")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Effectiveness of Clozapine on Employment Outcomes in Treatment-Resistant Schizophrenia: A Retrospective Bidirectional Mirror-Image Study
Authors Matsuzaki H, Hatano M , Iwata M, Saito T, Yamada S
Received 29 December 2022
Accepted for publication 9 March 2023
Published 15 March 2023 Volume 2023:19 Pages 615—622
DOI https://doi.org/10.2147/NDT.S402945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Taro Kishi
Haruna Matsuzaki,1,* Masakazu Hatano,1,* Miko Iwata,1 Takeo Saito,2 Shigeki Yamada1
1Department of Clinical Pharmacy, Fujita Health University School of Medicine, Toyoake, 470-1192, Japan; 2Department of Psychiatry, Fujita Health University School of Medicine, Toyoake, 470-1192, Japan
*These authors contributed equally to this work
Correspondence: Masakazu Hatano, Department of Clinical Pharmacy, Fujita Health University School of Medicine, 1-98 Dengakugakubo, Kutsukake, Toyoake, Aichi, Japan, Tel +81 562932157, Fax +81 562934537, Email [email protected]
Purpose: Clozapine is more effective than other antipsychotics and is the only antipsychotic approved for treatment-resistant schizophrenia. The objective of this study is to reveal the effect of clozapine on employment using a bidirectional mirror-image model.
Patients and Methods: This design was a retrospective observational study that investigated the employment status of patients with treatment-resistant schizophrenia based on medical records. The bidirectional mirror-image model consisted of 1) switching from other antipsychotics to clozapine and 2) switching from clozapine to other antipsychotics. The observation period was 1 year for each pre- and post-clozapine initiation and discontinuation.
Results: We included 36 patients in the bidirectional mirror-image model. The regular employment plus employment support rate was significantly higher in the clozapine phase than in the other antipsychotic phase in the bidirectional mirror-image model (30.6% vs 11.1%, P = 0.039). The days of regular employment plus employment support were also significantly longer in the clozapine phase (61.3 ± 106.2 vs 24.7 ± 82.7 days, P = 0.032). As per the unidirectional mirror-image model, switching to clozapine resulted in significantly higher regular employment plus employment support rates in the clozapine phase than those in the other antipsychotic phase (33.3% vs 10.0%, P = 0.039). Switching from clozapine to other antipsychotics did not exhibit significant differences in any outcomes.
Conclusion: The results suggest that clozapine is superior to other antipsychotics with respect to achieving employment in patients with treatment-resistant schizophrenia. However, biases specific to the mirror-image model need to be considered.
Keywords: clozapine, antipsychotic agents, treatment-resistant schizophrenia, observational study, mental health recovery
Introduction
Schizophrenia is a chronic mental disorder affecting approximately 7 per 1000 people in their lifetime.1 The psychiatric symptoms of schizophrenia are broadly classified into positive symptoms (ie, delusions and hallucinations), negative symptoms (ie, lack of volition and flattening of affect), and cognitive impairment. Although the primary goal of schizophrenia treatment is clinical recovery to improve these psychiatric symptoms, social recovery in terms of employment, education, and independent living is also essential.2 In Australian studies, rehabilitation model of care focused on social functioning has achieved overall favorable results. However, clinical recovery does not necessarily lead to social recovery,3,4 and the employment rate for patients with schizophrenia is generally only 10–30%.5 Previous studies have shown that social recovery is difficult to achieve relative to clinical recovery, and this is recognized as an important clinical issue.6,7 Additionally, the mean unemployment costs of schizophrenia are estimated to be as high as $1.58 billion (USD) in Japan.8 These results indicate that the societal burden of schizophrenia is larger than that of other psychiatric disorders, such as depression or anxiety disorders, contrary to its lower prevalence rate.8
Antipsychotic drugs blocking dopamine D2 receptor are effective in treating schizophrenia. However, it has been reported that approximately 30% of patients with schizophrenia have treatment-resistant schizophrenia (TRS) that is poorly responsive to antipsychotic drugs.9 Clozapine is the only antipsychotic approved for TRS and is recommended as a first-line treatment for TRS in major practice guidelines.10–12 Clozapine has the largest effect size in improving overall psychiatric symptoms compared to that of other antipsychotics and is also superior in preventing relapse.13,14 Conversely, a meta-analysis has shown that antipsychotic drugs significantly improve social functioning in schizophrenia. However, this study did not include results for clozapine, and its effects are not clear.15 Furthermore, studies assessing employment rates for direct outcomes of social functioning are limited, and for clozapine, only a small observational study has been reported.16
