")
Back to Journals » International Journal of General Medicine » Volume 16
Effectiveness and Safety of Bu Shen Kai Qiao Fang in the Treatment of Alzheimer’s Disease: Study Protocol for a Multicenter, Prospective, Real-World Clinical Trial
Authors Xu Z , Li O , Liang Y, Wu Z, Xu J, Wang L, Li L, Sun Y
Received 25 April 2023
Accepted for publication 9 June 2023
Published 17 June 2023 Volume 2023:16 Pages 2573—2583
DOI https://doi.org/10.2147/IJGM.S418700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
ZeYu Xu,1,* Ou Li,1,* YaTing Liang,1,* ZhiBing Wu,2 Jiamei Xu,2 Ling Wang,3 Ling Li,3 YongNing Sun1
1Department of Brain and Mental Disease, Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, ShangHai, 200040, People’s Republic of China; 2Department of Encephalopathy, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, 510405, People’s Republic of China; 3Department of Geriatrics, Shaanxi Provincial Hospital of Traditional Chinese Medicine, Xi’an, 710003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: YongNing Sun, Shanghai University of Traditional Chinese Medicine, Shanghai, 200040, People’s Republic of China, Tel +8618930177579, Email [email protected]
Background: Alzheimer’s disease (AD) is a common degenerative disease of the nervous system with serious impact on quality of life of patients and their families. With an aging population, AD has become a major public health problem in China and worldwide. However, the physiological and pathological mechanisms of AD have not been fully elucidated, and there is a lack of effective prevention and clinical treatment methods. Many studies have found that traditional Chinese medicine (TCM) has a good therapeutic effect on cognitive function in AD patients. Bu Shen Kai Qiao Fang (BSKQF) is one such Chinese herbal preparation used in the treatment of AD. We designed a protocol for a real-world clinical study of BSKQF combined with Donepezil hydrochloride (DH) to evaluate the efficacy and safety of this approach in the treatment of AD patients.
Methods: This is a protocol for a real-world, multicenter, prospective, observational cohort study. The study will recruit 860 AD patients from four hospitals across China. Equal numbers of patients will be treated with BSKQF and DH or with DH only. The criteria for grouping are based primarily on patient preference. Outcome measures include scores on the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment Scale (MOCA) and will be recorded at baseline, and at one, two and three months after enrollment. The plasma Aβ 42 and plasma Tau levels of participating patients will also be measured by ELISA at baseline and after 3 months of treatment. Safety metrics and adverse events (AEs) of participating patients will be monitored and recorded.
Discussion: This study will evaluate the clinical efficacy and safety of BSKQF in the treatment of AD. The results will provide reliable evidence for the clinical application of BSKQF in the treatment of AD.
Study Registration: Trial registration: Chinese Clinical Trial Registry, NO. ChiCTR2000039670, Registered 5 November 2020 https://www.chictr.org.cn/showprojEN.html?proj=63800.
Keywords: Alzheimer’s disease, Bu Shen Kai Qiao Fang, real-world trial, MMSE, MOCA, Aβ 42, tau
Introduction
Known for its deteriorating cognitive function and behavioral impairment, Alzheimer’s disease is a degenerative disease of the central nervous system, which mainly occurs in the elderly population.1 As one of the most important manifestations of dementia, about one third of dementia cases are classified as Alzheimer’s disease. According to a survey released by the World Health Organization in 2021, more than 55 million people globally suffer from dementia.2 With a large, increasingly aging population, the number of dementia patients in China has increased dramatically, and may account for about one quarter of patients worldwide.3
A cholinesterase inhibitor (donepezil) and N-methyl-D-aspartate receptor antagonist (memantine) are currently clinically approved drugs for AD treatment.4 Recent studies show that the above two categories of drugs can only improve the cognitive symptoms of AD patients. However, no drug has been shown to reliably slow or prevent the damage and destruction of neurons, key mechanisms in AD, so current medical treatment for AD does not fully address the condition.5–7
Traditional Chinese medicine is therapy with a long history. It has also shown excellent therapeutic effect in the treatment of AD.8,9 Clinical studies have shown that, in patients with mild to moderate AD dementia, traditional Chinese medicine and conventional Western medicine can significantly slow cognitive decline, and has significant benefits for AD patients compared with the use of Western medicine alone.10 Traditional Chinese medicine for AD is based on kidney essence deficiency and myelin sea deficiency being the core pathogenesis of AD dementia, and that treatment is based on kidney tonifying. Our research group has previously found that Yi shen formula can effectively improve cognitive and behavioral function in a rat model of dementia, reduce hippocampal neuronal cell apoptosis, and induce hippocampal neuronal cell repair.11 Bu Shen Kai Qiao Fang (BSKQF) is a Chinese herbal formulation developed by Professor Sun YongNing for treatment of AD, and has been found to reduce cognitive decline in AD patients. Therefore, in the present protocol BSKQF will be combined with Donepezil hydrochloride (DH) to form a new therapy for AD, the efficacy and safety of which will be tested in a multicenter, prospective, real-world study. Different from the traditional Chinese medicine treatment of AD clinical studies that only use scale evaluation, the innovative application of Aβ42 and other biomarker detection combined with scale evaluation in this study is expected to provide more convincing clinical evidence for evaluating the effectiveness of BSKQF in the treatment of AD.
