Back to Journals » International Journal of General Medicine » Volume 16
Effect of Type 2 Diabetes on the Development of Acute Respiratory Distress Syndrome (ARDS) in Patients with Lung Cancer After Surgery and Its Prognosis
Authors Zhang L, Guan L, Tang X, Zhao Y
Received 8 August 2023
Accepted for publication 27 September 2023
Published 9 October 2023 Volume 2023:16 Pages 4573—4584
DOI https://doi.org/10.2147/IJGM.S433412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Liang Zhang,1 Lanjun Guan,2 Xiaoyue Tang,2 Yong Zhao3
1Department of Endocrinology, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Department of Internal Medicine, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 3Department of Thoracic Surgery, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
Correspondence: Yong Zhao, Department of Thoracic Surgery, Affiliated Hospital of Jiangnan University, No. 1000, Hefeng Road, Wuxi, 214000, People’s Republic of China, Email [email protected]
Background: Type 2 diabetes mellitus (T2DM) is associated with the occurrence of lung cancer. Postoperative lung cancer complications with acute respiratory distress syndrome (ARDS) are characterized by rapid onset and severe disease. This study aimed to analyze the effect of T2DM on the occurrence of ARDS in patients with lung cancer after surgery and its prognosis and further investigate the risk factors of postoperative complications of ARDS.
Methods: A total of 530 patients who developed lung cancer from December 2016 to December 2021 were retrospectively analyzed. The t- and chi-square tests were used to determine the relationship between whether the patients had combined diabetes and other clinical characteristics. Binary logistic and Cox risk regressions were used to analyze the independent risk factors for the development of ARDS in patients after surgery and the effect of each factor on the survival status of patients, respectively.
Results: Fifty-three cases of ARDS occurred after lung cancer surgery, with an incidence of 10%. Binary logistic regression analysis demonstrated that the independent influencing factors that determined the occurrence of ARDS after surgery were the presence or absence of combined diabetes (odds ratio [OR] = 3.888, P< 0.001), history of radiotherapy (OR = 2.039, P = 0.024), surgery mode (OR = 2.521, P = 0.002), and so on. Moreover, Cox risk regression analysis demonstrated that the presence or absence of combined diabetes (OR = 1.389, P = 0.039) and occurrence of ARDS (OR = 2.028, P = 0.037) were independent influencing factors on the patient survival time.
Conclusion: In lung cancer patients with T2DM, postoperative ARDS is more likely to occur, and both diabetes and postoperative ARDS are risk factors affecting the survival of patients with lung cancer. Preoperative and postoperative glycemic control and improved pulmonary ventilation should be enhanced to minimize the chance of ARDS.
Plain Language Summary: This study initially clarified the effect of type 2 diabetes on the development of acute respiratory distress syndrome and its prognosis in lung cancer patients after surgery and other risk factors for the development of ARDS in lung cancer patients after surgery, which may provide a theoretical basis for the effective prevention and treatment of the risk of ARDS after surgery.
Keywords: type 2 diabetes mellitus, lung cancer, acute respiratory distress syndrome, prognosis
Introduction
Diabetes, a common metabolic disease in clinical practice, has a prevalence of 536.6 million worldwide in 2021 in individuals aged 20–79 years, according to the International Diabetes Federation, that is anticipated to rise to 783.2 million by 2045; China ranks first in the prevalence of diabetes in individuals aged 20–79 years.1 Chinese guidelines for the prevention and treatment point out that type 2 diabetes mellitus (T2DM) is predominant in the country, accounting for approximately 90% of the total population. The prevalence of diabetes in individuals aged 18 years and above has increased from 10.9% in 2013 to 12.4% in 2018 in China, according to statistics.2
Diabetes can cause damage to several target organs and is associated with a variety of diseases affecting patient prognosis. The target organs are the retina, kidneys, and lungs.3,4 A study demonstrated a significantly higher risk of developing lung diseases (such as asthma, COPD, pulmonary fibrosis, and pneumonia) in patients with diabetes compared to those without diabetes, which may be related to reduced lung function owing to diabetes.5 In 1930, Wilson et al found a correlation between T2DM and tumor development,6 and their correlation has again become a research hotspot. An epidemiological study found that the incidence of malignant tumors in patients with T2DM is 25% or more, among which patients with lung cancer are in the top three, and the combination accounts for approximately 15% of all lung cancers.7
Lung cancer is one of the most prevalent malignancies worldwide and accounted for 18% of all cancer deaths in 2020, thus, becoming the most common cause of cancer death.8,9 The 2020 Global Cancer Statistics report exhibits that China ranks first in lung cancer incidence and death rate in 2020, accounting for approximately 23.7% and 30.2% of global cancer incidence and death, respectively.10 In China, non-small cell lung cancer is the main type, accounting for approximately 80–85% of all patients with lung cancer. Currently, clinical treatment for non-small cell lung cancer primarily adopts surgical procedures. Traditional open-heart surgery is effective; however, it causes more damage to the patient’s body. The human thorax integrity is damaged, causing damage to the blood vessels, muscles, and intercostal nerves on the chest wall, creating a greater impact on the physiological function of the heart and lungs post-surgery. With the rapid advent of minimally invasive surgical operation technology, total thoracoscopic lobectomy is applied for treating lung cancer, which is more advantageous such as slight body trauma, less bleeding during surgery, pain, and impact on cardiopulmonary physiological function, with faster recovery after surgery.11 However, regardless of the surgical method, various complications may occur in patients with lung cancer postoperatively,12 such as pneumonia, pulmonary atelectasis, and respiratory failure. A serious postoperative complication is acute respiratory distress syndrome (ARDS). The main clinical manifestations are progressive hypoxemia, respiratory distress, and reduced pulmonary compliance, and rapid onset, rapid progression, and high morbidity and mortality are also observed,13 critically threatening the lives of patients with lung cancer postoperatively. It seriously affects their survival quality.
