Back to Journals » Journal of Pain Research » Volume 19
Effectiveness of Fu’s Subcutaneous Needling for Managing Postoperative Axial Symptoms After Cervical Laminoplasty: A Retrospective Observational Study
Authors Li HZ ![]() , Li YQ, Xia PH, Zhang YJ, Zhao C
, Li YQ, Xia PH, Zhang YJ, Zhao C ![]() , Xia WW, Wu YH, Zhang CF, Liu HY, Yu PF
, Xia WW, Wu YH, Zhang CF, Liu HY, Yu PF
Received 30 March 2026
Accepted for publication 2 June 2026
Published 10 June 2026 Volume 2026:19 611592
DOI https://doi.org/10.2147/JPR.S611592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Hong-Zhen Li,1,* Yu-Qiao Li,2,* Peng-Hui Xia,3,* Yue-Jiao Zhang,4 Chong Zhao,1 Wei-Wei Xia,1 Yong-Hao Wu,1 Chen-Fei Zhang,1 Hai-Ying Liu,1 Pan-Feng Yu1
1Department of Spine Surgery, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China; 2Department of Orthopedics, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China; 3Department of Radiology, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China; 4Department of Radiology, Shengli Oilfield Central Hospital, Dongying, Shandong, 257099, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pan-Feng Yu; Yu-Qiao Li, Email [email protected]; [email protected]
Purpose: Cervical expansive open-door laminoplasty (EOLP) effectively treats multilevel cervical spondylotic myelopathy, but postoperative axial symptoms (AS) remain common. Fu’s subcutaneous needling (FSN) may alleviate myofascial pain, yet evidence for postoperative AS is limited.
Methods: Medical records of patients treated at the Department of Spine Surgery, Peking University People’s Hospital, between August 2023 and December 2024 were reviewed. Based on actual rehabilitation strategies, patients were classified into an FSN group (n=48) and a control group (n=48). Outcomes were evaluated at four timepoints using VAS, NDI, JOA, cervical sagittal alignment parameters (C2– 7 Cobb angle, SVA, T1 slope), and cervical ROM. Exploratory subgroup analyses were performed according to pain severity and age.
Results: Baseline characteristics were comparable between groups. Compared with the control group, the FSN group showed significantly greater improvement in VAS, NDI, and JOA scores during follow-up (all P < 0.05). The FSN group also demonstrated better recovery of cervical sagittal alignment, greater cervical ROM, and a shorter duration of neck brace use. These benefits were maintained at the 12-week follow-up. Subgroup analysis suggested enhanced benefit in patients with higher preoperative pain. No FSN-related adverse events occurred.
Conclusion: FSN may be a safe and promising adjunct to standard rehabilitation for postoperative AS after EOLP and may be particularly beneficial in patients with higher baseline pain. Prospective controlled studies are warranted to further validate these findings.
Keywords: Fu’s subcutaneous needling, cervical posterior expansive open-door laminoplasty, axial symptoms, biomechanical parameter, neck brace wearing time
Introduction
Multilevel cervical spondylotic myelopathy (MCSM) is a common degenerative disease of the cervical spine that leads to neurological dysfunction caused by spinal cord compression.1 As a leading cause of spinal cord dysfunction in middle-aged and elderly populations, its incidence continues to rise with the increasing aging of society.2 In severe cases, MCSM can lead to paralysis, which has a significant impact on patients’ quality of life.3 Cervical posterior expansive open-door laminoplasty (EOLP) is a well-established surgical technique for treating MCSM, as it effectively enlarges the spinal canal, relieves spinal cord compression, and enhances spinal cord perfusion.4 Although EOLP generally achieves good neurological recovery, postoperative axial symptoms (AS), particularly neck pain and stiffness, remain a common complication and significantly affect postoperative rehabilitation and long-term outcomes.5
Postoperative AS after cervical laminoplasty is influenced by multiple factors, including surgical technique, posterior soft-tissue injury, and postoperative management.6 Previous studies have shown that cervical sagittal alignment is associated with axial neck pain and health-related quality of life after cervical laminoplasty.7 AS management often involves the use of cervical collars, which may reduce mechanical stress on the healing cervical spine and alleviate axial neck pain in the early postoperative period.8,9 However, prolonged use of cervical braces can lead to adverse effects, such as intervertebral joint capsule stiffness, reduced joint mobility, and atrophy of cervical paraspinal muscles. These complications may result in chronic pain that persists long after surgery, further limiting cervical spine motion, exacerbating functional impairment, and reducing overall quality of life.10 Thus, there is a need for more effective and minimally invasive strategies that can alleviate AS while preserving cervical mobility and facilitating recovery.11
Fu’s Subcutaneous Needling (FSN) is a novel, minimally invasive therapy that has shown promise in treating myofascial pain and related conditions.12 Small randomized and controlled studies report short-term reductions in pain and improvements in function after this technique.13 Recent preclinical work indicates that FSN may modulate mitochondrial homeostasis and signaling pathways via mechanical effects on subcutaneous connective tissue, producing changes in tissue stiffness, perfusion, and neuromuscular signaling; however, objective mechanistic validation is still limited.14,15 Other nonpharmacologic interventions, such as dry needling, acupuncture, electroacupuncture, and low-level laser therapy, show variable short-term benefit in reviews and trials, while structured physical rehabilitation remains central to postoperative recovery.16,17 Accordingly, existing evidence supports considering FSN as a promising adjunct to multimodal rehabilitation; however, its clinical value for postoperative AS after EOLP remains insufficiently defined.
In this study, we retrospectively analyzed the clinical data of patients who underwent EOLP and subsequently received FSN treatment for AS. The aim was to explore the potential effectiveness and safety of FSN in this context, and to preliminarily assess its association with pain relief, functional recovery, cervical mobility, and sagittal biomechanical parameters.
Materials and Methods
Study Design and Supervision
This retrospective observational study was designed to evaluate the clinical effectiveness and safety of FSN as an adjunctive treatment for AS after EOLP. Medical records of patients treated at the Department of Spine Surgery, Peking University People’s Hospital, between August 2023 and December 2024 were reviewed. Approval was obtained from the Institutional Review Board (No. 2024–159). All procedures were conducted in accordance with institutional ethical standards and the Declaration of Helsinki.
Study Subjects
A total of 96 patients who underwent EOLP for MCSM and developed axial pain after the procedure were included (Figure 1). Inclusion criteria: (1) Diagnosis of MCSM confirmed by clinical symptoms and imaging examinations. (2) Persistent neck and shoulder pain or stiffness after EOLP meeting the diagnostic criteria for AS. (3) Complete follow-up records for at least 12 weeks were available in the medical system. Exclusion criteria: (1) Concurrent cervical spine conditions, such as ossification of the posterior longitudinal ligament (long-segment), congenital cervical spine deformities, or ankylosing spondylitis. (2) Cervical spine infections, tuberculosis, primary or metastatic cervical spine tumors, or severe osteoporosis. (3) History of cervical trauma or previous cervical surgery. (4) Incomplete follow-up data or follow-up less than 12 weeks.
