Back to Journals » Journal of Pain Research » Volume 19
Effect of Vibration Anesthesia on Injection-Related Pain: A Prospective Crossover Study
Authors Martinez L, Orey D, Troche G, Goldfaden R ![]()
Received 5 March 2026
Accepted for publication 15 May 2026
Published 20 May 2026 Volume 2026:19 603981
DOI https://doi.org/10.2147/JPR.S603981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Luis Martinez,1 Dontia Orey,2 Gian Troche,1 Rebecca Goldfaden2
1Universal Axon Clinical Research, Doral, FL, USA; 2Rovia Clinical Research, Jacksonville, FL, USA
Correspondence: Rebecca Goldfaden, Rovia Clinical Research, 3550 University Blvd S #101, Jacksonville, FL, 32216, USA, Tel +1-904-854-1354, Fax +1-904-854-1355, Email [email protected]
Background: Needle-based procedures, including intramuscular (IM) and subcutaneous (SC) injections and fingersticks, are essential to healthcare but frequently associated with pain and anxiety. Vibration anesthesia leverages the gate control theory by stimulating competing sensory pathways to reduce nociceptive transmission. DigiVibe (Suthe Dermal) is a handheld, FDA-registered vibration device designed to mitigate needle-related pain. This study evaluated DigiVibe’s (Suthe Dermal) effect on pain during common needle procedures.
Methods: Twenty (20) healthy adults (50% female; mean age 37.5 years) reporting needle aversion underwent six procedures in a single visit including fingersticks, SC injections, and IM injections, each performed once without intervention (control) and once with DigiVibe (Suthe Dermal) applied before and during needle insertion. Pain was assessed immediately after each procedure using a 10-point Visual Analog Scale (VAS). Primary endpoints included mean paired VAS differences analyzed via Paired t-test and Wilcoxon signed-rank test.
Results: DigiVibe (Suthe Dermal) significantly reduced pain across all procedure types. Mean VAS reductions were − 2.65 for SC injections (p< 0.001; d= − 1.66), − 2.00 for IM injections (p< 0.001; d= − 1.23), and − 1.75 for fingersticks (p< 0.001; d= − 1.13). Nonparametric results confirmed large effect sizes (rank-biserial r = − 1.0, − 0.96, and − 0.88, respectively). Sixty-five percent (65%) of subjects experienced no pain with DigiVibe (Suthe Dermal) during fingersticks and 95% achieved ≥ 30% pain reduction for SC injections. No adverse events occurred.
Conclusion: DigiVibe (Suthe Dermal) produced statistically significant and clinically meaningful reductions in pain across IM, SC, and fingerstick procedures in adults with needle aversion. These findings support vibration anesthesia as a safe, non-pharmacologic method to enhance comfort and potentially improve adherence to needle-based care.
Keywords: vibration anesthesia, injection-related pain
A Letter to the Editor has been published for this article.
A Response to Letter by Miss Xu has been published for this article.
Introduction
Needle-based procedures, including intramuscular (IM) injections, subcutaneous (SC) injections, and fingersticks, are among the most frequently performed interventions in clinical practice worldwide.1 These procedures are critical for vaccine administration, chronic disease management, and point-of-care diagnostics.1 Despite their importance, needle-related pain and fear remain significant barriers to adherence, contributing to vaccine hesitancy and suboptimal compliance with injection-based therapies. Studies show that 20% to over 60% of children and adults experience needle fear or phobia, contributing to delayed immunizations, avoiding laboratory monitoring, and non-adherence to injections.2–4 One study with 2,098 participants noted 1,325 people had needle fear that led to avoiding blood draws (52.2%), blood donations (49%), and vaccinations (33.1%).2 The mitigation of needle fear using vibration anesthesia could reduce delayed therapy and enhance access to healthcare. Improving patient comfort during needle procedures is a public health priority to increase adherence and improve clinical outcomes.3
Pain perception arises from nociceptor activation and transmission through the spinal cord to cortical processing centers.5 Melzack and Wall’s Gate Control Theory provides a foundational framework for modulating pain. It states that non-painful sensory input can inhibit or “close the gate” on nociceptive transmission along the spinal cord. Specifically, activation of large-diameter, fast-conducting A-beta sensory fibers can dampen pain signals carried by smaller A-delta and C fibers, reducing perceived discomfort.5
Based on this mechanism, non-pharmacologic pain-reduction methods such as tactile stimulation, cooling, and vibration have been explored during needle procedures. Vibration anesthesia, which applies localized mechanical vibration to the skin, has emerged as a promising technique. By delivering non-noxious sensory stimulation prior to and during needle insertion, vibration may reduce pain perception through competitive neural signaling, aligning with gate control theory.5
Over the past several decades, devices such as transcutaneous electrical nerve stimulation (TENS) units, Buzzy®, and VibraCool® have demonstrated that non-noxious stimuli can reduce pain during dermatologic procedures, musculoskeletal injections, and intraoral anesthesia.5–7 For example, vibration has been shown to significantly reduce pain during upper-extremity injections and improve patient comfort during intraoral anesthetic administration. Although some results have not reached statistical significance, consistent numerical trends indicate meaningful clinical benefit, particularly in patients with heightened needle anxiety.