Methods
Objectives
This study aims to evaluate the clinical efficacy and safety of BSKQF prescription in the treatment of Alzheimer’s disease. This will be achieved by collecting large-scale, rich data in a real clinical environment.
Design
This study is a real-world, multicenter, prospective, observational cohort study. We will recruit a total of 860 AD patients from four hospitals in different regions of China between July 2021 and July 2024. Two groups of patients will be analyzed: exposed (BSKQF and DH treated) and non-exposed (DH only treated). The criteria for grouping are based primarily on patient preference. In addition to the baseline assessment, the evaluation will take place one, two, and three months after enrollment. Blinding will be applied to the assessors and statisticians analyzing the results.
The study method follows a rigorous scientific approach to clinical research and complies with the principles of the Declaration of Helsinki12 and Good Clinical Practice 2020.13 All staff involved in the study will be trained and will have passed the GCP.
The trial has been registered in the Chinese Clinical Trial Registry (NO. ChiCTR2000039670). It was approved by the Ethics Committee of the Shanghai Municipal Hospital of Traditional Chinese Medicine (No. 2020SHL-KY-30) as well as the ethics committees of each research branch center.
The four hospitals involved in the study are: (1) Shanghai Municipal Hospital of Traditional Chinese Medicine; (2) Shaanxi Provincial Hospital of Chinese Medicine; (3) The First Affiliated Hospital of Guangzhou University of Chinese Medicine; (4) Chengdu University of Traditional Chinese Medicine.
This study does not require the participation of patients or the public in the design, implementation, reporting or dissemination of our study. We drew a research flow chart to explain the whole research scheme (Figure 1).
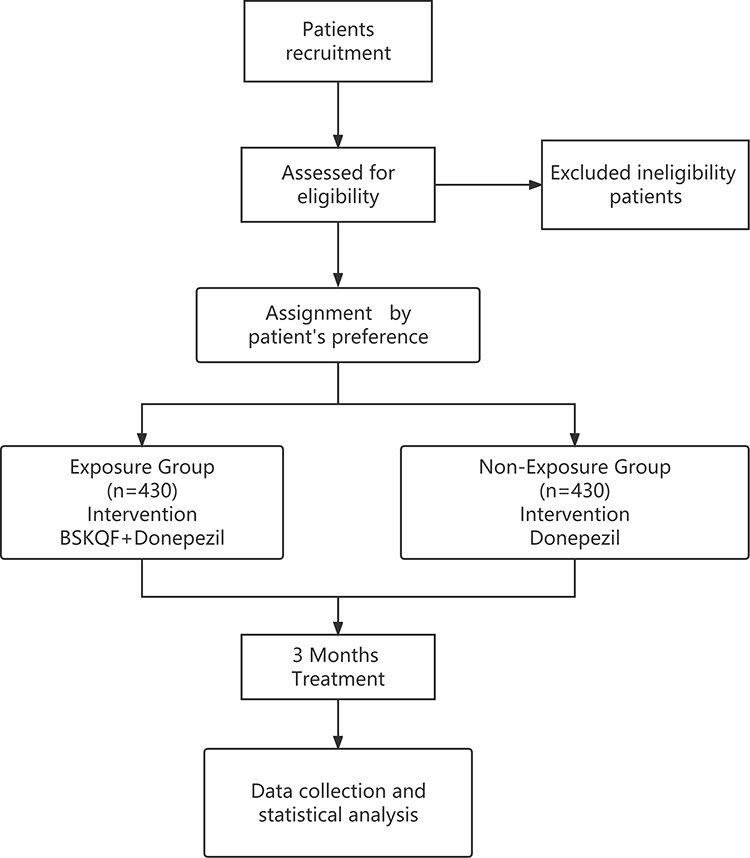 |
Figure 1 Flow chart of the study method. BSKQF: Bu Shen Kai Qiao Fang. |
Randomization and Blinding
Researchers will assign patients to different groups based on their preferred treatment, so randomization and blinding do not apply. However, when evaluating the results, statisticians and personnel responsible for the final analysis will be blinded. Statisticians will not be informed of the specific patient group when recording and analyzing relevant metrics for both groups of participants.
Participants
The trial plans to recruit potential eligible participants with a diagnosis of AD. Patients with AD in the above four hospitals will be encouraged to participate in this trial via recruitment posters posted and distributed in the hospitals. Concurrently, the wechat mini program for early screening of AD will be used to screen and encourage patients to participate in the study (The wechat mini program has been commissioned by Jinan University to help develop it), and recruitment advertisements will be published on the website. A close monitoring of patient recruitment will be conducted to ensure the target sample size is reached.
