")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Effectiveness and Quality of Life with Paliperidone Palmitate 3-Monthly in Comparison with Other Long-Acting Drugs
Authors Di Lorenzo R, Iorio A, Pinelli M, Magarini F, Marchi M , Sacchetti A , Calogero C, Galeazzi GM, Ferri P , Rovesti S , Minarini A
Received 11 January 2022
Accepted for publication 10 March 2022
Published 12 April 2022 Volume 2022:18 Pages 829—846
DOI https://doi.org/10.2147/NDT.S356341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Rosaria Di Lorenzo,1 Anita Iorio,2 Margherita Pinelli,3 Federica Magarini,3 Mattia Marchi,3 Andrea Sacchetti,3 Chiara Calogero,4 Gian Maria Galeazzi,5 Paola Ferri,5 Sergio Rovesti,5 Alessandro Minarini6
1Service of Psychiatric Diagnosis and Care, Department of Mental Health and Pathological Addictions, AUSL-Modena, Modena, Italy; 2Psychiatric Rehabilitation Technique Programme, University of Modena and Reggio Emilia, Reggio Emilia, Italy; 3School of Psychiatry, University of Modena and Reggio Emilia, Modena, Italy; 4Community Mental Health Center, Vignola (MO), Department of Mental Health and Pathological Addictions, AUSL-Modena, Modena, Italy; 5Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy; 6Community Mental Health Center, Vignola (MO), Department of Mental Health and Pathological Addictions, AUSL-Modena, Modena, MO, Italy
Correspondence: Rosaria Di Lorenzo, Department of Mental Health and Pathological Addictions, AUSL-Modena, Service of Psychiatric Diagnosis and Care, via P. Giardini n. 1355, Baggiovara (MO), 41126, Italy, Email [email protected]
Purpose: Antipsychotic long-acting injections (AP-LAIs) are indicated for patients affected by schizophrenia especially those with poor treatment adherence.
Patients and Methods: To compare paliperidone palmitate 3-monthly (PP3M), paliperidone palmitate one-monthly (PP1M) and haloperidol decanoate (HAL-D) treatment, we enrolled 90 patients with schizophrenia treated in Mental Health Center with one of the three AP-LAIs for at least six months and followed them for another 6 months. At 6 and 12 months of treatment we administered Clinical Global Impression-Severity, Global Assessment of Functioning and World Health Organization Quality of Life-26 items (WHOQOL-BREF). At 1-year treatment, we evaluated relapses (psychiatric hospitalizations and urgent consultations), side effects and drop-outs.
Results: We did not highlight any statistically significant difference among the three treatments in relapses and scale scores. Weight increase was significantly higher in PP1M and PP3M groups. Twelve patients (13.3%) discontinued AP-LAI. At 1-year AP-LAI treatment, 69% of patients rated quality of life as “good” or “very good” and 71% declared themselves to be “satisfied” or “very satisfied”.
Conclusion: HAL-D, PP1M and PP3M 1-year treatments were similarly effective in preventing relapses and improving quality of life and health satisfaction. All discontinuations in the new 3-monthly antipsychotic treatment were caused by patient refusal to continue it.
Keywords: antipsychotic long-acting injections, schizophrenia spectrum disorders, relapses, quality of life, health satisfaction
Introduction
Schizophrenia is a complex and severe mental disorder, which presents early onset and, in most cases, disabling lifelong course, with a global age-standardized prevalence ranged between 0.3–0.7%, without gender differences.1 Schizophrenia burden is heavy in terms of economic implications,2,3 social functioning and quality of life (QOL).4 The improvement of quality of life represents an important target in mental health context; in patients with schizophrenia, QOL is notably influenced by the severity of symptoms and cognitive impairment.5 A recent meta-analysis has shown that schizophrenic patients have lower QOL not only in the psychological domains, but also in the physical, social and environmental ones.6 For this reason, schizophrenia guidelines suggest implementing treatments focused on improving patients’ QOL and their adaptive skills in a recovery-oriented approach.7,8 Quality of life and social functioning play a fundamental role in adherence to treatment and patient satisfaction, thereby influencing clinical and prognostic outcomes.9
Up to now, antipsychotic drugs represent the primary treatment of schizophrenia for reducing positive symptoms due to their antagonism efficacy on dopamine D2 receptors located in the mesolimbic pathway.10,11
Poor treatment adherence with oral antipsychotic medication is a common occurrence among patients with schizophrenia and is associated with risk of relapses and hospitalizations.12 A recent study highlighted that nonadherence to oral antipsychotic drug treatments (OAPs) represents the most frequent reason for relapses, which are very common in patients with schizophrenia.13 Relapses lead to higher rates of hospitalization and further deterioration in global function.14–16 Relapse prevention represents a critical issue in long-term treatments of schizophrenia.
Long-acting injectable antipsychotic drugs (LAIs) have been formulated over the last few years in order to improve patients’ medication adherence, inducing lower discontinuation risk compared to oral antipsychotic drugs,17,18 also in patients with early psychosis.19 On the other hand, as a recent study has highlighted, some barriers to LAIs use could be represented by the patients’ perceptions regarding this treatment as invasive, painful or coercive.20 Differently, another recent study has pointed out that patients tend to prefer LAI drugs because they feel “healthier” and able to “return to their favourite activities without worrying about taking daily oral therapy”.21
The kinetics of LAIs guarantee adequate plasma concentrations sufficient to prevent relapses over the intervals of weeks or months between intramuscular injections.22 Compared to oral antipsychotic drugs, LAIs offer greater dosing precision, minimize peak-trough level differences, provide more reliable drug delivery and reduce adverse effects such as autonomic symptoms and tardive dyskinesia.23,24
Retrospective observational studies proved to be more suitable than randomized controlled studies in comparing LAIs and OAPs efficacy, in particular for showing the superior efficacy of LAIs in preventing relapses.25 A study, implemented in a Finnish cohort of over 2000 schizophrenic patients discharged after their first hospitalization, showed that patients treated with LAIs (fluphenazine decanoate, zuclopenthixol acetate, haloperidol decanoate and risperidone) presented lower rates of therapy discontinuation and re-hospitalizations in the following two years compared to those who received OAPs.26 A similar cohort study, conducted by the same authors on over 29,000 patients from 2006 to 2013, highlighted that LAIs as well as clozapine were associated with the lower number of relapses, both in terms of hospitalizations and clinical worsening.27 A meta-analysis of 25 mirror design studies comparing OAP and LAIs treatments in the same patient showed that LAIs are more effective than OAPs in preventing relapses, decreasing both number and duration of Psychiatric hospitalizations; these results were confirmed in the groups treated with different antipsychotics, both first generation antipsychotic (FGA) and second generation antipsychotic (SGA).28 Another study confirmed that patients in therapy with LAIs had lower rates of hospitalization and that LAIs improved quality of life and reduced health care costs.29
A systematic review focused on the comparison between oral and long-acting antipsychotics highlighted that both pharmacological formulations present overlapping efficacy and tolerability, with the only exception LAI aripiprazole, compared to its oral formulation.30 Most studies highlighted that patients with schizophrenia who received LAIs presented lower rates of hospitalizations and shorter lengths of hospitalizations than patients treated with OAPs.31–35 A recent meta-analysis showed that SGA-LAIs formulations presented many advantages compared to the FGAs in terms of tolerability, subjective well-being, positive attitudes towards treatment and QOL.36 The same study also found that both modality and frequency of LAIs administration could reduce the risk of self-stigma, improving social acceptability and daily-life activities.
