Back to Journals » Journal of Pain Research » Volume 15
Effect of Sufentanil Combined with Gabapentin on Acute Postoperative Pain in Patients Undergoing Intraspinal Tumor Resection: Study Protocol for a Randomized Controlled Trial
Authors Zhang Y, Yue H, Qin Y ![]() , Wang J, Zhao C, Cheng M
, Wang J, Zhao C, Cheng M ![]() , Han B, Han R
, Han B, Han R ![]() , Cui W
, Cui W ![]()
Received 20 May 2022
Accepted for publication 22 August 2022
Published 1 September 2022 Volume 2022:15 Pages 2619—2628
DOI https://doi.org/10.2147/JPR.S374898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Yuan Zhang,1,* Hongli Yue,1,* Yirui Qin,1 Jiajing Wang,1 Chenyang Zhao,1 Miao Cheng,1 Bo Han,2 Ruquan Han,1 Weihua Cui1,*
1Department of Anesthesiology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Neurosurgery, Beijing Tian Tan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruquan Han; Weihua Cui, Department of Anesthesiology, Beijing Tian Tan Hospital, Capital Medical University, No. 119, Nan Si Huan Xi Lu, Fengtai District, Beijing, 100070, People’s Republic of China, Tel +8613701285393 ; Tel +8613701285393, Fax +861059976658, Email [email protected]; [email protected]
Purpose: Patients undergoing intraspinal tumor resection usually experience severe postoperative pain. Inadequate postoperative analgesia usually leads to severe postsurgical pain, which could cause patients to suffer from many other related complications. Recently, an increasing number of studies have found that gabapentin can relieve hyperalgesia, postoperative pain, and postoperative inflammation. However, there have been no reports on the use of gabapentin combined with sufentanil preoperatively for acute pain following intraspinal tumor resection.
Study Design and Methods: This is a protocol for a randomized, placebo-controlled, and double-blinded trial. One-hundred and sixty-eight participants with chronic pain related to the intraspinal tumor will be randomized into the gabapentin and placebo groups in a 1:1 ratio. In the gabapentin group, patients will be given 300 mg gabapentin orally 36 h, 24 h, and 12 h before surgery; the placebo group will receive a placebo orally at the same time points preoperatively. To estimate the efficacy and safety endpoints, all the researchers and patients will be blinded until the completion of this study. The primary outcome will be the consumption of sufentanil within 48 h postoperatively. The secondary outcomes include the visual analog scale pain score and Von Frey mechanical pain threshold 36 h and 24 h before and 24 h and 48 h after surgery, the incidence of postoperative nausea, vomiting, and drowsiness, the length of hospital stay and medical expenses.
Discussion: This trial is to evaluate the efficacy and safety of gabapentin combined with sufentanil for postoperative analgesia in patients who complain of pain before intraspinal tumor resection. The findings will provide a new strategy for multimode perioperative analgesia management in these patients.
Keywords: gabapentin, intraspinal tumor resection, multimode perioperative analgesia, opiates
Background
Patients undergoing intraspinal tumor resection usually experience severe and long-lasting pain, which causes the dysfunctions of various systems, such as the cardiovascular, respiratory, digestive, endocrine, and immune systems, to varying degrees, leading to postoperative complications and thus affecting the prognosis.1–5 Postoperative pain in patients with intraspinal tumors is not only caused by tissue injury but also associated with neuropathic pain and inflammatory pain. Peripheral and central sensitization both contribute to pain.6–9 It is difficult to achieve satisfactory analgesia by using a single drug. Therefore, identifying ways to relieve the postoperative pain of patients who have undergone intraspinal tumor resection, especially those with intramedullary tumors and preoperative chronic pain, is an urgent clinical problem.
In recent years, multimodal analgesia for postoperative pain management promotes patient recovery, shortens the length of hospital stay, and reduces costs.10–14 Studies have shown that perioperative multimodal analgesia with gabapentin can play a critical role in accelerating the recovery of patients.10,15,16 Gabapentin is an antiepileptic drug with anti-paralgesia and antihyperalgesia properties and has little effect on normal nociceptive stimulation. In recent years, studies have found that oral gabapentin administration before hysterectomy,17 breast cancer resection,18–20 cholecystectomy,21,22 prostatectomy,23 and spinal surgery24–26 can significantly reduce postoperative opioid consumption, which in turn is positively correlated with the dose of preoperative gabapentin. However, the same results were not found in patients undergoing cesarean section,27,28 or thoracotomy.29–31 Therefore, the analgesic effect of the preoperative administration of gabapentin may vary with the type of operation. A review found that the analgesic effect with perioperative use of gabapentin is only for those surgical models associated with acute hyperalgesia mechanisms.32 To date, there have been no reports on the use of preoperative gabapentin for intraspinal tumor resection, which may involve the mechanism of hyperalgesia due to the large dose of intraoperative remifentanil and the neuropathic pain associated with the intraspinal tumor.1,9
Study Design and Methods
We hypothesized that oral gabapentin administration before intraspinal tumor resection could alleviate existing preoperative neuropathic pain, acute pain caused by nerve stimulation, tissue damage, and remifentanil-induced hyperalgesia, reduce the incidence of opioid-related side effects, and hasten patient recovery.
