Back to Journals » Advances in Medical Education and Practice » Volume 16
Effectiveness of Case-Based Narrative Medicine Education in the Standardized Training of Obstetric Residents
Authors Du L, Zheng R, Zhu X, Jia J, Yang Z
Received 6 May 2025
Accepted for publication 2 August 2025
Published 22 August 2025 Volume 2025:16 Pages 1511—1520
DOI https://doi.org/10.2147/AMEP.S538754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Lijia Du,1 Rui Zheng,1 Xiaoxiong Zhu,1 Junjun Jia,2 Zhifen Yang1
1Obstetrical Department, The Fourth Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Hepatobiliary Pancreatic Surgery, The First Affiliated Hospital of ZheJiang Province, Hangzhou,People’s Republic of China
Correspondence: Zhifen Yang, Obstetrical Department, The Fourth Hospital of Hebei Medical University, 169 Tianshan Street, Shijiazhuang, 050000, People’s Republic of China, Tel +8615100111990, Email [email protected]
Purpose: As the demand for humanistic and patient-centered care grows in clinical practice, integrating narrative medicine into residency training has become increasingly important. This study aimed to investigate the narrative competencies of obstetric residents undergoing standardized training and to evaluate the effectiveness of narrative medicine education empowered by case-based teaching in enhancing clinical practice and professional competency.
Patients and Methods: A total of 46 obstetric residents enrolled in standardized training programs between October 2021 and May 2024 were randomly assigned to either the experimental group (n = 23) or the control group (n = 23). Residents in the experimental group received case-based narrative medicine education, while those in the control group received conventional clinical teaching. Following the obstetrics rotation, knowledge tests and objective structured clinical examinations (OSCEs) were administered. Subjective evaluations of narrative competencies and teaching effectiveness were assessed using validated questionnaires.
Results: After the obstetrics rotation, OSCE scores were significantly higher in the experimental group compared to the control group (P < 0.05). Narrative competencies also showed a significant improvement among residents in the experimental group after the training (P < 0.05). Moreover, residents in the experimental group reported higher narrative competency scores and greater satisfaction with teaching effectiveness compared to the control group (P < 0.05).
Conclusion: Narrative medicine education empowered by case-based teaching effectively enhances narrative competencies, obstetric clinical skills, doctor-patient communication abilities, critical thinking, and learning engagement among obstetric residents undergoing standardized training. This innovative teaching approach addresses the gap in humanistic medical education and provides an effective strategy for cultivating comprehensive professional competency in obstetric residents.
Keywords: narrative competencies, case-based learning in obstetrics, obstetrics training, residency education, medical humanities in clinical education
Introduction
Medical education is a lifelong process encompassing institutional education, postgraduate training, and continuing education.1 Among these stages, standardized residency training is particularly critical – it not only shapes clinical competency but also lays the foundation for professional identity. In Obstetrics and Gynecology, where clinical decision-making and patient interaction are often high specialized and emotionally charged, the demands on both technical proficiency and humanistic care are uniquely high. However, current residency training in obstetrics is often constrained by short rotation periods and traditional teacher-centered instructional models. These often leads to insufficient training in both clinical skills and humanistic care. Obstetric patients experience profound physiological and psychological changes during pregnancy and childbirth, making communication skills and empathetic care critically important for obstetricians.2,3 Yet, Studies have shown that while residents may become proficient in procedural skills, they often struggle with narrative competence and patient-centered communication.4,5
Narrative medicine is an important supporting discipline linking the transition from the evidence-based medicine to precision medicine. It paves the way to enhance medical service quality and cultivate medical humanities.6,7 Narrative medicine, first conceptualized by Rita Charon in 2001, offers a potential solution.8 By incorporating practices such as close reading, reflective writing, and storytelling into clinical education, narrative medicine helps trainees better understand patient experiences, strengthen empathy, and reflect on their own clinical behaviors.9 Globally, narrative competence is now seen as a core attribute of modern physicians, enabling more humane, precise, and ethically grounded care.10–12 However, systematic narrative medicine training programs remain limited in China.13
Case-based teaching, a learner-centered strategy, integrates theoretical knowledge with clinical application through real-world scenarios.14–17 It encourages students to actively engage in problem-solving while developing critical thinking and empathy. Combining case-based teaching with narrative medicine offers a promising approach to address the deficiencies of traditional obstetric education.
Therefore, this study aimed to evaluate the effectiveness of narrative medicine education empowered by case-based teaching in enhancing narrative competencies, clinical skills, doctor-patient communication, and critical thinking among obstetric residents undergoing standardized training. We hypothesized that this integrated model would improve both professional competencies and humanistic literacy compared to conventional clinical teaching.
Methods
Subjects
Physicians participating in the standardized residency training program in the department of Obstetrics and Gynecology at the Fourth Hospital of Hebei Medical University between October 2021 and May 2024 were enrolled in the present study. All participants underwent obstetrics rotations lasting at least three months per academic year. Written informed consent was obtained from all participants.
Study Design
Eligible participants were licensed physicians who actively cooperated with the survey and successfully passed both the knowledge test and the objective structured clinical examination (OSCE) after the obstetrics rotation. Participants who failed the National Medical Licensing Examination, failed the knowledge test or OSCE, or did not complete the full rotation or the questionnaires were excluded.
From January 1, 2024, a total of 46 residents were randomly assigned to either the experimental group (n=23) or the control group (n=23) using a random number table method. The two groups underwent parallel, non-overlapping teaching interventions to minimize the risk of information cross-contamination. Participants were trained and evaluated separately, and they were explicitly instructed not to share teaching content between groups. Importantly, both groups received the same total amount of instructional time, including daily clinical training and two-hour weekly offline sessions; only the teaching approach differed between groups. Assessments included knowledge tests, OSCEs, evaluations of teaching satisfaction, and the Narrative Competencies Scale for Medical Practitioners,18 conducted both before and after the obstetrics rotation.
