Back to Journals » Nature and Science of Sleep » Volume 17

Effective Dexmedetomidine Dose for Stage N2 Sleep Induction and Associated Factors in Depression-Related Insomnia: A Polysomnography-Based Analysis
Authors Li Y, Zuo M, Wang R, Li Y, Williams JP ![]() , An J
, An J ![]()
Received 3 July 2025
Accepted for publication 11 August 2025
Published 4 September 2025 Volume 2025:17 Pages 2111—2118
DOI https://doi.org/10.2147/NSS.S550428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Yaozu Li,1– 4 Muyan Zuo,1– 4 Ruoguo Wang,2,3 Yongxiang Li,2,3 John P Williams,5 Jianxiong An1– 5
1Medical School, University of Chinese Academy of Sciences, Beijing, People’s Republic of China; 2Center for Pain & Sleep Medicine, Affiliated Hospital of Shandong Second Medical University (Weifang Medical University), Weifang, People’s Republic of China; 3Institute for Innovation Diagnosis & Treatment in Anesthesiology, Shandong Second Medical University (Weifang Medical University), Weifang, People’s Republic of China; 4Brain Disease Institute & Department of Anesthesiology for the Integrated Traditional Chinese and Western Medicine Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 5Department of Anesthesiology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
Correspondence: Jianxiong An, Email [email protected]
Background: Insomnia is a common symptom of depression, and their complex, bidirectional relationship poses significant challenges for treatment. Dexmedetomidine (Dex), an α2-adrenergic receptor agonist, shows unique advantages in inducing sleep closely resembling physiological sleep and is gaining interest as a potential therapy for insomnia.
Objective: This study aimed to determine the average effective Dex dose for inducing stage N2 sleep in patients with depression-related insomnia via polysomnography (PSG), and to identify factors affecting dose variability.
Methods: From April to August 2023, 91 patients with depression-related insomnia were recruited from the Center for Pain and Sleep Medicine at the Affiliated Hospital of Shandong Second Medical University. All patients received intravenous Dex infusion (diluted to 4 μg/mL and administered at 60 mL/h) under continuous PSG monitoring. The cumulative Dex dose required to induce stage N2 sleep was recorded. Clinical data were collected, and univariate and multiple linear regression analyses were performed to identify factors influencing Dex dose.
Results: A total of 82 patients were included in the final analysis. The mean effective dose of Dex required to induce stage N2 sleep was 49.0 ± 16.4 μg. Multivariate regression analysis identified age (P < 0.001) and body weight (P = 0.022) as independent predictors of Dex dose, with age exerting a stronger predictive effect. Simple linear regression further demonstrated a positive association between age and Dex dose (R² = 0.181). During titration, patients’ vital signs remained stable, with heart rate significantly decreasing (68.2 ± 10.0 vs 57.0 ± 13.3 bpm, P < 0.05), whereas mean arterial pressure and oxygen saturation showed no significant changes (P > 0.05).
Conclusion: Dex could effectively induces stage N2 sleep in patients with depression-related insomnia and has a favorable safety profile, with the required dose increasing with age.
Keywords: polysomnography, depression, insomnia, dexmedetomidine, stage N2 sleep
Introduction
Insomnia is a common symptom across psychiatric disorders and is particularly prominent in patients with depression, with approximately 80% to 90% experiencing sleep disturbances 1. The relationship between insomnia and depression is complex and bidirectional, contributing to disease progression and complicating both diagnosis and treatment. In healthy adults, sleep architecture follows a cyclic pattern comprising non-rapid eye movement (NREM) stages—N1, N2, and N3—followed by rapid eye movement (REM) sleep, which typically recurs 4 to 5 times per night.2 In contrast, patients with depression-related insomnia often exhibit delayed N2 onset, a reduced N2-to-N3 ratio, and frequent nocturnal awakenings, leading to fragmented sleep architecture. 3
Current clinical interventions for insomnia include cognitive behavioral therapy for insomnia (CBTI),4 physical therapies, 5 and pharmacological treatments. 6 Although CBTI is the first-line recommended therapy, its delayed onset of action and limited patient compliance reduce its overall effectiveness. Physical therapies are generally considered safe, but high-quality evidence supporting their efficacy remains limited. Benzodiazepines and non-benzodiazepine hypnotics remain widely used due to their convenience; however, long-term use may disrupt normal sleep architecture and elevate the risks of dependence, cognitive impairment, and withdrawal symptoms.7 Consequently, there is an urgent need for safer and more effective therapeutic alternatives.