This study is a single-center, randomized, placebo-controlled, double-blinded trial designed to evaluate the efficacy and safety of gabapentin combined with sufentanil for perioperative analgesia in patients undergoing intraspinal tumor resection. All patients who complain of chronic pain related to the tumor will be enrolled consecutively at Beijing Tiantan Hospital, Capital Medical University, China. The flow chart for this study is shown in Figure 1, and the trial schedule is presented in Table 1. Patients will be screened, recruited, and followed up. All researchers will be trained using the same protocol.
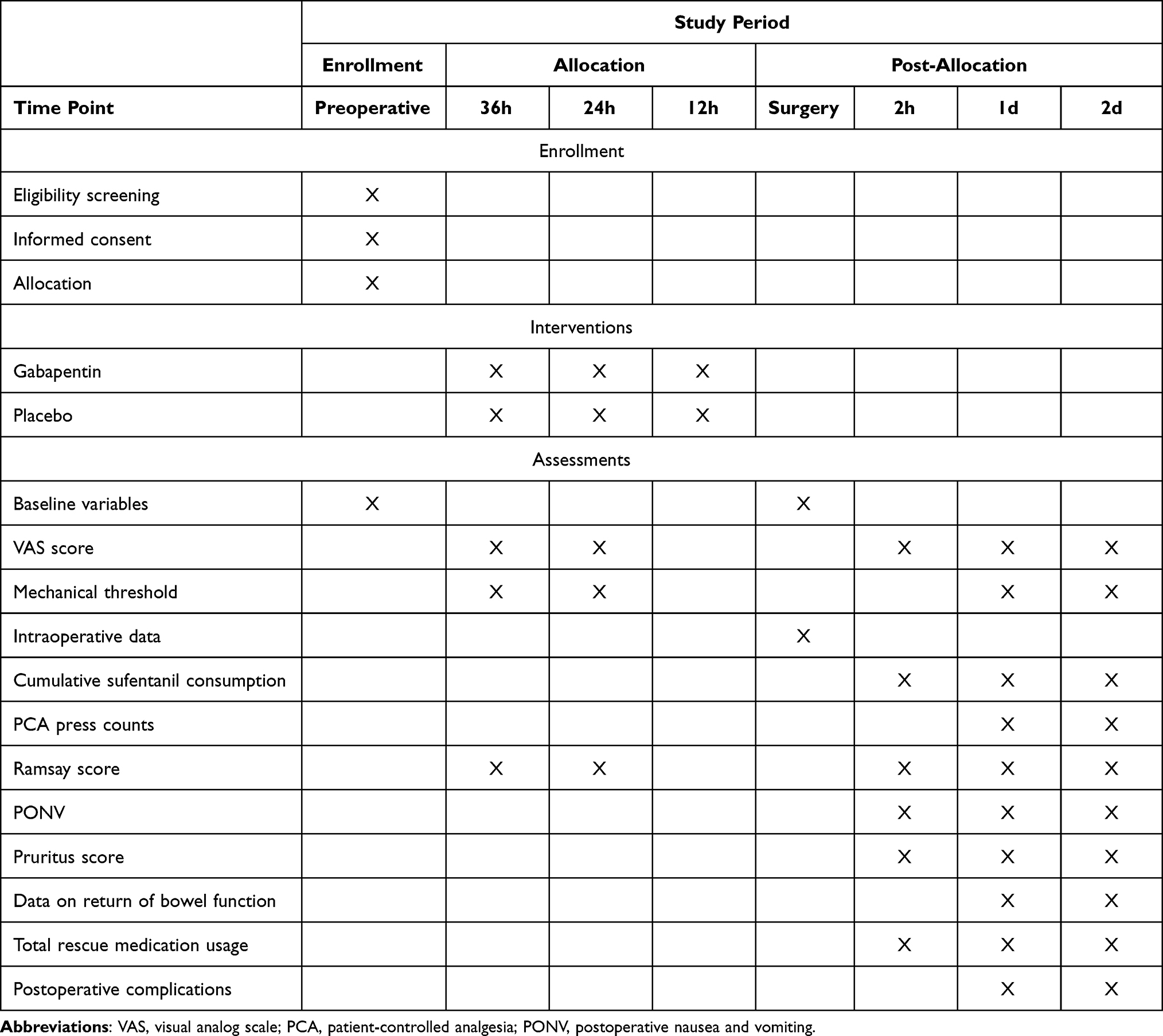 |
Table 1 Trial Schedule |
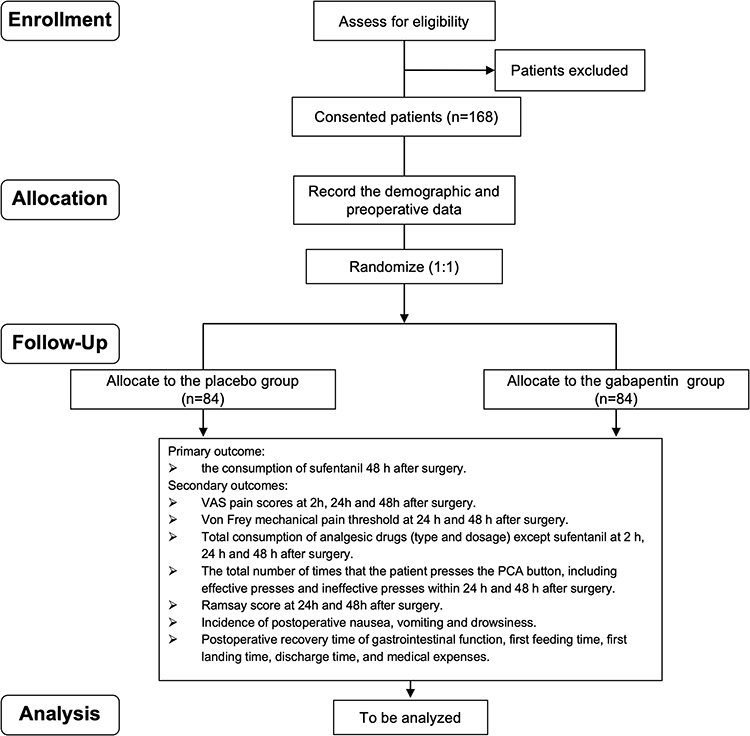 |
Figure 1 Flowchart of the study procedure. Abbreviations: VAS, visual analog scale; PCA, patient-controlled analgesia. |
Approval of the Study Protocol
All procedures in the trial will be conducted in accordance with the World Medical Association’s “Helsinki Declaration (version 19 October 2013)”. The study plan (protocol version 2.0) was approved by the Ethics Committee of Beijing Tiantan Hospital, Capital Medical University, China (KY2020-141-02). This study protocol has been registered at chictr.org.cn (ChiCTR2100046055).
Informed Consent
All participants in this trial will sign informed consent forms. Moreover, all participants will be given sufficient time to decide whether to participate in the study. Patients who participate in the study will have the right to obtain all relevant information and will be allowed to withdraw their consent or discontinue participation without restrictions at any time during the study. The confidentiality of participant records will be protected.
Study Population
Inclusion Criteria Will Be as Follows
- Age 18–65 years.
- American Society of Anesthesiologists (ASA) physical status I–II.
- Scheduled elective intraspinal tumor resection and with chronic pain related to the tumor.
Exclusion Criteria Will Be as Follows
- History of drug abuse, psychiatric disorders, or obesity (> 130% standard weight).
- Currently taking opioids, carbamazepine, gabapentin or pregabalin.
- Communication disorders.
- Contraindications for propofol, opioids, and gabapentin (eg, allergy).
- Failure to use a patient-controlled analgesia (PCA) device.
Randomization and Blinding
