Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Effectiveness of a Care Plan Based on the Multi-Theory Model in Reducing Fear of Disease Progression and Improving Quality of Life in Breast Cancer Patients: A Randomized Controlled Trial
Authors Zhang J, Zhuang J, Chen X, Chu T, Zhang Q, Ma L, Zhou H ![]() , Wu Y
, Wu Y ![]() , Chen L
, Chen L
Received 29 May 2025
Accepted for publication 17 July 2025
Published 25 July 2025 Volume 2025:17 Pages 653—667
DOI https://doi.org/10.2147/BCTT.S534595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Pranela Rameshwar
Jiajia Zhang,1,* Jiaru Zhuang,1,* Xian Chen,1 Tianyu Chu,1 Qian Zhang,1 Linlin Ma,1 Hui Zhou,1 Yibo Wu,1 Ling Chen2
1Obstetrics, Gynecology and Reproduction Research Center, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 2Department of Breast Surgery, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yibo Wu, Obstetrics, Gynecology and Reproduction Research Center, Affiliated Hospital of Jiangnan University, Wuxi, 214062, People’s Republic of China, Email [email protected] Ling Chen, Department of Breast Surgery, Affiliated Hospital of Jiangnan University, Wuxi, 214062, People’s Republic of China, Email [email protected]
Purpose: Fear of progression has become a prominent mental health problem. Our research aimed to evaluate the effectiveness of a care plan based on the Multi-Theory Model of health behavior change in reducing fear of progression in breast cancer patients undergoing adjuvant chemotherapy.
Patients and Methods: This randomized controlled trial enrolled 108 eligible participants receiving adjuvant chemotherapy at Jiangnan University Affiliated Hospital between May and December 2024. Routine care was administered to the control group, while the intervention group received the multi-theoretical model-based nursing intervention program integrated with general nursing. The evaluation time points included pre-intervention, immediately post-intervention (after 6 weeks), and 1-month post-intervention. Data were analyzed using Fisher’s exact test or chi-square test, Mann–Whitney U-test, independent samples t-test, generalized estimating equations, or repeated measures ANOVA.
Results: At various post-intervention assessments, the Multi-Theory Model group demonstrated significantly lower fear of progression scores along with higher self-management efficacy and quality of life scores, compared to the control group (p < 0.05). There were time, between-group, and interaction effects for the differences in the total scores of quality of life, self-management efficacy, and fear of progression between the two groups of participants (p < 0.05).
Conclusion: A nursing program grounded in the multi-theoretical model reduced the level of fear of progression, and improved quality of life and self-management efficacy in patients with breast cancer undergoing postoperative chemotherapy. These findings can provide a reference for psychological interventions in clinical settings for breast cancer patients.
Keywords: the multi-theory model, breast cancer, self-management efficacy, quality of life, fear of progression
Introduction
Breast cancer (BC) is a globally prevalent type of cancer.1,2 Breast cancer in the US is predicted to account for 32% of new cases in women in 2025.3 Surgery and post-operative treatment combined with chemotherapy have led to significant improvements in outcomes for breast cancer patients.4 Patients’ survival has been prolonged.5 During postoperative chemotherapy, BC patients experience varying degrees of cancer-related fatigue, negative mood, and insomnia.6–8 Among the many psychological distresses associated with breast cancer, fear of progression (FoP) is considered a pervasive and destructive distress.9
FoP has been shown to cause varying degrees of central nervous system stress in breast cancer patients at any stage of the disease, which in turn causes a decrease in the body’s immune function.10 Studies have shown that FoP also affects patients’ health outcomes, with higher FoP levels directly reducing patients’ quality of life (QoL).11 Studies have shown that patients often feel uncertainty and worry about FoP while undergoing chemotherapy, and this fear may further amplify their sensitivity to the side effects of chemotherapy.12 Thus, FoP interferes with treatment compliance, which in turn affects chemotherapy efficacy and prognosis.13 Moreover, FoP appears and remains relatively stable after the diagnosis of the disease and does not necessarily disappear over time.14 Patients with high FoP levels reported significant psychological distress, an inability to perform important social roles, and negative behavioral changes.15 Therefore, early identification and resolution of FoP-related emotional distress are needed to prevent psychological problems from impacting recovery and QoL.
Several research have found that interventions for BC patients can reduce FoP, fatigue, and improve QoL. Johns et al16 conducted a 6-week acceptance and commitment therapy intervention for BC patients and found that FoP scores were significantly reduced. Park et al17 conducted a positive thought-based cognitive therapy. The results suggested that the intervention could alleviate psychological distress, and reduce FoP and fatigue in BC patients. Research has shown that the Conquer Fear psychological intervention can reduce FoP in cancer patients by reducing intrusive cancer-related thinking and changing negative worry beliefs.18 In summary, there are a number of FoP-specific intervention approaches that have a positive effect on reducing FoP. However, current interventions require high qualifications for healthcare, are costly, and are not applicable to all patients. On the other hand, current interventions rarely focus on patient health behaviors to regulate negative emotions in breast cancer patients by motivating patients to manage their FoP.
