Back to Journals » Nature and Science of Sleep » Volume 17

Effect of Transcutaneous Electrical Acupoint Stimulation on Postoperative Sleep Disorders in Older Patients After Urologic Laparoscopic Surgery by Regulating Intestinal Microbiota: Study Protocol for a Prospective Controlled Trial
Authors Liu X ![]() , Fan Y, Wu C
, Fan Y, Wu C ![]() , Hu R
, Hu R ![]() , Wang T, Cao Y, Liu G, Zhang L
, Wang T, Cao Y, Liu G, Zhang L ![]() , Han T
, Han T
Received 17 November 2024
Accepted for publication 13 September 2025
Published 29 September 2025 Volume 2025:17 Pages 2387—2398
DOI https://doi.org/10.2147/NSS.S503267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Xuming Liu,1 Yichang Fan,1 Chen Wu,1 Ran Hu,2 Tengti Wang,1 Yang Cao,1 Guokai Liu,2 Li Zhang,3 Tiandong Han4
1Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Department of Anesthesiology and Operating Room, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 4Department of Urology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Tiandong Han, Email [email protected] Li Zhang, Email [email protected]
Background: Postoperative sleep disorders (PSD) are common complications that may impair recovery and increase the risk of adverse events after surgery. Transcutaneous electrical acupoint stimulation (TEAS), a non-invasive therapy based on traditional Chinese medicine, has shown potential in improving sleep quality. This study aims to investigate whether TEAS can alleviate PSD in older patients undergoing urologic laparoscopic surgery.
Methods: This is a prospective, randomized, double-blind, controlled clinical trial. A total of 124 patients scheduled for urologic laparoscopic surgery will be randomly assigned to either the TEAS group (receiving active stimulation) or the sham group (receiving placebo stimulation). Randomization will also be stratified according to the use of dexmedetomidine. The primary outcome is the Athens Insomnia Scale (AIS) score on the postoperative night (D2), compared between groups using ANCOVA adjusted for preoperative (baseline) AIS and the dexmedetomidine stratification factor. Secondary outcomes include the night-to-night trajectory of AIS across D0–D2, objective sleep parameters measured by a portable monitor on D0–D2, postoperative VAS pain scores, perioperative changes in intestinal microbiota and serum brain–gut peptides, intraoperative hemodynamics and drug consumption, durations of surgery/anesthesia/extubation, postoperative complications, and healthcare-related costs.
Discussion: This trial aims to explore whether TEAS can improve postoperative sleep quality in older patients by regulating intestinal microbiota. The findings are expected to provide evidence supporting the clinical application of TEAS for managing PSD in this patient population.
Clinical Trial Registration: ChiCTR2400086911 (Registered on 15 July 2024) https://www.chictr.org.cn/showproj.html?proj=220900.
Keywords: transcutaneous electrical acupoint stimulation, postoperative sleep disorders, intestinal microbiota, urologic surgery
Background
Postoperative sleep disorders (PSD), which are frequently seen right away after surgery, include symptoms like falling asleep difficulty and irregular circadian rhythms in the postoperative period caused by surgical stimulation, anesthetic usage, pain, stress, and anxiety. Sleep disorders can cause postoperative delirium, increase pain sensitivity, and even promote postoperative cardiovascular adverse events in high-risk patients and affect postoperative recovery from pre-existing conditions.1–3 Many studies have confirmed the high incidence of PSD in response to surgical stimulation, especially laparoscopic surgery, with an incidence of up to 44%.4 And advanced age is a risk factor for developing PSD.5 Therefore, reducing the occurrence of PSD in the elderly after laparoscopy is of great significance in promoting postoperative recovery.
Transcutaneous electrical acupoint stimulation (TEAS) is a traditional Chinese medicine technique that affects certain functions by electroacupuncture to specific parts of the body. Numerous studies have shown that TEAS can repair the sleep structure, reconstruct the continuity of sleep, and improve the sleep quality of insomnia patients.6,7 Evidence from a recent systematic review and meta-analysis of randomized trials indicates that acupuncture-based interventions can also improve objective sleep indices—extending total sleep time, increasing sleep efficiency, and reducing wake after sleep onset and nocturnal awakenings.8 Our group has also found in previous studies that electroacupuncture stimulation of bilateral Shen Men and Neiguan acupoints can improve postoperative sleep quality in patients undergoing thoracoscopic surgery. However, the mechanism by which TEAS improves postoperative sleep is still not known.
As the “microbial organ” of the human body, the intestinal flora is an important part of various physiological and pathological processes and is intimately linked to neuromodulation as part of the brain-gut axis. Sen et al9 discovered that the brain-gut-microbiota axis might be associated with the regulation of the Sleep-Wake mechanism, through neurological, endocrine, immunological, and metabolic pathways. Thompson et al10 also found a connection between gut microbiota and sleep physiology. Therefore, using some interventions to regulate gut microbiota may improve sleep quality, which can offer some fresh diagnostic ideas for the treatment of PSD.
Based on the above research status, we designed a clinical randomized controlled trial and hypothesized that TEAS of dominant acupoints could improve PSD after urologic laparoscopic surgery by regulating the intestinal microbiota through some clinical outcomes, such as postoperative sleep quality scores in the elderly.