DigiVibe (Suthe Dermal) is a handheld, Food and Drug Administration (FDA)-registered device designed to deliver localized mechanical vibration to the skin prior to and during needle penetration. Operating at approximately 130–170 Hz with an amplitude of 1.5–2.5 mm, the device is engineered to activate mechanoreceptors and modulate pain signaling according to gate control principles.7 While vibration therapy has demonstrated success in specific injection settings, comprehensive evaluation across commonly performed procedures, including IM injections, SC injections, and fingersticks, has been limited.6–8
Given the prevalence of needle fear, its negative impact on healthcare adherence, and the growing interest in non-pharmacologic pain-mitigation strategies, further evaluation of vibration anesthesia is warranted. The present study assesses the DigiVibe (Suthe Dermal) device in a prospective, crossover design to determine whether vibration anesthesia significantly reduces pain across IM, SC, and fingerstick procedures in adults with needle aversion. Findings may support broader application of vibration-based analgesia as a simple, low-cost intervention to enhance comfort, reduce procedure-related stress, and improve uptake of medically necessary needle procedures.
Ethical Approval
This study received approval from the Advarra Institutional Review Board (IRB) (approval number: Pro00087329), was conducted in accordance with Good Clinical Practice (GCP), the Health Insurance Portability and Accountability Act (HIPAA) regulations, and adhered to the Tenets of the Declaration of Helsinki. Written informed consent was obtained from all subjects prior to any study procedures. The registration number of this study on the National Institute of Health (NIH) website https://clinicaltrials.gov is NCT06987201.
Methods
Study Design
This was a single-center, prospective, open-label, crossover study. All subjects completed the injections without the vibration device applied and crossed over to the injections with the vibration device applied.
Participants: Inclusion and Exclusion Criteria
A total of twenty (20) healthy adult subjects (10 men and 10 women) aged ≥18 years and a body mass index (BMI) between 18.5–29.9 kg/m2 with a self-reported fear or dislike of needles were enrolled. Key exclusion criteria included chronic daily use of non-steroidal anti-inflammatory drugs (NSAIDs), antiplatelets, anticoagulants, or analgesics within three days of enrollment, and any condition that could confound pain assessment or interfere with study participation.
Interventions and Study Procedures
Each subject underwent six procedures during a single study visit. Two fingersticks were performed using a 30-gauge Unistik® lancing device on the pulp of the middle fingers. The first was performed without intervention (control), followed by a 5-minute wait period. The second fingerstick with DigiVibe (Suthe Dermal) was then applied for 20 seconds before and during lancing (see Figure 1). Two SC injections of 0.5 mL normal saline were administered using a 30-gauge 4 mm needle in the lower abdominal quadrants (≥2 inches from the umbilicus). The first injection was performed without intervention (control), followed by a 5-minute wait period. The second injection was performed with DigiVibe (Suthe Dermal) applied for 20 seconds before and throughout the injection. Finally, two IM injections of 0.5 mL normal saline were administered in the deltoid muscles using either a 25-gauge or 30-gauge 1-inch needle, with alternating assignments to balance gauge distribution across sexes. As with the other procedures, the first injection was performed without intervention (control) and a 5-minute wait period, and the second injection with DigiVibe (Suthe Dermal) applied for 20 seconds before and throughout the injection.
 |
Figure 1 Fingerstick with DigiVibe Vibration Anesthesia. |
Outcomes: Primary Outcome
The primary outcome was a 10-point visual analog scale (VAS), and the primary endpoint was the difference in VAS pain scores between control and DigiVibe-assisted procedures immediately after each procedure. Subjects completed six separate VAS assessments, one after each fingerstick, SC injection, and IM injection (after both non-intervention and intervention).