Diagnostic Criteria for Alzheimer’s Disease
The study will apply diagnostic criteria for AD that are consistent with the Chinese Guidelines for Diagnosis and treatment of Alzheimer’s Disease and Dementia published in 202014 and NIA-AA (2011)15 (Box 1).
 |
Box 1 Alzheimer’s Disease Clinical Diagnostic Criteria |
In addition to meeting the above criteria for dementia diagnosis, the following should apply:
- Insidious onset
- Clear reported history or observation of cognitive deterioration
- History and examination confirming early and significant cognitive impairment with one of the following: amnestic presentation or non-amnestic presentations
Diagnostic Criteria of Dementia in TCM
According to the Guidelines for Clinical Research of Chinese Medicine (New Drug)16 and International Clinical Practice Guide for Traditional Chinese Medicine-Alzheimer disease,17 the patient will have primary symptoms of aging, mental decline or forgetfulness, recent memory loss. In addition, secondary symptoms include dizziness and tinnitus, tooth decay, waist and knees sour and soft, lazy thinking lying, walking difficulty, thin tongue, white moss, deep thready pulse. A patient must present with at least two secondary symptoms as well as one primary symptom.
Inclusion Criteria
It is necessary for patients to meet the following requirements:
- Meet the diagnostic criteria for Alzheimer’s disease.
- Meet the diagnostic criteria of Dementia in TCM;
- 10≤The MMES score≤26 (Adjust the decision value according to the patient’s education level, illiteracy≤22, primary education≤23, Middle school education level≤24, University education level≤26)
- Of either sex and between 50 and 80 years old
- Based on history from the patients or caregivers, the patient’s memory loss has existed for at least 6 months, and is gradually worsening;
- Signed informed consent (patient or caregiver) and willingness to perform all tests and evaluations at the time of the trial visit;
- Primary school education or above, and be able to complete cognitive ability measurement and other tests specified in the program;
- Patients should have a stable caregiver, or at least a caregiver who the researchers can contact frequently (spending at least two hours per day with the patient for at least 4 days per week). Caregivers will help patients to participate in the research process, accompanying them to participate in the research, and must have sufficient interaction and communication with them so that the results of each evaluation scale can provide valuable information.
Exclusion Criteria
- Not meeting the diagnostic criteria for Alzheimer’s disease.
- Younger than 50 years or older than 80 years;
- No signed informed consent (participant or caregiver), or patient unable to conduct examinations and assessments within the duration of the trial, or unable to complete the cognitive ability measurement and other tests specified in the protocol;
- With end-stage dementia;
- With severe neurological deficits, such as aphasia, agnosia, and others;
- Patients with serious primary diseases such as cardiovascular disease, liver, kidney, hematopoietic system and malignant tumor, or psychiatric illness
- Participated in other clinical studies within the past two months;
- Suspected or confirmed allergy to the study drug.
Withdrawal Criteria
- Meeting exclusion criteria or not meeting inclusion criteria;
- During the treatment, additional treatment is needed and may affect the outcome of this study;
- Study drugs not used according to the study protocol;
- No record of post-treatment visit
- Development of drug allergy during the study.
(Enrolled patients who meet Withdrawal Criteria during the study will be discontinued from the study)
Shedding Criteria
- The patient withdraws voluntarily for any reason;
- The investigators determined that the patient was not appropriate to continue treatment in the study.
Trial Suspension Criteria
If there is a serious security incident during the trial, the trial will be suspended. The lead supervisor will be responsible for dealing with any such incident. Key problems related to accidents shall be recorded in detail and handled properly.
Sample Size Estimation
This study is a superiority trial. The sample size estimate is based on published randomized controlled trial (RCT) findings of Donepezil for the treatment of AD.We estimated the response rate of 70% in the Donepezil group and 80% in the BSKQF+Donepezil group, unilateral test was used, α= 0.025, 1- β=0.9. The treatment group and the control group were included in the number of cases at a ratio of 1:1. According to the sample size calculated using PASS 15.0 software, each group should include 389 people, and the expected attrition rate is 10%. The number of people in the each group should therefore be 430 respectively, with a total sample size of 860.
Interventions
According to their wishes, patients meeting the inclusion criteria and signing the informed consent form will be allocated to either the exposure group or non-exposure group. In order to facilitate the trial and minimize attrition, enrolled patients will be instructed to take medication, cognitive and other tests, and receive necessary health education before the trial. They will also be informed in detail about the possible risks and benefits of participation in this study, their rights and obligations during the research process, and how to deal with emergencies. Patients in the non-exposed group will be treated with DH, 5mg by mouth once per day for three months. The exposed group will be given the same DH dose plus BSKQF Chinese medicine granule, twice per day (morning and evening), with 100mL warm water, for three months. The traditional Chinese medicine granule composition is as follows: Radix Rehmanniae Praeparata 15g, Acorus tatarinowii Schott 9g, Radix Cyathulae 10g, Poria Cocos 15g, and Fructus Alpiniae Oxyphyllae 10g. Patients in these two groups will be instructed to take no other traditional Chinese medicine during the study period. As this is a real-world study, patients’ conditions (such as hypertension or heart disease) and complications will be treated with Western medicine according to relevant clinical guidelines. All drugs taken by the patients will be recorded in the case report forms (CRFs). The traditional Chinese medicine granule used in this research has been produced by Sichuan Neo-Green Pharmaceutical Technology Development Co., Ltd. Donepezil hydrochloride tablets are manufactured by Eisai Co., Ltd. (SFDA approval number H20070181).