Methods/Design
Study Design, Randomization, and Blinding
This trial was a prospective, randomized, controlled, double-blind study conducted by the Department of Anaesthesiology, Beijing Friendship Hospital, Capital Medical University. It has been authorized by the Bioethics Committee of Beijing Friendship Hospital (2023-P2-107-01) and the Chinese Clinical Trial Registry (ChiCTR2400086911). A total of 124 older patients who underwent laparoscopy were enrolled in this trial.
We used a randomized computer-generated numbered table of four numbers in a block, and participants were assigned natural numbers. Then, they were divided into two groups in a 1:1 ratio: the TEAS group and the sham electric stimulation group (the sham group), and stratified by planned intraoperative dexmedetomidine use. Subsequently, using the same method, each group was equally divided into two subgroups based on whether dexmedetomidine was used to maintain intraoperative anesthesia (n=31) (Figure 1).
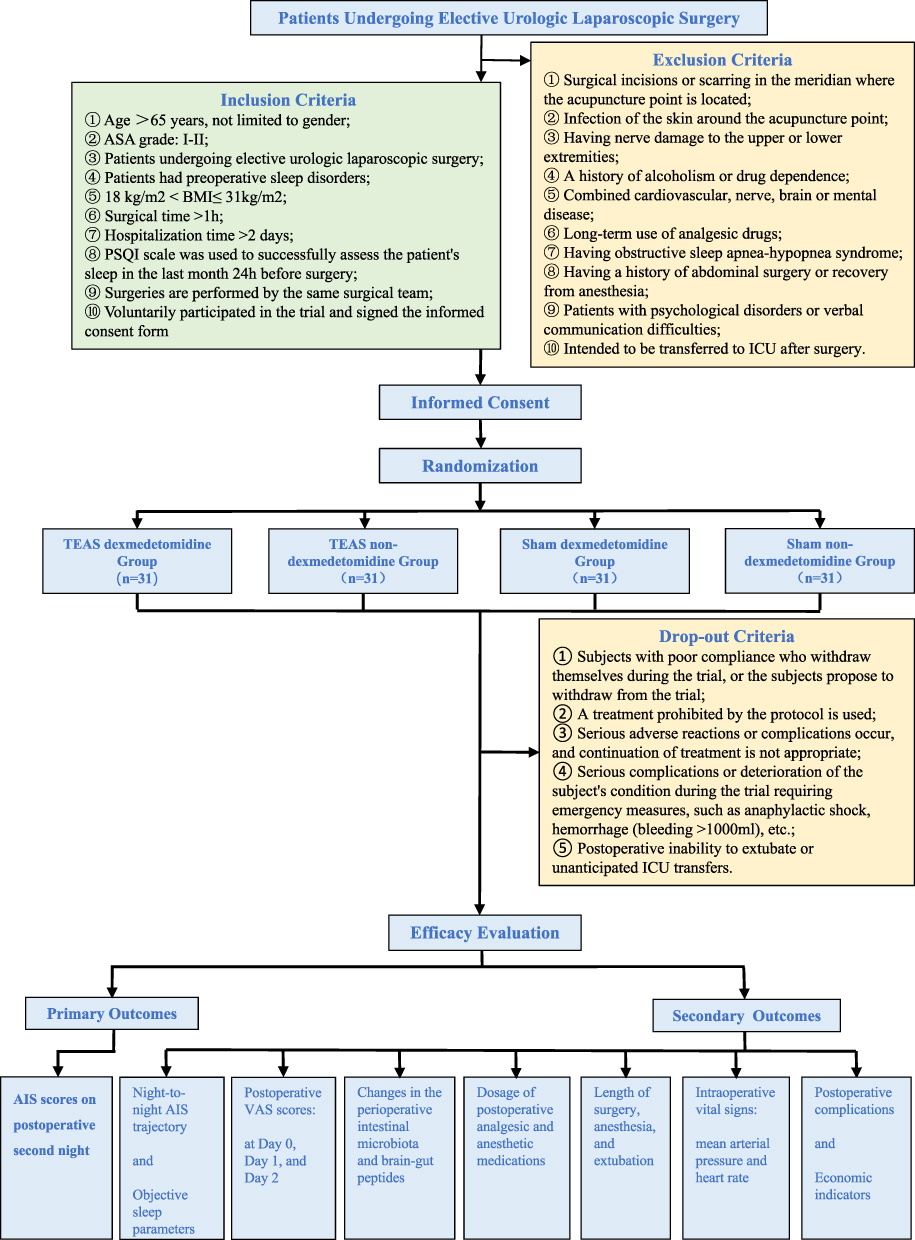 |
Figure 1 Flowchart. |
For the results of the trial to be evaluated objectively, a double-blind method was used. After the participants were randomized, a researcher placed the subject numbers and groups in a sequentially numbered, opaque, sealed envelope. This envelope was then opened by the anesthesiologist (A), who performed the TEAS and processed it accordingly. Anesthesiologist (A) had completed formal training in TEAS procedures and was certified before trial initiation. The perioperative clinical data were recorded by another anesthesiologist (B) who was unaware of the grouping. Throughout the trial, the recorder (B) and the participants were unaware of the grouping. Devices in both groups displayed identical lights/sounds. To preserve credibility, the sham group used a minimal-dose active-sham (continuous 4 mA, sensory-level).11
We will assess blinding at two prespecified time points (after the first session and on the postoperative second day) using a short questionnaire and Bang’s Blinding Index (BI) with 95% CIs; if unblinding is suggested, prespecified sensitivity analyses will include treatment-belief as a covariate and provide stratified results. Emergency unblinding is permitted only for participant safety and requires authorization by the principal investigator; all unblinding events will be documented.
