Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Effectiveness of an Interpersonal Influence Intervention to Increase Commitment to Adopt Health-Promoting Behavior in Nursing Students
Authors Zambrano Bermeo RN, Estrada González C ![]() , Herrera Guerra EDP
, Herrera Guerra EDP ![]()
Received 8 August 2023
Accepted for publication 7 November 2023
Published 7 December 2023 Volume 2023:16 Pages 3911—3922
DOI https://doi.org/10.2147/JMDH.S434413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rosa Nury Zambrano Bermeo,1 Catalina Estrada González,2 Eugenia del Pilar Herrera Guerra3
1School of Health, Universidad Santiago de Cali, Cali, Colombia; 2School of Health Sciences, Research Group EPICRITICA, Universidad Libre, Seccional Cali, Cali, Colombia; 3School of Health Sciences, Universidad de Córdoba, Montería, Colombia
Correspondence: Rosa Nury Zambrano Bermeo, School of Health, Universidad Santiago de Cali, Calle 5 # 62-00, Cali Valle del Cauca, Cali, 760032, Colombia, Tel +57 3007760830, Email [email protected]
Purpose: To determine the efficacy of the “interpersonal influence intervention” conducted by health professionals to increase the commitment to adopt health-promoting behavior in nursing students compared to the usual care of a university wellness program.
Patients and Methods: A quasi-experimental study was performed. The study included 114 nursing students from a university in Cali, Colombia, who were divided into a control group (n = 57) that received usual care and an experimental group (n = 57) that received the intervention designed and validated according to Nola Pender’s Health Promotion Model. The main outcome was the lifestyle measured before and after the test using the Health-Promoting Lifestyle Profile II Spanish version. The effect of the intervention was carried out through the average comparison, effect size measures were calculated using Cohen’s d and analysis of the effect of possible confounding variables on the intervention (ANCOVA).
Results: A statistically significant difference was observed between the experimental group and the control group (p = 0.015; 95% CI − 0.42, − 0.05). The effect size of the intervention was 0.49. The interpersonal influences exhibited by health professionals can increase the commitment to adopt health-promoting behaviors (Hypothesis 1), and the greater the commitment to a specific action plan, the more likely it is that health-promoting behaviors will be maintained over time (Hypothesis 2).
Conclusion: The effectiveness of the intervention interpersonal influences exerted by health professionals to increase the commitment to adopt health-promoting behavior is proven. Evidence demonstrates the practical utility of the Health Promotion Model.
Keywords: healthy lifestyle, health promotion, students’ health, interpersonal relations
Introduction
Strategies to promote healthy lifestyles are aimed to improve and maintain behaviors that favor the prevention of chronic noncommunicable diseases (NCDs). Healthy behaviors are acquired in the early stages of life, especially in childhood, and are influenced by internal and external factors of the human being, are maintained over time and can be modified over the years.1 Adolescence is a fundamental stage of the human being, since it represents the transition to adulthood, having biological, psychological, sexual, and social changes. This life cycle is where the habits and behaviors established in childhood are consolidated, therefore in this period of life it is more complex to modify the lifestyle.2
In recent years, the health of young people has been affected by modifiable risk factors such as a sedentary lifestyle and physical inactivity, causing the development of obesity and overweight. Approximately 80% of students in the world do not follow the recommendations on the minimum time required for daily physical activity, causing a health risk now and in the future.3 Overweight and obesity have reached exponential figures and, as a result, have become a phenomenon of public health concern. The WHO determined that in 2016 more than 340 million children and adolescents between 5 and 19 years of age suffered from obesity or overweight affecting both sexes equally and by the year 2020 obesity generated the loss of 2.8 million people worldwide.4
University students are a social group prone to adopt health risk behaviors.5 Sedentary behavior among them and vulnerability to symptoms of anxiety, depression and stress are very common.6 In addition, unhealthy eating habits such as not consuming vegetables and fruits at least once a day,7 skipping breakfast, eating sweets and fast food on a daily basis and the tendency to consume psychoactive substances are very common.8 Likewise, the World Health Organization indicates that people vulnerable to metabolic risk factors can trigger hyperglycemia, hyperlipidemia, overweight or obesity and arterial hypertension, and eventually lead to cardiovascular disease, considered the main non-communicable disease (NCD) responsible for premature deaths.9
A health-promoting lifestyle is an important factor in maintaining and improving the health of young people and emerging adults.5 An important way to halt the growth of NCDs is to target the reduction of modifiable risk factors through low-cost interventions.9 Nursing as a science that encompasses autonomous and collaborative care of the individual, family and community, establishes strategies for health promotion and disease prevention, seeking to minimize the development of chronic diseases that affect the health and lives of individuals. Therefore, nursing students need to adopt health-promoting behavior demonstrated in healthy lifestyle behaviors that include consuming a balanced diet, daily breakfast and having good eating habits, regular exercise, and good sleep for the development of their physical and mental health, to provide better services.10
According to the Health Promotion Model (HPM), healthy behavior is determined by individual characteristics and experiences that affect health actions. This model allows prediction of overall health promotion systems and specific behaviors in diverse and vulnerable populations to examine evidence-based practice.11 There are background factors that influence health-promoting behaviors that can be assessed by the nurse and are critical points for nursing intervention to assist individuals in changing behavior to achieve a healthy lifestyle,11 at different stages of life and generate a positive impact at the health level.
The MPS allows the assessment of lifestyle that can provide valuable information to develop interventions with counseling strategies to help people change negative behavior or adopt a new healthy behavior.11 Universities are ideal settings to implement health promotion programs, through behavioral interventions, considering that healthy behaviors contribute to maintain an adequate physical and mental balance reflected in an optimal quality of life, fulfillment of personal goals and capabilities to carry out multiple activities in a proactive manner.12 Therefore, universities have the responsibility to implement programs that motivate students to be more responsible for their own health,5 promote a healthy lifestyle and periodic evaluation.8
Therefore, the purpose of this study was to determine the effectiveness of the intervention interpersonal influences exercised by health professionals to increase the commitment to adopt health-promoting behavior in nursing students, compared to the care provided by the conventional university wellness program.
Materials and Methods
Design and Setting
A quasi-experimental study was conducted with two groups (control and experimental). Pre-test and post-test measurements were performed on undergraduate nursing students at a university in Cali, Colombia, from September to October 2022. Due to contextual limitations, it was not possible to randomly assign participants to groups, which prevented the experimental design.