Dexmedetomidine (Dex), a highly selective α2-adrenergic receptor agonist, exerts its sedative effects primarily by inhibiting norepinephrine release from the locus coeruleus. 8 Studies have shown that Dex-induced sedation closely mimics the physiological features of natural sleep.9,10 Moreover, Dex has been recommended for the management of withdrawal symptoms associated with alcohol and opioid dependence 11,12 and has exhibited neuroprotective effects in various models of neurological injury. 13 Importantly, it appears to have a low risk of addiction and withdrawal even with long-term use. 14
Building on these pharmacological advantages, our team proposed the concept of patient-controlled sleep (PCSL) therapy, in which patients with chronic insomnia receive preprogrammed doses of Dex via a patient-operated device to induce and maintain sleep.15
The core of PCSL therapy lies in the precise titration of Dex dosage for effective sleep induction. Therefore, this study aimed to determine the average effective dose of Dex required to induce stage N2 sleep, as assessed by polysomnography (PSG), and to identify associated influencing factors. The findings are intended to support the clinical application of Dex in insomnia treatment and inform dosage form optimization.
Materials and Methods
Participants
This study was approved by the Ethics Committee of the Affiliated Hospital of Shandong Second Medical University (Approval No. wyfy-2023-ky-057).
This study is a prespecified substudy within the registered clinical trial entitled“Clinical study of rapid antidepressant combined with sleep regulation for depression and insomni” (China Clinical Trial Registration No. ChiCTR2300070756). The purpose of this substudy was to determine the effective dose of dexmedetomidine for stage N2 sleep induction and to explore associated influencing factors. The study was registered in March 2023, and participants were enrolled between April and August 2023. All participants received multidisciplinary evaluation by psychiatry, sleep medicine, respiratory medicine, and other relevant specialties. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Inclusion criteria: Patients diagnosed with depressive disorder based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), between April and August 2023, with a Hamilton Depression Rating Scale (HAMD-17) score ≥17, self-reported symptoms of insomnia, a Pittsburgh Sleep Quality Index (PSQI) score ≥8, and who provided written informed consent to undergo dexmedetomidine (Dex) titration were enrolled.
Exclusion criteria: Patients with severe cardiopulmonary, hepatic, renal, cerebrovascular, or other psychiatric disorders; known allergy to Dex; a history or titration-based detection of obstructive sleep apnea or restless leg syndrome; or those who were pregnant or lactating were excluded.
Sleep Quality Assessment
Subjective sleep quality prior to treatment was assessed using the Pittsburgh Sleep Quality Index (PSQI), which evaluates seven components: sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component is rated on a scale from 0 to 3, with higher total scores indicating poorer sleep quality and reflecting sleep status over the past month.
Psychological Assessment
Prior to treatment, two trained attending physicians assessed patients’ emotional states using the 17-item Hamilton Depression Rating Scale (HAMD-17) and the 14-item Hamilton Anxiety Scale (HAMA). Higher scores on these scales reflect greater severity of depressive and anxiety symptoms.
Dexmedetomidine Titration Based on Polysomnography
Prior to titration, patients fasted for 6 hours and refrained from water intake for 2 hours. An intravenous line was established and connected to cardiac and oxygen saturation monitors, followed by the administration of 250–500 mL of saline. Polysomnography (PSG) was used to continuously monitor the electroencephalogram (EEG). Dexmedetomidine was diluted to a concentration of 4 μg/mL and continuously infused at a rate of 60 mL/h. The infusion was terminated immediately upon EEG confirmation of stage N2 sleep onset. Vital signs were continuously monitored throughout the procedure. If blood pressure deviated from the target range, norepinephrine or nitroglycerin was administered as needed. In cases of bradycardia (<45 bpm), anisodamine, or isoproterenol was administered as clinically indicated. If patients exhibited significant snoring or apneic episodes accompanied by oxygen desaturation (SpO2 < 90%) during titration, they were considered to show evidence of obstructive sleep apnea and were excluded from further analysis.
