Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Effectiveness of a Structured 2-Year Diabetes Health Education Program of Patients with Type 2 Diabetes Mellitus in Disease-Related Serum Markers
Authors Hsieh YS ![]() , Lo CL, Lin YY
, Lo CL, Lin YY
Received 27 January 2025
Accepted for publication 27 May 2025
Published 4 June 2025 Volume 2025:18 Pages 1849—1858
DOI https://doi.org/10.2147/DMSO.S519747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Yu-Shan Hsieh,1,2 Chin-Lan Lo,3 Yan-Yu Lin3,4
1School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei City, Taiwan; 2Department of Research, Taipei Medical University Hospital, Taipei City, Taiwan; 3Division of Endocrinology and Metabolism, Department of Internal Medicine, Taipei Medical University Hospital, Taipei City, Taiwan; 4Caringlink Clinic, Taipei City, Taiwan
Correspondence: Yu-Shan Hsieh, School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei City, Taiwan, Email [email protected]
Introduction: Previous studies on the impact of diabetes education on disease management have shown that different educational approaches yield varying degrees of effectiveness across different populations. Adopting face-to-face education with long-term follow-up not only allows for monitoring changes in numerical values but also facilitates the observation of patients’ learning status.
Methods: This study investigates the impact of a two-year structured Diabetes Health Education (DHE) program on disease-related serum markers in patients with type 2 diabetes mellitus (T2DM). A five-year observational cohort study with retrospective analysis was conducted, involving 1,080 participants who completed the DHE program and 192 non-participants.
Results: The DHE program included regular educational sessions every three months, covering topics such as blood glucose management, lipid profiles, and healthy lifestyle practices. Results demonstrated significant improvements among DHE participants: HbA1c levels decreased by 37%, fasting glucose by 4%, total cholesterol by 7%, LDL cholesterol by 13%, and triglycerides by 20%, with HDL cholesterol increasing by 3%. Body weight and diastolic blood pressure (DBP) also showed reductions of 4% and 3%, respectively, while systolic blood pressure (SBP) exhibited no significant changes. The improvements in lipid profiles were evident within six months, whereas glycemic markers required at least 1.5 years to achieve significance.
Conclusion: These results suggest that a structured DHE program significantly improves glycemic control, lipid profile, and other metabolic-related markers in patients with T2DM. Notably, HbA1c and fasting glucose levels significantly improved after 1.5 years of consistent DHE participation, highlighting the importance of long-term engagement for glycemic benefits.
Keywords: diabetes health education program, type 2 diabetes mellitus, structured 2-years diabetes program
Introduction
Diabetes ranks as the fifth leading cause of death in Taiwan, with a prevalence of 11.8% among adults. This rate has been steadily increasing and is anticipated to rise further. To address this issue, Taiwan launched the “Diabetes Shared Care Network” in 1997, integrating healthcare providers nationwide and adjusting health insurance reimbursements for diabetes management.1 Patients enrolled in this program gain access to various free services at participating institutions, including health education, blood glucose monitoring, blood pressure and lipid profile testing, as well as annual foot and eye examinations. As the aging population continues to expand, the prevalence of diabetes is expected to increase, exacerbating the associated medical and economic burdens.
Lifestyle modification plays a central role in the prevention and management of type 2 diabetes mellitus (T2DM). Numerous studies have demonstrated that structured interventions focusing on diet, physical activity, and behavioral change can significantly reduce the risk of developing T2DM and improve glycemic control in patients with existing disease. For example, the Diabetes Prevention Program (DPP) showed that intensive lifestyle interventions reduced the incidence of T2DM by 58% among high-risk individuals compared to standard care.2 A meta-analysis by Uusitupa et al further confirmed that such interventions are associated with sustained reductions in HbA1c, fasting glucose, and lipid profiles.3 A meta-analysis study demonstrated that long-term lifestyle interventions significantly reduce the progression from prediabetes to T2DM, highlighting the effectiveness of sustained behavioral changes in high-risk populations.4 Additionally, another meta-analysis in 2025 found that combining lifestyle interventions with metformin therapy leads to greater reductions in HbA1c levels and T2DM incidence compared to lifestyle interventions alone, suggesting a synergistic effect between pharmacological and behavioral strategies.5 These findings have led to the widespread implementation of lifestyle-based education programs in clinical settings as an integral part of chronic disease management.
While promoting a healthy lifestyle plays a critical role in preventing and managing diabetes, lifestyle modification counseling is rarely incorporated into existing diabetes care systems. Therefore, research in this area may be vital for informing future practices and improving outcomes.