The Multi-Theory Model of health behavior change (MTM), as a fourth-generation health education model, integrates the core concepts of multiple theories and emphasizes the precision of interventions and the sustainability of behavior change.19 The theoretical framework is illustrated in Figure 1. Over the past few years, multi-theoretical frameworks have gained increasing recognition and empirical validation in a number of health behavioral domains, such as smoking cessation, physical activity, dietary behaviors, health care, and mental health.20–24 The multi-theoretical model has the characteristics of being intervenable, measurable, having a low input cost, and simple and easy-to-implement intervention methods, which can not only improve people’s compliance but also help individuals to effectively integrate social resources to correct and repair the harm caused by bad moods. The validity of this theory has been demonstrated in thyroid cancer.25 In summary, although the multi-theoretical model shows promising applications, more experimental studies are needed to validate its effectiveness. In particular, there is a need to compare the effectiveness of interventions based on multi-theoretical models with those guided by other theories.26 In addition, the applicability of the multi-theoretical model in different cultural contexts and the standardization of intervention protocols need further study. Moreover, no studies have been retrieved on the validity of the multi-theoretical model on FoP in BC patients. Therefore, the present study used the multi-theoretical model as a framework to implement a nursing intervention program for BC patients, aiming to relieve their FoP and alleviate their negative psychological state, which will provide a reference for clinical care.
 |
Figure 1 Multi-theory model diagram. |
Materials and Methods
Study Design and Participants
The study utilized a two-group parallel randomized controlled trial methodology. Eligible breast cancer patients receiving adjuvant chemotherapy during the postoperative period were enrolled according to predefined inclusion criteria. Patients were selected from May 2024 to December 2024 in the department of breast surgery at the Affiliated Hospital of Jiangnan University. Inclusion criteria: (1) age ≥ 18 years; (2) histopathologic diagnosis of breast cancer, and receiving postoperative chemotherapy; (3) clear mental awareness without speech disorders; (4) FoP scale score ≥ 34; and (5) informed consent and voluntary participation in the survey. Exclusion criteria (fulfilling one of them): (1) combination of other serious diseases, such as heart failure; (2) stage IV breast cancer, cancer recurrence, or distant metastasis; (3) previously participated in or are participating in other similar clinical trials. During the intervention, a worsening of the condition or loss of visit was considered withdrawal from the study.
Calculation of Sample Size
The sample size was calculated using G*Power 3.1 software. Based on the results of a previous study,27 the effect value was set at 0.50, with a power of 0.8 and a two-sided test coefficient α = 0.05. The result of the calculation was 86 cases. Considering a 20% loss-to-follow-up rate, the final sample size was 86 / (1–20%) = 107.5, determining a total final sample content of 108 cases (54 cases per group).
Randomization, Blinding, and Allocation Hiding
For participants who met the criteria, informed consents were obtained, and random assignment was performed using the random number table method. We placed the 108 random numbers in sealed opaque envelopes. The process of randomization was carried out by personnel who were not involved in the intervention process and outcome assessment. Those involved in data analysis and statistical results were unaware of the details of the study.
Intervention Procedure
Pre-Intervention Preparation
The intervention team was made up of two breast surgeons, three breast surgery nurses, one psychologist, and four graduate nursing students. The study participants were screened based on their psychological condition and relevant medical documents, such as medical records. The nursing graduate students, led by the head nurse or attending physician, had in-person communications and conversations with the study participants.
Intervention Programs
All participants obtained routine oncological nursing support, which included: introduction to breast cancer-related knowledge and common misconceptions, safety education during hospitalization, guidance on nutrition and exercise, medication guidance, psychological care, and out-of-hospital follow-up education. The intervention group received a 6-week, 6-session MTM nursing intervention in addition to the usual care. Supplementary Table S1 illustrates the comprehensive intervention protocol. The preliminary draft of the intervention program was formed by combining the literature review, quantitative research,28 and theoretical framework. The final intervention plan was refined through expert correspondence. See the supplementary material for details of the expert correspondence (Tables S2–S7). The entire intervention process strictly followed the six phases of the MTM theory. There were six intervention themes, including “First Acquaintance - Paying Attention to Psychology”, “Transferring Knowledge - Enhancing Behavior”, “Reinforcing Knowledge - Building Beliefs”, “Relaxation - Rebuilding Hope”, “Positive Coping - Making Plans”, and “Social Support - Joint Supervision”. Each intervention lasted approximately 20–30 minutes, and the location was chosen to be in a breast surgery ward or demonstration room in a quiet environment. The forms of intervention included face-to-face group and individual interventions, as well as WeChat and telephone interventions. A combination of online and offline methods was used, with face-to-face interventions during hospitalization and WeChat and telephone interventions during discharge.
To ensure the quality of the intervention, team members were trained in the methodology and content of the intervention before it began. The time and place of each intervention were notified one day in advance to increase the participation rate of the study participants. Post-intervention, participants were sought for their feedback to ensure its effectiveness. Study participants were asked to perform online check-ins to monitor completion. Good communication was maintained with study participants throughout the intervention to address questions and needs in a timely manner, thereby improving compliance with the intervention. During the intervention period, the research team set up a regular meeting mechanism to monitor and evaluate factors that may affect the study results and to ensure the standardized implementation and consistency of the intervention program. Simultaneously, the team regularly summarized the progress and reported to the project leader and relevant experts to adjust and optimize the intervention strategy in a timely manner, thereby ensuring the scientific and effective implementation of the intervention measures.
Measurements
Questionnaire for General Information
The questionnaire consisted of two sections. The first part included age, marital status, number of children, education level, per capita monthly household income, employment status, place of residence, and type of medical expenses paid. The second part was clinical information including tumor stage, surgical method, axillary lymph node metastasis, presence of comorbid chronic diseases, and knowledge of the disease.
