Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Effectiveness of cognitive behavioral therapy integrated with systematic desensitization, cognitive behavioral therapy combined with eye movement desensitization and reprocessing therapy, and cognitive behavioral therapy combined with virtual reality exposure therapy methods in the treatment of flight anxiety: a randomized trial
Authors Triscari MT, Faraci P ![]() , Catalisano D, D’Angelo V, Urso V
, Catalisano D, D’Angelo V, Urso V
Received 30 July 2015
Accepted for publication 21 August 2015
Published 7 October 2015 Volume 2015:11 Pages 2591—2598
DOI https://doi.org/10.2147/NDT.S93401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Maria Teresa Triscari,1 Palmira Faraci,2 Dario Catalisano,3 Valerio D’Angelo,1 Viviana Urso1
1Laboratory for Psychosomatic Disorders, Local Health Trust, Palermo, Italy; 2Faculty of Human and Social Sciences, University of Enna “Kore”, Enna, Italy; 3Italian Flight Safety Committee, Aeroporto di Fiumicino, Fiumicino (RM), Italy
Abstract: The purpose of the research was to compare the effectiveness of the following treatment methods for fear of flying: cognitive behavioral therapy (CBT) integrated with systematic desensitization, CBT combined with eye movement desensitization and reprocessing therapy, and CBT combined with virtual reality exposure therapy. Overall, our findings have proven the efficacy of all interventions in reducing fear of flying in a pre- to post-treatment comparison. All groups showed a decrease in flight anxiety, suggesting the efficiency of all three treatments in reducing self-report measures of fear of flying. In particular, our results indicated significant improvements for the treated patients using all the treatment programs, as shown not only by test scores but also by participation in the post-treatment flight. Nevertheless, outcome measures maintained a significant effect at a 1-year follow-up. In conclusion, combining CBT with both the application of eye movement desensitization and reprocessing treatment and the virtual stimuli used to expose patients with aerophobia seemed as efficient as traditional cognitive behavioral treatments integrated with systematic desensitization.
Keywords: flight anxiety, fear of flying, aerophobia, cognitive behavioral therapy, EMDR, VRET
Introduction
Although commercial air travels have become one of the safest forms of transport, many people are still affected by aerophobia. In fact, the last years have been characterized by a growing request for fear of flying intervention programs. Nevertheless, rather few controlled studies on the compared effectiveness of different treatments for flight anxiety were conducted.1,2 Phobias are the experiences of an unreasonable amount of anxiety regarding a particular object or situation, causing the stimulus to be completely avoided or endured with intense anxiety, which interferes with one’s normal functioning.3 Specific phobias are set apart from ordinary fears by their impact on daily functioning: distress may lead to impairments, such as being unable to maintain a job or social relations.4 As regards their etiology, phobias result from an interaction between a disposition to physiologically experienced fear and a psychological vulnerability to experience anxiety.5 The flying phobia appears as a heterogeneous phenomenon, with many components, not all of which are specific to flight itself, characterized by three different kinds of symptoms: physiological, psychological, and behavioral reactions. Fear of flying can interfere with one’s personal and work life, and it can range from moderate apprehension, to considerable discomfort, to a disabling phobia.
As flying has become a more frequently integrated part of our industrialized society, several treatment programs – concerning anxiety management approaches, provision of accurate information regarding airplanes and flying, and exposure techniques – have been developed to treat patients who suffer from fear of flying and are now available to those who are motivated to overcome their problem. Most of the treatment protocols usually include exposure in vivo or in-flight simulators, stress inoculation training, systematic desensitization, and relaxing training.6
While cognitive behavioral therapy (CBT) is considered to be the first-line therapy for fear of flying, there are limited data on whether other psychotherapeutic techniques are also effective in treating aerophobia. Eye movement desensitization and reprocessing (EMDR) is a relatively new technique of treatment based on the theory that disturbing experiences are stored in the brain and the associated negative emotions become trapped in the body, preventing the person from processing them during periods of rapid eye movement. EMDR may aid to unlock these thoughts, helping the brain to process them without experiencing the negativity that was once associated, therefore reducing anxiety. Specifically, the therapist helps the person to recall events, images, or thoughts and gently couples rapid eye movements to each event by careful observation and then redirects the eye movements using a stimulant or distraction such as a light, object, or music.