In order to improve subject enthusiasm and adherence, the head researcher will give them some small gifts, such as keychains, water bottles, etc, during recruitment.
Study Population
We will recruit 124 patients proposed for elective urologic laparoscopic surgery to participate in the trial at the preoperative visit based on the following criteria.
Inclusion criteria: ① Age >60 years, not limited to gender; ② ASA grade: I–II; ③ Patients undergoing elective urologic laparoscopic surgery; ④ Patients had preoperative sleep disorders; ⑤ Body mass index (BMI): 18 kg/m2 < BMI≤ 31kg/m2; ⑥ Surgical time >1h; ⑦ Hospitalization time >2 days; ⑧ The Pittsburgh Sleep Quality Index (PSQI) scale was used to successfully assess the patient’s sleep in the last month 24h before surgery; ⑨ Surgeries are performed by the same surgical team; ⑩ Voluntarily participated in the trial and signed the informed consent form.
Exclusion criteria: ① Surgical incisions or scarring in the meridian where the acupuncture point is located; ② Infection of the skin around the acupuncture point; ③ Having nerve damage to the upper or lower extremities; ④ A history of alcoholism or drug dependence; ⑤ Combined cardiovascular, nerve, brain or mental disease; ⑥ Long-term use of analgesic drugs; ⑦ Having obstructive sleep apnea–hypopnea syndrome; ⑧ Having a history of abdominal surgery or recovery from anesthesia; ⑨ Patients with psychological disorders or verbal communication difficulties; ⑩ Intended to be transferred to ICU after surgery.
Recruited subjects will be dropped out from the trial in the event of the following: ① Subjects with poor compliance who withdraw themselves during the trial, or the subjects propose to withdraw from the trial; ② A treatment prohibited by the protocol is used; ③ Serious adverse reactions or complications occur, and continuation of treatment is not appropriate; ④ Serious complications or deterioration of the subject’s condition during the trial requiring emergency measures, such as anaphylactic shock, hemorrhage (bleeding >1000mL), etc.; ⑤ Postoperative inability to extubate or unanticipated ICU transfers.
Procedure
At the preoperative visit, patients who met the inclusion and exclusion criteria were recruited to participate in the trial. The Pittsburgh Sleep Quality Index (PSQI; used for academic, non-commercial purposes) scale was used to assess the patient’s sleep quality in the last month.12 We will additionally collect a baseline AIS on the night before surgery. To ensure the results are as objective as possible, we will select the same surgical team to assist in this trial.
- Five milliliters of venous blood and a small amount of feces were retained from the patients to test for brain-gut peptide in blood and intestinal microbiota in feces when patients were recruited on the ward preoperatively.
- Noninvasive blood pressure, heart rate (HR), electrocardiogram, and pulse oxygen saturation (SpO2) were routinely monitored after the patient entered the operating room. Radial artery puncture was performed under local anesthesia to measure invasive arterial blood pressure. Bispectral index (BIS) was also performed to monitor the patient’s depth of anesthetic consciousness.
- Patients were given midazolam (0.04 mg/kg), cis-atracurium (0.15 mg/kg), sufentanil (0.3 μg/kg), and propofol (2.0 mg/kg) for rapid anesthetic induction. And intubation was performed using a spiral-flex reinforced tracheal tube 3 min after induction (7.0mm for females and 7.5mm for males).
- The ventilator was used in volume-controlled ventilation mode, with a set inspiratory/expiratory ratio of 1:2, a tidal volume (VT) of 8 mL/kg, and a respiratory rate of 12–15 breaths/min (maintaining PETCO2 at 35–45 mmHg).
- Anesthesia was maintained by intravenous infusion of propofol 3–6 mg/(kg·h), remifentanil 0.1–0.2 μg/(kg·min), and BIS was controlled at 40–60.
- The intraoperative fluid infusion rate was 6–8 mL/(kg·h), maintaining mean arterial pressure (MAP) fluctuation not more than 30% of the basal value. When MAP <30% of the basal value, ephedrine 6mg was infused intravenously. About 0.5mg of atropine was infused intravenously when HR <50 beats/min, and 10mg of esmolol was infused intravenously when HR >120 beats/min.
- Intraoperative use of sufentanil and cis-atracurium was based on the judgment of the anesthesiologist performing the TEAS based on the surgical course and hemodynamics.
- To prevent postoperative pain from affecting the quality of sleep, patients were given sufentanil 0.1 μg/kg and flurbiprofen 50mg before suturing the surgical incision. After surgery, we will give the patient an electronic analgesic pump formulated with sufentanil 100 μg and ondansetron 16 mg diluted into 100 mL of saline. The analgesic pump was set to a background rate of 2 mL/h, a self-control dose of 2 mL/times, and a lock time of 30 minutes.