Study Sample
The sample size was calculated using Software Stata 17 following the procedure of comparing means of two groups of independent samples and the variability of these differences.13
The sample consisted of 136 senior nursing students. Based on the results of the pilot test, the sample for the experiment was calculated, taking into account the comparison of groups of independent samples with a sample size of n=57 subjects per group, according to the following statistical parameters: a delta or expected difference of 4.7 between both groups, a power of 95%, an alpha type error of 5%, a standard deviation in the scores of 7.5 and a loss adjustment of 30%. The participants were selected by non-probability sampling, by convenience, considering the following inclusion criteria: (1) nursing students of students of the last year of their degree, (2) voluntary participation. Excluded were (1) students with health problems that preclude physical activity (2) pregnant women (Figure 1).
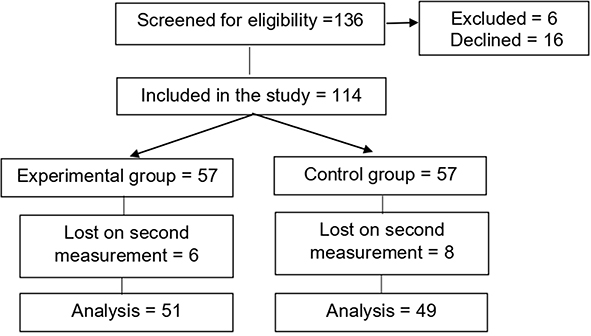 |
Figure 1 Selection and retention of study participants. |
The effectiveness of the intervention was evaluated by posing the following hypotheses:
H1. The commitment to adopt post-intervention health-promoting behavior in participants in the experimental group is significantly higher than that of participants in the control group receiving conventional care. H2. Commitment to adopt post-intervention health-promoting behavior in participants in the experimental group is more likely to be maintained over time than in participants in the control group receiving conventional care.
Intervention
The experimental group received the interpersonal influence intervention exerted by health professionals to increase the commitment to adopt a health-promoting behavior, which was designed and validated using a methodological study that followed the four phases proposed by Sidani and Braden.14 The theoretical reference framework was Nola Pender’s HPM, whose differential elements emerged from the theoretical propositions. Those selected for the intervention were as follows: 1) “health professionals are important sources of interpersonal influence that can increase or decrease the commitment to adopt a health-promoting behavior” and 2) “the greater the commitment to a specific action plan, the more likely it is that health-promoting behaviors will be maintained over time”.
The active components of the intervention correspond to the six dimensions of the HPLP-II instrument that influence health-promoting behavior: diet, physical activity, spiritual growth, interpersonal relationships, stress management, and responsibility for health. These are supported by scientific evidence to strengthen the content validity of the intervention and ensure logical consistency with the current state of knowledge. Based on the review and critique of the scientific evidence supporting the predictive capacity of the HPM, the content of the intervention protocol was defined, with the following active ingredients: cognitive (understanding the current situation and the importance of a healthy lifestyle), behavioral (developing skills to make commitments to adopt health-promoting behaviors), and motivational (active participation in a specific action plan to adopt health-promoting behaviors).
In order to define the content of the study protocol, three experts conducted an assessment to determine the theoretical fidelity of the intervention based on the analysis of the coherence between the concepts and propositions of N. Pender’s HPM and the active ingredients of the interpersonal influence intervention exerted by health professionals to increase the commitment to adopt a health-promoting behavior. The assessment was satisfactory, with a compliance rate of 90%. The intervention protocol was refined based on the experts’ observations. Interventionists were trained to ensure that the intervention was delivered according to the study protocol. The intervention involved participants developing an action plan under the interpersonal influence of the health professionals delivering the intervention and making a commitment to themselves. At each session, participants’ motivation and the cognitive and behavioral skills taught in the intervention were assessed through self-reported measurements of goal attainment to provide feedback about the proposed objectives. The components of the intervention protocol are summarized in Table 1.
 |
Table 1 Components of the Intervention Protocol |
The control group received conventional care offered by the wellness program of the university where the study was conducted. This program is characterized by health welfare benefits through medical services, including health promotion and disease prevention activities; sports and recreational activities through programs that aim to contribute to comprehensive training and maintenance of life quality by organizing events that integrate the university community through formative, recreational, and competitive sports in different sport disciplines; and psychological counseling, which provides support for mental health care to prevent anxiety and stress. Students are monitored by a team of professionals consisting of a general practitioner, a nurse, a sports medicine physician, and a psychologist. Students receive counseling as needed.
Study Instruments
Personal Factors Questionnaire
A questionnaire developed by the researchers based on the HPM, where personal characteristics include important relationships with health behavior in the target population, such as age, body mass index, race, ethnicity, education, and socioeconomic status.
Health-Promoting Lifestyle Profile-II (HPLP-II)
The HPLP-II Spanish version questionnaire was administered to participants in the control group and the experimental group at the beginning and end of the study. The HPLP-II Spanish version is considered valid and reliable. It consisted of 52 items grouped into six subscales: 1) responsibility for health involves an active sense of responsibility for one’s well-being, 2) physical activity assesses regular participation in light, moderate, and/or vigorous activities, 3) nutrition assesses the consumption of foods essential for health and well-being, 4) growth assesses internal resources, 5) interpersonal relationships assess the use of communication to achieve a sense of intimacy and closeness within meaningful relationships, and 6) stress management assesses the identification and mobilization of resources to effectively control or reduce stress. The items are answered on a Likert scale with four response options from 1 to 4: never = 1, sometimes = 2, often = 3, and regularly = 4. The overall and subscale scores are obtained by calculating the mean of the responses to the items.15
Before applying the Spanish version of the HPLP-II to the study sample (n = 763), validity and reliability tests were performed on a sample of the local population of university students, yielding goodness-of-fit indices that demonstrate validity (χ2 = 7168.98; gl = 1268; p < 0.001; RMSEA = 0.08; NFI, NFI, and AGFI = 0.95) and overall reliability (Cronbach’s alpha, 0.94) and by the six subscales the HPLP-II (Cronbach’s alpha, 0.68–0.89).
Internal Validity of the Study
The following control mechanisms were used to ensure the internal validity of the study: implementation of a control group design with pre- and post-test measurements, calculation of a 30% attrition rate, use of a valid and reliable pre- and post-test measurement instrument, training of two research assistants to collect data according to the inclusion and exclusion criteria, monitoring of changes in routine care such as training sessions with similar components to the intervention protocol, and blinding of the research assistants who collected the data. A placebo or Hawthorne effect was difficult to control for, as participants were ethically informed of the intervention they were to receive.
External Validity of the Study
For the external validity of the study, the following control mechanisms were used: design and validation of the intervention protocol, maintenance of fidelity to the intervention protocol, measurements of fidelity in the implementation of the intervention protocol, and no participation of researchers in data collection.