Previous studies on the impact of diabetes education on disease management have shown that different educational approaches yield varying degrees of effectiveness across different populations. Whether using mobile apps,6 tablet-based applications,7 or self-reporting methods,8 these tools effectively improve participants’ blood glucose control. However, these methods often focus on improving a single or limited number of disease indicators. In contrast, adopting face-to-face education with long-term follow-up not only allows for monitoring changes in numerical values but also facilitates the evaluation of patients’ overall health, awareness, and cognitive changes. This approach significantly aids in the early detection of diabetic complications.
The aim of this study was to evaluate the long-term effects of a structured, two-year diabetes health education (DHE) program on disease-related serum markers, including HbA1c, fasting and postprandial glucose, lipid profiles, and liver function, among patients with type 2 diabetes mellitus in a real-world clinical setting. We hypothesized that patients who received the DHE program would show greater improvements in glycemic control and metabolic indicators over time compared to those who did not participate in the program.
Therefore, a two-year Diabetes Health Education (DHE) program was planned. This program establishes structured educational goals and content. In this study, we compared changes in glycemic, lipid, and blood pressure-related indicators in patients with type 2 diabetes mellitus (T2DM) before and after participating in the DHE. Additionally, we analyzed the differences and changes in these physiological indicators between patients who received DHE and those who did not.
Methods
Study Population and Study Design
This was a 5-year observational cohort study with retrospective analysis, conducted at a regional hospital in Taiwan. The study aimed to evaluate the relationship between participation in a diabetes health education (DHE) program and changes in disease-related serum markers among patients with type 2 diabetes mellitus (T2DM).
Baseline data were collected between January and December 2019. Patients were enrolled in the research cohort during the first half of 2019 (January to June) and began receiving structured DHE interventions in the second half of 2019 (July to December). The DHE program continued through 2023 as part of the hospital’s routine care under the national diabetes shared care program. Participants were not recruited specifically for research purposes; rather, data were retrospectively extracted from patients who had enrolled in the DHE program as part of standard care. Attendance at education sessions was recorded by certified diabetes educators. Each participant was expected to receive a minimum of eight educational contacts across two years, with follow-ups approximately every three months. To evaluate long-term changes, we tracked patients’ metabolic indicators using blood tests conducted every six months over the five-year period (Figure 1).
 |
Figure 1 Process flow for participants enrolled in the Diabetes Health Education program. |
The inclusion criteria for this study were as follows: (1) Adults aged 18 years or older diagnosed with T2DM, capable of understanding, speaking, and writing in Chinese, and willing to provide both verbal and written informed consent; (2) Patients with a T2DM diagnosis classified under ICD-10 codes E10.X-E11.X; and (3) Individuals proficient in Chinese (or Taiwanese) and agreeing to participate through oral and written consent.
Exclusion criteria included: (1) Patients with diabetes types other than T2DM; (2) Those who are pregnant, breastfeeding, or have severe comorbidities with a life expectancy of less than five years, or any condition preventing them from attending or completing the study appointments; and (3) Individuals involved in other research studies that might influence the primary outcomes of the present study.
In this study, blood sugar and metabolic abnormalities during pregnancy may become an obvious confounding variable. In addition, breastfeeding women were excluded because postpartum dietary practices in Taiwan commonly include traditional “confinement meals” (zuo yue zi), which are typically high in fat and protein. These dietary patterns, although culturally important, could significantly alter glucose and lipid metabolism, potentially confounding the primary outcomes of our study.
A total of 1,272 patients who were diagnosed with type 2 diabetes mellitus (T2DM) within the past 90 days and had received care from the same physician at least twice in our hospital were initially identified. All participants provided written informed consent. Among them, 1,080 patients agreed to participate in the Diabetes Health Education (DHE) program and were assigned to the DHE group, while 192 patients declined the DHE intervention but consented to have their data included as the non-DHE group.
Of the 1,080 patients enrolled in the DHE program, 1,018 completed the minimum required follow-up and educational sessions and were included in the final analysis. The remaining 62 patients were excluded due to incomplete follow-up or missing laboratory data. The attrition rate in the DHE group was approximately 5.7% over the two-year follow-up period.
Exposure and Outcome Measures
DHE is a multi-year process. When newly diagnosed diabetes patients agree to join the Diabetes Shared Care Program, the first session takes 30–40 min to explain the upcoming process and emphasize the importance of disease management. The diabetes educator provides a 5–10-minute educational session every three months during the patient’s follow-up visits. Each session covers different topics, extending over 2 years. If participants wished to continue beyond this period, they could choose to remain in the program as part of their follow-up visits (Table 1).
