Quality
Risk of bias was assessed by JK and LA using The National Institutes of Health (NIH) quality assessment tool of controlled intervention study and quality assessment tool for before-after (pre-post) studies with no control group for RCTs, and pre-and post- studies respectively.21 The strength/quality of evidence generated by this review was independently assessed by JK and LA using the GRADE checklist.22
Assessing Heterogeneity and Data Analysis/Synthesis and Report
Due to the heterogeneity in study design and measurement of HIV status disclosure outcomes a narrative synthesis was undertaken following guidance by Popay et al, 2006, which suggests four main elements of narrative review23 These include 1) Developing a theory of how the intervention works, why and for whom 2) Developing a preliminary synthesis of findings of included studies 3) Exploring relationships in the data, and 4) Assessing the robustness of the synthesis23 For this review, reporting was done using the Reporting checklist for systematic review which is based on the PRISMA guidelines24 (Supplementary Table 1).
Results
The literature search yielded a total of 260 articles of which 235 were from the included databases while 25 were grey literature from Google Scholar. Ninety-four duplicates were removed. Following screening by title and abstract 65 full-text papers were further reviewed. Six papers fulfilled the inclusion criteria and hence were considered for data extraction and synthesis as indicated in the PRISMA flow diagram (Figure 1).
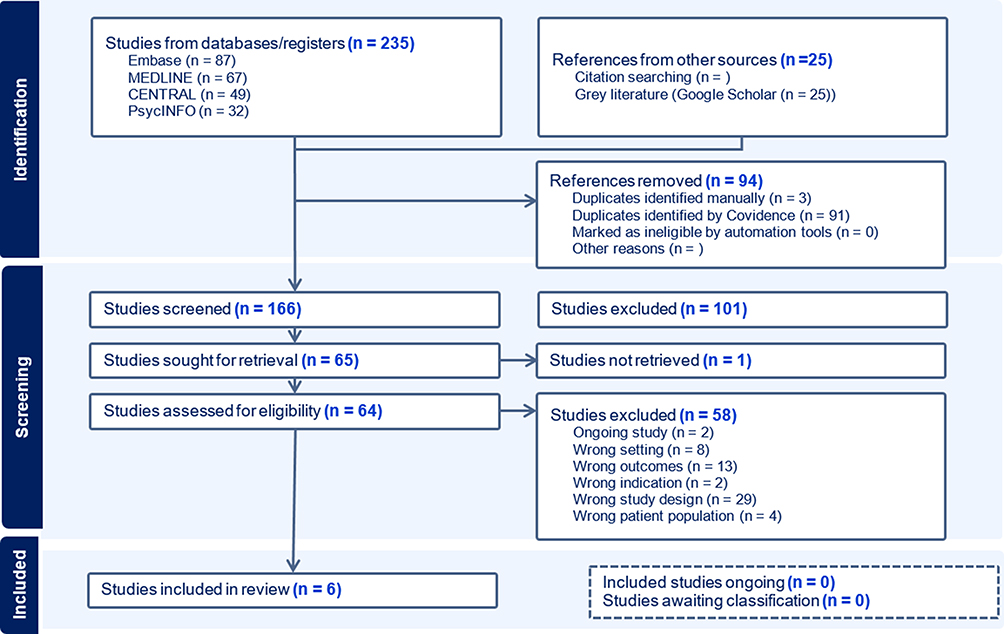 |
Figure 1 PRISMA flow chart for steps taken during screening and selection of potential studies. |
Summary of Included Studies
The included studies were all conducted in health facility settings (HIV clinics) and 2 used quasi-experimental/pre-post intervention design,16,25 3 were randomized controlled trials while one was a longitudinal with mixed methods where the quantitative aspect used pre- and post-intervention study design.17 All 3 randomized control trials had comparison groups which included, usual care,26 current guidelines for pediatric HIV status disclosure14 and routine counseling on adherence and the benefits of adherence.27 The assessed pediatric HIV status disclosure-related outcomes varied whereby 4 studies assessed the proportion of children disclosed to.14,16,26,27 One study assessed efficacy, safety, and acceptability25 and one assessed perceptions and experiences of using intervention.17 Other commonly assessed outcomes knowledge and health outcomes like adherence to ART and viral load16,27 (Table 2).