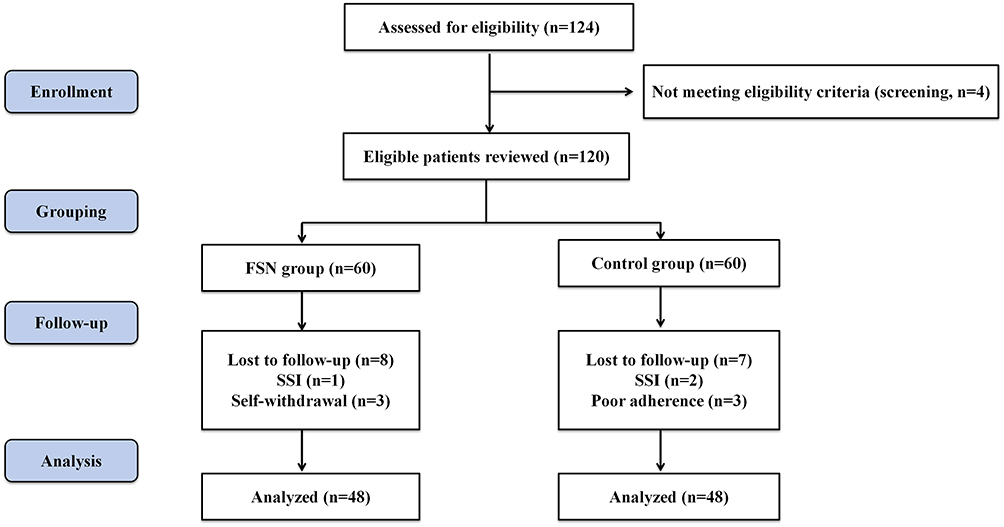 |
Figure 1 Flowchart of patient screening, grouping, follow-up, and final analysis. Patients were retrospectively grouped according to the postoperative treatment actually received. Abbreviations: FSN, Fu’s subcutaneous needling; SSI, surgical site infection. |
Classification and Bias Control
Patients were retrospectively categorized into two groups based on the postoperative treatment they received. The FSN group included patients who underwent FSN in addition to standard rehabilitation (n=48), while the control group consisted of those who received standard rehabilitation alone (n=48). FSN was considered an adjunctive treatment for patients with evident postoperative axial symptoms after EOLP. The decision to add FSN was made by the attending physicians based on the patient’s axial symptoms, physical examination findings, willingness to receive FSN, and absence of contraindications. Clinical data were extracted and analyzed by independent evaluators who were not involved in patient care, in order to reduce potential assessment bias.
Treatment Modalities
- Control group: The control group received a standardized postoperative rehabilitation program. During hospitalization, patients were encouraged to mobilize within the limits permitted by the surgeon and received instruction in basic cervical range-of-motion and posture-correction exercises. After discharge, patients were advised to attend outpatient rehabilitation follow-up approximately once every two weeks for four weeks. Each follow-up session included supervised guidance on cervical mobility, deep neck flexor strengthening, scapular stabilizer activation, and postural correction. Patients were instructed to continue these exercises at home under self-monitoring, with periodic adjustments during outpatient follow-up.
- Treatment group: In addition to the standardized rehabilitation described above, the FSN group received FSN therapy following a standardized institutional protocol. Single-use sterile FSN needles (Nanjing Paifu Medical Science and Technology Company, Nanjing, China) were used for all sessions. Treatments began after removal of the postoperative drainage tube and were completed during hospitalization, typically totaling two to three sessions depending on the patient’s length of stay. Each session lasted approximately three minutes. After disinfection of the skin with 75% ethanol, an FSN needle was swiftly inserted through the skin into the subcutaneous layer. The needle was advanced until the tip gently contacted the muscular surface, then slightly withdrawn to remain within the subcutaneous plane. It was then directed parallel to the skin toward the symptom-related myofascial trigger points and moved with gentle sweeping manipulation to engage the local connective tissue. In this study, FSN was mainly targeted at myofascial trigger points associated with postoperative axial symptoms rather than fixed acupuncture points. These trigger points were identified in painful or stiff areas of the posterior cervical and cervicothoracic shoulder region by palpation, based on localized tenderness, palpable myofascial tension, and reproduction of the patient’s familiar axial pain. All treatments were performed by licensed practitioners trained in FSN, under aseptic conditions. Any immediate adverse reactions such as bleeding, infection, vasovagal response, or severe local pain were recorded and monitored.
- Postoperative management, including analgesic administration, rehabilitation schedule, and brace-weaning strategy, was standardized in both groups according to the same institutional postoperative pathway. Neck brace removal followed the same institutional criteria and was guided by early postoperative stability, wound condition, pain tolerance, cervical muscle spasm, and the patient’s ability to maintain head and neck posture during mobilization.
Main Observations
- Visual Analog Scale (VAS): Pain severity quantified using the VAS, a validated tool for pain assessment on a scale of 0 (no pain) to 10 (worst pain).
- Neck disability index (NDI): A 10-item questionnaire evaluating the impact of cervical symptoms on daily functioning, scored from 0 to 50 (higher scores indicate greater disability).
- Japanese Orthopaedic Association (JOA) score: A measure of neurological function, with a maximum score of 17. Lower scores indicate worse neurological status.
Biomechanical Cervical Spine Parameters
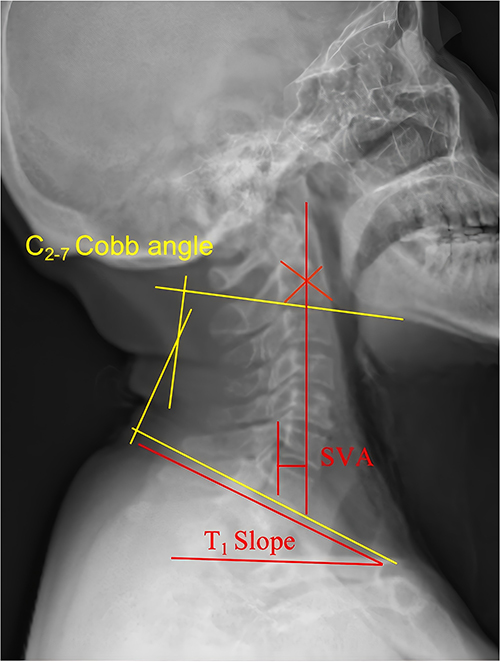
- C2-7 Cobb angle (Figure 2): The angle between the tangent line of C2 and the lower endplate of C7 on lateral cervical spine radiographs. This angle can effectively assess the cervical curvature.

Figure 2 Measurement of cervical sagittal parameters on lateral radiographs. C2–7 Cobb angle was measured as the angle between the lines tangent to the inferior endplates of C2 and C7. C2–7 sagittal vertical axis was measured as the distance from the plumb line of C2 to the posterior-superior corner of C7. The T1 slope was measured as the angle between the superior endplate of T1 and the horizontal line.
Abbreviation: SVA, sagittal vertical axis.
- C2-7 Sagittal Vertical Axis (SVA): The distance from the plumb line over the midpoint of the C2 vertebra to the posterior-superior angle of the C7 vertebra on lateral cervical spine radiographs.
- T1 Slope: The angle between the plane of the endplate on the T1 vertebra and the horizontal plane on lateral cervical radiographs.
