Back to Journals » Journal of Pain Research » Volume 15
Effect of Thoracic Paravertebral Nerve Block on Blood Coagulation in Patients After Thoracoscopic Lobectomy: A Prospective Randomized Controlled Clinical Trial
Authors Yuan B ![]() , Liu D, Zhu Z, Hao Y, He K, Deng S
, Liu D, Zhu Z, Hao Y, He K, Deng S
Received 22 December 2021
Accepted for publication 24 February 2022
Published 28 February 2022 Volume 2022:15 Pages 633—641
DOI https://doi.org/10.2147/JPR.S355227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Baohong Yuan, Danyan Liu, Zunyan Zhu, Yonggang Hao, Kaihua He, Shiyun Deng
Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Danyan Liu, Tel/Fax +86 23 8901 1069, Email [email protected]
Purpose: Ultrasound-guided thoracic paravertebral block (TPVB) has become increasingly popular for postoperative analgesia after thoracic surgery. We designed this prospective, randomized, double-blind, placebo-controlled trial to investigate the effect of TPVB on blood coagulation in patients after thoracoscopic lobectomy.
Patients and Methods: Sixty patients scheduled for thoracoscopic lobectomy were randomly allocated to two groups. Patients underwent ultrasound-guided TPVB with 0.33% ropivacaine (T group) or 0.9% saline (C group) at the end of the surgery under general anesthesia. Patient-controlled intravenous analgesia (PCIA) was administered for both group after the surgery. The primary outcome was the thromboelastogram (TEG) parameters before anesthesia (T0), at the end of operation (T1) and in 1 day (T2) and 2 days (T3) after the operation, the second outcomes were the analgesic effect and the amount of intraoperative opioid consumption, operation time, infusion volume, blood loss and urine volume.
Results: The visual analog scale (VAS) scores in group T were lower than group C (P < 0.05). In group T, compared with T0, the R value at T1 and T2 is significantly reduced, and the K value at T1 were significantly shortened, the α-angle and MA value at T1 were significantly increased (P < 0.05). In group C, compared with T0, the R value and K value were significantly shortened, the α-angle and MA value were significantly increased at all postoperative time points (P < 0.05). Compared with group C at the same time point, the R and K values of group T were significantly longer, and the α-angle and MA values were significantly reduced at T2 and T3 points, with statistically significant differences (P< 0.05).
Conclusion: TPVB is beneficial to improve postoperative hypercoagulability and promote postoperative rehabilitation of patients after thoracoscopic lobectomy.
Keywords: paravertebral nerve block, thoracoscopic lobectomy, thrombelastogram, blood coagulation
Introduction
Lung cancer has a high incidence of morbidity and mortality, and accounts for a large proportion of thoracic surgeries, which is the most effective treatment for early and middle stage of lung cancer.1 Studies have confirmed that lung cancer is a high-risk factor for venous thromboembolism (VTE),2 especially the incidence of the postoperative VTE is as high as 13.2%-19.5%, which is an important risk factor for common postoperative complications and unexpected death in hospitals.3–5 In addition, surgical resection may carry increased risk of VTE. The intense trauma, stress response and postoperative pain in patients undergoing thoracic surgery will aggravate the hypercoagulability of patients and lead to the occurrence of VTE.6 Perfect postoperative analgesia can help to improve postoperative hypercoagulability of gastric cancer by inhibiting platelet hyperactivation,7 and help patients carry out early postoperative rehabilitation training, which is helpful to reduce the risk of VTE. Thoracic epidural analgesia (TEA) has long been regarded as the mainstay of multimodal analgesia for thoracic surgeries. Numerous studies have shown that epidural anesthesia and analgesia can relieve the coagulation status of patients and reduce postoperative thromboembolic complications.8–10
Due to several contraindications and side effects, a series of potential alternative modalities to TEA (thoracic paravertebral nerve block, intercostal nerve blocks) has been proposed, especially for patients undergoing minimally invasive surgery. Ultrasound-guided thoracic paravertebral nerve block, as the most commonly used multimodal postoperative analgesia in thoracic surgery, has a definite blocking effect and fewer complications.11
At present, almost no studies have investigated the impact of TPVB on postoperative coagulation function in patients with thoracoscopic lobectomy.
In this study, patients who underwent thoracoscopic lobectomy were enrolled. The dynamic monitoring of TEG at different times were selected to evaluate the effect of TPVB on postoperative coagulation function of patients, so as to evaluate TPVB more comprehensively and provide a basis for the selection of postoperative pain treatment. It was hypothesized that postoperative hypercoagulability could be reduced by TPVB.
Materials and Methods
Study Design and Setting
This study is a single center, prospective, randomized, controlled, double-blind study. The protocol was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (Ethics approval number: 20195801) and registered at chictr.org.cn (ChiCTR2100041783). Written informed consent was obtained from all participants. All of the procedures were performed in accordance with the Declaration of Helsinki.