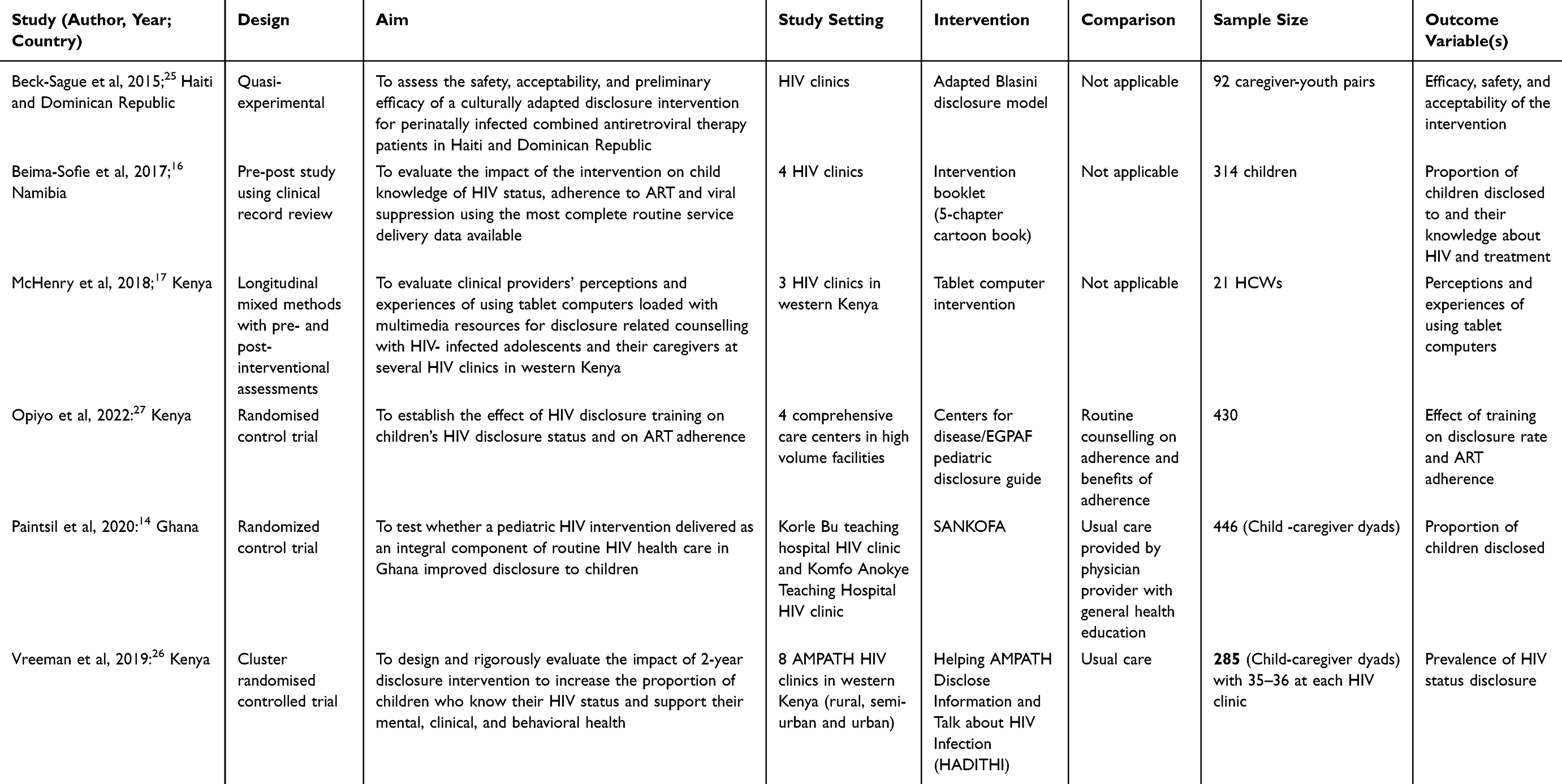 |
Table 2 Characteristics of Included Studies |
Methodological Quality or Risk of Bias Assessment for the Studies Included in This Review
All studies were assessed as poor quality Common sources of bias included poor sampling techniques leading to selection bias, lack of allocation concealment, no blinding, use of non-validated tools to measure outcomes, and missing information on reporting, among others For example, the RCT by Vreeman et al, 2019 was conducted at 8 conveniently selected clinics, and the Sankofa study by Paintsil was conducted at only 2 sites A summary of the methodological quality of RCTs and pre- and post- studies is indicated in Table 3
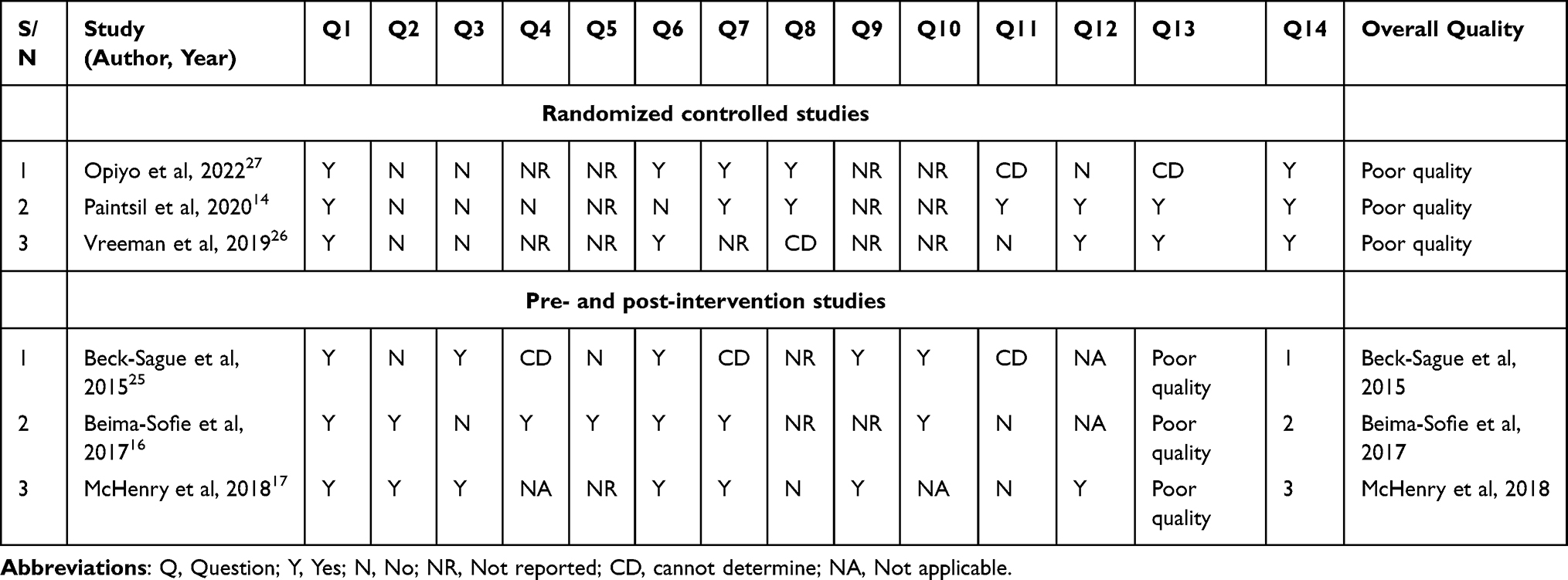 |
Table 3 Quality or Risk of Bias Assessment for the Randomized Controlled and Pre-Post-Intervention Studies |
Characteristics of Study Participant
All studies focused on improving HIV status disclosure among CALH, and five of the six interventions focused on children or youths living with HIV and their caregivers (child-caregiver dyads), and one intervention targeted HCWs and adolescents17 The ages of children and adolescents included in these studies ranged from 6 to 19 years (Table 4). Only three studies (all RCTs) had comparison groups who were also CALH within similar settings.14,26,27
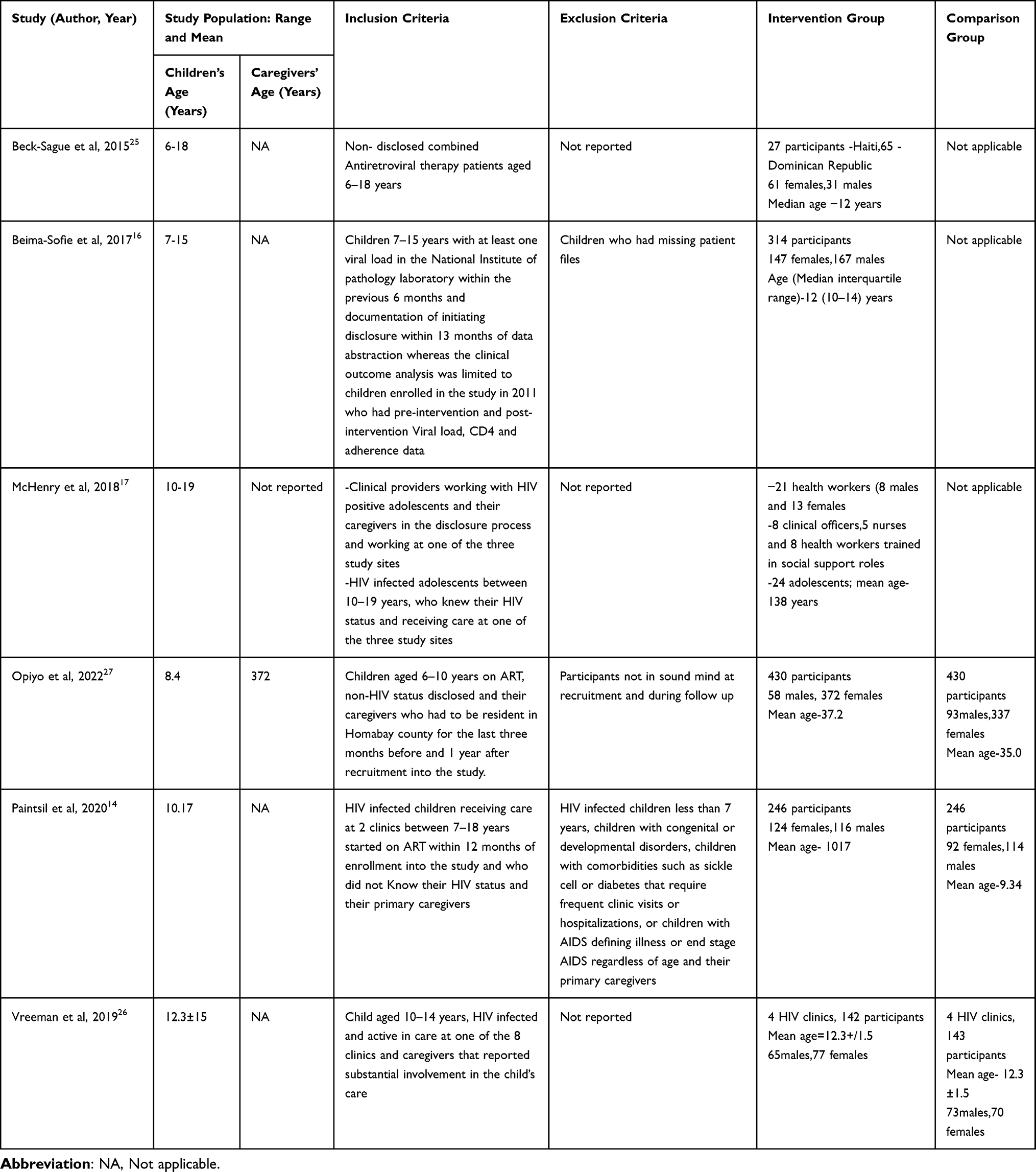 |
Table 4 Characteristics of Study Participants for Each Included Study |
Summary of Pediatric HIV Status Disclosure Intervention and Their Treatment Effects on Disclosure
In the 3 RCTs, the intervention was delivered by trained HCWs including counsellors and physicians though, Opiyo et al, 2022, additionally used peer counsellors14,26,27 The study by McHenry et al, 2018, the intervention was delivered to HCWs by independently trained research assistants17 The cartoon book and adapted Blasini disclosure model interventions by Beima-Sofie et al, 2017, and Beck-Sague et al, 2015, were delivered by HCWs16,25 The adapted Blasini disclosure model by Beck-Sague et al had the highest number of intervention components which included education/training, multimedia/videos, disclosure book and disclosure support25 A further two disclosure interventions used multi-faceted interventions while the rest used a single intervention component.25–27 Education/training, media/videos and books for disclosure were the most used intervention components (Table 5).