Nowadays, no guidelines indicating which LAIs can be used in specific clinical cases are available. In any case, some authors highlighted that, although differences in specific clinical dimensions have been observed, no evidence is available indicating the better efficacy of a LAI than others.37 The randomized QUALIFY study compared paliperidone palmitate to aripiprazole long-acting formulation;38 both treatments were associated with good tolerability, even if PP1M caused more adverse effects with higher discontinuation rate and aripiprazole long-acting formulation showed better long-term outcomes in terms of quality of life and efficacy, especially in younger patients, results confirmed by another study.39 On the contrary, other two studies highlighted the better efficacy of PP1M associated with a better quality of life and low relapse rate in comparison with other SGA-LAIs.40,41 The use of paliperidone palmitate one-monthly formulation (PP1M) compared to both FGA and SGA-LAIs in schizophrenia highlighted similar efficacy in improving disease severity and hospitalization rate with reduced extrapyramidal symptoms.42,43 These results were in accordance with those of another study and were further confirmed by a recent review.44,45 A study conducted in six different US states highlighted a reduction in healthcare costs due to the decrease in hospital and residential stays with SGA-LAI use, which seem economically advantageous despite their higher cost compared to oral therapy.46 An observational Italian study, comparing haloperidol decanoate, paliperidone palmitate and aripiprazole long-acting formulations, highlighted similar efficacy in reducing psychiatric hospitalizations and urgent consultations with superimposable clinical improvement.47 Few studies focused on the comparison between PP1M and palmitate three-monthly formulation (PP3M) regarding their clinical and economic impact on schizophrenic course. One study found that both PP1M and PP3M presented similar efficacy in relapse and discontinuation rate.48 A review highlighted that PP3M was effective in maintaining a longer symptoms-free period after discontinuation.49 A French study reported a reduction in global costs (therapy and relapse related costs) and a better QALY (quality adjusted life years) when using PP3M rather than PP1M.50
The results of a study conducted on the Medicaid care program for low-income people showed that both PP1M and PP3M use reduced hospitalizations compared to treatment with oral antipsychotics.51 Another study reported equal levels in both therapeutic adherence and healthcare cost utilization before and after the transition from PP1M to PP3M.52 A real-world survey carried out by the same authors on a sample of 152 patients suggested that the switch to PP3M from PP1M may be associated with improved adherence and a concomitant reduction in comorbidities (substance abuse and diabetes) without any increase in health costs.53 Well-being and quality of life appeared to be the priorities for choosing LAI. In particular, the choice of PP3M can be motivated by fewer injections whereas PP1M can be chosen for its flexibility in dosage. A better understanding of patients’ views on therapy and greater sharing in its implementation could therefore overcome the barriers against LAI and foster more personalized treatment for schizophrenia, improving patient satisfaction and therapeutic adherence.21
The aim of this observation study was to compare the effectiveness and quality of life of one-year treatment of paliperidone palmitate three-monthly formulation (PP3M), a recently introduced drug, with two other LAIs available in clinical practice, paliperidone palmitate one-monthly formulation (PP1M) and haloperidol decanoate, among a group a patients with schizophrenia spectrum disorders treated in outpatient Mental Health Centre.
Materials and Methods
The Design, The Period and the Place of the Study
Observational cohort study. Data collection was both retrospective, as regards the selection of the sample, and prospective, upon reaching at least 12 months of LAI therapy for outcome evaluation. Data collection and processing period: from 1st June 2019 to 28th October 2020. Place of activity: all outpatient community Mental Health Centers (MHCs) of the Department of Mental Health and Pathological Addictions of AUSL-Modena.
LAI Drugs
We compared PP3M,54 a recently introduced drug, with monthly paliperidone (PP1M),55 the same drug but with different bio-availability for a less extensive formulation over time, and with the haloperidol decanoate (HAL-D),56 a gold standard of first generation long-acting drugs, available for a long time in clinical practice and, to date, one of the most used formulations, also within our MHCs.
The Sample
We selected all patients diagnosed with schizophrenic spectrum disorders, according to the ICD-9-CM (2007), treated with one of the three LAIs at the MHCs of the Department of Mental Health and Pathological Addictions of AUSL-Modena, in accordance with our inclusion criteria:
• age over 18 years;
• informed consent;
• LAI therapy for at least 6 months.
We included patients who started LAI after switching from either oral or another long-acting antipsychotic drug. During the observation period of the study, patients could concomitantly take other oral psychiatric drugs in accordance with the referring therapist recommendations.
The Selected Variables of Our Sample
For each patient the following were examined:
1. Demographic variables: age, gender, nationality, marital status, occupational status, housing environment, socio-economic problems.
2. Clinical variables: psychiatric diagnosis according to International Classification of Diseases-9th revision-Clinical Modification,57 years of psychiatric illness, psychiatric, substance/alcohol abuse and medical co-morbidities.
3. Pharmacological variables: reason for introducing the LAI antipsychotic into therapy (ineffectiveness of previous therapy, lack of therapy adherence, adverse effects with previous therapy), switch from previous LAI or oral therapy, mean dose, interval between administrations, number of administrations in a year, oral drugs associated.
The demographic, clinical and pharmacological variables of the three groups were compared to evaluate the sample homogeneity.
Clinical data were collected from patient medical records, MHC information systems and, if necessary, from the psychiatrist who treated the patient.
The Scales Administered
The quality of life was assessed by administering the Italian version of the World Health Organization quality of life-26 items (WHOQOL-BREF), a tool developed by the WHO which investigates four areas concerning quality of life: physical health, psychological conditions, social relations, environment.58 The answers are expressed on a 5-level Likert scale (1=very dissatisfied, 5=very satisfied); the score is subsequently converted into a scale of 4–20 to make it comparable with WHOWQOL-100 and subsequently processed into a standardized score ranging from 1 to 100. Separately, the first two questions are processed: question no. 1 relating to overall perception of quality of life and question 2 relating to the satisfaction with health conditions.
The Clinical Global Impression-Severity (CGI-S) scale is a 7-point scale that requires the physician to rate the severity of the patient’s disease at the time of assessment, on a scale ranging from 1 (no disease) to 7 (disorder extremely severe).59
The scale for the Global Assessment of Functioning (GAF), which expresses the clinician’s judgment of global functioning (social, occupational and psychological) in a score ranged between 1 (severely impaired) to 100 (extremely high operation). The GAF is reported on the V Axis of the DSM IV.60
Outcomes
We compared the following outcomes in the three LAI groups during 1-year treatment:
• number of urgent psychiatric consultations;
• number and days of psychiatric hospitalizations;
• adverse effects and weight increase as change in Body Mass Index (BMI);
• number of drop-out patients and reasons for therapy interruption.
We evaluated the WHOQOL-BREF, GAF and CGI-S scale scores in the three LAI groups at 6 and 12 months of treatment.
Statistical Analysis
Descriptive statistical tests were applied: mean ± standard deviation and t-test for continuous variables; percentages and chi-squared for categorical variables. Cronbach’s alpha was applied to evaluate the internal consistency of the WHOQOL-BREF scale. The Spearman correlation and the multiple simple linear regression model (backward stepwise model) were used to highlight possible correlations between CGI-S, GAF and WHOQOL-BREF scores (dependent variables) and the variables selected (independent variables). Statistical analysis was carried out using STATA programs (Stata version 12, 2011). The level of statistical significance was set at p <0.05.
Ethical Considerations
The study was conducted according to the principles of the Declaration of Helsinki. We obtained the approval of the Ethics Committee of the Vasta Emilia Nord Area (Prot.n.0009228/19 of 28/03/2019) and the authorization of the AUSL of Modena (Decision Number 1104 of 23/05/2019). Before participating in the study, each patient gave his/her written informed consent. Scales were administered after patient’s written informed consent. For each patient, the collected data were transformed into numerical code then anonymously reported in an Excel database by the study researchers.
Results
Demographic and Clinical Characteristics of the Sample
Our sample consists of 90 patients who agreed to participate in this study after having provided their written informed consent. Only 3 patients who were asked to participate in the study were excluded because they refused to provide their informed consent. The patients of our sample were divided into three groups based on the AP-LAI treatment: HAL-D (n=37), PP1M (n=27) and PP3M (n=26). After 6 months of treatment, 12 patients (13.3%) discontinued therapy with AP-LAI due to different reasons, as shown in Table 1: patient refusal (6.7%), medical indications (3.3%), ineffectiveness (1.1%), side effects (1.1%), death (1.1%). Other 5 patients (5.6%) switched from PP1M to PP3M.