A total of 63 patients, who underwent elective operations of unilateral thoracoscopic lobectomy with three trocar ports for lung cancer at the first Affiliated Hospital of Chongqing Medical University from January 2021 to June 2021, were recruited for the study. Inclusion criteria were as follows: aged 18–65 years, BMI 18–25 kg/m2, American Society of Anesthesiologists (ASA) grade I–II. The exclusion criteria were a history of mental illness, cognitive impairment, spinal or thoracic deformity, infection at the puncture site, chronic pain or regular administration of analgesic drugs, preoperative use of drugs that affect coagulation function, a known allergy to local anesthetics, or with significant heart, lung, liver, kidney and endocrine or blood disorders, loss of core data during follow-up, withdrawal from the study for any reason. Enrolled patients were randomized to receive ultrasound-guided TPVB with 0.33% ropivacaine (T group) or 0.9% saline (C group). The randomization was performed in a 1:1 ratio according to a computer-generated table by an investigator not involved in patient care or perioperative assessment. Group assignments were enclosed in sealed, opaque envelopes opened, which were given to an anesthesia nurse not involved with the study. The nurse prepared identical syringes containing study injectate (0.33% ropivacaine or 0.9% saline). The patients, attending anesthesiologists, surgeons, and data collectors were blinded to group assignments throughout the entire study period.
Preoperative Preparations and Anesthesia Protocol
Upon arrival in the operating room, patients were monitored with electrocardiography, pulse oximetry, body temperature, invasive blood pressure and the Narcotrend Index. Patients were randomly allocated using sealed envelopes with computer-generated numbers.
After checking the patient by surgeon, anesthesiologist, and nurse, general anesthesia was induced with 2 mg/kg propofol, 0.5 µg/kg sufentanil, and 1 mg/kg vecuronium. Patients were intubated with double-lumen tracheal tube, with the optimal position for one-lung ventilation confirmed by bronchoscopy. General anesthesia was maintained with intravenous infusion of remifentanil 0.08–0.15 µg/kg/min, propofol (2–4 mg/kg/h) and sevoflurane (1–2%) to maintain Narcotrend Values between 40 and 60, intermittent intravenous infusion of vecuronium (0.4 mg/kg) was added per 40–60 min. Mechanical ventilation was maintained at 8 mL/kg tidal volume during two lung ventilations or 6 mL/kg tidal volume and 5 cm H2O positive end expiratory pressure (PEEP) during one lung ventilation. The respiratory rate was adjusted to keep end tidal carbon dioxide pressure between 37 and 45 mmHg. The fluctuation ranges of the HR and MAP were maintained at no more than 20% of the baseline values. Hypotension (>20% decrease from baseline blood pressure lasting more than 3 minute) was treated with 250 m L 6% hydroxyethyl starch 130/0.4 infusion over 15 minutes. If the hypotension was not corrected, intravenous ephedrine (6 mg) or phenylephrine (50 µg) was used. Bradycardia (HR <40/min) was treated with atropine 0.5 mg.
Application of TPVB
After closing the incision for anastomosis, anesthesia was discontinued, TPVB was performed in lateral position by experienced anesthetists who were blinded to the study protocol.
According to the location of the surgical incision, the two-point method (T4–5 and T6–7) was selected. After an initial anatomic scan by ultrasonography to confirm the thoracic levels, appearance, and depth of structures, the procedural site was identified. The parathoracic long-axis out-plane technique for puncture was performed. After the correct location was confirmed by hydrodissection and the pleura moving downwards with 2 mL of physiological saline solution, and 15mL of 0.33% ropivacaine or 0.9% saline was injected at each point (Figure 1).
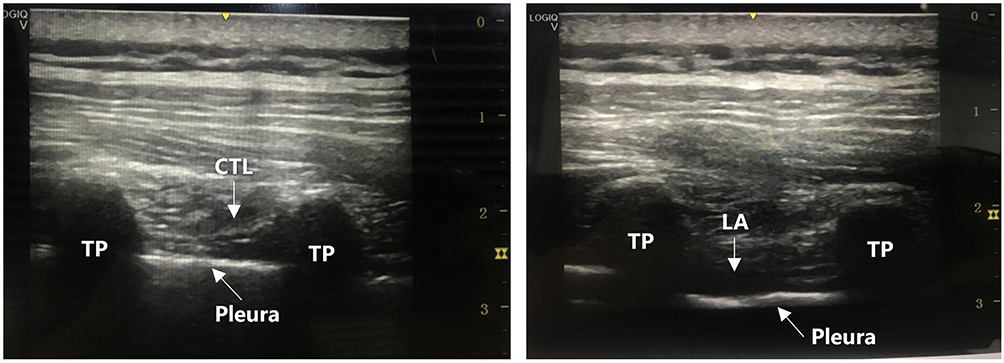 |
Figure 1 Ultrasound-guided paravertebral nerve block. Abbreviations: TP, the transverse process; CTL, costotransverse ligament; LA, spread of the local anesthetic. |
PCIA was administered for both group at the end of the surgery. A total of 800 mg tramadol and 100 mg flurbiprofen were mixed with 54 mL normal saline in each PCIA device, started by a basal continuous intravenous infusion (1 mL/hour) plus patient controlled additional intravenous bolus (2 mL, lockout time, 15 minutes). On the day before surgery, patients received instruction on how to use the PCA device. PCIA was used for 2 days after surgery.
All patients were replaced with 7.5# single endotracheal tube and then transferred to the thoracic surgical care unit. The blinding principle was well controlled in the present study.