Adverse events (AEs) and serious AEs (SAEs) were recorded from consent through the end of the study visit. AEs were categorized by intensity (mild, moderate, severe) and causality (related, possibly related, or not related).
Statistical Analysis
A sample size of 20 subjects provided at least 80% power to detect a mean paired difference of at least 1.0 with a SD of 1.5, using a two-sided alpha level of 0.05. VAS pain scores were analyzed using both parametric and nonparametric approaches and were summarized as mean ± standard deviation (SD). Paired t-tests were used to compare mean pain scores between control and DigiVibe-assisted procedures for each injection type (fingerstick, SC, IM). To account for potential non-normality, Wilcoxon signed-rank tests were performed on the paired differences. Hodges–Lehmann (HL) estimators of the location shift with 95% confidence intervals (CIs) were calculated as robust measures of the median paired difference. Effect sizes were expressed as rank-biserial correlation coefficients (r), with |r| ≥ 0.5 considered a large effect. Statistical significance was set at two-sided p < 0.05.
Results
Table 1 outlines the baseline characteristics of the study population, which included 20 subjects (50% male; mean age 37.5 ± 13.4 years) that enrolled and completed the study. The majority (95%) identified as Hispanic or Latino, and all were White. Mean BMI was 26.0 ± 2.4 kg/m2 and mean systolic and diastolic blood pressure values were 115.4 ± 8.3 mmHg and 71.1 ± 7.6 mmHg, respectively.
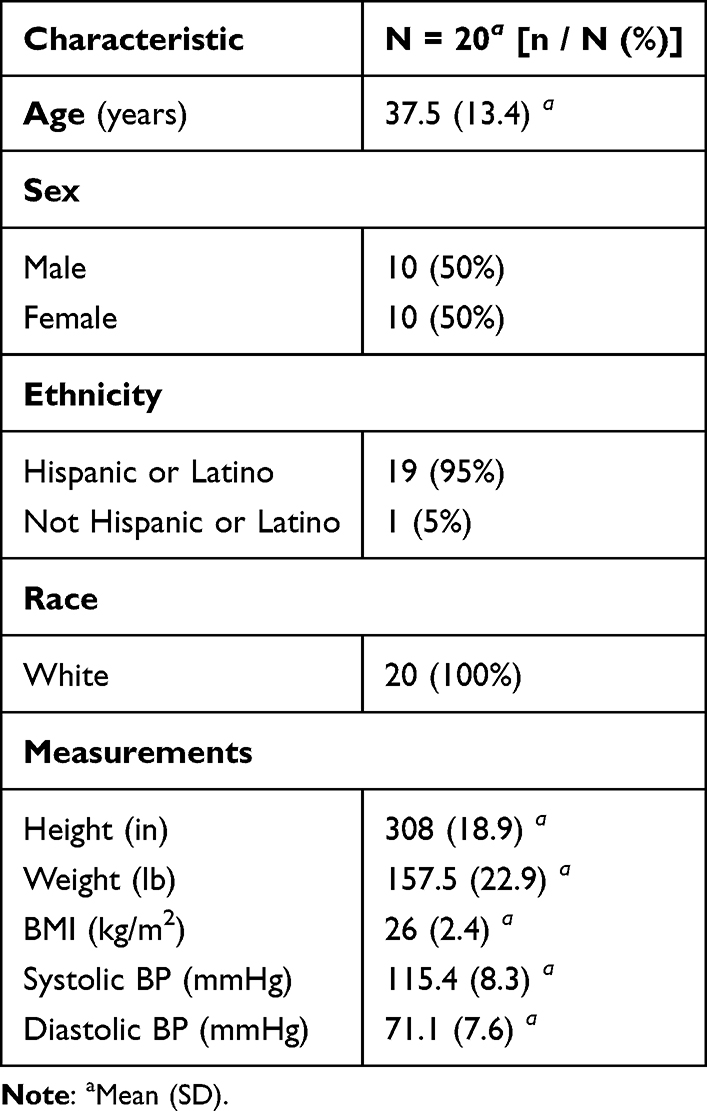 |
Table 1 Baseline Characteristics |
Table 2 summarizes the primary endpoint results (analyzed with the Paired T-test) and Table 3 summarizes the primary endpoint results (analyzed with Wilcoxon Signed-Rank Test across all three injection types. DigiVibe (Suthe Dermal) usage was associated with statistically significant reductions in pain scores compared with procedures performed without vibration anesthesia. For SC injections in the abdomen (Figure 2), the mean reduction in VAS pain score was −2.65 (95% CI, −3.40 to −1.90), representing a large effect size (Cohen’s d = −1.66; t(19) = −7.41; p < 0.001). Nonparametric analysis confirmed these findings, with an HL shift of −2.5 (95% CI, −3.5 to −2.0), W = 0, rank-biserial r = −1.00, p < 0.001, indicating that every subject experienced lower pain scores with DigiVibe (Suthe Dermal).