Data Analysis
Comparison of groups was performed under baseline conditions to examine the equivalence of the groups at the beginning of the study according to the variables of interest, applying univariate techniques (Shapiro–Wilk test) to verify the data normality assumption (p ≥ 0.05) and bivariate techniques to evaluate the hypothesis of independence between groups (Pearson’s Chi-square test [χ2] and Fisher’s exact test for the cases in which expected frequencies <5 were obtained). To demonstrate the homogeneity of the study groups, the Student’s t-test for independent samples or the Mann–Whitney U-test was used to compare means if the normality assumption was not met (p ≥ 0.05). Similarly, the study groups in terms of the means of the scores obtained in the global HPLP-II and the six subscales were compared. A multivariate analysis was used to control for possible confounding variables (logistic regression).
To evaluate the effect of the intervention, the means of the responses to the items of the HPLP-II subscales were compared by taking into consideration the significant bilateral p-value (p < 0.05). Effect size (ES) measurements were calculated using Cohen’s d, considering a null effect < 0.20; 0.20 ≤ small ES < 0.50; 0.50 ≤ medium ES < 0.80; and large ES ≥ 0.80.10 In the case where the Student’s t-test and the probability of superiority measure were applied, the following was considered when applying the Mann–Whitney U-test: null effect < 0.56; 0.56 ≤ small ES < 0.64; 0.64 ≤ medium ES < 0.71; and large ES ≥ 0.71.11 Lastly, an analysis of the effect of the possible confounding variables on the intervention was conducted (analysis of covariance, ANCOVA, and partial eta-squared ( ) ES (null effect < 0.01; 0.01 ≤ small ES < 0.06; 0.06 ≤ medium ES < 0.14; large ES ≥ 0.14).10 All statistical analyses were performed using IBM SPSS version 22 statistical software.
) ES (null effect < 0.01; 0.01 ≤ small ES < 0.06; 0.06 ≤ medium ES < 0.14; large ES ≥ 0.14).10 All statistical analyses were performed using IBM SPSS version 22 statistical software.
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki16 for health research involving human subjects, international ethical guidelines,17 and national ethical guidelines.18 The study was approved by the ethics committee of the Universidad Santiago de Cali (2020–2606, record No. 1). Permission was obtained from the author of the HPLP-II scale, and informed consent was obtained from each participant before data collection, guaranteeing anonymity, confidentiality, privacy, autonomy, fairness, and reciprocity.
Results
Sample Characteristics
A total of 100 students participated in the study: 49 in the control group and 51 in the experimental group. The majority of the participants were female, belonged to middle or low socioeconomic levels, and identified themselves as mestizos according to their culture. Half of them had a healthy weight (Table 2). The variables of interest were evenly distributed. No significant differences (p > 0.05) were found between the means of quantitative variables and in the test of independence of the categorical variables with the groups studied, nor were there any significant differences (p > 0.05) between the groups in the subscale scores of the HPLP-II, which calculates the mean of the subscale item responses. Therefore, it can be concluded that the control and experimental groups were equivalent at the beginning of the study (Table 3).
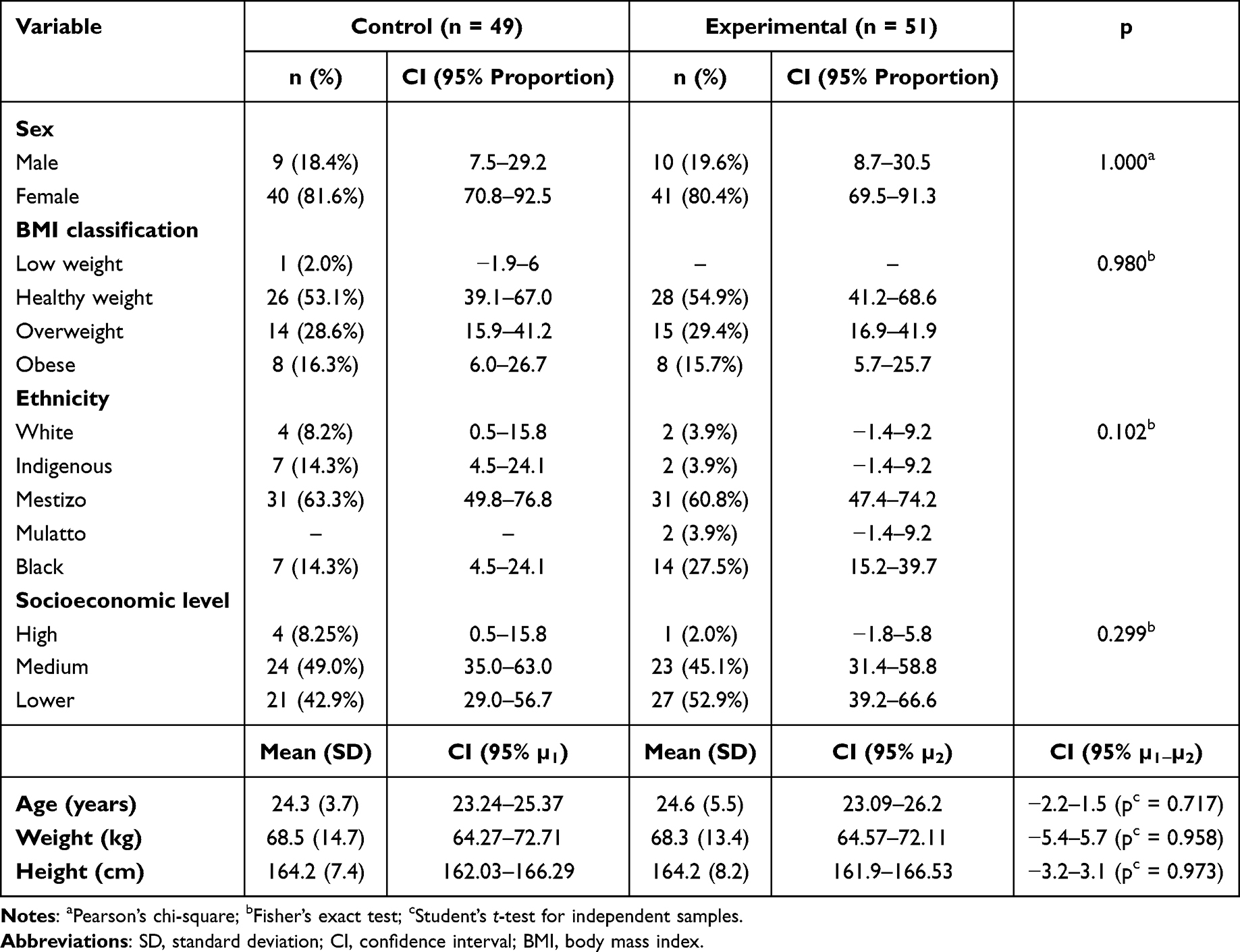 |
Table 2 Characteristics of Nursing Students at Baseline |
 |
Table 3 Health-Promoting Lifestyle Profile- II Subscale Scores at the Start of the Study |
Commitment to Adopt Health-Promoting Behavior at the Beginning of the Study
Given that the HPLP-II items are answered on a Likert scale from 1 to 4 (never = 1, sometimes = 2, often = 3, and regularly = 4) and that the subscale scores are obtained by calculating the mean of the responses to the subscale items, a mean score ≥3 indicates that the participant is committed to adopting a health-promoting behavior (Hypothesis 1), and when the mean score is close to 4, the greater the commitment to an action plan, the more likely it is that health-promoting behaviors will be maintained over time (Hypothesis 2). At baseline, 15% of participants were committed to a health-promoting behavior, whereas 85% were not. No statistical differences were found between the groups (p = 0.6339).