Measurements
The primary outcome was the TEG parameters at the end of operation (T1) and in 1 day (T2) and 2 days (T3) after the operation. The second outcomes were changes of analgesic effect after the surgery, PCA press times, the amount of intraoperative opioid consumption, operation time, infusion volume, blood loss and urine volume.
Arterial blood was collected at T0, T1, T2 and T3. The thrombus tracer Haemoscope (TEG 5000, Haemoscope Corporation, Niles, Illinois, USA) is used to detect the TEG, including determination of the blood coagulation reaction time (R), the blood clots forming time (K), the blood clots form rate (alpha), and the maximum amplitude of blood clots (MA). Postoperative pain level was assessed by VAS (with 0 representing no pain and 10 representing the worst pain imaginable) at 6h,12h,24h and 48 h after surgery at rest and when coughing. Times of analgesia pump pressure and other incidence of postoperative complications were recorded.
Sample Size Calculation
The sample size was calculated with “Power and SampleSize.com,” an online power and sample size calculator. Based on the findings from our pilot study, a sample size of 24 patients per group was estimated with a power of 80% and a two-sided P-value of 0.05 to detect a 20% decrease in the level of MA value 48 h after surgery. Considering patients who may withdraw from the study, 30 patients were enrolled in each group.
Statistical Analysis