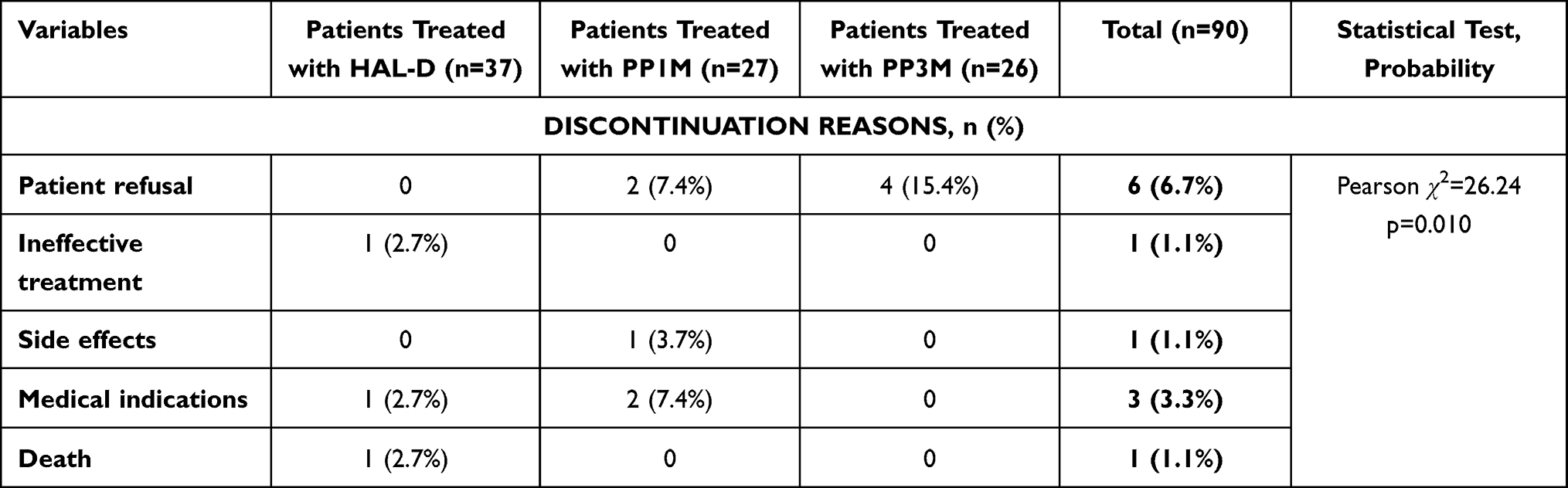 |
Table 1 Reasons for AP-LAI Discontinuation at 6 Month Treatment |
The demographic characteristics of the three treatment groups and the patients who discontinued statistically significantly differed for two variables: occupational status (p=0.003), with a significant prevalence of employed patients in the PP3M group (59.2%), and socio-economic problems (need for support from the social service), which was more frequent in the group treated with HAL-D (37.9%) and in that of patients who stopped treatment (41.4%). Among the demographic characteristics of patients who discontinued the AP-LAI therapy we observed the prevalence of males (64.4%), an average age of over 50 years, and the Italian nationality (Table 2).
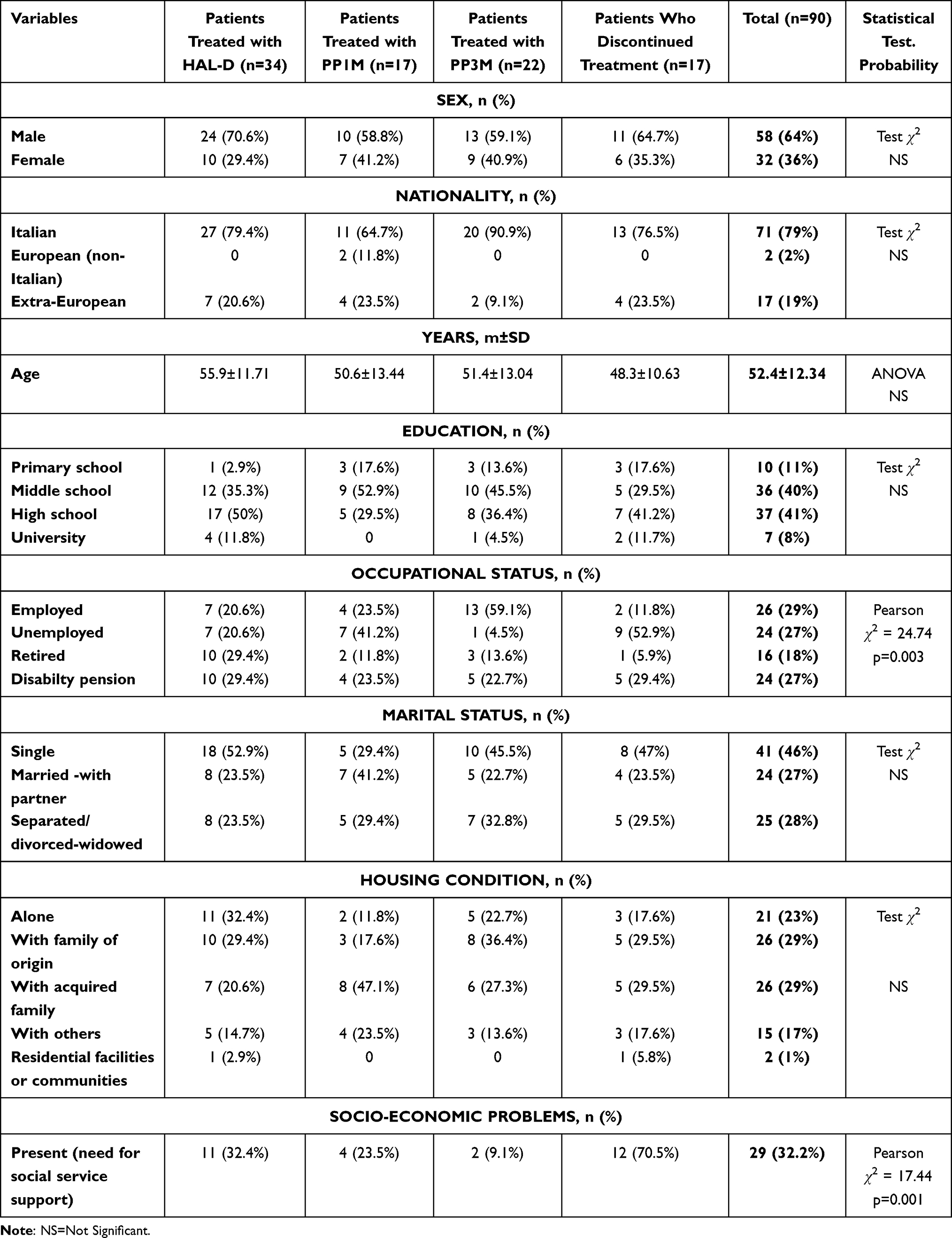 |
Table 2 Demographic Characteristics of the Sample |
In the three treatment groups, the diagnosis of “paranoid schizophrenia” was prevalent in the groups treated with HAL-D (32.4%) and PP3M (31.8%), while the diagnosis of “undifferentiated schizophrenia” prevailed in the PP1M group (35.4%) and that of “delusional disorders” in the PP3M group (Table 3).
 |
Table 3 Clinical Characteristics of the Sample |
The sample was homogeneous for psychiatric comorbidities (including alcohol or substance abuse), present in 18.9% of individuals (Table 3). The prevalence of medical comorbidity was also homogeneously distributed in the three treatment groups, with an average prevalence of 50%. In particular, 50% of patients had only one medical comorbidity; 48% had at least two comorbidities. The most frequent medical comorbidity was diabetes mellitus, followed by dyslipidaemia and arterial hypertension. In our sample, 55 individuals (75%) presented a BMI ≥ 25, which is the threshold for overweight, with average BMI of 27.46.
The three groups statistically significantly differed (ANOVA, F=6.49, p=0.0005) for the illness duration, which was significantly longer in patients treated with HAL-D compared to the PP1M 11.76±8.34 and the PP3M (12.23±5.03) group (Table 3).
Pharmacological Variables in the Three AP-LAI Groups
The clinical reasons for the introduction of long-acting therapy do not differ between the three LAI groups, in which poor adherence was the prevalent motivation (89%) (Table 4). We observed a statistically significant difference (p=0.0000) in the duration of treatment with the long-acting drug, which was approximately three and a half years in the HAL-D group, approximately two and a half in the PP1M and almost two years for the PP3M (Table 4). The mean LAI antipsychotic posology taken during the evaluation period was 112.5 mg (median 100 mg, with min-max values: 25–225 mg) for HAL-D, 85.29 mg (median 75 mg, with min-max values: 50–150 mg) for PP1M, and 293.27 mg (median 263, with min-max values: 175–525 mg) for PP3M (Table 4). The average interval between administrations was different in accordance with the prescription indications: 25.56 days for HAL-D, 29.35 for PP1M and 87.27 for PP3M.
 |
Table 4 Pharmacological Variables of AP-LAI Treatments |
Associated oral drugs were prescribed in 64.4% of the sample on average. The three LAI treatment groups differed statistically significantly at both 6 months (p=0.011) and 12 months (p=0.002) for associated oral therapy, which prevailed in the HAL-D group (Table 4). No statistically significant difference was observed between 6 and 12 months of all three AP-LAI treatments. Regarding the pharmacological classes of the associated therapies, we did not observe any statistically significant difference in the three treatment groups (Figure 1).