Outcome Measures
Primary outcome: The total dose of Dex (μg) required to induce the transition to stage N2 sleep.
Stage N2 sleep was defined according to the American Academy of Sleep Medicine (AASM) criteria by the presence of sleep spindles or K-complexes. Sleep spindles were characterized by a frequency of 11–16 Hz, spindle-like morphology, clustered distribution, duration ≥ 0.5 seconds, and amplitude < 50 μV. K-complexes consisted of a sharp negative wave followed by a positive wave, with a duration ≥ 0.5 seconds.16
Secondary outcomes: Mean arterial pressure (MAP), heart rate (HR), and oxygen saturation (SpO2) measured before and after Dex titration.
Statistical Analysis
All data were analyzed using SPSS 25.0. Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data and compared using independent samples t-tests. Non-normally distributed variables were presented as medians with interquartile ranges (IQR). Categorical variables were reported as frequencies and percentages. To identify factors influencing Dex dose for N2 sleep induction, univariate analyses were first performed. Correlations between variables were then assessed using independent samples t-tests, Pearson’s correlation, or Spearman’s rank correlation analyses, depending on data distribution. Variables with P < 0.1 or clinical relevance were included in a multiple linear regression model to evaluate independent associations. To validate the assumptions of the linear regression model, residual plots were examined for homoscedasticity, and the Durbin–Watson statistic was used to assess the independence of residuals. Model fit was assessed using adjusted R², and multicollinearity was evaluated using the variance inflation factor (VIF). Statistical significance was defined as a two-tailed P value < 0.05.
Results
General Information
A total of 82 patients with depression-related insomnia were enrolled, comprising 30 males and 52 females. The median age was 27.0 years (interquartile range [IQR]: 17.0–43.5), and the median weight was 65.0 kg (IQR: 57.5–75.0). Among the participants, 57 (69.5%) were taking antidepressants, 40 (48.8%) were using hypnotics, and 15 (18.3%) were receiving antipsychotic medications. Additionally, 13 (15.9%) had a history of electroconvulsive therapy (ECT), and 14 (17.1%) had undergone repeated transcranial magnetic stimulation (rTMS). Additional details can be found in Table 1.
 |
Table 1 Clinical Characteristics (n=82) |
Mean Effective Dose and Univariate Analysis
The mean effective intravenous dose of dexmedetomidine required to induce stage N2 sleep was 49.0 ± 16.4 μg, with substantial interindividual variability (range: 20–100 μg). To explore potential influencing factors, univariate analyses were conducted. Pearson’s correlation was used for normally distributed continuous variables, Spearman’s rank correlation for non-normally distributed variables, and independent samples t-tests for categorical variables. The results indicated that age, weight, illness duration, gender, and hypnotic use were significantly associated with Dex dosage (P < 0.1). Antidepressant use and HAMD scores showed trends toward significance (P = 0.142 and P = 0.158, respectively). Detailed results are presented in Table 2.
 |
Table 2 Univariate Analysis of Factors Associated with Dex Dose |
Multiple Linear Regression Analysis of Dex Dosage
A multiple linear regression model was constructed with Dex dosage as the dependent variable. Independent variables included age, weight, duration of illness, gender, HAMD-17 score, use of hypnotics, and use of antidepressants. The standardized residuals were randomly distributed around the predicted values, indicating acceptable homoscedasticity. The Durbin–Watson statistic was 2.082, suggesting no significant autocorrelation and confirming the independence of residuals. The model demonstrated a good overall fit (adjusted R² = 0.258, P < 0.001), and all variance inflation factors (VIFs) were below 2.0, indicating no evidence of significant multicollinearity. Age (B = 0.498, 95% CI: 0.244–0.752, P < 0.001) and weight (B = 0.246, 95% CI: 0.036–0.456, P = 0.022) were identified as independent predictors of Dex dosage. None of the other variables reached statistical significance. Detailed results are provided in Table 3.
 |
Table 3 Multiple Linear Regression Analysis for Predictors of Dex Dose |
Linear Relationship Between Age and Dex Dosage
To further assess the association between age and Dex dosage, an initial scatterplot suggested a possible linear relationship. Simple linear regression revealed a significant positive association (R² = 0.181, P < 0.001), indicating that Dex dosage increased with age. This association remained significant in the multivariate linear regression model after adjusting for potential confounders, confirming age as an independent predictor of Dex dosage. The fitted regression line is shown in Figure 1.