Logistic Regression Analysis
Considering the above and to determine the factors that explained the variability, a binary logistic regression model was designed. The variables measured were age, weight (in kg), height (in cm), sex, BMI classification, ethnicity, and socioeconomic level (Table 4). When evaluating the individual effect (OR) of the possible factors that affect commitment to adopt health-promoting behavior, values of OR<1 were obtained, in the BMI classification underweight, in the control group, in the low and medium socioeconomic level, such that compared to the reference categories, an individual with these characteristics is less likely to increase the commitment to adopt health-promoting behavior, and in the weight variable (OR= 0.992) it is inferred that the lower the weight, the lower the probability of increasing the commitment to adopt health-promoting behavior.
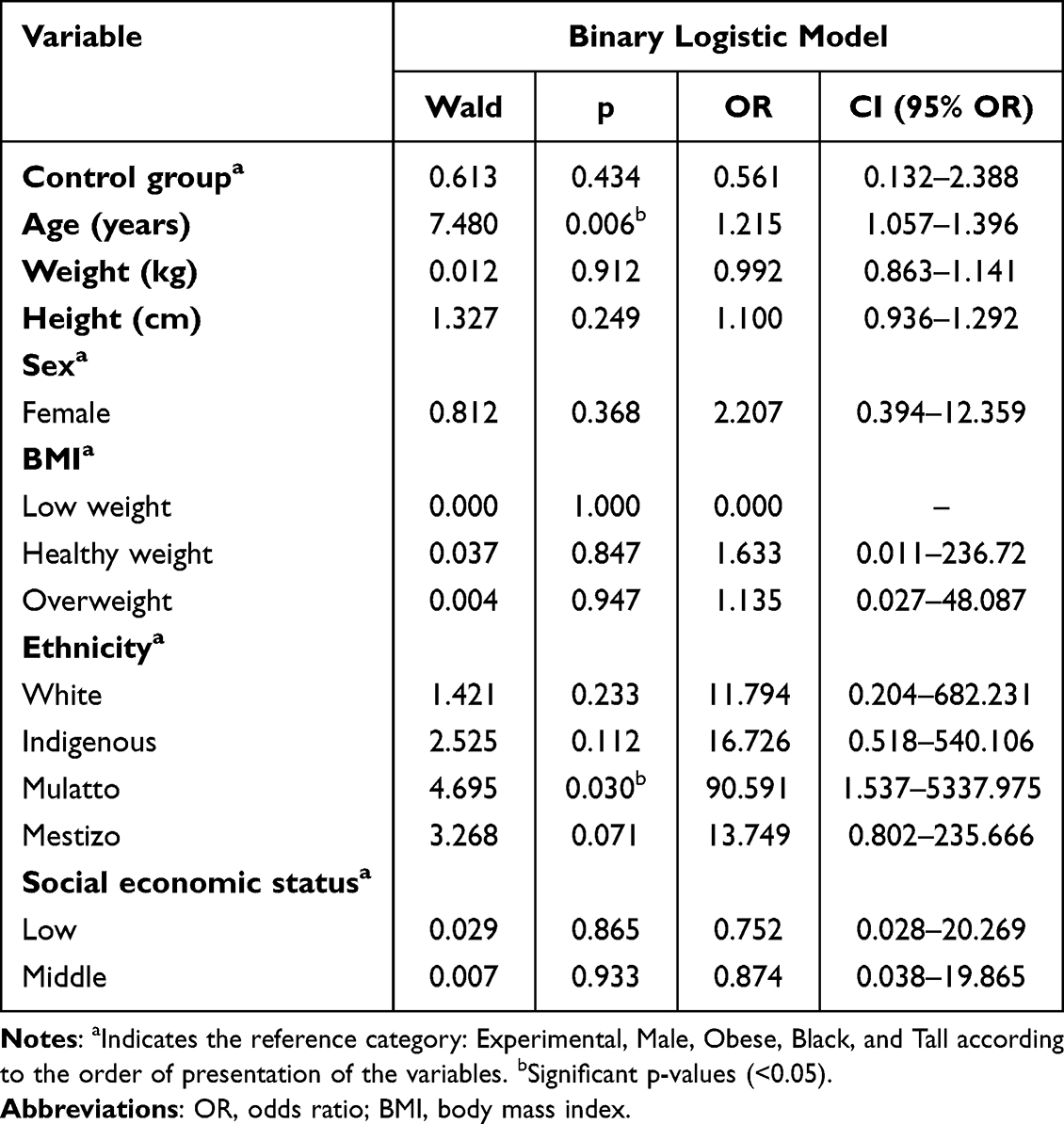 |
Table 4 Individual and Joint Effect of Factors Affecting the Health-Promoting Lifestyle Profile- II Scores of Nursing Students at the Beginning of the Study |
On the other hand, OR>1 values were estimated in the classification of BMI overweight and healthy weight, in the female sex, white, mestizo, indigenous and mulatto ethnic groups, so that compared to the reference categories, an individual with these characteristics has a greater probability of increasing the commitment to adopt health-promoting behavior. For the height and age variables, it is inferred that, as their values increase, the greater the probability that the individual will increase the commitment to adopt health-promoting behavior. However, it was found that only age and mulatto ethnicity registered significant Wald statistics (p<0.05), giving statistical significance to the individual effect; in the other cases it was observed that the 95% confidence interval for the ORs contains unity, indicating that there is no association between the factors considered and the commitment to adopt health-promoting behavior.
In this sense, age has a risk effect (OR > 1) such that participants with an age similar to the characteristic of the study population are 1.215 more likely to increase their commitment to adopt health-promoting behavior. According to the Nagelkerke coefficient of determination, the variables mentioned above explain the variability in the outcome by 31.3% (R2 = 0.313).