With the gradual increase in the incidence of diabetes and lung cancer, the group of lung cancer patients with combined T2DM has gained more and more attention.14 In addition, a meta-analysis showed a significant association between diabetes mellitus and the development of ARDS after infection with COvid-19,15 which may be specifically attributed to the fact that diabetes mellitus is associated with a state of chronic inflammation, which promotes the development of an excessive inflammatory response that ultimately leads to the development of acute respiratory distress syndrome.16 This study aimed to analyze the effect of T2DM on the development of ARDS in patients with lung cancer after surgery and to initially investigate other risk factors for the development and impact of multiple factors on patient prognosis. This study provides a reference for reducing the occurrence of postoperative complications, enhancing postoperative care, and improving the quality of life and prognosis of lung cancer patients with T2DM.
Materials and Methods
A total of 530 patients with lung cancer who underwent surgery at Affiliated Hospital of Jiangnan University from December 2016 to December 2021 were included.
The inclusion criteria were as follows: (I) age >18 years; (II) clinical diagnosis of primary lung cancer (based on medical history, symptoms, tumor markers, pathology, computed tomography (CT), positron emission tomography-CT and other imaging data); (III) with surgical indications and tolerating surgery; (IV) signed informed consent; and (V) cases with complete follow-up information.
The exclusion criteria were as follows: (I) combined gestational and type 1 diabetes mellitus; (II) metastasis to other sites inducing metastatic lung cancer; (III) having severe cardiopulmonary insufficiency and unable to tolerate surgery; (IV) expected survival time <3 months; and (V) incomplete follow-up data (Figure 1).
 |
Figure 1 Flow chart of patient selection. |
This case-control study aimed to determine the effect of T2DM on the development of ARDS and assess the prognosis of patients with lung cancer after surgery. According to the group’s previous study and related literature, the probability of ARDS development in patients with lung cancer after surgery ranged from 4 to 11%. The sample size of N1 = 58 cases and N2 = 490 cases to be investigated was calculated using PASS 11 software, with a specified tolerance error of 3% and confidence level of 1-α= 0.95. Eighteen cases were lost to follow-up and actual attrition, and 530 cases were finally counted.
General Information Questionnaire
The general information questionnaire included demographic (age, sex, body mass index) and clinical data (lung cancer stage, lung cancer pathology type, whether diabetes mellitus was comorbid, smoking history, whether chemotherapy was received preoperatively, whether the underlying respiratory disease was comorbid, whether cardiac insufficiency was comorbid, whether electrolyte disturbances were comorbid, surgical approach, operative time, intraoperative bleeding volume, surgical crystal input volume, and the relevant laboratory and prognostic indicators).
Diagnostic Criteria for Primary Lung Cancer
The diagnostic criteria for primary lung cancer are as follows: (1) pathologic diagnosis of primary lung cancer, such as sputum exfoliative cytology, pleural fluid cytology, needle aspiration biopsy, respiratory endoscopy, and other methods of obtaining a pathologic diagnosis; (2) clinical manifestations include cough, blood in sputum, hemoptysis, fever, chest pain, shortness of breath, dyspnea, emaciation, sometimes accompanied by hoarseness, dysphagia, pleural or pericardial effusion, etc.; (3) X-ray, CT, MRI, PET-CT, and other imaging suggestive of pulmonary space-occupying lesions and vascular or lymphatic-related changes; (4) abnormal elevation of serum tumor markers such as carcinoembryonic antigen (CEA), neurospecific enolase (NSE), cytokeratin 19 fragment (CYFRA21-1), and gastrin-releasing peptide precursor (ProGRP); (5) molecular pathology diagnosis, such as EGFR gene mutation, ALK fusion gene and ROS1 fusion gene in tumor tissue; (6) physical examination may reveal superficially enlarged lymph, limited or unilateral rales on auscultation, and so on. The final diagnosis was made by synthesizing the clinical manifestations, pathology, laboratory tests and imaging findings.