 |
Table 5 Components Used by the Various HIV Status Disclosure Interventions |
Four of the six interventions were not based on any well-defined pre-existing theory16,17,26,27 Only two interventions were based on pre-existing theories/models which were the Taker Theory of Disclosure,25 Bio-ecological Systems Theory and Information Motivation- Behavioral Skills (IMB) model of Health Behavior Change14 A study by Vreeman et al, 2019 was not grounded on any specific theory, model, or framework but rather based on supporting the resilience of CALH through the disclosure process26 All interventions were delivered either in groups, one-on-one, or both Table 6 summarises the existing pediatric HIV status disclosure intervention in LMICs, their key components, and outcomes.
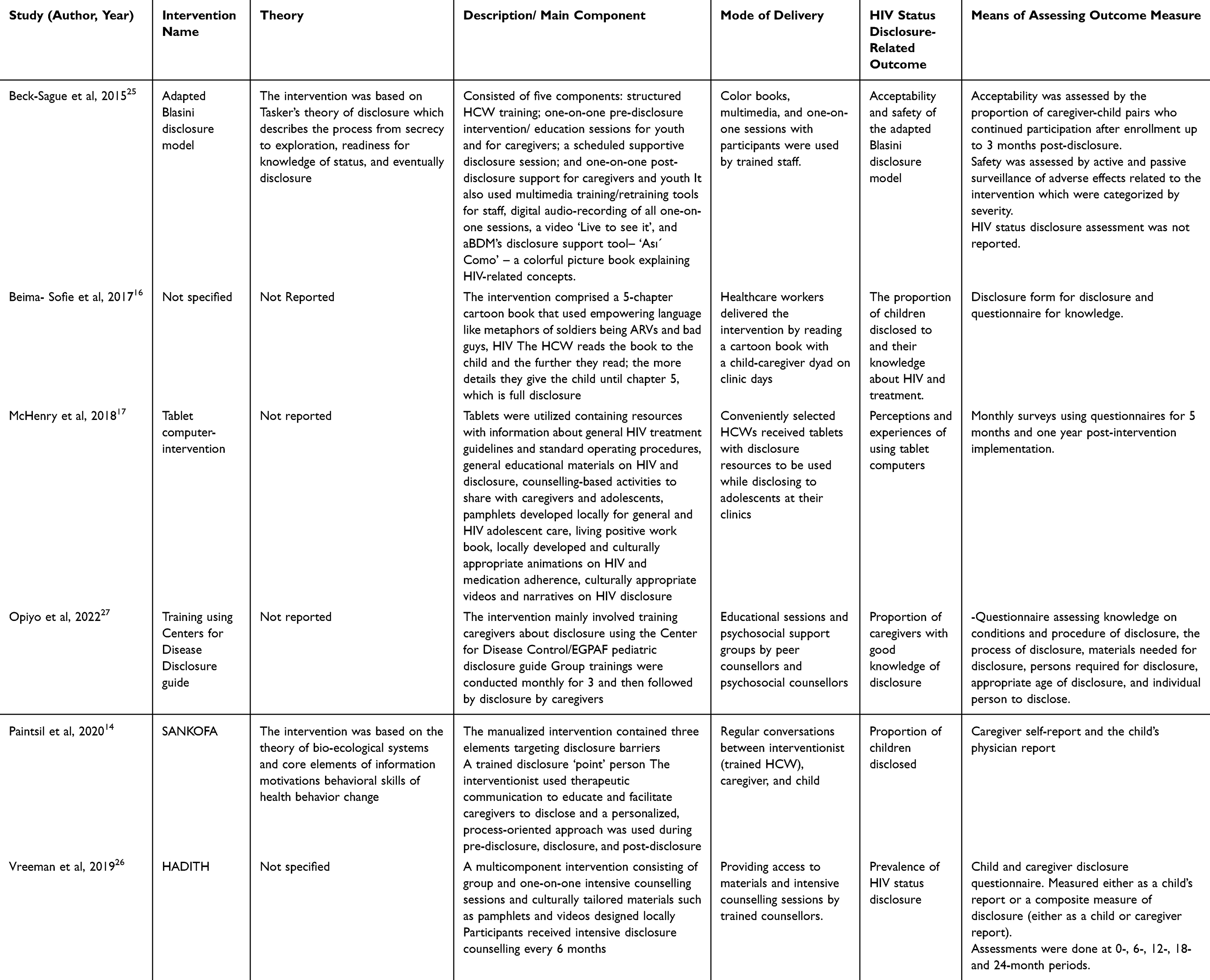 |
Table 6 Interventions for Pediatric HIV Status Disclosure and Their Outcome Measures |
Efficacy of HIV Status Disclosure Interventions
The assessment of the effect of the interventions on disclosure varied across studies as different outcome measures were used. Notably, most studies used more than one HIV status disclosure-related outcome measure. Only 3 studies assessed HIV status disclosure as the main outcome expressed as a proportion of CALH who get to know their HIV status disclosure at the end of the study/intervention period.14,16,26 Two of these studies reported significant changes in the proportion of children disclosed to in intervention group versus the control group14,26 while one did not report the significance of the findings.16 However, these studies measured disclosure using different means, and assessment was conducted at different time intervals. For example, Vreeman et al, 2019, used a child and caregiver disclosure questionnaire26 and findings were significant at 6 months26 while Paintsil et al, 2020 used caregiver self-report, and the child’s physician report was significant at 1 and 2-year periods14 Opiyo et al, 2022, also reported significant differences in disclosure knowledge between the two groups after the intervention27 Four studies measured other intervention outcomes related to HIV status disclosure including safety, acceptability, knowledge, perceptions, and experiences16,17,25,27 Table 7 below summarises the outcome measures of each study/intervention and the corresponding findings. It also summarises the statistical significance of findings depending on the comparison between intervention and control groups (for RCTs) or baseline and end line (for quasi-experimental studies).