A detailed overview of the participant enrollment, group allocation, intervention, assessments, and data analysis is shown in Figure 1.
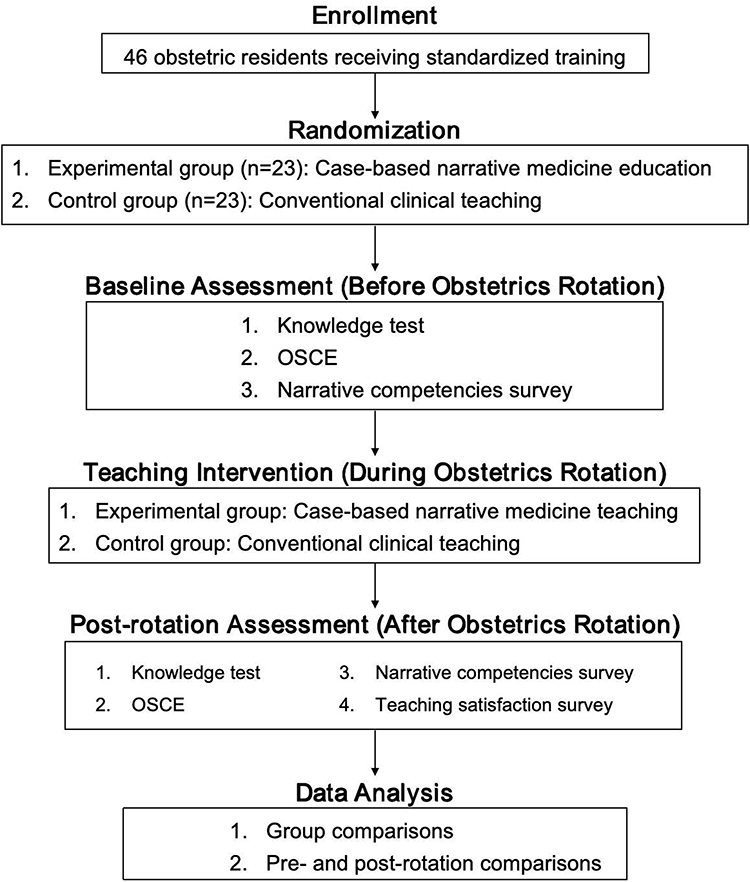 |
Figure 1 Overall Study Flowchart. This flowchart illustrates participant enrollment, randomization, intervention allocation, baseline and post-rotation assessments, and data analysis. |
Interventions
Conventional Clinical Teaching (Control Group)
Participants in the control group received conventional clinical teaching, which included daily theoretical instruction, clinical skills training, and a two-hour weekly offline session consisting of lectures, skill practices, teaching rounds, and medical record discussions.
Case-Based Teaching of Narrative Medicine (Experimental Group)
Participants in the experimental group received case-based teaching of narrative medicine with the same schedule and time allocation as the control group, including routine daily training and.two-hour weekly offline sessions. In this group, the offline sessions integrated narrative medicine education into clinical case-based discussions, emphasizing clinical reasoning, decision-making, and doctor-patient communication skills.
The intervention consisted of three phases:
Before-class: Online lectures on the conceptual framework of narrative medicine, along with intensive reading and reflective writing exercises based on recommended literary works (eg, A Doctor’s Stories, The Real Doctor Will See You Shortly, A Way of Life).
During class: Presentation of slightly modified classic obstetric cases from the hospital’s medical record system, categorized into two types: ① cases focusing on clinical management skills, and ② cases focusing on doctor-patient communication and humanistic care. Teaching strategies included guided discussion, group analysis, paper-based materials, video resources, and simulated patients (SPs).
After class: Group-based replay and discussion of clinical scenarios, supplemented with additional reference materials to promote independent learning and clinical reasoning.
Outcome Assessments
Academic Performances
Academic performances were evaluated using: ①A knowledge test covering physiological and pathological obstetrics (100-point scale). ②An OSCE assessing history taking, physical examination, diagnostic abilities, clinical decision-making, doctor-patient relationship handling, and professional attitude.
Narrative Competencies
Narrative competencies were assessed using the Narrative Competencies Scale for Medical Practitioners developed and validated by Yang et al (2023),18 including: ① Narrative Cognitive Competency Subscale (23 items, assessing basic narrative cognition). ② Narrative Behavior Competency Subscale (38 items, assessing behavioral expression of narrative competencies). Each item was rated on a four-point scale: completely disagree, slightly agree, strongly agree, and completely agree.
Teaching Satisfaction
Teaching satisfaction was measured through a five-item questionnaire evaluating improvements in active learning interest, clinical thinking, medical skills, doctor-patient communication skills, and satisfaction with teaching methods (binary response: applicable (I/A) or not applicable (N/A).
Statistical Analysis
Data were analyzed using SPSS 26.0 software. Continuous variables were expressed as mean ± standard deviation (SD) and compared using independent-sample t-tests. Categorical variables were compared using Chi-square tests or Fisher’s exact tests as appropriate. A P-value of < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 46 eligible obstetric residents were enrolled in this study. No significant differences were observed in baseline characteristics between the experimental group and the control group (P > 0.05; Tables 1 and 2).