The objective of this study was to reveal the effect of clozapine on employment using a bidirectional mirror-image model. The mirror-image study was designed to compare outcomes for the same length of period before and after switching treatment in the same patients. The patients themselves were set as controls and thus could better reflect the relative impact of the treatments in clinical practice.17
Materials and Methods
Study Design
This design was a retrospective observational study in a mirror-image model based on medical records at Fujita Health University Hospital. The study adopted a bidirectional mirror-image model as follows: 1) switching from other antipsychotics to clozapine and 2) switching from clozapine to other antipsychotics. The index date in switching from other antipsychotics to clozapine was the date of clozapine initiation, the pre-index period was the other antipsychotic phase for 1 year, and the post-index period was the clozapine phase for 1 year (Figure 1). The index date in switching from clozapine to other antipsychotics was the date of clozapine discontinuation, the pre-index period was the clozapine phase for 1 year, and the post-index period was the other antipsychotic phase for 1 year (Figure 1). If clozapine was initiated or discontinued during hospitalization, then the hospitalization period was excluded, and the pre- or post-index period was defined as before admission or after discharge, respectively. This study focused on whether or not clozapine was used, and the period involving the use of a combination of clozapine and other antipsychotics was included as the clozapine phase of the analysis. If patients who continued treatment with other antipsychotics for more than one year switched to clozapine and then returned to other antipsychotics more than one year later, they were included in both mirror image models for analysis.
 |
Figure 1 Bidirectional mirror-image model. |
We obtained data on patient characteristics (age, sex, height, weight, body mass index, duration of illness, history of modified electroconvulsive therapy, and medication history) at the time of clozapine initiation or discontinuation and the employment status during the observation period from the medical records. The medications included antipsychotics, benzodiazepines, and antiparkinsonian agents, and the total dose of each was calculated by converting to chlorpromazine equivalents, diazepam equivalents, and biperiden equivalents.18 Employment status was evaluated separately for regular employment (including attending school) and employment support (eg, transition support for employment and support for continuous employment). Short-term employment of 4 weeks or less was not counted.
Study procedures were performed in accordance with the principles of the Declaration of Helsinki, and this study was approved by the Institutional Review Board of Fujita Health University (HM21-514). No informed consent was required since this was an observational study conducted using medical records, although patients had the right to revoke their consent and opt out of the study.
Patients
Inclusion criteria for patients were as follows: 1) patients who met the diagnostic criteria for schizophrenia in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; 2) patients who met criteria for TRS according to the Clozaril Patient Monitoring Service in Japan (“failure to respond to at least two antipsychotics for a sufficient period” or “when the dose cannot be sufficiently increased due to extrapyramidal symptom with monotherapy of two or more atypical antipsychotics”);19 3) patients who were initiated on or discontinued from clozapine treatment between October 2010 and June 2021; and 4) patients who continued clozapine and other antipsychotics for at least 1 year each. Patients who could not be followed for a 1-year pre- or post-index period and those over the age of 65 (age limit for employment support in Japan) were excluded.
Assessment
The primary endpoints were the employment rate (ie, the rate of patients who achieved employment excluding short-term employment periods of 4 weeks or less) in the clozapine phase and the other antipsychotic phase, evaluated using bidirectional and unidirectional mirror-image models. Employment was defined as the composite outcome of regular employment and employment support, and the regular employment and employment support rates were also calculated separately.
The secondary endpoints were the number of employment days in the clozapine phase and the other antipsychotic phase, evaluated using bidirectional and each unidirectional mirror-image models. As with the employment rate, the number of employment days was categorized into regular employment and employment support and was further calculated as a composite outcome of these two categories.