The participants will be randomized into gabapentin combined with sufentanil and sufentanil groups in a 1:1 ratio 2 days before surgery. Randomization will be performed with a computer-generated list of random numbers. Each patient will be provided with an opaque sealed envelope containing the participant’s group on the inside and the participant’s order on the outside. Oral placebo or gabapentin will be administered by a nurse who will not be involved in the evaluation at 36 and 24 h prior to surgery, according to the patient’s distribution information. The participants, the surgeons in charge of the operation, and the anesthesiologists performing the anesthesia or follow-up will be blinded to the group assignment. In an emergency, the anesthesiologist can unblind the participant to the treatment and exclude the case. In this study, patients in the gabapentin group will be given gabapentin capsules, while patients in the control group will be given starch capsules, which are identical in appearance. According to the patient’s distribution information, an oral placebo or gabapentin will be administered by a nurse who will not be involved in the evaluation at 36h, 24h, and 12h before surgery.
Subject Eligibility and Identification
The patients will be visited 2 days before surgery to evaluate whether they meet the inclusion criteria. All enrolled patients will be privy to all information about the objective, procedure, benefits, and potential risks of the trial and will be given sufficient time to decide whether to participate in this study. Every participant will sign an informed consent form. The researcher will then complete a qualification checklist based on the items listed in the case report form (CRF) and the patient’s demographic characteristics, including age (years), sex (male or female), height, weight, and ASA grade. If the patient does not meet all the inclusion criteria, he or she will be excluded. Every participant will have the right to discontinue participation at any time.
Intervention
All participants will be randomly divided into two groups for perioperative analgesia:
Sufentanil group (group S): On the basis of maintaining the original analgesic drugs, the patients will receive an oral placebo at 36 h, 24 h, and 12 h preoperatively. Gabapentin combined with sufentanil group (group GS): On the basis of maintaining the original analgesic drugs, the patients will be given 300 mg gabapentin orally 36 h, 24 h, and 12 h before surgery. In addition, both groups of patients will be administered the same anesthesia regime and postoperative analgesia strategy by the anesthesiologists. The anesthesiologists will be blinded to the grouping.