Fear of Progression Questionnaire-Short Form (FoP-Q-SF)
The scale was developed by Mehnert et al29 and translated and revised by Wu et al.30 The FoP-Q-SF consists of two dimensions, physical health and social family, with six entries each. A 5-point Likert scale was used, with 1–5 points assigned from “never” to “always”, with higher scores representing higher levels of FoP. Scores of 12–23 points represent low fear, 24–36 points represent moderate fear, and 37–60 points represent high fear. A score of ≥ 34 suggests that the patient needs intervention. The Cronbach’s alpha coefficient of the scale was 0.886.
Chinese-Version Strategies Used by People to Promote Health (C-SUPPH)
The scale was developed by Lev et al31 and translated and revised into Chinese by Qian et al.32 The scale includes three dimensions: positive attitude, self-decision making, and self-stress reduction, with a total of 28 entries. A 5-point Likert scale was used, with a score of 1–5 indicating no confidence to very confident. The Cronbach’s alpha coefficients for the total scale and each dimension ranged from 0.849–0.970.
Functioned Assessment of Cancer Therapy-Breast (FACT-B)
The scale was translated by Wan et al.33 The scale includes five dimensions: physical situation, social-family situation, somatic situation, emotional situation, and additional concerns. There are a total of 36 entries, which are divided into positively scored (17) and negatively scored (19) entries. The FACT-B has a score range of 0–144, with higher scores indicating better QoL. The Cronbach’s α values for the five dimensions of this scale ranged from 0.772–0.810, with a total value of 0.88.34
Data Collection
Data were gathered by two uniformly trained team members. Prior to data collection, the study’s objective, the questionnaire’s application, the time required to complete it, and precautions were introduced to the study participants, and informed consents were gained. When collecting baseline data, patients filled out the forms independently. If they were unable to do so due to writing difficulties or other reasons, the researcher used questioning to assist in filling out the forms. The data were reviewed after collection, and incomplete or non-compliant questionnaires were explained and supplemented. Baseline data were collected face-to-face before the intervention, and included patients’ general information, FoP-Q-SF, C-SUPPH, and FACT-B. Longitudinal assessments were conducted at three time points: baseline prior to intervention initiation (T0), post-intervention completion (T1), and one-month follow-up (T2).
Data Analysis
The original questionnaires collected were double-checked, and then data were entered and analyzed using SPSS 26.0. Continuous data were expressed as mean ± standard deviation or the interquartile range. Categorical data were described using frequencies and percentages. Comparisons between groups of categorical data were made using the chi-square test or Fisher’s exact test. Comparisons between groups of continuous data were made using the independent samples t-test or the Mann–Whitney U-test. In order to compare the trends in outcome indicators over time in the two groups of patients at T0, T1, and T2, normally distributed variables were examined using repeated measures ANOVA, and skewed distribution data were analyzed using generalized estimating equations. A p-value of < 0.05 for all tests was considered statistically significant.
Ethical Considerations
The study was approved by the Medical Ethics Committee of the Affiliated Hospital of Jiangnan University (Approval number: JNMS04230719) and conducted in strict accordance with the Declaration of Helsinki and local laws. All participants provided written informed consents. This study was registered with the Chinese Clinical Trial Registry (Registration number: ChiCTR2400083463).
Results
Baseline Information on Participants
Two cases in the control group dropped out of the study and two cases in the intervention group dropped out of the study, resulting in 104 patients completing the entire study (Figure 2). The mean age of the patients in the intervention group was 48.44 ± 8.50 years, and the mean age of the control group was 48.79 ± 9.74 years. Differences in general information such as age, education level, and work situation, were not statistically significant between the intervention group and the control group (p > 0.05) (Table 1).
 |
Table 1 Comparison of Demographic Data of the Two Groups of Patients |
 |
Figure 2 Flowchart of the study. Abbreviation: MTM, the Multi-Theoretical Models. |
Primary Outcome
Participant’s FoP
We compared FoP scores between groups at different time points (Table 2). The analysis revealed no significant differences in total FoP scores and dimension scores between the groups at baseline (T0) (p > 0.05). The total FoP score and the scores of each dimension in the intervention group were lower than those in the control group at T1 and T2 (p < 0.05). Figure 3A displays the FoP score trends for both groups. The outcomes of the generalized estimating equations suggested that there were between-group effects, time effects, and interaction effects between the two groups for the total FoP score and the dimension scores (p < 0.05), as shown in Table 3. To further analyze the changes in total FoP scores and dimension scores in the intervention group, we performed within-group comparisons at different time points. The analysis indicated that the FoP total score and the social-family dimension scores were significantly different in pairwise comparisons between the three time points (p < 0.05). Physiological health dimension scores were significantly different between T0 and T1, and between T0 and T2 (p < 0.05), as shown in Table 4.