The effectiveness of CBT for fear of flying has been scientifically well established,2 whereas the effectiveness of EMDR in the treatment of a specific phobia has not been long since investigated.7–9 This method is still lacking empirical evidence supporting its efficacy with complex or trauma-related phobias.10–13 Therefore, the application of EMDR with specific phobias merits further clinical and research attention.
Virtual reality exposure therapy (VRET14,15) provides a controlled environment for people who are exposed to a computer-generated virtual world that simulates a real experience with the feared object or situation. Some experimental studies to examine the efficacy of VRET have found encouraging results in treating anxiety disorders and a wide range of specific phobias,16 including claustrophobia,17 acrophobia,18–20 agoraphobia,21,22 and flying phobia.17,23–25
The aim of the present paper was to compare the effectiveness of the following treatment methods for fear of flying: cognitive behavioral therapy integrated with systematic desensitization (CBT-SD), cognitive behavioral therapy combined with eye movement desensitization and reprocessing therapy (CBT-EMDR), and cognitive behavioral therapy combined with virtual reality exposure therapy (CBT-VRET). Sequence of the design included a pre-treatment assessment, an intervention phase consisting of 10 weekly treatment sessions, a post-treatment assessment 1 week after the last treatment session, and a 1-year follow-up assessment. It was hypothesized that CBT-SD, CBT-EMDR, and CBT-VRET would similarly reduce flying anxiety and avoidance between pre- and post-treatment assessments based on outcome measures, which included self-report instruments and flying avoidance. Fear of flying levels were derived from the participants’ mean scores obtained at pre-treatment and post-treatment assessment phases. It was expected that the analyses would reveal statistically significant changes in fear of flying measures with a decreasing trend from pre- to post-treatment assessments. To reduce measurement error, self-report measures with adequate psychometric properties and sensitivity to treatment effects were included.
Methods
Participants
Participants were 65 flight phobics self-referred to the Laboratory for Psychosomatic Disorders of the Local Health Trust of Palermo, asking for a training program aimed to reduce or eliminate fear of flying. They were 30.8% males and 69.2% females, with a mean age of 43.52 (standard deviation [SD] =10.42; range =24–70). All participants were involved in the assessment phase before and after the treatment program. They were interviewed with the Millon Clinical Multiaxial Inventory (MCMI-III26,27), conducted by a trained psychologist and met the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) criteria for neurotic diseases, phobia, anxiety, and panic attacks. Exclusion criteria were neurological disorders, posttraumatic stress disorder or acute stress disorder not related to fear of flying, severe agoraphobia, and a comorbid psychiatric diagnosis. Subjects were also excluded if they had suicidal tendencies or did not want to stabilize their antidepressant medication during the course of treatment.
The first group received the CBT-SD program. It consisted of 22 patients (36.4% men and 63.6% women), with a mean age of 43.57 years (SD =10.13; range =29–70). They were employers (57.1%), teachers (4.8%), freelancers (23.7%), pensioners (4.8%), housewives (4.8%), and managers (4.8%). The most frequent marital status was married (60%), followed by single (30%), single in a committed relationship (5%), and divorced (5%). Educational level ranged from lower school certificate (4.8%) to university graduates (28.6%), with 57.1% high-school graduates and 9.5% postuniversity certificates.
The second group received the CBT-EMDR program. It consisted of 22 patients (31.8% men and 68.2% women), with an average age of 41.55 years (SD =10.89; range =24–63). They were employers (45.5%), teachers (4.5%), freelancers (18.2%), unemployed people (9.1%), housewives (4.5%), manager (9.1%), students (4.5%), and entrepreneurs (4.5%). The most frequent marital status was married (47.6%), followed by single (42.9%), single in a committed relationship (4.8%), and widowed (4.8%). Educational level ranged from lower school certificate (4.5%) to university graduates (63.6%), with 31.8% high-school graduates.
The third group received the CBT-VRET program. It consisted of 21 patients (23.8% men and 76.2% women), with an average age of 45.52 years (SD =10.32; range =27–67). They were employers (33.3%), teachers (14.3%), freelancers (23.8%), pensioners (4.8%), housewives (9.5%), manager (9.5%), and students (4.8%). The most frequent marital status was married (57.1%), followed by single (28.6%), single in a committed relationship (4.8%), and divorced (9.5%). Educational level ranged from high-school graduates (33.3%) to university graduates (47.6%), with 19% postuniversity certificates.