Diagnostic Criteria for T2DM
Diabetes was diagnosed based on the Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes (2020 edition).
Note: Typical diabetes symptoms include irritable thirst and excessive drinking, polyuria, polyphagia, and unexplained weight loss. Random blood glucose was defined as the blood glucose at any time of the day regardless of the time of the last meal. Random blood glucose cannot be used to diagnose impaired fasting glucose or glucose tolerance. The fasting state was defined as no caloric intake for a minimum of 8 h.
Diagnostic Criteria for ARDS
The diagnostic criteria for ARDS are based on the 2011 Berlin diagnostic criteria, which are as follows:13 (1) acute onset; (2) oxygenation index (PaO2/FiO2) ≤ 200 mmHg (1 mmHg = 0.133 kPa) and positive end-expiratory pressure ventilation ≥ 5 cm H2O (1 cmH2O = 0.098 kPa); (3) orthopantomogram showing bilateral pulmonary infiltrates; (4) source of pulmonary edema, that is, a respiratory failure that cannot be explained by cardiac insufficiency or fluid overload; and (5) no other physiological disturbances.
Lung Injury Prediction Score
The lung injury prediction score (LIPS),17 proposed by American scholars, assesses the degree of lung injury in patients in terms of susceptibility factors, high-risk surgery, and trauma and risk modification, and accurately screens those with ARDS who are at high risk for acute lung injury.
Acute Physiology and Chronic Health Evaluation (APACHE) II
The APACHE II is a common scoring method used to determine the condition of patients in intensive care units and predict the prognosis, and studies have demonstrated it as a good assessment of the condition of patients with ARDS.17 The APACHE II scoring system comprises the following three parts: acute physiology score (APS), age score, and chronic health status score. APS contains 12 physiological parameters, namely, body temperature, mean arterial pressure, heart rate, respiratory rate, arterial partial pressure of oxygen, pH, blood potassium concentration, sodium concentration, creatinine concentration, cell pressure, white blood cell (WBC) count, and Glasgow score, as well as age and chronic health status, and the final score was the sum of the three scores. The theoretical maximum score is 71, with a higher score indicating more disease severity.
Sequential Organ Failure Assessment (SOFA) Score
The SOFA score, often used by nursing staff in intensive care units, requires a scoring system to determine the degree of major organ function impairment to judge a patient’s healing. The scoring system is divided into the following six main sections: respiratory, coagulation, liver, cardiovascular system, central nervous system, and renal functions, with scores ranging from 0 to 4.
Kaplan-Meier Survival Curve
A 1-year postoperative follow-up was performed through telephone, SMS, and outpatient review. The follow-up included pulmonary function, inflammation index, and functional score. Any discomfort was observed at the hospital at any time. The follow-up endpoint and deadline were death or 1 year and December 2022, respectively.
Statistical Analysis
Statistical analysis was performed using SPSS 26 (IBM SPSS, USA), and measured data were expressed as mean and standard deviation, while count data were expressed as frequency and percentage. Statistical analysis between groups was performed using a t-test and chi-square test, and binary logistic regression was used to analyze the factors influencing the occurrence of ARDS after surgery; independent risk factors affecting survival were analyzed using Cox regression. A two-sided p-value < 0.05 was considered statistically significant.
Results
Baseline Data
Baseline data are shown in Table 1. Fifty-three cases of ARDS occurred after surgery, with a prevalence of 10.0%. The t- and chi-square test results demonstrated significant differences (P < 0.05) between the ARDS and non-ARDS groups for the presence of combined T2DM, history of chemotherapy, combined underlying respiratory disease, electrolyte disturbance, and mode of surgery. In the ARDS group, 13 (24.5%) cases had combined TZDM, 32 (60.4%) cases had a history of chemotherapy, 22 (41.5%) cases had combined underlying respiratory diseases, 20 (37.7%) cases had electrolyte disturbances, 29 (54.7%) cases underwent traditional open-heart surgery, and 24 (45.3%) cases underwent thoracoscopic surgery. In the non-ARDS group, there were 41 (8.6%) cases with T2DM, 216 (46.2%) cases with a history of chemotherapy, 226 (47.4%) cases with underlying respiratory diseases, 120 (25.2%) cases with electrolyte disturbances, 141 (29.6%) cases underwent traditional open-heart surgery, and 336 cases (70.4%) underwent thoracoscopic surgery.