- Cervical range of motion (ROM): The C2-7 Cobb angle is measured separately in the extension and flexion positions. A positive cervical Cobb angle represents physiological lordosis (anterior sagittal curvature of the cervical spine), whereas a negative value indicates kyphotic deformity (posterior sagittal curvature). The formula used for cervical ROM: Cervical ROM = C2-7 Cobb angle in extension – C2-7 Cobb angle in flexion.
Follow-Up and Assessment Schedule
Clinical evaluations documented in the medical records were retrospectively reviewed at four predefined timepoints: preoperatively, postoperative day 3, post-rehabilitation/before discharge, and the 12-week outpatient follow-up. Data included pain levels, functional scores, and radiographic findings.
Postoperative neck brace management in both groups followed the routine institutional protocol. Brace weaning was determined according to the treating team’s clinical assessment, including wound condition, early postoperative stability, pain tolerance, and the patient’s ability to maintain head and neck posture safely during mobilization and rehabilitation.
Supplementary Material
Supplementary materials are provided and include Bonferroni-adjusted post hoc pairwise comparisons based on estimated marginal means for outcomes across four timepoints (Pre-op, Post-op 3 days, Post-rehab, and Post-op 3 months) in both the FSN and control groups. Supplementary Table S1 reports pairwise comparisons of VAS scores. Supplementary Table S2 reports pairwise comparisons of NDI scores. Supplementary Table S3 reports pairwise comparisons of JOA scores. Supplementary Table S4 reports pairwise comparisons of the C2-7 Cobb angle. Supplementary Table S5 reports pairwise comparisons of C2-7 SVA. Supplementary Table S6 reports pairwise comparisons of the T1 slope. Supplementary Table S7 reports pairwise comparisons of cervical ROM. All supplementary tables apply the Bonferroni correction for multiple comparisons.
Statistical Analysis
Statistical analyses were performed using SPSS (Statistics for Windows, Version 22.0, IBM Corp., Chicago, IL, USA) and R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables as frequencies or percentages. Between-group comparisons were conducted using the independent-samples t-test or Mann–Whitney U-test for continuous data, and the chi-square test for categorical data. Changes over time within and between groups were assessed using repeated-measures ANOVA with Bonferroni-adjusted post hoc comparisons, and between-group differences at each follow-up time point were further examined using independent-samples tests. Exploratory subgroup analyses were performed using generalized linear models adjusted for baseline VAS, BMI, and surgical parameters. Patients were stratified by preoperative pain, postoperative pain, and age according to median cutoffs. Detailed Bonferroni-adjusted post hoc pairwise comparisons for clinical and radiographic outcomes are provided in Supplementary Tables S1–S7. Two-sided p-values < 0.05 were considered statistically significant.
Results
Baseline Characteristics
A total of 96 patients who met the inclusion criteria were retrospectively categorized into two groups based on the treatment they received: the FSN treatment group (n=48) and the standard rehabilitation group (n=48). Baseline demographic and perioperative characteristics were comparable between the two groups (Table 1). Clinical and radiographic outcomes before and after rehabilitation are summarized (Tables 2–4).
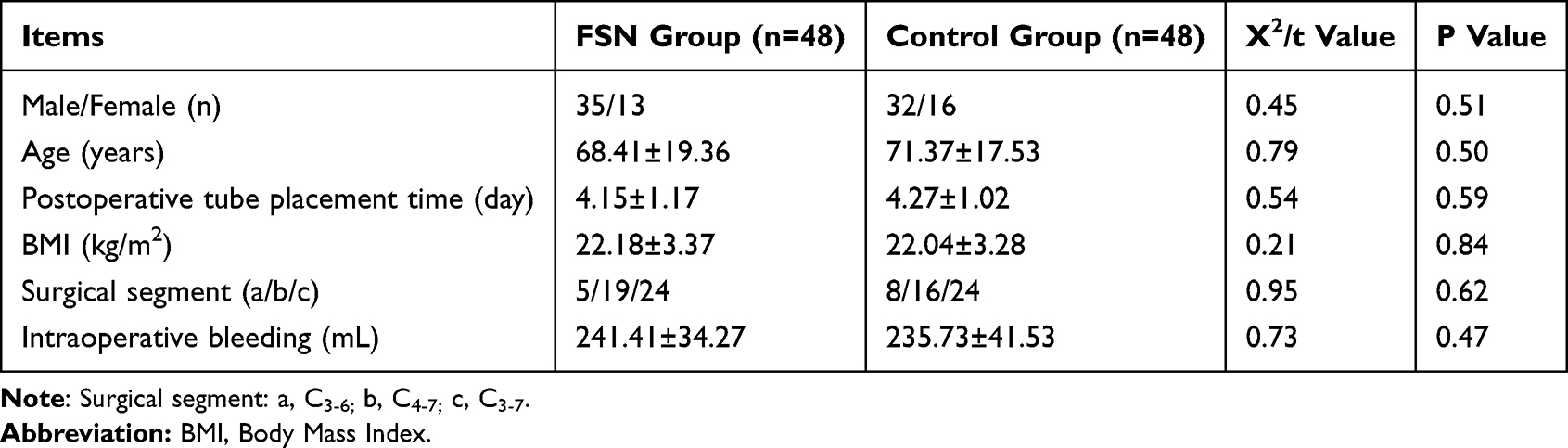 |
Table 1 Baseline Comparisons Between the Two Groups (Mean ± SD) |
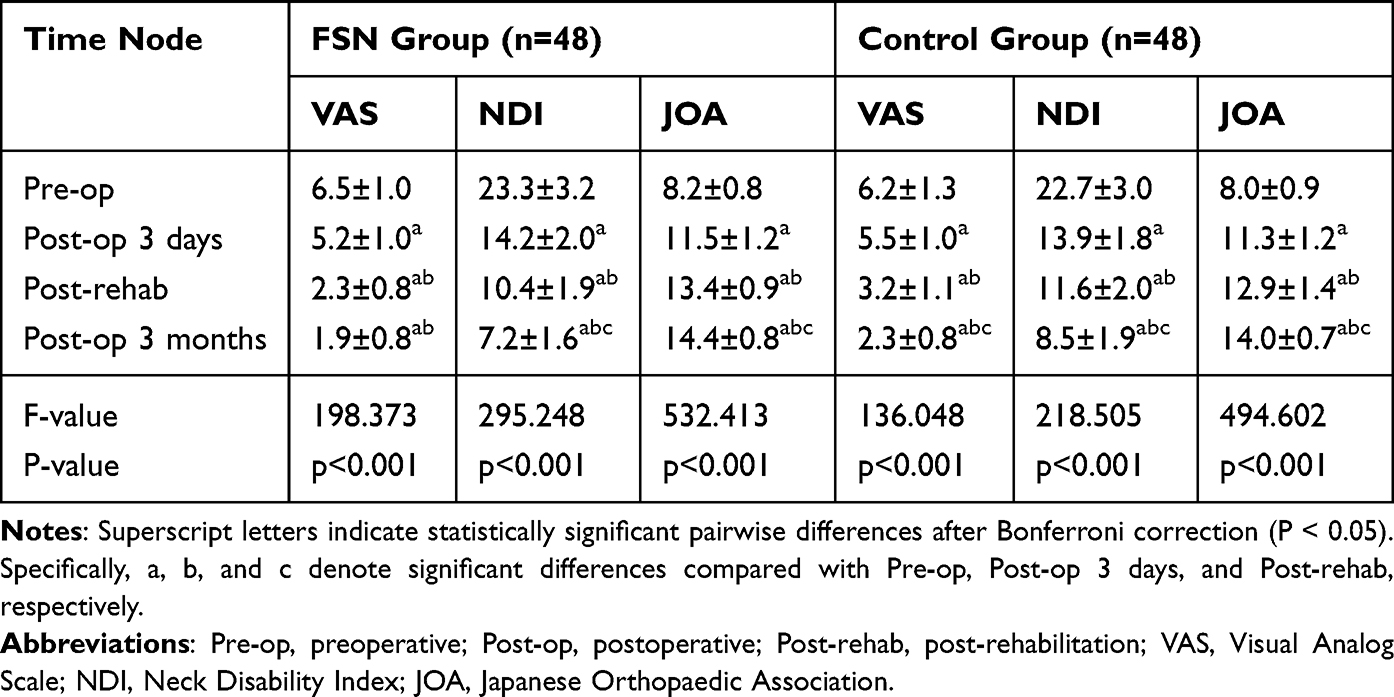 |
Table 2 Comparison of Function Indicators Across Groups: Pre-op, Post-op 3 Days, Post-Rehab, and 3-Month Post-op Evaluation (Mean ± SD) |
Cervical Functional Indicators
Retrospective analysis of follow-up data showed significant time-dependent improvement in cervical functional outcomes in both groups, with superior post-rehabilitation and 12-week outcomes in the FSN group (Table 2 and Table 3). Prior to rehabilitation, no statistically significant differences were observed between the FSN group and the control group in neurological functional parameters, including the JOA score, VAS score, and NDI score (P > 0.05), indicating baseline comparability. However, after rehabilitation treatment, the FSN group exhibited superior outcomes compared to the control group. Specifically, at the post-rehabilitation assessment and the final follow-up, the FSN group showed lower VAS and NDI scores and a higher JOA score than the control group (all P < 0.05). At postoperative day 3, no significant between-group differences were observed in VAS, NDI, or JOA scores (all P > 0.05). These findings indicate that FSN was associated with better postoperative pain relief and functional recovery during follow-up (Table 3).
