Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Effectiveness of Benralizumab in Reducing Asthma and COPD Exacerbations in Patients with Severe Asthma and Concomitant COPD: Real-World Evidence from the ZEPHYR-5 Study
Authors Adrish M ![]() , DeMartino JK, Carstens D, Jackson M, Wilson K, Schinkel J, Tkacz J
, DeMartino JK, Carstens D, Jackson M, Wilson K, Schinkel J, Tkacz J
Received 22 August 2025
Accepted for publication 10 December 2025
Published 14 January 2026 Volume 2026:21 562498
DOI https://doi.org/10.2147/COPD.S562498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Muhammad Adrish,1 Jessica K DeMartino,2 Donna Carstens,2 Mandy Jackson,2 Kathleen Wilson,3 Jill Schinkel,3 Joseph Tkacz3
1Baylor College of Medicine, Houston, TX, USA; 2AstraZeneca, Wilmington, DE, USA; 3Inovalon, Bowie, MD, USA
Correspondence: Joseph Tkacz, Inovalon, 4321 Collington Road, Bowie, MD, 20716, USA, Email [email protected]
Purpose: This real-world evidence study sought to evaluate the effectiveness of benralizumab on reducing both asthma and COPD exacerbations among patients with a diagnosis of asthma and concomitant COPD.
Patients and Methods: This study was a non-interventional, single-arm, retrospective database analysis of the MORE2 Registry® and the 100% Medicare Fee-for-Service (FFS) claims databases from 2017– 2022. Inclusion criteria were as follows: 1) prescription claim for benralizumab and ≥ 1 refill within 90 days (earliest claim=index date), 2) 12 months of database enrollment preceding (baseline) and following (follow-up) the index date, 3) medical claims with diagnoses of asthma and COPD during the baseline period, and 4) presence of ≥ 2 asthma exacerbations during the baseline period. Percent change in the annual rates of both asthma and COPD exacerbations were assessed from the baseline to follow-up, with paired t-tests used to examine statistically significant differences. Subgroup analyses were also conducted among the subset of patients with blood eosinophil levels, and by payer type.
Results: A total of 2894 patients with asthma and concomitant COPD were included. Following initiation of benralizumab, the mean (SD) number of total asthma exacerbations decreased by 39.2% (from 4.0 (2.2) to 2.4 (2.4) exacerbations/year; p < 0.001), while COPD exacerbations decreased by 45.6% (from 3.6 (2.5) to 1.9 (2.2) exacerbations/year; p < 0.001). The proportion of patients receiving systemic corticosteroids decreased by 11.4% from 100% to 88.6% (p < 0.001). Subgroup analyses revealed that patients with the highest eosinophil levels (≥ 300 eosinophils/μL) experienced the greatest reductions in asthma exacerbations (42.7%) and COPD exacerbations (50.8%; all p < 0.001).
Conclusion: This study provides real-world evidence supporting the effectiveness of benralizumab in reducing both asthma and COPD exacerbations and decreasing reliance on corticosteroids, particularly among those with elevated eosinophil levels.
Keywords: benralizumab, COPD, asthma, exacerbations, biologics, blood eosinophils
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are both chronic inflammatory airway diseases.1,2 Asthma is characterized by shortness of breath, wheezing, coughing, chest tightness, variable airflow limitation, and tissue remodeling, often driven by eosinophilic pathways.1 In contrast, COPD is a progressive disease associated with persistent airflow limitation and predominantly neutrophilic inflammation.1 While considered to be distinct conditions, a subset of patients presents with overlapping features of both diseases.3 Asthma and concomitant COPD affect approximately 15–35% of the overall asthma population,4–7 with prevalence rates varying based on diagnostic criteria and population characteristics.
Patients with features of asthma and COPD tend to have a higher burden of comorbidities, including cardiovascular conditions, obesity, other metabolic disorders, and depression, complicating disease management.8–11 Many also continue to experience greater symptom burden and more frequent or severe exacerbations despite the use of maintenance and other respiratory medications.12,13 This increased exacerbation frequency and severity often lead to hospitalizations and progressive lung function decline over time,6,14 underscoring the need for effective targeted therapeutic strategies that address both inflammatory and clinical aspects of these diseases.
Eosinophilic inflammation has emerged as a shared biological mechanism among several respiratory conditions.15 Elevated blood eosinophil levels are associated with a greater risk of exacerbations,16,17 corticosteroid responsiveness,18 and heightened airway inflammation across both diseases.17,19 This overlapping inflammatory profile supports the therapeutic rationale for targeting interleukin-5 (IL-5) mediated pathways in patients exhibiting features of both asthma and COPD.15
In clinical trials benralizumab, an anti–IL-5 receptor α monoclonal antibody that depletes eosinophils through antibody-dependent cell-mediated cytotoxicity, has demonstrated significant reductions in asthma exacerbation rates and oral corticosteroid dependence in patients aged 6 years and older with severe asthma of the eosinophilic phenotype.20,21 However, no randomized clinical trials have evaluated the safety and efficacy of benralizumab in patients with both asthma and concomitant COPD. However, a recent real-world study demonstrated that benralizumab reduced both asthma and COPD exacerbations in individuals with both asthma and concomitant COPD, particularly among those with elevated eosinophil levels.22
Real-world data provides an opportunity to further examine the effectiveness of benralizumab in this heterogeneous and complex population, particularly among older patients who were not evaluated in prior real-world studies or were excluded from clinical trials due to factors such as smoking status, which is more characteristic of COPD. As such, this real-world analysis aimed to assess the changes in both asthma and COPD exacerbations following initiation of benralizumab among patients with severe asthma and concomitant COPD in a real-world setting. Analyses also assessed changes in both asthma and COPD exacerbations by baseline blood eosinophil levels and by payer (Medicare, commercial, and Managed Medicaid). Analysis of Medicare beneficiaries provides new insights into treatment effectiveness of benralizumab among older adults, who are disproportionately affected by both asthma and concomitant COPD.