All statistical analyses were performed using IBM SPSS for Windows version 19.0 (IBM Corp., Armonk, NY, USA) software. Continuous data were expressed as the mean ± SD or median (range). Repeated-measures ANOVA was used for the analysis of repeatedly measured data, the independent sample t-test was used for inter-group comparison, Mann–Whitney U-test was used for comparison of non-parametric data, and χ2 test was used for counting data. P < 0.05 was considered statistically significant.
Results
Characteristics of the Patients
A total of 63 patients were recruited for this study, 3 patients were excluded due to patient refusal, and 60 patients were enrolled and randomly allocated into two groups. Another 3 patients were withdrawn from the study (due to conversion to open thoracotomy). Finally, 57 patients completed the study and were included in the final statistical analysis (Figure 2). Demographic and intraoperative variables were similar between the two groups (Table 1). During the surgery, there was no significant difference in the amount of opioid consumption, infusion volume, blood loss and urine volume during the operation between the two groups (Table 1).
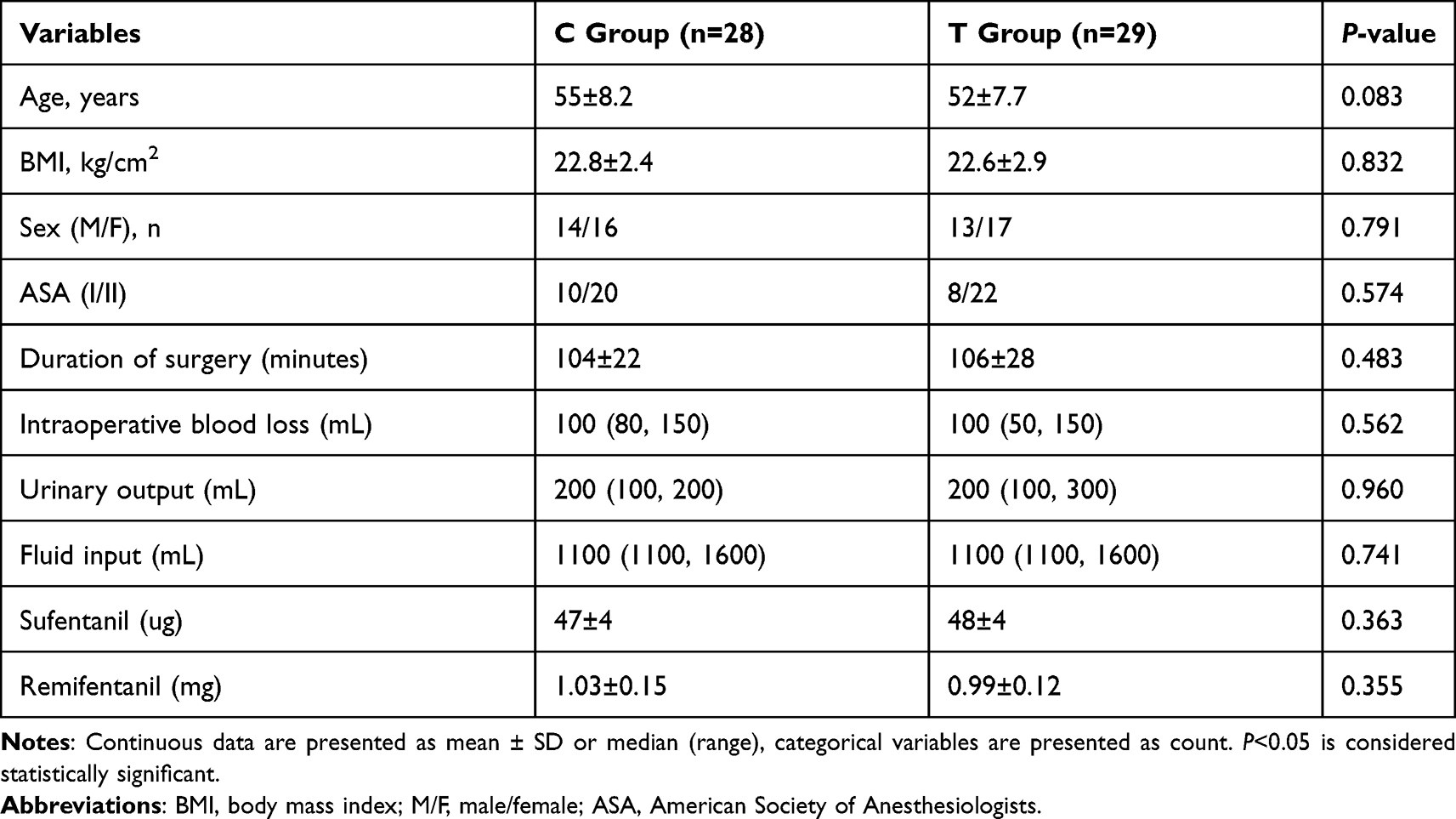 |
Table 1 Demographic Data and Intraoperative Variables |
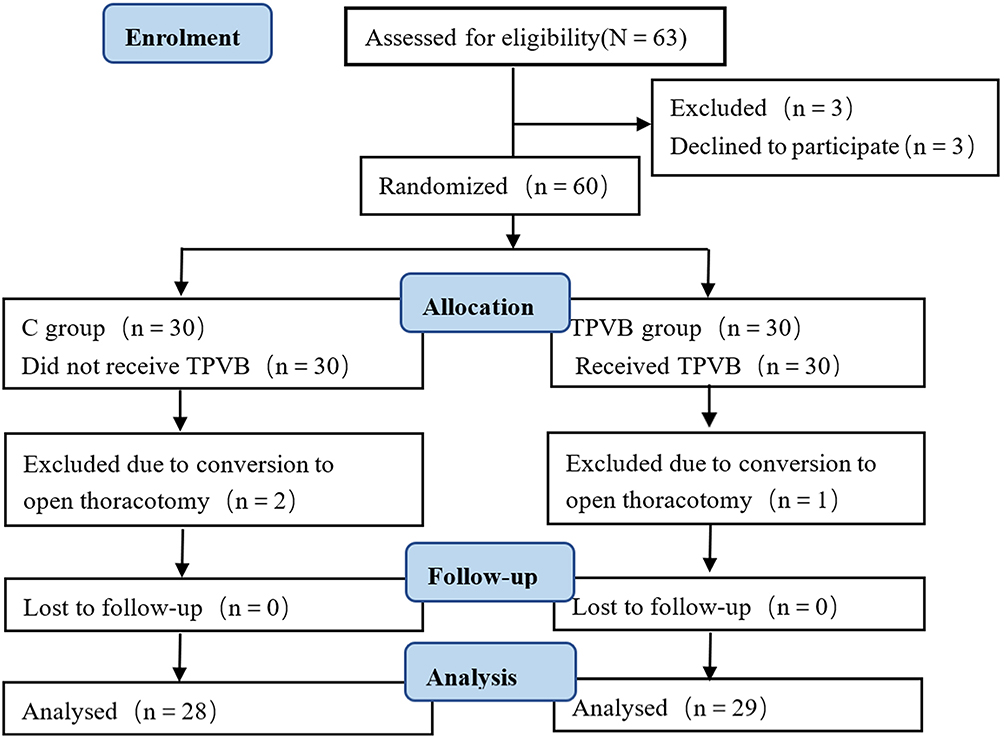 |
Figure 2 Diagram of the progress through the phases of the trial. Abbreviation: TPVB, thoracic paravertebral block. |
Postoperative Analgesia Effect
The visual analogue pain scores both at rest and on coughing were lower in the TPVB group at all postoperative time points (P < 0.05). The times of patient-controlled pressing in group C were higher (Table 2).