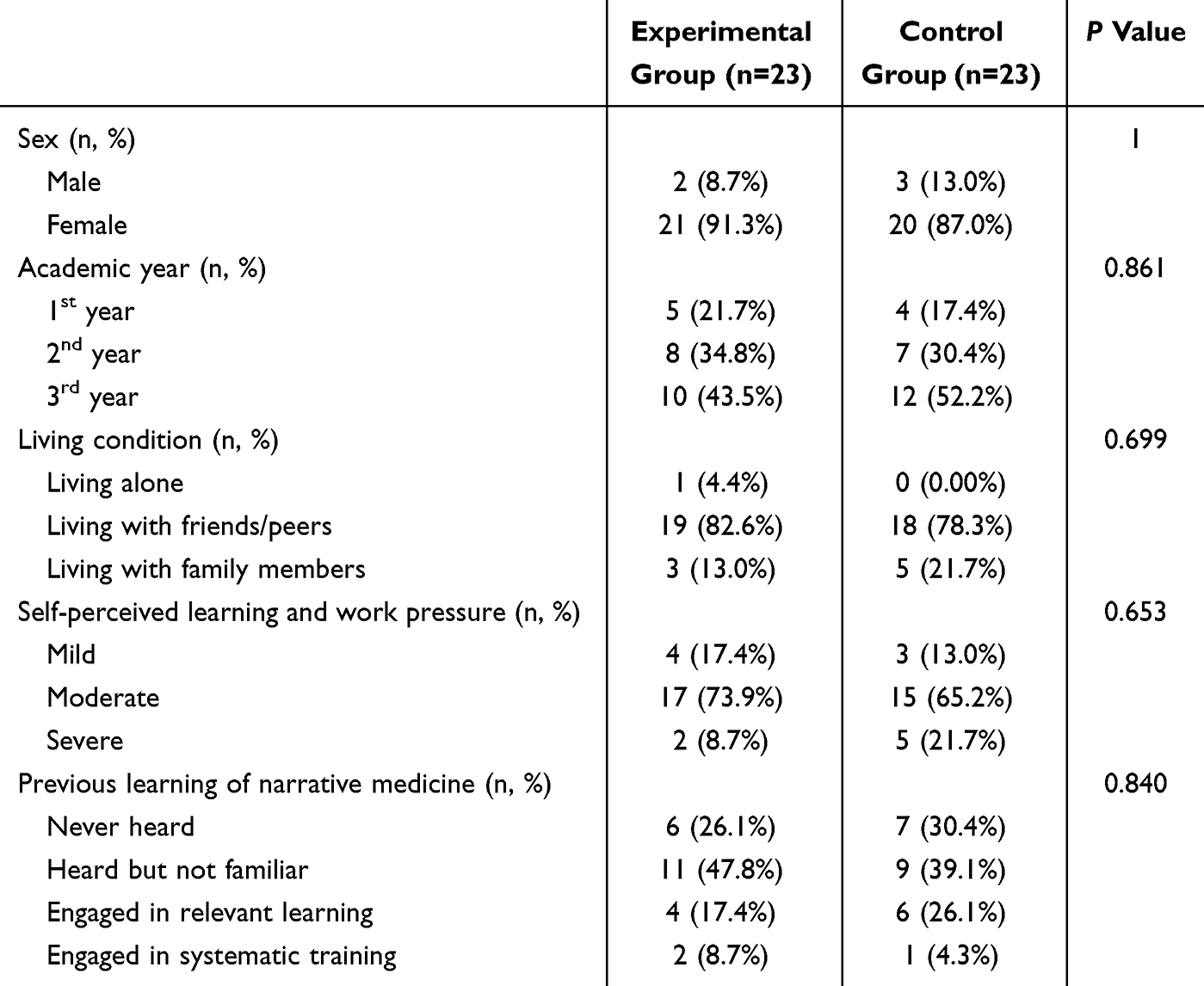 |
Table 1 Baseline Characteristics |
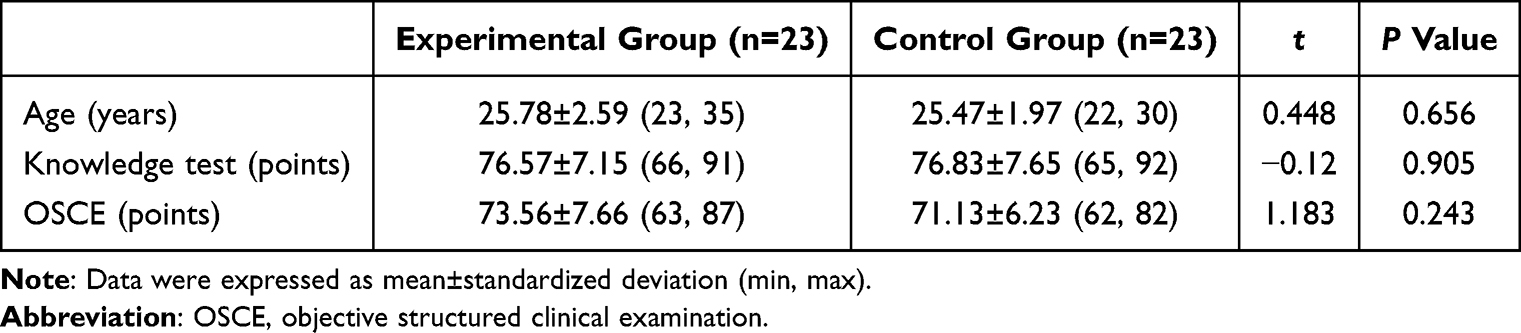 |
Table 2 Academic Performances Before Rotation |
Knowledge Test and OSCE Scores After Obstetric Rotation
Following the obstetrics rotation, knowledge test scores were comparable between the two groups (P > 0.05). However, OSCE scores were significantly higher in the experimental group compared to the control group (P < 0.05; Table 3).
 |
Table 3 Academic Performances After Rotation |
Questionnaire Survey
A questionnaire survey was conducted both at the beginning and after completion of the obstetrics rotation using the Sojump online platform. All 46 residents completed the questionnaires, yielding a response rate of 100%.