- Perioperative antibiotics were prescribed according to clinical decision and recorded (agent, start/stop date).
- First oral intake and diet stage by night (clear liquids/soft or semi-solid/regular) were recorded based on nursing documentation and patient self-report during postoperative visits.
Intraoperative complications were managed by the anesthesiologist (A), who performed the TEAS according to clinical guidelines. Anesthesia-related data, intraoperative medication doses, and intraoperative adverse events were recorded by another anesthesiologist (B) who was unaware of the subgroups. Opioid use was converted to intravenous morphine milligram equivalents (MME) by period. All patients were catheterized preoperatively.
Intervention
Patients in the TEAS group received electrical stimulation at different time points, and patients in the sham group received sham electrical stimulation with an intensity of 4 mA at the same time points.11
Before each session, target acupoints were pre-marked per anatomical landmarks; placement was cross-checked by a second team member whenever feasible. Skin was cleaned, and initial skin impedance was verified; electrodes were re-prepped/repositioned if impedance was above the acceptable range. Operators recorded planned/actual duration, intensity, frequency, maximum stimulation, skin impedance, and adverse sensations.
TEAS Procedure
We selected the patient’s bilateral Shenmen, Neiguan, Fuliu points for stimulation using Han’s acupoint nerve stimulator (HANS200A Nanjing Jisheng Medical Technology Co., Nanjing, Jiangsu Province, China, a device designed for TEAS application; Figure 2). The Shenmen point is located at the ulnar end of the palmar transverse stripe of the wrist, in the radial depression of the ulnar flexor carpi radialis tendon. The Neiguan point is located 2 inches above the distal transverse stripe on the palmar side of the wrist, between the tendon of the palmaris longus and the tendon of the radial flexor carpi radialis. The Fuliu point is located 2 inches above the tip of the inner ankle, in the depression of the anterior border of the Achilles tendon (Figure 3).
- Before each implementation of TEAS, mark the patient’s bilateral Shenmen, Neiguan, and Fuliu points. The self-adhesive gel electrodes were placed after sterilizing the skin where the points are located.
- Set the frequency of Han’s acupoint nerve stimulator to 2/100 Hz; the intensity was 2–3 times the subject’s sensory threshold.
- The maximum stimulation threshold was 15 mA.
- We will give patients 30 minutes of electrical stimulation 30 minutes before the anesthesia induction and apply it continuously during surgery.
- Postoperatively, we will give patients 30 minutes of electrical stimulation on the day of surgery (D0), day 1 (D1), and day 2 (D2) before bedtime.
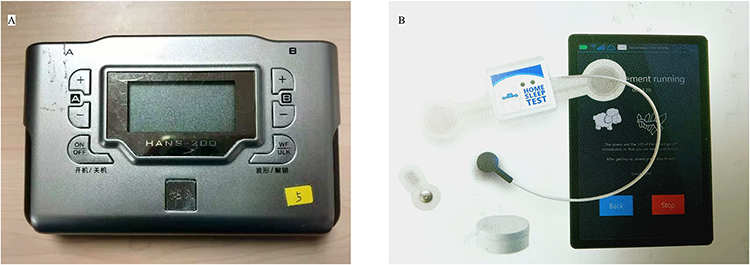 |
Figure 2 Han’s acupoint nerve stimulator. (A) HANS200A (the device for TEAS application); (B) The self-adhesive gel electrodes. |
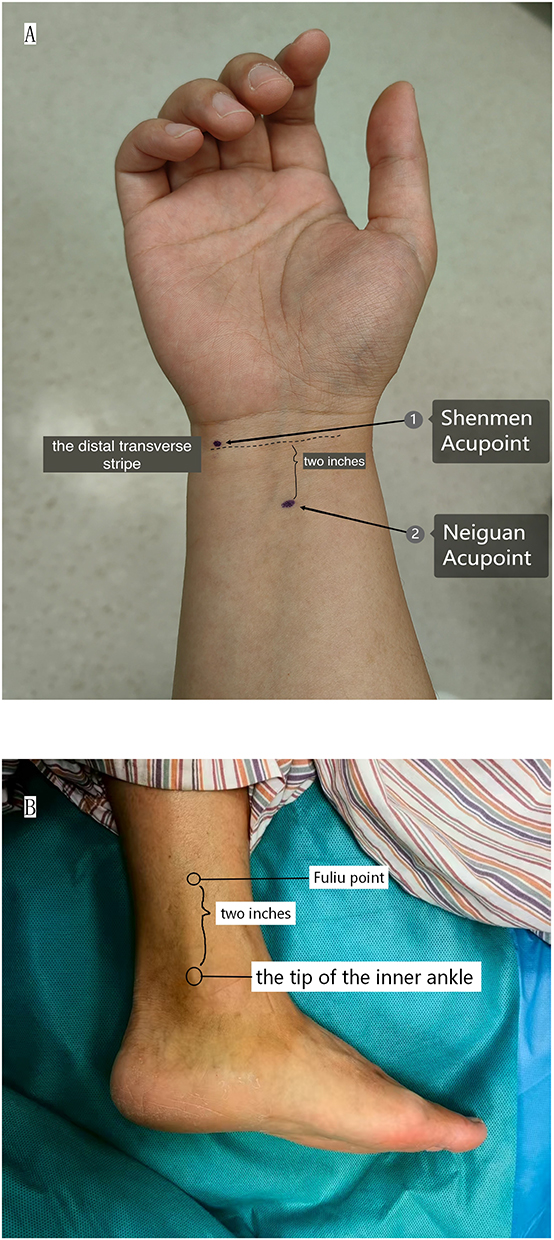 |
Figure 3 Electrode placement for TEAS and sham. (A) Wrist view showing Shenmen and Neiguan with landmarks; (B) Inner ankle view showing Fuliu point 2 inches above the tip of the inner ankle. |
Intravenous Infusion of Dexmedetomidine
Patients in the dexmedetomidine subgroup were maintained under intraoperative anesthesia with the addition of dexmedetomidine 0.2 μg/(kg·h) intravenously. Patients in the non-dexmedetomidine subgroup were given continuous intravenous saline infusion at the same rate.