 |
Table 2 Comparison of FoP Between the Two Groups at Different Time Points |
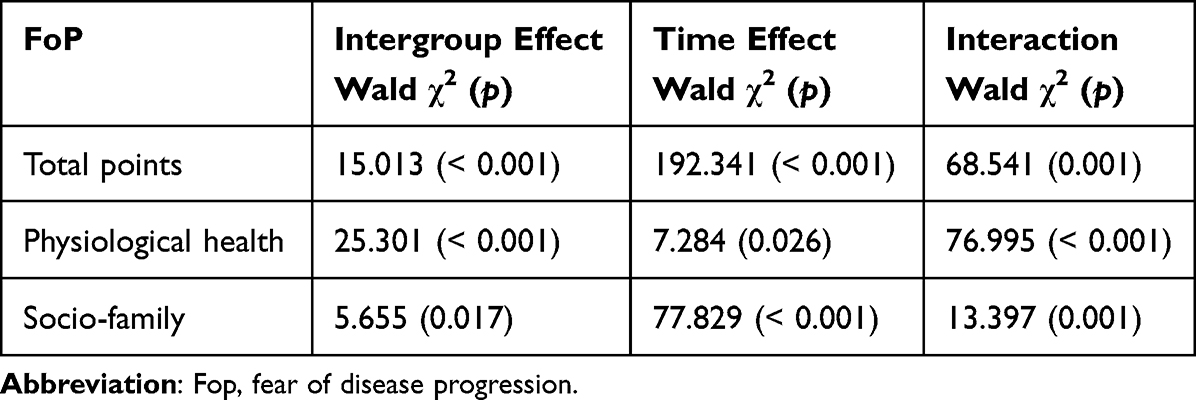 |
Table 3 Generalized Estimation Equation of FoP Scores Between the Two Groups |
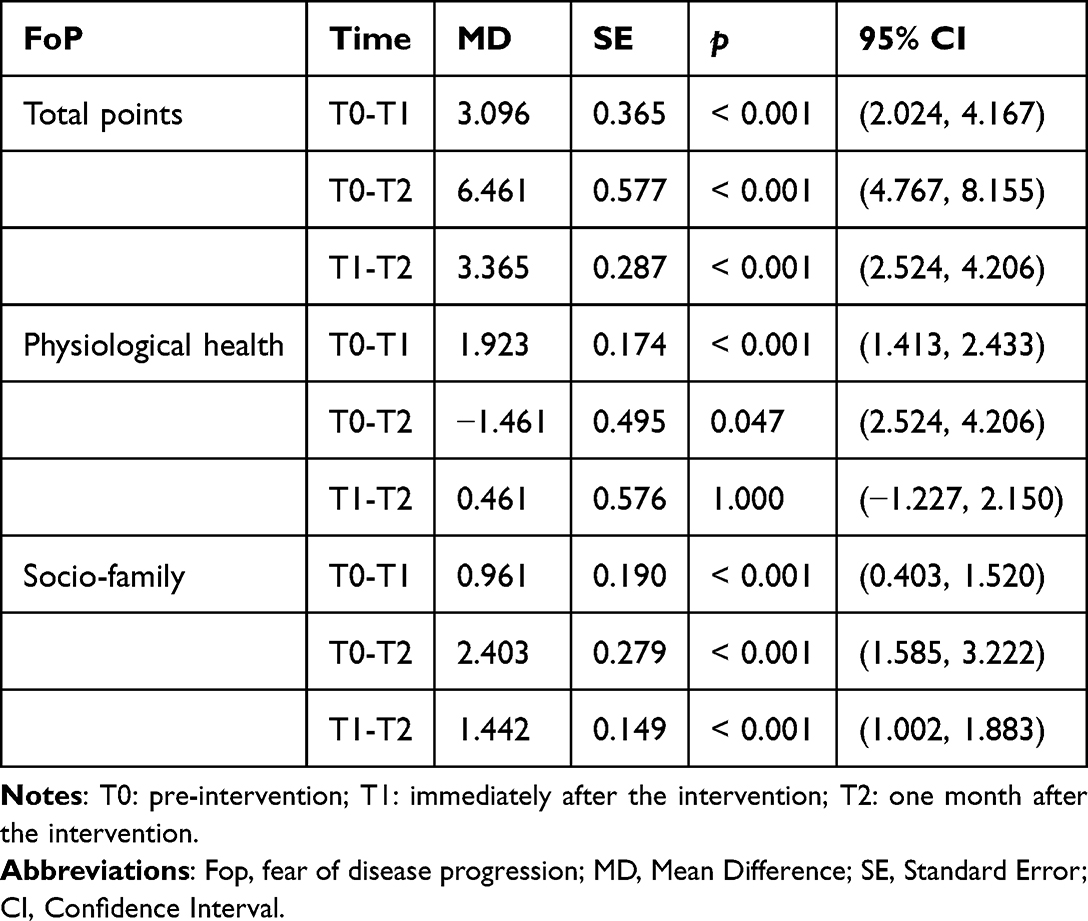 |
Table 4 Intra-Group Comparison of FoP at Different Time Points in the Intervention Group |
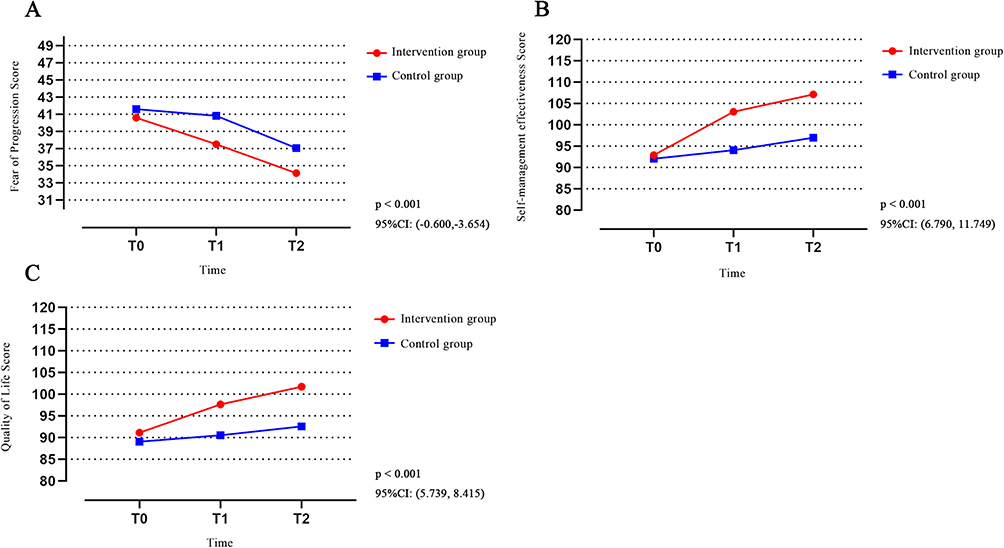 |
Figure 3 Trend charts of primary and secondary outcomes at different time points for both groups of patients. (A) Fop score. (B) Self-management efficacy score. (C) Quality of life score. |
Secondary Outcomes
Participants’ Self-Management Efficacy (SME)
We conducted between-group comparisons of SME scores at different time points (Table 5). The analysis revealed no statistically significant differences in total SME scores and dimension scores between the groups at baseline (T0) (p > 0.05). The total SME score and the scores of each dimension in the intervention group were higher than those of the control group at T1 and T2 (p < 0.05). Figure 3B displays the SME score trends for both groups. The outcomes of the generalized estimating equations suggested that there were between-group effects, time effects, and interaction effects between the two groups for the total SME score and the dimension scores (p < 0.05), as shown in Table 6. To further analyze changes in SME and dimension scores in the intervention group, within-group comparisons were made at three time points. The results showed that there were significant differences in the total SME score, the self-stress reduction dimension, and the self-decision-making dimension scores in the pairwise comparisons between the different time points (p < 0.05). The positive attitude dimension was significantly different between T0 and T1, and between T0 and T2 (p < 0.05). See Table 7.