Narrative Competencies
At baseline, there were no significant differences between the two groups in the scores of the Narrative Cognitive Competency Subscale and the Narrative Behavior Competency Subscale (P > 0.05; Table 4). After the rotation, significant improvements were observed in the experimental group in the competencies of narrative cognition of wellness, professional narrative thinking, narrative behavior of career construction, narrative behavior of peer communications, and narrative behavior of doctor-patient communication (all P < 0.05). The competencies of narrative behavior of wellness and family connection did not show significant changes (P > 0.05; Table 5). In contrast, no significant improvements in narrative cognitive or behavior competencies were detected in the control group following the conventional teaching intervention (P > 0.05; Table 6). Moreover, post-rotation comparisons revealed that the experimental group exhibited significantly higher competencies in narrative cognition of wellness, professional narrative thinking, narrative behavior of career construction, narrative behavior of peer communications, and narrative behavior of doctor-patient communication compared to the control group (P < 0.05). Competencies related to narrative behavior of wellness and family connection remained comparable between groups (P > 0.05; Table 7).
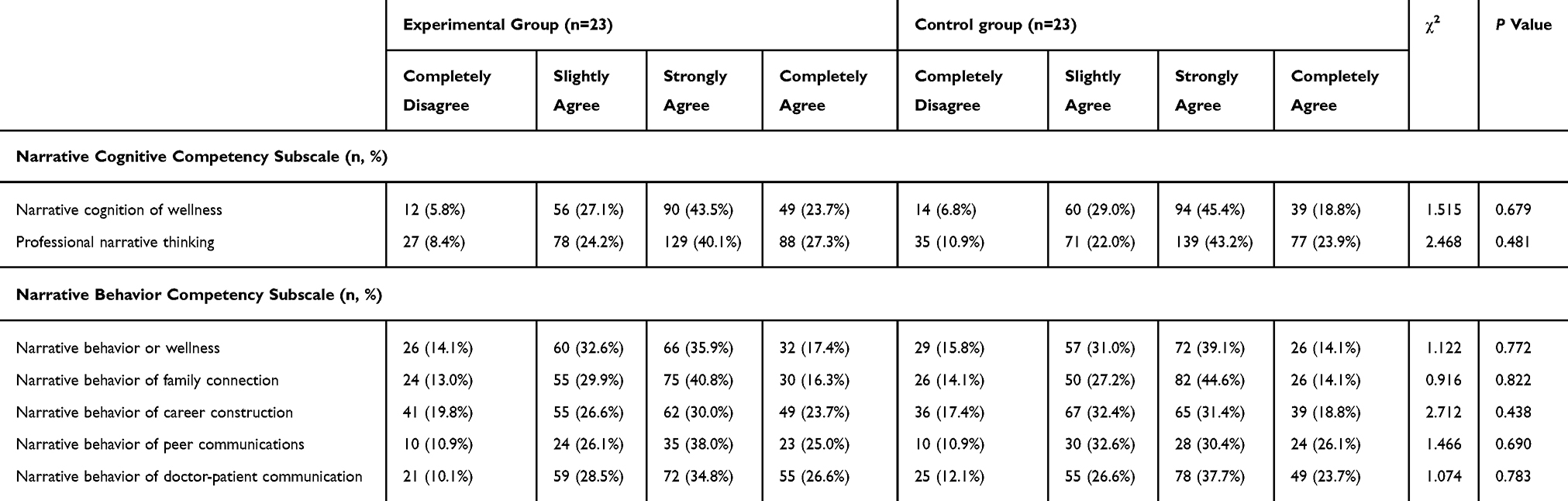 |
Table 4 Narrative Competencies Before Rotation |
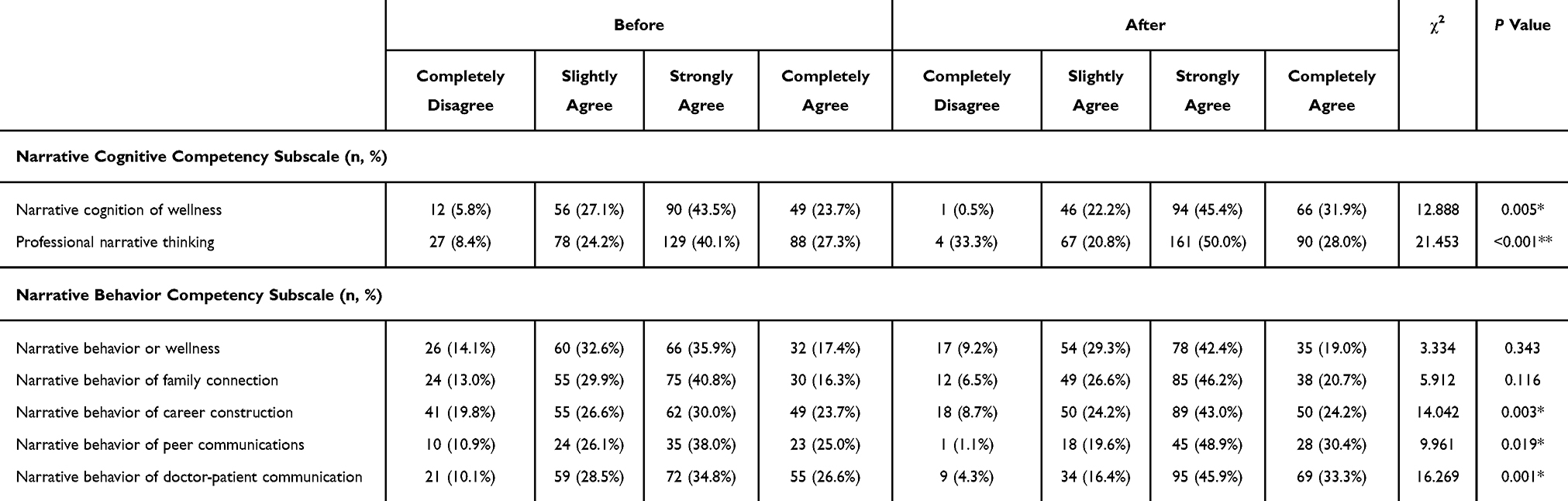 |
Table 5 Changes in Narrative Competencies Before and After Rotation (Experimental Group) |
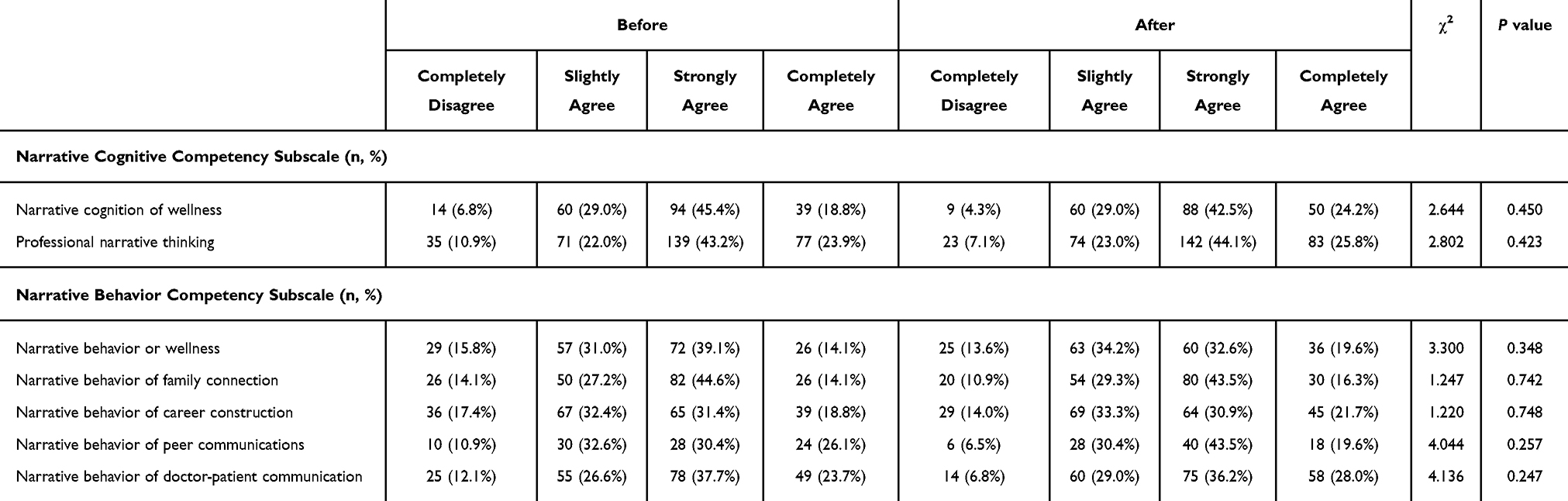 |
Table 6 Changes in Narrative Competencies Before and After Rotation (Control Group) |
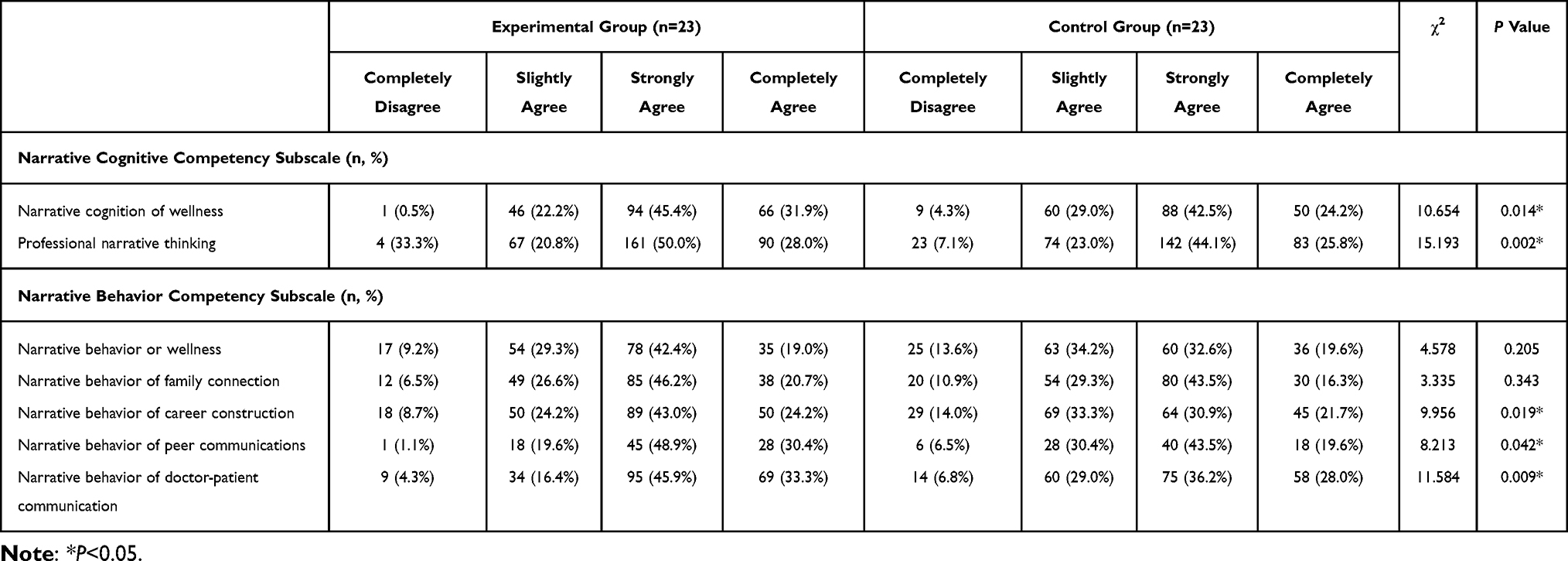 |
Table 7 Comparison of Narrative Competencies Between Groups After Rotation |
Teaching Satisfaction
Teaching satisfaction, including improvement in interest in active learning, clinical thinking ability, medical skills, doctor-patient communication skills, and teaching methods, was significantly higher in the experimental group compared to the control group (all P < 0.05; Table 8).