 |
Table 1 Baseline Data of Included Patients in Two Groups |
Perioperative Indicators in Two Groups
In the ARDS group, the mean operative time was (160.96 ±10.55) h, mean intraoperative bleeding was (259.96 ±25.17) mL, and mean crystal input was (2669.28 ±273.00) mL, while in the non-ARDS group, the values were 135.54 ±14.14 h, 247.92 ±28.47 mL, and 2002.01 ±288.90 mL, respectively; the differences between the two groups in the parameters were statistically significant (P<0.05) (Table 2).
 |
Table 2 Perioperative Indicators in Two Groups |
Laboratory Indices of Patients in Two Groups
In the ARDS group, preoperative fasting plasma glucose (FPG) was 6.47 ±1.92 mmol/L, preoperative triglyceride (TG) was 1.67 ±0.44 mmol/L, preoperative high-density lipoprotein-cholesterol (HDL-C) was 1.14 ±0.18 mmol/L, preoperative ALb was 43.55 ±4.72 g/L, preoperative carcinoembryonic antigen (CEA) was 34.51 ±5.63 ng/mL, preoperative WBC was 6.53 ±0.77 × 109/L, and postoperative WBC was 14.92 ±1.23 × 109/L; in the non-ARDS group, preoperative FPG was 5.83 ±1.41 mmol/L, preoperative TG was 1.69 ±0.28 mmol/L, preoperative HDL-C was 1.13 ±0.18 mmol/L, preoperative ALb was 43.86 ±5.05 g/L, preoperative CEA was 34.27 ±5.86 ng/mL, preoperative WBC was 6.72 ±0.76 × 109/L, and postoperative WBC was 12.45 ±1.50 × 109/L. The differences between the two groups in preoperative FPG and TG, and postoperative WBC were statistically significant (P<0.05), while those in preoperative HDL-C, ALb, CEA, and WBC were not significant (P>0.05) (Table 3).
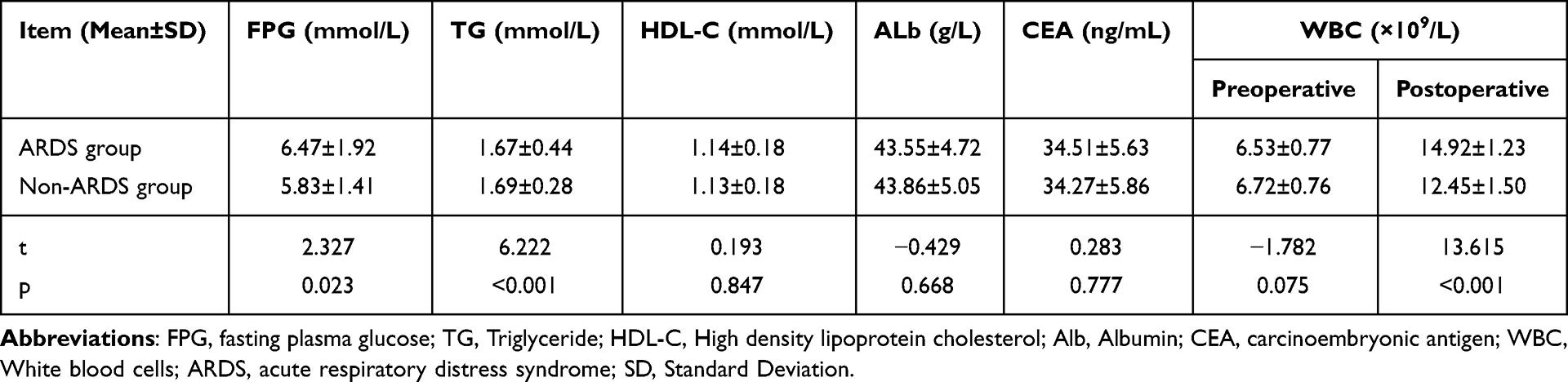 |
Table 3 Laboratory Indices of Patients in Two Groups |
Comparison of the Lung Function Indices Between the Two Groups
In the ARDS group, the mean FEV1% and DLCO% predicted value was 61.15 ±4.97% and 65.94 ±4.74%, respectively, while in the non-ARDS group, the values were 75.74 ±4.26% 73.57 ±4.24%, respectively and the differences were statistically significant (P < 0.05) (Table 4).
 |
Table 4 Comparison of the Lung Function Indexes Between the Two Groups |
Prognosis Assessment After Surgery
In the ARDS group, the mean postoperative APACHE II, LIPS, and SOFA scores were 19.19 ±3.17, 4.15 ±1.21, and 11.23 ±2.06, respectively, while in the non-ARDS group, the scores were 0.04 ±3.17, 2.05 ±1.18, and 4.96 ±2.56 points, respectively. The differences between the two groups in scores were statistically significant (P<0.05) (Table 5).