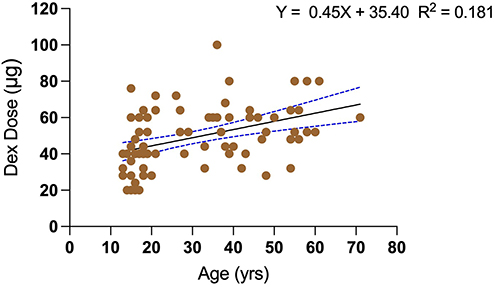 |
Figure 1 Linear regression analysis of the relationship between Dex dose and age. The solid line represents the best-fit linear regression line (R² = 0.181, p < 0.001). |
Changes in Vital Signs During Dex Titration
Vital signs were continuously monitored throughout the Dex titration procedure. At the end of titration, heart rate was lower compared with pre-titration values (68.2 ± 10.0 bpm vs 57.0 ± 13.3 bpm, P < 0.001). In contrast, no significant changes were observed in mean arterial pressure (86.1 ± 9.5 mmHg vs 84.5 ± 12.4 mmHg, P = 0.187) or oxygen saturation (97.2 ± 2.3% vs 96.6 ± 2.3%, P = 0.093). Detailed results are presented in Table 4.
 |
Table 4 Changes in Vital Signs Before and After Dex Titration |
Discussion
This study is the first to objectively evaluate the dose of dexmedetomidine (Dex) required to induce stage N2 sleep, along with its associated factors, in patients with depression-related insomnia using polysomnography (PSG). The results revealed substantial interindividual variability in Dex-induced N2 sleep, with a mean effective dose of 49.0 ± 16.4 μg and a range of 20–100 μg. Multivariate regression analysis identified age as the primary determinant of Dex dose, indicating an increasing requirement with advancing age. Weight was also associated with Dex dose, although the effect was less pronounced. The observed associations between Dex dose and patient characteristics suggest avenues for future research on dose optimization.
The multiple linear regression model developed in this study demonstrated a moderate fit, with an adjusted R² of 0.258, which is acceptable for clinical observational research. In univariate analysis, age alone explained 18.1% of the variance in Dex dose (R² = 0.181), underscoring its predictive value. Sensitivity analysis excluding a 36-year-old patient who received 100 μg of Dex showed minimal change in model fit (adjusted R² decreased slightly to 0.251), with age remaining a significant predictor (P < 0.001), indicating robust and reliable results.
The observed increase in Dex dosage with age contrasts with the typical pattern for conventional oral sedatives, which generally require lower doses in older adults due to slowed metabolism, as reported by Greil et al.17 This discrepancy suggests that Dex may act through distinct mechanisms. Studies have shown that Dex induces physiological N2 sleep by activating endogenous sleep pathways,9 whereas normal sleep architecture depends on intact brain structures and balanced neurotransmitter systems.18,19 Age-related declines in neuroplasticity20 and endogenous regulatory mechanisms21 may reduce responsiveness to Dex, necessitating higher doses to achieve comparable sleep depth.
Furthermore, many patients had a history of long-term use of antidepressants or hypnotics. Univariate analysis indicated that hypnotic use (P = 0.069) and antidepressant use (P = 0.142) might influence Dex dose. Although these factors were not significant predictors in the multivariate model, chronic medication use may alter neurotransmitter regulation or induce tolerance, thereby indirectly affecting Dex efficacy. While the exact mechanisms remain unclear, these variables should be regarded as potential confounders warranting further investigation in future studies.22
Dex titration was generally well tolerated. A mild decrease in heart rate was the most common physiological change, consistent with Dex’s mimicry of the natural sleep state.23 Only one patient developed sinus bradycardia, which promptly resolved following anisodamine administration. Mean arterial pressure and oxygen saturation remained stable before and after titration. These findings suggest that Dex titration is safe and provides a basis for its wider clinical application.