The researchers will contact the participants throughout the study and ensure that they receive treatment and tests as soon as possible.Related examination results will be collected at baseline and at one month intervals during treatment, including patient information records, efficacy related cognitive performance tests, biomarkers, and safety related indicators. (The data to be recorded and related time points are shown in Table 1).
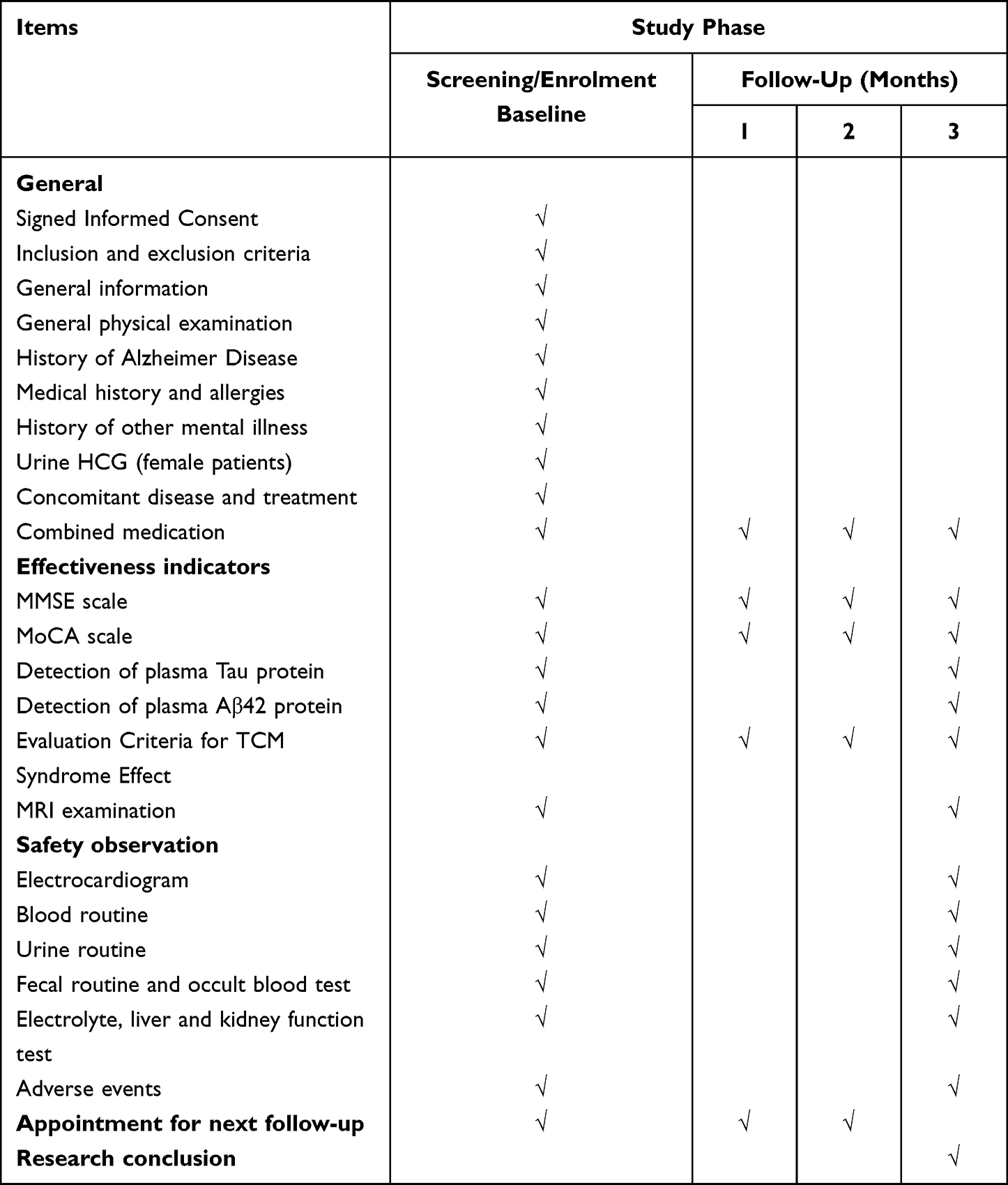 |
Table 1 Schedule of Intervention and Assessments |
Outcomes
Primary outcomes
Primary outcomes will be scores on MMSE and MOCA scales, and the detection of Aβ42 and Tau plasma proteins. They will be assessed at screening (V0 phase), one month (V1 phase), two months (V2 phase), and three months (V3 phase).