Study Outcomes
The Primary Outcomes
The primary outcome is subjective sleep quality on the postoperative second night (D2), assessed with the Athens Insomnia Scale (AIS; used for academic, non-commercial purposes).13 The primary comparison is the between-group difference (TEAS vs sham) at D2. An AIS score of ≤4 was classified as no sleep disorders; 4–6 as suspected insomnia; and >6 as insomnia.
The Secondary Outcomes
The secondary outcomes included the night-to-night AIS trajectory, objective sleep parameters, postoperative visual analog scale (VAS) scores, changes in the perioperative intestinal microbiota and brain-gut peptides, dosage of postoperative analgesic and anesthetic medications, intraoperative vital signs, length of surgery, anesthesia, and extubation, postoperative complications, and economic indicators.
- Night-to-night AIS trajectory: We will record the AIS score at bedtime on the day of the surgery (D0), on the postoperative first (D1) and second day (D2). Assessing improvement over time and the group-by-time interaction.
- Objective sleep parameters: We will monitor objective postoperative sleep quality by wearing a portable sleep monitoring device (SOMNO screen V3 Taihemed Medical Technology Co., Beijing, China; Figure 4) for the patient at bedtime across D0-D2, and after administration of TEAS or sham electrical stimulation. Through the data monitored by the device, the patient’s nocturnal sleep process (sleep latency, number of awakenings, awakening time, fast-wave sleep latency, sleep efficiency, and total sleep time) and sleep structure (slow-wave sleep and fast-wave sleep) were analyzed.
- Postoperative VAS scores: We will assess the patient’s pain at rest and during exercise using the VAS score at D0, D1, and D2, respectively.
- Changes in the perioperative intestinal microbiota and brain-gut peptides: On the second postoperative day (D2), 5 mL of venous blood and a small amount of feces were retained and sent for examination to observe the changes of 5-hydroxytryptamine (5-HT), substance P (S.P.), vasoactive intestinal peptide (VIP) in the blood and intestinal microbiota in the feces compared with those of the preoperative period.
- Dosage of postoperative analgesic and anesthetic medications.
- Length of surgery, anesthesia, and extubation.
- Intraoperative vital signs: MAP and HR were recorded before anesthesia induction (T0), 5 min after anesthesia induction (T1), 30 min before the end of the surgery (T2), at the end of the surgery (T3), and at the time of extubation (T4).
- Postoperative complications: We will record complications occurring within 48 hours postoperatively. The occurrence of the following events will be defined as a positive postoperative complication.
- Nausea and vomiting.
- Pulmonary complications: One of the following events occurring was considered a postoperative pulmonary complication.14
- Pulmonary atelectasis: Diagnosed by CT or X-ray;
- Pneumothorax or pleural effusion: Diagnosed by X-ray;
- Acute respiratory distress syndrome: Oxygenation index ≤300mmHg;
- Pulmonary embolism: Diagnosed by CT;
- Aspiration pneumonia: Diagnosed by tracheoscopy.
- Respiratory depression: Patients were defined as respiratory depression if they experienced one of the following postoperative events: slowed respiratory rate (<12 breaths/min), decreased tidal volume (VT <400 mL), decreased partial pressure of oxygen (arterial partial pressure of oxygen <80 mmHg), and increased partial pressure of carbon dioxide (arterial partial pressure of carbon dioxide >45 mmHg).
- Tachycardia, bradycardia, hypertension, and hypotension: the fluctuation of more than 30% of the preoperative basal value.
- Economic indicators: Length of hospitalization, hospitalization costs, and anesthesia costs.
 |
Figure 4 SOMNO screen V3 (the portable sleep monitoring device). |
Biospecimen Assessments
Fecal samples will be collected twice per participant: at baseline (preoperative ward visit) and on postoperative day 2 (D2), using sterile screw-cap tubes. Samples will be frozen at −80°C within 2 hours of collection and transported on dry ice. Negative controls (blank extraction tubes) and a mock community will be included to monitor batch effects and contamination.