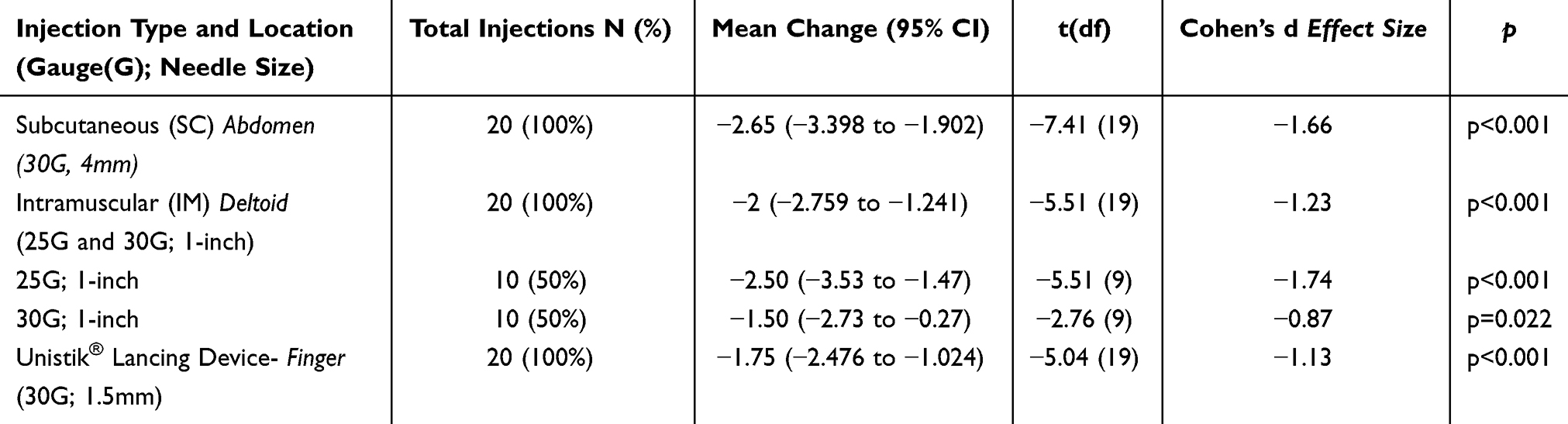 |
Table 2 Primary Endpoint Results (Paired T-Test) |
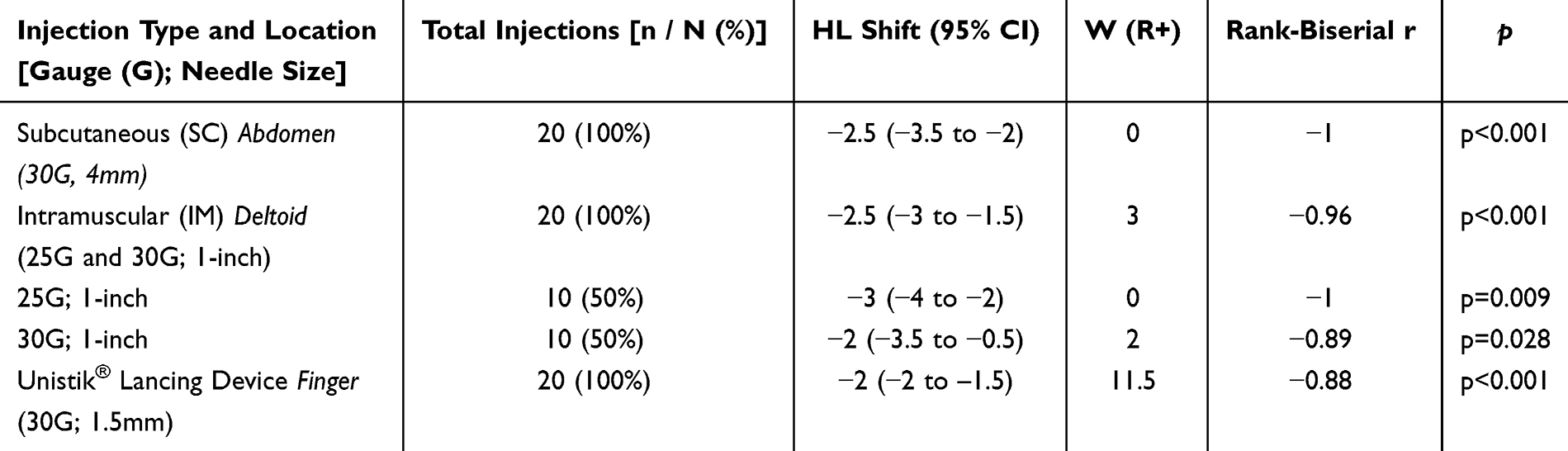 |
Table 3 Primary Endpoint Results (Wilcoxon Signed-Rank Test) |
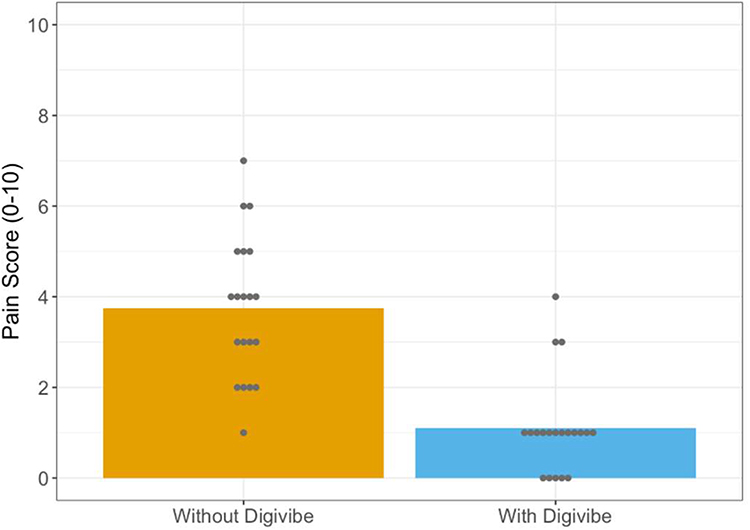 |
Figure 2 Abdomen (SC) Pain Scales (30G, 4mm). |
Similarly, IM injections in the deltoid muscle (Figure 3) demonstrated a mean reduction of −2.00 points (95% CI, −2.76 to −1.24; t(19) = −5.51; p < 0.001), corresponding to a large effect size (Cohen’s d = −1.23). Wilcoxon results demonstrated an HL shift of −2.5 (95% CI, −3.0 to −1.5), W = 3, rank-biserial r = −0.96, p < 0.001, confirming a strong and consistent reduction in pain across nearly all subjects.