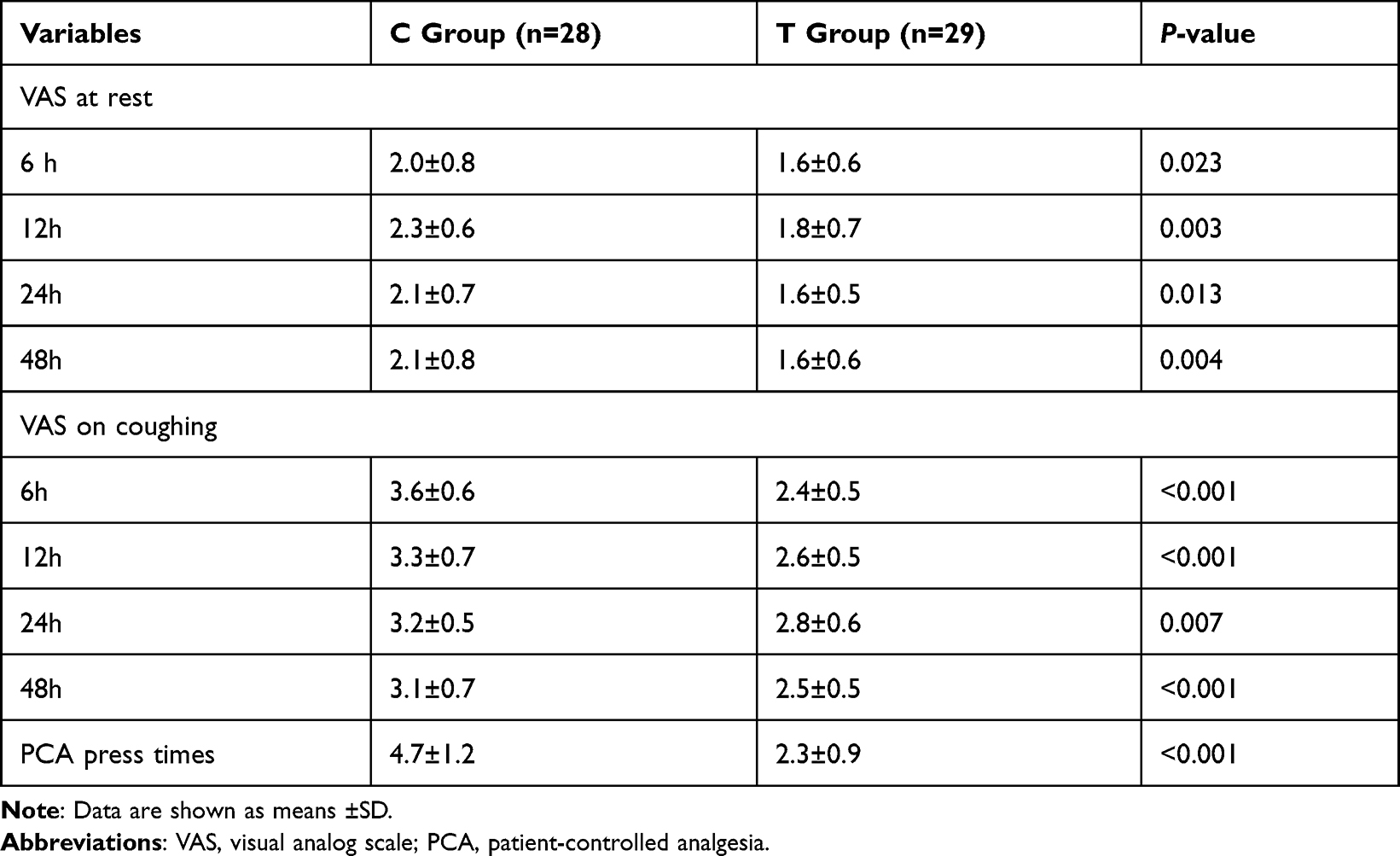 |
Table 2 The Analgesic Effect of Patients After Surgery |
Changes of TEG Parameters at Each Time Points After Operation
In group T, compared with the T0 time point, the R value at T1 and T2 is significantly reduced, and the K value at T1 were significantly shortened, the α-angle and MA value at T1 were significantly increased (P < 0.05).
In group C, compared with T0, the R value and K value were significantly shortened, the α-angle and MA value were significantly increased at all postoperative time points (P < 0.05). Compared with the C group at the same time point, the R and K values of the TPVB group were significantly longer, and the α-angle and MA values were significantly reduced at T2 and T3 points, with statistically significant differences (P<0.05) (Table 3).
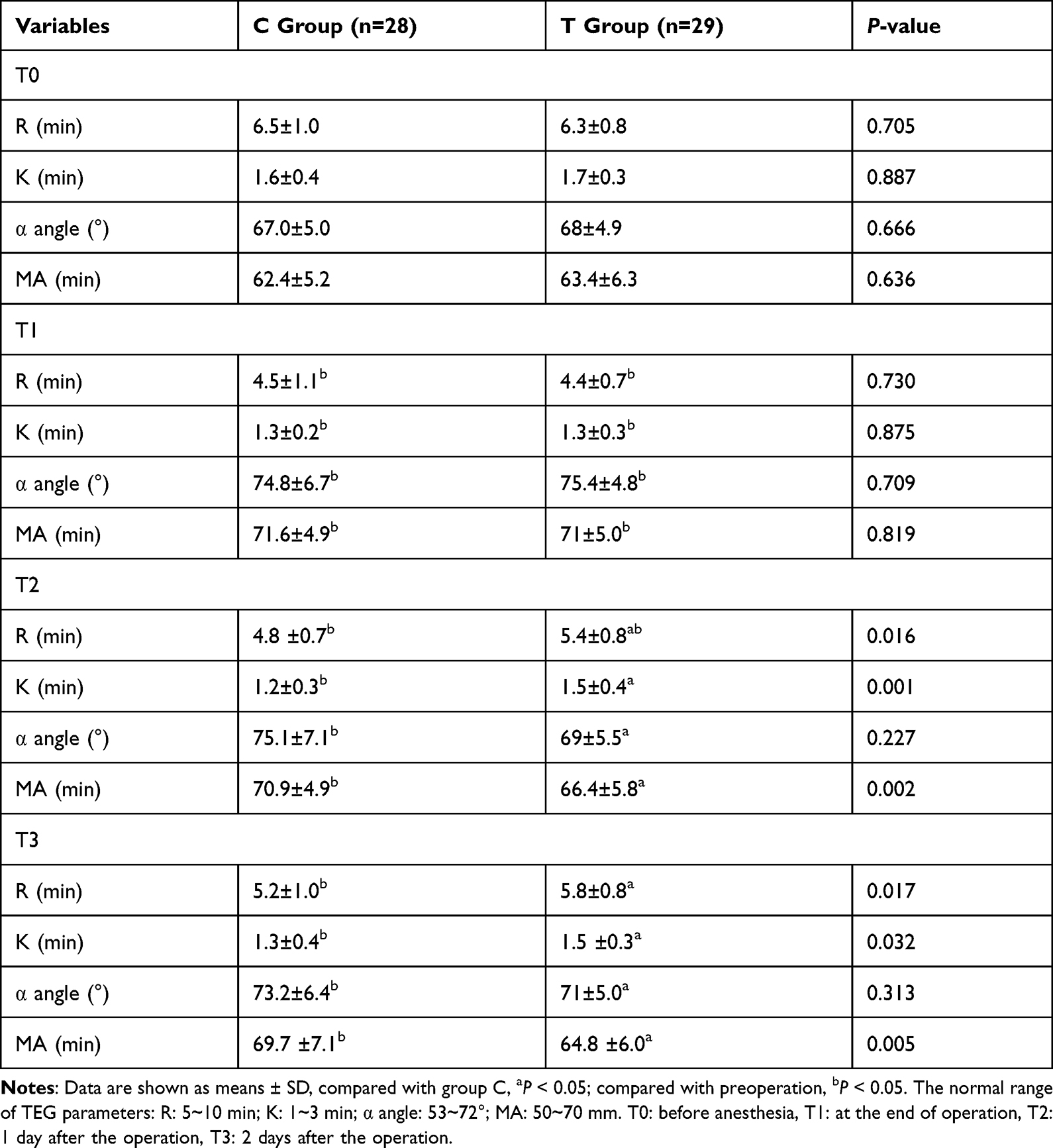 |
Table 3 Variation of TEG Parameters at Different Time Points |
Discussion
VTE consists of deep venous thrombosis (DVT) and pulmonary embolism (PE), and the latter can be serious because of its lethality or the resultant neurologic deficits, and remain prevalent causes of morbidity and mortality.
Thromboembolism is a well-recognized complication of malignant disease; cancer growth is associated with the development of a hypercoagulable state. Malignant cells can activate blood coagulation in several ways: by producing procoagulant, fibrinolytic, and proaggregating activities; by releasing proinflammatory and proangiogenic cytokines; and by interacting directly with host vascular and blood cells, such as endothelial cells, leucocytes, and platelets, by means of adhesion molecules.2
Intuitively, patients undergoing cancer surgery remain at a high risk for VTE as they meet criteria for Virchow’s triad of hypercoagulability, stasis, and endothelial injury. Furthermore, previous studies have shown that the patients with lung cancer undergoing operative treatment is believed to carry a fourfold increased risk of VTE and thromboembolic complications.12,13