MMSE Scale
The MMSE scale has irreplaceable value for the diagnosis, stratification and prediction of cognitive disorders.18 Will be conducted by qualified investigators at 1-month intervals.
MOCA Scale
The MOCA scale is used to assess cognitive impairment in older adults19 and will be administered by qualified investigators at 1-month intervals.
Improvements on MMSE and MOCA scale scores are primary outcomes, and any change in their mean value will be used to represent changes in intelligence, and to determine whether there is a significant difference in this change between the exposed and the non-exposed groups. The pre-post treatment mean score will also be used as the evaluation index:
Improvement Rate = ((baseline score - post-treatment score)/baseline score)×100
Detection of Aβ42 and Tau Plasma Proteins
Aβ42 and Tau proteins are important biomarkers of AD. Plasma Aβ42 levels are dynamically correlated with clinical stages of dementia20 and elevated plasma T-tau concentrations are associated with the progression of cognitive impairment.21 The plasma concentrations of Aβ42 and Tau proteins will be measured in the third month of treatment using the relevant ELISA kit (SMC™ Amyloid Beta 42 Kit, Millipore, 03–0146-00; Tau Total Human ELISA Kit, Thermo Fisher Scientific, KHB0042).
Secondary Outcomes
Evaluation Criteria for TCM Syndrome Effect
We will evaluate the effectiveness of the treatment by assessing the improvement in clinical symptoms based on the Guidelines for Clinical Research of Chinese Medicine (New Drug). There are four levels of severity for the primary symptoms of dementia with syndrome of marrow sea insufficiency: mild, moderate, and severe with 4, 8, and 12 points. There are four levels of severity for the secondary symptoms mild, moderate, and severe with 2, 4, and 8 points. The total TCM symptoms score will be used to calculate the efficacy indicator (EI) as follows:
EI = ((baseline total symptom score – post-treatment total symptom score)/baseline symptom score)×100
The EI is adopted to evaluate treatment efficacy with symptom improvement levels categorized as follows: clinical control (EI≥95%), significant effect (94% > EI≥ 70%), effective (69% > EI≥30%) an ineffective (EI<30%).
This test will be carried out during the third month of treatment.
MRI Examination
The Improvement in Frontal atrophy will be measured by visual score based on MRI coronal imaging of the head, in the screening period and third month of treatment.
Safety Outcomes
The safety outcomes and vital signs in patients will be tested at baseline and every month during medication, and detailed results will be recorded on the CRF in a timely fashion. In addition, all AEs occurring throughout the study will be closely observed and documented by the investigator, and the patients will be appropriately managed.
Safety and Adverse Events
An adverse event is defined as any medical presentation that is negative or adverse during the course of the study, regardless of whether a causal relationship can be established. BSKQF has shown beneficial effects in clinical application for many years, and no obvious adverse reactions have been observed during treatment. According to information provided with DH, it may be associated with headaches, fatigue, muscle cramps, insomnia, or gastrointestinal symptoms such as nausea and diarrhea. All relevant events occurring throughout the study will be recorded systematically in detail, including cause, subsequent interventions, treatment outcomes, and other relevant information, using a table If AEs occur, appropriately qualified full-time researchers will be assigned to closely observe the patient’s condition and give necessary treatment and proper care to the patient until the AEs are resolved. There are three categories of serious adverse events: (1) serious or life-threatening complications; (2) hospitalization, disability or even death; (3) Other serious events that cause patients significant harm. Furthermore, the ethics committee will be informed as soon as possible of any serious adverse events so they can determine whether the patient should be removed from the trial.
Data Collection
True and accurate records of information from all patients participating in the study will be maintained in the CRFs by specially trained investigators. The research supervisor will critically review each CRF on completion and deliver it to the data manager, who will use EpiData software to enter and manage patient data. The personal information of patients will be strictly confidential, and all CRF data will use code numbers and non-identifying information. Other researchers will not be permitted to access any data without permission of the research supervisor. According to the GCP, all patient data will remain in the database for five years after the trial is completed.
Statistical Analysis
The principle of intention-to-treat analysis will be used to analyze efficacy. The intention-to-treat sample is defined as the cohort of eligible cases, including withdrawn cases, but not cases excluded from the study. The data from cases in which not all treatment processes were observed will be estimated by carrying forward the last observed values, and the results will be analyzed using intention-to-treat analysis. Continuous variables such as age and height will be expressed by mean ± standard deviation if normally distributed, or median and 1st and 3rd quartiles if not. Between-group comparisons will be made using t-tests in the former case, or Wilcoxon rank test and inspection in the latter case. Statistics will be conducted using two-sided tests, and a level of significance of P<0.05 will be considered significant.