 |
Table 5 Prognosis Assessment After Surgery in Patients in Two Groups |
Risk Factors of ARDS Analyzed Using Binary Logistic Regression Models
Binary logistic regression analysis demonstrated that the independent factors influencing ARDS occurrence after surgery was the presence of combined diabetes (odds ratio [OR] = 3.888, P<0.001), history of radiotherapy (OR = 2.039, P = 0.024), surgical procedure (OR = 2.521, P = 0.002), time to surgery (OR = 0.041, P = 0.008), crystal input (OR = 1.016, P = 0.003), postoperative WBC (OR = 35.265, P = 0.034), FEV1% predicted value (OR = 0.216, P = 0.002) and DLCO% predicted value (OR = 0.397, P = 0.009) (P<0.05) (Table 6, Figure 2).
 |
Table 6 Risk Factors of Recurrence Analyzed by Binary Logistic Regression Models |
 |
Figure 2 Risk factors of recurrence analyzed by binary logistic regression models. |
Survival-Related Prognostic Factors in Cox Risk Regression Analysis
Cox risk regression analysis showed that the presence or absence of combined diabetes (OR = 1.389, P = 0.039) and occurrence of ARDS (OR = 2.028, P = 0.037) were independent influences on the patient survival time (P<0.05) (Table 7).
 |
Table 7 Survival-Related Prognostic Factors in Cox Risk Regression Analysis for All Patients |
Discussion
In recent years, a study has pointed out18,19 that patients with T2DM may be associated with the occurrence and development of many major malignancies. Moreover, some epidemiological studies have demonstrated that the incidence of malignant tumors in patients with T2DM is 25% or more, among which those with lung cancer are among the top three, and lung cancer patients with combined T2DM account for approximately 15% of all lung cancers.7 Currently, surgery is the treatment of choice for patients with lung cancer. Diabetes is an important risk factor affecting the surgical procedure, perioperative period, and prognosis.20 ARDS is a serious postoperative complication in patients with lung cancer, which can endanger patients’ lives. Therefore, the prognosis of patients with lung cancer should be improved by recognizing and determining the effect of T2DM on the development of ARDS after surgery and initially investigating other risk factors and their impact on the prognosis of patients with lung cancer who develop ARDS after surgery, thus, intervening early. Based on this, this study analyzed the risk factors and prognosis of ARDS in patients with lung cancer patients after surgery.
The results showed that the presence of combined T2DM, history of radiotherapy, surgical procedure, time of surgery, crystal input, TG, postoperative WBC, FEV1% predicted value, and DLCO% predicted value independently influenced whether ARDS occurred after lung cancer surgery.
First, the prevalence of diabetes mellitus was significantly higher in the ARDS group (24.5%) than that in the non-ARDS group (8.6%), and the presence of T2DM and postoperative WBC levels were independent risk factors for the development of ARDS after lung cancer surgery. Lung infection is an important causative factor for the occurrence of ARDS after lung cancer surgery,21 and higher perioperative blood glucose reduces the patient’s surgical tolerance, and many chronic complications and metabolic disorders exist., This may lead to postoperative infection of multiple organs or tissues and even ARDS in patients. Thus, the mechanisms of the influence of T2DM on the occurrence of ARDS in patients with lung cancer patients after surgery may be as follows: (i) Disorders of sugar, protein, and fat metabolism in patients with diabetes; high glucose increases the body catabolism, causing negative nitrogen balance, inhibiting neovascularization and collagen aggregation, weakening the tissue repair ability, lowering body’s immune function, and lowering defense and clearance function of the respiratory tract; thus, increasing the incidence of lung infection.22 (ii) Diabetes mellitus can also increase the incidence of pulmonary infections owing to elevated blood glucose that increases plasma osmolality and inhibits the phagocytic ability of leukocytes, which facilitates bacterial growth.23 (iii) Hyperglycemia causes osmotic diuresis and dehydration, easily leading to water-electrolyte balance imbalance and triggering acute pulmonary edema during rehydration, increasing the risk of pulmonary infections. (iii) The pathogenesis of ARDS caused by severe infection is still ambiguous; however, it may be related to poisoning, infection, and immune factors, leading to alveolar epithelial cell capillary endothelial cell injury and eventually ARDS, while the damage of alveolar type II epithelial cells reduces surface-active substances and pulmonary compliance. This accelerates the ARDS occurrence. Early diagnosis and effective treatment significantly impact the prognosis. Infectious shock is often the precursor of ARDS and multiple organ failure, and early detection and timely treatment can assist in inhibiting the occurrence and development of ARDS. Therefore, blood glucose fluctuation should be monitored dynamically during the perioperative period in patients with combined diabetes mellitus, and the dosage of hypoglycemic drugs or insulin should be adjusted accordingly to control blood glucose; therefore, the risk of ARDS after lung cancer surgery can be avoided owing to high blood glucose and the morbidity and mortality rate can be reduced.