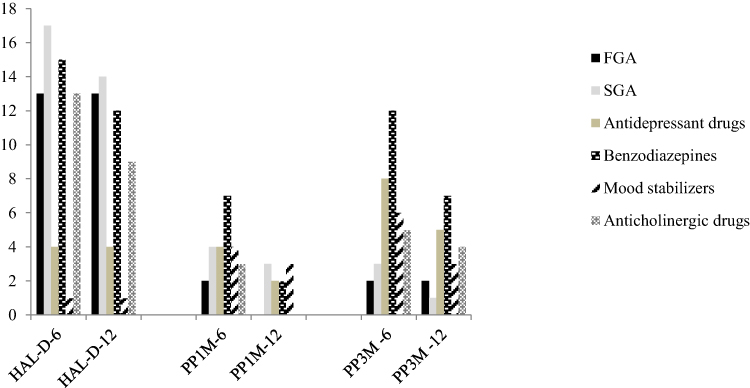 |
Figure 1 Oral drugs associated with the LAI treatments. |
Urgent Psychiatric Consultations, Hospitalizations and Side Effects at 1-Year AP-LAI Treatment
Comparing the three AP-LAI treatments, there were no statistically significant differences in urgent psychiatric consultations or in the number and days of hospitalizations (ANOVA test) after 12 months of AP-LAI treatments (Table 5). 49.3% of patients in the three treatment groups presented side effects (Table 5), with a statistically significant difference in the three groups (p=0.001): more individuals (41.7%) in the PP1M and PP3M groups complained of adverse effects (Table 5). In particular, weight gain prevailed, in a statistically significant way, in the PP3M and PP1M groups (Table 5).
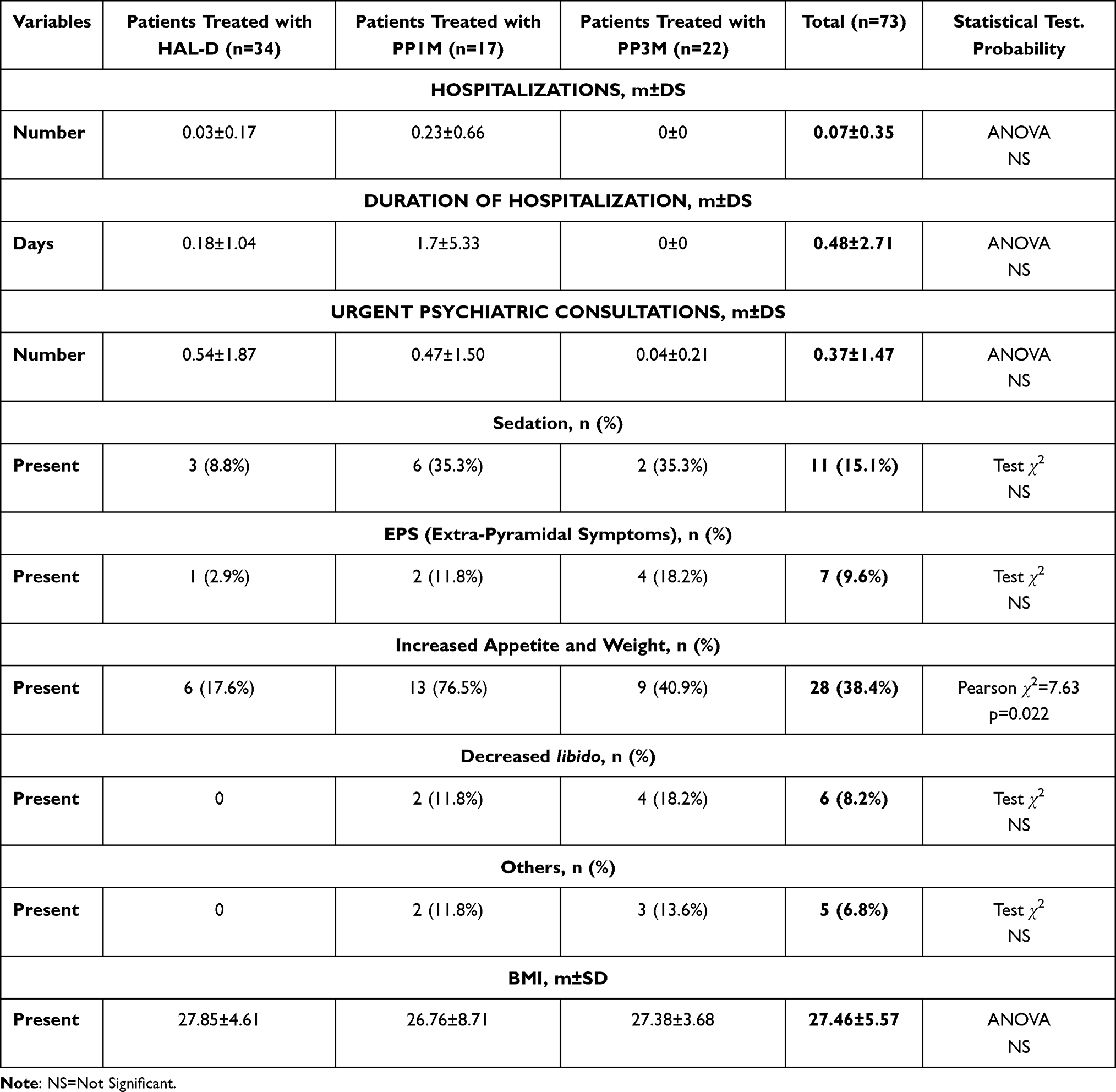 |
Table 5 Hospitalizations. Urgent Psychiatric Consultations and Side Effects in 1-Year AP-LAI Treatments |
CGI-S, GAF and WHOQOL-BREF Scale Scores at 6- and 12-Month AP-LAI Treatment
The mean score of the CGI-S scale did not show any statistically significant difference in the three treatment groups, characterized by mild severity (“at the limit of normal”) (Table 6). Likewise, the GAF scale scores were similar in the three groups, with a medium-high level of global functioning (Table 6). The score of the CGI-S scale at 6 months did not differ statistically from that obtained at 12 months of treatment, whereas the GAF scores showed a statistically significant reduction at 12 months compared to those at 6 months, suggesting a further improvement in global functioning (GAF-12 months: m=66.78 ± 1.64 SD; GAF-6 months: m=68.35 ± 1.56 SD; t=−2.44, p=0.01, t-test).
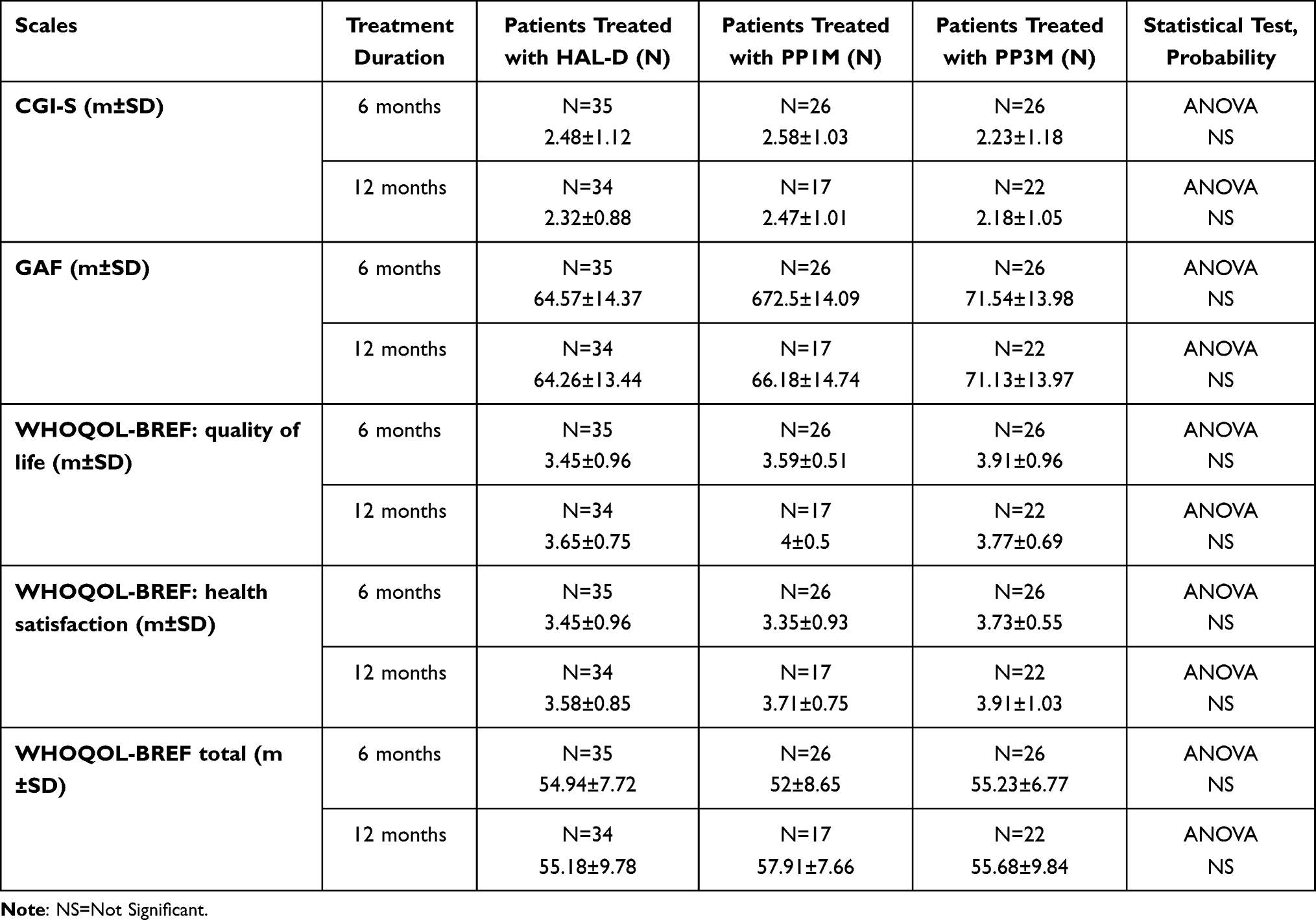 |
Table 6 CGI-S. VGF e WHOQOL-BREF Scores at 6 and 12-Month AP-LAI Treatments |
The score of the two items of the WHOQOL-BREF scale, which assess general quality of life and perception of health respectively, showed that 69% of the respondents rated the quality of life as “good” or “very good”, whereas 3% called it “bad” or “very bad”. 71% also stated that they were “satisfied” or “very satisfied” with their health, while 13% were “dissatisfied” or “very dissatisfied”. The percentage of individuals who showed a better perception of Quality of Life (QOL) and their own health satisfaction (HS) appeared significantly increased after 12 months of treatment with AP-LAI compared to the previous 6 months, as shown in Figure 2 (12-month QOL vs 6-month QOL: Pearson chi2=36.6; p=0.000; 12-month HS vs 6-month HS: Pearson chi2 =33.85; p=0.006).