Perioperative Anesthesia Management
Preoperative Visit and Evaluation
Two days before surgery, the patients will be interviewed. After signing the informed consent form, the patients will be evaluated, and the degree of preoperative pain will be recorded using a visual analog scale (VAS) pain score (0–10 points, 0=no pain, 10=excruciatingly severe pain), the use of analgesics (type and dose) and the mechanical pain thresholds using a Von Frey electronic pain meter. A patient-controlled analgesia pump (PCA) will be introduced to apply the medication.
Intraoperative Anesthesia
All participants will be anesthetized according to a standard procedure. After transfer to the operating room (OT), peripheral intravenous (IV) access will be secured, and blood pressure, electrocardiogram findings, pulse oxygen saturation, and the bispectral index (BIS) will be monitored. Radial artery catheterization will be performed to monitor continuous arterial pressure before anesthesia induction. Hydroxyethyl starch 130/0.4 7 mL/kg will be infused at a rate of 20 mL/kg·h.
Anesthesia will be induced with midazolam (Nhwa Pharma. Corporation, Xuzhou, China) at 0.03 mg/kg, sufentanil (Humanwell Pharma. Corporation, Yichang, China) at 0.4 μg/kg, and propofol (Fresenius Kabi, Uppsala, Sweden) 1.5–2 mg/kg in sequence. Rocuronium (Xianju Pharma. Corporation, Taizhou, China) 0.9 mg/kg will be administered when the patient loses consciousness, and the BIS reaches 40–60. Anesthesia will be maintained with propofol and remifentanil (Humanwell Pharma. Corporation, Yichang, China) pumped continuously keeping blood pressure and BIS in normal range. Sufentanil 0.15 μg/kg and 0.05–0.1μg/kg will be administered at the beginning of the operation and after removal of the microscope respectively. Ondansetron 8 mg and tramadol 100 mg will be given immediately after the incision is closed. End-expiratory partial pressure of carbon dioxide (ETCO2) will be maintained at 35–45 mmHg during anesthesia. Propofol and remifentanil will be discontinued after surgery. Endotracheal intubation will be removed when the patient’s tidal volume is > 6 mL/kg, ETCO2 is < 45 mmHg, and the swallowing and coughing reflexes recover.
Vital signs will be closely monitored during the operation. Blood pressure will be maintained within ±20% of baseline, body temperature within 35.8–37.0°C, and BIS within 40–60.
Postoperative Pain Management
The patients will be transferred to the postoperative anesthesia recovery room (PACU) after extubation. Sufentanil (2 μg/time) will be given until the VAS pain score less than or equal to 3. If the VAS pain score less than or equal to 3, the Ramsay score is Grade 2–3, or the respiratory rate less than 12 beats/min, the intravenous sufentanil injection will be stopped. PCA intravenous analgesia will be administered 2 h after surgery. The PCA device will administer sufentanil 2 μg/kg diluted to 150 mL with normal saline and be set to a background infusion of 2 mL/h, a demand dose of 0.5 mL, a lockout interval of 15 minutes, and a maximum dosage of 4 mL/h. If a patient complains of pain, PCA button can be pressed repeatedly until pain relief. If VAS score is higher than 4, flurbiprofen axetil will be administered intravenously twice a day at most. The doses and frequency of rescue analgesics will be documented.
Follow-Up
The VAS pain score, Von Frey mechanical pain threshold, consumption of sufentanil, Ramsay score, incidence of nausea, vomiting, drowsiness, or dizziness, postoperative gastrointestinal function recovery time, the time of first feeding, and the time to first rise from the bed will be observed from 36 h before surgery to 48 h after surgery. Other analgesic remedies (drug type and dose) for poor analgesia will be recorded. The length of hospital stay and medical expenses will be collected upon discharge. All follow-up subjects will receive the same training and will not be informed of the grouping.
Outcomes
The aim of the study will be to evaluate the efficacy and safety of multimodal analgesia combining gabapentin with sufentanil for patients undergoing intraspinal tumor resection.
Primary Outcome
The primary outcome will be the consumption of sufentanil 48 h after surgery.
Secondary Outcomes
The secondary outcomes will be as follows:
- Pain score: VAS pain score (at rest and at movement) at 2 h, 24 h, and 48 h after surgery.
- Von Frey pain threshold: Mechanical pain thresholds between the first and second metacarpal bones on the dorsal side of both hands according to the Von Frey electronic pain meter at 24 h and 48 h after surgery.
- Total consumption of analgesic drugs (type and dosage) except sufentanil at 2 h, 24 h, and 48 h after surgery.
- The total number of times that the patient presses the PCA button, including effective presses and ineffective presses within 24 h and 48 h after surgery.
- Ramsay score at 24 h and 48 h after surgery.
- Incidence of postoperative nausea, vomiting, and drowsiness.