Thoracic surgery is widely performed worldwide and has the characteristics of a high incidence of pain, severe stress response, increased inflammation. In recent years, thoracoscopic lobectomy has become increasingly popular as a minimally invasive procedure resulting in lower levels of pain, fewer pulmonary complications, less blood loss, shorter hospital stays. In this surgical approach the pain directly from the surgical incision is greatly reduced, whereas the visceral pain and the thoracic drainage catheters all add to the range of dermatomes for which analgesia needs to be considered. Severe pain caused by nerve damage and postoperative chest drainage tube can produce a stress response, which can induce platelet activation and aggregation, adhesion, increase the amount of VIII factor, prothrombin and fibrinogen, boost the agglutinative and decrease fibrinolytic function at the same time, make the body in a state of high coagulation.6,14 In addition, drainage tube stimulate diaphragm wall or pleura produces pain, making patients reluctant to cough and breathe deeply, and prone to complications such as atelectasis and pulmonary infection. Prolongation of postoperative bed rest slows the blood flow of lower limbs, which further increases the risk of VTE.15 Early bedside activities after surgery are helpful for rapid recovery and can provide the basic conditions for postoperative recovery.
It has been found that perfect postoperative analgesia can help to improve postoperative hypercoagulability by inhibiting platelet hyperactivation.16,17 Ultrasound-guided thoracic paravertebral nerve block refers to the injection of local anesthesia into the thoracic paravertebral space guided by ultrasound technology to block the dorsal branch, abdominal branch, communicating branch and sympathetic trunk of the intercostal nerve in the space, so as to achieve the purpose of ipsilateral body and sympathetic nerve block. The paravertebral nerve bundle is sensitive to local anesthetics due to the lack of the sheath and fascia. Unilateral TPVB can avoid contralateral sympathetic nerve block, reduce hypotension and maintain circulatory stability.18 Furthermore, the development of TPVB techniques using ultrasound has made it easier and more accessible. Its exact analgesic effect is comparable to an epidural block, therefore it is highly recommended in the latest enhanced recovery programs for patients undergoing thoracoscopic surgery.19
Our results demonstrated that the postoperative VAS scores of TPVB group were better than that of the control group, consistent with numerous previous studies that TPVB can reduce postoperative acute pain.