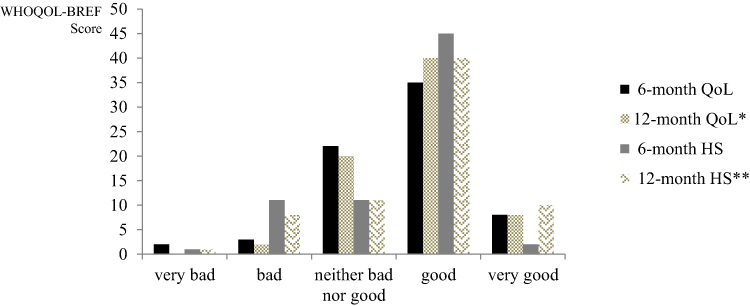 |
Figure 2 The quality of life (QOL) and health satisfaction (HS) scores at 6 and 12 months of treatment with AP-LAI (*vs 6-month QoL, Pearson chi2=36.6; p=0.000 **vs 6-month HS, Pearson chi2 =33.85; p=0.006). |
Regarding the total scale and four domain WHOQOL-BREF scores, we did not appreciate any statistically significant differences in the three AP-LAI treatment groups (Table 6). The reliability of the WHOQOL-BREF scale was confirmed by the value of Cronbach’s alpha equal to 0.92, which indicates a good internal consistency.
The 12-month WHOQOL-BREF score did not correlate statistically significantly with 12-month CGI-S and GAF scale scores in the three AP-LAI treatment groups, whereas, the 12-month CGI-S and GAF scale scores in the three LAI treatment groups were statistically significantly correlated (Spearman’s rho=−0.75, p=0.000).
The multiple linear regression model showed a statistically significant negative correlation of the WHOQOL-BREF total score with three variables (Table 7): medical comorbidity, presence of socioeconomic problems, and length of hospitalization during the LAI treatment period.
 |
Table 7 Statistically Significant Regressions Between WHOQOL-BREF, GAF and CGI-S Scores and Selected Variables |
In our multiple linear regression model, the GAF score was negatively correlated with the 12- month CGI-S score and with the length of hospitalization during the LAI treatment period, and, positively with medical comorbidity, in a statistically significant way (Table 7). The CGI-S score was positively correlated with the number of urgent psychiatric consultations, disability pension, unemployment and, indirectly, with the prescription of PP3M, in a statistically significant way (Table 7).
Discussion
The present study compared the effectiveness and quality of life of 1-year treatment with a new long-acting antipsychotic, paliperidone palmitate 3-monthly (PP3M), with its monthly equivalent, PP1M, and a typical AP-LAI, haloperidol decanoate (HAL-D).
The patients in the three AP-LAI groups were statistically comparable for most demographic and clinical characteristics, differing significantly only for employment, presence of socio-economic problems and duration of illness. In particular, employed persons were mostly represented in the PP3M group, unemployed prevailed in the PP1M group and people retired due to disability in the group with HAL-D. Long duration of illness, high number of hospitalizations over life course and disability pensions were the statistically significantly more frequent characteristics among HAL-D group patients than in the other two groups. Similarly, the period of long-acting treatment differed in the three groups, being markedly longer for the HAL-D group, in line with the longer clinical history of these patients, probably because haloperidol decanoate has been used for many years in clinical practice. Therefore, our group of patients treated with HAL-D could be representative of a population with long-term maintenance therapy, as suggested by their long history of disease and disability. Furthermore, the differences in the demographic and clinical characteristics of the three treatment groups can be explained by the prescribing guideline indications, which recommend prescribing a SGA in newly diagnosed patients with schizophrenia, for their better profile in terms of neurological side effects and greater patient therapeutic adherence.36,61
Regarding the group of patients treated with PP3M, our preliminary results confirm that, in accordance with the guideline indications, the therapists proposed it to clinically stable patients. This observation was further supported by the result of multiple linear regression, which showed an inversely significant correlation between the clinical severity scale (CGI-S) score and the PP3M prescription. Moreover, the majority of patients treated with PP3M had regular employment and therefore they could benefit from longer drug administration times.
In our sample, medical comorbidity was highly represented, being present in 50% of patients, with a prevalence of metabolic diseases: 75% of our patients had a ≥25 BMI with an average BMI of 27.46 indicating a state of overweight. This observation is in line with the literature, which reports a high percentage of metabolic syndrome in patients with schizophrenia.62
Among our sample, 12 patients discontinued the treatment due to various reasons represented more often by patient refusal, immediately followed by the change of therapy from PP1M to PP3M.
In particular, in our sample, all discontinuation of PP3M therapy (15.4% of all patients) was caused by patient refusal to continue it. The number of patients who persisted in LAI treatments is higher than that reported by international literature,63 probably because the patients enrolled in this study were more careful followed during the LAI treatments, showing the so-called Hawthorne effect. In any case, our sample can be representative of both Italian patients and mental health service organization due to the real world design of this study. A recent study has reported a dropout rate of 5% in the population treated with PP3M for one-year, of which 57% discontinued this LAI treatment due to patients’ refusal to continue the treatment.64 Among demographic characteristics, the patients who discontinued AP-LAI treatment were more frequently unemployed, living with a disability pension or presenting socio-economic problems, suggesting that precarious socio-environmental conditions can reduce adherence to therapy, as reported by other authors.65,66 Furthermore, the older age of patients treated with HAL-D could be inversely related to the likelihood of stopping treatment with LAI due to longer psychiatric treatments performed or to social environmental conditions such as being retired, as suggested by other authors.67
In our sample, lack of therapy adherence represented the main reason for choosing all three LAIs, in accordance with international guidelines.7,29,68,69 The prescription of AP-LAI represented a choice of the patient in only 6.8% of our sample.
Our results show that the average posology of the three AP-LAIs was lower than the maximum doses indicated in the technical data sheet. This data, comparable to that of other studies,29,38,70 indicates the prudential attitude of therapists, which is in accordance with most recent guidelines that recommend prescribing the minimum effective dosage.68 In particular, the relatively smallest dosages were used in HAL-D treatment, probably due to the known cardiologic and neurological side effects of this drug, although some clinical studies indicate a dose of 200 mg/month as the most effective dose for preventing relapses.71 The prudent prescription of LAI drugs was indirectly confirmed by the frequent use of associated oral therapy, which we observed especially in the HAL-D group, probably due to the low doses prescribed.