 |
Table 5 The Scores of Self-Management Efficacy Between the Two Groups Before and After Intervention |
 |
Table 6 Generalized Estimation Equation of Self-Management Efficacy Scores Between the Two Groups |
 |
Table 7 Intra-Group Comparison of Self-Management Efficacy at Different Time Points in the Intervention Group |
Quality of Life of Participants
We compared QoL scores between groups at different time points (Table 8). The analysis revealed no statistically significant differences in total QoL scores and dimension scores between the groups at baseline (T0) (p > 0.05). The total QoL score, emotional status dimension, and additional concerns dimension scores of the intervention group were higher than those of the control group at T1 and T2. The physical, social-family, and functional status dimension scores of the intervention group were higher than those of the control group at T2 (p < 0.05). Figure 3C displays the QoL score trends for both groups. The results of the generalized estimating equations showed that there were between-group effects between the two groups for the total QoL score, the physical dimension, and the emotional and functional status dimension scores (p < 0.05). There were time effects and interaction effects between the two groups for the total QoL score and the dimension scores (p < 0.05), as shown in Table 9. To further analyze changes in QoL and dimension scores in the MTM group, within-group comparisons were made at different times. The analysis indicated that the total QoL, physical dimension, and functional status dimension scores were significantly different in pairwise comparisons between time points (p < 0.05). The social-family dimension, the emotional status dimension, and the additional attention dimension were significantly different between T0 and T1, and between T0 and T2 (p < 0.05). See Table 10.
 |
Table 8 Comparison of Quality of Life Between the Two Groups at Different Time Points |
 |
Table 9 Generalized Estimation Equation of Quality of Life Scores Between the Two Groups |
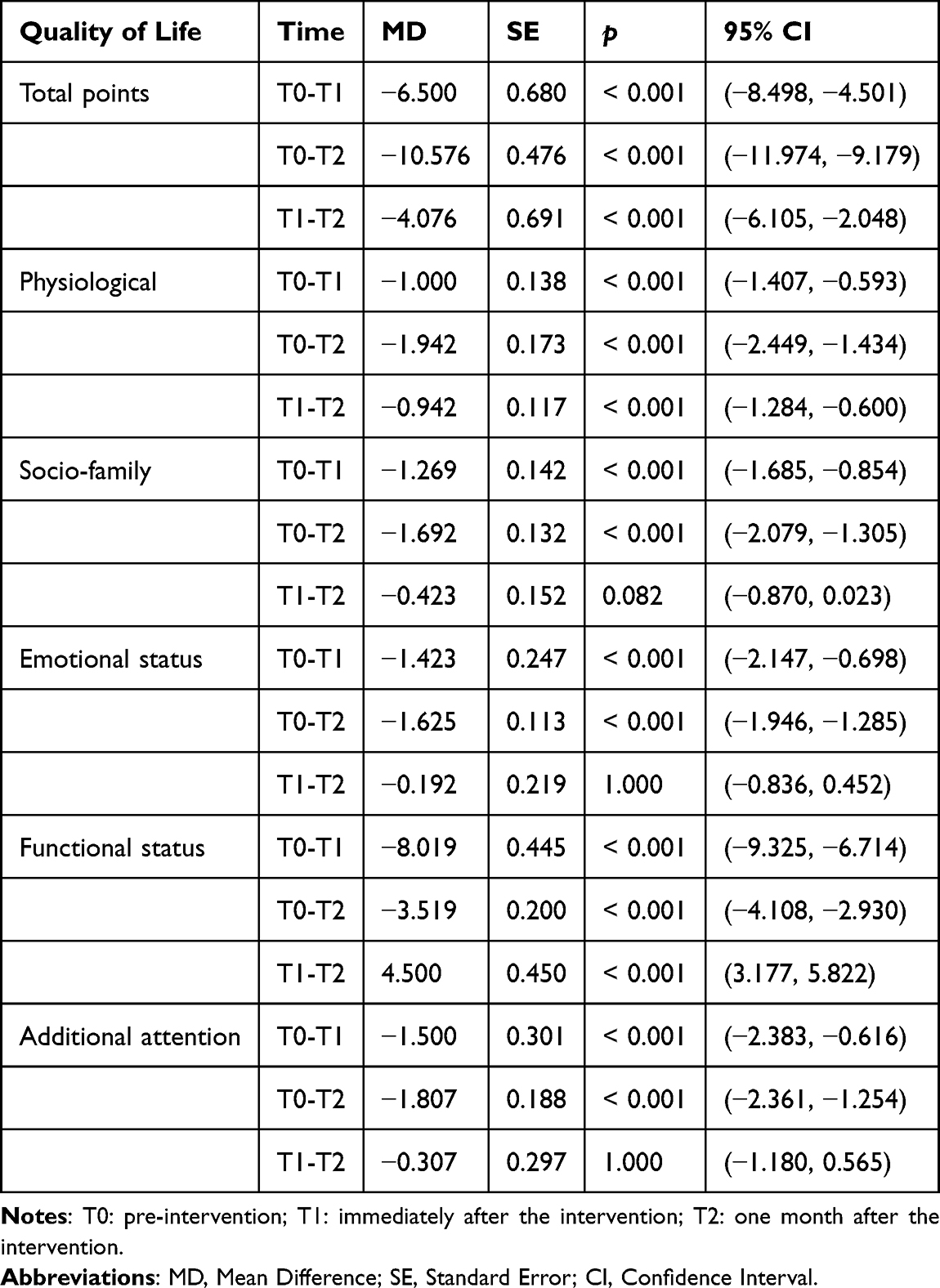 |
Table 10 Intra-Group Comparisons of the Quality of Life of Patients in the Intervention Group at Different Time Points |
Discussion
Our research examined the efficacy of an MTM-guided nursing approach in reducing FoP in patients undergoing postoperative chemotherapy for BC. The findings indicated that a care plan based on the MTM model had a positive impact on FoP, SME, and QoL in postoperative chemotherapy patients with BC.
The MTM-based nursing intervention reduced FoP levels in BC patients. In this study, FoP levels were higher in both groups at baseline. This was attributed to the predominance of young and middle-aged participants, who would be unable to continue their family and social roles if the disease progressed, thus affecting the family’s economic resources and the realization of personal social values.35 Both groups exhibited reductions in FoP levels post-intervention, with the MTM group demonstrating a significantly greater decrease compared to the routine care group. This is consistent with the survey of Ozhanli et al,36 which indicated that conducting skills training based on healthy behaviors was effective in reducing FoP and feelings of isolation. Our intervention plan had a positive influence on reducing FoP levels. This may be due to the sound theoretical and scientific basis of our intervention program. On the other hand, it has been shown that FoP scores are highly associated with depression and anxiety scores in post-chemotherapy BC patients.37 We not only conducted disease knowledge lectures to help patients and their spouses understand disease-related knowledge and correct cognitive biases, but also engaged in one-on-one communication to listen to and encourage patients, thereby stimulating positive emotions. In addition, the combination of group and individual interventions promoted experience sharing among patients. These pathways may have alleviated the patients’ anxiety and depression, thereby further reducing FoP levels.