Commitment to Adopt Health-Promoting Behavior at the End of the Study
When comparing the total score by groups at the beginning and end of the study, statistical differences were found: in the control group, the median was 2.6 and the IQR was 0.7, with 50% of the scores being between 2.2 and 2.9 points; and in the experimental group, the median was 2.9 and the IQR was 0.7, with 50% of the scores being between 2.4 and 3.1 points.
When comparing HPLP-II scores at the beginning and end of the study within groups, significant differences were found: the estimated difference in the experimental group (p = 0.0001; difference = −0.317, 95% CI µbaseline–µend: −0.475–−0.161) was greater than that of the control group (p = 0.03519; difference = −0.088, 95% CI µbaseline−µend: −0.170–−0.006). Regarding the comparisons of the HPLP-II score at the end of the study between groups, significant differences were found (p = 0.015; 95% CI: −0.42, −0.05); The negative interval indicated that, on average, the scores of the experimental group were higher than those of the control group.
The effect size of the intervention was 0.49. In terms of dimension, significant differences were observed in physical activity (p = 0.002), nutrition (p = 0.002), and stress management (p = 0.002), with the experimental group scoring higher on average than the control group. The effect size scores for the physical activity dimension (0.63) and diet (0.65) were medium, while the stress management dimension (0.32) scores were low (Table 5). No significant differences were found in the scores for the dimensions of health responsibility (p = 0.070), spiritual growth (p = 0.871), and interpersonal relationships (p = 0.392). However, in terms of the effect size of the intervention, there was a greater impact on the spiritual growth dimension (0.49), followed by health responsibility (0.37), while the effect on interpersonal relationships was not significant (0.17).
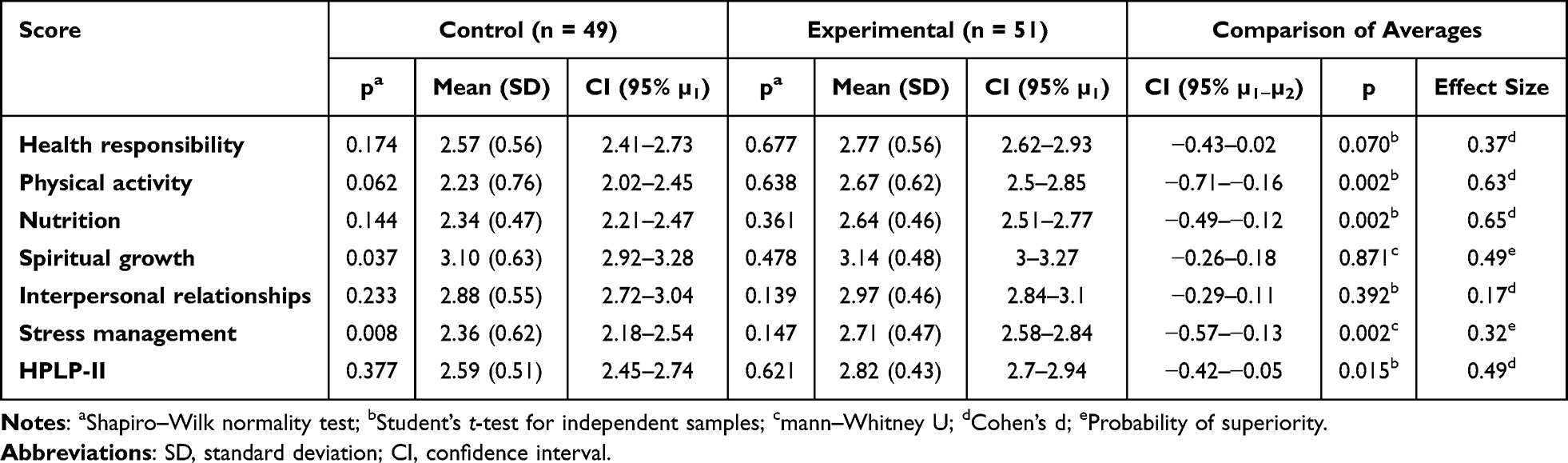 |
Table 5 Health-Promoting Lifestyle Profile- II Subscale Scores at the End of the Study |
Logistic Regression Analysis
Table 6 shows the individual and joint effect of the factors affecting lifestyle (HPLP- II) of the participants after the intervention; it was identified that receiving the intervention was independently associated with the opportunity for commitment to adopt health-promoting behavior (p=0.612, not significant), with evidence that age is a significant risk factor (OR=1.150) for the decision to commit to increasing health-promoting behavior (p=0.010). By dimensions, intervention was significant as a factor explaining variability in stress management (p=<0.001). Age as a factor of variability in dimension scores was significant in health responsibility (p=0.004), physical activity (p=0.002) and nutrition (p=<0.001).