Studies have found that TPVB can inhibit stress response, reduce inflammatory stimulation, improve postoperative lung function, reduce postoperative pulmonary complications, improve patient outcomes, and even can be used for the treatment of chronic pain syndrome after chest surgery.20 Yet our analysis demonstrates that, to a certain extent, TPVB can improve the postoperative coagulation status of patients.
Traditional coagulation function tests such as prothrombin time (PT), fibrinogen (FIB), and partial thromboplastin time (APTT), simply reflect coagulation function, with a long feedback time and insensitivity to the function of fibrinogen, hyper fibrinolysis and platelet dysfunction. Whereas thromboelastography (TEG), which mimics the entire dynamic of coagulation and fibrinogenesis in vivo with a small amount of field blood over a short period of time, comprehensive monitoring of coagulation factor activity, platelet function, plasma coagulation factor activity, fibrinogen function and other general features of coagulation process.21,22 The test results are closer to the occurrence and development of coagulation reaction in vivo, and can reflect the coagulation function status in vivo more comprehensively. Compared with traditional coagulation tests, TEG can better reflect postoperative hypercoagulability,23 and timely predict the occurrence of thromboembolic complications.24,25 Bedside, TEG test in our study can produce fast responsiveness and calculable improvement of coagulation status in patients.
Therefore, TEG was used in this study to monitor the effect of thoracic paravertebral nerve block after thoracoscopic lobectomy on coagulation function. It was found that TPVB could not only relieve the pain of patients, but also inhibit the enhancement of coagulation function caused by surgical stress, and improve the post-operative hypercoagulability.
We found that blood coagulation function of the two groups were significantly enhanced at the end of the operation, the control group are at higher levels at all time points after the surgery. However, blood coagulation status of TPVB group was consistent with preoperative level in 24 h and 48 h after surgery. These results indicated that the vertebral nerve block analgesia can restrain the enhanced coagulation function caused by stress reaction and postoperative pain from the thoracoscope surgery, hence, it can effectively prevent early perioperative high coagulation state and reduce the incidence of TVE. Based on the conclusions, early rehabilitation after thoracoscopic surgery can be enhanced by TPVB.
Analysis of the reasons might be: TPVB associated with PCIA can provide perfect analgesic effect, reduce the catecholamine release and the stress reaction, decrease activated clotting factors and platelet activity, and inhibit platelet aggregation. At the same time, because of the block of the sympathetic nerve, it will cause the dilation of the blood vessels in the nerve block area, a relative increase in blood volume and a decreased blood viscous degrees to prevent the further occurrence of blood hypercoagulability, thus improving the tendency of hypercoagulability. In addition, it may be related to the inhibition of platelet aggregation by local anesthetics.26
Patient controlled analgesia (PCIA) can meet the basic analgesic needs of patients in the resting state, but there will be obvious pain when breathing deeply, coughing, and turning over. However, TPVB can prevent the transmission of regional stimulation to the center nervous system through the spinal cord level, and can improve the analgesia combined with PCIA. Perfect postoperative analgesia makes patients more comfortable, and it is beneficial for patients to get out of bed early and to do rehabilitation training, which helps to reduce the risk of DVT and PTE, and achieve the purpose of rapid recovery.
There are several limitations in this study: limited by experimental conditions, the sample size is relatively small, leading to the increase of systematic error; continuous thoracic paravertebral block has been used in some studies, and it is believed to provide more perfect postoperative analgesia, and may be able to produce a more persuasive result, but its wide use is limited to some extent by the difficulty of catheter placement and easy displacement.27 The exact mechanism of action of TPVB on patients’ blood coagulation system still needs to be further explored.
Conclusion
To sum up, TPVB can effectively alleviate pain after thoracoscope surgery, and to a certain extent, prevent postoperative hypercoagulability in patients at an early stage after the surgery. The changes of coagulation function should be closely monitored during perioperative period, and the complications of blood embolism should be actively prevented to achieve rapid postoperative recovery of lung cancer patients.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Danyan Liu) on reasonable request.
Acknowledgments
This work was supported by awards from National Clinical Key Specialty Construction Project of Ministry of Health [Ministry of Finance (2011) No. 170]; Medical Key Discipline Construction Project of Chongqing Province [Chongqing Health Science and Education (2007) No. 2].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China. Chin J Cancer Res. 2018;30:1–12. doi:10.21147/j.issn.1000-9604.2018.01.01
2. Prandoni P, Falanga A, Piccioli A. Cancer and venous thromboembolism. Lancet Oncol. 2005;6:401–410. doi:10.1016/S1470-2045(05)70207-2
3. Shinagare AB, Okajima Y, Oxnard GR, et al. Unsuspected pulmonary embolism in lung cancer patients: comparison of clinical characteristics and outcome with suspected pulmonary embolism. Lung Cancer. 2012;78:161–166. doi:10.1016/j.lungcan.2012.08.007
4. Dentali F, Malato A, Ageno W, et al. Incidence of venous thromboembolism in patients undergoing thoracotomy for lung cancer. J Thorac Cardiovasc Surg. 2008;135:705–706. doi:10.1016/j.jtcvs.2007.10.036
5. Falanga A. The incidence and risk of venous thromboembolism associated with cancer and nonsurgical cancer treatment. Cancer Invest. 2009;27:105–115. doi:10.1080/07357900802563028
6. Van Haren RM, Valle EJ, Thorson CM, et al. Long-term coagulation changes after resection of thoracoabdominal malignancies. J Am Coll Surg. 2014;218:846–854. doi:10.1016/j.jamcollsurg.2013.12.039
7. Osada J, Rusak M, Kamocki Z, et al. Platelet activation in patients with advanced gastric cancer. Neoplasma. 2010;57:145–150. doi:10.4149/neo_2010_02_145
8. Liu D, Sun C, Zhang X, et al. Influence of epidural anesthesia and general anesthesia on thromboembolism in patients undergoing total knee arthroplasty. Am J Transl Res. 2021;13:10933–10941.