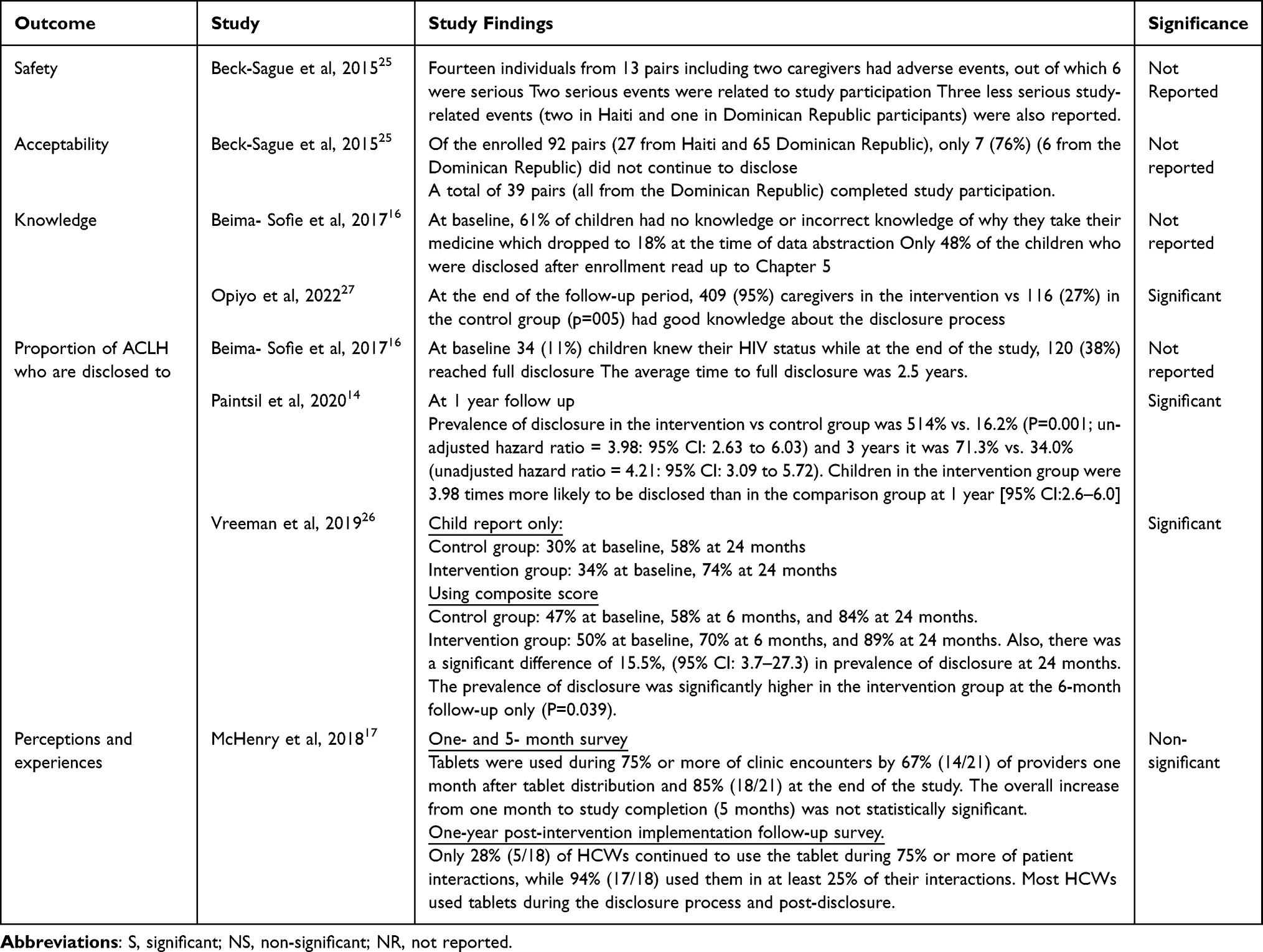 |
Table 7 Summary of Findings and Their Significance for the Different HIV Status Disclosure-Related Outcome Measures Across Different Studies |
Strength of Evidence Generated by This Review
This was a narrative review because of the heterogeneity of the retrieved studies. Assessment of quality of evidence using GRADE was attempted but most criteria are based on point estimate from various studies which was not calculated as there were many (five) outcomes assessed differently by the different studies. Additionally, most interventions (4 out of 6) used multi-component interventions making it difficult to establish the effect of each component onto the measured outcome across studies. Also, whereas all interventions were aiming at improving disclosure among CALH, some interventions focused on different populations such as healthcare workers.27 However, the following scores (with reasons) were generally assigned for the different criteria of GRADE checklist (see Table 8).
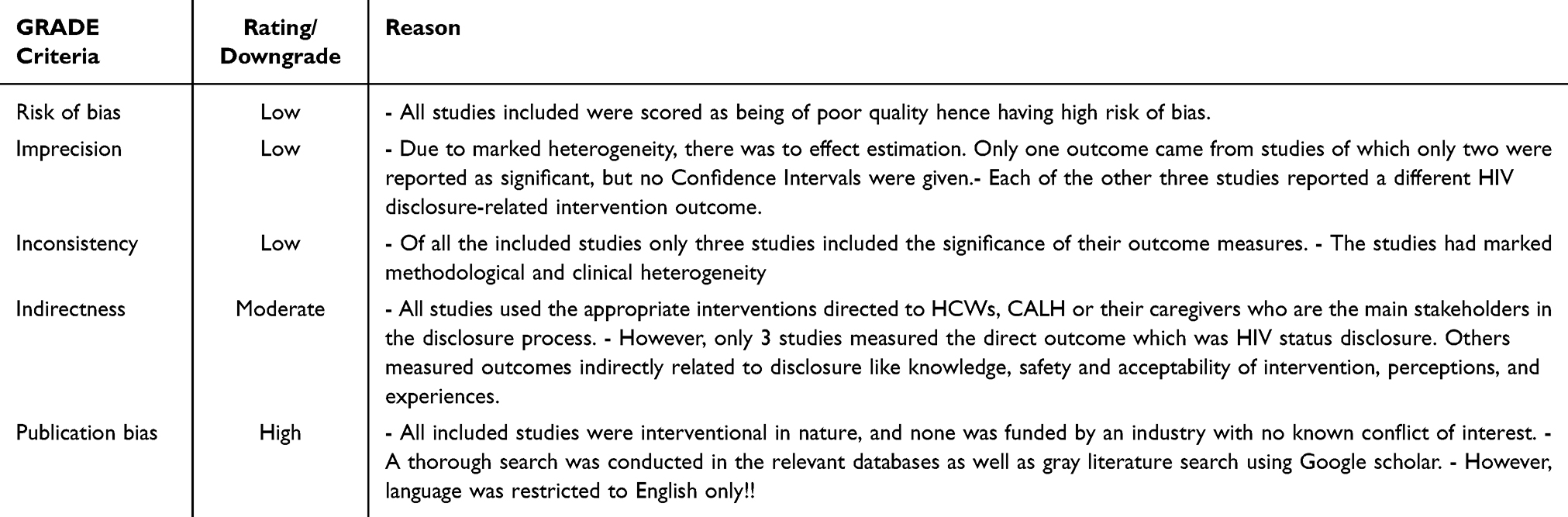 |
Table 8 Summary of GRADE Scoring for Quality of Evidence |
Discussion
This review aimed to describe the existing interventions for pediatric HIV status disclosure and their efficacy/effectiveness among CALH in LMICs and six eligible papers were included in this review. Six interventions were found with four of them having multiple components14,25–27 while only two were informed by pre-existing theories.14,25 The study participants included CALH, caregivers, and HCWs and the interventions were delivered by HCWs, peer support staff, or trained HCWs. The prevalence of HIV status disclosure was only assessed in three studies.14,16,26 The difference in the proportion of CALH disclosed to was only significant in two studies and the significance in differences of outcome measure in other studies was not reported.14,26 Other disclosure-related outcomes that were assessed included safety, acceptability, knowledge, and perceptions and experiences. Three of the studies use pre-post (quasi-experimental) study design16,17,25 while others were RCTs.14,17,27
Study Design and Methodological Quality of Studies
Included studies were either RCTs which are considered to provide the second highest level of evidence after systematic reviews28 or quasi-experimental (pre-and post-) which are not purely experimental in design but involve pre- and post-intervention assessments.28 Whereas the two are interventional studies, the evidence generated depends on methodological quality. Unfortunately, all the studies included in this review were scored as being of low quality based on the appropriate quality assessment tools. This is because most of the studies missed important aspects of randomization, allocation concealment, and blinding which have been documented to minimize bias in interventional studies. Since HIV status disclosure is a psychosocial issue, most of the interventions were psychosocial in nature involving approaches such as education, training, counselling, and providing support to participants. Scholars have established that the main limitations of psychosocial interventions are related to sampling/randomization which limits the representativeness and generalizability of findings.29 Also, such interventions pose a high risk of contamination among participants or therapists in the control and intervention arms.30 However, the commonest method of minimizing contamination in psychosocial interventions involves using cluster randomization, though this was used in only one study.26,31
Lack of blinding is another possible source of bias and ideally for an interventional study, it can be at the level of participants, people delivering the intervention, outcome assessors, statisticians/analysts, or those making conclusions, among others.32 Unlike randomization, blinding can easily be effected in psychosocial interventions at the level of the assessors, data managers, and analysts among others to minimize bias though this is not commonly done.33 In this review, all studies did not report blinding and this is in line with findings from a review by et which found that of 63 psychological interventional studies, none had reported blinding of all key persons and only two and three studies reported blinding of data managers and statisticians respectively.34
Other causes of poor quality for the included studies included selective reporting of results, which can be avoided by authors by following standard reporting guidelines for RCTs such as Consolidated Standards of Reporting Trials.35–37 Also, the use of non-standardised tools to assess outcomes was due to a lack of standardised ones pointing to the need to develop and validate more tools to assess HIV status disclosure and other related outcomes with appropriate validation and adaptation whenever necessary.
Use of Theory, Framework, or Models in Developing Health Interventions
Only two interventions were based on pre-existing theories which were Tasker’s theory of disclosure and the theory of bio-ecological systems combined with components of information, motivation, and behavioral (IMB) skills model.14,25 The Tasker theory of disclosure contends that utilizing disclosure is a continuum that goes through four phases (Four Phase Model) of secrecy, exploration, readiness, and disclosure.38,39 This theory has been used in several studies aimed at understanding how parents disclose HIV status to their children.40,41 The theory of bio-ecological systems theory contends that a person’s development depends on mainly five environmental factors which are the micro-, meso-, exo-macro-, and chrono-system.42–44 Unlike Tasker’s theory, this has not been widely used in explaining HIV status disclosure-related concepts but rather more applied in developmental and educational psychology.45 The IMB skills model is based on the understanding that disclosure is influenced by the information, motivation, and behavioral skills of the caregivers about HIV and this has been widely used to understand several HIV-related behaviors like prevention and treatment adherence.46–49 The utilization of disclosure theories and models in intervention development is strongly recommended as it helps to understand the different factors influencing the process of behavioral change and intervention implementation and the outcomes or consequences of disclosure.50 Since pediatric HIV status disclosure is influenced by various sociocultural factors that vary geographically, applying pre-existing theories or frameworks can help to ensure that these are addressed. Additionally, evidence has shown that using theories to design interventions helps to guide sample size collection, study population and context/ setting, interpretation of outcomes, and the scalability of findings among other benefits.51–53 Theories can also guide the adaptation of existing interventions and identify potential barriers and facilitators to the implementation which need to be addressed during intervention development.54,55 Conversely, developing interventions without considering any theory, framework, or model, can negatively impact their implementation and effectiveness hence this could probably explain the poor quality of some studies included in this review.56,57