Regarding the primary outcomes of the study we found that, during the 12-month treatment period with the three AP-LAIs, there were no significant differences in the number and days of psychiatric hospitalizations or in urgent psychiatric consultations, in line with most studies on AP-LAI.72–77 As evidenced by the registration studies, the new 3-monthly AP-LAI showed a similar efficacy in comparison with the other monthly treatments.48
Our research did not report any significant difference in the scale scores between 6 and 12 months of AP-LAI treatments in the three groups, but put in evidence that the perception of QOL and health satisfaction were much improved at the end of 1-year AP-LAI treatments in comparison with the previous 6 months. These results suggest that our sample was composed of clinically stable patients, probably maintained so by LAI treatments, which had progressively greatly favoured the improvement of their personal well-being. In fact, the improvement of psychiatric symptoms can favourably condition the psychological dimension and, indirectly, also the physical and social dimensions, all determining factors in the subjective quality of life. In our opinion, the clinical stabilization obtained by our patients with AP-LAI therapy could explain the good quality of life, which, in turn, could reinforce treatment adherence, in line with other studies that highlighted the close correlation between quality of life perception and clinical improvement.78 The regression between the total WHOQOL-BREF score and our selected variables suggests that medical comorbidity, precarious socio-economic conditions and duration of hospitalizations could be the worsening factors for quality of life, as potential conditions of behavioural regression and social exclusion, as indicated by other studies.78,79 This result is in line with the correlations we found between some variables and specific areas of WHOQOL-BREF, indicating that good medical, relational and social conditions can favourably condition QOL and in turn conditioned attitude towards therapy.80 The good value of Cronbach’s alpha confirms the reliability of WHOQOL-BREF scale for measuring quality of life also studies in a naturalistic setting, as observed by some authors.79
Finally, based on our preliminary data, we highlight that PP3M treatment showed equally effective in preventing relapses as monthly paliperidone palmitate and a gold standard such as haloperidol, similarly improving quality of life in our patients after 12 months of treatment. This result is in line with that reported by other recent studies.52,53,81,82 Nevertheless, the relative high rate of PP3M discontinuation due to patients’ refusal should draw our attention to the lack of therapeutic adherence exhibited by patients with schizophrenia, which is not overcome by well-tolerated and stigma-reducing treatments such as PP3M. We can hypothesize that the extended interval between injections, which allows patients greater freedom from therapy, should be integrated into a new therapeutic attitude of the outpatient service in order to promote good adherence to treatment even in this less stringent therapeutic modality. Therefore, we emphasize that more attention to patient therapy attitude and patient-reported outcomes permit us to prescribe a tailored treatment, preventing its discontinuation.36
Limitations and Advantages of the Study
This study can be considered preliminary given the small sample size, conditioned by the recent and non-extensive use of PP3M therapy. Furthermore, the non-homogeneity of treatment duration in the three AP-LAI groups and the relatively short observation period constitute other important limits due to the observational nature of this study. Other limits are strictly related to study observational design: it was not possible to compare patients’ medical conditions before starting LAI treatments because many data were not available for all participants (eg the measurement of BMI, which only currently is part of routine clinical practice; laboratory metabolic profiles, lipid and carbohydrate, etc.); the extrapyramidal effects were not measured in a standardized way (with the administration of specific scales). Moreover, nonrandomized sample, lack of control group represent other limitations of this study.
Despite the aforementioned limitations, our study represents a faithful observation of psychiatric treatments in an outpatient service. Moreover, this study has the merit of having analyzed not only data relating to psychopathology or drug treatment, but also the perception of subjective well-being and personal satisfaction among patients treated with LAI.
Conclusion
In our study, the three AP-LAI treatments showed similar effectiveness in preventing relapses, represented by urgent psychiatric consultations and hospitalizations, as well as in patients’ perception of quality of life and health satisfaction, both significantly improved at the end of 12- month treatment. As regards the tolerability profile, the three LAI antipsychotics were different in the number of side effects recorded, with a clear prevalence of weight gain for the two groups treated with paliperidone palmitate. About 9% of patients discontinued treatment due to refusal, ineffectiveness and side effects.
The PP3M showed an efficacy comparable to the other two AP-LAI drugs, with the advantage of reducing the number of administrations, thus allowing patients greater freedom and lower risk of stigma and dependence on services. At the same time, the PP3M, ensuring a constant blood plateau for a longer time than the other LAIs, could have contributed to the low rate of relapse in our sample. A drug like this could further promote rehabilitation and greater social inclusion. However, we emphasizes that, despite PP3M showing a good tolerability profile, this AP-LAI treatment was interrupted due to patients’ refusal, suggesting that poor therapeutic adherence represents a critical issue to be resolved in schizophrenia treatment.
In light of our results, we conclude that antipsychotic therapy in long-acting formulation represents an important therapeutic option for patients suffering from a serious and long-lasting disorder, which can favour the implementation of rehabilitative programs and social support as well as regular psychological support. All together these treatments represent the multimodal approach for reducing severity symptoms and, in the same time, improving social functioning and subjective well-being in individuals affected by schizophrenia.
This observational investigation helped highlight the complexities of real-world psychiatric activities as well as the subjective perceptions of individuals treated in a community outpatient service.
Abbreviations
AP-LAIs, Antipsychotic Long-Acting Injections; BMI, Body Mass Index; CGI-S, Clinical Global Impression-Severity; FGA, First Generation Antipsychotic; GAF, Global Assessment of Functioning; HAL-D, Haloperidol Decanoate; HS, Health Satisfaction; LAI, Long-Acting Injectable; MHCs, Mental Health Centers; NS, Not Significant; OAPs, Oral Antipsychotics; PP3M, Paliperidone Palmitate 3-Monthly; PP1M, Paliperidone Palmitate one-Monthly; QALY, Quality Adjusted Life Years; QOL, Quality Of Life; SGA, Second Generation Antipsychotic; WHOQOL-BREF, World Health Organization Quality of Life-26 items.
Ethics Approval and Informed Consent
We obtained the approval of the Ethics Committee of the Vasta Emilia Nord Area (Prot.n.0009228/19 of 28/03/2019) and the authorization of the AUSL of Modena (Decision Number 1104 of 23/05/2019).
Acknowledgments
The authors thank Orianna Raggioli for her precious help in language revision.
Disclosure
The authors report no actual or potential conflicts of interest.
References
1. Charlson FJ, Ferrari AJ, Santomauro DF, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. 2018;44(6):1195–1203. doi:10.1093/schbul/sby058
2. Cloutier M, Aigbogun MS, Guerin A, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77(6):764–771. doi:10.4088/JCP.15m10278
3. Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. 2016;388(10039):86–97. doi:10.1016/S0140-6736(15)01121-6
4. Dziwota E, Stepulak MZ, Włoszczak-Szubzda A, Olajossy M. Social functioning and the quality of life of patients diagnosed with schizophrenia. Ann Agric Environ Med. 2018;25(1):50–55. doi:10.5604/12321966.1233566
5. Pîrlog MC, Alexandru DO, Popescu RE, et al. Quality of life-a goal for schizophrenia’s therapy. Curr Health Sci J. 2018;44(2):122–128. doi:10.12865/CHSJ.44.02.05
6. Dong M, Lu L, Zhang L, et al. Quality of life in schizophrenia: a meta-analysis of comparative studies. Psychiatr Q. 2019;90(3):519–532. doi:10.1007/s11126-019-09633-4
7. Lehman F, Lieberman JA, Dixon LB, et al.; Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry. 2004;161:1–56.
8. National Institute for Health and Care Excellence. Psychosis and schizophrenia in adults: prevention and management. Clinical guideline [CG178]; 2014. Available from: https://www.nice.org.uk/guidance/cg178.