Materials and Methods
Study Design and Data Sources
This non-interventional, single-arm, retrospective cohort study used administrative claims from the Inovalon MORE2 Registry® of Closed Claims (MORE2 Registry®) and the 100% Medicare Fee For Service (Medicare FFS) databases. The study period began at the time of commercial availability of benralizumab (November 14, 2017) and ended on December 31, 2022 among patients appearing in the 100% Medicare FFS database, and on May 31, 2023 among patients appearing in the MORE2 Registry®. The study used a 12-month pre-post design to evaluate the effectiveness of benralizumab among patients with severe asthma and concomitant COPD, with the index date defined as the earliest prescription claim for benralizumab during the study period. The 12-month timeframe for both pre- and post-index observation periods provided a sufficient baseline period to establish exacerbation rates and a sufficient follow-up period to evaluate treatment effects following benralizumab initiation.
The 100% Medicare FFS database contains enrollment information and medical claims for Parts A, B, and prescription drug data for all Part D plans. The MORE2 Registry contains claims from all 50 states and is sourced from over 140 health plans. Baseline eosinophil values were obtained from the Prognos laboratory results database. Databases are de-identified and in compliance with the confidentiality requirements outlined in the Health Insurance Portability and Accountability Act (HIPAA) of 1996. Therefore, this study was exempt from Institutional Review Board review and did not require patient consent.
Study Population and Subgroups
The study population included individuals who had 1) a prescription claim for benralizumab and at least one refill within 90 days (earliest prescription claim was defined as the index date), 2) 12 months of database enrollment preceding (pre-index period) and following (post-index period) the index date, 3) 40 years of age or older on the index date, 4) one or more inpatient or two or more outpatient claims with an International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis code for asthma (J45*) during the pre-index period, 5) ≥ 1 inpatient claim with an ICD-10-CM diagnosis for COPD (J41*-J44*) in the primary position or ≥ 2 outpatient claims with an ICD-10-CM diagnosis code for COPD in any position during the 12-month baseline period, and 6) presence of at least two asthma exacerbations during the pre-index period. Patients were grouped based on payer type: commercial, Medicare (Medicare FFS and Medicare Advantage), or Managed Medicaid. Among patients with available, non-missing eosinophil data, a subgroup analysis was conducted by categorizing individuals according to the highest recorded blood eosinophil count in the 12-month baseline period: <150 cells/µL, 150–299 cells/µL, and ≥300 cells/µL.
Study Outcomes and Analysis
Asthma22–25 and COPD22,25,26 exacerbations were defined based on previously published claims-based algorithms. Asthma exacerbations were defined as meeting one of the following criteria: 1) at least one inpatient claim with a diagnosis of asthma in the primary position; 2) at least one claim with a procedure code for mechanical ventilation and corresponding asthma diagnosis on the same day; or 3) at least one emergency department visit, urgent care visit, or other outpatient visit claim with an asthma diagnosis and treated with short course of systemic corticosteroids, either one administration of injectable corticosteroids or oral corticosteroids for at least three days, within (±) seven days. A maximum of one exacerbation event was counted in any 14-day period.
COPD exacerbations were classified as either 1) moderate, defined as an outpatient visit with a diagnosis of COPD accompanied by a filled prescription for a course of theophylline, aminophylline, or an oral corticosteroid or an oral antibiotic within (±) 7 days of the outpatient visit, or an outpatient visit with a diagnosis of COPD and a corticosteroid injection; 2) severe, defined as an inpatient admission with a diagnosis of COPD, acute lower respiratory infection, simple and mucopurulent chronic bronchitis, unspecified chronic bronchitis, or emphysema in the primary position, or a diagnosis of respiratory failure or lower respiratory tract infection (not pneumonia-related) in the primary position with a diagnosis of COPD in the secondary position. Only one exacerbation event was counted in any 14-day period. COPD exacerbations were evaluated in total and stratified by severity level (moderate or severe). However, due to the low counts of severe events, COPD exacerbations by severity level were not reported for the baseline blood eosinophil level or payer type subgroups.
Study outcomes included the percentage change in the annual asthma exacerbation rate (AAER) and annual COPD exacerbation rate (ACER) per year and were evaluated by comparing the 12-month pre-index period to the 12-month post-index period.
Additional outcomes included changes in respiratory medication and treatment utilization prior to and following the initiation of benralizumab and included oxygen therapy, nebulizer use, inhaled corticosteroids (ICS), systemic corticosteroids, short-acting β2-agonists (SABA), short-acting muscarinic antagonists (SAMA), long-acting β-agonists (LABA), long-acting muscarinic antagonists (LAMA), ICS/LABA combinations, ICS/LABA/LAMA combinations, leukotriene modifiers, mast cell stabilizers, methylxanthines, and PDE-4 inhibitors.