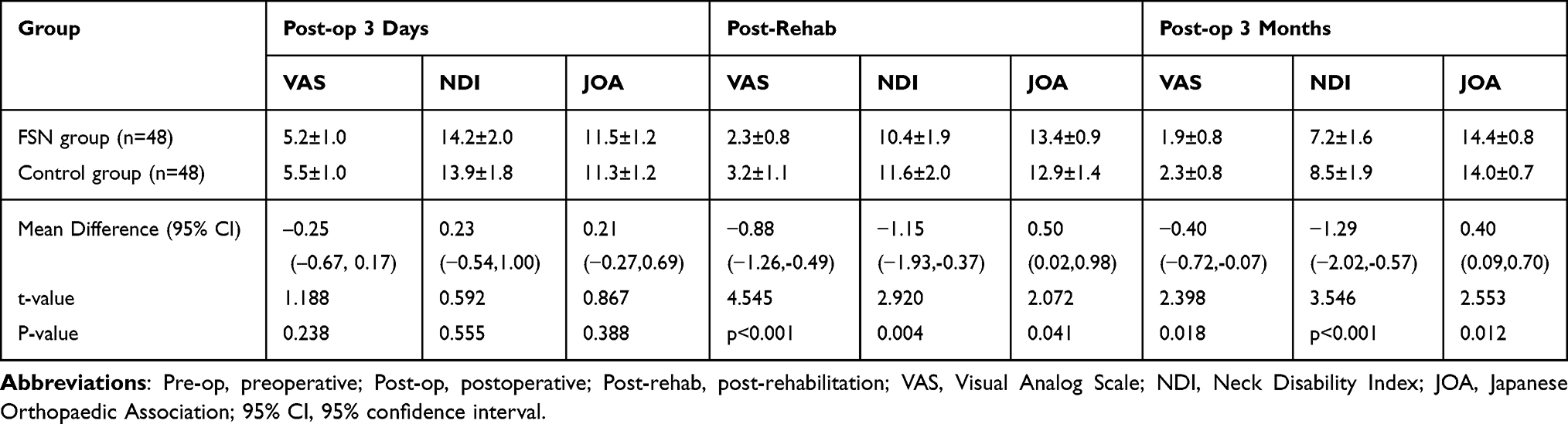 |
Table 3 Comparison of Function Indicators Between Groups: Post-op 3 Days, Post-Rehab, and 3-Month Post-op Evaluation (Mean ± SD) |
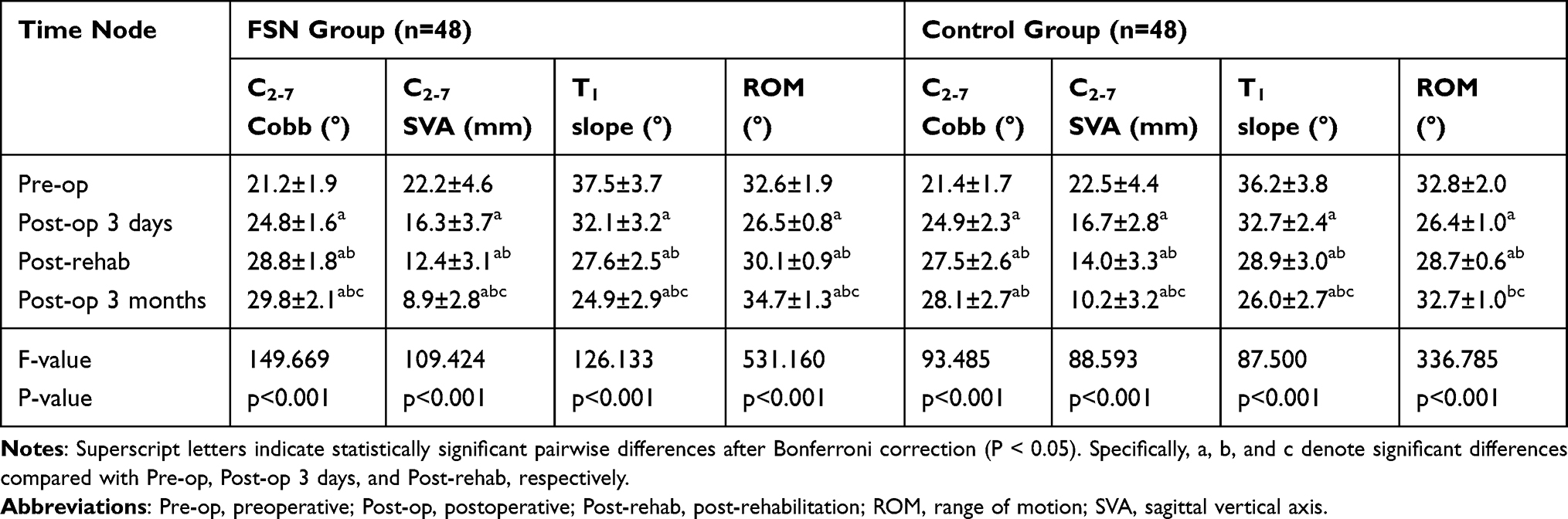 |
Table 4 Comparison of Imaging Parameters Between Groups: Pre-op, Post-op 3 Days, Post-Rehab, and 3-Month Post-op Evaluation (Mean ± SD) |
Cervical Spine Sagittal Balance Parameters
Serial imaging results showed significant time-dependent changes in cervical parameters in both groups (Table 4). Between-group comparisons further showed greater improvement in cervical sagittal parameters in the FSN group at post-rehabilitation and 3-month follow-up (Table 5). Prior to rehabilitation treatment, no statistically significant differences were observed in cervical sagittal balance parameters, including the C2-7 Cobb angle, C2-7 SVA, and T1 slope, between the FSN group and the control group (P > 0.05), indicating baseline comparability. Following rehabilitation treatment, significant improvements in cervical sagittal balance parameters were observed in both groups. In the FSN group, the C2-7 Cobb angle increased significantly, while the C2-7 SVA and T1 slope showed marked decreases compared to preoperative values (P < 0.05). At the final follow-up, the FSN group demonstrated greater improvement in cervical sagittal balance parameters than the control group, including a larger C2–7 Cobb angle, a smaller C2–7 SVA, and a lower T1 slope (all P < 0.05, Table 5), indicating better postoperative recovery of cervical sagittal alignment.