9. Tuman KJ, McCarthy RJ, March RJ, et al. Effects of epidural anesthesia and analgesia on coagulation and outcome after major vascular surgery. Anesth Analg. 1991;12:696–704.
10. Wu Z, Zhu Y, Tan S. Comparison of the effects of epidural anesthesia and general anesthesia on perioperative cognitive function and deep vein thrombosis in patients undergoing total knee arthroplasty. Evid Based Complement Alternat Med. 2021;2021:1565067. doi:10.1155/2021/1565067
11. Pintaric TS, Potocnik I, Hadzic A, et al. Comparison of continuous thoracic epidural with paravertebral block on perioperative analgesia and hemodynamic stability in patients having open lung surgery. Reg Anesth Pain Med. 2017;36:256–260. doi:10.1097/AAP.0b013e3182176f42
12. Afshari A, Ageno W, Ahmed A, et al. European guidelines on perioperative venous thromboembolism prophylaxis: executive summary. Eur J Anaesthesiol. 2018;35:77–83. doi:10.1097/EJA.0000000000000729
13. De Martino RR, Goodney PP, Spangler EL, et al. Variation in thromboembolic complications among patients undergoing commonly performed cancer operations. J Vasc Surg. 2012;55:1335. doi:10.1016/j.jvs.2011.10.129
14. Kelly DJ, Ahmad M, Brull SJ. Preemptive analgesia I: physiological pathways and pharmacological modalities. Can J Anaesth. 2001;48:1000–1010. doi:10.1007/BF03016591
15. Freedman KB, Brookenthal KR, Fitzgerald RH, et al. A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am. 2000;82:929–938. doi:10.2106/00004623-200007000-00004
16. Capdevila X, Ponrouch M, Choquet O. Continuous peripheral nerve blocks in clinical practice. Curr Opin Anaesthesiol. 2008;21:619–623. doi:10.1097/ACO.0b013e32830c66c2
17. Trueblood A, Manning DW. Analgesia following total knee arthroplasty. Curr Opin Orthop. 2007;18:76–80. doi:10.1097/BCO.0b013e3280119635
18. Karmakar MK. Thoracic paravertebral block. Anesthesiology. 2001;95:771–780. doi:10.1097/00000542-200109000-00033
19. Komatsu T, Sowa T, Takahashi K, et al. Paravertebral block as a promising analgesic modality for managing post thoracotomy pain. Ann Thorac Cardiovasc Surg. 2014;20:113–116. doi:10.5761/atcs.oa.12.01999
20. Richardson J, Lönnqvist PA, Naja Z. Bilateral thoracic paravertebral block: potential and practice. Br J Anaesth. 2011;106:164–171. doi:10.1093/bja/aeq378
21. Konig G, Yazer MH, Waters JH. The effect of salvaged blood on coagulation function as measured by thromboclastography. Transfusion. 2013;53:1235–1239. doi:10.1111/j.1537-2995.2012.03884.x
22. Hepner DL, Concepcion M, Bhavani-Shankar K. Coagulation status using thromboelastography in patients receiving warfarin prophylaxis and epidural analgesia. J Clin Anesth. 2002;14:405–410. doi:10.1016/S0952-8180(02)00373-2
23. Ågren A, Wikman AT, Holmström M, et al. Thromboelastography (TEG®) compared to conventional coagulation tests in surgical patients – a laboratory evaluation. Scand J Clin Lab Invest. 2013;73:214–220. doi:10.3109/00365513.2013.765960
24. Dai Y, Lee A, Critchley LA, et al. Does thromboelastography predict postoperative thromboembolic events? A systematic review of the literature. Anesth Analg. 2009;108:734–742. doi:10.1213/ane.0b013e31818f8907
25. Kashuk JL, Moore EE, Sabel A, et al. Rapid thrombelastography (r-TEG) identifies hypercoagulability and predicts thromboembolic events in surgical patients. Surgery. 2009;146:764–772. doi:10.1016/j.surg.2009.06.054
26. Kohrs R, Hoenemann CW, Feirer N, et al. Bupivacaine inhibits whole blood coagulation in vitro. Reg Anesth Pain Med. 1999;24:326–330. doi:10.1016/s1098-7339(99)90106-2
27. D’Ercole F, Arora H, Kumar PA. Paravertebral block for thoracic surgery. J Cardiothorac Vasc Anesth. 2018;32:915–927. doi:10.1053/j.jvca.2017.10.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.