Descriptive statistics of means, medians, and standard deviations were presented for continuous variables, while frequencies and percentages were presented for binary or categorical variables. For all descriptive statistics with comparisons between pre-index and post-index periods, percentage change from pre-index to post-index was calculated and statistically significant differences were determined via paired Student’s t-test or the Wilcoxon signed-rank test for continuous variables, and McNemar’s test for binary or categorical variables. The critical alpha level was set at 0.05 for all analyses.
Results
Study Population and Patient Characteristics
A total of 2894 patients with asthma and concomitant COPD were included in the study. The mean (SD) age of the sample was 67.2 (11.1) years, and the majority of patients were female (66.7%) and resided in the southern region of the US (40.2%; Table 1). The sample included representation of the following payer types: 273 (9.4%) with commercial insurance, 2202 (76.1%) with Medicare, and 419 (14.5%) with Managed Medicaid. The mean (SD) Elixhauser Comorbidity Index was 7.4 (8.1). Cardiovascular conditions and other comorbidities were common and reflected an older patient population with multiple comorbid conditions such as hypertension (77.0%), dyslipidemia (66.7%), anxiety (37.7%), depression (33.0%), gastroesophageal reflux disease (59.3%), obesity (42.4%), and ischemic heart disease (27.0%). Approximately 15.9% of patients had a diagnosis of tobacco dependence.
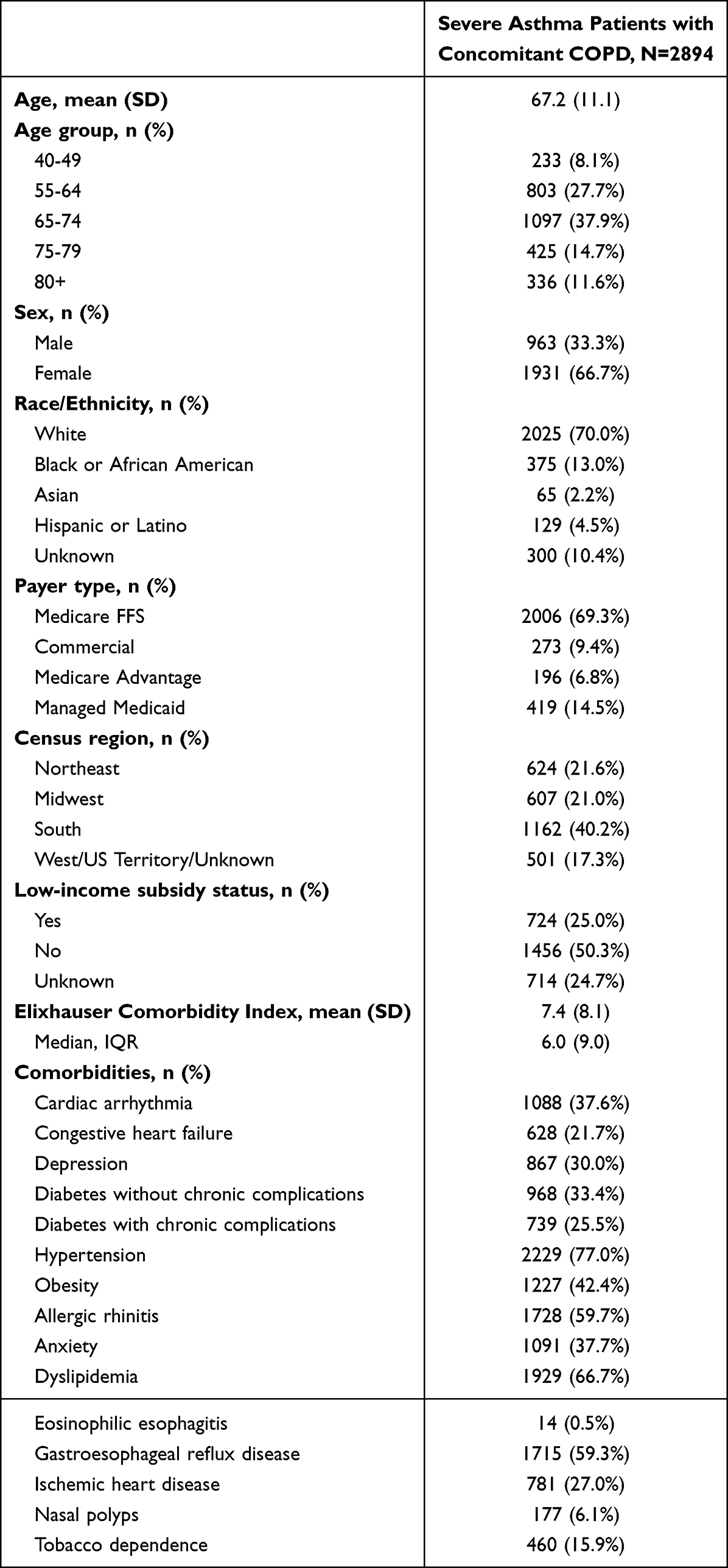 |
Table 1 Patient Characteristics Among Severe Asthma Patients with Concomitant COPD Initiating Benralizumab |
Changes in Respiratory-Related Medications Utilization Following Initiation of Benralizumab
Use of respiratory medications in the baseline period was common and decreased after initiation of benralizumab, except for ICS/LAMA/LABA triple therapy (Table 2). The proportion of patients receiving systemic corticosteroids decreased by 11.4% from 100% to 88.6% (p < 0.001), and the proportion using SABA rescue medications decreased by 12.5% from 89.1% to 78.0% (p < 0.001). The proportion of patients receiving closed ICS/LAMA/LABA triple therapy increased by 22.8% from 12.9% to 15.8%.