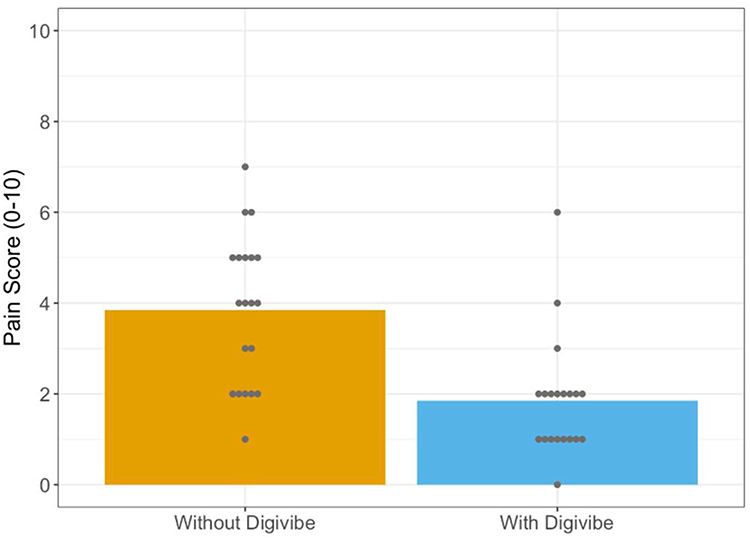 |
Figure 3 Deltoid (IM) Pain Scales (25G and 30G; 1-inch). |
The fingerstick procedures (Figure 4) also showed a mean pain reduction of −1.75 points (95% CI, −2.48 to −1.02; t(19) = −5.04; p < 0.001) and a large effect size (Cohen’s d = −1.13). The Wilcoxon analysis yielded an HL shift of −2.0 (95% CI, −2.0 to −1.5), W = 11.5, rank-biserial r = −0.88, p < 0.001, reflecting a large, clinically meaningful decrease in pain perception. Fingerstick procedures also showed a significant improvement, with 65% of the fingerstick subjects indicating that they felt no pain when DigiVibe (Suthe Dermal) was administered (Figure 5).
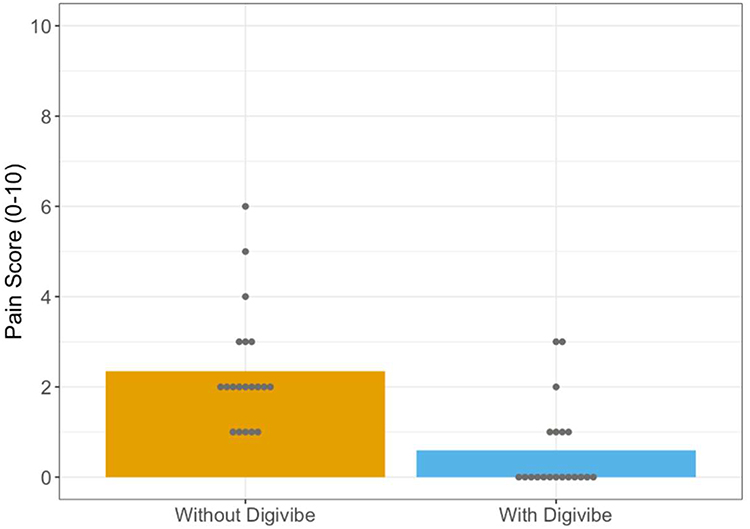 |
Figure 4 Fingerstick Pain Scales (30G; 1.5mm). |
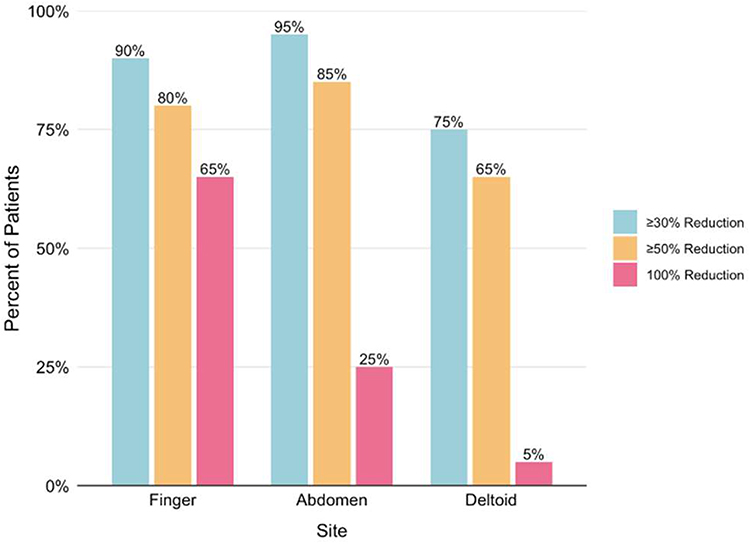 |
Figure 5 Proportion of Subjects Experiencing ≥ 30%, ≥50% and ≥100% Reductions in Pain. |
Finally, the proportion of patients who experienced meaningful reductions in injection-site pain across three anatomical sites (finger, abdomen, deltoid) is displayed in Figure 5. Many patients achieved at least a 30% reduction in pain at all sites, with the abdomen showing the highest response (95%). Notably, up to 85% of subjects achieved ≥50% pain reduction in the abdomen, and a substantial subset had complete pain elimination with the fingersticks (65%) and subcutaneous injections (25%).