In this study, there were 248 patients with a history of chemotherapy, including 32 (60.4%) and 216 (46.2%) cases in the ARDS and non-ARDS groups, respectively, and the analysis demonstrated that a history of chemotherapy was an independent risk factor for the development of ARDS after lung cancer surgery. Therefore, nutritional support therapy should be provided after surgery to inhibit or reverse the development of malnutrition, improve immune function, and reduce the incidence of ARDS in patients with a history of chemotherapy before surgery. Jakobsen E et al24 demonstrated a significantly higher increase in immunoglobulin levels in patients treated with enteral nutritional support than that in those treated with parenteral support. Enteral nutrition therapy has a more positive effect on the recovery of immune function than intravenous nutritional support in postoperative patients with lung cancer. Enteral nutrition support absorbed through the portal system is more conducive to the recovery of gastrointestinal absorption and digestion, and the improvement of patients’ postoperative nutritional status and immune function.
In addition, the mode of surgery was an independent risk factor for the development of ARDS after surgery. In this study, in the ARDS and non-ARDS groups, a total of 29 (54.7%) and 141 (29.6%) cases underwent traditional open-heart surgery, and 24 (45.3%) and 336 (70.4%) cases underwent thoracoscopic surgery, respectively. In recent years, various surgical treatment measures have started to appear with the rapid development of medical technology, among which the traditional open-chest surgery is often a long surgical incision. Moreover, certain challenges during the surgery can easily damage important muscle groups, causing critical pain to the patients after the surgery, which can adversely affect the quality of life and lung function. In contrast, thoracoscopic surgery has less side damage to surrounding tissues and organs, less stressful organism stimulation, relatively small surgical incision, short exposure time of the chest cavity, and less impact on the internal environment, thus, enhancing postoperative recovery. Post-thoracoscopic incision pain is also reduced.
Autonomous sputum evacuation reduces postoperative pneumonia incidence. The relatively small surgical incision also reduces the incidence of postoperative incisional infections. The time of surgery is an independent risk factor for the occurrence of ARDS after lung cancer surgery because longer surgery time indicates more trauma to the body. Consequently, more anesthesia drugs are absorbed, and the later the awakening time is, the more damage to the patient’s heart and lungs, and other important organs. Therefore, the risk of ARDS in patients after lung cancer surgery is prevented by accurate and quick surgical care coordination, while shortening the operation time.
ALAM N et al have reported25 that the risk of developing ARDS increased by 10% for every 5% decrease in postoperative FEV1% predictive value. The results of this study demonstrated that postoperative FEV1% predicted value was an independent risk factor for the development of postoperative ARDS in lung cancer, with a mean FEV1% and DLCO% predicted value of 61.15 ±4.97% and 65.94 ±4.74% in the ARDS group, and 75.74 ±4.26% and 73.57 ±4.24% in the non-ARDS group, respectively. The predicted values averaged 73.57 ±4.24%. Patients with poor lung function generally have poorer lung compliance and are more prone to intraoperative lung injury, increasing the incidence of ARDS. In thoracic surgery, the upper lung is better ventilated but poorer perfused than the lower lung as the patient is predominantly in the lateral position, resulting in a more pronounced imbalance in the ventilation/flow ratio than that in other surgical patients, which is more severe with single-lung ventilation. Additionally, intraoperative anesthetic suppression and postoperative pain deter patients with lung cancer postoperatively from breathing hard and coughing, which interferes with sputum evacuation and lung expansion. These factors may result in a low postoperative FEV1% prediction, thus, making patients prone to ARDS. Therefore, the maintenance of the patient’s pulmonary function should be enhanced, and reasonable and effective analgesia should be provided. Additionally, SAERPA NETO A et al found26 that ventilator-associated lung injury can be induced in patients with non-ARDS, even with the application of conventional tidal volumes. Therefore, the tidal volume during mechanical ventilation is reduced from the conventional 10–12 mL/kg body weight to 6–8 mL/kg body weight, even in patients with healthy lungs, to prevent the occurrence of ARDS.
ALAM N et al reported25 that every 500 mL increase in perioperative fluid volume was associated with a 17% increase in postoperative ARDS risk. The results of this study showed that the perioperative crystalloid infusion amount was an independent risk factor for the development of ARDS after lung cancer, with a mean crystalloid input of (2669.28 ±273.00) mL and (2002.01 ±288.90) mL in the ARDS and non-ARDS groups, respectively. The increased pulmonary capillary osmolarity after pneumonectomy and an excessive amount of crystals could lead to pulmonary edema, thus, increasing the ARDS development risk. Idealized perioperative fluid management is a concern in thoracic surgery treatment and care. Strictly limiting rehydration will decrease blood volume leading to inadequate tissue perfusion, yet excessive rehydration will lead to pulmonary complications.27 Therefore, the amount of perioperative crystalloid infusion should be controlled, while maintaining circulatory stability and ensuring tissue and organ perfusion.