After complete description of the study to the participants, written informed consent was obtained. Institutional review board (IRB) approval was obtained. This research was approved by the Italian Ministry of Health with registration n. 311 and protocol n. DGPREV/P/28610 F.3 A.D./317.
Procedure
Prior to enrolling in the study, participants were informed about the aim of the research, and a strong emphasis was put on voluntary adherence and data confidentiality. To minimize the subject characteristics that might differentially affect treatment effects across individuals, flight phobic patients were randomly assigned to one of three experimental groups based on a previously generated random numbers table.
The three treatment programs were carried out in 10 weekly sessions, each one lasting 2 hours, by an experienced clinical psychotherapist and two psychologists. All the participants were treated in small groups during the first three sessions consisting of 1) psychoeducation, providing information about anxiety, teaching how to manage anxiety, and enhancing a differential analysis of fear, phobia, and anxiety; 2) cognitive and behavioral techniques, introducing both in vivo and imaginal exposure and teaching how to restructure dysfunctional thoughts; 3) relaxation techniques, teaching how to practice Schultz’s autogenic training or progressive relaxation; and 4) education about flying, providing data regarding the basic notions of flight and aviation, including safety issues, objective risks, turbulence, and accidents. Sessions 4–6 were specific to each treatment group. From sessions 7–10, the program was carried out identically for the three treatment groups. After visiting the air traffic control tower, patients could ask their questions to both an airline pilot and an air traffic controller. A demo flight allowed them to go through the different phases that precede a real flight. A simulated departure in a real airplane and a real flight ended the treatment.
Instruments
Two inventories were administered to the participants for assessing several aspects of fear of flying, focusing on feelings, attitudes, and cognitions referring to specific flight-related events:
- Flight Anxiety Situations Questionnaire (FAS28) (32 items), which measures the level of anxiety produced by specific flying situations. It consists of three subscales: Generalized Flight Anxiety, referring to anxiety experienced in connection with airplanes in general, regardless of personal involvement in a flight situation (eg, seeing or hearing planes or bringing someone to the airport); Anticipatory Flight Anxiety, pertaining to anxiety experienced before the time the flight actually starts (eg, planning a trip, boarding the plane); and In-Flight Anxiety, concerning anxiety experienced during a flight, from takeoff until landing (eg, different situations in flight). Respondents are asked to circle the number corresponding to their level of anxiety in the situations mentioned, using a scale from 1 (no anxiety) to 5 (overwhelming anxiety).
- Flight Anxiety Modality Questionnaire (FAM28), which focuses on symptom expressions, such as physiological responses of anxiety and thoughts related to the danger of flying. The FAM consists of 18 items structured into two subscales: Somatic Modality, referring to physical symptoms, and Cognitive Modality, pertaining to the presence of distressing cognitions. Here the respondents are asked to rate the degree to which each item accurately describes the intensity of their own reaction using a scale from 1 (not at all) to 5 (very intensely).
Both FAS and FAM revealed good psychometric properties and cover distinct reactions to aerophobia, in terms of behavior, physiology, and cognitions. Besides, FAS allows assessing one’s responses at various stages of a flight, from the preliminary phase to the actual flight. Therefore, the administered instruments seem helpful in obtaining a thorough and accurate assessment of the most relevant phobic stimuli. Based on their sensitivity to change, they appear suitable to evaluate treatment outcomes on flight anxiety. In particular, both FAS and FAM may be supportive in measuring differential treatment effects on specific aspects of fear of flying.29,30
Design
An experimental group design was applied with measurements at three stages: pre-treatment, post-treatment, and at a follow-up of 1 year postflight. The first group received the CBT-SD treatment, the second group received the CBT-EMDR treatment, and the third group received the CBT-VRET treatment. As dependent variables, data were collected regarding 1) flight anxiety situations, in terms of generalized flight anxiety, anticipatory flight anxiety, and in-flight anxiety and 2) flight anxiety modality, in terms of somatic modality and cognitive modality.
We analyzed differences both in pre- and post-treatment measures and in pre- and follow-up measures on the FAS and FAM with paired t-tests to evaluate the degree of change. Besides, as a measure of effect size, we calculated Cohen’s d coefficients within groups. For the purpose of interpretation, according to Cohen’s conventional criteria, d=0.20 is considered to be a slight effect, d=0.50 is considered to be a moderate effect, and d=0.80 is considered to be a substantial effect. An analysis of means comparison, computed with a one-way analysis of variance (ANOVA), was performed to determine whether there was any evidence that the average scores of the three groups were different at the pre-test. A comparison of both the post-treatment and follow-up scores between groups was also conducted via one-way ANOVA.