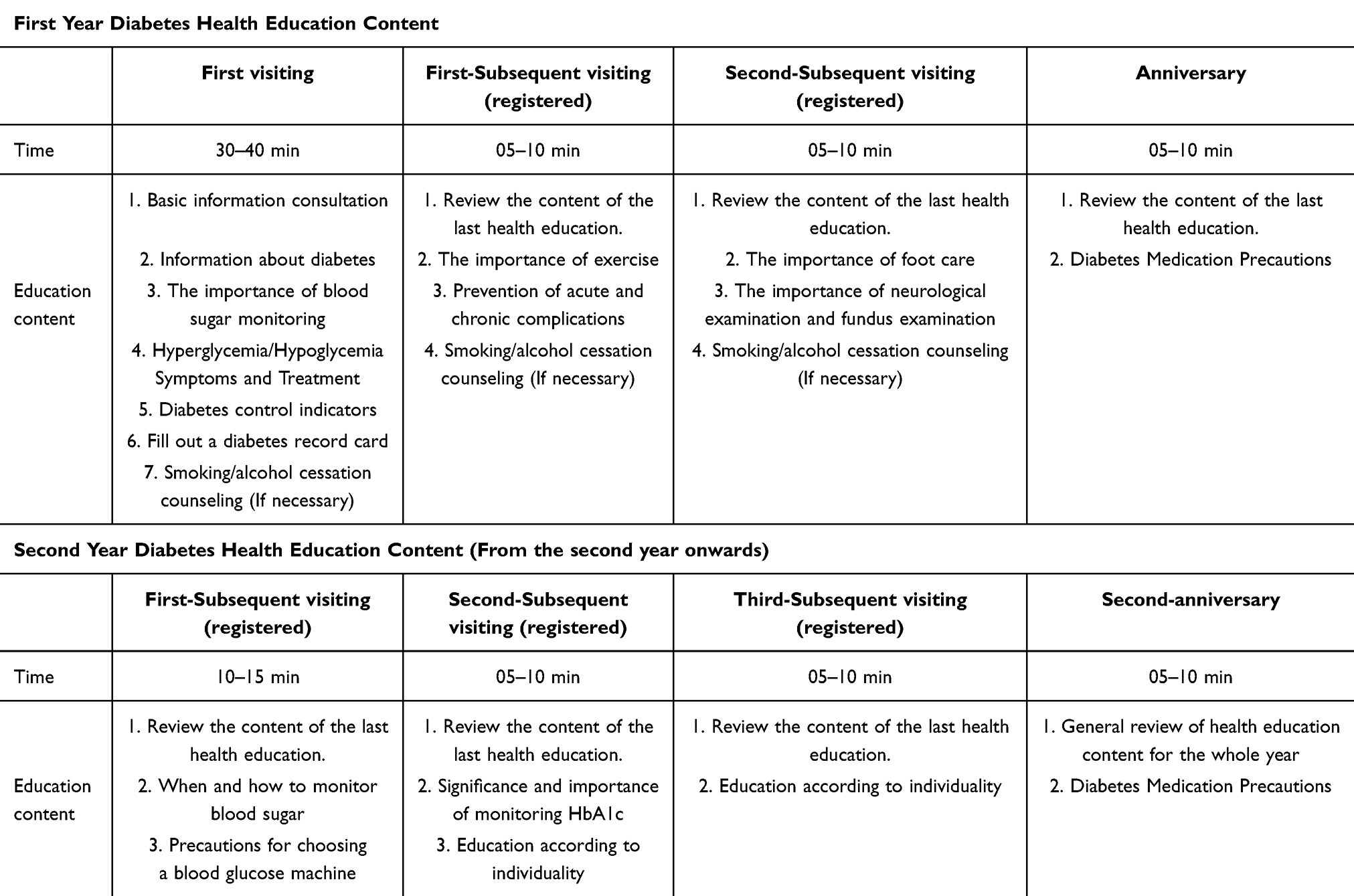 |
Table 1 Schedule for the Diabetes Health Education Program Over 2 years |
Hematologic Analysis
Information about demographics, lipid profile, liver function, and blood pressure status were obtained by our diabetes educators. Patients received examinations for blood pressure, fasting and postprandial glucose glucose (glucose AC/PC), glycated hemoglobin (HbA1c), alanine aminotransferase (ALT), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG) levels.
Fasting glucose (glucose AC) was analyzed according to the hexokinase method (ADVIA Chemistry XPT System, Siemens, Berlin, Germany), and HbA1c was determined by high-performance liquid chromatography using an automatic analyzer (Bio-Rad Variant II Turbo 2.0 System, Hercules, CA, USA). ALT, TC, TG, LDL-C, and HDL-C levels were analyzed by enzymatic methods using an automatic analyzer (ADVIA Chemistry XPT).