Additionally, factors that may affect the patient prognosis based on Cox risk regression screening included whether or not they had combined T2DM. In this study, the combination of T2DM in patients with lung cancer was both an independent risk factor for the ARDS development after surgery and a reflection of the patient’s condition, which was associated with the survival prognosis. The complex pathophysiological mechanism of ARDS owing to type 2 diabetic lung cancer after surgery leads to rapid deterioration and disease progression and often has a poor survival prognosis. To improve the prognosis of patients with lung cancer undergoing surgical treatment, focusing on multiple factors contributing to the development of ARDS after surgery and minimizing the occurrence of postoperative ARDS is beneficial.
This study has some limitations. This was a retrospective analysis, where the study indicators were from the same hospital data; however, owing to the collection period, the influence of laboratory tests and treatment methods on the data in different periods, and the study sample size being small, the risk factors included in the analysis of indicators was limited.
In conclusion, this study clarified the effect of T2DM on the development of ARDS and its prognosis in patients with lung cancer after surgery and other risk factors, thus, providing a theoretical basis for the effective prevention and treatment of the risk of ARDS after surgery. However, many factors associated with the development of ARDS after lung cancer surgery exist, and more randomized controlled studies with large samples should be performed to further explore the valuable risk factors.
Conclusion
In lung cancer patients with type 2 diabetes, postoperative ARDS is more likely to occur, and both diabetes and postoperative ARDS are risk factors affecting the survival of patients with lung cancer. The control of preoperative and postoperative blood glucose to reduce the chances of ARDS should be reviewed.
Ethical Statement
The authors are accountable for all aspects of the work, including ensuring that any questions related to the accuracy or integrity of any part of the work have been appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Ethics Committee of Affiliated Hospital of Jiangnan University (No. LCKY2016281) and all the patients have provided informed consent.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes At⁃las: global, regional and country⁃level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013-2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
3. Giblin MJ, Ontko CD, Penn JS. Effect of cytokine⁃induced alterations in extracellular matrix composition on diabetic retinopathy⁃relevant endothelial cell behaviors. Sci Rep. 2022;12(1):12955. doi:10.1038/s41598-022-12683-7
4. Zhang R, Chen J, Xiong Y, et al. Increased neutrophil count Is associated with the development of chronic kidney disease in patients with diabetes. J Diabetes. 2022;14(7):442–454. doi:10.1111/1753-0407.13292
5. Ehrlich SF, Quesenberry CP, Van Den Eeden SK, Shan J, Ferrara A. Patients diagnosed with diabetes are at increased risk for asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and pneumonia but not lung cancer. Diabetes Care. 2010;33(1):55–60. doi:10.2337/dc09-0880
6. Wilson EB. A correlation curiosity. Science. 1932;76(1979):515–516. doi:10.1126/science.76.1979.515
7. Jia H, Tian Y, Jiang CG, Han W. Evaluation of 29 indicators for the prognosis of advanced non---small cell lung cancer with cytokine--induced killer cell therapy combined with chemotherapy. Exp Ther Med. 2016;11(5):1601–1610. doi:10.3892/etm.2016.3102
8. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149(4):778–789. doi:10.1002/ijc.33588
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
10. Cao W, Chen HD, Yu YW, Li N, Chen WQ. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
11. Ye B, Wang M. Video-assisted Thoracoscopic Surgery versus Thoracotomy for Non-Small Cell Lung Cancer: a Meta-Analysis. Comb Chem High Throughput Screen. 2019;22(3):187–193. doi:10.2174/1386207322666190415103030
12. Dell’Amore A, Lomangino I, Cannone G, et al. Comparison of operative and postoperative characteristics and outcomes between thoracoscopic segmentectomy and lobectomy for non-small-cell lung cancer: a propensity score matching study from the Italian VATS Group Registry. Eur J Cardiothorac Surg. 2022;61(3):533–542. doi:10.1093/ejcts/ezab430
13. Ranieri VM, Rubenfeld GD, Thompson BT, et al.; ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. doi:10.1001/jama.2012.5669
14. Wang CR, Hu TY, Hao FB, et al. Type 2 Diabetes-Prevention Diet and All-Cause and Cause-Specific Mortality: a Prospective Study. Am J Epidemiol. 2022;191(3):472–486. doi:10.1093/aje/kwab265
15. Huang I, Lim MA, Pranata R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020;14(4):395–403. doi:10.1016/j.dsx.2020.04.018
16. Lima-Martínez MM. COVID-19 and diabetes: a bidirectional relationship. Clin investigacion en arteriosclerosis. 2020;33(3).