- The time of recovery of gastrointestinal function after surgery, the time of first feeding, the time of postoperative getting out of bed, the length of hospital stay and medical expenses.
Sample Size Calculation
According to the results of previous studies, the consumption of postoperative analgesics for patients who used gabapentin preoperatively was lower than that of the control group. The sample size was calculated with the model of Test for Two independent samples in PASS V.14 software (NCSS, Kaysville, Utah, USA) on the basis of the consumption of postoperative opioids on the second postoperative day from our exploration study (in which the consumption of postoperative opioids in the gabapentin group was 15% lower than that in the control group) as the primary endpoint and the difference test as the study design. Given an α level of 0.05, a β level of 0.2, and an additional dropout rate of 20%, the total sample size required is 84 in each group. Therefore, 168 patients (84 in each group) will be enrolled in the study.
Statistical Analysis
The SPSS 18.0 (SPSS Inc., California, USA) statistical software package will be used for statistical analysis. Continuous variables such as age, weight, height, VAS pain scores, mechanical pain threshold, temperature, BIS, heart rate (HR), mean arterial pressure (MAP), duration of anesthesia, duration of operation, consumption of propofol and sufentanil during operation, total consumption of analgesic drugs except for sufentanil, the total number of times that the patient presses the PCA button effectively or ineffectively, the time of recovery of gastrointestinal function after surgery, the length of hospital stay and medical expenses will be analyzed by the Kolmogorov–Smirnov test to determine the normality of the data distribution. Normally distributed data will be expressed as the means ± standard deviations and analyzed by independent t-tests or one-way ANOVA between groups or linear mixed models for repeatedly-measured outcomes. Nonnormally distributed data will be expressed as medians and interquartile ranges and analyzed by the Wilcoxon signed-rank test. Categorical data, such as sex, ASA score, use of analgesic drugs except for sufentanil, and postoperative complications, will be expressed as numbers of patients (percentages) and analyzed by Pearson’s chi-square test. P< 0.05 will be considered statistically significant. In this study, the dropout rate of 20% is considered when calculating the sample size. We will analyze the data by both intent-to-treat and per-protocol approaches. Missing data will be credited by the appropriate method to perform ITT analysis.
Reporting of Adverse Events
All adverse events will be recorded in detail, handled properly, and tracked until they are resolved, or the patient stabilizes. Serious adverse events and unexpected events will be reported to the ethics committee, competent authorities, sponsors, and drug regulatory authorities immediately as required. The principal investigator will conduct a cumulative review of all adverse events on a regular basis and hold an investigator meeting when necessary to assess the risks and benefits of the study. If necessary, emergency unblinding can be performed in the double-blind test to ensure the safety and rights of the subjects. For studies with greater than minimal risk, independent data monitors will be assigned to monitor the study data. For high-risk studies, an independent data safety oversight committee will be established to monitor the accumulated safety data and validity data to make recommendations on whether to proceed with the study.
Discussion
This single-center, prospective, randomized, placebo-controlled and double-blinded clinical trial is designed to explore gabapentin combined with sufentanil for perioperative analgesia of intraspinal tumor resection.
Intraspinal tumors are tumors and metastatic tumors occurring in various tissues of the spinal canal, such as the spinal cord, nerve root, meningeal membrane and adjacent tissues. Postoperative pain in patients with intraspinal tumors can be severe and long lasting,33 leading to a series of factors that are not conducive to patient recovery.1 For example, sympathetic hyperexcitability will increase the occurrence of cardiovascular adverse events, and continuous pain can suppress immunity, delay wound healing and movement, increase the risk of postoperative infection and thromboembolism, prolong hospital stay and raise medical costs.4,5 In addition, severe postoperative pain can increase the risk of chronic pain and even mood disorders such as anxiety and depression.34,35 Effective perioperative analgesia can alleviate adverse effects.
Studies have shown that the mechanism of postoperative pain in patients with intraspinal tumors is different from that of other surgeries. Neuropathic pain from tumor compression or invasion of the nerve roots or spinal cord is usually present before surgery and manifests as spontaneous pain, tactile pain, hyperalgesia, and paresthesia. In addition to the central pain caused by injuries of the local spinal cord and nerve root due to tumor invasion and operation, peripheral pain and central sensitization are also present. Factors such as direct injury at the surgical site, local inflammatory edema, the release of inflammatory mediators, and stimulation of peripheral receptors to produce pain (peripheral pain).6,7 At the same time, harmful sensory impulses can be transmitted to the spinal cord and brain, leading to hypersensitivity of central pain in the early postoperative period, lowering the pain threshold and aggravating central pain.8 In addition, large doses of remifentanil are often used for intraoperative SSEP and MEP monitoring during intraspinal tumor resection, which results in postoperative hyperalgesia.9
A previous study by our group confirmed that some patients still experienced poor analgesia and moderate pain when administered sufentanil or tramadol PCIA after intraspinal tumor resection. However, one disadvantage of sufentanil is that it has a dose-dependent respiratory inhibitory effect. The incidence of nausea, vomiting, and excessive sedation also increases with increasing dosage.6,36 Therefore, sufentanil still has some risks when used for postoperative analgesia, especially for elderly individuals, children, and patients with central nervous system diseases. Currently, the combination of local anesthetics or other analgesics with opioids can effectively alleviate pain and reduce the side effects of opioids, according to an increasing number of clinical studies. In a single-center randomized controlled study, Liu et al37 confirmed that compared to traditional postoperative analgesia in a control group, an ERAS program that combined local anesthesia with postoperative analgesia can accelerate recovery in patients undergoing intraspinal tumor resection, shorten hospital stay and alleviate pain from 1 day after surgery to discharge, but the patient’s pain on the day of surgery was still severe. A previous study by our group administered lidocaine in the perioperative period of intraspinal tumor resection and found that it can reduce the pain scores on the first and second days after surgery, but only for patients with extramedullary tumors and no chronic pain before surgery.