Results
Based on paired t-test results, both FAS and FAM subscales seemed to be sensitive to the CBT-SD treatment intervention. On all scales, the difference between pre- and post-treatment scores revealed a high effect size (Cohen’s d ranged from 1.32 to 2.23) (Table 1).
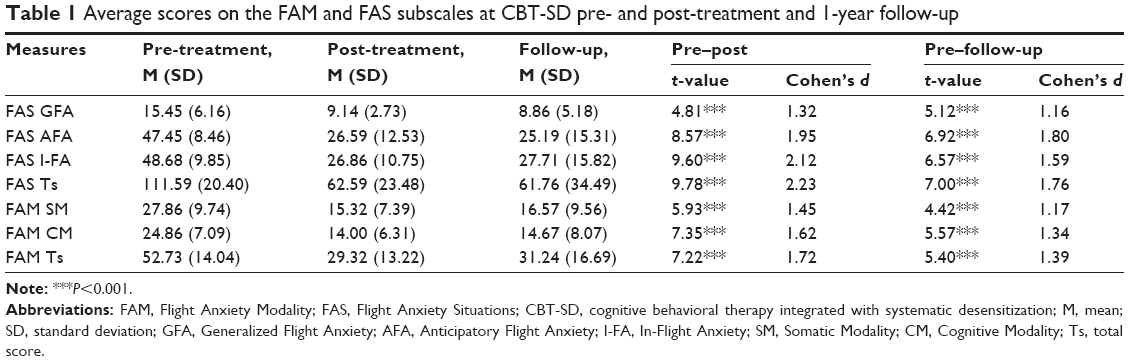 | Table 1 Average scores on the FAM and FAS subscales at CBT-SD pre- and post-treatment and 1-year follow-up |
As shown in Table 2, both FAS and FAM scales seemed to be sensitive to the CBT-EMDR treatment intervention. The difference between pre- and post-treatment scores reported a very high effect size for all self-report instruments’ subscales (Cohen’s d ranged from 1.23 to 2.67).
 | Table 2 Average scores on the FAM and FAS subscales at CBT-EMDR pre- and post-treatment and 1-year follow-up |
As shown in Table 3, both FAS and FAM scales seemed to be sensitive to the CBT-VRET treatment intervention. On all subscales, the difference between pre- and post-treatment scores showed a very high effect size (Cohen’s d ranged from 1.11 to 2.55). Composite scores for each measure were computed by summing the responses of subset of the subscales’ items. The min–max possible values for each composite score is 6–30 (FAS Generalized Flight Anxiety), 11–55 (FAS Anticipatory Flight Anxiety), 12–60 (FAS In-Flight Anxiety), 29–145 (FAS Total score), 10–50 (FAM Somatic Modality), 7–35 (FAM Cognitive Modality), and 17–85 (FAM Total score).
 | Table 3 Average scores on the FAM and FAS subscales at CBT-VRET pre- and post-treatment and 1-year follow-up |
A one-way ANOVA was performed to contrast pre-treatment measures between the three experimental groups. No mean differences were found between CBT-SD, CBT-EMDR, and CBT-VRET groups, indicating that the three groups did not differ previously to the intervention: FAS Generalized Flight Anxiety (F=1.54; P=0.223), FAS Anticipatory Flight Anxiety (F=0.90; P=0.413), FAS In-Flight Anxiety (F=0.15; P=0.860), FAS Total score (F=0.54; P=0.584), FAM Somatic Modality (F=0.48; P=0.624), FAM Cognitive Modality (F=0.96; P=0.389), and FAM Total score (F=0.47; P=0.627). Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET pre-treatment are reported in Figure 1.