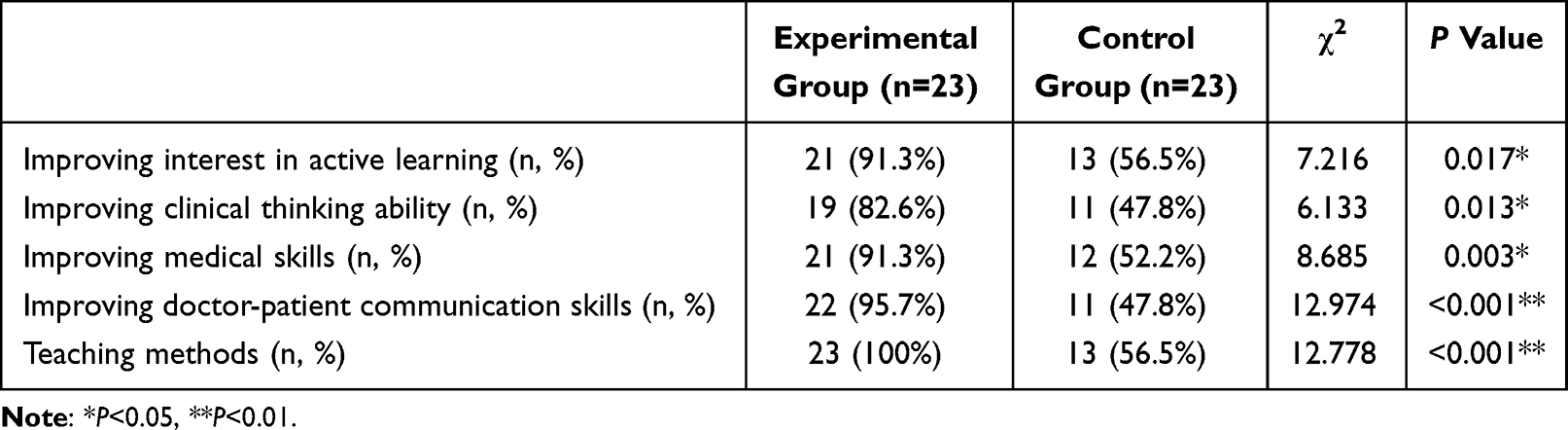 |
Table 8 Comparison of Teaching Satisfaction Between Groups (n=46) |
Discussion
Current Teaching Status of Standardized Residency Training in the Obstetrics Department
Pregnancy is often associated with critical conditions that are severe and constantly changing. Without timely and effective intervention, the safety of both mother and fetus is at risk. With the implementation of the two-child and three-child policies in China, pregnancy-related complications such as multiparity, advanced maternal age, uterine scarring, and placenta accreta have become increasingly common. The heavy workload resulting from routine clinical tasks often contributes to emotional stress among medical staff, manifested as irritability, impatience, and a decline in the delivery of humanistic care. Meanwhile, increasing patient awareness of privacy has led to frequent refusals of participation in clinical teaching sessions by pregnant women in obstetrical departments. Case-based teaching is a well-recognized approach that encourages students to independently address real-world scenarios, stimulating learning interest, enthusiasm, autonomy, critical thinking, and creativity.19
While pregnancy and childbirth bring immense joy, they are also accompanied by considerable physical and psychological burdens, including labor pain, postpartum challenges, breastfeeding, and family planning concerns. Emotional sensitivity is heightened during pregnancy, with increased incidences of anxiety, fear, and depression, particularly in cases complicated by pregnancy-associated disorders. Stressful life events during pregnancy or the postpartum period are well-established risk factors for perinatal depression, which can adversely affect both maternal and neonatal outcomes.20 The Healthy China Action Plan (2019–2030) emphasizes the importance of training talents in obstetrics and midwifery, strengthening humanistic care, and promoting maternal and child health. Thus, there is an urgent need to accelerate the incorporation of medical humanities into standardized residency training, particularly within obstetrics. A domestic survey of 130 medical students from Xiangya School of Medicine, Central South University, found that 61.5% of respondents believed that narrative medicine significantly benefits clinical practice.21 Consequently, integrating case-based teaching with narrative medicine education holds great promise for strengthening the humanistic aspects of current training programs.
Effect of Case-Based Teaching on Narrative Competencies
Traditional teacher-centered and didactic teaching methods rarely stimulate intrinsic motivation among students or enthusiasm among teachers. The disconnect between theoretical learning and real-world clinical practice hampers the development of critical thinking, humanistic qualities, and professional spirit essential for future physicians. In contrast, case-based teaching of narrative medicine adopts a student-centered approach, encouraging residents to integrate narrative knowledge with clinical cases. Through direct engagement with real obstetric patients, residents are guided to independently reflect on treatment planning by combining clinical theory with practical application. More importantly, narrative medicine education fosters respect, empathy, and humanistic care toward patients.
Recent research has demonstrated the efficacy of narrative medicine in enhancing empathy and humanistic care among medical trainees. A study integrating narrative medicine into clinical internship teaching found significant improvements in students’ empathy skills, highlighting the value of narrative approaches in medical education.22 Furthermore, structured narrative and case-based learning strategies have been shown to significantly enhance clinical reasoning and critical thinking skills among medical trainees through the use of semantic qualifiers and dual-process theory.23 Simulation-based learning models, progressing from simple to complex clinical situations, have also been reported to effectively strengthen students’ adaptability, empathy, and humanistic competencies.24 These findings support the educational value of narrative medicine when combined with case-based teaching, providing a robust framework for fostering the holistic development of obstetric residents.