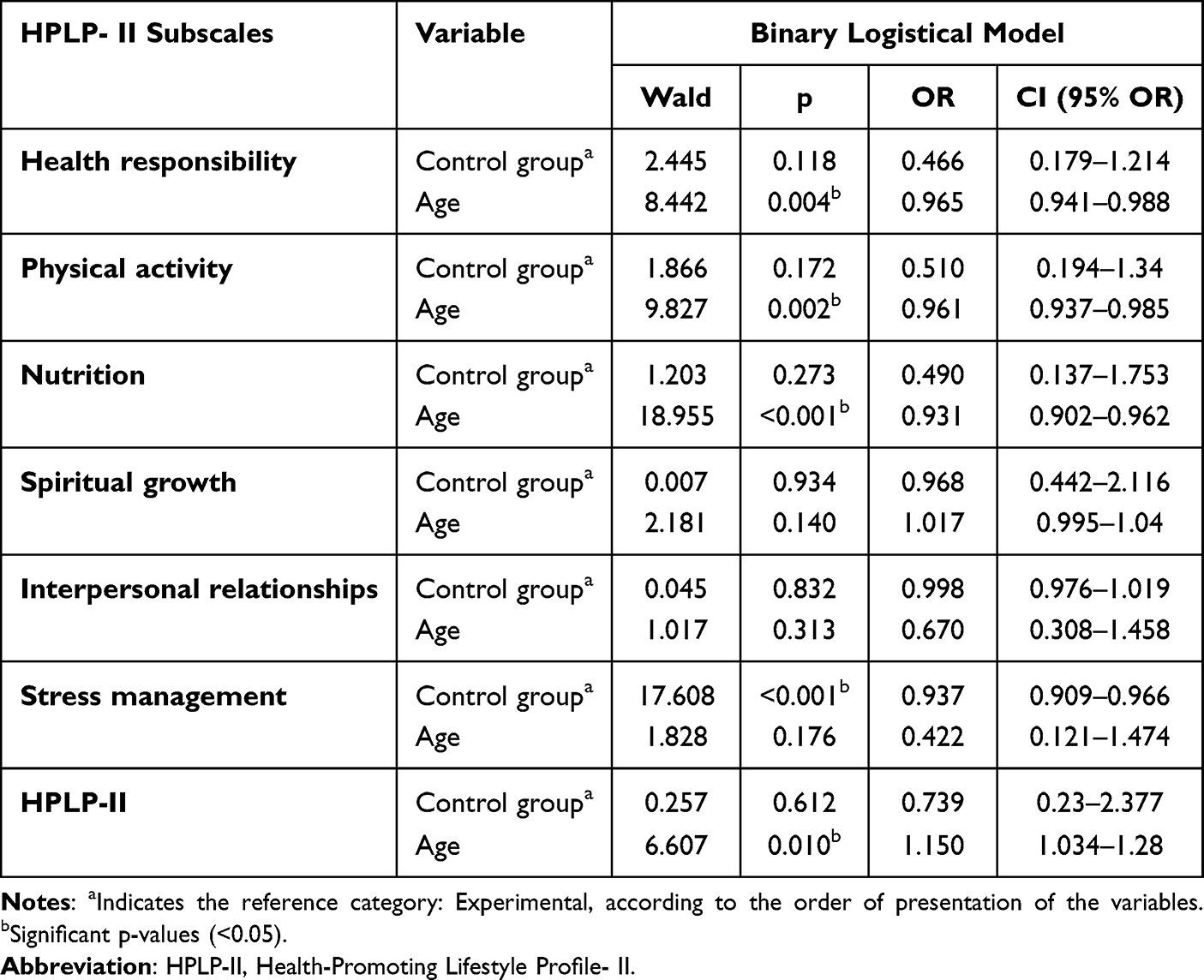 |
Table 6 Individual and Joint Effect of Factors Affecting Commitment to Adopt Health-Promoting Behavior (Health-Promoting Lifestyle Profile- II) After the Intervention |
On the other hand, taking the experimental group as a reference, for the control group in each of the dimensions and in the global instrument a value of OR<1 was obtained, this being indicative that an individual without access to the intervention has a lower probability of increasing the commitment to adopt health-promoting behavior. Likewise, when considering age as a covariate, OR<1 was obtained in the dimensions of health responsibility, physical activity, nutrition, interpersonal relationships and stress management; consequently, the older the individual, the less likely he/she is to increase the commitment to adopt health-promoting behavior in these dimensions. On the contrary, in the spiritual growth dimension (OR>1), the higher the age, the greater the probability that an individual will increase the commitment to adopt health-promoting behavior in this dimension.
Effect of the Intervention on Lifestyle
In order to evaluate the effect of the intervention on the mean final score of the HPLP-II, and of age in the dimensions that contribute variability to it, an analysis of covariance (ANCOVA) was carried out. Table 7 shows that, when comparing and evaluating the effect of the intervention, the ANCOVA evidenced a statistically significant difference in the health responsibility and nutrition dimensions with respect to age as a covariate (p=0.071 and p=0.018, respectively). Similarly, the stress management intervention (p=0.002) is significant, reporting a medium effect size measure (0.094).
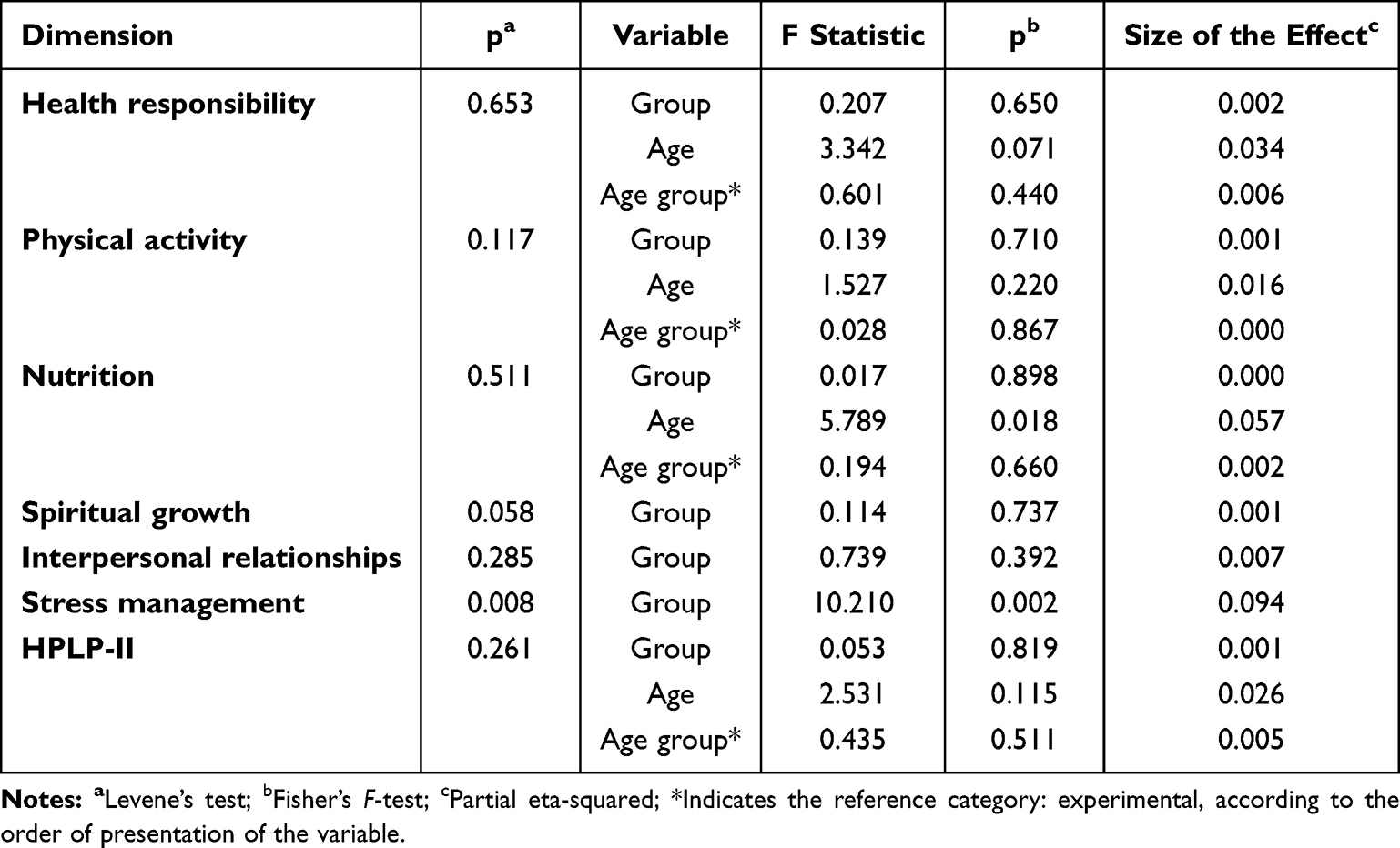 |
Table 7 Analysis of the Effect of the Intervention on Lifestyle (Analysis of Covariance) |
Therefore, the intervention interpersonal influences exerted by health professionals is effective in increasing the commitment to adopt health-promoting behavior in nursing students, compared to the care provided by the conventional university wellness program.