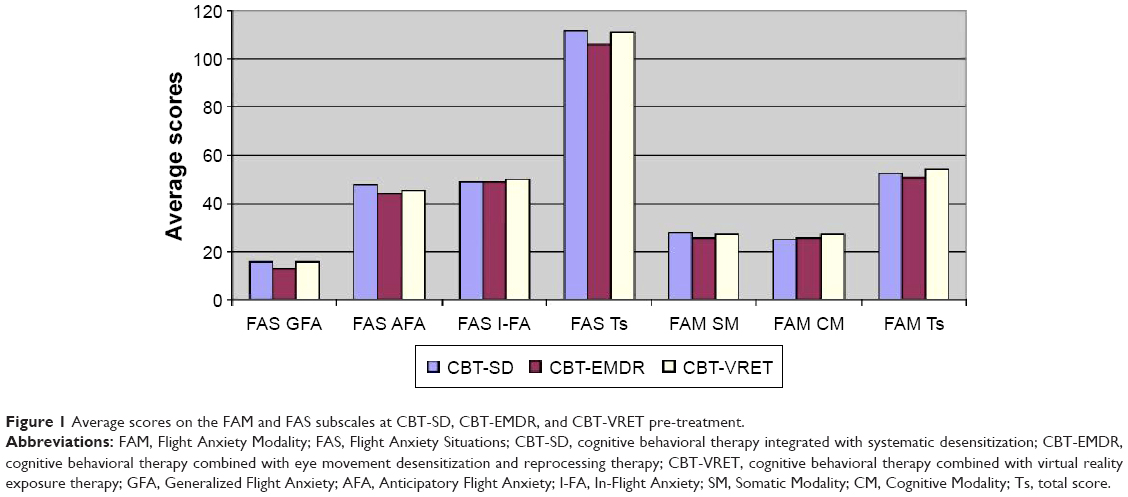 | Figure 1 Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET pre-treatment. |
Based on our findings, CBT-SD, CBT-EMDR, and CBT-VRET treatments seemed to be effective in reducing fear of flying without statistical significant differences. No mean differences were found between the three groups after treatment: FAS Generalized Flight Anxiety (F=1.22; P=0.303), FAS Anticipatory Flight Anxiety (F=0.39; P=0.682), FAS In-Flight Anxiety (F=0.44; P=0.649), FAS Total score (F=0.28; P=0.757), FAM Somatic Modality (F=0.00; P=0.996), FAM Cognitive Modality (F=0.22; P=0.800), and FAM Total score (F=0.06; P=0.947). Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET post-treatment are presented in Figure 2.
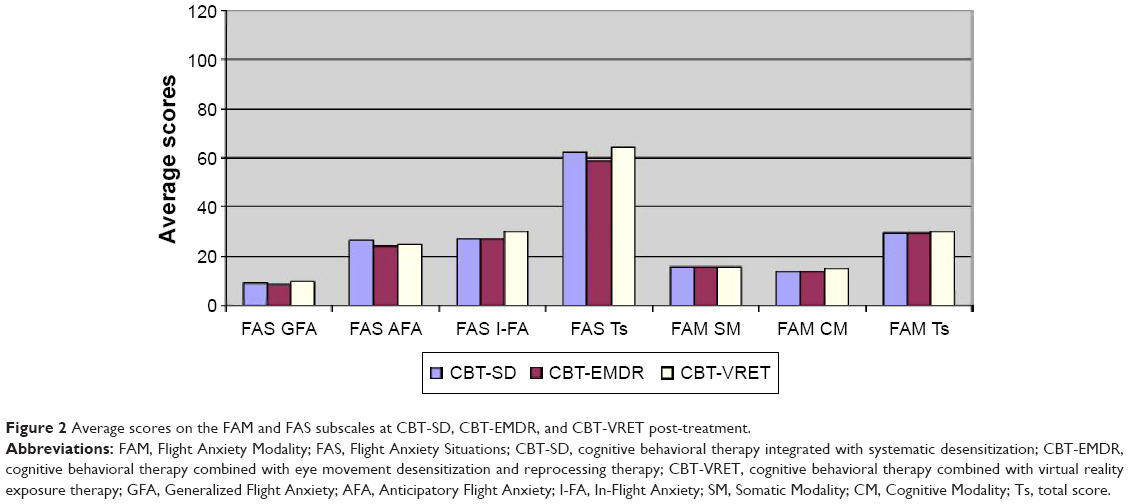 | Figure 2 Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET post-treatment. |
Similarly, no mean differences were found between the three groups at the follow-up: FAS Generalized Flight Anxiety (F=1.30; P=0.281), FAS Anticipatory Flight Anxiety (F=0.05; P=0.954), FAS In-Flight Anxiety (F=0.51; P=0.604), FAS Total score (F=0.30; P=0.745), FAM Somatic Modality (F=1.10; P=0.341), FAM Cognitive Modality (F=0.10; P=0.907), and FAM Total score (F=0.55; P=0.580). Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET follow-up measures are reported in Figure 3. Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET pre-test, post-test and follow-up are represent in Figure 4.