In our study, we compared the academic performances of residents undergoing case-based teaching of narrative medicine versus conventional clinical teaching. Both knowledge test and OSCE scores improved after the obstetrics rotation in the experimental group; however, a statistically significant difference was observed only in OSCE scores. This suggests that while both approaches supported knowledge acquisition, the integrated teaching method had a more pronounced impact on practical performance. The OSCE, which assesses not only procedural skills but also clinical reasoning, communication, and professionalism, is particularly sensitive to improvements in humanistic and interpersonal competencies. It is important to note that both groups received the same total instructional time. Therefore, the enhanced OSCE performance in the experimental group is more likely attributable to the content and structure of the narrative medicine based intervention, rather than increased exposure or repetition. This minimizes the possibility of bias due to self-fulfilling expectations. These results demonstrate that case-based teaching of narrative medicine not only solidified residents’ theoretical knowledge and clinical procedures but also notably enhanced their empathy, patient-centered thinking, and doctor-patient communication skills. An increased focus on patients’ experiences during clinical management contributed to building greater trust between patients and physicians. Additionally, teaching satisfaction—evaluated via questionnaire—was significantly higher among residents in the experimental group, particularly in areas such as active learning interest, clinical thinking ability, medical skills, doctor-patient communication, and overall teaching methods. These findings align with the objective performance outcomes and further confirm the perceived value of this educational model. Subjectively, residents recognized case-based teaching of narrative medicine as an effective and innovative enhancement to the traditional teaching model within standardized residency training, well-suited to current clinical realities.
Effect of Case-Based Teaching of Narrative Medicine on Improving Narrative Competencies
In this study, case-based teaching of narrative medicine was systematically implemented through a combination of online instruction (conceptual framework lectures and intensive literary reading) and offline sessions focusing on narrative thinking, reading, and reflective writing. Intensive interaction between narrative medicine and clinical cases in the obstetrics department further enriched the residents’ comprehensive quality. After the obstetrics rotation, residents in the experimental group demonstrated significant improvements in competencies related to narrative cognition of wellness, professional narrative thinking, career construction, peer communication, and doctor-patient communication. However, no significant improvements were observed in narrative behavior of wellness and family connection, which may be attributed to residents’ limited life experiences during prolonged periods of academic training. Additionally, most residents (82.61%) lived with friends or et al, rather than with family members, possibly resulting in reduced exposure to family-related narrative contexts. Future efforts should focus on further intensifying narrative medicine education to facilitate deeper internalization of narrative competencies.
Although slight improvements were observed in the control group through conventional training and peer communication, no significant differences were detected, highlighting the necessity and effectiveness of case-based teaching of narrative medicine in standardized residency training. According to the Stages of Competence model, young physicians progress through four stages to develop narrative competencies: unconscious narrative incompetence, conscious narrative incompetence, conscious narrative competence, and unconscious narrative competence. In the initial stage, physicians are unaware of their deficiencies in narrative and clinical skills. In the second stage, they recognize their shortcomings and seek improvement. In the third stage, they acquire the necessary knowledge and skills but require regular practice for mastery. Finally, in the unconscious competence stage, narrative and clinical skills become second nature.25
Case-based teaching of narrative medicine offers a holistic view of clinical practice. Patients seek not only treatments but also respect, empathy, and attentive listening. By integrating the objectivity, technical rigor, and regularity advocated by evidence-based medicine with the humanistic perspective promoted by narrative medicine, case-based teaching cultivates multidimensional narrative competencies, supplementing traditional biomedical training and ultimately enhancing healthcare quality.26
There is an urgent need to reform clinical teaching concepts, designs, and programs within standardized residency training to improve the comprehensive quality of future physicians. Focusing on medical humanities, narrative medicine has been shown to significantly improve clinical outcomes and reduce unnecessary doctor-patient conflicts.27 Case-based teaching remains superior in stimulating learners’ active participation.19 Combining narrative medicine and case-based teaching provides obstetric residents with both fundamental obstetric knowledge and essential narrative competencies, paving the way toward a three-dimensional training goal encompassing knowledge, skills, and humanistic competencies, and preparing residents for excellence in clinical practice.
Conclusion
This study demonstrated that narrative medicine education empowered by case-based teaching significantly improved obstetric residents’ OSCE scores, narrative competencies, and teaching satisfaction compared to conventional clinical instruction. Notably, residents in the experimental group showed marked gains in areas such as professional narrative thinking, doctor-patient communication, and active learning engagement. These findings highlight the effectiveness of this integrated teaching approach in enhancing both clinical performance and humanistic qualities within standardized residency training.
This teaching model is not limited to Obstetrics and Gynecology. With its focus on humanistic care, empathy, and clinical reflection, the integration of narrative medicine and case-based teaching has the potential to benefit various medical specialties.Therefore, this model holds promise for broader application in other disciplines, and future studies should explore its generalizability and specialty-specific impact.