Statistical Analysis
Employment rates in the clozapine and other antipsychotic phases were compared using a binomial test. The number of employment days in the clozapine and other antipsychotic phases is compared using the paired t-test. P-values were two-sided, and statistical significance was set at those less than 0.05. The sample size was determined from the number of subjects enrolled within the study period. All statistical analyses were performed using R 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
Thirty-two patients initiated clozapine treatment during the observation period, and six patients discontinued. Of these, one patient who could not be followed up for a 1-year pre- or post-index period and one patient over the age of 65 were excluded. A total of 36 patients were included in the bidirectional mirror-image model. Thirty patients switched from other antipsychotics to clozapine, and six patients switched from clozapine to other antipsychotics (three patients were included in both unidirectional mirror-image models). The patient characteristics at the index date are summarized in Table 1. About half of the patients had a duration of illness of more than 10 years. The average antipsychotic dose at clozapine initiation was as high as 987.0 ± 413.2 mg (chlorpromazine equivalent). Olanzapine was the most common antipsychotic used at clozapine initiation (11 cases, 36.7%).
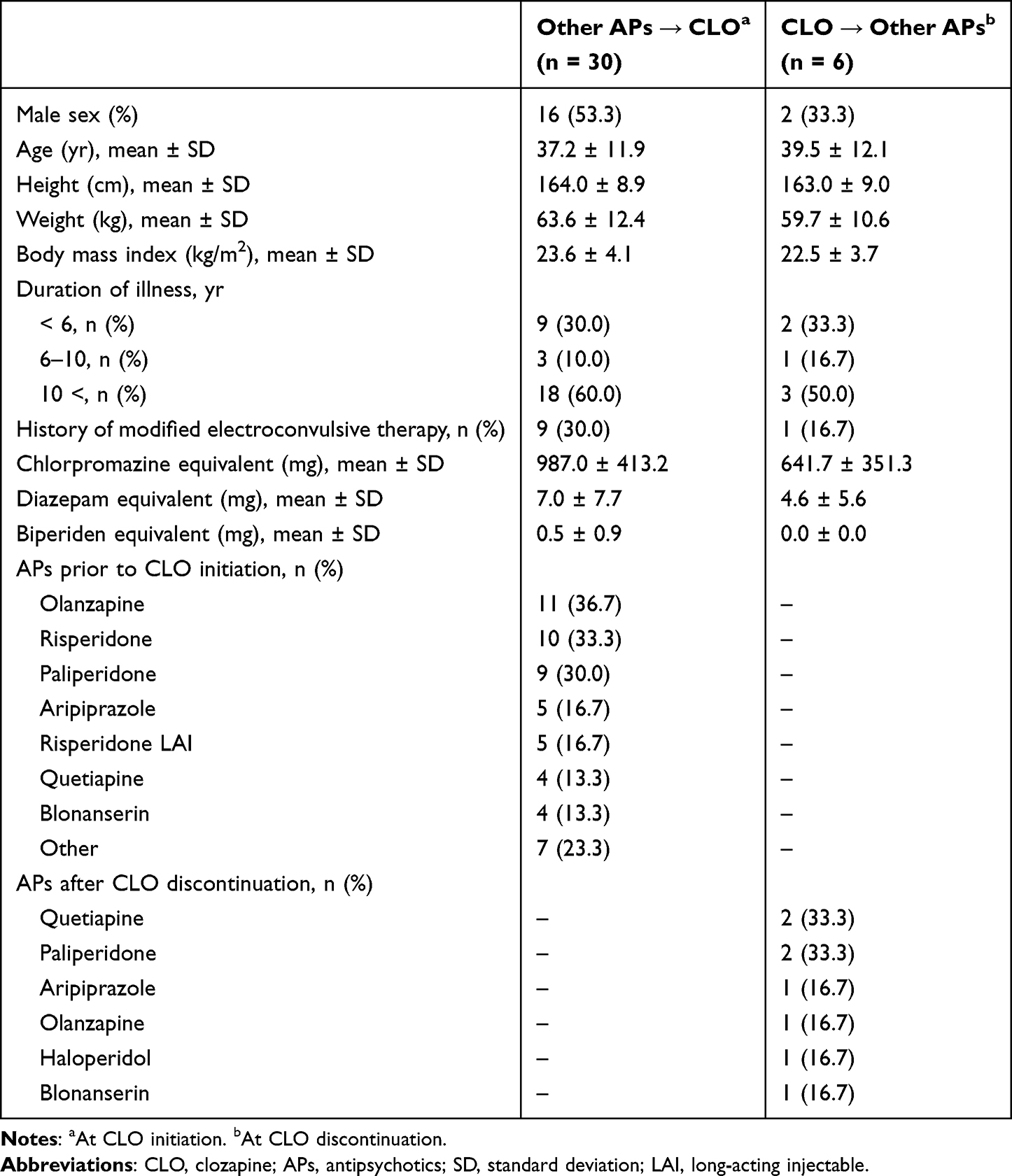 |
Table 1 Patient Characteristics |
Employment Rates
The employment rates in the clozapine and other antipsychotic phases are summarized in Table 2. In the bidirectional mirror-image model, the regular employment plus employment support rate was significantly higher in the clozapine phase than in the other antipsychotic phase (30.6% vs 11.1%, P = 0.039). The rates for each of regular employment and employment support were higher for the clozapine phase but were not significantly different from each other (22.2% vs 11.1%, P = 0.22; and 8.3% vs 0.0%, P = 0.25; respectively).