In the program, patients undergo metabolic-related serum testing every 3–6 months on average. Accordingly, we conducted a five-year observational cohort study of changes in their serum indicators.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS version 22.0 for Windows (IBM Corp, Armonk, NY, USA). The Chi-square test was used for comparing results of nominal scale. Data distributions were analyzed by the Shapiro–Wilk test for normality. Between-group differences in non-parametric data were analyzed using the Mann–Whitney U-test with the Kruskal–Wallis test with the Dunn post hoc test. The Wilcoxon signed-rank test was used to analyze within-group differences in the paired results of patients. Continuous variables are reported as the mean±standard deviation, whereas categorical variables are presented as count and percentage. A confidence interval of 95% was employed, and p < 0.05 indicated statistical significance.
Results
Characteristics of the Overall Study Population
Clinical characteristics and baseline levels of glucose AC, HbA1c, ALT, and lipid parameters (including TC, LDL-C, HDL-C, and TG) are presented in Table 1. The average age of participants was approximately 65 years, with a majority being male. At baseline, no significant differences were observed between the DHE and non-DHE groups in terms of glycemic or lipid-related markers (Table 1).
Characteristics of the DHE Study Population
Since this group participated in the DHE program, more comprehensive baseline records were available compared to the non-DHE group. Clinical characteristics, including systolic blood pressure (SBP), glycemic indices (glucose AC/PC, HbA1c), liver enzymes, and lipid profiles (TC, LDL-C, HDL-C, and TG), are presented in Table 2. The average participant age was approximately 63 years, and most were male. Overall, baseline metabolic and cardiovascular markers indicated suboptimal glycemic and lipid control, with elevated HbA1c, fasting and postprandial glucose levels, and moderately elevated blood pressure. (Table 2). These findings might reflect the high cardiometabolic risk typically observed in patients newly diagnosed with T2DM in routine care settings.