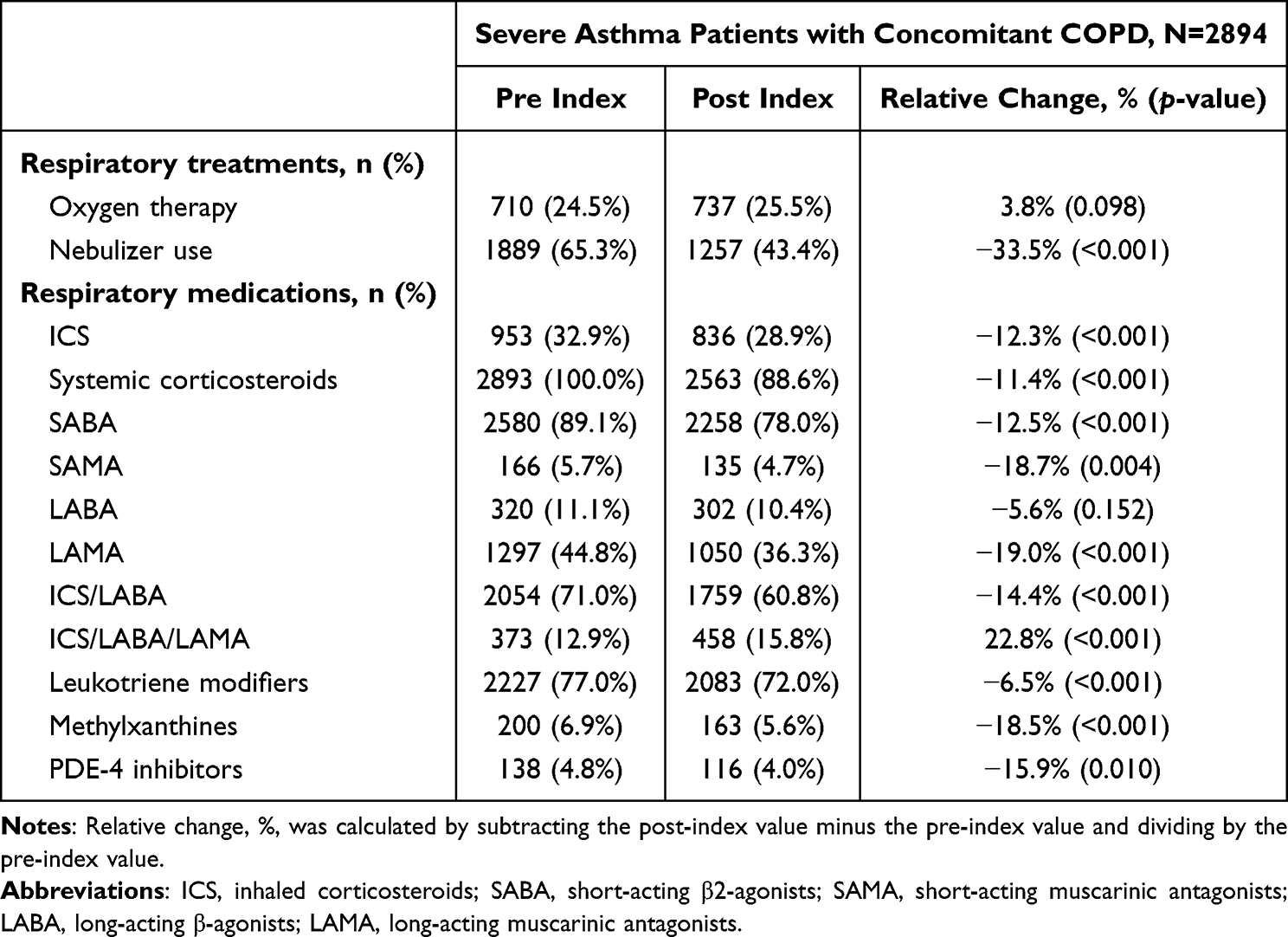 |
Table 2 Respiratory Medications Among Severe Asthma Patients with Concomitant COPD Initiating Benralizumab |
Reduction in Asthma Exacerbation Following Initiation of Benralizumab
Following initiation of benralizumab, the mean (SD) number of asthma exacerbations per year decreased by 39.2% from 4.0 (2.2) to 2.4 (2.4) exacerbations per year (p < 0.001; Figure 1 and Supplemental Table 1). Accordingly, the proportion of patients experiencing fewer asthma exacerbations increased, while the proportion of patients with 4 or more asthma exacerbations decreased from 47.5% in the baseline period to 25.5% during the follow-up period (Figure 2 and Supplemental Table 2). By payer type, greater reductions in asthma exacerbations were observed among patients with Medicare or commercial plan types (Figure 1). Among Medicare patients, the mean (SD) annual rate of asthma exacerbations decreased by 40.4% from 3.9 (2.1) to 2.3 (2.3) exacerbations per year (p < 0.001); among those with commercial insurance by 38.8% from 3.9 (2.1) to 2.4 (2.4) exacerbations per year (p < 0.001); and among those with Managed Medicaid by 34.1% from 4.5 (2.5) to 3.0 (2.7) exacerbations per year (p < 0.001; Supplemental Table 3).