Abbreviations
OSCE, objective structured clinical examination; S-CVI, scale-level content validity index; CFA, confirmatory factor analysis; GFI, goodness of fit index.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of the Fourth Hospital of Hebei Medical University. No biomedical, clinical or biometric data were obtained, and all methods were carried out in accordance with relevant guidelines and regulations in ethical declarations. Informed consent was shown along with the questionnaire before the survey. Informed consent was obtained from all participants and all of were over 18 years old.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Provincial Graduate Demonstration Course in 2024 (KCJSX2024040) and the Medical Science Research Project of Hebei (Grant No. 20240817).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ma X, Zhao Q, Sun B, et al. New Advancements in the Residency Training System in the United States and Our Acquired Knowledge[M];Beijing;People’s Medical Publishing House;2009.1
2. Miniotti M. Empathy for patient care in medical students: new evidence on the importance of self-transcendence. Psychol Health Med. 2022;27(5):1035–1041. doi:10.1080/13548506.2020.1842897
3. Kagawa Y, Ishikawa H, Son D, et al. Using patient storytelling to improve medical students’ empathy in Japan: a pre-post study. BMC Med Educ. 2023;23(1):67. doi:10.1186/s12909-023-04054-1
4. Nasser JS, Chung KC. Recommendations for the reform of medical education in China: a SWOT analysis. Health Policy Open. 2020;1:100018. doi:10.1016/j.hpopen.2020.100018
5. Mei A, Gao D, Jiang J, Qiao T, Wang F, Li D. The medical education systems in China and Thailand: a comparative study. Health Sci Rep. 2022;5(6):e826. doi:10.1002/hsr2.826
6. Savsar L, Savsar M. Healthcare quality and narrative medicine Ijasos. 2019;5(15):1404–1413. doi:10.18769/18769/ijasos.592112
7. Milota MM, van Thiel GJMW, van Delden JJM, van Thiel GJMW. Narrative medicine as a medical education tool: a systematic review. Med Teach. 2019;41(7):802–810. doi:10.1080/0142159X.2019.1584274
8. Charon R. The patient-physician relationship. Narrative medicine: a model for empathy, reflection, profession, and trust. JAMA. 2001;286(15):1897–1902. doi:10.1001/jama.286.15.1897
9. Charon R. Narrative medicine: form, function, and ethics. Ann Intern Med. 2001;134(1):83–87. doi:10.7326/0003-4819-134-1-200101020-00024
10. Charon R. Narrative Medicine: Honoring the Stories of Ilness[M]. New York: Oxford University Press, 2006.
11. Yu M. When I say … narrative competence. Med Educ. 2017;51(12):1203–1205. doi:10.1111/medu.13374
12. Mi M, Wu L, Zhang Y, Wu W. Integration of arts and humanities in medicine to develop well-rounded physicians: the roles of health sciences librarians. J Med Libr Assoc. 2022;110(2):247–252. doi:10.5195/jmla.2022.1368
13. Yang N, Xiao H, Cao Y, Li S, Yan H, Wang Y. Does narrative medicine education improve nursing students’ empathic abilities and academic achievement? A randomised controlled trial. J Int Med Res. 2018;46(8):3306–3317. doi:10.1177/0300060518781476
14. Bi M, Zhao Z, Yang J, Wang Y. Comparison of case-based learning and traditional method in teaching postgraduate students of medical oncology. Med Teach. 2019;41(10):1124–1128. doi:10.1080/0142159X.2019.1617414
15. Wei F, Sun Q, Qin Z, Zhuang H, Jiang G, Wu X. Application and practice of a step-by-step method combined with case-based learning in Chinese otoendoscopy education. BMC Med Educ. 2021;21(1):89. doi:10.1186/s12909-021-02513-1
16. Yang HC. Teaching LGBT+ health and gender education to future doctors: implementation of case-based teaching. Int J Environ Res Public Health. 2021;18(16):8429. doi:10.3390/ijerph18168429
17. Li X, Li Y, Li X, Chen X, Yang G, Yang L. Comparison of case-based learning combined with rain classroom teaching and traditional method in complete denture course for undergraduate interns. BMC. Med Educ. 2022;22(1):610. doi:10.1186/s12909-022-03678-z
18. Yang X, Jia Y, Zhao C, Jin H, Ling Z. Development and reliability/validity testing of the narrative competencies scale for medical practitioners. Medicine and Philosophy. 2023;44(21):39–44. doi:10.12014/j.issn.1002-0772.2023.21.09
19. Kolahdouzan M, Mahmoudieh M, Rasti M, Omid A, Rostami A, Yamani N. The effect of case-based teaching and flipped classroom methods in comparison with lecture method on learning and satisfaction of internship students in surgery. J Educ Health Promot. 2020;9:256. doi:10.4103/jehp.jehp_237_19
20. Obstetric Subgroup. Society of obstetrics and gynecology, chinese medical association. experts consensus on screening and diagnosis of perinatal depression. Chin J Obstetrics Gynecol. 2021;56(8):521–527. doi:10.3760/cma.j.cn112141-20210115-00022.
21. Xiao S, Yuan J, Lan H, et al. Investigation of clinical medicine undergraduates’ recognition of narrative medicine. BMC Med Educ. 2024;24(1):321. doi:10.1186/s12909-024-05279-4
22. Yuan J, Zeng X, Cheng Y, Lan H, Cao K, Xiao S. Narrative medicine in clinical internship teaching practice. Med Educ Online. 2023;28(1):2258000. doi:10.1080/10872981.2023.2258000
23. Tokushima Y, Hirata R, Yamashita S, Shikino K, Shimizu T, Tago M. Enhancing clinical reasoning education: implementing case conferences with semantic qualifiers and the dual-process theory. Adv Med Educ Pract. 2024;15:1149–1154. doi:10.2147/AMEP.S486420
24. Changuiti O, Moustarhfir N, Marfak A, Saad E, Hilali A, Youlyouz-Marfak I. simulation based-learning from simple to complicated clinical situations for midwifery students. Adv Med Educ Pract. 2021;12:881–886. doi:10.2147/AMEP.S318560
25. Yang XL. Chinese Narrative Medicine and Medical Profes Sionals’ Competencies[M]. Guangzhou: Guangdong Higher Education Press; 2023.
26. Chu SY, Wen CC, Lin CW. A qualitative study of clinical narrative competence of medical personnel. BMC Med Educ. 2020;20(1):415. doi:10.1186/s12909-020-02336-6
27. Scott-Conner CEH, Agarwal D. Applications of narrative medicine to surgical education. Am Surg. 2022;88(12):2851–2856. doi:10.1177/00031348211029851
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.