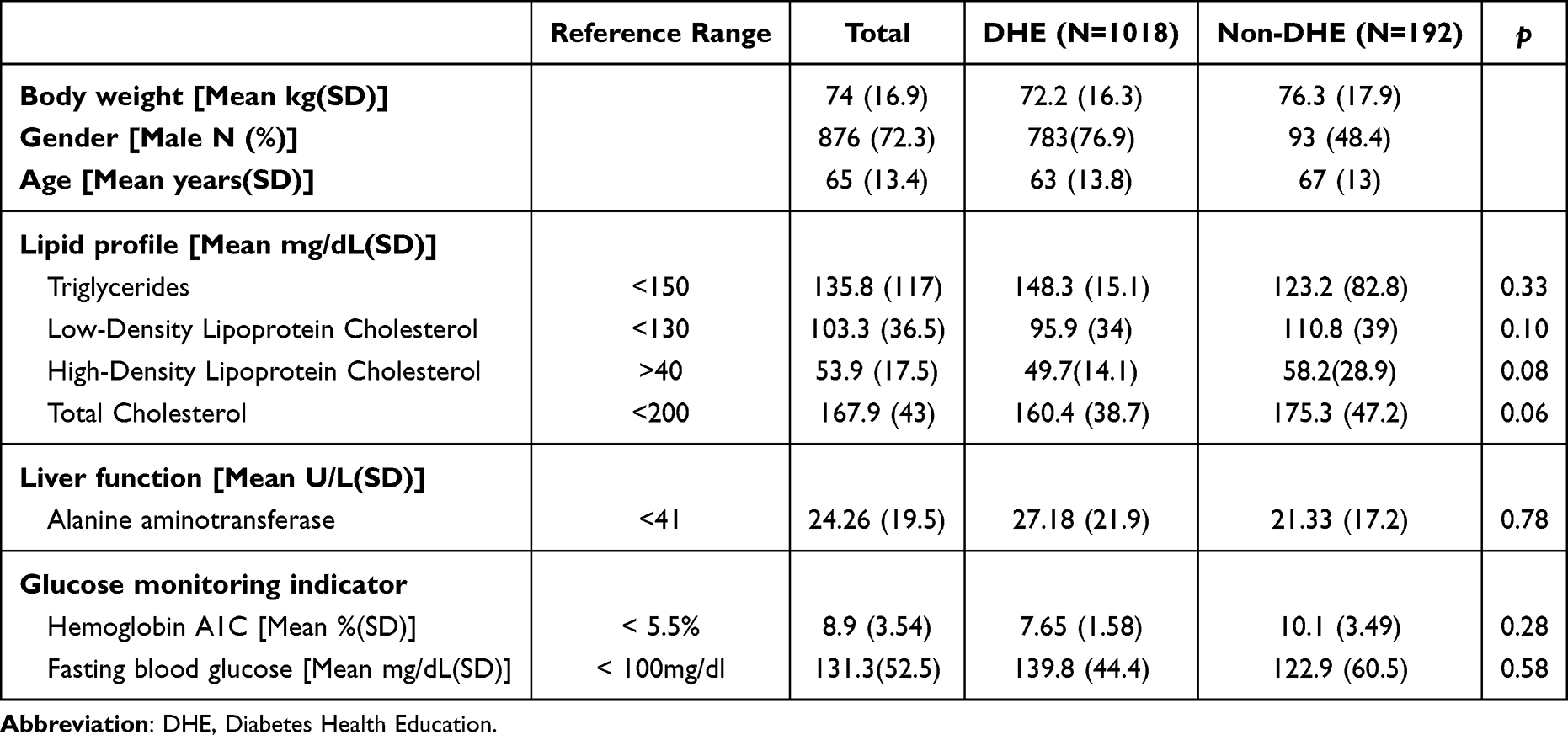 |
Table 2 Baseline Characteristics of the Participants in the Diabetes Health Education (DHE) Program Group and Non-DHE Program Group |
Follow-up Data for the DHE Population After 5 years
To evaluate changes in clinical and metabolic parameters among participants who consistently received DHE interventions, we assessed body weight, blood pressure, glycemic indices (glucose AC/PC, HbA1c), and lipid profiles (TG, TC, LDL-C, HDL-C) every six months over a two-year period. Repeated-measures ANOVA was used to analyze longitudinal trends.
As shown in Figure 2a–c, significant improvements were observed in glycemic control and lipid markers, including reductions in HbA1c, glucose levels, body weight, triglycerides, and LDL-C. HDL-C levels showed a modest increase, while total cholesterol also decreased significantly. Diastolic blood pressure showed a mild but significant reduction, whereas systolic blood pressure remained stable over time (Figure 2a–c).
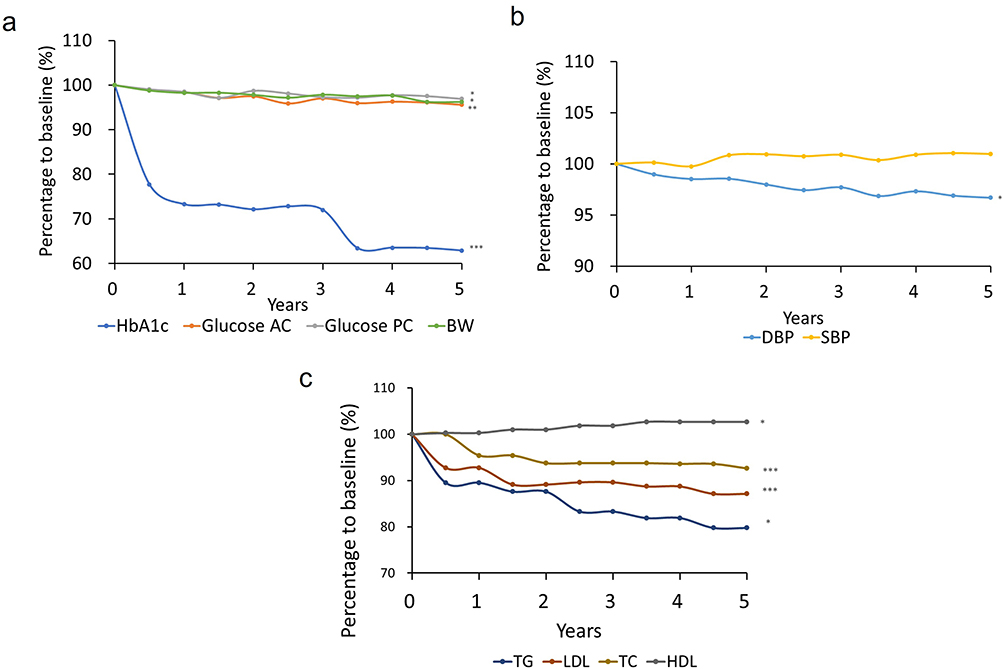 |
Figure 2 Changes from baseline at the 5-year follow-up in (a) glucose AC, glucose PC, and HbA1c, (b) body weight and blood pressure, (c) TC, LDL, HDL, and TG levels among participants who consistently received Diabetes Health Education interventions. *:p<0.05;**:p<0.01;***:p<0.001. Abbreviations: HbA1c, glycated hemoglobin; glucose AC, fasting glucose; glucose PC, Postprandial glucose; BW, body weight; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; TG, triglyceride. |
Between-Group Differences in the Overall Study Population at 5 years of Follow-up
To further examine the effect of the DHE program compared to non-participation, we compared changes in disease-related markers between the DHE and non-DHE groups across multiple time points (Figure 3). Overall, patients in the DHE group showed significantly better outcomes in glycemic control and lipid metabolism compared to the control group.