The common theories that have been used to design HIV status disclosure interventions in different populations include progression theory which contends that HIV/AIDS progress makes people disclose and the theory of competing consequences whereby people carefully consider the positive and negative consequences of disclosure.58,59
Use of Multi- Versus Single- Component Interventions
Half of the studies used multiple components to promote HIV status disclosure, and the commonest components applied included education/training, and the use of media or videos and books. These are crucial components of psychosocial interventions and have been used in other settings to improve HIV status disclosure in different populations. For example in Mozambique, a peer-educator training intervention was used to enhance HIV testing, counselling, and disclosure among adult persons living with HIV while in Uganda, training of community health workers improved disclosure among HIV-affected sexual partners.60,61
Other intervention components such as the use of media, videos, and books provide important information related to HIV to the participants which fosters behavioral change. The “HEADS-UP” study used dramatized videos alongside other components to foster HIV disclosure among young adults living with HIV62 while a survey conducted in Malawi highlighted that HCWs, caregivers, and children endorsed the use of a book to promote disclosure among CALH.63 Evidence has indicated that the use of visuals improves memory retention and analytical skills which are critical for the uptake of HIV status disclosure-related information that is relevant for decision-making by caregivers.64,65
Similar disclosure intervention components (multi-component) have been used in high-income countries to foster pediatric HIV status disclosure, For example, a psychotherapy intervention by Nicastro et al, 2012 used psychoeducation, counselling, and providing disclosure support to caregivers to encourage them to disclose HIV status to children66 Another intervention by Evangeli et al, 2020, conducted to improve HIV status disclosure among young persons with perinatally acquired HIV in the United Kingdom and Uganda applied, education/training, role-playing, cognitive behavioral therapy, and the use of media/videos.67
On the other hand, unlike most of the existing literature, three studies used single-component interventions that involved the use of a disclosure book, media/videos, and education/training.14,16,17
Due to the heterogeneity of the studies, statistical comparisons could not be made between the efficacy of single- and multi-component interventions. However, most of the HIV status disclosure interventions in other settings conducted among children and adults living with HIV used multiple components. This could be because disclosure is a behaviour that may be influenced by several factors which need to be approached from various perspectives.68 The limitation of multi-component interventions is the challenge to assess the contribution of each component to the registered outcomes and the effect of each component on other components.68 Notably, our results highlight the need for research to compare the effectiveness of single- vs multi- component HIV status disclosure interventions in LMICs.
Efficacy of Existing Pediatric HIV Status Disclosure Interventions in LMICs
The main intervention outcome of this review was the proportion of children that were disclosed to after the intervention. Two of the three studies that assessed this outcome found a statistically significant difference between the intervention and control groups.14,26
In this review, the main limitation to pooling of the estimates for comparison purposes was that the outcomes were assessed differently with no standardized assessment tools. Beima-Sofie et al, 2017, and Vreeman et al, 2019 used non-validated investigator-designed questionnaires administered either to the child, caregiver, or both and these reported marked differences in responses16,26 On the other hand, Paintsil et al, 2020 assessed disclosure based on the child’s or child’s physician’s report which was non-validated but also different from the former two studies14 The most likely form of bias with this mode of disclosure assessment is social desirability bias whereby the caregivers and healthcare workers are more likely to report having disclosed to especially older children as this is what is expected, and it is their responsibility.69,70 Consequently, this can result in an inaccurate higher prevalence of disclosure.70
From existing literature measuring HIV status disclosure remains a public health challenge as several studies conducted in other settings have used similar approaches to assess HIV status disclosure while others never report how it was assessed.66,71–73
The above limitation notwithstanding, this review has highlighted that there is some evidence that interventions can be designed to improve pediatric HIV status disclosure in LMIC settings. This is in line with findings from other studies like the quality improvement project in the United States which used Plan-Do-Study-Act cycles and the family group therapy in Italy.66,71
Like HIV status disclosure, other intervention outcomes like knowledge, safety, acceptability, perceptions, and experiences, that were reported in some of the included studies were not assessed using validated or standardised tools.16,17,25,27 Whereas these are not direct disclosure outcomes, they are very crucial aspects of intervention effectiveness and implementation. Unfortunately, the significance in the difference between baseline and end-line or intervention and control groups was not reported in most of the studies which creates uncertainty in their interpretation.