 |
Table 2 Employment Rates |
Based on the unidirectional mirror-image model, switching to clozapine resulted in significantly higher regular employment plus employment support rates in the clozapine phase than those in the other antipsychotic phase (33.3% vs 10.0%, P = 0.039). In switching from clozapine to other antipsychotics, there was no significant difference in the employment rates between the clozapine and other antipsychotic phases.
Employment Days
The number of employment days in the clozapine and other antipsychotic phases is summarized in Table 3. In the bidirectional mirror-image model, patients in the clozapine phase had a significantly higher number of regular employment plus employment support days than those in the other antipsychotic phase (61.3 ± 106.2 vs 24.7 ± 82.7 days, P = 0.032). There was no significant difference in the number of regular employment and employment support days, respectively. In the unidirectional mirror-image model, there were no significant differences in the number of employment days between the clozapine phase and the other antipsychotic phase for both switching to and from clozapine.
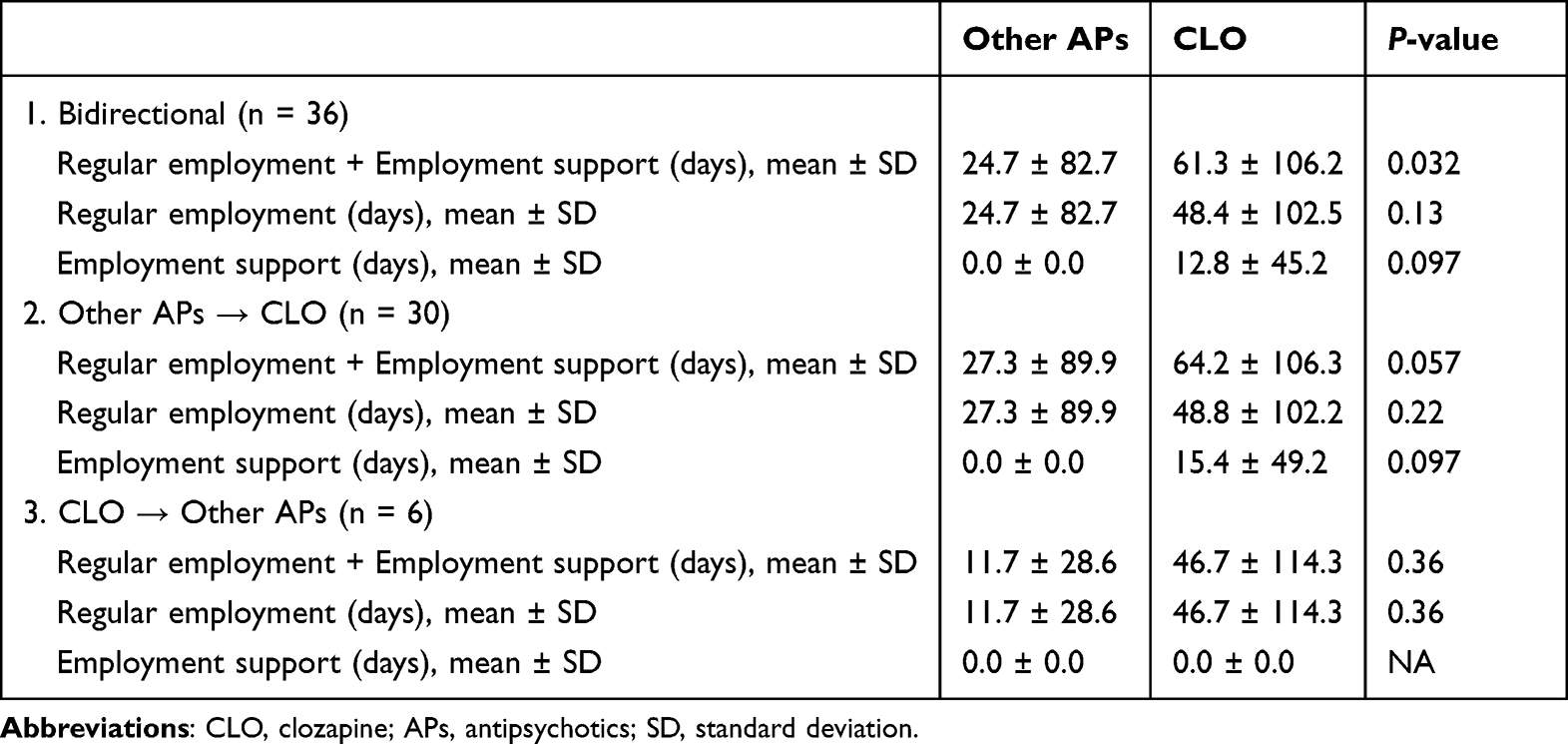 |
Table 3 Employment Days |
Discussion
This study evaluated the effect of clozapine on employment using a mirror-image model based on real-world data. Clozapine was significantly superior to other antipsychotics in terms of the rate and duration of employment (regular employment plus employment support) in the observation period. The employment rate for treatment with non-clozapine antipsychotics in this study was 11%, which was lower than the employment rate for patients with schizophrenia in Japan (4–31%).8 This may be because the study population had TRS, and hence, clozapine is applicable for its treatment. Clozapine treatment increased employment rates in this population with TRS to the same level as in patients with general schizophrenia; this finding provides important evidence of social recovery.
There is limited evidence on the effect of antipsychotic treatment on employment status. The Cochrane Database of Systematic Reviews has evaluated the number of patients subjected to antipsychotic treatment having employment. However, only three randomized controlled trials have been included, and the results have not been significantly different from those of the placebo.20 For clozapine, no randomized controlled trials measuring employment status or social functioning have