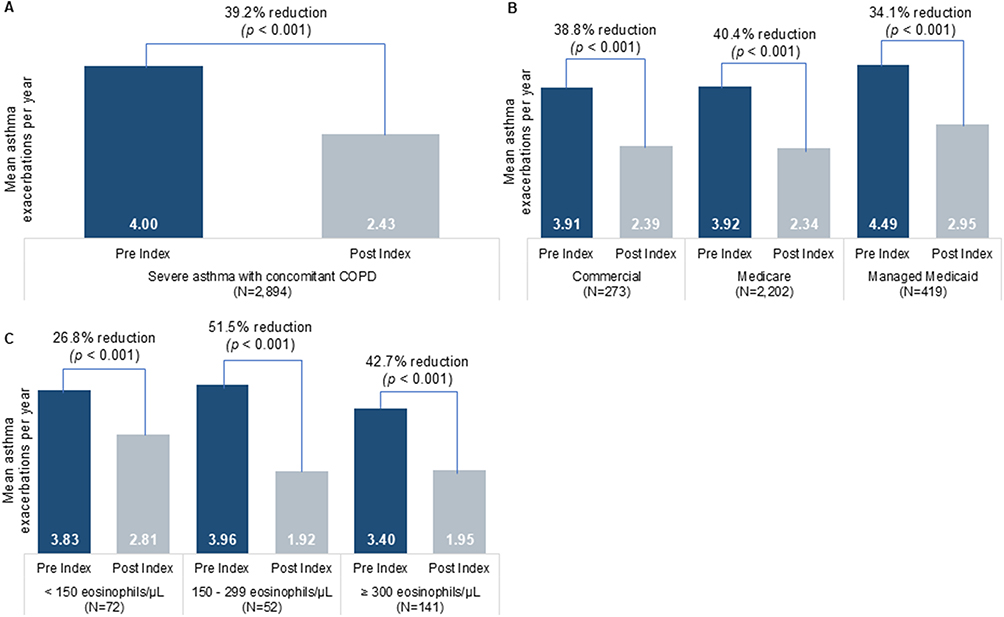 |
Figure 1 Reduction of annual asthma exacerbation rate among severe asthma patients with concomitant COPD initiating benralizumab (A) overall, (B) by payer, and (C) by baseline blood eosinophil levels. Abbreviation: COPD, chronic obstructive pulmonary disease. Notes: Relative change, %, was calculated by subtracting the post-index value minus the pre-index value and dividing by the pre-index value. |
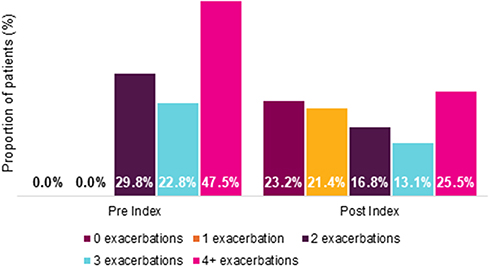 |
Figure 2 Number of asthma exacerbations among severe asthma patients with concomitant COPD initiating benralizumab. Abbreviation: COPD, chronic obstructive pulmonary disease. Notes: Relative change, %, was calculated by subtracting the post-index value minus the pre-index value and dividing by the pre-index value. |
Reductions in asthma exacerbations were more pronounced among patients with elevated baseline eosinophil levels, with mean (SD) annual asthma exacerbation rates decreasing by 42.7% [from 3.4 (1.7) to 2.0 (1.9) exacerbations per year; p < 0.001] in the ≥ 300 cells/µL cohort, 51.5% [from 4.0 (2.3) to 1.9 (1.7) exacerbations per year; p < 0.001] in the 150–299 cells/µL cohort, and 26.8% [from 3.8 (2.0) to 2.8 (2.3) exacerbations per year; p < 0.001] in the < 150 cells/µL cohort (Figure 1).
Reduction in COPD Exacerbations Following Initiation of Benralizumab
Following initiation of benralizumab, the mean (SD) number of total COPD exacerbations per year decreased by 45.6% from 3.6 (2.5) to 1.9 (2.2) exacerbations per year (p < 0.001; Figure 3). The proportion of patients experiencing 0 or 1 COPD exacerbations increased, while the proportion of patients with 4 or more COPD exacerbations decreased from 43.0% in the baseline period to 19.0% during the follow-up period (Figure 4). Moderate COPD exacerbations were more common than severe COPD exacerbations, although there were significant reductions in both COPD exacerbation severities. The mean (SD) number of moderate COPD exacerbations decreased by 44.9% from 3.4 (2.4) to 1.9 (2.1) exacerbations per year; whereas severe COPD exacerbations decreased by 59.7% from 0.16 (0.55) to 0.07 (0.33) exacerbations per year (p < 0.001; Figure 3).