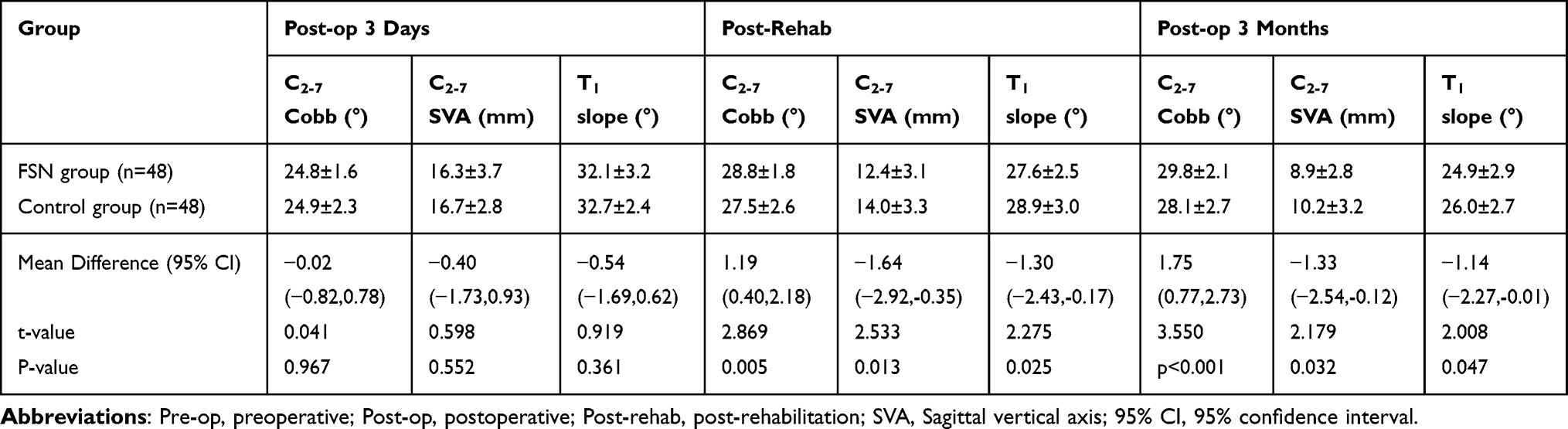 |
Table 5 Comparison of Imaging Parameters Between Groups: Post-op 3 Days, Post-Rehab, and 3-Month Post-op Evaluation (Mean ± SD) |
Cervical Spine Mobility and Neck Brace Wearing Time
Cervical mobility was comparable between the FSN group and the control group prior to rehabilitation, with no statistically significant differences observed (P > 0.05). Significant improvements in cervical mobility were observed in both groups during follow-up. Compared with the control group, the FSN group achieved greater ROM recovery at the post-rehabilitation and 3-month assessments (both P < 0.05, Figure 3 and Table 6). In addition, the mean duration of neck brace use was significantly shorter in the FSN group than in the control group (P < 0.001, Table 6).
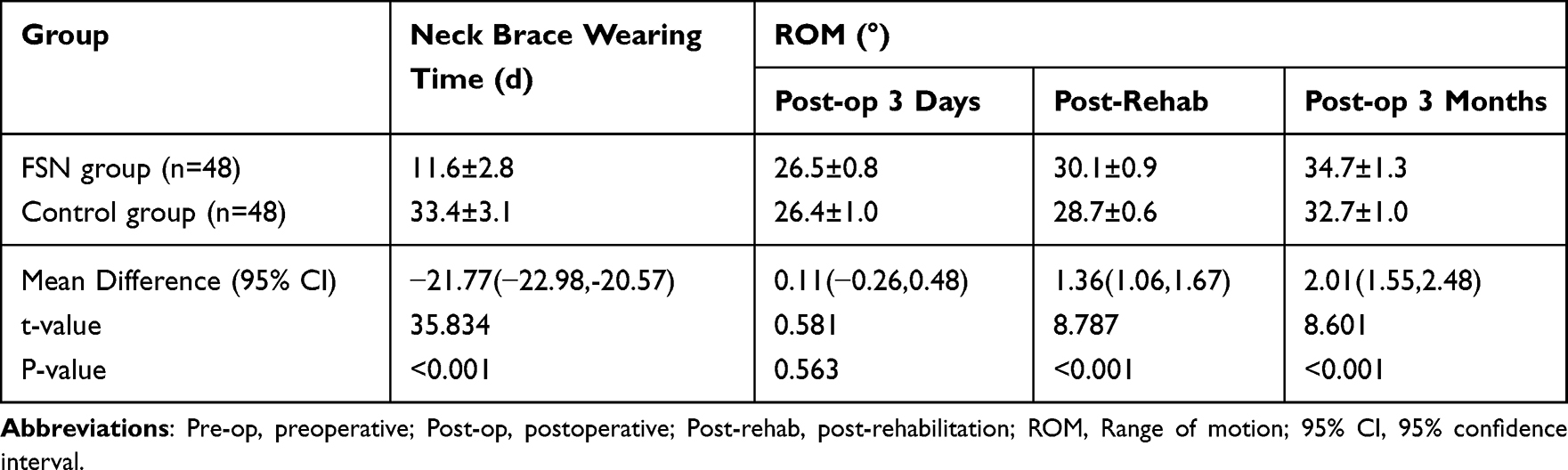 |
Table 6 Comparative Analysis of Duration of Neck Brace Wear and Changes in ROM Across Groups (Mean ± SD) |
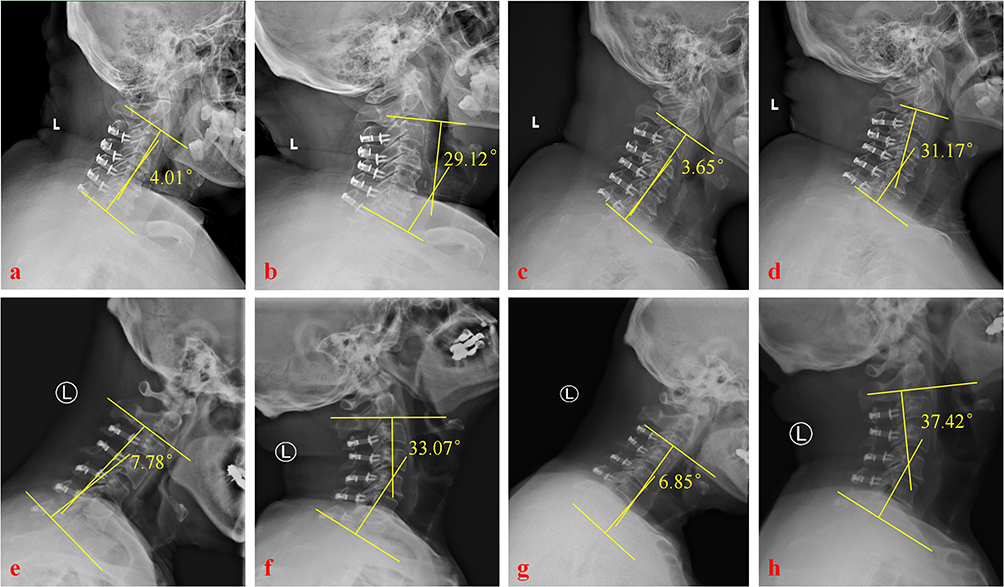 |
Figure 3 Representative cervical flexion–extension radiographs showing cervical range of motion in the control and FSN groups. Panels a–d show the control group, and panels e–h show the FSN group. Cervical ROM was calculated as the C2–7 Cobb angle in extension minus the C2–7 Cobb angle in flexion. Abbreviations: FSN, Fu’s subcutaneous needling; ROM, range of motion. |
Exploratory Subgroup Analysis
Exploratory subgroup analysis showed that the magnitude of benefit associated with FSN appeared greater in patients with higher preoperative pain. In this subgroup, FSN was associated with significantly greater pain improvement than standard rehabilitation (RR = 1.59, 95% CI 1.09–2.32, P = 0.016, Figure 4), whereas no significant difference was observed in patients with lower baseline pain.