Venous blood samples (5 mL) will be collected preoperatively and on postoperative day 2. Samples will be transported on ice, centrifuged, aliquoted, and stored at −80°C.
All biospecimens will be centrally stored and analyzed by an external certified laboratory.
Data Collection and Monitoring
Recording of basic characteristics, intraoperative medication doses, vital signs, postoperative AIS scores, and other observations that need to be obtained in the post-anesthesia care unit or ward was done by the anesthesiologist (B), who was unaware of the subgroups. Intraoperative dexmedetomidine infusions, other drug infusions, intraoperative and postoperative TEAS or sham electrical stimulation administered by the anesthesiologist (A) who was aware of the grouping (patient groupings were obtained by opening sealed envelopes before administering the intervention).
All raw data are recorded in the case report form (CRF), and missing data are recorded as such. The CRFs are available at this website: https://www.chictr.org.cn/showproj.html?proj=220900.
The data monitoring committee (DMC) consists of three anesthesiologists, a statistician, and a scientific researcher. The functions of the DMC are trial protocol development and improvement, case grouping, data analysis and management, and results proofreading. When approximately 50% of participants have completed outcome assessments, the DMC will conduct a blinded interim data review focused on safety events, protocol adherence, data completeness, and recruitment progress. No hypothesis testing of the primary endpoint will be undertaken at interim; there are no efficacy-based stopping rules, and the final significance level remains as prespecified.
Electronic data will be placed into a password-protected Email that will not be shared with the public until the results are released, together with the original data and results, which will be delivered to DMC. To aid in the retention and thorough follow-up of participants, all original records (CRFs, informed consent forms, and related documents) will be preserved and retained for ten years before being destroyed following hospital regulations.
Sample Size Calculation
The primary outcomes in this trial were postoperative sleep quality assessments. According to the results of our pre-trial (N=12; descriptive statistics calculated in SPSS 26.0), the AIS score on postoperative day 2 was 3.6±0.8 in the TEAS group and 4.1±0.7 in the sham group. For sample-size planning, we assumed a between-group mean difference (Δ) of 0.5 AIS points and a common standard deviation (σ) of 0.8 (chosen conservatively as the larger SD observed in the pre-trial). The sample size was calculated in PASS 15.0 using a one-sided superiority test with α=0.025 and power (1−β)=0.90 and using a test of superiority for comparison of the means of the two groups, with the superiority cutoff set at 0, to arrive at the need for a total of 110 cases. Adding a 10% dropout rate, a total of 124 patients were needed, 31 in each subgroup.
A mid-trial data review by the DMC will be conducted for safety, data quality, adherence, and recruitment monitoring only. No interim efficacy testing or alpha-spending will be performed, so the final significance level remains α=0.025.
Statistical Analysis
We will use SPSS 26.0 to analyze the data. All quantitative indicators that meet the normal distribution are expressed as mean ± standard deviation and analyzed using parametric tests. Those that do not meet the normal distribution are expressed as median (quartiles) and analyzed by non-parametric tests. All qualitative indicators were expressed as frequencies (percentages) and analyzed by chi-square test or Fisher’s exact test.
The longitudinal trajectory of AIS across D0–D2 and objective sleep parameters (D0–D2) will be analyzed using linear mixed-effects models with a random intercept for participants and fixed effects for group, time (categorical: D0, D1, D2), and group × time interaction; baseline AIS and the dexmedetomidine factor will be included as covariates. Perioperative antibiotics, other additional medications, and postoperative diet stage were recorded and will be included as covariates in sensitivity analyses of AIS and microbiota outcomes. Logistic regression analysis was also applied to identify risk factors for PSD.
Subgroup analysis will be performed to explore whether dexmedetomidine affects PSD. The incidence of PSD will also be analyzed by the chi-square test or Fisher’s exact test. For repeated-measures outcomes (eg, AIS D0–D2, objective sleep indices), mixed-effects models inherently accommodate missing-at-random data. For non-longitudinal outcomes (including the primary D0 AIS if missing), we will conduct multiple imputation by chained equations (MICE) as a sensitivity analysis (eg, m = 20 imputations), including treatment group, baseline AIS, dexmedetomidine factor, age, sex, BMI, antibiotic/opioid use, and other outcome-related covariates in the imputation model; estimates will be pooled using Rubin’s rules. A complete-case analysis will be reported as a sensitivity check.
We prespecify a single primary endpoint (AIS at D2), controlling the family-wise error for the primary analysis. Key secondary endpoints will follow a hierarchical sequence: (1) overall group × time effect for AIS (D0–D2); (2) AIS between-group difference at D0; (3) AIS at D1; (4) objective sleep efficiency (D2). If an earlier step is not significant, subsequent inferences will be considered supportive/exploratory. Remaining secondary/exploratory outcomes will be summarized with 95% CIs and, where appropriate, controlled by false discovery rate (Benjamini–Hochberg, q<0.05).
Discussion
This is a prospective, double-blind, randomized, controlled trial. It aims to verify whether preoperative, intraoperative, and early postoperative application of TEAS can effectively improve PSD in elderly urologic laparoscopic patients by modulating the brain-gut axis through intestinal flora.