been reported, and only a few observational studies have been reported. Kaneda et al reported improved employment rates in schizophrenic patients after 12 months of clozapine initiation.16 Two other studies reported a trend toward higher rates of regular occupational activity with an increasing duration of clozapine treatment,21 as well as improved occupational functioning score.22 Although this study is similarly a small observational study, our findings support previously reported results through a different study design using a mirror-image model.
Clozapine is more effective than other antipsychotics in improving psychiatric symptoms and preventing hospitalization,13,14 and it is reasonable to assume that this contributed to the successful employment of the patients. However, the influence of possible poor medication adherence can affect the interpretation of real-world data. One study using the Medication Event Monitoring System showed that patients receiving clozapine had better medication adherence rates than those receiving other antipsychotic medications.23 Although adherence was not directly measured in our study, it may be considered that the patients were available for employment since they maintained medication adherence.
With respect to the pharmacological profile, clozapine has a high affinity for dopamine (D1, D2, and D4), serotonin (5-HT2A, 5-HT2C, 5-HT6, and 5-HT7), histamine (H1), and α-adrenergic (α1, α2) receptors.24,25 In particular, the serotonin receptors 5-HT6 and 5-HT7 have been suggested to be associated with cognitive function, and affinity of clozapine to these receptors may result in a favorable effect on employment status.26 A study among patients with schizophrenia found no effect of either clozapine or total anticholinergic burden on cognitive performance,27 despite 2021 meta-analysis by Baldez et al, which ranked clozapine low among other APs.28 This uncertainty in the evidence regarding the effects of clozapine on cognition puts the findings of this study in an even more interesting light. In addition, the authors of that meta-analysis pointed out that all the clozapine studies included patients with TRS, which may have underestimated the effect of clozapine on cognitive function. The lack of efficacy of non-clozapine antipsychotics may have resulted in the superiority of clozapine since our study included only TRS. Future statistical comparisons with non-TRS results should be interpreted with caution.