Data Quality Control
Prior to the commencement of the trial, a trial process training session will be held online to ensure that all researchers are adequately trained and have a thorough understanding of the trial process and regulations and that observations and results are recorded accurately and in a timely fashion. The study methodology was developed under the guidance of researchers with professional knowledge and clinical experience to ensure that the study protocol is fully scientific and operable. Patients will be screened in strict accordance with inclusion and exclusion criteria, and the trial will follow the clinical design principles of a multicenter, prospective, observational cohort study. Blood, urine and other test samples collected by each research sub-center will be uniformly sent to the central laboratory for analysis, testing and destruction, to minimize detection bias. If an AE occurs during the trial, the subject will be treated appropriately and the ethics committee will be informed immediately. Medical statisticians have been involved in the design of the trial and will be involved in the collection of analytical data until the end of the trial. The data manager will systematically check the main data after completion. A data monitoring committee will organize a centralized review every three months to monitor the progress of the trial and assess the collected data for quality control.
Ethics Approval
The trial will be conducted in strict accordance with the ethical principles of the Declaration of Helsinki and has been approved by the Ethics Committee of Shanghai Hospital of Traditional Chinese Medicine (No.2020SHL-KY-30) and ethics committees of each of the other three hospitals. On enrolment of each patient, the investigator will explain the purpose, process and possible risks of the study according to the provisions of the patient’s informed consent, and will ask the patient to provide a signed declaration of informed consent. Throughout the trial, the personal information of patients who are enrolled or potential participants will be kept strictly confidential and will not be available to anyone other than trial staff.
Discussion
According to recent studies, TCM can reverse AD symptoms by reducing Aβ deposition and neurofibrillary tangles,22 controlling abnormalities of cholinergic transmission and other neurotransmitters,23 providing protection for the cerebrovascular system,24 improve cognitive function in AD patients,25 increasing the circulation of blood in the brain,26 improving mitochondrial function of hippocampal neurons,27 and preventing hippocampal neuron apoptosis.28 BSKQF contains five main active ingredients of Rehmanniae, Calamus acorus, Achyranthes bidentata, Poria cocos and Fructus Alpiniae Oxyphyllae. Studies have shown that these may improve cognitive function in AD by up-regulating NTFs expression, antiinflammation and antioxidant, reducing Aβ deposition, improving gut dysbiosis, and modulating tau protein phosphorylation.29–33 Therefore, it is feasible that BSKQF can effectively improve the clinical symptoms of AD patients.
At present, MMSE and MOCA remain commonly used in clinical diagnosis of AD due to their convenience and high sensitivity to AD. Cerebrospinal fluid detection of p-tau, Aβ42 and total tau protein is a mature diagnostic biomarker for AD. Although this approach has a high diagnostic accuracy, its popularity remains low due to its invasiveness and long periods to obtain results.34 Blood biomarkers are much easier to collect. Plasma Aβ42, Aβ40 and tau protein levels are now established biomarkers for AD, and all of them have good sensitivity in the diagnosis of AD.35,36
RCTs and their systematic reviews/meta-analyses are often considered as the “best evidence” for evaluating interventions in evidence-based medicine and are used to guide clinical practice. In recent years, increasing numbers of experts have pointed out that the results from RCTs are limited in clinical practice.37,38 Real world research (RWR) refers to the use of epidemiological research methods to conduct a minimally biased study of the actual application of interventions in a population.39 Compared with the RCT approach, RWR focuses more on the efficacy and long-term adverse effects of the intervention in the actual medical setting, includes more subjects and a more complex population.40 In addition, RWR involves treatment or prognosis in the real environment, as part of the actual medical process, which is conducive to long-term follow-up of patients.41 Since we have observed good symptom improvement in AD patients with BSKQF in our clinical application, we hope that the current RWR will help to obtain direct clinical evidence of the effectiveness of BSKQF in AD treatment.
Due to the lack of similar RWR studies, we believe that conduct of this study and publication of its results will provide scientific support for the use of BSKQF intervention to improve cognitive function in AD patients.
Abbreviations
AD, Alzheimer’s disease; BSKQF, Bu Shen Kai Qiao Fang; DH, Donepezil Hydrochloride; TCM, Traditional Chinese medicine; AEs, Adverse events; CRFs, Case report forms; Aβ, Amyloid β-protein; Tau, Microtubule-associated protein tau; EI, Efficacy indicator; RWR, Real world research; RCT, Randomized Controlled Trial; NTFs, Neurotrophic factors.
Data Sharing Statement
This is a research proposal, so there are currently no available data. Further information not included in this article will be provided by the corresponding author upon completion of the trial.
Ethical Approval and Consent to Participate
The protocol was approved by the Ethics Committee of Shanghai Municipal Hospital of Traditional Chinese Medicine (No. --2020SHL-KY-30) and other ethics committees at each center. In accordance with the Declaration of Helsinki, participants will not participate in the trial until written informed consent has been obtained. (The Informed Consent is shown in Supplementary Materials 1).