This study has several limitations. First, as a single-center study with a relatively small sample size—particularly with few elderly participants—the generalizability of the findings may be limited. Second, Dex was infused continuously during titration, and due to pharmacodynamic delay, the recorded dose at PSG-confirmed N2 onset may slightly overestimate the true minimal effective dose. Future studies should refine titration protocols to optimize dosing. Lastly, all patients received subsequent esketamine treatment post-titration, so this study does not report subjective adverse effects attributable solely to Dex titration. In addition, although patients with clinically diagnosed OSA were excluded, subtle upper airway factors such as nasal resistance, craniofacial structure, and habitual oral breathing were not systematically assessed. These variables may affect sleep continuity and Dex response, and thus represent an additional limitation.
Future research involving larger, prospectively enrolled cohorts stratified by age should investigate dose–response relationships to determine the ED50 and ED90 for Dex-induced physiological sleep. Integration of neuroimaging and metabolic biomarkers may further elucidate the neurobiological mechanisms underlying age-related variability in Dex dosing. Age-related jaw shrinkage and increased airborne allergens, both of which may impair sleep quality, should also be considered in future studies examining anatomical and environmental influences on interindividual variability.
Conclusion
This study objectively determined the Dex dose required to induce stage N2 sleep in patients with depression-related insomnia, as measured by PSG. The findings suggest that Dex can induce N2 sleep in this population, with dosage positively correlated with age—identifying age as the primary predictor of Dex dose.
Data Sharing Statement
The deidentified data used and analyzed during this study are available from the corresponding author on reasonable request.
Ethics Statement
This study was approved by the Ethics Committee of the Affiliated Hospital of Shandong Second Medical University (Approval No. wyfy-2023-ky-057), and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment. For participants under 18 years of age, informed consent was obtained from their legal guardians, and an assent form was signed by the minors after explanation in age-appropriate language.
Acknowledgments
We gratefully acknowledge the contributions of all participants who took part in this study.
Author Contributions
Conceptualization: Yaozu Li and Jianxiong An; Investigation: Yaozu Li, Muyan Zuo, Ruoguo Wang and Yongxiong Li; Formal analysis: Yaozu Li, Jianxiong An and John P Williams; Visualization: Yaozu Li; Funding acquisition: Jianxiong An; Writing - original draft: Yaozu Li and John P Williams; Writing - review & editing: Yaozu Li, John P Williams, Muyan Zuo, Ruoguo Wang, Yongxiong Li and Jianxiong An.
All authors have made substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data. All authors have drafted or substantially revised the manuscript, approved the version to be published, and agreed on the journal to which the article was submitted. They all agree to be accountable for all aspects of the work and to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The work was supported by the National Key R&D Program of China (2024YFC2510200).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Hutka P, Krivosova M, Muchova Z, et al. Association of sleep architecture and physiology with depressive disorder and antidepressants treatment. Int J Mol Sci. 2021;22(3):1333. doi:10.3390/ijms22031333
2. Steiger A, Pawlowski M. Depression and sleep. Int J Mol Sci. 2019;20(3):607. doi:10.3390/ijms20030607
3. Riemann D, B KL, Wulff K, et al. Sleep, insomnia, and depression. Neuropsychopharmacol. 2019;45(1):74–89. doi:10.1038/s41386-019-0411-y
4. Dujardin S, Pijpers A, Pevernagie D. prescription drugs used in insomnia. Sleep Med Clinics. 2020;15(2):133–145. doi:10.1016/j.jsmc.2020.02.002
5. Jiang C-G, Zhang T, Yue F-G, et al. Efficacy of repetitive transcranial magnetic stimulation in the treatment of patients with chronic primary insomnia. Cell Biochem Biophys. 2013;67(1):169–173. doi:10.1007/s12013-013-9529-4
6. Sateia MJ, J BD, Krystal AD, et al. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in Adults: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(02):307–349. doi:10.5664/jcsm.6470
7. Pillai V, Roth T, Roehrs T, et al. Effectiveness of benzodiazepine receptor agonists in the treatment of insomnia: an examination of response and remission rates. Sleep. 2017;40(2). doi:10.1093/sleep/zsw044.