No adverse events or tolerability concerns were reported during the study. These findings indicate that DigiVibe (Suthe Dermal) provided clinically meaningful and statistically significant pain relief across all tested procedures, with the greatest absolute reduction observed in abdominal SC injections.
Discussion
This prospective crossover study demonstrated that the DigiVibe (Suthe Dermal) vibration anesthesia device significantly reduced pain associated with IM injections, SC injections, and fingersticks. The two IM injections showed the 25-gauge needles presented greater benefit (−2.5-point mean reduction; d = −1.74) than 30-gauge (−1.5-point reduction; d = −0.87). This suggests DigiVibe’s (Suthe Dermal) analgesic effect is pronounced with larger-bore (more painful) needles, similar to a dose-response trend. Notably, 65% of subjects reported complete absence of pain during fingerstick procedures when DigiVibe (Suthe Dermal) was applied (Figure 5). Across all three procedure types, mean pain scores decreased by 1.7 to 2.7 points on a 10-point Visual Analog Scale (VAS), Cohen’s d values ranging from −1.13 to −1.66 (with Cohen’s d > 1.0 representing large effect sizes) and confirming both statistical and clinical significance. The largest absolute pain reduction was observed in SC abdominal injections, though IM injections and fingersticks also showed clinically meaningful improvements. The SC injections displayed a Wilcoxon test of W = 0 and r = −1.00, meaning every subject reported lower pain with DigiVibe (Suthe Dermal). Similarly, IM injections (r = −0.96) and fingersticks (r = −0.88) showed more than 90% of subjects saw improvements with pain when the DigiVibe (Suthe Dermal) device was used, representing a close to “universal benefit” of the DigiVibe (Suthe Dermal) device. No adverse events or device-related issues were observed in any of the 120 total procedures, underscoring the safety and tolerability of the DigiVibe (Suthe Dermal) device.
This study has several limitations. First, the study population was predominantly Hispanic or Latino, which may limit generalizability to broader populations. Second, the study did not include a sham control. DigiVibe is an externally applied vibration device that generates both audible and tactile stimuli during use, making it inherently difficult to blind participants. Potential sham conditions, such as device application without activation, activation without skin contact, or use of a non-vibrating device, would be readily distinguishable due to the absence of these sensory cues. As a result, such approaches would not preserve blinding and would offer limited value in reducing bias. This challenge is well recognized in studies of vibration-based and other sensory-dependent interventions, where the mechanism of action cannot be concealed without removing the core therapeutic component. In this context, inclusion of a sham arm was not considered a valid or methodologically sound control.
Our findings are consistent with and build upon prior work evaluating vibration anesthesia to mitigate needle pain. Vibration applied before dermatologic procedures meaningfully decreased perceived discomfort, supporting the concept that non-noxious sensory input can attenuate pain perception.6 Weeks and Faillace extended these findings to musculoskeletal injections, showing that vibratory stimulation significantly reduced pain compared with both no intervention and vapocoolant spray in subjects receiving upper-extremity corticosteroid injections.7,9 Similarly, Shaefer et al reported that the DentalVibe® system decreased discomfort during intraoral nerve blocks, particularly among subjects with elevated baseline anxiety.8 The magnitude of pain reduction observed in our study was comparable to or greater than that seen in these prior trials, likely aided by the crossover design, which minimized inter-individual variability in pain perception by allowing each subject to serve as their own control.
The biological plausibility of these results is well supported by Melzack and Wall’s gate control theory of pain.5 Vibratory stimulation activates large-diameter A-beta afferents that compete with nociceptive A-delta and C fiber transmission at the dorsal horn, effectively “closing the gate” to painful input.5 This mechanism explains why the reduction in pain was consistent across three distinct needle-based procedures and suggests that vibration therapy has broad applicability beyond a single injection type. Furthermore, because the intervention is entirely non-pharmacologic, there is no risk of systemic drug effects, drug–drug interactions or altered pharmacokinetics that can complicate pharmacologic anesthetic use.