9. Boyer L, Baumstarck K, Boucekine M, Blanc J, Lançon C, Auquier P. Measuring quality of life in patients with schizophrenia: an overview. Expert Rev Pharmacoecon Outcomes Res. 2013;13(3):343–349. doi:10.1586/erp.13.15
10. Stępnicki P, Kondej M, Kaczor AA. Current concepts and treatments of schizophrenia. Molecules. 2018;23(8):2087. doi:10.3390/molecules23082087
11. Kokurcan A, Güriz SO, Karadağ H, Erdi F, Örsel S. Treatment strategies in management of schizophrenia patients with persistent symptoms in daily practice: a retrospective study. Int J Psychiatry Clin Pract. 2021;25(3):238–244. doi:10.1080/13651501.2021.1879157
12. Kane JM. Improving patient outcomes in schizophrenia: achieving remission, preventing relapse, and measuring success. J Clin Psychiatry. 2013;74(9):e18. doi:10.4088/JCP.12117tx1c
13. Lauriello J. Prevalence and impact of relapse in patients with schizophrenia. J Clin Psychiatry. 2020;81(2):MS19053BR1C. doi:10.4088/JCP.MS19053BR1C
14. Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Lancet. 2012;379(9831):2063–2071. doi:10.1016/S0140-6736(12)60239-6
15. Emsley R, Oosthuizen P, Koen L, Niehaus D, Martinez L. Comparison of treatment response in second-episode versus first-episode schizophrenia. J Clin Psychopharmacol. 2013;33(1):80–83. doi:10.1097/JCP.0b013e31827bfcc1
16. Jääskeläinen E, Juola P, Hirvonen N, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. 2013;39(6):1296–1306. doi:10.1093/schbul/sbs130
17. Greene M, Yan T, Chang E, Hartry A, Touya M, Broder MS. Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. J Med Econ. 2018;21(2):127–134. doi:10.1080/13696998.2017.1379412
18. Kane JM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5):IN18031AH1C. doi:10.4088/JCP.IN18031AH1C
19. Titus-Lay EN, Ansara ED, Isaacs AN, Ott CA. Evaluation of adherence and persistence with oral versus long-acting injectable antipsychotics in patients with early psychosis. Ment Health Clin. 2018;8(2):56–62. doi:10.9740/mhc.2018.03.056
20. Lindenmayer JP, Glick ID, Talreja H, Underriner M. Persistent barriers to the use of long-acting injectable antipsychotics for the treatment of schizophrenia. J Clin Psychopharmacol. 2020;40(4):346–349. doi:10.1097/JCP.0000000000001225
21. Blackwood C, Sanga P, Nuamah I, et al. Patients’ preference for long-acting injectable versus oral antipsychotics in schizophrenia: results from the patient-reported medication preference questionnaire. Patient Prefer Adherence. 2020;14:1093–1102. doi:10.2147/PPA.S251812
22. Spanarello S, La Ferla T. The pharmacokinetics of long-acting antipsychotic medications. Curr Clin Pharmacol. 2014;9(3):310–317. doi:10.2174/15748847113089990051
23. Ereshefsky L, Mascarenas CA. Comparison of the effects of different routes of antipsychotic administration on pharmacokinetics and pharmacodynamics. J Clin Psychiatry. 2003;64(Suppl 16):18–23.
24. Suda A, Hattori S, Kishida I, et al. Effects of long-acting injectable antipsychotics versus oral antipsychotics on autonomic nervous system activity in schizophrenic patients. Neuropsychiatr Dis Treat. 2018;14:2361–2366. doi:10.2147/NDT.S173617
25. Fagiolini A, Rocca P, De Giorgi S, Spina E, Amodeo G, Amore M. Clinical trial methodology to assess the efficacy/effectiveness of long-acting antipsychotics: randomized controlled trials vs naturalistic studies. Psychiatry Res. 2017;247:257–264. doi:10.1016/j.psychres.2016.11.044
26. Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6):603–609. doi:10.1176/appi.ajp.2011.10081224
27. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29,823 patients with schizophrenia. JAMA Psychiatry. 2017;74(7):686–693. doi:10.1001/jamapsychiatry.2017.1322
28. Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74(10):957–965. doi:10.4088/JCP.13r08440
29. Taylor DM, Sparshatt A, O’Hagan M, Dzahini O. Effect of paliperidone palmitate on hospitalisation in a naturalistic cohort - a four-year mirror image study. Eur Psychiatry. 2016;37:43–48. doi:10.1016/j.eurpsy.2016.04.009
30. Ostuzzi G, Bighelli I, So R, Furukawa TA, Barbui C. Does formulation matter? A systematic review and meta-analysis of oral versus long-acting antipsychotic studies. Schizophr Res. 2017;183:10–21. doi:10.1016/j.schres.2016.11.010
31. Miura G, Misawa F, Kawade Y, Fujii Y, Mimura M, Kishimoto T. Long-acting injectables versus oral antipsychotics: a retrospective bidirectional mirror-image study. J Clin Psychopharmacol. 2019;39(5):441–445. doi:10.1097/JCP.0000000000001082
32. Fang SC, Liao DL, Huang CY, Hsu CC, Cheng SL, Shao YJ. The effectiveness of long-acting injectable antipsychotics versus oral antipsychotics in the maintenance treatment of outpatients with chronic schizophrenia. Hum Psychopharmacol. 2020;35(3):e2729. doi:10.1002/hup.2729
33. Lin CH, Chen FC, Chan HY, Hsu CC. A comparison of long-acting injectable antipsychotics with oral antipsychotics on time to rehospitalization within 1 year of discharge in elderly patients with schizophrenia. Am J Geriatr Psychiatry. 2020;28(1):23–30. doi:10.1016/j.jagp.2019.08.005
34. Mahlich J, Olbrich K, Wilk A, Wimmer A, Wolff-Menzler C. Hospitalization rates and therapy costs of German schizophrenia patients who are initiated on long-acting injectable medication: a mirror-image study. Clin Drug Investig. 2020;40(4):355–375. doi:10.1007/s40261-020-00900-y
35. Patel C, Emond B, Morrison L, et al. Risk of subsequent relapses and corresponding healthcare costs among recently-relapsed Medicaid patients with schizophrenia: a real-world retrospective cohort study. Curr Med Res Opin. 2021;37(4):665–674. doi:10.1080/03007995.2021.1882977
36. Pietrini F, Albert U, Ballerini A, et al. The modern perspective for long-acting injectables antipsychotics in the patient-centered care of schizophrenia. Neuropsychiatr Dis Treat. 2019;15:1045–1060. doi:10.2147/NDT.S199048
37. Miyamoto S, Wolfgang Fleischhacker W. The use of long-acting injectable antipsychotics in schizophrenia. Curr Treat Options Psychiatry. 2017;4(2):117–126. doi:10.1007/s40501-017-0115-z
38. Naber D, Hansen K, Forray C, et al. Qualify: a randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophr Res. 2015;168(1–2):498–504. doi:10.1016/j.schres.2015.07.007
39. Pae CU, Wang SM, Han C, et al. Comparison between long-acting injectable aripiprazole versus paliperidone palmitate in the treatment of schizophrenia: systematic review and indirect treatment comparison. Int Clin Psychopharmacol. 2017;32(5):235–248. doi:10.1097/YIC.0000000000000177
40. Druais S, Doutriaux A, Cognet M, et al. Cost effectiveness of paliperidone long-acting injectable versus other antipsychotics for the maintenance treatment of schizophrenia in France. Pharmacoeconomics. 2016;34(4):363–391. doi:10.1007/s40273-015-0348-x
41. Einarson TR, Pudas H, Goswami P, van Impe K, Bereza BG. Pharmacoeconomics of long-acting atypical antipsychotics for acutely relapsed chronic schizophrenia in Finland. J Med Econ. 2016;19(2):111–120. doi:10.3111/13696998.2015.1100115
42. Decuypere F, Sermon J, Geerts P, et al. Treatment continuation of four long-acting antipsychotic medications in the Netherlands and Belgium: a retrospective database study. PLoS One. 2017;12(6):e0179049. doi:10.1371/journal.pone.0179049
43. Morris MT, Tarpada SP. Long-acting injectable paliperidone palmitate: a review of efficacy and safety. Psychopharmacol Bull. 2017;47(2):42–52.