Consent for Publication
The trial results will be published in a peer-reviewed journal or presented at academic conferences. All participants contributing substantively to the trial are recognized in the form of granting authorship. Professional authors are not necessary.
Trial Status
Protocol version 2.0, June 2023. Patient enrollment began on July 6, 2021. Due to the recurrence of COVID-19, the recruitment of participating patients has been slow and is expected to be completed in June 2024.
Acknowledgments
The authors would like to thank all the staff and funders for their hard work in the development of this protocol and their efforts in its future implementation. We gratefully acknowledge the contributions of the following hospitals: (1) Shanghai Municipal Hospital of Traditional Chinese Medicine; (2) Shaanxi Provincial Hospital of Chinese Medicine; (3) The First Affiliated Hospital of Guangzhou University of Chinese Medicine; (4) Chengdu University of Traditional Chinese Medicine.
Funding
This study is supported by grants from the National Key R&D Program of China (NO. 2018YFC2002504) and the Three-Year Action Plan for Public Health 2020–2022 (Key Discipline Construction-TCM psychology/TCM psychiatry), and Shanghai Municipal Health Commission (GWV-10. 1-XK20). The funding sources have had no role in the study design and will not have a role in the execution, analyses, interpretation of the data, or decision to submit results.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Feng YS, Tan ZX, Wu LY, Dong F, Zhang F. The involvement of NLRP3 inflammasome in the treatment of Alzheimer’s disease. Ageing Res Rev. 2020;64:101192.
2. World Health Organization. Global Status Report on the Public Health Response to Dementia. World Health Organization; 2021.
3. Zhang Y, Li Y, Ma L. Recent advances in research on Alzheimer’s disease in China. J Clin Neurosci. 2020;2020:81.
4. As Association. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement. 2021;17(3):327–406. doi:10.1002/alz.12328
5. Grossberg GT, Tong G, Burke AD, Tariot PN. Present algorithms and future treatments for Alzheimer’s disease. J Alzheimers Dis. 2019;67(4):1157–1171. doi:10.3233/JAD-180903
6. As Association. 2020 Alzheimer’s disease facts and figures. Alzheimers Dement. 2020;2020:1.
7. Hane FT, Lee BY, Leonenko Z. Recent progress in Alzheimer’s disease research, part 1: pathology. J Alzheimers Dis. 2017;57(1):1–28. doi:10.3233/JAD-160882
8. Pei H, Ma L, Cao Y, et al. Traditional Chinese medicine for Alzheimer’s disease and other cognitive impairment: a review. Am J Chinese Med. 2020;48(3):487–511. doi:10.1142/S0192415X20500251
9. Klimova B, Kuca K. Alzheimer’s disease and Chinese medicine as a useful alternative intervention tool: a mini-review. Curr Alzheimer Res. 2017;14(6):680–685. doi:10.2174/1567205014666170117103656
10. Shi J, Ni J, Lu T, et al. Adding Chinese herbal medicine to conventional therapy brings cognitive benefits to patients with Alzheimer’s disease: a retrospective analysis. BMC Complem Altern M. 2017;17(1):533. doi:10.1186/s12906-017-2040-5
11. Li Ou ZJXJ. Effect of Xiangxuan Yishen prescription on neuronal apoptosis in vascular dementia rats. Shaanxi J Tradit Chin Med. 2021;42(6):687–691.
12. World MA. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama J Am Med Assoc. 2013;310:20.
13. Administration NMP. Good clinical practice 2020; 2020.
14. JinZhou T, HengGe X, LuNing W, et al. Chinese guidelines for the diagnosis and treatment of Alzheimer’s disease Dementia(2020). Chin J Geriatr. 2021;40:3.
15. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–279. doi:10.1016/j.jalz.2011.03.008
16. Zheng YY. Guidelines for Clinical Research of Chinese Medicine (New Drug). Beijing, China: Chinese Medicine and Science Publication House; 2002.
17. Zhang YL. International clinical practice guide for traditional Chinese medicine Alzheimer disease(2019-10-11). World Chin Med. 2021;16(08):1181–1187.