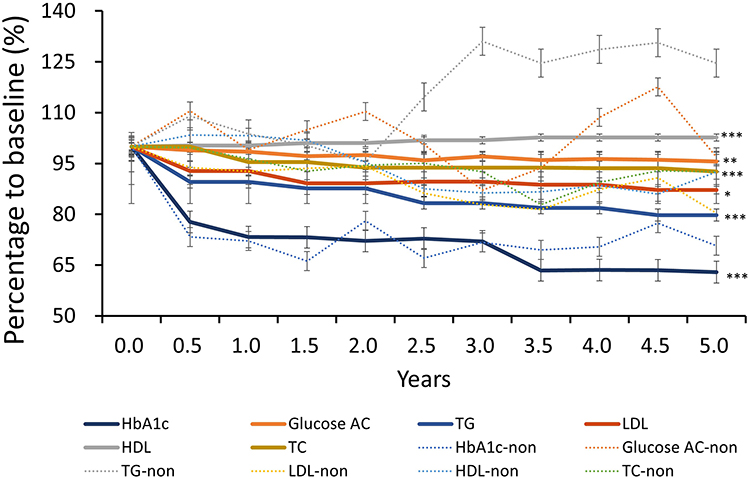 |
Figure 3 Integration of a multidisciplinary team, comprising certified diabetes educators, nurses, nutritionists, doctors, and pharmacists, into Diabetes Health Education improves patient outcomes by optimizing blood glucose levels, HbA1c, lipid profile, and blood pressure. *:p<0.05;**:p<0.01;***:p<0.001. Abbreviations: HbA1c, glycated hemoglobin; glucose AC, fasting glucose; glucose PC, Postprandial glucose; BW, body weight; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol; TG, triglyceride; -non, non-DHE group. |
Specifically, differences in lipid profiles—including TC, LDL-C, HDL-C, and TG—became apparent within the first six months of the program. In contrast, significant improvements in glycemic indices, such as HbA1c and fasting glucose, emerged after approximately 1.5 years of consistent DHE participation (Supplementary Table 1). These findings suggest that lipid-related benefits may manifest earlier than improvements in glucose regulation.
Discussion
For patients with T2DM, the benefits of lifestyle changes on blood glucose and disease control have been well-documented.9 However, how individuals can effectively modify their lifestyles vary significantly, leading to different outcomes. This study introduced a two-year DHE approach and tracked improvements in various disease indicators among participants involved in the project. Figure 4 provides an overview of the structure of the DHE program. In this educational model, we engaged a multidisciplinary team consisting of physicians, dietitians, nurses, and diabetes educators, working collaboratively to ensure the highest quality of education (Figure 4).
 |
Figure 4 In this educational model, we engaged a multidisciplinary team consisting of physicians, dietitians, nurses, and diabetes educators, working collaboratively to ensure the highest quality of education. |
The DHE program may contribute to improved glycemic outcomes through enhanced patient engagement, although knowledge and self-management behaviors were not directly measured in this study. Potential mechanisms may include improved patient motivation, adherence, or health behaviors. In previously study have reported that short-term diabetes education (<6 months) can significantly improve patients’ knowledge levels, the frequency and accuracy of self-monitoring blood glucose, dietary habits, and blood glucose control.10 Significant improvements have been reported in self-management and quality of life among individuals who received three months of diabetes education.11 Diabetes self-management education positively influences patients’ knowledge levels and self-management abilities. However, its effect on blood glucose control may not be evident in the short term (eg, three months), and there is a need for a longer-duration interventions to observe significant changes.12 This aligns with our study’s findings, in which notable improvements in blood glucose and lipid profiles were observed only six months to 1.5 years after receiving diabetes education.
In this study, the inclusion of nutritional education sessions allowed patients to better understand how to adjust their diets to normalize lipid levels. This aligns with previous research demonstrating the utility of educational interventions in improving blood glucose control, weight reduction, diabetes knowledge, self-efficacy, quality of life, dietary behaviors, and physical activity in patients with T2DM.12 Moreover, in this study, the patients’ body weight was also significantly controlled.