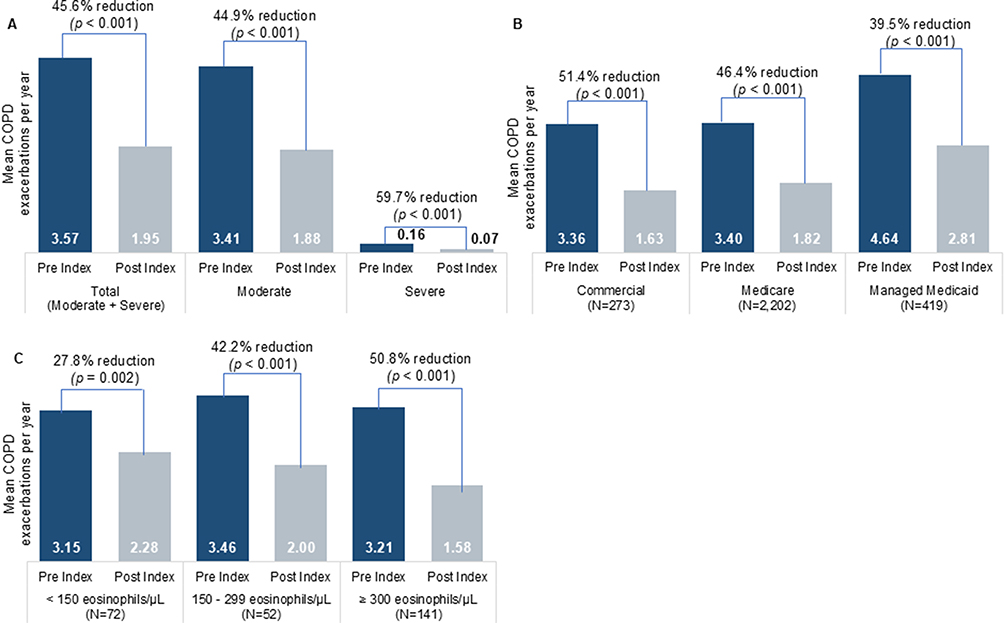 |
Figure 3 Reduction of annual COPD exacerbation rate among severe asthma patients with concomitant COPD initiating benralizumab (A) overall, (B) by payer, and (C) by baseline blood eosinophil levels. Abbreviation: COPD, chronic obstructive pulmonary disease. Notes: Relative change, %, was calculated by subtracting the post-index value minus the pre-index value and dividing by the pre-index value. |
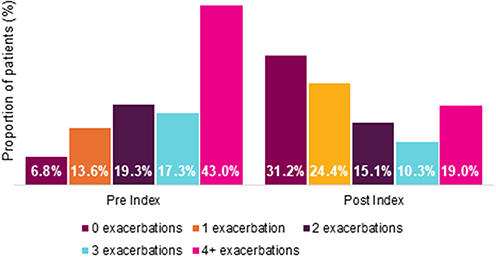 |
Figure 4 Number of COPD exacerbations among severe asthma patients with concomitant COPD initiating benralizumab. |
The largest reductions in the number of total COPD exacerbations following the initiation of benralizumab were observed among patients with Medicare or commercial insurance plan types (Figure B). Among Medicare patients, the mean (SD) annual rate of total COPD exacerbations decreased by 46.4% from 3.4 (2.4) to 1.8 (2.1) exacerbations per year (p < 0.001); among patients with commercial insurance, the mean (SD) annual rate of total COPD exacerbations decreased by 51.4% from 3.4 (2.2) to 1.6 (2.0) exacerbations per year (p < 0.001). The reductions in the annual rate of total COPD exacerbations among patients with Managed Medicaid were more moderate, decreasing by 39.5% from 4.6 (2.8) to 2.8 (2.7) exacerbations per year (p < 0.001).
A total of 265 patients had available baseline blood eosinophil levels, and of those, 72 (27.2%) had < 150 cells/µL; 52 (19.6%) had 150–299 cells/µL, and 141 (53.2%) had ≥ 300 cells/µL. Subgroup analyses based on baseline eosinophil levels demonstrated that the greatest reductions in total COPD exacerbations were observed following benralizumab initiation among patients with elevated baseline eosinophil levels, decreasing by 50.8% in the ≥ 300 cells/µL cohorts compared to 42.2% in the 150–299 cells/µL cohort and 27.8% in the < 150 cells/µL cohort (Figure 3).
Discussion
This retrospective, single-arm, observational study evaluated the real-world effectiveness of benralizumab in reducing both asthma and COPD exacerbation rates among patients with severe asthma and concomitant COPD. The study population consisted of older adults, at least 40 years of age (mean age 67.2 years), with multiple comorbidities, reflecting the complex disease burden associated with the population with severe asthma and concomitant COPD. Primary analyses showed a 39.2% reduction in the annual asthma exacerbation rate and a 45.6% reduction in the annual COPD exacerbation rate. These results highlight meaningful reductions in both asthma and COPD exacerbations, outcomes that are critical for reducing hospitalizations and overall healthcare utilization in this high-risk patient population.
In the present study, meaningful reductions in both asthma and COPD exacerbations were observed across all baseline eosinophil levels. Subgroup analyses based on baseline eosinophil levels showed that patients with the highest eosinophil counts (≥300 eosinophils/µL) experienced the greatest reductions in the rate of asthma (42.7%) and COPD (50.8%) exacerbations, while those with lower eosinophil counts (<150 eosinophils/µL) showed more modest improvements (26.8% reduction in asthma and 27.8% reduction in COPD exacerbations). These results support the potential use of elevated eosinophil levels as a biomarker to predict response to benralizumab in individuals with asthma and concomitant COPD,25,27 and suggest that personalized treatment strategies may result in improved outcomes, particularly for patients with elevated blood eosinophil counts.