This study has potential limitations. Since mirror-image models generally compare pre- and post-treatment switching, it is necessary to consider the influence that expectations of the new treatment can have on the effectiveness (ie, expectation bias).17 We therefore adopted a bidirectional mirror-image model; however, only a few patients switched from treatment with clozapine. Thus, this problem could not be sufficiently solved, and furthermore, the resulting sample sizes differed greatly in each mirror image model, which may have skewed the statistical analyses. These two mirror-image models may reflect different phases of disease progression, which may explain the relatively poorer employment outcomes among those switching from clozapine than among those switching to clozapine, irrespective of antipsychotic treatment. In other words, a patient switching from clozapine to another antipsychotic may do so because of clozapine-resistant schizophrenia, intolerable side-effects of clozapine, or difficulty in maintaining regular hematological monitoring. However, patients who are switched from other antipsychotics to clozapine are likely to be freshly identified as those with TRS. Although our study did not assess treatment responsiveness to antipsychotics, we cannot rule out the possibility that these differences in the background of each mirror-image model exerted different effects on psychiatric symptoms. In addition, it should be noted that the treatment response rate to TRS for clozapine is only 40%.29 Other disadvantages of the mirror-image model include the absence of an active control group and time-dependent effects (eg, changes in healthcare policy), which are difficult to ignore.30 Furthermore, it is possible that false negatives were obtained (especially for the switch from clozapine) due to the small sample size of the study. Finally, this was a retrospective observational study conducted at a single center, making it difficult to generalize the results due to various confounding factors.
Conclusion
In conclusion, to the best of our knowledge, this is the first study to use a bidirectional mirror-image model to reveal the effects of clozapine on employment status. Although various biases must be considered, clozapine was shown to improve employment status when compared with other antipsychotics, indicating that treatment with clozapine may contribute to social recovery. Future validation studies should be conducted using larger sample sizes and multicenter data to reduce the influence of confounding factors. Moreover, it would be important to conduct a long-term evaluation in terms of continuity of employment.
Acknowledgments
We would like to thank Mr Takahito Goto and Ms Mayumi Tomoyose, Psychiatric social workers (Fujita Health University Hospital), for their cooperation in data collection.
We would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by TAIHO PHARMACEUTICAL for English editing and publication of the article through a scholarship donation. This study also received funding from TAIHO PHARMACEUTICAL through a scholarship donation. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Disclosure
All authors declare no competing interests in this work.
References
1. McGrath J, Saha S, Chant D, et al. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30(1):67–76. doi:10.1093/epirev/mxn001
2. Lloyd C, Waghorn G, Williams PL. Conceptualising recovery in mental health rehabilitation. Br J Occupat Ther. 2008;71(8):321–328. doi:10.1177/030802260807100804
3. Parker S, Arnautovska U, Siskind D, et al. Community-care unit model of residential mental health rehabilitation services in Queensland, Australia: predicting outcomes of consumers 1-year post discharge. Epidemiol Psychiatr Sci. 2020;29:e109. doi:10.1017/S2045796020000207
4. Parker S, Arnautovska U, Korman N, et al. Comparative effectiveness of integrated peer support and clinical staffing models for community-based residential mental health rehabilitation: a prospective observational study. Community Ment Health J. 2022. doi:10.1007/s10597-022-01054-1
5. Marwaha S, Johnson S, Bebbington P, et al. Rates and correlates of employment in people with schizophrenia in the UK, France and Germany. Br J Psychiatry. 2007;191:30–37. doi:10.1192/bjp.bp.105.020982
6. Lambert M, Schimmelmann BG, Naber D, et al. Prediction of remission as a combination of symptomatic and functional remission and adequate subjective well-being in 2960 patients with schizophrenia. J Clin Psychiatry. 2006;67(11):1690–1697. doi:10.4088/JCP.v67n1104