18. Folstein MF, Folstein SE, McHugh PR. ”Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
19. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
20. Chen TB, Lai YH, Ke TL, et al. Changes in plasma amyloid and tau in a longitudinal study of normal aging, mild cognitive impairment, and Alzheimer’s disease. Dement Geriatr Cogn. 2019;48(3–4):180–195. doi:10.1159/000505435
21. Mielke MM, Hagen CE, Wennberg A, et al. Association of plasma total tau level with cognitive decline and risk of mild cognitive impairment or dementia in the mayo clinic study on aging. Jama Neurol. 2017;74(9):1073–1080. doi:10.1001/jamaneurol.2017.1359
22. Zhao S, Zhang L, Yang C, Li Z, Rong S. Procyanidins and Alzheimer’s Disease. Mol Neurobiol. 2019;56(8):5556–5567. doi:10.1007/s12035-019-1469-6
23. Yang G, Wang Y, Tian J, Liu JP. Huperzine A for Alzheimer’s disease: a systematic review and meta-analysis of randomized clinical trials. PLoS One. 2013;8(9):e74916. doi:10.1371/journal.pone.0074916
24. Singh SK, Srivastav S, Castellani RJ, Plascencia-Villa G, Perry G. Neuroprotective and antioxidant effect of ginkgo biloba extract against AD and other neurological disorders. Neurotherapeutics. 2019;16(3):666–674. doi:10.1007/s13311-019-00767-8
25. Gregory J, Vengalasetti YV, Bredesen DE, Rao RV. Neuroprotective herbs for the management of Alzheimer’s disease. Biomolecules. 2021;11(4):543. doi:10.3390/biom11040543
26. Zhao YN, Wu XG, Li JM, Chen CX, Rao YZ, Li SX. 中药补阳还五汤对沙鼠脑缺血再灌注损伤及微循环障碍的治疗作用 [Effect of BuYangHuanWu recipe on cerebral microcirculation in gerbils with ischemia-reperfusion]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2010;41(1):53–56. Chinese.
27. Kim MS, Bang JH, Lee J, et al. Salvia miltiorrhiza extract protects white matter and the hippocampus from damage induced by chronic cerebral hypoperfusion in rats. BMC COMPLEM ALTERN M. 2015;15:415. doi:10.1186/s12906-015-0943-6
28. Zhang ZL, Gao YG, Zang P, et al. 天麻素对羟基苯甲醇对中枢神经系统作用机制研究进展 [Research progress on mechanism of gastrodin and p-hydroxybenzyl alcohol on central nervous system]. Zhongguo Zhong Yao Za Zhi. 2020;45(2):312–320. Chinese. doi:10.19540/j.cnki.cjcmm.20190730.401
29. Lin LW, Tsai FH, Lan WC, Cheng YD, Lee SC, Wu CR. Steroid-enriched fraction of achyranthes bidentata protects amyloid beta peptide 1-40-induced cognitive dysfunction and neuroinflammation in rats. Mol Neurobiol. 2019;56(8):5671–5688. doi:10.1007/s12035-018-1436-7
30. Wei S. Potential therapeutic action of natural products from traditional Chinese medicine on Alzheimer’s disease animal models targeting neurotrophic factors. Fund Clin Pharmacol. 2016;30(6):490–501. doi:10.1111/fcp.12222
31. Mikami M, Takuya O, Yoshino Y, et al. Acorus calamus extract and its component alpha-asarone attenuate murine hippocampal neuronal cell death induced by l-glutamate and tunicamycin. Biosci Biotech Bioch. 2021;85(3):493–501. doi:10.1093/bbb/zbaa071
32. Sun Y, Liu Z, Pi Z, Song F, Wu J, Liu S. Poria cocos could ameliorate cognitive dysfunction in APP/PS1 mice by restoring imbalance of Aβ production and clearance and gut microbiota dysbiosis. Phytother Res. 2021;35:2678–2690. doi:10.1002/ptr.7014
33. Li J, Du Q, Li N, Du S, Sun Z. Alpiniae oxyphyllae Fructus and Alzheimer’s disease: an update and current perspective on this traditional Chinese medicine. Bio Pharmacoth. 2021;135:111167. doi:10.1016/j.biopha.2020.111167
34. Khan S, Barve KH, Kumar MS. Recent advancements in pathogenesis, diagnostics and treatment of Alzheimer’s disease. Curr Neuropharmacol. 2020;18(11):1106–1125. doi:10.2174/1570159X18666200528142429
35. Illan-Gala I, Lleo A, Karydas A, et al. Plasma tau and neurofilament light in frontotemporal lobar degeneration and Alzheimer disease. Neurology. 2021;96(5):e671–e683. doi:10.1212/WNL.0000000000011226
36. Janelidze S, Stomrud E, Palmqvist S, et al. Plasma beta-amyloid in Alzheimer’s disease and vascular disease. Sci Rep. 2016;6:26801. doi:10.1038/srep26801
37. Grapow MT, von Wattenwyl R, Guller U, Beyersdorf F, Zerkowski HR. Randomized controlled trials do not reflect reality: real-world analyses are critical for treatment guidelines. J Thorac Cardiov Sur. 2006;132(1):5–7. doi:10.1016/j.jtcvs.2006.03.035
38. Price D, Brusselle G, Roche N, Freeman D, Chisholm A. Real-world research and its importance in respiratory medicine. Breathe. 2015;11(1):26–38. doi:10.1183/20734735.015414
39. Knottnerus JA, Tugwell P. Real world research. J Clin Epidemiol. 2010;63(10):1051–1052. doi:10.1016/j.jclinepi.2010.08.001
40. Ford I, Norrie J. Pragmatic Trials. New Engl J Med. 2016;375(5):454–463. doi:10.1056/NEJMra1510059
41. Kremers HM. Methods to analyze real-world databases and registries. Bull Nyu Hosp J Dis. 2009;67(2):193–197.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.