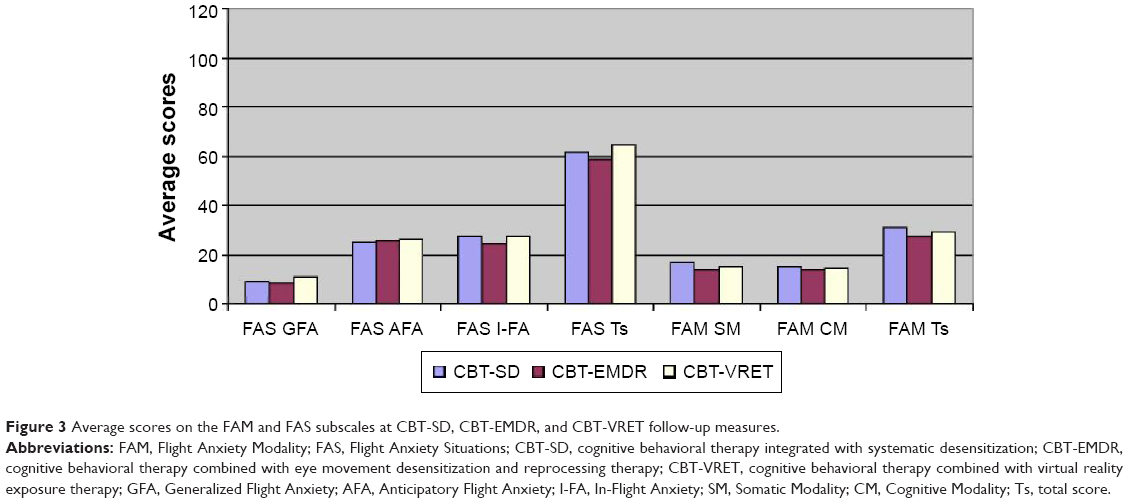 | Figure 3 Average scores on the FAM and FAS subscales at CBT-SD, CBT-EMDR, and CBT-VRET follow-up measures. |
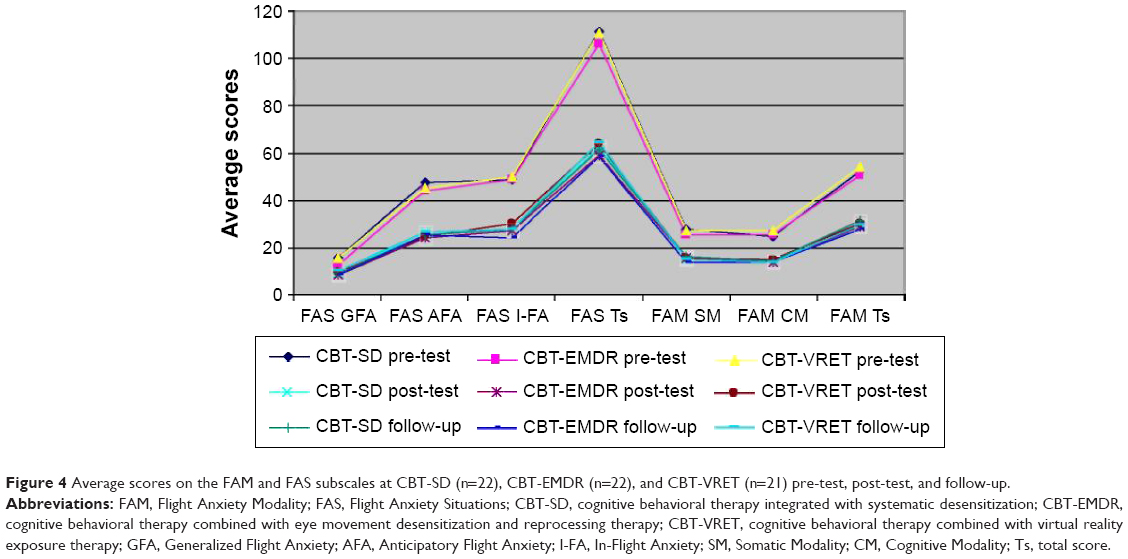 | Figure 4 Average scores on the FAM and FAS subscales at CBT-SD (n=22), CBT-EMDR (n=22), and CBT-VRET (n=21) pre-test, post-test, and follow-up. |
As a very important outcome index, 21 patients (95.5%) were able to board on a real flight at the end of the CBT-SD program, 20 patients (90.9%) flew at the end of the CBT-EMDR program, whereas all the 21 phobics (100%) flew at the end of the CBT-VRET program.