In many analgesia guidelines, gabapentin is also recommended for use in multimodal analgesia.14 Gabapentin binds to the α2δ subunit of voltage-gated calcium channels in the spinal cord and peripheral nerves, decreases excitatory neurotransmitter release from activated nociceptors, inhibits ascending pain transmission, activates descending inhibitory pathways, and prevents hyperalgesia and central sensitization. Animal experiments have shown that gabapentin can act on central sensitization and other noxious stimulus pathways to relieve hyperalgesia, postoperative pain, and postoperative inflammation caused by nerve damage.38,39 In a study by Koea and colleagues40 on 100 patients undergoing liver resection, the patients who received a combination of an intrathecal injection of morphine and oral gabapentin during the perioperative period ate and were discharged earlier than patients who were only administered postoperative epidural analgesia. In a study on cervical spinal surgery, multimodal analgesia reportedly achieved the same analgesic effect as PCA, but it required less consumption of anesthetic drugs and had a lower incidence of nausea and vomiting and a shorter hospital stay.41 Whether the perioperative use of gabapentin combined with sufentanil as multimodal analgesia for intraspinal tumor resection can optimize pain treatment of such patients is a question of concern in this study.
Safety is another of our concerns. Studies show that the use of gabapentin before surgery slightly increases the incidence of drowsiness. However, the drowsiness is mild, brief, and gradually decreases as the treatment time increases. Gabapentin has no effect on the incidence of postoperative nausea and vomiting;42 however, there is no research focusing on the effect of preoperative gabapentin on its side effects, such as nausea, vomiting, drowsiness, and postoperative recovery after intraspinal tumor resection. In the proposed study, we will strictly limit patients to those 18–65 years old with ASA grades I–II. In addition, every patient will be monitored intensively to detect and manage potential adverse events in a timely manner. If the patients exhibit any adverse events associated with the experimental drugs, such as signs of vertigo, somnolence, headache, ataxia, nystagmus, peripheral edema, digestive symptoms (diarrhea, bloating, and nausea), and allergies (rashes and dermatitis), the drug will be stopped at once. However, we note that overly stringent inclusion and exclusion criteria may affect the generalization of the conclusion.
In summary, there are few studies on postoperative analgesia for patients with intraspinal tumors, while those that have investigated this topic have employed small sample sizes. The efficiency and safety of multimodal analgesia using different analgesia methods or drugs after intraspinal tumor resection need to be confirmed by more trials. In this study, gabapentin, a clinical drug for the treatment of neuropathic pain, will be used for the first time in perioperative pain management for patients with intraspinal tumors. If the results of this randomized, double-blind, and controlled prospective clinical study show that perioperative multimodal analgesia combining gabapentin with sufentanil can significantly decrease postoperative sufentanil consumption, this study will help improve the analgesic effect and accelerate postoperative recovery for these patients.
Trial Status
The trial was registered at chictr.org.cn on May 3rd, 2021 (identifier ChiCTR2100046055). The study was approved by the Institutional Review Board at Beijing Tiantan Hospital, Capital Medical University, on February 8th, 2021 (reference number KY2020-141-02). The first participant was recruited on 20 June 2021, and the anticipated completion date will be 31 December 2022.
Data Sharing Statement
The CRF will be stored at Beijing Tiantan Hospital. The datasets will be available from the primary investigator upon reasonable request after the publication of the study results.
Acknowledgments
This work was supported by funding from WUJIEPING medical foundation (320.6750.2022-05-1).
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. Yuan Zhang and Hongli Yue contributed equally to this work. Ruquan Han and Weihua Cui are the co-corresponding authors of the article.
Disclosure
The authors declare no competing interests.