Discussion
The intervention Interpersonal influences exerted by health professionals to increase commitment to adopt health-promoting behavior in nursing students was based on the MPS, the content of the sessions focused on participants developing an action plan and making a commitment to themselves to improve their lifestyle.
According to the MPS,11 the commitment to adopt a health-promoting behavior through an action plan involved the following underlying cognitive processes: (1) commitment to perform a specific action at a specific time and place and with specific people or alone, (2) identification of permanent strategies to provoke, carry out and reinforce behavior with interpersonal influences exercised by professionals in: health nutrition, physical activity, psychology and nursing, to adopt a healthy lifestyle.
The data obtained in this study showed that the age of nursing students correlated with the development of a healthy lifestyle. Similar results were reported in the study by Baykal et al, where age was found to correlate with the nutrition subdimension of the HPLP-II.19 Age as a factor of variability in the post-intervention dimension scores was statistically significant in the physical activity and nutrition dimensions. Another study points out that physical activity and mental health are positively related to the well-being of college students and physical activity interventions can improve perceived stress after a few weeks of intervention improving both psychological and physiological subjective well-being.6 However, there is evidence that at the age at which most young college students are, they do not meet the recommended levels of physical activity.20
This study managed to identify that the ethnic subgroups: white, mestizo, indigenous and mulatto, have a greater probability of increasing the commitment to adopt a health-promoting behavior by improving their lifestyle. Other studies demonstrate similar results, where the prevalence of lifestyle risk factors among young adults varies substantially by race and ethnicity.21–23 The unique patterns of racial and ethnic disparities occur due to a wide range of experiences and ongoing changes in many domains of life at this stage.23
On the other hand, this study found that overweight individuals are more likely to increase their commitment to adopt health-promoting behaviors (OR>1). By dimensions of the HPLP-II, significant differences were observed between the groups in physical activity (p=0.002), nutrition (p=0.002). According to the evidence, there is a positive association between health education of college students and lifestyle behaviors.24 A better understanding of eating habits and overweight/obesity in college students supports the development of programs to promote healthy lifestyles in this population.7,11,25 In this regard, Aljefree et al recommend that in order to reduce obesity among students, universities should guarantee access to healthy snacks and provide health education programs that promote healthy eating habits and lifestyles.26
By dimensions of the HPLP-II the intervention was also significant as a factor explaining variability in nutrition (p=<0.0001) and stress management (p=<0.0001). According to Nogueira et al, a higher level of anxiety is associated with anthropometric indicators among college students, specifically for overweight or obesity. Therefore, effective ways to overcome overweight may depend, in part, on the ability to identify mood disorders and their association with overeating and weight gain.27 Likewise, Choi et al consider that adequate nutritional education and stress management intervention measures are necessary for proper eating behavior and better lifestyle, considering that stress is positively correlated with emotional eating behavior.28
Interpersonal influences exerted by health professionals (nutrition, physical activity, psychology, and nursing) to increase commitment to health-promoting behavior in nursing students is effective in a short period. Similar studies have also shown that interventions to improve lifestyles have been effective in achieving behavior change in a short time in the educational setting, both in high school students29,30 and college students.31 According to Kim et al, combined interventions are considered necessary, which means, interventions that simultaneously intervene physical activity, nutrition, and stress management for effective health management.32
According to the MPS,11 the commitment without associated strategies frequently results in good intentions but fails to perform health behavior. Therefore, the commitment to adopt a health-promoting behavior supported by a team of health professionals is stronger if it is complemented by why and how the commitment will be made that drives the individual to action, thereby increasing the likelihood that the action plan will be successfully implemented.
This study demonstrates the practical usefulness of the MPS as a theoretical basis for designing and testing interventions to increase the commitment to adopt health-promoting behavior through interdisciplinary actions and proves its power to explain the relationships among the factors believed to influence the commitment to adopt health-promoting behavior. However, further studies are needed to determine the effectiveness of the intervention in the medium and long term, considering other variables such as personal influences, preferences, and immediate competing demands.
Conclusion
The MPS allowed the articulation of different disciplines (nursing, psychology, nutrition, physical education), through combined interventions, to increase commitment to an action plan, helping nursing students to have a planned strategy to achieve health-promoting behavior which is understood as a motivated behavior aimed at positive health outcomes driven by the desire to increase optimal well-being.
The effectiveness of the interpersonal influence’s intervention implemented by health professionals to increase the commitment to adopt health-promoting behavior is demonstrated. Evidence indicating the practical utility of the Health Promotion Model for developing and testing interventions focused on mechanisms of change to adopt new health-promoting behavior.
Acknowledgments
The authors wish to acknowledge the cooperation of the health sciences students and their participation in this study.
Funding
This research was supported by the project “Fortalecimiento grupo de investigación cuidado de la Salud”, grant No. 441-62122-3507, funded by Dirección General de Investigaciones of Universidad Santiago de Cali.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sánchez-Ojeda MA, Luna-Bertos ED. Healthy lifestyles of the university population. Nutrición hospitalaria. 2015;31(5):1910–1919. doi:10.3305/nh.2015.31.5.8608
2. Orcasita LT, Gil JAM, González TC. Self-concept, self-efficacy and risky sexual behaviors in adolescents. Psychological Reports. 2018;18(2):141–168. doi:10.18566/infpsic.v18n2a08
3. World Health Organization. [Press release]; 2019. https://www.who.int/es/news/item/22-11-2019-new-who-led-study-says-majority-of-adolescents-worldwide-are-not-sufficiently-physically-active-putting-their-current-and-future-health-at-risk.
4. World health organization. Obesity and overweight. [Descriptive notes]; 2021. Descriptive notes: https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight.