Interestingly, after more than two years of dietary education and lifestyle modifications, participants showed significant improvements in DBP control, but there was no significant decrease in SBP. This could be attributed to several factors. First, some participants may have undiagnosed chronic cardiovascular conditions, and the progression of age-related and diabetes-associated arterial stiffness may have contributed to the persistence of elevated SBP.13 Although lifestyle changes were implemented through education, arterial stiffness, other chronic diseases, or other medications may potentially limit improvements in SBP.
Lifestyle changes are reported to rapidly affect DBP, whereas significant reductions in SBP may require longer-term interventions.14 This suggests that lifestyle modifications have a more pronounced impact on microvasculature-related blood pressure (such as DBP), whereas SBP may be associated with other complications and require extended time or additional treatments to significantly improve. A meta-analysis of diabetes education studies conducted in developed countries between 1990 and 2006 found that that diabetes education leads to significant reductions in blood lipid levels but has a limited impact on lowering blood pressure, which is consistent with our observations.15
Results of the present study show that prolonged diabetes dietary education leads to a significant improvement in the lipid profile (including HDL-C, LDL-C, TG, and TC). The patients may have gained a better understanding of the importance of healthy eating after receiving the education, which would have resulted in a reduced intake of high-fat and high-caloric foods, along with an increased intake of dietary fiber and unsaturated fatty acids.16 Regular meal planning also helps stabilize blood glucose levels, thereby preventing lipid metabolism abnormalities caused by blood glucose level fluctuations.17 Furthermore, improvements in weight management and increased physical activity among patients may have contributed to enhanced lipid breakdown and lower blood lipid levels.18
Another interesting observation is that most participants in the DHE intervention group showed a significant reduction in HbA1c and fasting blood glucose compared to the control group during the first half year of the program. However, no significant difference was observed between the two groups after the second year. A possible explanation could be that although the DHE group received targeted education, the control group was simultaneously receiving medication or insulin therapy. It is challenging to avoid the influence of differing diabetes medications among participants, which could also potentially affect the data. However, since all participants in this study share the same diagnosis and were enrolled within 90 days of their diagnosis, we have made every effort to minimize heterogeneity among the participants. Nonetheless, the results suggest that while the significant difference disappeared after the second year, there was a decreasing trend in blood glucose levels, indicating better glycemic stability in the DHE group than in the control group. These findings suggest that long-term DHE participation may be associated with improved glycemic stability, though further research is needed to confirm causality.19,20
This study has some limitations. First, due to constraints in insurance coverage, most patients underwent assessment of their lipid profile, fasting blood glucose, and HbA1c only every three to six months. Second, no restrictions were placed on the primary medication types used by patients when enrolling participants in this study. This may have led to variations in the patients’ final laboratory test results due to differences in medications or treatment types. Third, although this study included a control group (patients who did not receive DHE), it is important to consider that participants who declined DHE may have had poorer baseline medical adherence and worse initial disease control compared to those in the DHE group. Finally, the sample sizes between the intervention group (n = 1080) and non-intervention group (n = 192) were unbalanced. However, this reflects the actual enrollment pattern in our real-world setting, where most newly diagnosed patients opted to participate in the diabetes education program. To preserve the representativeness and integrity of this naturalistic cohort, we chose not to perform matched or reduced analyses. We plan to explore propensity score matching in future studies to better account for baseline imbalances. These factors should be considered in future studies to ensure more robust findings.
Conclusion
These results suggest that participation in a structured DHE program may be associated with improvements in glycemic control, lipid profile, and other metabolic-related markers in patients with T2DM.Over the two-year intervention, participants in the DHE program exhibited substantial reductions in HbA1c, blood glucose levels, TG, LDL-C, TC, and body weight, alongside an increase in HDL-C level. Notably, HbA1c and fasting glucose levels significantly improved after 1.5 years of consistent DHE participation, suggesting that long-term engagement with structured education may contribute to sustained glycemic improvement.
Although SBP did not significantly improve, DBP showed a modest yet significant reduction. The findings also indicate that the DHE group achieved earlier and more pronounced improvements in the lipid profile than the non-DHE group, particularly within the first six months of intervention.
These findings support the potential value of incorporating structured health education into diabetes care systems to improve clinical outcomes and address the metabolic and cardiovascular risks associated with T2DM. Further research is warranted to explore the long-term sustainability of these benefits and their impact on overall diabetes-related complications and quality of life.
Ethical Considerations
According to the ethical standards of the Helsinki Declaration, this study was approved by Taipei medical university Institutional Review Board approved the study (approval number: 202211060). The consent form and information sheet were provided to participants prior to the interviews. Interviewees were informed of their voluntary participation and their right to withdraw at any time. Confidentiality was ensured by assigning codes to each participant.