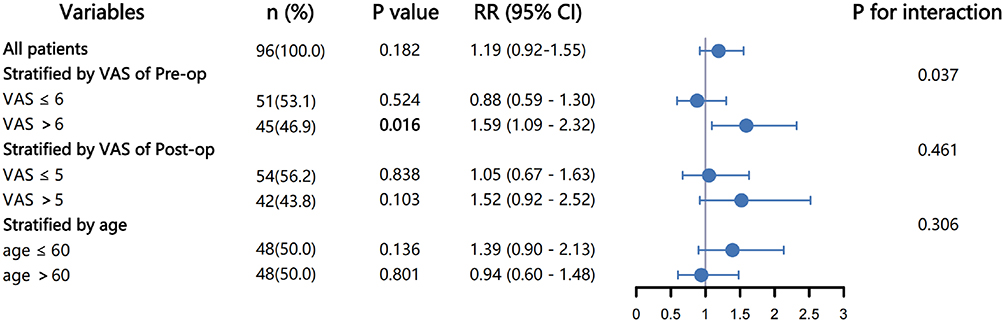 |
Figure 4 Forest plot of exploratory subgroup analyses comparing FSN with standard rehabilitation. Subgroups were stratified by preoperative VAS score, postoperative VAS score, and age. The highlighted bold P value (P = 0.016) indicates the significant result observed in the subgroup with preoperative VAS > 6. Abbreviations: FSN, Fu’s subcutaneous needling; VAS, Visual Analog Scale; RR, risk ratio; CI, confidence interval. |
Discussion
MCSM is a common degenerative condition of the cervical spine. As the disease progresses, spinal cord compression not only results in significant impairment of patients’ quality of life but also imposes substantial economic burdens on society and healthcare systems.18 In 1977, Hirabayashi introduced the concept of EOLP, a procedure designed to expand the spinal canal by unilaterally opening the door of the lamina. This technique effectively preserves spinal stability compared to traditional laminectomy by minimizing structural destruction.19 However, the persistence of postoperative AS remains a well-documented concern. Patients with AS often experience neck and shoulder pain, stiffness, or limitations in motion that can significantly impact their long-term quality of life.20 The primary etiology of AS is thought to involve stripping and injury to the posterior cervical muscles and their attachment points during surgical exposure.21 After surgery, muscles such as the trapezius, rhomboid, and cervical semispinalis may undergo atrophy, fibrosis, or scar formation, leading to persistent pain and stiffness.22 Furthermore, the supraspinous and interspinous ligaments, crucial for cervical stability and serving as muscle attachment points, are severed during EOLP, exacerbating the development of AS.23 Changes in cervical alignment, such as reduced cervical lordosis or kyphosis, may impose additional strain on the cervical posterior muscles, further contributing to discomfort.24 Although EOLP preserves portions of the lamina and spinous structures, thereby having a relatively small impact on cervical mobility, postoperative AS often results in subjective activity limitations. At long-term follow-up, some patients exhibit decreased cervical mobility, likely due to posterior cervical muscle stiffness and alterations in cervical curvature. These findings support the consideration of additional interventions to potentially mitigate AS and improve long-term recovery for patients undergoing EOLP.
Management of postoperative AS typically involves Nonsteroidal anti-inflammatory drugs (NSAIDs) as the first-line therapy for pain relief and reduction of inflammation.25 However, the long-term use of NSAIDs is often limited by adverse effects, including gastrointestinal discomfort, cardiovascular risks, and renal impairment.26 Therefore, physical therapy has become an increasingly important adjunctive approach, focusing on muscle recovery, strength enhancement, and pain reduction to improve overall quality of life.27 Neck braces may also be prescribed postoperatively to limit cervical motion and reduce muscle strain, thereby alleviating pain and discomfort. But long-term use of neck braces may bring a series of adverse effects. Prolonged use of neck braces can limit normal cervical spine movement and keep the small joints immobilized for a long period of time, resulting in reduced circulation of synovial fluid, which may lead to joint stiffness or functional deterioration. In addition, the lack of normal movement may also lead to degeneration of the cartilage of the small joints, increasing the risk of degenerative joint disease. At the same time, the immobilizing effect of the neck brace reduces the normal activity of the neck muscles, leading to muscle atrophy and ligamentous laxity, weakening the supportive effect of the triple-joint complex on the stability of the cervical vertebrae, and further affecting cervical spine stability and physiological curvature.28 Consequently, it is essential to avoid prolonged brace use and incorporate structured rehabilitation training to restore cervical spine dynamics, improve muscle and ligament function, and prevent degeneration of the triple-joint complex.
This retrospective study provides preliminary evidence that Fu’s subcutaneous needling may be a safe adjunct to conventional rehabilitation for postoperative AS after EOLP. In the present study, patients who received FSN in addition to standard rehabilitation experienced greater pain relief, better recovery of cervical sagittal alignment, and greater postoperative ROM than those who received standard rehabilitation alone. These improvements may collectively contribute to better functional recovery and quality of life. These findings are consistent with prior studies showing the effectiveness of FSN for musculoskeletal pain, particularly in the neck and back regions.12,13 Previous studies have suggested that FSN may act through several mechanisms, including targeting myofascial trigger points, reducing muscle adhesions, promoting local blood circulation, and modulating neuromuscular function, which may contribute to pain relief and improved cervical biomechanics.12 FSN also appears to enhance proprioceptive function, as shown in previous studies on acupuncture and neuromuscular coordination in patients with cervical spondylosis. This is particularly relevant for patients with neck pain, as proprioceptive improvement not only increases the accuracy of head repositioning but also reduces pain intensity and restores cervical ROM.29,30 Together, these studies suggest that FSN may have potential advantages in treating postoperative AS.