44. Stone JM, Roux S, Taylor D, Morrison PD. First-generation versus second-generation long-acting injectable antipsychotic drugs and time to relapse. Ther Adv Psychopharmacol. 2018;8(12):333–336. doi:10.1177/2045125318795130
45. Saucedo Uribe E, Carranza Navarro F, Guerrero Medrano AF, et al. Preliminary efficacy and tolerability profiles of first versus second-generation long-acting injectable antipsychotics in schizophrenia: a systematic review and meta-analysis. J Psychiatr Res. 2020;129:222–233. doi:10.1016/j.jpsychires.2020.06.013
46. Pilon D, Alcusky M, Xiao Y, et al. Adherence, persistence, and inpatient utilization among adult schizophrenia patients using once-monthly versus twice-monthly long-acting atypical antipsychotics. J Med Econ. 2018;21(2):135–143. doi:10.1080/13696998.2017.1379413
47. Di Lorenzo R, Ferri P, Cameli M, Rovesti S, Piemonte C. Effectiveness of 1-year treatment with long-acting formulation of aripiprazole, haloperidol, or paliperidone in patients with schizophrenia: retrospective study in a real-world clinical setting. Neuropsychiatr Dis Treat. 2019;15:183–198. doi:10.2147/NDT.S189245
48. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. 2016;19(7):pyw018. doi:10.1093/ijnp/pyw018
49. Brasso C, Bellino S, Bozzatello P, Montemagni C, Rocca P. Role of 3-monthly long-acting injectable paliperidone in the maintenance of schizophrenia. Neuropsychiatr Dis Treat. 2017;13:2767–2779. doi:10.2147/NDT.S150568
50. Arteaga Duarte CH, Fakra E, Van Gils C, Guillon P. The clinical and economic impact of three-monthly long-acting formulation of paliperidone palmitate versus the one-monthly formulation in the treatment of schizophrenia in France: a cost-utility study. Encephale. 2019;45(6):459–467. doi:10.1016/j.encep.2019.03.001
51. Basu A, Benson C, Alphs L. Projecting the potential effect of using paliperidone palmitate once-monthly and once-every-3-months long-acting injections among Medicaid beneficiaries with schizophrenia. J Manag Care Spec Pharm. 2018;24(8):759–768. doi:10.18553/jmcp.2018.24.8.759
52. Emond B, El Khoury AC, Patel C, et al. Real-world outcomes post-transition to once-every-3-months paliperidone palmitate in patients with schizophrenia within US commercial plans. Curr Med Res Opin. 2019;35(3):407–416. doi:10.1080/03007995.2018.1560220
53. Emond B, Joshi K, Khoury ACE, et al. Adherence, healthcare resource utilization, and costs in Medicaid beneficiaries with schizophrenia transitioning from once-monthly to once-every-3-months paliperidone palmitate. Pharmacoecon Open. 2019;3(2):177–188. doi:10.1007/s41669-018-0089-9
54. European Medicines Agency. (2020) Paliperidone Janssen-Cilag International (paliperidone). An overview of Paliperidone Janssen-Cilag International and why it is authorised in the EU; 2020. Available from: https://www.ema.europa.eu/documents/overview/paliperidone-janssen-cilag-international-epar-medicine-overview_en.pdf.
55. European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP). Assessment report. Xeplion. International nonproprietary name: paliperidone palmitate (xeplion); 2011. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR__Public_assessment_report/human/002105/WC500103370.pdf.
56. Codifa - The Pharmacy Informer. Haldol Decanoas; 2021. Available from: https://www.codifa.it/farmaci/h/haldol-decanoas-aloperidolo-decanoato-antipsicotici-butirrofenonici.
57. Ministry of Labour, Health and Social Policy. International Classification of Diseases-9th Revision-Clinical Modification (ICD-9-CM). Rome: Istituto Poligrafico e Zecca dello Stato; 2008.
58. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28(3):551–558. doi:10.1017/s0033291798006667
59. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
60. Goldman HH, Skodol AE, Lave TR. Revising axis V for DSM-IV: a review of measures of social functioning. Am J Psychiatry. 1992;149(9):1148–1156. doi:10.1176/ajp.149.9.1148
61. Dolder CR, Lacro JP, Dunn LB, Jeste DV. Antipsychotic medication adherence: is there a difference between typical and atypical agents? Am J Psychiatry. 2002;159(1):103–108. doi:10.1176/appi.ajp.159.1.103
62. Meyer JM, Stahl SM. The metabolic syndrome and schizophrenia. Acta Psychiatr Scand. 2009;119(1):4–14. doi:10.1111/j.1600-0447.2008.01317.x
63. Mahlich J, Olbrich K, Wilk A, Wimmer A, Wolff-Menzler C. Time to treatment discontinuation in German patients with schizophrenia: long-acting injectables versus oral antipsychotics. Clin Drug Investig. 2021;41(1):99–113. doi:10.1007/s40261-020-00990-8
64. Garcia-Portilla MP, Llorca PM, Maina G, et al. Symptomatic and functional outcomes after treatment with paliperidone palmitate 3-month formulation for 52 weeks in patients with clinically stable schizophrenia. Ther Adv Psychopharmacol. 2020;10:2045125320926347. doi:10.1177/2045125320926347
65. Sapra M, Weiden PJ, Schooler NR, Sunakawa-McMillan A, Uzenoff S, Burkholder P. Reasons for adherence and nonadherence: a pilot study comparing first- and multi-episode schizophrenia patients. Clin Schizophr Relat Psychoses. 2014;7(4):199–206. doi:10.3371/CSRP.SAWE.020813
66. Stentzel U, van den Berg N, Schulze LN, et al. Predictors of medication adherence among patients with severe psychiatric disorders: findings from the baseline assessment of a randomized controlled trial (Tecla). BMC Psychiatry. 2018;18(1):155. doi:10.1186/s12888-018-1737-4
67. Kreyenbuhl J, Slade EP, Medoff DR, et al. Time to discontinuation of first- and second-generation antipsychotic medications in the treatment of schizophrenia. Schizophr Res. 2011;131(1–3):127–132. doi:10.1016/j.schres.2011.04.028
68. Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Aust NZ J Psychiatry. 2016;50(5):410–472. doi:10.1177/0004867416641195
69. National Institute for Health and Care Excellence. Psychosis and schizophrenia in adults. Quality standard [QS80]; 2015. Available from: https://www.nice.org.uk/guidance/qs80.
70. Vincent PD, Demers MF, Doyon-Kemp V, Duchesneau J, Halme A, Masson V. One year mirror-image study using paliperidone palmitate for relapse prevention of schizophrenia in four university hospitals in Canada. Schizophr Res. 2017;185:96–100. doi:10.1016/j.schres.2017.01.013
71. Kane JM, Davis JM, Schooler N, et al. A multidose study of haloperidol decanoate in the maintenance treatment of schizophrenia. Am J Psychiatry. 2002;159(4):554–560. doi:10.1176/appi.ajp.159.4.554
72. Lammers L, Zehm B, Williams R. Risperidone long-acting injection in Schizophrenia Spectrum Illnesses compared to first generation depot antipsychotics in an outpatient setting in Canada. BMC Psychiatry. 2013;13:155. doi:10.1186/1471-244X-13-155
73. McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of paliperidone palmitate vs haloperidol decanoate for maintenance treatment of schizophrenia: a randomized clinical trial [published correction appears in JAMA. 2014;312(14):1473]. JAMA. 2014;311(19):1978–1987. doi:10.1001/jama.2014.4310
74. Majer IM, Gaughran F, Sapin C, Beillat M, Treur M. Efficacy, tolerability, and safety of aripiprazole once-monthly versus other long-acting injectable antipsychotic therapies in the maintenance treatment of schizophrenia: a mixed treatment comparison of double-blind randomized clinical trials. J Mark Access Health Policy. 2015;3. doi:10.3402/jmahp.v3.27208
75. Nielsen J, Jensen SO, Friis RB, Valentin JB, Correll CU. Comparative effectiveness of risperidone long-acting injectable vs first-generation antipsychotic long-acting injectables in schizophrenia: results from a nationwide, retrospective inception cohort study. Schizophr Bull. 2015;41(3):627–636. doi:10.1093/schbul/sbu128
76. Yu HY, Hsiao CY, Chen KC, et al. A comparison of the effectiveness of risperidone, haloperidol and flupentixol long-acting injections in patients with schizophrenia–a nationwide study. Schizophr Res. 2015;169(1–3):400–405. doi:10.1016/j.schres.2015.09.006
77. Di Lorenzo R, Cameli M, Piemonte C, et al. Clinical improvement, relapse and treatment adherence with paliperidone palmitate 1-month formulation: 1-year treatment in a naturalistic outpatient setting. Nord J Psychiatry. 2018;72(3):214–220. doi:10.1080/08039488.2017.1420819
78. Galuppi A, Turola MC, Nanni MG, Mazzoni P, Grassi L. Schizophrenia and quality of life: how important are symptoms and functioning? Int J Ment Health Syst. 2010;4:31. doi:10.1186/1752-4458-4-31
79. Eack SM, Newhill CE. Psychiatric symptoms and quality of life in schizophrenia: a meta-analysis. Schizophr Bull. 2007;33(5):1225–1237. doi:10.1093/schbul/sbl071
80. Di Lorenzo R, Perrone D, Montorsi A, Balducci J, Rovesti S, Ferri P. Attitude towards drug therapy in a community mental health center evaluated by the drug attitude inventory. Patient Prefer Adherence. 2020;14:995–1010. doi:10.2147/PPA.S251993
81. Patel R, Chesney E, Taylor M, Taylor D, McGuire P. Is paliperidone palmitate more effective than other long-acting injectable antipsychotics? Psychol Med. 2018;48(10):1616–1623. doi:10.1017/S0033291717003051
82. Zhdanava M, Lin D, Lafeuille MH, et al. Antipsychotic adherence, resource use, and costs before and after the initiation of once-monthly paliperidone palmitate therapy among Medicaid beneficiaries with prior schizophrenia relapse. Clin Ther. 2021;43(3):535–548. doi:10.1016/j.clinthera.2021.01.011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.