Overall, this highlights the need to conduct high-quality hybrid effectiveness-implementation research studies to address all important aspects of intervention to better inform health decision-making. Researchers should consider developing, validating, or adapting tools that will effectively assess the intended outcomes of their interventions before implementing the intervention as this will improve the validity and reliability of the findings.74,75
Conclusions and Recommendations
There are limited studies conducted within LMICs addressing pediatric disclosure, targeting different stakeholders in the disclosure process with different outcomes been assessed. Since pediatric HIV status disclosure mainly involves three stakeholders (child/adolescent, caregiver and healthcare worker), it is important to design interventions that address all three levels of stakeholders to empower them for the process with clear measurable outcomes. Additionally, most studies were not grounded in pre-existing theories, frameworks and models, were of poor quality, heterogeneous, do not use validated assessments for outcome measure. This, therefore, points to the need to conduct studies of high quality that are methodologically more rigorous in addressing the pediatric HIV status disclosure gap.
There is a limitation of the lack of standard tools to assess pediatric HIV status disclosure and other related outcomes highlighting a need to develop valid and reliable tools to assess pediatric HIV status disclosure outcomes. The above limitations possibly explain why the prevalence of pediatric HIV status disclosure remains low and challenging in LMICs calling for health policymakers and funding bodies to invest more resources in this key area to ensure better and productive lives of CALH. Finally, further studies should explore the comparative benefit of single-component over multi-component interventions.
Protocol Registration
The protocol was developed but not registered.
Abbreviations
ART: Anti-retroviral Therapy; CALH: Children and Adolescents Living with HIV; CI: Confidence Interval; HCWs: Healthcare workers; HIV: Human Immunodeficiency Virus; LMICs: Low and Middle-Income countries; RCT: Randomised Controlled Trial; WHO: World Health Organisation.
Data Sharing Statement
All data and material used in this review are available upon reasonable request to the corresponding author.
Ethical Considerations
The systematic review was registered with PROSPERO, registration number CRD42024600328.
Acknowledgments
We appreciate Dr. Christine Atala Etoko for the continuous support and encouragement during the entire review process and the administration of Busitema University for providing a favorable work environment that enabled the review to be conducted successfully. We are also grateful for the support offered by Drs, Yen Huang-Ken, Yesim Tozan, and Lawrence Yang of New York University towards the smooth completion of this review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this review.
Disclosure
All authors have no competing interest to declare for this work.
References
1. UNICEF. HIV statistics - global and regional trends. UNICEF DATA. 2025 [Cited May 5, 2026]. Available from: https://data.unicef.org/topic/hivaids/global-regional-trends/.
2. UNICEF. UNICEF DATA. Adolescent HIV prevention. Available from: https://data.unicef.org/topic/hivaids/adolescents-young-people/.
3. Elizabeth Glaser Pediatric AIDS Foundation. About Pediatric AIDS. Elizabeth Glaser Pediatric AIDS Foundation. 2024 [Cited May 5, 2024]. Available from: https://pedaids.org/about/about-pediatric-aids/.
4. WHO. Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. 2021 [Cited May 5, 2024]. Available from: https://www.who.int/publications-detail-redirect/9789240031593.
5. Girum T, Yasin F, Wasie A, Shumbej T, Bekele F, Zeleke B. The effect of “universal test and treat” program on HIV treatment outcomes and patient survival among a cohort of adults taking antiretroviral treatment (ART) in low income settings of Gurage zone, South Ethiopia. AIDS Res Ther. 2020;17:19. doi:10.1186/s12981-020-00274-3
6. Opito R, Mpagi J, Bwayo D, Okello F, Mugisha K, Napyo A. Treatment outcome of the implementation of HIV test and treat policy at The AIDs Support Organization (TASO) Tororo clinic, Eastern Uganda: a retrospective cohort study. PLoS One. 2020;15:e0239087. PMID: 32960927; PMCID: PMC7508381. doi:10.1371/journal.pone.0239087
7. Glaser E. Disclosure of HIV status toolkit for pediatric and adolescent populations. 2016. Available from: https://www.childrenandaids.org/sites/default/files/2019-02/New-Horizons_HIV-Status-Disclosure-Toolkit.pdf.
8. WHO. Guideline on HIV disclosure counselling for children up to 12 years of age. 2011 [Cited May 5, 2024]. Available from: https://www.who.int/publications-detail-redirect/9789241502863.
9. Doat AR, Negarandeh R, Hasanpour M. Disclosure of HIV status to children in Sub-Saharan Africa: a systematic review. Medicina. 2019;55:433. PubMed PMID: 31382540; PubMed Central PMCID: PMC6722600. doi:10.3390/medicina55080433
10. Amankwah-Poku M, Klutsey DA, Asante KO. Disclosure and health-related outcomes among children living with HIV and their caregivers. AIDS Res Ther. 2021;18:13. doi:10.1186/s12981-021-00337-z
11. Vreeman RC, Gramelspacher AM, Gisore PO, Scanlon ML, Nyandiko WM. Disclosure of HIV status to children in resource-limited settings: a systematic review. J Int AIDS Soc. 2013;16:18466. PubMed PMID: 23714198; PubMed Central PMCID: PMC3665848. doi:10.7448/IAS.16.1.18466
12. Atwiine B, Kiwanuka J, Musinguzi N, Atwine D, Haberer JE. Understanding the role of age in HIV disclosure rates and patterns for HIV-infected children in southwestern Uganda. AIDS Care. 2015;27:424–18. PubMed PMID: 25397994. doi:10.1080/09540121.2014.978735
13. Klitzman RL, Marhefka S, Mellins C, Wiener L. Ethical issues concerning disclosures of HIV diagnoses to perinatally infected children and adolescents. J Clin Ethics. 2008;19:31–42. doi:10.7916/d8-hfwz-5111
14. Paintsil E, Kyriakides TC, Antwi S, et al. Clinic-Based pediatric disclosure intervention trial improves pediatric HIV status disclosure in Ghana. J Acquir Immune Defic Syndr. 2020;84:122–131. doi:10.1097/QAI.0000000000002316
15. Budhwani H, Mills L, Marefka LEB, Eady S, Nghiem VT, Simpson T. Preliminary study on HIV status disclosure to perinatal infected children: retrospective analysis of administrative records from a pediatric HIV clinic in the southern United States. BMC Res Notes. 2020;13:253. PubMed PMID: 32448309; PubMed Central PMCID: PMC7247121. doi:10.1186/s13104-020-05097-z
16. Beima-Sofie KM, Brandt L, Hamunime N, et al. Pediatric HIV disclosure intervention improves knowledge and clinical outcomes in HIV-Infected children in Namibia. J Acquir Immune Defic Syndr. 2017;75:18–26. doi:10.1097/QAI.0000000000001290
17. McHenry MS, Apondi E, McAteer CI, et al. Tablet-based disclosure counselling for HIV-infected children, adolescents, and their caregivers: a pilot study. Afr J AIDS Res. 2018;17:249–258. doi:10.2989/16085906.2018.1509101
18. United Nations. THE 17 GOALS | sustainable development. 2024 [Cited February 26, 2024]. Available from: https://sdgs.un.org/goals.