Our study further emphasizes the importance of cervical sagittal parameters, such as C2-7 Cobb angle, C2-7 SVA, and T1 slope, in postoperative recovery. The importance of cervical spine biomechanical imbalance has received increasing attention as research on spinal sagittal balance and its impact on patient function and quality of life has progressed. Imbalances in cervical sagittal alignment may lead to persistent AS, limited mobility, and diminished quality of life.31 Bębenek et al demonstrated that biomechanical parameters such as cervical lordosis and SVA are important predictors of postoperative recovery outcomes.32 In line with this, our findings showed that FSN was associated with significant improvements in major biomechanical parameters, including T1 slope and ROM. These changes may be related to pain relief, reduced posterior muscle stiffness, and improved cervical mobility during postoperative recovery. Fujibayashi et al found that patients with insufficient neck muscle strength were more likely to develop AS.33 Yu et al suggest that shorter brace use and early mobilization improve cervical mobility and reduce long-term symptoms.34 Consistent with this, our study found that patients in the FSN group showed greater improvements in T1 slope and cervical ROM during postoperative recovery. These findings may be related to reduced posterior muscle stiffness and improved cervical biomechanical function, potentially contributing to a lower risk of persistent AS. Wu et al highlighted the safety of FSN in the treatment of chronic musculoskeletal pain, which aligns with the findings of the present study.35 During the 12-week follow-up period, no significant adverse events were observed in the FSN group. As a micro-invasive therapy, FSN may avoid the risks associated with long-term medication use, such as gastrointestinal and cardiovascular complications, as well as the potential hazards of invasive procedures like nerve blocks. Its micro-invasive nature and minimal risk profile make FSN particularly suitable for postoperative patients, potentially supporting recovery while minimizing treatment-related complications.
In addition, our exploratory subgroup analysis suggested that patients with higher baseline or early postoperative pain experienced more pronounced improvement following FSN. This finding may indicate that patients with more severe postoperative axial symptoms or myofascial hyperactivity are more likely to benefit from adjunctive FSN treatment. One possible explanation is that these patients may have greater soft-tissue tension and neuromuscular dysfunction, making them more responsive to the mechanical modulation effects of FSN.36 Therefore, FSN may have potential value as an adjunctive component of postoperative pain management and comprehensive rehabilitation for selected patients with persistent axial symptoms after EOLP. However, this finding remains exploratory, and future studies are needed to optimize the postoperative application protocol of FSN and clarify its underlying mechanisms.
Despite its promising findings, this study has several limitations. First, the retrospective non-randomized design means that residual confounding cannot be excluded. Although both groups followed the same institutional postoperative pathway, individual analgesic exposure was not quantitatively analyzed. In addition, the exploratory subgroup analyses were based on dichotomized variables, and the clinical relevance of some statistically significant changes was not further assessed using predefined MCID thresholds. Second, this was a single-center study with a modest sample size and a 12-week follow-up, which may limit generalizability and assessment of long-term durability. Further prospective studies with standardized FSN protocols and longer follow-up are needed to confirm these findings.
Conclusion
AS substantially affects the quality of life after posterior cervical surgery when persistent neck pain and stiffness occur. Although EOLP effectively relieves spinal cord compression and improves neurological function, postoperative AS may reduce overall patient satisfaction. In this retrospective observational study, FSN combined with standard rehabilitation was associated with greater pain relief, better functional recovery, improved cervical sagittal alignment, and greater cervical ROM than standard rehabilitation alone in patients with postoperative axial symptoms after EOLP. No obvious FSN-related adverse events were observed during the 12-week follow-up. These findings suggest that FSN may be a promising adjunctive modality associated with improved postoperative recovery, although further prospective studies are warranted to confirm its efficacy, optimize its postoperative application protocol, and determine best practices for implementation.
Abbreviations
AS, Axial symptoms; C2-7 SVA, C2-7 sagittal vertical axis; EOLP, Expansive open-door laminoplasty; FSN, Fu’s subcutaneous needling; MCSM, Multilevel cervical spondylotic myelopathy; JOA, Japanese Orthopedic Association score; ROM, Range of motion; VAS, Visual Analog Score.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Pan-Feng Yu. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Institutional Ethics Review Board of Peking University People’s Hospital (IRB No. 2024-159) and conducted in accordance with the Declaration of Helsinki. Given the retrospective design and use of anonymized data, the requirement for informed consent was waived by the Ethics Committee.
Author Contributions
Hong-Zhen Li, Yu-Qiao Li, and Peng-Hui Xia are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by a grant from the Natural Science Foundation of Beijing Municipality (No.2150000099), Special Work of the Ministry of Industry and Information Technology (No.zbys-zyc-2023-8), and the National Key R&D Program of China (No. 2022YFB4703000).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tetreault L, Goldstein CL, Arnold P, et al. Degenerative cervical myelopathy: a spectrum of related disorders affecting the aging spine. Neurosurgery. 2015;77(Suppl 4):S51–13. doi:10.1227/NEU.0000000000000951
2. Fehlings MG, Tetreault L, Nater A, et al. The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery. 2015;77(Suppl 4):S1–5. doi:10.1227/NEU.0000000000000953
3. Fehlings MG, Ibrahim A, Tetreault L, et al. A global perspective on the outcomes of surgical decompression in patients with cervical spondylotic myelopathy: results from the prospective multicenter AOSpine international study on 479 patients. Spine. 2015;40(17):1322–1328. doi:10.1097/BRS.0000000000000988
4. Su N, Fei Q, Wang BQ, et al. Comparison of clinical outcomes of expansive open-door laminoplasty with unilateral or bilateral fixation and fusion for treating cervical spondylotic myelopathy: a multi-center prospective study. BMC surgery. 2019;19(1):116. doi:10.1186/s12893-019-0583-8