Discussion
To our knowledge, this is the first study in which CBT-SD, CBT-EMDR, and CBT-VRET are directly compared with patients fearful of flying. The outcomes of the reported randomized trial indicate that combining CBT with both the application of eye movement desensitization and reprocessing treatment, and the virtual stimuli used to expose patients with aerophobia seemed as efficient as traditional cognitive behavioral treatments integrated with systematic desensitization.
Overall, our findings have proven the efficacy of all interventions in reducing fear of flying in a pre- to post-treatment comparison. All groups showed a decrease in flight anxiety as evidenced by the test scores, suggesting the efficiency of the three treatments in reducing self-report measures of fear of flying. In particular, our results indicated significant improvements for the treated patients using all the treatment programs, as shown not only by test scores but also by participation in the post-treatment flight. Nevertheless, outcome measures maintained a significant effect at a 1-year follow-up.
Although all applied treatment methods seem equally efficient, each of these three methods have positive and negative aspects, advantages, and disadvantages: on the one hand, the CBT is the cheapest and less complex method, and on the other hand, CBT-VRET is the most expensive method (the cost of the entire equipment is high), but sessions are very short (just half an hour). Finally, CBT-EMDR method needs very high professional competences because EMDR is a complex psychotherapeutic approach that integrates many aspects of a variety of theoretical orientations. Moreover, it is crucial that in the use of EMDR, appropriate attention is paid to treatment fidelity; the standardized procedures and protocols are being used and have been receiving preliminary testing: untested additions to standardized protocols will diminish treatment effectiveness. However, all three methods and their integrations seemed to be effective ways to address pressing a social and widespread pathology called “fear of flying”.
Even though these preliminary results showed the comparable effectiveness of all three examined treatment procedures, upcoming research is strongly recommended. Purposely, new developments are needed with a larger sample size and the incorporation of both control groups and additional experimental groups such as EMDR and VRET treatment method without CBT combination.
In conclusion, given the powerful effects observed, our findings suggest that further investigation of both EMDR and VRET for fear of flying is warranted. It was hoped that results from this study would encourage future research with patients who suffer from fear of flying to be investigated in the long term.
Disclosure
The authors report no conflicts of interest in this work.
References
Bor R, Van Gerwen LJ. Psychological Perspectives on Fear of Flying. Hampshire: Ashgate; 2003. | ||
Van Gerwen LJ, Spinhoven P, Diekstra RF, Van Dyck R. Behavioral and cognitive group treatment for fear of flying: a randomized controlled trail. J Behav Ther Exp Psychiatry. 2006;37(206):358–371. | ||
Durand VM, Barlow DH. Essentials of Abnormal Psychology. 3rd ed. Belmont, CA: Wadsworth-Thomson Learning; 2003. | ||
Mogotsi M, Kaminer D, Stein DJ. Quality of life in the anxiety disorders. Harv Rev Psychiatry. 2000;8(6):273–282. | ||
Barlow DH. Anxiety and its Disorders: The Nature and Treatment of Anxiety and Panic. 2nd ed. New York, NY: Guilford Press; 2002. | ||
Foreman EI, Van Gerwen L. Fly Away Fear: Overcoming Your Fear of Flying. London: Karnac Books; 2008. | ||
Shapiro F. Eye Movement Desensitization and Reprocessing Basic Principles, Protocols, and Procedures. New York, NY: The Guilford Press; 2001. | ||
Bae HK, Park YC. Eye movement desensitization and reprocessing for adolescent depression. Psychiatry Investig. 2008;5:60–65. | ||