References
1. Nakamura M, Tsuji O, Iwanami A, et al. Central neuropathic pain after surgical resection in patients with spinal intramedullary tumor. J Orthop Sci. 2012;17(4):352–357. doi:10.1007/s00776-012-0236-6
2. Carli F. Physiologic considerations of Enhanced Recovery After Surgery (ERAS) programs: implications of the stress response. Can J Anaesth. 2015;62(2):110–119. doi:10.1007/s12630-014-0264-0
3. Mathiesen O, Dahl B, Thomsen BA, et al. A comprehensive multimodal pain treatment reduces opioid consumption after multilevel spine surgery. Eur Spine J. 2013;22(9):2089–2096. doi:10.1007/s00586-013-2826-1
4. Fletcher D, Stamer UM, Pogatzki-Zahn E, et al. Chronic postsurgical pain in Europe: an observational study. Eur J Anaesthesiol. 2015;32(10):725–734. doi:10.1097/EJA.0000000000000319
5. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–540. doi:10.1213/01.ANE.0000068822.10113.9E
6. Bajwa SJ, Haldar R. Pain management following spinal surgeries: an appraisal of the available options. J Craniovertebr Junction Spine. 2015;6(3):105–110. doi:10.4103/0974-8237.161589
7. Devin CJ, McGirt MJ. Best evidence in multimodal pain management in spine surgery and means of assessing postoperative pain and functional outcomes. J Clin Neurosci. 2015;22(6):930–938. doi:10.1016/j.jocn.2015.01.003
8. Rivkin A, Rivkin MA. Perioperative nonopioid agents for pain control in spinal surgery. Am J Health Syst Pharm. 2014;71(21):1845–1857. doi:10.2146/ajhp130688
9. Koppert W, Schmelz M. The impact of opioid-induced hyperalgesia for postoperative pain. Best Pract Res Clin Anaesthesiol. 2007;21(1):65–83. doi:10.1016/j.bpa.2006.12.004
10. Shah SA, Guidry R, Kumar A, White T, King A, Heffernan MJ. Current trends in pediatric spine deformity surgery: multimodal pain management and rapid recovery. Global Spine J. 2020;10(3):346–352. doi:10.1177/2192568219858308
11. Kurd MF, Kreitz T, Schroeder G, Vaccaro AR. The role of multimodal analgesia in spine surgery. J Am Acad Orthop Surg. 2017;25(4):260–268. doi:10.5435/JAAOS-D-16-00049
12. Dunn LK, Durieux ME, Nemergut EC. Non-opioid analgesics: novel approaches to perioperative analgesia for major spine surgery. Best Pract Res Clin Anaesthesiol. 2016;30(1):79–89. doi:10.1016/j.bpa.2015.11.002
13. Seki H, Ideno S, Ishihara T, Watanabe K, Matsumoto M, Morisaki H. Postoperative pain management in patients undergoing posterior spinal fusion for adolescent idiopathic scoliosis: a narrative review. Scoliosis Spinal Disord. 2018;13(1):17. doi:10.1186/s13013-018-0165-z
14. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
15. Gilron I, Orr E, Tu D, O’Neill JP, Zamora JE, Bell AC. A placebo-controlled randomized clinical trial of perioperative administration of gabapentin, rofecoxib and their combination for spontaneous and movement-evoked pain after abdominal hysterectomy. Pain. 2005;113(1–2):191–200. doi:10.1016/j.pain.2004.10.008
16. Muhly WT, Sankar WN, Ryan K, et al. Rapid recovery pathway after spinal fusion for idiopathic scoliosis. Pediatrics. 2016;137(4):25. doi:10.1542/peds.2015-1568
17. Rorarius MG, Mennander S, Suominen P, et al. Gabapentin for the prevention of postoperative pain after vaginal hysterectomy. Pain. 2004;110(1–2):175–181. doi:10.1016/j.pain.2004.03.023
18. Rai AS, Khan JS, Dhaliwal J, et al. Preoperative pregabalin or gabapentin for acute and chronic postoperative pain among patients undergoing breast cancer surgery: a systematic review and meta-analysis of randomized controlled trials. J Plast Reconstr Aesthet Surg. 2017;70(10):1317–1328. doi:10.1016/j.bjps.2017.05.054
19. Chiu C, Aleshi P, Esserman LJ, et al. Improved analgesia and reduced post-operative nausea and vomiting after implementation of an enhanced recovery after surgery (ERAS) pathway for total mastectomy. BMC Anesthesiol. 2018;18(1):41. doi:10.1186/s12871-018-0505-9
20. Jiang Y, Li J, Lin H, et al. The efficacy of gabapentin in reducing pain intensity and morphine consumption after breast cancer surgery: a meta-analysis. Medicine. 2018;97(38):e11581. doi:10.1097/MD.0000000000011581
21. Wang L, Dong Y, Zhang J, Tan H. The efficacy of gabapentin in reducing pain intensity and postoperative nausea and vomiting following laparoscopic cholecystectomy: a meta-analysis. Medicine. 2017;96(37):e8007. doi:10.1097/MD.0000000000008007