The MTM-based nursing intervention improved SME levels in BC patients. Baseline assessment revealed moderate SME levels in both cohorts. This could be because BC usually involves surgery and chemotherapy, and patients need to cope with medication side effects (eg, hot flashes, osteoporosis), regular reviews, and lifestyle modifications over a long period.38 This continuous management burden results in fatigue and decreased confidence. The results of our study showed an upward trend in SME scores and dimension scores over time, confirming the effectiveness of the intervention program. We established communication channels through the WeChat group, which enabled patients’ problems to be addressed in a timely manner after discharge. Pushing and reminding participants to complete the intervention content through the WeChat platform after discharge alleviated the fear caused by the lack of knowledge about the disease, which may increase the patients’ confidence in self-management. In addition, based on the MTM model, the intervention aimed to enhance patients’ awareness and motivation for self-management and help them perceive the danger of negative emotions to physical and mental health. It also aimed to stimulate their health awareness, promote the maintenance of health behaviors, and improve their confidence in self-management.
The MTM-based nursing intervention improved QoL in BC patients. Findings demonstrated a marked enhancement in QoL for patients in the MTM group versus the control group post-intervention, aligning with the conclusions reached by Li et al.39 While no significant intergroup differences were observed at T1 for physical, social-family, or functional status dimensions, the intervention group demonstrated statistically superior outcomes at T2 across these dimensions, similar to the outcomes of Geng et al.40 Our intervention used techniques such as progressive muscle relaxation training and aerobic exercise to relax patients physically and mentally. Research has indicated that progressive muscle relaxation training may alleviate chemotherapy side effects and enhance QoL in BC patients.41 QoL tended to increase over time in our study. Other studies have shown that improvements in QoL are the result of the interaction of multiple factors and depend on the long-term maintenance of healthy behaviors.42 This suggests that future studies could improve the QoL of patients through various approaches, such as social, psychological, and physical factors, and highlights the importance of extending the follow-up period to dynamically observe changes in QoL.
Our research does, however, have a few limitations. First, the study design was single-center, which may affect the representativeness of the results and limit the scope of our conclusions. It is possible to expand the sample size and organize multicenter randomized controlled trials in different provinces and cities in future studies. Second, due to the time constraints of the topic, this study was only followed up to 1-month post-intervention. Future studies should increase the evaluation time points to clarify the lasting impact of the intervention program.