Postoperative sleep disorders are a condition that can severely impact a patient’s recovery from surgery by contributing to increased chronic pain,15 changes in a patient’s circadian rhythms,16 and an increased risk of postoperative delirium,2 to name a few. Therefore, choosing appropriate methods to reduce the occurrence of PSD has become an urgent problem in recent years.
Transcutaneous electrical acupoint stimulation is a traditional Chinese medical treatment that produces therapeutic effects by stimulating points with electroacupuncture. Many studies have confirmed the efficacy of TEAS in improving PSD by stimulating dominant acupoints.17,18 However, the pathway through which TEAS regulates sleep architecture remains unknown.
The brain-gut axis is an important mediator linking the brain and the gut. Existing studies have demonstrated that brain-gut peptides such as 5-HT, S.P, VIP, etc., are not only involved in related metabolism but also may be involved in the modulation of the Sleep-Wake mechanism by regulating the intestinal microbiota.19–21 Jang et al22 have demonstrated in recent years in animal models that acupuncture can regulate the intestinal microbiota and thus play a neuroprotective role. Zhang et al23 have also found that recovery of cerebral neurological function after ischemic stroke may be facilitated by acupuncture at major acupoints.
Notwithstanding this rationale, the microbiome component of our protocol has important limitations. Sampling is restricted to a short perioperative window (baseline to D2), which is appropriate for detecting early perturbations but may miss durable compositional change. In addition, perioperative exposures—prophylactic antibiotics, diet transitions, bowel preparation, and opioid dose—may introduce residual confounding despite prospective recording and planned sensitivity analyses. Accordingly, microbiome and peptide readouts are prespecified as exploratory.
Based on the current state of research above, we hypothesized that the improvement of PSD by TEAS also acts through intestinal microbiota. This trial will confirm that TEAS does improve sleep disorders after urologic laparoscopy and that the mechanism of action may be related to the regulation of intestinal flora. It will provide new clinical evidence that TEAS can accelerate patients’ recovery after urologic laparoscopic surgery.
Trial Status
This trial protocol was approved on April 18, 2023, and the first subject was successfully recruited on the same day. The current protocol version is V2.3/2024.02.18, and if we need to update it in the future, we will submit amendments to the ethics committee and clinical trial registry. To date, we have enrolled a total of 48 patients with an enrollment deadline of February 28, 2025. This trial is now ongoing.
Abbreviations
PSD, Postoperative Sleep Disorders; TEAS, Transcutaneous Electrical Acupoint Stimulation; ASA, American Society of Anesthesiologists; BMI, Body Mass Index; PSQI, Pittsburgh Sleep Quality Index; ICU, Intensive Care Unit; HR, Heart Rate; SpO2, Pulse Oxygen Saturation; BIS, Bispectral Index; VT, Tidal Volume; PETCO2, Pressure of end-tidal CO2; MAP, Mean Arterial Pressure; VAS, Visual Analog Scale; AIS, Athens Insomnia Scale; 5-HT, 5-hydroxytryptamine; S.P., Substance P; VIP, Vasoactive Intestinal Peptide; CT, Computed Tomography; CRF, Case Report Form; DMC, Data Monitoring Committee.
Data Sharing Statement
Patients’ personal information and all data collected are kept confidential and not available to the public until this trial is completed. After completion, they will be open to the public (including participants) by contacting the corresponding author via e-mail.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and followed the SPIRIT guidelines. The protocol, informed consent form, and other materials have been approved by the Ethics Committee of Beijing Friendship Hospital (Approval number: 2023-P2-107-01). All patients will be informed about the trial at the preoperative visit and will voluntarily sign the informed consent form. And they could withdraw at any time without affecting standard care.
All biospecimens were coded, stored at −80°C for a maximum of 5 years, and analyzed by an external certified laboratory. These procedures were approved by the ethics committee. Participants were informed during the consent process that the risks of TEAS are minimal, mainly limited to mild skin sensations, and that biospecimen collection (blood/stool) carries standard clinical risks (eg, venipuncture discomfort).
Acknowledgments
Many thanks to all the participants and investigators of the trial and the urology team for their cooperation. We would like to express our sincere gratitude here.
Author Contributions
Conceptualization: Han TD, Zhang L, Liu XM; Methodology (protocol design and revisions): Han TD, Zhang L, Liu XM, Fan YC; Investigation (trial conduct, patient recruitment, clinical anesthesia): Liu XM, Wu C, Hu R, Wang TT, Cao Y; Data curation (case report forms, database management): Liu XM, Fan YC, Liu GK; Formal analysis: Liu XM, Fan YC; Validation (data monitoring): Liu GK; Project administration/Supervision: Han TD, Zhang L; Resources: Han TD, Zhang L; Writing – original draft: Liu XM; Writing – review & editing: Liu XM, Fan YC, Wu C, Hu R, Wang TT, Cao Y, Liu GK, Zhang L, Han TD; Supervision: Han TD, Zhang L; Project administration: Zhang L, Liu XM; Funding acquisition: Zhang L.
All authors meet ICMJE authorship criteria; all authors made substantial contributions as detailed above, approved the final version of the paper, agree to be accountable for all aspects of the work, and agree on the journal to which this paper has been submitted.