7. Revier CJ, Reininghaus U, Dutta R, et al. Ten-year outcomes of first-episode psychoses in the MRC AESOP-10 study. J Nerv Ment Dis. 2015;203(5):379–386. doi:10.1097/NMD.0000000000000295
8. Sado M, Inagaki A, Koreki A, et al. The cost of schizophrenia in Japan. Neuropsychiatr Dis Treat. 2013;9:787–798. doi:10.2147/NDT.S41632
9. Conley RR, Kelly DL. Management of treatment resistance in schizophrenia. Biol Psychiatry. 2001;50(11):898–911. doi:10.1016/S0006-3223(01)01271-9
10. Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Aust N Z J Psychiatry. 2016;50(5):410–472. doi:10.1177/0004867416641195
11. Barnes TR, Drake R, Paton C, et al. Evidence-based guidelines for the pharmacological treatment of schizophrenia: updated recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2020;34(1):3–78. doi:10.1177/0269881119889296
12. Japanese Society of N. Japanese society of neuropsychopharmacology: “Guideline for pharmacological therapy of schizophrenia”. Neuropsychopharmacol Rep. 2021;41(3):266–324. doi:10.1002/npr2.12193
13. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29 823 patients with schizophrenia. JAMA Psychiatry. 2017;74(7):686–693. doi:10.1001/jamapsychiatry.2017.1322
14. Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939–951. doi:10.1016/S0140-6736(19)31135-3
15. Leucht S, Leucht C, Huhn M, et al. Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia: systematic review, bayesian meta-analysis, and meta-regression of efficacy predictors. Am J Psychiatry. 2017;174(10):927–942. doi:10.1176/appi.ajp.2017.16121358
16. Kaneda Y, Jayathilak K, Meltzer H. Determinants of work outcome in neuroleptic-resistant schizophrenia and schizoaffective disorder: cognitive impairment and clozapine treatment. Psychiatry Res. 2010;178(1):57–62. doi:10.1016/j.psychres.2009.04.001
17. Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74(10):957–965. doi:10.4088/JCP.13r08440
18. Inada T, Inagaki A. Psychotropic dose equivalence in Japan. Psychiatry Clin Neurosci. 2015;69(8):440–447. doi:10.1111/pcn.12275
19. Clozaril® (clozapine) [package insert]. Tokyo: Novartis Pharma K.K.; 2021.
20. Ceraso A, Lin JJ, Schneider-Thoma J, et al. Maintenance treatment with antipsychotic drugs for schizophrenia. Cochrane Database Syst Rev. 2020;8(8):CD008016. doi:10.1002/14651858.CD008016.pub3
21. Wheeler A, Humberstone V, Robinson G. Outcomes for schizophrenia patients with clozapine treatment: how good does it get? J Psychopharmacol. 2009;23(8):957–965. doi:10.1177/0269881108093588
22. Grover S, Naskar C, Chakrabarti S. Impact of clozapine on disability and course of illness in patients with schizophrenia: a study from North India. Indian J Psychiatry. 2021;63(6):588–592. doi:10.4103/psychiatry.IndianJPsychiatry_244_20
23. Takeuchi H, Borlido C, Sanches M, et al. Adherence to clozapine vs. other antipsychotics in schizophrenia. Acta Psychiatr Scand. 2020;142(2):87–95. doi:10.1111/acps.13208
24. Bymaster FP, Calligaro DO, Falcone JF, et al. Radioreceptor binding profile of the atypical antipsychotic olanzapine. Neuropsychopharmacology. 1996;14(2):87–96. doi:10.1016/0893-133X(94)00129-N
25. Arnt J, Skarsfeldt T. Do novel antipsychotics have similar pharmacological characteristics? A review of the evidence. Neuropsychopharmacology. 1998;18(2):63–101. doi:10.1016/S0893-133X(97)00112-7
26. Meltzer HY, Massey BW, Horiguchi M. Serotonin receptors as targets for drugs useful to treat psychosis and cognitive impairment in schizophrenia. Curr Pharm Biotechnol. 2012;13(8):1572–1586. doi:10.2174/138920112800784880
27. Arnautovska U, Neill E, Rossell SL, et al. Does the clozapine/norclozapine ratio predict cognitive performance in patients with clozapine-resistant schizophrenia? Aust N Z J Psychiatry. 2022;56(7):875–878. doi:10.1177/00048674211062828
28. Baldez DP, Biazus TB, Rabelo-da-ponte FD, et al. The effect of antipsychotics on the cognitive performance of individuals with psychotic disorders: network meta-analyses of randomized controlled trials. Neurosci Biobehav Rev. 2021;126:265–275. doi:10.1016/j.neubiorev.2021.03.028
29. Siskind D, Siskind V, Kisely S. Clozapine response rates among people with treatment-resistant schizophrenia: data from a systematic review and meta-analysis. Can J Psychiatry. 2017;62(11):772–777. doi:10.1177/0706743717718167
30. Miura G, Misawa F, Kawade Y, Fujii Y, Mimura M, Kishimoto T. Long-acting injectables versus oral antipsychotics: a retrospective bidirectional mirror-image study. J Clin Psychopharmacol. 2019;39(5):441–445. doi:10.1097/JCP.0000000000001082
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.