Conclusion
A nursing intervention program based on the multi-theoretical model can reduce fear of progression, increase self-management efficacy, and improve quality of life in postoperative chemotherapy patients with breast cancer. Our findings may provide new insights for healthcare professionals to implement psychological support strategies for breast cancer patients.
Data Sharing Statement
Upon reasonable request, communicating the correspondence author (Yibo Wu) may present data in favor of the results of this research.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki.
Acknowledgments
The authors express their gratitude to the team members, patients, and breast surgery nurses who participated in this study for their cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Wuxi Taihu Lake Talent Plan Leading Talents in Medical and Health Professions (Mading academician, 4532001THMD), Wu Jieping Medical Foundation (320.6750.2024-6-100), General Project of Wuxi Health Commission (M202408, M202418).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Arnold M, Morgan E, Rumgay H, et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast. 2022;66:15–23. doi:10.1016/j.breast.2022.08.010
3. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10–45. doi:10.3322/caac.21871
4. Omranipour R. Surgery for pregnancy-associated breast cancer. Adv Exp Med Biol. 2020;1252:95–99. doi:10.1007/978-3-030-41596-9_12
5. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
6. Ruiz-Casado A, Álvarez-Bustos A, de Pedro CG, Méndez-Otero M, Romero-Elías M. Cancer-related fatigue in breast cancer survivors: a review. Clin Breast Cancer. 2021;21(1):10–25. doi:10.1016/j.clbc.2020.07.011
7. Yi JC, Syrjala KL. Anxiety and depression in cancer survivors. Med Clin North Am. 2017;101(6):1099–1113. doi:10.1016/j.mcna.2017.06.005
8. Zhang J, Qin Z, So TH, et al. Acupuncture for chemotherapy-associated insomnia in breast cancer patients: an assessor-participant blinded, randomized, sham-controlled trial. Breast Cancer Res. 2023;25(1):49. doi:10.1186/s13058-023-01645-0
9. Zhang Q, Cai Y, Yu S, et al. Effects of fear of cancer recurrence on subjective physical and mental health in breast cancer patients: the intermediary role of heart rate variability. Cancer Med. 2023;12(15):16570–16579. doi:10.1002/cam4.6250
10. Zhou L, Li Y, Li X, et al. Propranolol attenuates surgical stress-induced elevation of the regulatory T cell response in patients undergoing radical mastectomy. J Immunol. 2016;196(8):3460–3469. doi:10.4049/jimmunol.1501677
11. Ban Y, Li M, Yu M, Wu H. The effect of fear of progression on quality of life among breast cancer patients: the mediating role of social support. Health Qual Life Outcomes. 2021;19(1):178. doi:10.1186/s12955-021-01816-7
12. He JL, Xu HQ, Yang J, et al. Fear of disease progression among breast cancer patients in China: a meta-analysis of studies using the fear of progression questionnaire short form. Front Psychol. 2023;14:1222798. doi:10.3389/fpsyg.2023.1222798
13. Wang Y, Li J, Zhai M, Zhao Y, Li Q. Exploring readiness for discharge, quality of discharge teaching, and fear of disease progression in lung cancer patients undergoing chemotherapy: a correlation analysis. Thorac Cancer. 2024;15(1):66–76. doi:10.1111/1759-7714.15164
14. Stanton AL, Danoff-Burg S, Huggins ME. The first year after breast cancer diagnosis: hope and coping strategies as predictors of adjustment. Psychooncology. 2002;11(2):93–102. doi:10.1002/pon.574
15. Dinkel A, Herschbach P. Fear of progression in cancer patients and survivors. Recent Results Cancer Res. 2018;210:13–33. doi:10.1007/978-3-319-64310-6_2
16. Johns SA, Stutz PV, Talib TL, et al. Acceptance and commitment therapy for breast cancer survivors with fear of cancer recurrence: a 3-arm pilot randomized controlled trial. Cancer. 2020;126(1):211–218. doi:10.1002/cncr.32518
17. Park S, Sato Y, Takita Y, et al. Mindfulness-based cognitive therapy for psychological distress, fear of cancer recurrence, fatigue, spiritual well-being, and quality of life in patients with breast cancer-a randomized controlled trial. J Pain Symptom Manag. 2020;60(2):381–389. doi:10.1016/j.jpainsymman.2020.02.017
18. Sharpe L, Turner J, Fardell JE, et al. Psychological intervention (ConquerFear) for treating fear of cancer recurrence: mediators and moderators of treatment efficacy. J Cancer Surviv. 2019;13(5):695–702. doi:10.1007/s11764-019-00788-4
19. Kapukotuwa S, Nerida T, Batra K, Sharma M. Utilization of the multi-theory model (MTM) of health behavior change to explain health behaviors: a systematic review. Health Promot Perspect. 2024;14(2):121–135. doi:10.34172/hpp.42887
20. Sharma M, Khubchandani J, Nahar VK. Applying a new theory to smoking cessation: case of multi-theory model (MTM) for health behavior change. Health Promot Perspect. 2017;7(2):102–105. doi:10.15171/hpp.2017.18
21. Hayes T, Sharma M, Shahbazi M, Sung JH, Bennett R, Reese-Smith J. The evaluation of a fourth-generation multi-theory model (MTM) based intervention to initiate and sustain physical activity. Health Promot Perspect. 2019;9(1):13–23. doi:10.15171/hpp.2019.02