5. Almutairi KM, Alonazi WB, Vinluan JM, et al. Health promoting lifestyle of university students in Saudi Arabia: a cross-sectional assessment. BMC Public Health. 2018;18(1):1093. doi:10.1186/s12889-018-5999-z
6. Herbert C. Enhancing mental health, well-being and active lifestyles of university students by means of physical activity and exercise research programs. Front Public Health. 2022;10:849093. doi:10.3389/fpubh.2022.849093
7. Suwalska J, Kolasińska K, Łojko D, et al. Eating behaviors, depressive symptoms and lifestyle in university students in Poland. Nutrients. 2022;14(5):1106. doi:10.3390/nu14051106
8. Rodríguez M, Carmona T, Rivera-Picón C, et al. Risky behaviours of Spanish university students: association with Mediterranean diet, sexual attitude and chronotype. Nutrients. 2021;13(11):4042. doi:10.3390/nu13114042
9. World health organization. Noncommunicable diseases. [Press Center]; 2022. https://www.who.int/es/news-room/fact-sheets/detail/noncommunicable-diseases.
10. Farokhzadian J, Karami A, Azizzadeh Forouzi M. Health-promoting behaviors in nursing students: is it related to self-efficacy for health practices and academic achievement? Int J Adolesc Med Health. 2018;32(3). doi:10.1515/ijamh-2017-0148
11. Pender NJ, Murdaugh CL, Parsons MA. Health Promotion in Nursing Practice.
12. Aristizábal Hoyos GP, Blanco Borjas DM, Sánchez Ramos A, Ostiguín Meléndez RM. Nola Pender’s model of health promotion: A reflection on its understanding. Enferm. University. 2011;8(4):16–23.
13. Marrugat J, Vila J, Pavesi M, et al. Sample size estimation in clinical and epidemiologic research. Med Clin. 1998;111:267–276.
14. Sidani S, Braden CJ. Design, Evaluation, and Translation of Nursing Interventions. Nueva Jersey: John Wiley & Sons; 2011. Online ISBN:9781118785553. doi:10.1002/9781118785553
15. Serrano-Fernández M, Boada-Grau J, Vigil-Colet A, Gil-Ripoll C. Spanish adaptation of the HPLP-II scale with a sample of employees. Univ Psychol. 2016;15(4):1–14. doi:10.11144/Javeriana.upsy15-4.aeem29
16. Asociación medica mundial. Declaración de Helsinki de la AMM – principios éticos para las investigaciones médicas en seres humanos. Available from: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/.
17. Organización Panamericana de la Salud y Consejo de Organizaciones Internacionales de las Ciencias Médica. Pautas éticas internacionales para la investigación relacionada con la salud con seres humanos.
18. Ministry of Health of Colombia. Scientific, technical and administrative standards for health administration; 1993. Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF.
19. Baykal D, Kutlu L, Demir BD. The correlation between nursing students’ healthy lifestyle behaviors, cardiovascular disease risk factors’ knowledge level, and obsession symptoms. J Educ Health Promot. 2022;11(1):281. doi:10.4103/jehp.jehp_902_21
20. Keating XD, Guan J, Piñero JC, Bridges DM. A meta-analysis of college students’ physical activity behaviors. J Am Coll Salud. 2005;54(2):116–126. doi:10.3200/JACH.54.2.116-126
21. Wang L, Li X, Wang Z. Trends in prevalence of diabetes and control of risk factors in diabetes among US adults, 1999–2018. JAMA. 2021;326(8):704–716. doi:10.1001/jama.2021.9883
22. He J, Zhu Z, Bundy JD, Dorans KS, Chen J, Hamm LL. Trends in cardiovascular risk factors in US adults by race and ethnicity and socioeconomic status, 1999–2018. JAMA. 2021;326(13):1286–1298. doi:10.1001/jama.2021.15187
23. Shi S, Huang H, Huang Y, Zhong VW, Feng N. Lifestyle behaviors and cardiometabolic diseases by race and ethnicity and social risk factors among US young adults, 2011 to 2018. J Am Heart Assoc. 2023;12(17). doi:10.1161/JAHA.122.028926
24. Tian H, Chen J. The association and intervention effect between eHealth literacy and lifestyle behaviors among Chinese university students. Revista da Escola de Enfermagem da U S P. 2022;56:e20220147. doi:10.1590/1980-220X-REEUSP-2022-0147
25. Al-Qahtani AM. Lifestyle habits among Najran University students, Najran, Saudi Arabia. Front Public Health. 2022;10:938062. doi:10.3389/fpubh.2022.938062
26. Aljefree NM, Shatwan IM, Almoraie NM. Impact of the intake of snacks and lifestyle behaviors on obesity among university students living in Jeddah, Saudi Arabia. Healthcare. 2022;10(2):400. doi:10.3390/healthcare10020400
27. Nogueira M, de Assis B, Ferreira C, et al. Is level of anxiety associated with overweight and obesity risk in university students? The NUTSAU Study. Nutr. Hosp. 2021;38(3):488–494. doi:10.20960/nh.03376
28. Choi O, Kim J, Lee Y, et al. Association between stress and dietary habits, emotional eating behavior and insomnia of middle-aged men and women in Seoul and Gyeonggi. Nutr Res Pract. 2021;15(2):225–234. doi:10.4162/nrp.2021.15.2.225
29. Sabio J, Correas Bodas A, Giménez N. Promotion of healthy eating habits in adolescents from primary care. Med Fam Semer. 2016;42(5):349–350. doi:10.1016/j.semerg.2015.08.002
30. Pareja S, Roura C, Milà-Villarroel R, et al. Estudio y promoción de hábitos alimentarios saludables y de actividad física entre los adolescentes españoles: programa TAS (tú y Alicia por la salud). Nutrición Hospitalaria. 2018;35(spe4):121–129. doi:10.20960/nh.2137
31. Pérez L, Rivera G, Delgado F. Improvement of healthy lifestyle habits in university students through a gamification proposal. Nutr Hosp. 2017;34(4):942–951. doi:10.20960/nh.669
32. Kim J, Choi O, Lee Y, et al. A comparison on health-related lifestyle, dietary habits, and depression by exercise frequency of college students. Nutr Res Pract. 2021;15(3):355–366. doi:10.4162/nrp.2021.15.3.355
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influence of Personal Factors on Health-Promoting Behavior in College Students: A Structural Equation Modeling Approach
Zambrano Bermeo RN, Estrada Gonzalez C, Guerra EDPH
Journal of Multidisciplinary Healthcare 2023, 16:1259-1270
Published Date: 5 May 2023
Health-Promoting Lifestyle and Its Predictors in Renal Transplant Recipients in Hunan, China: A Cross-Sectional Study
Chen ZL, Ding X, Zhuo L, Li RH, Zhang H
Patient Preference and Adherence 2024, 18:1205-1215
Published Date: 12 June 2024