The study findings are consistent with prior real-world evidence evaluating the effectiveness of benralizumab in reducing the rate of asthma and COPD exacerbations.22 The ZEPHYR-2 study assessed treatment-naïve individuals aged 12 years and older with a diagnosis of asthma and concomitant COPD who initiated benralizumab and had at least one COPD exacerbation during the baseline period. Despite differences in the patient populations being evaluated, the present study showed similar reductions in the overall rate of both asthma and COPD exacerbations compared to the ZEPHYR-2 study. The ZEPHYR-2 study found a 40% reduction in the annual rate of asthma exacerbations and a 51% reduction in the annual rate of COPD exacerbations. Differences between the two studies are likely attributable to variations in patient populations, including the number of baseline COPD exacerbations, minimum age criteria, and insurance plan types, as this study focused on individuals aged 40 years and older with or without prior COPD exacerbations, many of whom were covered by Medicare FFS.
Consistent with the prior ZEPHYR-2 study,22 a notable trend in respiratory medication use was also observed in the present study, with a decrease in the proportion of patients using most maintenance and short-acting rescue therapies following benralizumab initiation, with the exception of ICS/LAMA/LABA triple therapy. A decline in the frequency of systemic corticosteroid and ICS use suggests that patients may be experiencing better disease control, potentially reducing their reliance on these medications. Given the risks associated with long-term corticosteroid use, including metabolic and cardiovascular complications, this reduction represents a potential added benefit of benralizumab treatment.28
There are several limitations of this study. The single-arm study design, without a placebo or control group, limits the ability to distinguish natural variations in disease activity from the true effect of benralizumab. Observed reductions in exacerbations may be influenced by confounding factors rather than by the treatment itself. Concurrent changes in respiratory medications, especially the decrease in systemic corticosteroid and ICS use following benralizumab initiation, may have independently influenced exacerbation frequency. Smoking status and exposure were likely substantially underreported, with only 15.9% of patients having documented tobacco dependence despite evaluating a COPD population. Additionally, highly prevalent comorbidities in this elderly patient population, including cardiovascular disease, obesity, and other conditions may have independently contributed to exacerbation risk. These factors could not be adequately controlled in this observational analysis. Furthermore, the potential for regression to the mean cannot be excluded, as patients may have been enrolled during periods of high exacerbation frequency, and subsequent improvements may reflect natural disease fluctuation rather than treatment effect.
Additionally, a limitation inherent to claims-based studies is the reliance on ICD-10-CM diagnosis codes for identification of both asthma and COPD, without spirometric confirmation. Spirometry is the gold standard for confirming obstructive airway disease and distinguishing asthma from COPD phenotypes; its absence precludes definitive characterization of disease severity and lung function in the study population. This use of diagnosis codes, rather than physiologic measures, may result in diagnostic misclassification, as coding practices can vary across providers and healthcare settings. Additionally, identification of asthma and COPD exacerbations was based upon previously published claims-based algorithms, with each event attributed to asthma or COPD based on the ICD-10-CM diagnosis code recorded on the medical claim. Although it is assumed that these events represent true exacerbations as classified by the diagnosis code, this assumption was not validated through medical chart review. Finally, baseline blood eosinophil data were available for only a small subset of patients (9.2% of the cohort), limiting the generalizability of eosinophil subgroup analysis. Patients with baseline blood eosinophil data may differ systematically from those without such data, potentially introducing selection bias in the subgroup analyses.
Conclusion
This study provides real-world evidence supporting the effectiveness of benralizumab in reducing both asthma and COPD exacerbations and decreasing reliance on corticosteroids among patients with asthma and concomitant COPD. Importantly, these results were observed in a population that included older Medicare beneficiaries with substantial comorbidity burden, a demographic frequently underrepresented in clinical trials yet comprising a significant proportion of patients in clinical practice. These findings underscore the potential role of benralizumab as an important therapeutic option for patients with asthma and COPD, particularly those with elevated eosinophil levels.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author. Restrictions apply to the availability of these data, which were used under license for this study. Data access may be requested directly from Inovalon.
Ethics Approval and Informed Consent
The data were de-identified and complied with the patient privacy requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA); therefore, Institutional Review Board (IRB) review was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by AstraZeneca. AstraZeneca reviewed the manuscript to ensure scientific and medical accuracy and to support compliance with legal and regulatory requirements, without influencing the authors’ interpretations or conclusions.
Disclosure
JKD, DC, and MJ are employees of AstraZeneca. JS, KW, and JT are employees of Inovalon, which received research consulting fees from AstraZeneca. MA is a clinical consultant for AstraZeneca and has no financial disclosures. The authors report no other conflicts of interest.
References
1. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2025 update. 2025. Available from: https://ginasthma.org/2025-gina-strategy-report/.
2. (GOLD) GIfCOLD. Global strategy for the diagnosis, management, and prevention of COPD. 2025 Report. 2025. Available from: https://goldcopd.org/2025-gold-report/.