22. Williams JL, Sharma M, Mendy VL, Leggett S, Akil L, Perkins S. Using multi theory model (MTM) of health behavior change to explain intention for initiation and sustenance of the consumption of fruits and vegetables among African American men from barbershops in Mississippi. Health Promot Perspect. 2020;10(3):200–206. doi:10.34172/hpp.2020.33
23. Sharma M, Johansen C, Batra K, et al. Using the multi-theory model (MTM) of health behavior change to explain the seeking of stool-based tests for colorectal cancer screening. Int J Environ Res Public Health. 2023;20(16):6553. doi:10.3390/ijerph20166553
24. K Nahar V, K Wells J, E Davis R, C Johnson E, W Johnson J, Sharma M. Factors associated with initiation and sustenance of stress management behaviors in veterinary students: testing of multi-theory model (MTM). Int J Environ Res Public Health. 2020;17(2):631. doi:10.3390/ijerph17020631
25. Sun X, Jiang Y, Wang J, et al. Effects of a mobile health intervention based on a multitheoretical model of health behavior change on anxiety and depression, fear of cancer progression, and quality of life in patients with differentiated thyroid cancer: a randomized controlled trial. BMC Med. 2024;22(1):466. doi:10.1186/s12916-024-03652-0
26. Sharma M, Awan A, Kapukotuwa S. Mini review: possible role of the multi-theory model of health behavior change in designing substance use prevention and treatment interventions. Front Public Health. 2024;12:1298614. doi:10.3389/fpubh.2024.1298614
27. Herschbach P, Berg P, Waadt S, et al. Group psychotherapy of dysfunctional fear of progression in patients with chronic arthritis or cancer. Psychother Psychosom. 2010;79(1):31–38. doi:10.1159/000254903
28. Jiaru Z, Yuan W, Shan W, Renjing H, Yibo W, Ling C. Fear of disease progression, self-management efficacy, and family functioning in patients with breast cancer: a cross-sectional relationship study. Front Psychol. 2024;15:1400695. doi:10.3389/fpsyg.2024.1400695
29. Mehnert A, Herschbach P, Berg P, Henrich G, Koch U. Fear of progression in breast cancer patients--validation of the short form of the fear of progression questionnaire (FoP-Q-SF). Z Psychosom Med Psychother. 2006;52(3):274–288. doi:10.13109/zptm.2006.52.3.274
30. Wu Q, Ye Z, Li L, Liu P. Reliability and validity of Chinese version of fear of progression questionnaire-short form for cancer patients. Chin J Nurs. 2015;50(12):1515–1519.
31. Lev EL, Owen SV. A measure of self-care self-efficacy. Res Nurs Health. 1996;19(5):421–429. doi:10.1002/(SICI)1098-240X(199610)19:5<421::AID-NUR6>3.0.CO;2-S
32. Qian H, Yuan C. Reliability and validity of the Chinese version of the Cancer self-management efficacy scale. Chin J Nurs. 2011;46(01):87–89. issn.0254-1769. doi:10.3761/j
33. Wan C, Zhang D, Yang Z, et al. Validation of the simplified Chinese version of the FACT-B for measuring quality of life for patients with breast cancer. Breast Cancer Res Treat. 2007;106(3):413–418. doi:10.1007/s10549-007-9511-1
34. Matthies LM, Taran FA, Keilmann L, et al. An electronic patient-reported outcome tool for the FACT-B (functional assessment of cancer therapy-breast) questionnaire for measuring the health-related quality of life in patients with breast cancer: reliability study. J Med Internet Res. 2019;21(1):e10004. doi:10.2196/10004
35. Hu C, Weng Y, Wang Q, et al. Fear of progression among colorectal cancer patients: a latent profile analysis. Support Care Cancer. 2024;32(7):469. doi:10.1007/s00520-024-08660-7
36. Ozhanli Y, Akyuz N. The effect of progressive relaxation exercise on physiological parameters, pain and anxiety levels of patients undergoing colorectal cancer surgery: a randomized controlled study. J Perianesth Nurs. 2022;37(2):238–246. doi:10.1016/j.jopan.2021.08.008
37. Vandraas KF, Reinertsen KV, Kiserud CE, Lie HC. Fear of cancer recurrence among young adult cancer survivors-exploring long-term contributing factors in a large, population-based cohort. J Cancer Surviv. 2021;15(4):497–508. doi:10.1007/s11764-020-00943-2
38. Rademaker LM, Gal R, May AM, et al. Side-effects in women treated with adjuvant endocrine therapy for breast cancer. Breast. 2025;80:104416. doi:10.1016/j.breast.2025.104416
39. Li L, Zhu C, Yan Q, Li J, Chen Y, Hu X. Effectiveness of dyadic interventions on quality of life for cancer patients and family caregivers: a systematic review and meta-analysis of randomised controlled trials. J Clin Nurs. 2025. doi:10.1111/jocn.17700
40. Geng Z, Wang J, Lyu W, et al. Effectiveness of a theory-based tailored mHealth physical activity intervention for women undergoing chemotherapy for breast cancer: a quasi-experimental study. Int J Nurs Sci. 2024;11(4):405–413. doi:10.1016/j.ijnss.2024.08.006
41. Yoo HJ, Ahn SH, Kim SB, Kim WK, Han OS. Efficacy of progressive muscle relaxation training and guided imagery in reducing chemotherapy side effects in patients with breast cancer and in improving their quality of life. Support Care Cancer. 2005;13(10):826–833. doi:10.1007/s00520-005-0806-7
42. Zhang T, Ren Z, Wakefield CE, et al. Are digital psychological interventions for psychological distress and quality of life in cancer patients effective? A systematic review and network meta-analysis. Clin Psychol Rev. 2025;115:102520. doi:10.1016/j.cpr.2024.102520
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.