8. Akeju O, J PK, B WM, et al. A comparison of propofol- and dexmedetomidine-induced electroencephalogram dynamics using spectral and coherence analysis. Anesthesiology. 2014;121(5):978–989. doi:10.1097/ALN.0000000000000419
9. Huupponen E, Maksimow A, Lapinlampi P, et al. Electroencephalogram spindle activity during dexmedetomidine sedation and physiological sleep. Acta Anaesthesiologica Scandinavica. 2007;52(2):289–294. doi:10.1111/j.1399-6576.2007.01537.x
10. Akeju O, E HL, Gao L, et al. Dexmedetomidine promotes biomimetic non-rapid eye movement stage 3 sleep in humans: a pilot study. Clin Neurophysiol. 2018;129(1):69–78. doi:10.1016/j.clinph.2017.10.005
11. Muzyk AJ, Fowler JA, Norwood DK, et al. Role of α 2 -agonists in the treatment of acute alcohol withdrawal. Ann Pharmacother. 2011;45(5):649–657. doi:10.1345/aph.1P575
12. Darrouj J, Puri N, Prince E, et al. Dexmedetomidine Infusion as adjunctive therapy to benzodiazepines for acute alcohol withdrawal. Ann Pharmacother. 2008;42(11):1703–1705. doi:10.1345/aph.1K678
13. Unchiti K, Leurcharusmee P, Samerchua A, et al. The potential role of dexmedetomidine on neuroprotection and its possible mechanisms: evidence from in vitro and in vivo studies. Eur J Neurosci. 2021;54(9):7006–7047. doi:10.1111/ejn.15474
14. Weerink MS, Struys MMRF, Hannivoort LN, et al. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
15. An J-X, P WJ, Fang Q-W, et al. Feasibility of patient-controlled sleep with dexmedetomidine in treating chronic intractable insomnia. Nat Sci Sleep. 2020;12:1033–1042. doi:10.2147/NSS.S262991
16. Kokkinos V, Kostopoulos GK. Human non‐rapid eye movement stage II sleep spindles are blocked upon spontaneous K‐complex coincidence and resume as higher frequency spindles afterwards. J Sleep Res. 2011;20(1pt1):57–72. doi:10.1111/j.1365-2869.2010.00830.x
17. Greil W, De Bardeci M, Seifert J, et al. Treatment of depression: are psychotropic drugs appropriately dosed in women and in the elderly? Dosages of psychotropic drugs by sex and age in routine clinical practice. Human Psychopharmacol. 2021;37(1). doi:10.1002/hup.2809.
18. Cheng W, T RE, Ruan H, et al. Functional connectivities in the brain that mediate the association between depressive problems and sleep quality. JAMA Psychiatry. 2018;75(10):1052. doi:10.1001/jamapsychiatry.2018.1941
19. Liu D, Dan Y. A motor theory of sleep-wake control: arousal-action circuit. Ann Rev Neurosci. 2019;42(1):27–46. doi:10.1146/annurev-neuro-080317-061813
20. Damoiseaux JS. Effects of aging on functional and structural brain connectivity. NeuroImage. 2017;160:32–40. doi:10.1016/j.neuroimage.2017.01.077
21. Urbanski HF, Sorwell KG. Age-related changes in neuroendocrine rhythmic function in the rhesus macaque. Age. 2011;34(5):1111–1121. doi:10.1007/s11357-011-9352-z
22. Shi Y, Cui M, Ochs K, et al. Long-term diazepam treatment enhances microglial spine engulfment and impairs cognitive performance via the mitochondrial 18 kDa translocator protein (TSPO). Nat Neurosci. 2022;25(3):317–329. doi:10.1038/s41593-022-01013-9
23. Kang D, Lim C, Shim D-J, et al. The correlation of heart rate between natural sleep and dexmedetomidine sedation. Korean J Anesthesiol. 2019;72(2):164–168. doi:10.4097/kja.d.18.00208
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.