19. WHO. Adolescent health. [Cited May 5, 2024]. Available from: https://www.who.int/health-topics/adolescent-health.
20. Covidence. [Cited May 5, 2024]. Covidence - better systematic review management. Available from: https://www.covidence.org/.
21. NHLBI, NIH. Study quality assessment tools. [Cited May 5, 2024]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
22. Ryan R, Hill S. How to GRADE. 2018. doi:10.26181/5b57d95632a2c.
23. Popay J, Roberts H, Sowden A, et al. Guidance on the conduct of narrative synthesis in systematic reviews. 2006. Available from: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf.
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PubMed PMID: 33782057. doi:10.1136/bmj.n71
25. Beck-Sague CM, Devieux J, Pinzon-Iregui MC, et al. Disclosure of their HIV status to perinatally infected youth using the adapted Blasini disclosure model in Haiti and the Dominican Republic: preliminary results. AIDS. 2015;29:S91–8. doi:10.1097/QAD.0000000000000665
26. Vreeman RC, Nyandiko WM, Marete I, et al. Evaluating a patient-centred intervention to increase disclosure and promote resilience for children living with HIV in Kenya. AIDS. 2019;33:S93. doi:10.1097/QAD.0000000000002183
27. Opiyo R, Ndunyu L, Onyango P. Effect of caregivers’HIV disclosure training on pediatric hiv status disclosure and art adherence in homabay county, Kenya: a Comparative Longitudinal Study. J Health Med Nurs. 2022;8:65–83.
28. Munnangi S, Boktor SW. Epidemiology of Study Design. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
29. Bottomley A. To randomise or not to randomise: methodological pitfalls of the RCT design in psychosocial intervention studies. Eur J Cancer Care. 1997;6:222–230. doi:10.1046/j.1365-2354.1997.00035.x
30. Jacobsen P, Wood L. Risk of contamination when planning psychological therapy trials can be assessed using a simple framework. J Clin Epidemiol. 2020;124:8–15. doi:10.1016/j.jclinepi.2020.04.005
31. Magill N, Knight R, McCrone P, Ismail K, Landau S. A scoping review of the problems and solutions associated with contamination in trials of complex interventions in mental health. BMC Med Res Methodol. 2019;19:4. doi:10.1186/s12874-018-0646-z
32. Monaghan TF, Agudelo CW, Rahman SN, et al. Blinding in clinical trials: seeing the big picture. Medicina. 2021;57:647. PubMed PMID: 34202486; PubMed Central PMCID: PMC8308085. doi:10.3390/medicina57070647
33. Juul S, Gluud C, Simonsen S, Frandsen SS, Kirsch I, Jakobsen JC; BMJ EBM Spotlight. Seeing is believing – the problem of blinding in psychological research. Available from: https://blogs.bmj.com/bmjebmspotlight/2020/10/07/seeing-is-believing-the-problem-of-blinding-in-psychological-research/.
34. Juul S, Gluud C, Simonsen S, Frandsen FW, Kirsch I, Jakobsen JC. Blinding in randomised clinical trials of psychological interventions: a retrospective study of published trial reports. BMJ Evid-Based Med. 2021;26:109. PubMed PMID: 32998993. doi:10.1136/bmjebm-2020-111407
35. Cochrane. 8.4 Introduction to sources of bias in clinical trials. [Cited May 8, 2024]. Available from: https://handbook-5-1.cochrane.org/chapter_8/8_4_introduction_to_sources_of_bias_in_clinical_trials.htm.
36. Butcher NJ, Monsour A, Mew EJ, et al. Guidelines for reporting outcomes in trial reports: the CONSORT-outcomes 2022 extension. JAMA. 2022;328:2252–2264. PubMed PMID: 36511921. doi:10.1001/jama.2022.21022
37. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10:28–55. doi:10.1016/j.ijsu.2011.10.001
38. Qiao S, Li X, Stanton B. Theoretical models of parental HIV disclosure: a critical review. AIDS Care. 2013;25:326–336. PubMed PMID: 22866903; PubMed Central PMCID: PMC3508317. doi:10.1080/09540121.2012.712658
39. Tasker M. How can i tell you? Secrecy and disclosure with children when a family member has aids. Association for the Care of Children’s Health, 7910 Woodmont Ave; 1992 [Cited May 8, 2024]. Available from: https://eric.ed.gov/?id=ED360768.
40. Jemmott JB, Heeren GA, Sidloyi L, Marange CS, Tyler JC, Ngwane Z. Caregivers’ intentions to disclose HIV diagnosis to children living with HIV in South Africa: a theory-based approach. AIDS Behav. 2014;18(6):1027–1036. doi:10.1007/s10461-013-0672-0
41. Gachanja G, Burkholder GJ. A model for HIV disclosure of a parent’s and/or a child’s illness. PeerJ. 2016;4:e1662. doi:10.7717/peerj.1662
42. Tudge J, Rosa EM. Bronfenbrenner’s Ecological Theory. In: The Encyclopedia of Child and Adolescent Development. John Wiley & Sons, Ltd; 2020:1–11.
43. Bronfenbrenner U. Ecological systems theory. In: Encyclopedia of Psychology. Washington, DC, US: American Psychological Association;2000:3. 129–133. doi:10.1037/10518-046
44. Bronfenbrenner U, Ceci SJ. Nature-nurture reconceptualized in developmental perspective: a bioecological model. Psychol Rev. 1994;101:568–586. PubMed PMID: 7984707. doi:10.1037/0033-295x.101.4.568
45. Tong P, An IS. Review of studies applying Bronfenbrenner’s bioecological theory in international and intercultural education research. Front Psychol. 2024;14. doi:10.3389/fpsyg.2023.1233925
46. Knox J, Kutner BA, Shiau S, et al. Assessing the information-motivation-behavioral skills model to predict pre-exposure prophylaxis adherence among black men who have sex with men and transgender women in a community setting in New York City. AIDS Behav. 2022;26:2494–2502. PubMed PMID: 35098392; PubMed Central PMCID: PMC9167713. doi:10.1007/s10461-022-03588-7
47. Wang H, Chang R, Shen Q, et al. Information-Motivation-behavioral skills model of consistent condom use among transgender women in Shenyang, China. BMC Public Health. 2020;20:394. doi:10.1186/s12889-020-08494-y
48. Pollard R, Kennedy CE, Hutton HE, et al. HIV prevention and treatment behavior change and the situated information motivation behavioral skills (sIMB) model: a qualitative evaluation of a community health worker intervention in Rakai, Uganda. AIDS Behav. 2022;26:375–384. doi:10.1007/s10461-021-03391-w
49. Iyiola D, Lanier B. Digication ePortfolio: GH 720 Encyclopedia of Public Health Theories. 2016 [Cited May 8, 2024]. Information-Motivation-Behavioral Skills Model. Available from: https://bu.digication.com/GH720_PublicHealthTheories/Information-Motivation-Behavioral_Skills_Model.
50. Chaudoir SR, Fisher JD, Simoni JM. Understanding HIV disclosure: a review and application of the disclosure processes model. Soc Sci Med. 2011;72:1618–1629. doi:10.1016/j.socscimed.2011.03.028
51. Fleury J, Sidani S. Using theory to guide intervention research. Springer Publishing Company; 2023 [Cited May 8, 2024]. Available from: https://connect.springerpub.com/content/book/978-0-8261-5571-9/part/part02/chapter/ch04.