Consent to Participate Declaration
Written informed consent was obtained from all participants.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Welfare TMoHa. Diabetes share care work guideline. Taiwan Taiwan Ministry of Health and Welfare; 2019. Available from: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=359&pid=1234.
2. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403.
3. Uusitupa M, Khan TA, Viguiliouk E, et al. Prevention of type 2 diabetes by lifestyle changes: a systematic review and meta-analysis. Nutrients. 2019;11(11):2611. doi:10.3390/nu11112611
4. Portal Teixeira P, Pozzer Zucatti K, Strassburger Matzenbacher L, et al. Long-term lifestyle intervention can reduce the development of type 2 diabetes mellitus in subjects with prediabetes: a systematic review and meta-analysis. Diabet Res Clin Pract. 2024;210:111637.
5. Han C, Xue H, Yang S, Gao B. Resistance exercise training and its impact on metabolic syndrome in type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabet Res Clin Pract. 2025;222:112077.
6. Holmen H, Torbjørnsen A, Wahl AK, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR mHealth UHealth. 2014;2(4):e57. doi:10.2196/mhealth.3882
7. Hsu WC, Lau KH, Huang R, et al. Utilization of a cloud-based diabetes management program for insulin initiation and titration enables collaborative decision making between healthcare providers and patients. Diabetes Technol Ther. 2016;18(2):59–67. doi:10.1089/dia.2015.0160
8. Sarfo FS, Treiber F, Gebregziabher M, et al. Phone-based intervention for blood pressure control among Ghanaian stroke survivors: a pilot randomized controlled trial. Int J Stroke. 2019;14(6):630–638. doi:10.1177/1747493018816423
9. Howells L, Musaddaq B, McKay AJ, Majeed A. Clinical impact of lifestyle interventions for the prevention of diabetes: an overview of systematic reviews. BMJ Open. 2016;6(12):e013806. doi:10.1136/bmjopen-2016-013806
10. Norris SL, Engelgau MM, Venkat Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care. 2001;24(3):561–587.
11. Pai L-W, Hung C-T, Chen -L-L, Lin R-L, Lockwood C. Efficacy of a health education technology program in improving adherence to self-management behaviors and quality of life among adults with type 2 diabetes: a randomized controlled trial. Primary Care Diabetes. 2024;18(5):479–485. doi:10.1016/j.pcd.2024.08.003
12. Powers MA, Bardsley JK, Cypress M, et al. Diabetes self-management education and support in adults with type 2 diabetes: a consensus report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. Diabetes Care. 2020;43(7):1636–1649. doi:10.2337/dci20-0023
13. Adler AI, Stratton IM, Neil HA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321(7258):412–419. PMID: 10938049; PMCID: PMC27455. doi:10.1136/bmj.321.7258.412
14. Marin-Couture E, Moulin J-A, Thibault A-S, et al. Impact of lifestyle medicine interventions on the management of systemic hypertension in primary care: a Canadian randomized controlled trial. Am J Lifestyle Med. 2024;18(5):703–720.
15. Fan L, Sidani S. Effectiveness of diabetes self-management education intervention elements: a meta-analysis. Can J Diabetes. 2009;33(1):18–26.
16. Mikhael EM, Hassali MA, Hussain SA. Effectiveness of diabetes self-management educational programs for type 2 diabetes mellitus patients In Middle East Countries: a systematic review. Diabetes Metab Syndr Obes. 2020;13:117–138. doi:10.2147/DMSO.S232958
17. Kubota S, Liu Y, Iizuka K, Kuwata H, Seino Y, Yabe D. A review of recent findings on meal sequence: an attractive dietary approach to prevention and management of type 2 diabetes. Nutrients. 2020;12(9):2502. doi:10.3390/nu12092502
18. Wang Y, Xu D. Effects of aerobic exercise on lipids and lipoproteins. Lipids Health Dis. 2017;16(1):132. doi:10.1186/s12944-017-0515-5
19. Susanti S, Bistara DN. Influence Self Monitoring Blood Glucose (SMBG) and Diabetes Self Management Education (DSME) on the stability of blood glucose levels. Jurnal Keperawatan Respati Yogyakarta. 2023;10(2):140–146.
20. Lai Y-C, Chen Y-S, Jiang Y-D, et al. Diabetes self-management education on the sustainability of metabolic control in type 2 diabetes patients: diabetes share care program in Taiwan. JFormos Med Assoc. 2024;123(2):283–292. doi:10.1016/j.jfma.2023.09.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.