5. Kimura A, Shiraishi Y, Inoue H, Endo T, Takeshita K. Predictors of persistent axial neck pain after cervical laminoplasty. Spine. 2018;43(1):10–15. doi:10.1097/BRS.0000000000002267
6. Wang SJ, Jiang SD, Jiang LS, Dai LY. Axial pain after posterior cervical spine surgery: a systematic review. Eur Spine J. 2011;20(2):185–194. doi:10.1007/s00586-010-1600-x
7. Fujiwara H, Oda T, Makino T, et al. Impact of cervical sagittal alignment on axial neck pain and health-related quality of life after cervical laminoplasty in patients with cervical spondylotic myelopathy or ossification of the posterior longitudinal ligament: a prospective comparative study. Clin Spine Surg. 2018;31(4):E245–e251. doi:10.1097/BSD.0000000000000619
8. Oyekan AA, LeVasseur CM, Chen SR, et al. The effects of cervical orthoses on head and intervertebral range of motion. Spine. 2023;48(22):1561–1567. doi:10.1097/BRS.0000000000004755
9. Cheung JPY, Cheung PWH, Law K, et al. Postoperative rigid cervical collar leads to less axial neck pain in the early stage after open-door laminoplasty-a single-blinded randomized controlled trial. Neurosurgery. 2019;85(3):325–334. doi:10.1093/neuros/nyy359
10. Brannigan JFM, Dohle E, Critchley GR, et al. Adverse events relating to prolonged hard collar immobilisation: a systematic review and meta-analysis. Glob spine J. 2022;12(8):1968–1978. doi:10.1177/21925682221087194
11. Li J, Liu J, Yang R, Shen Y, Wang L. Hounsfield units of vertebrae as a predictor of cervical deep paraspinal muscles atrophy and neck pain in degenerative cervical myelopathy. J Neurosurg Spine. 2024;41(6):726–733. doi:10.3171/2024.5.SPINE231330
12. Fu ZH, Wang JH, Sun JH, Chen XY, Xu JG. Fu’s subcutaneous needling: possible clinical evidence of the subcutaneous connective tissue in acupuncture. J Altern Complementary Med. 2007;13(1):47–51. doi:10.1089/acm.2006.6125
13. Huang CH, Tsai LH, Sun MF, et al. Rapid improvement in neck disability, mobility, and sleep quality with chronic neck pain treated by Fu’s subcutaneous needling: a randomized control study. Pain Res Manag. 2022;2022:7592873. doi:10.1155/2022/7592873
14. Langevin HM, Churchill DL, Cipolla MJ. Mechanical signaling through connective tissue: a mechanism for the therapeutic effect of acupuncture. FASEB J. 2001;15(12):2275–2282. doi:10.1096/fj.01-0015hyp
15. Chiu P-E, Fu Z, Pan H-C, et al. Fu’s subcutaneous needling facilitates muscle repair by regulating mitochondrial homeostasis in rat with chronic peripheral nervous pain. Front Physiol. 2025;16. doi:10.3389/fphys.2025.1640735
16. Bosque M, Margalef R, Carvajal O, Álvarez D, Santafe MM. Dry needling produces mild injuries irrespective to muscle stiffness and tension in ex vivo mice muscles. Pain Res Manag. 2022;2022:8920252. doi:10.1155/2022/8920252
17. Rodríguez-Huguet M, Vinolo-Gil MJ, Góngora-Rodríguez J. Dry needling in physical therapy treatment of chronic neck pain: systematic review. J Clin Med. 2022;11(9):2370. doi:10.3390/jcm11092370
18. Houten JK, Shahsavarani S, Verma RB. The natural history of degenerative cervical myelopathy. Clin Spine Surg. 2022;35(10):396–402. doi:10.1097/BSD.0000000000001405
19. Hirabayashi K, Watanabe K. A Review of My Invention of Expansive Laminoplasty. Neurospine. 2019;16(3):379–382. doi:10.14245/ns.1938272.136
20. Wang M, Luo XJ, Deng QX, Li JH, Wang N. Prevalence of axial symptoms after posterior cervical decompression: a meta-analysis. Eur Spine J. 2016;25(7):2302–2310. doi:10.1007/s00586-016-4524-2
21. Ruan C, Jiang W, Lu W, et al. Analysis of risk factors for axial symptoms after posterior cervical open-door laminoplasty. J Orthopaedic Surg Res. 2023;18(1):954. doi:10.1186/s13018-023-04426-9
22. Pinter ZW, Salmons H, Townsley S, et al. Semispinalis cervicis sarcopenia is associated with worsening cervical sagittal balance and junctional alignment following posterior cervical fusion for myelopathy. Clin Spine Surg. 2023;36(7):E288–e293. doi:10.1097/BSD.0000000000001366
23. Chen C, Yang C, Yang S, et al. Clinical and radiographic outcomes of modified unilateral open-door laminoplasty with posterior muscle-ligament complex preservation for cervical spondylotic myelopathy. Spine. 2019;44(24):1697–1704. doi:10.1097/BRS.0000000000003158
24. Kim BJ, Cho SM, Hur JW, Cha J, Kim SH. Kinematics after cervical laminoplasty: risk factors for cervical kyphotic deformity after laminoplasty. Spine J. 2021;21(11):1822–1829. doi:10.1016/j.spinee.2021.06.010
25. Borgeat A, Ofner C, Saporito A, Farshad M, Aguirre J. The effect of nonsteroidal anti-inflammatory drugs on bone healing in humans: a qualitative, systematic review. J Clin Anesth. 2018;49:92–100. doi:10.1016/j.jclinane.2018.06.020
26. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: a current perspective. Biochem Pharmacol. 2020;180:114147. doi:10.1016/j.bcp.2020.114147
27. Lorentz NA, Galetta MS, Zabat MA, et al. Post-operative physical therapy following cervical spine surgery: analysis of patient-reported outcomes. Cureus. 2023;15(6):e40559. doi:10.7759/cureus.40559
28. McKeon JF, Alvarez PM, Castaneda DM, et al. Cervical collar use following cervical spine surgery: a systematic review. JBJS Reviews. 2024;12(9). doi:10.2106/JBJS.RVW.24.00114
29. Gao Z, Liu GF, Zhang J, Ji LX. Acupuncture for neck pain caused by cervical spondylosis: a systematic review and meta-analysis protocol. BMJ open. 2020;10(12):e038455. doi:10.1136/bmjopen-2020-038455
30. Espí-López GV, Aguilar-Rodríguez M, Zarzoso M, et al. Efficacy of a proprioceptive exercise program in patients with nonspecific neck pain: a randomized controlled trial. Eur J Phys Rehabil Med. 2021;57(3):397–405. doi:10.23736/S1973-9087.20.06302-9
31. Patwardhan AG, Khayatzadeh S, Havey RM, et al. Cervical sagittal balance: a biomechanical perspective can help clinical practice. Eur Spine J. 2018;27(Suppl 1):25–38. doi:10.1007/s00586-017-5367-1
32. Bębenek A, Dominiak M, Godlewski B. Cervical sagittal balance: impact on clinical outcomes and subsidence in anterior cervical discectomy and fusion. Biomedicines. 2023;11(12):3310. doi:10.3390/biomedicines11123310
33. Fujibayashi S, Neo M, Yoshida M, et al. Neck muscle strength before and after cervical laminoplasty: relation to axial symptoms. J Spinal Disord Tech. 2010;23(3):197–202. doi:10.1097/BSD.0b013e3181a1a73e
34. Yu Q, Ren Y, Wang Z, et al. The effect of a cervical brace on postoperative axial symptoms following single-level anterior cervical discectomy and fusion. Clin Spine Surg. 2025;38(3):E181–e185. doi:10.1097/BSD.0000000000001696
35. Wu CY, Chou LW, Huang SW, et al. Effects of Fu’s subcutaneous needling on postoperative pain in patients receiving surgery for degenerative lumbar spinal disorders: a single-blind, randomized controlled trial. J Pain Res. 2024;17:2325–2339. doi:10.2147/JPR.S465417
36. Chiu PE, Fu Z, Tsai YC, et al. Fu’s subcutaneous needling promotes axonal regeneration and remyelination by inhibiting inflammation and endoplasmic reticulum stress. Transl Res. 2024;273:46–57. doi:10.1016/j.trsl.2024.06.005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.