52. Hagger MS, Weed M. DEBATE: Do interventions based on behavioral theory work in the real world? Int J Behav Nutr Phys Act. 2019;16:36. doi:10.1186/s12966-019-0795-4
53. Thapa S, Hannes K, Buve A, Bhattarai S, Mathei C. Theorizing the complexity of HIV disclosure in vulnerable populations: a grounded theory study. BMC Public Health. 2018;18:162. doi:10.1186/s12889-018-5073-x
54. Hankonen N. Intervention Theories. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer; 2013:1111–1114.
55. Heath G, Cooke R, Cameron E. A theory-based approach for developing interventions to change patient behaviours: a medication adherence example from paediatric secondary care. Healthcare. 2015;3:1228–1242. PubMed PMID: 27417822; PubMed Central PMCID: PMC4934641. doi:10.3390/healthcare3041228
56. French SD, Green SE, O’Connor DA, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implement Sci. 2012;7:38. doi:10.1186/1748-5908-7-38
57. Pérez D, Van der Stuyft P, Del C ZM, Castro M, Lefèvre P. A modified theoretical framework to assess implementation fidelity of adaptive public health interventions. Implement Sci. 2016;11:91. doi:10.1186/s13012-016-0457-8
58. Serovich JM. A TEST OF TWO HIV DISCLOSURE THEORIES. AIDS Educ Prev off Publ Int Soc AIDS Educ. 2001;13:355–364. PubMed PMID: 11565594; PubMed Central PMCID: PMC1237028. doi:10.1521/aeap.13.4.355.21424
59. Yang X, James TA, Brown MJ, et al. Patterns of HIV disclosure and its impact on the HIV care continuum among black men who have sex with men in South Carolina. Am J Mens Health. 2023;17:15579883231177981. doi:10.1177/15579883231177981
60. Dawson-Rose C, Gutin SA, Mudender F, Hunguana E, Kevany S. Effects of a peer educator program for HIV status disclosure and health system strengthening: findings from a clinic-based disclosure support program in Mozambique. PLoS One. 2020;15:e0232347. PubMed PMID: 32374752; PubMed Central PMCID: PMC7202645. doi:10.1371/journal.pone.0232347
61. Lukyamuzi Z, Nabisere RM, Nakalega R, et al. Community health workers improve HIV disclosure among HIV-Affected Sexual Partners in Rural Uganda: a Quasi-Experimental Study. Glob Health Sci Pract. 2022;10:e2100631. PubMed PMID: 36316143; PubMed Central PMCID: PMC9622292. doi:10.9745/GHSP-D-21-00631
62. Evangeli M, Gnan G, Musiime V, et al. The HIV empowering adults’ decisions to share: UK/Uganda (HEADS-UP) Study—a randomised feasibility trial of an HIV disclosure intervention for young adults with perinatally acquired HIV. AIDS Behav. 2024. doi:10.1007/s10461-024-04294-2
63. Kalembo FW, Kendall GE, Ali M, Chimwaza AF. Need and acceptability of story books intended to help with the process of informing children about their HIV status in Malawi: a mixed methods study. AIDS Care. 2019;31:298–305. PubMed PMID: 29992833. doi:10.1080/09540121.2018.1497137
64. Raiyn J. The role of visual learning in improving students’ high-order thinking skills. J Educ Pract. 2016;7.
65. Sushmeta K. eLearning Industry. 2023 [Cited May 10, 2024]. Unlocking The Magic: The transformative power of visuals in the learning process. Available from: https://elearningindustry.com/unlocking-the-magic-the-transformative-power-of-visuals-in-the-learning-process.
66. Nicastro E, Continisio GI, Storace C, et al. Family group psychotherapy to support the disclosure of HIV status to children and adolescents. 2012. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3671625/pdf/apc.2012.0465.pdf.
67. Evangeli M, Foster C, Musiime V, Fidler S, Seeley J, Gnan G. A randomised feasibility trial of an intervention to support sharing of HIV status for 18–25-year olds living with perinatally acquired HIV compared with standard care: HIV empowering adults’ decisions to share—UK/Uganda project (HEADS-UP). Pilot Feasibility Stud. 2020;6:141. doi:10.1186/s40814-020-00688-w
68. Collins LM, Kugler KC, Gwadz MV. Optimization of multicomponent behavioral and biobehavioral interventions for the prevention and treatment of HIV/AIDS. AIDS Behav. 2016;20:197–214. PubMed PMID: 26238037; PubMed Central PMCID: PMC4715714. doi:10.1007/s10461-015-1145-4
69. Thorne-Lyman AL, Lama TP, Heidkamp RA, et al. How does social desirability bias influence survey-based estimates of the use of antenatal care in rural Nepal? A validation study. BMJ Open. 2023;13:e071511. PubMed PMID: 37495390. doi:10.1136/bmjopen-2022-071511
70. Phillips DL, Clancy KJ. Some effects of “Social desirability” in survey studies. Am J Sociol. 1972;77:921–940. doi:10.1086/225231
71. Dantuluri K, Carlucci JG, Howard LM, Johnson D, Garguilo K, Wilson G. 2523. Optimizing disclosure of HIV status to a diverse population of HIV-Positive pediatric patients at an urban HIV clinic in the Southeastern United States. Open Forum Infect Dis. 2019;6(Supplement_2):S877. doi:10.1093/ofid/ofz360.2201
72. Sirikum C, Sophonphan J, Chuanjaroen T, et al. HIV disclosure and its effect on treatment outcomes in perinatal HIV-infected Thai children. AIDS Care. 2014;26:1144–1149. PubMed PMID: 24625136. doi:10.1080/09540121.2014.894614
73. Cluver LD, Hodes RJ, Toska E, et al. “HIV is like a tsotsi. ARVs are your guns”: associations between HIV-disclosure and adherence to antiretroviral treatment among adolescents in South Africa. AIDS Lond Engl. 2015;29:S57–65. PubMed PMID: 26049539. doi:10.1097/QAD.0000000000000695
74. Chiang ICA, Jhangiani RS, Price PC. Reliability and validity of measurement. 2015 [Cited May 12, 2024]. Available from: https://opentextbc.ca/researchmethods/chapter/reliability-and-validity-of-measurement/.
75. Jm L. The role of measurement reliability in clinical trials. Clin Trials Lond Engl. 2004:1. PubMed PMID: 16279296. doi:10.1191/1740774504cn057oa
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence, Management, and Risk Factors of Asthma Among School-Age Children in Yogyakarta, Indonesia
Triasih R, Setyowireni D, Nurani N, Setyati A
Journal of Asthma and Allergy 2023, 16:23-32
Published Date: 5 January 2023
Perceptions of the Intervention Utility and Effectiveness in Supporting and Reintegrating Youths Born of Genocidal Rape in Rwanda
Nyirandamutsa F, Niyonsenga J, Gaju KL, Izabayo J, Kambibi E, Munderere S, Sebuhoro C, Muhayisa A, Sezibera V
Adolescent Health, Medicine and Therapeutics 2023, 14:141-151
Published Date: 12 September 2023
The Effect of School-Linked Module-Based Friendly-Health Education on Adolescents’ Sexual and Reproductive Health Knowledge, Guji Zone, Ethiopia - Cluster Randomized Controlled Trial
Boku GG, Garoma Abeya S, Ayers N, Abera Wordofa M
Adolescent Health, Medicine and Therapeutics 2024, 15:5-18
Published Date: 23 January 2024