Clinically, these findings have important implications. Needle pain and fear are well-documented contributors to vaccine hesitancy, poor adherence to injectable medications, and avoidance of routine health maintenance procedures such as fingerstick glucose monitoring.3,5 Reducing pain during such procedures may improve patient experience, enhance adherence, and ultimately improve health outcomes. The DigiVibe (Suthe Dermal) device offers a low-cost, portable, and easy-to-implement solution that requires no special training, electricity, or additional clinical infrastructure. Its rapid onset of effect (within seconds) also makes it well-suited for busy outpatient and point-of-care settings.
Conclusion
In this prospective crossover study, DigiVibe (Suthe Dermal) vibration anesthesia significantly reduced pain associated with IM injections, SC injections, and fingersticks in adults with needle aversion. The intervention was safe, well tolerated, and produced large, clinically meaningful reductions in pain scores across all three procedure types. These results support the integration of vibration anesthesia into routine clinical practice as a simple, noninvasive strategy to improve patient comfort and potentially enhance adherence to recommended needle-based interventions such as vaccinations, glucose monitoring, and injectable therapies.
Abbreviations
IM, Intramuscular; SC, Subcutaneous; VAS, Visual Analog Scale; TENS, Transcutaneous Electrical Nerve Stimulation; FDA, Food And Drug Administration; BMI, Body Mass Index; NSAIDs, Non-Steroidal Anti-Inflammatory Drugs; GCP, Good Clinical Practice; IRB, Institutional Review Board; AEs, Adverse Events; SAEs, Serious Adverse Events; HL, Hodges–Lehmann; CI, Confidence Intervals; r, Rank-Biserial Correlation Coefficients; SD, Standard Deviation.
Data Sharing Statement
All data are available upon reasonable request to the corresponding author.
Acknowledgment
The DigiVibe device was obtained from Suthe Dermal.
Funding
This study was financially supported by Suthe Dermal (the manufacturer of the DigiVibe device).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gandell DL, Bienen EJ, Gudeman J. Mode of injection and treatment adherence: results of a survey characterizing the perspectives of health care providers and US women 18–45 years old. Patient Prefer Adherence. 2019;13:351–9.PMID: 30863023; PMCID: PMC6391128. doi:10.2147/PPA.S187120
2. Alsbrooks K, Hoerauf K. Prevalence, causes, impacts, and management of needle phobia: an international survey of a general adult population. PLoS One. 2022;17(11):e0276814. doi:10.1371/journal.pone.0276814
3. McLenon J, Rogers MAM. The fear of needles: a systematic review and meta-analysis. J Adv Nurs. 2019;75(1):30–42.PMID: 30109720. doi:10.1111/jan.13818
4. Taddio A, Ipp M, Thivakaran S, et al. Survey of the prevalence of immunization non-compliance due to needle fears in children and adults. Vaccine. 2012;30(32):4807–4812.PMID: 22617633. doi:10.1016/j.vaccine.2012.05.011
5. Campbell TS, Johnson JA, Zernicke KA. Gate Control Theory of Pain. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. Cham: Springer International Publishing; 2020. doi:10.1007/978-3-030-39903-0_100174.
6. Smith K, Comite S, Balasubramanian S, Carver A, Liu J. Vibration anesthesia: a noninvasive method of reducing discomfort prior to dermatologic procedures. Dermatol Online J. 2004;10(2):1. doi:10.5070/D348Q9S83P
7. Weeks D, Faillace J. Vibratory Anesthesia’s effect on pain perception in upper extremity corticosteroid injections. US National Library of Medicine. July 2022.
8. Shaefer JR, Lee SJ, Anderson NK. A vibration device to control injection discomfort. Compend Contin Educ Dent. 2017;38(6):e5–e8. PMID: 28586233.
9. Weeks D, Faillace J. Randomized comparison of vapocoolant spray versus vibration anesthesia versus no anesthesia for upper extremity injections. US Natl Libr Med. Published. Available from: https://pubmed.ncbi.nlm.nih.gov/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.