Triscari MT, Faraci P, D’Angelo V, Urso V, Catalisano D. Two treatments for fear of flying compared: cognitive behavioral therapy combined with systematic desensitization or eye movement desensitization and reprocessing (EMDR). Aviat Psychol Appl Hum Factors. 2011;1(1):9–14. | ||
Fernandez I, Faretta E. EMDR in the treatment of panic disorder with agoraphobia. Clin Case Stud. 2007;6:44–63. | ||
Gauvreau P, Bouchard SP. Preliminary evidence for the efficacy of EMDR in treating generalized anxiety disorder. J EMDR Pract Res. 2008;2:26–40. | ||
Newgent RA, Paladino DA, Reynolds CA. Single session treatment of nontraumatic fear of flying with eye movement eesensitization reprocessing: pre and post September 11. Clin Case Stud. 2006;5:25–36. | ||
Schurmans K. EMDR treatment of choking phobia. J EMDR Pract Res. 2007;1:118–121. | ||
Glantz K, Durlach NI, Barnett RC, Aviles WA. Virtual reality (VR) for psychotherapy: from the physical to social environment. Psychotherapy. 1996;33:464–473. | ||
Rothbaum BO, Hodges LF, Kooper IR. Virtual reality exposure therapy. J Psychother Pract Res. 1997;6:219–226. | ||
Parsons TD, Rizzo AA. Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: a meta-analysis. J Behav Ther Exp Psychiatry. 2008;39:250–261. | ||
Botella C, Osma J, Garcia-Palacios A, Quero S, Baños RM. Treatment of flying phobia using virtual reality: data from a 1-year follow-up using a multiple baseline design. Clin Psychol Psychother. 2004;11:311–323. | ||
Coelho CM, Waters AM, Hine TJ, Wallis G. The use of virtual reality in acrophobia research and treatment. J Anxiety Disord. 2009;23(5):563–574. | ||
Emmelkamp PM, Krijn M, Hulsbosch AM, de Vries S, Schuemie MJ, van der Mast CA. Virtual reality treatment versus exposure in vivo: a comparative evaluation in acrophobia. Behav Res Ther. 2002;40(5):509–516. | ||
Krijn M, Emmelkamp PMG, Biemond R, de Wilde de Ligny C, Schuemie MJ, van der Mast CAPG. Treatment of acrophobia in virtual reality: the role of immersion and presence. Behav Res Ther. 2004;42:229–239. | ||
North MM, North SM, Coble JR. Effectiveness of virtual environment desensitization in the treatment of agoraphobia. Presence. 1996;5:346–352. | ||
Peñate W, Pitti CT, Bethencourt JM, de la Fuente J, Gracia R. The effects of a treatment based on the use of virtual reality exposure and cognitive-behavioral therapy applied to patients with agoraphobia. Int J Clin Health Psychol. 2008;8(1):5–22. | ||
Muhlberger A, Herrmann MJ, Wiedemann G, Ellring H, Pauli P. Repeated exposure of flight phobics to flights in virtual reality. Behav Res Ther. 2001;39:1033–1050. | ||
Rothbaum BO, Hodges LF, Smith S, Lee JH, Price L. A controlled study of virtual reality exposure therapy for the fear of flying. J Consult Clin Psychol. 2000;6:1020–1026. | ||
Rothbaum BO, Hodges LF, Anderson PL, Price L, Smith S. Twelve-month follow-up of virtual reality and standard exposure therapy for the fear of flying. J Consult Clin Psychol. 2002;70:428–432. | ||
Millon T, Millon C, Davis R. Millon Clinical Multiaxial Inventory-III Manual. Minneapolis, MN: National Computer Systems; 1994. | ||
Zennaro A, Ferracuti S, Lang M, Sanavio E. Millon Clinical Multiaxial Inventory-III (MCMI-III Italian Adaptation). Florence: Giunti O.S; 2008. | ||
Van Gerwen LJ, Spinhoven P, Van Dyck R, Diekstra RFW. Construction and psychometric characteristics of two self-report questionnaires for the assessment of fear of flying. Psychol Assess. 1999;11:146–158. | ||
Triscari MT, Faraci P, D’Angelo V, Urso V. Paura di volare: struttura fattoriale di due questionari. [Fear of flying: factor analyses of two questionnaires]. Psicoterapia Cognitiva e Comportamentale. 2011;17(2):211–226. | ||
Faraci P, Triscari MT, D’Angelo V, Urso V. Fear of flying assessment: a contribution to the Italian validation of two self-report measures. Rev Psychol. 2011;18(2):91–100. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.