Funding
This study was funded by the National Natural Science Foundation of China (NO. 81901125 to Zhang L), Capital Medical University Research Foundation (No. PYZ22065 to Zhang L) and Beijing Natural Science Foundation (NO. 7232103 to Liu GK).
Disclosure
There are no competing interests disclosed by the authors.
References
1. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. doi:10.1038/s41386-019-0439-z
2. Fadayomi AB, Ibala R, Bilotta F, Westover MB, Akeju O. A systematic review and meta-analysis examining the impact of sleep disturbance on postoperative delirium. Crit Care Med. 2018;46(12):e1204–e1212. doi:10.1097/CCM.0000000000003400
3. Fernandes NM, Nield LE, Popel N, et al. Symptoms of disturbed sleep predict major adverse cardiac events after percutaneous coronary intervention. Can J Cardiol. 2014;30(1):118–124. doi:10.1016/j.cjca.2013.07.009
4. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
5. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
6. Zhang M, Zhao N, He JH, Li JL. Effects of transcutaneous electrical acupoint stimulation on the postoperative sleep quality and inflammatory factors in frail elderly patients. Zhongguo Zhen Jiu. 2023;43(7):751–755. doi:10.13703/j.0255-2930.20220919-k0002
7. Luo M, Song B, Zhu J. Electroacupuncture: a new approach for improved postoperative sleep quality after general anesthesia. Nat Sci Sleep. 2020;12:583–592. doi:10.2147/NSS.S261043
8. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
9. Sen P, Molinero-Perez A, O’Riordan KJ, McCafferty CP, O’Halloran KD, Cryan JF. Microbiota and sleep: awakening the gut feeling. Trends Mol Med. 2021;27(10):935–945. doi:10.1016/j.molmed.2021.07.004
10. Thompson RS, Vargas F, Dorrestein PC, Chichlowski M, Berg BM, Fleshner M. Dietary prebiotics alter novel microbial dependent fecal metabolites that improve sleep. Sci Rep. 2020;10(1):3848. doi:10.1038/s41598-020-60679-y
11. Tahmasbi F, Sanaie S, Eslami S, Rahimi-Mamaghani A. Application of Transcutaneous Electrical Acupoint Stimulation (TEAS) for management of postoperative pain after gynecological surgeries: a meta-analysis. Pain Manag Nurs. 2025;26(1):111–124. doi:10.1016/j.pmn.2024.12.005
12. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
13. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. 2000;48(6):555–560. doi:10.1016/S0022-3999(00)00095-7
14. Paul PG, Mathew T, Shintre H, Bulusu S, Paul G, Mannur S. Postoperative pulmonary complications following laparoscopy. J Minim Invasive Gynecol. 2017;24(7):1096–1103. doi:10.1016/j.jmig.2017.06.029
15. Varallo G, Giusti EM, Manna C, et al. Sleep disturbances and sleep disorders as risk factors for chronic postsurgical pain: a systematic review and meta-analysis. Sleep Med Rev. 2022;63:101630. doi:10.1016/j.smrv.2022.101630
16. Wang Q, Yu C. Negative role of sleep disturbance in the recovery of gastrointestinal postoperative patients. Expert Rev Gastroenterol Hepatol. 2020;14(4):229–230. doi:10.1080/17474124.2020.1738925
17. Wang J, Lu FF, Ge MM, et al. Transcutaneous electrical acupoint stimulation improves postoperative sleep quality in patients undergoing laparoscopic gastrointestinal tumor surgery: a prospective, randomized controlled trial. Pain Ther. 2023;12(3):707–722. doi:10.1007/s40122-023-00493-2
18. Song B, Chang Y, Li Y, Zhu J. Effects of transcutaneous electrical acupoint stimulation on the postoperative sleep quality and pain of patients after video-assisted thoracoscopic surgery: a prospective, randomized controlled trial. Nat Sci Sleep. 2020;12:809–819. doi:10.2147/NSS.S270739
19. Zhang M, Zhang M, Kou G, Li Y. The relationship between gut microbiota and inflammatory response, learning and memory in mice by sleep deprivation. Front Cell Infect Microbiol. 2023;13:1159771. doi:10.3389/fcimb.2023.1159771
20. Smith RP, Easson C, Lyle SM, et al. Gut microbiome diversity is associated with sleep physiology in humans. PLoS One. 2019;14(10):e0222394. doi:10.1371/journal.pone.0222394
21. Wang Z, Wang Z, Lu T, et al. The microbiota-gut-brain axis in sleep disorders. Sleep Med Rev. 2022;65:101691. doi:10.1016/j.smrv.2022.101691
22. Jang JH, Yeom MJ, Ahn S, et al. Acupuncture inhibits neuroinflammation and gut microbial dysbiosis in a mouse model of Parkinson’s disease. Brain Behav Immun. 2020;89:641–655. doi:10.1016/j.bbi.2020.08.015
23. Zhang Q, Deng P, Chen S, et al. Electroacupuncture and human iPSC-derived small extracellular vesicles regulate the gut microbiota in ischemic stroke via the brain-gut axis. Front Immunol. 2023;14:1107559. doi:10.3389/fimmu.2023.1107559
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.