3. Maselli DJ, Hanania NA. Management of asthma COPD overlap. Ann Allergy Asthma Immunol. 2019;123(4):335–11. doi:10.1016/j.anai.2019.07.021
4. Hosseini M, Almasi-Hashiani A, Sepidarkish M, Maroufizadeh S. Global prevalence of asthma-COPD overlap (ACO) in the general population: a systematic review and meta-analysis. Respir Res. 2019;20(1):229. doi:10.1186/s12931-019-1198-4
5. de Marco R, Pesce G, Marcon A, et al. The coexistence of asthma and chronic obstructive pulmonary disease (COPD): prevalence and risk factors in young, middle-aged and elderly people from the general population. PLoS One. 2013;8(5):e62985. doi:10.1371/journal.pone.0062985
6. Vaz Fragoso CA, Murphy TE, Agogo GO, Allore HG, McAvay GJ. Asthma-COPD overlap syndrome in the US: a prospective population-based analysis of patient-reported outcomes and health care utilization. Int J Chron Obstruct Pulmon Dis. 2017;12:517–527. doi:10.2147/copd.S121223
7. Barrecheguren M, Esquinas C, Miravitlles M. The asthma–chronic obstructive pulmonary disease overlap syndrome (ACOS): opportunities and challenges. Curr Opin Pulm Med. 2015;21(1):74–79. doi:10.1097/MCP.0000000000000118
8. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL. Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest. 2005;128(4):2099–2107. doi:10.1378/chest.128.4.2099
9. Wijnhoven HA, Kriegsman DM, Hesselink AE, de Haan M, Schellevis FG. The influence of co-morbidity on health-related quality of life in asthma and COPD patients. Respir Med. 2003;97(5):468–475. doi:10.1053/rmed.2002.1463
10. Llanos J-P, Hector O, Guillaume G, et al. Health characteristics of patients with asthma, COPD and asthma–COPD overlap in the NHANES database. Int J Chronic Obstr. 2018;13(null):2859–2868. doi:10.2147/COPD.S167379
11. Syamlal G, Dodd KE, Mazurek JM. Asthma, chronic obstructive pulmonary disease, and asthma-COPD overlap among US working adults. J Asthma. 2023;60(4):718–726. doi:10.1080/02770903.2022.2089997
12. Hardin M, Silverman EK, Barr RG, et al. The clinical features of the overlap between COPD and asthma. Respir Res. 2011;12(1):127. doi:10.1186/1465-9921-12-127
13. Leung C, Sin DD. Asthma-COPD overlap: what are the important questions? CHEST. 2022;161(2):330–344. doi:10.1016/j.chest.2021.09.036
14. Lange P, Çolak Y, Ingebrigtsen TS, Vestbo J, Marott JL. Long-term prognosis of asthma, chronic obstructive pulmonary disease, and asthma-chronic obstructive pulmonary disease overlap in the Copenhagen City Heart study: a prospective population-based analysis. Lancet Respir Med. 2016;4(6):454–462. doi:10.1016/s2213-2600(16)00098-9
15. Tashkin DP, Wechsler ME. Role of eosinophils in airway inflammation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:335–349. doi:10.2147/copd.S152291
16. Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037–2047.e10. doi:10.1016/j.jaci.2018.04.010
17. Singh D, Wedzicha JA, Siddiqui S, et al. Blood eosinophils as a biomarker of future COPD exacerbation risk: pooled data from 11 clinical trials. Respir Res. 2020;21(1):240. doi:10.1186/s12931-020-01482-1
18. Barnes NC, Sharma R, Lettis S, Calverley PMA. Blood eosinophils as a marker of response to inhaled corticosteroids in COPD. Eur Respir J. 2016;47(5):1374–1382. doi:10.1183/13993003.01370-2015
19. George L, Brightling CE. Eosinophilic airway inflammation: role in asthma and chronic obstructive pulmonary disease. Ther Adv Chronic Dis. 2016;7(1):34–51. doi:10.1177/2040622315609251
20. FitzGerald JM, Bleecker ER, Nair P, et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled Phase 3 trial. Lancet. 2016;388(10056):2128–2141. doi:10.1016/S0140-6736(16)31322-8
21. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/S0140-6736(16)31324-1
22. Carstens DD, Maselli DJ, Cook EE, et al. Real-world effectiveness of benralizumab among patients with asthma and concomitant chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:1813–1818. doi:10.2147/copd.S468887
23. Jackson DJ, Pelaia G, Emmanuel B, et al. Benralizumab in severe eosinophilic asthma by previous biologic use and key clinical subgroups: real-world XALOC-1 programme. Eur Respir J. 2024;64(1):2301521. doi:10.1183/13993003.01521-2023
24. Chung Y, Katial R, Mu F, et al. Real-world effectiveness of benralizumab: results from the ZEPHYR 1 Study. Ann Allergy Asthma Immunol. 2022;128(6):669–676.e6. doi:10.1016/j.anai.2022.02.017
25. Carstens D, Maselli DJ, Mu F, et al. Real-world effectiveness study of benralizumab for severe eosinophilic asthma: ZEPHYR 2. J Allergy Clin Immunol Pract. 2023;11(7):2150–2161.e4. doi:10.1016/j.jaip.2023.04.029
26. Mapel DW, Roberts MH, Susan S, et al. Development and validation of a healthcare utilization-based algorithm to identify acute exacerbations of chronic obstructive pulmonary disease. Int J Chronic Obstr. 2021;16(null):1687–1698. doi:10.2147/COPD.S302241
27. Singh D, Criner GJ, Agustí A, et al. Benralizumab prevents recurrent exacerbations in patients with chronic obstructive pulmonary disease: a post hoc analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:1595–1599. doi:10.2147/copd.S418944
28. Zeiger R, Sullivan P, Chung Y, Kreindler JL, Zimmerman NM, Tkacz J. Systemic corticosteroid-related complications and costs in adults with persistent asthma. J Allergy Clin Immunol. 2020;8(10):3455–3465.e13. doi:10.1016/j.jaip.2020.06.055
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.