22. Kochhar A, Chouhan K, Panjiar P, Vajifdar H. Gabapentinoids as a part of multi-modal drug regime for pain relief following laproscopic cholecystectomy: a randomized study. Anesth Essays Res. 2017;11(3):676–680. doi:10.4103/0259-1162.204208
23. Wang J, Fu G, Liu J, Yu Y, Wang N. Effect of preoperative gabapentin after transurethral prostate resection under general anesthesia. A randomized double-blind, placebo-controlled trial. Saudi Med J. 2020;41(6):640–644. doi:10.15537/smj.2020.6.25132
24. Peng C, Li C, Qu J, Wu D. Gabapentin can decrease acute pain and morphine consumption in spinal surgery patients: a meta-analysis of randomized controlled trials. Medicine. 2017;96(15):e6463. doi:10.1097/MD.0000000000006463
25. Moore L, Norwood C, Stackhouse R, Nguyen K, Brown W, Sevak RJ. Gabapentin reduces postoperative pain and opioid consumption in patients who underwent lumbar laminectomy. J Am Pharm Assoc (2003). 2021;61(5):e78–e83. doi:10.1016/j.japh.2021.05.002
26. Trzcinski S, Rosenberg RE, Vasquez Montes D, et al. Use of gabapentin in posterior spinal fusion is associated with decreased postoperative pain and opioid use in children and adolescents. Clin Spine Surg. 2019;32(5):210–214. doi:10.1097/BSD.0000000000000783
27. Felder L, Saccone G, Scuotto S, et al. Perioperative gabapentin and post cesarean pain control: a systematic review and meta-analysis of randomized controlled trials. Eur J Obstet Gynecol Reprod Biol. 2019;233:98–106. doi:10.1016/j.ejogrb.2018.11.026
28. Carvalho B, Sutton CD, Kowalczyk JJ, Flood PD. Impact of patient choice for different postcesarean delivery analgesic protocols on opioid consumption: a randomized prospective clinical trial. Reg Anesth Pain Med. 2019;44(5):578–585. doi:10.1136/rapm-2018-100206
29. McGauvran MM, Ohnuma T, Raghunathan K, et al. Association between gabapentinoids and postoperative pulmonary complications in patients undergoing thoracic surgery. J Cardiothorac Vasc Anesth. 2021;36(8 Pt A):2295–2302. doi:10.1053/j.jvca.2021.10.003
30. Grosen K, Drewes AM, Hojsgaard A, Pfeiffer-Jensen M, Hjortdal VE, Pilegaard HK. Perioperative gabapentin for the prevention of persistent pain after thoracotomy: a randomized controlled trial. Eur J Cardiothorac Surg. 2014;46(1):76–85. doi:10.1093/ejcts/ezu032
31. Zakkar M, Frazer S, Hunt I. Is there a role for gabapentin in preventing or treating pain following thoracic surgery? Interact Cardiovasc Thorac Surg. 2013;17(4):716–719. doi:10.1093/icvts/ivt301
32. Eipe N, Penning J, Yazdi F, et al. Perioperative use of pregabalin for acute pain-A systematic review and meta-analysis. Pain. 2015;156(7):1284–1300. doi:10.1097/j.pain.0000000000000173
33. Engelhard HH, Villano JL, Porter KR, et al. Clinical presentation, histology, and treatment in 430 patients with primary tumors of the spinal cord, spinal meninges, or cauda equina. J Neurosurg Spine. 2010;13(1):67–77. doi:10.3171/2010.3.SPINE09430
34. Ghoneim MM, O’Hara MW. Depression and postoperative complications: an overview. BMC Surg. 2016;16:5. doi:10.1186/s12893-016-0120-y
35. Woo AK. Depression and anxiety in pain. Rev Pain. 2010;4(1):8–12. doi:10.1177/204946371000400103
36. Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–20.
37. Liu B, Liu S, Wang Y, et al. Enhanced recovery after intraspinal tumor surgery: a single-institutional randomized controlled study. World Neurosurg. 2020;136:e542–e552. doi:10.1016/j.wneu.2020.01.067
38. Bannister K, Qu C, Navratilova E, et al. Multiple sites and actions of gabapentin-induced relief of ongoing experimental neuropathic pain. Pain. 2017;158(12):2386–2395. doi:10.1097/j.pain.0000000000001040
39. Mao J, Chen LL. Gabapentin in pain management. Anesth Analg. 2000;91(3):680–687. doi:10.1097/00000539-200009000-00034
40. Koea JB, Young Y, Gunn K. Fast track liver resection: the effect of a comprehensive care package and analgesia with single dose intrathecal morphine with gabapentin or continuous epidural analgesia. HPB Surg. 2009;2009:271986. doi:10.1155/2009/271986
41. Bohl DD, Louie PK, Shah N, et al. Multimodal versus patient-controlled analgesia after an anterior cervical decompression and fusion. Spine. 2016;41(12):994–998. doi:10.1097/BRS.0000000000001380
42. Arumugam S, Lau CS, Chamberlain RS. Use of preoperative gabapentin significantly reduces postoperative opioid consumption: a meta-analysis. J Pain Res. 2016;9:631–640. doi:10.2147/JPR.S112626
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.