17. Soto GJ, Kor DJ, Park PK, et al. Lung Injury Prediction Score in Hospitalized Patients at Risk of Acute Respiratory Distress Syndrome. Crit Care Med. 2016;44(12):2182–2191. doi:10.1097/CCM.0000000000002001
18. Akash MSH, Rehman K, Liaqat A. Tumor Necrosis Factor-Alpha: role in Development of Insulin Resistance and Pathogenesis of Type 2 Diabetes Mellitus. J Cell Biochem. 2018;119(1):105–110. doi:10.1002/jcb.26174
19. Guo J, Liu C, Pan J, Yang J. Relationship between diabetes and risk of gastric cancer: a systematic review and meta-analysis of cohort studies. Diabetes Res Clin Pract. 2022;187:109866. doi:10.1016/j.diabres.2022.109866
20. Ikeda F, Doi Y, Yonemoto K, et al. Hyperglycemia increases risk of gastric cancer posed by helicobacter pylori infection: a population-based cohort study. Gastroenterology. 2009;136(4):1234–1241. doi:10.1053/j.gastro.2008.12.045
21. Hughes M, MacKirdy FN, Ross J, Norrie J, Grant IS; Scottish Intensive Care Society. Acute respiratory distress syndrome: an audit of incidence and outcome in Scottish intensive care units. Anaesthesia. 2003;58(9):838–845. doi:10.1046/j.1365-2044.2003.03287.x
22. Inoue M, Iwasaki M, Otani T, Sasazuki S, Noda M, Tsugane S. Diabetes mellitus and the risk of cancer: results from a large-scale population-based cohort study in Japan. Arch Intern Med. 2006;166(17):1871–1877. doi:10.1001/archinte.166.17.1871
23. Weekers F, Giulietti AP, Michalaki M, et al. Metabolic, endocrine, and immune effects of stress hyperglycemia in a rabbit model of prolonged critical illness. Endocrinology. 2001;144(12):5329–5338. doi:10.1210/en.2003-0697
24. Jakobsen E, Palshof T, Osterlind K, Pilegaard H. Data from a national lung cancer registry contributes to improve outcome and quality of surgery: Danish results. Eur J Cardiothorac Surg. 2009;35(2):348–352. doi:10.1016/j.ejcts.2008.09.026
25. Alam N, Park BJ, Wilton A, et al. Incidence and risk factors for lung injury after lung cancer resection. Ann Thorac Surg. 2007;84(4):1085–1091. doi:10.1016/j.athoracsur.2007.05.053
26. Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syn drome: a meta analysis. JAMA. 2012;308(16):1651–1659. doi:10.1001/jama.2012.13730
27. Matthias J, Daniel C, Markus R. Clinical update: perioperative fluid management. Lancet. 2007;369(9578):1984–1986. doi:10.1016/S0140-6736(07)60926-X
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Mutational and Transcriptional Characterization Establishes Prognostic Models for Resectable Lung Squamous Cell Carcinoma
Liu Y, Duan J, Zhang F, Liu F, Luo X, Shi Y, Lei Y
Cancer Management and Research 2023, 15:147-163
Published Date: 17 February 2023
GABRP is a Promising Prognostic Biomarker and Associated with Immune Cell Infiltration in Lung Squamous Cell Carcinoma
Fu J, Lin J, Zeng X, Li G, Wei Y, Xian L
Pharmacogenomics and Personalized Medicine 2023, 16:357-371
Published Date: 15 April 2023
Metabolic Score for Insulin Resistance (METS-IR) Predicts Adverse Cardiovascular Events in Patients with Type 2 Diabetes and Ischemic Cardiomyopathy
Zhang X, Liu F, Li W, Zhang J, Zhang T, Yu X, Luo J, Zhao Q, Zhang J, Fang B, Yang Y, Li X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1283-1295
Published Date: 5 May 2023
Risk Factors and Prognostic Analysis of Immune Checkpoint Inhibitor-Related Colitis in Lung Cancer
Wang S, Tian B, Wang H
Journal of Inflammation Research 2024, 17:7535-7542
Published Date: 21 October 2024
Influence of Type 2 Diabetes Mellitus on the Clinical Outcomes in Hospitalized Patients with Active Pulmonary Tuberculosis: A Retrospective, Single-Center, Real-World Study in China
Shi C, Shen X, Liu J, Huang L, Ni H, Tang P, Feng Y, Wu M, Zhang J
Infection and Drug Resistance 2025, 18:2415-2425
Published Date: 8 May 2025