Back to Journals » Journal of Pain Research » Volume 18
Effect of Spinal Cord Stimulation on Skin Temperature in Patients with Neuropathic Pain: An Observational Study
Authors Gehling M ![]() , Bertelmann-Barge K, Roth C
, Bertelmann-Barge K, Roth C
Received 9 July 2025
Accepted for publication 18 December 2025
Published 31 December 2025 Volume 2025:18 Pages 7327—7333
DOI https://doi.org/10.2147/JPR.S552635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Markus Gehling,1,2 Katrin Bertelmann-Barge,2 Christian Roth3,4
1Pain Center, Kassel, Germany; 2Department of Anesthesiology and Intensive Care Medicine, University of Marburg, Marburg, Germany; 3Department of Neurology, Klinikum Kassel, Kassel, Germany; 4Department of Neurology, Philipps University of Marburg, Marburg, Germany
Correspondence: Markus Gehling, Email [email protected]
Background: Spinal cord stimulation (SCS) can successfully treat neuropathic pain when conventional medication fails. Current evaluation methods, however, are primarily subjective. This study explored the use of infrared thermography as an objective method to detect physiological effects of SCS.
Methods: This prospective observational study included 25 patients treated with SCS for neuropathic pain. Skin temperature was measured using infrared thermography before and during the first 60 minutes of stimulation. Pain intensity was assessed using an 11-point Numerical Rating Scale (NRS). The primary hypothesis was that SCS would lead to a significant skin temperature increase of at least 1°C.
Results: Mean skin temperature in the affected area increased significantly from 29.1 ± 2.3°C to 30.8 ± 1.8°C (p = 0.0002). On the contralateral side, it increased from 29.3 ± 2.2°C to 30.0 ± 1.8°C (p = 0.0037). Temperature responses varied among individuals. A post hoc analysis showed that patients with a temperature increase of ≥ 1°C (responders) demonstrated significantly greater long-term improvement in pain chronification scores compared to non-responders (p = 0.002).
Conclusion: SCS produces measurable increases in skin temperature in patients with neuropathic pain. A ≥ 1°C temperature increase may indicate favorable long-term response. Infrared thermography may serve as a valuable objective measure for evaluating SCS efficacy.
Keywords: spinal cord stimulation, skin temperature, clinical response, patient selection
Introduction
Spinal cord stimulation (SCS) has been shown to effectively relieve neuropathic pain even in cases where conventional pharmacological interventions have failed.1–4 Indications for SCS are determined based on the underlying condition. Randomized controlled trials support its use for failed back surgery syndrome with back or leg pain, complex regional pain syndrome (CRPS), and polyneuropathy.
Decisions about permanent SCS implantation are based on both diagnosis and acute effects observed during a trial phase of 5–7 days.5 Psychosocial factors, including depression, anxiety, catastrophizing, low self-efficacy, personality disorders, and poor social support, can influence long-term outcomes, although standardized assessments of these contraindications remain lacking.
Currently, SCS indications rely heavily on subjective patient reports during the trial phase. We aimed to support decision-making with objective parameters that are independent of patient cooperation and feasible in routine clinical settings. Increased skin temperature, as a marker of sympathetic inhibition (sympatholysis), appeared promising in this context.
Sympatholysis has been shown to alleviate neuropathic pain in CRPS,6,7 diabetic neuropathy,8 and postherpetic neuralgia.9 While its effects are typically transient, SCS may offer a more sustainable alternative.
Previous studies have demonstrated the sympatholytic effect of SCS, improving coronary and peripheral blood flow.10–13 These effects may explain improvements in wound healing observed in peripheral artery disease.14,15 Enhanced microcirculation has also been documented with SCS.
Sympathetic dysfunction has been particularly studied in CRPS,16 where SCS has been proven effective.2,17 We hypothesized that part of the analgesic effect of SCS may be mediated by sympatholysis, detectable via changes in skin temperature.
However, some studies question the clinical relevance of sympatholysis in SCS. For example, microcirculation did not improve in some patients with critical limb ischemia.18 In neuropathic pain, consistent changes in skin blood flow or skin temperature were not demonstrated.19,20 Furthermore, SCS-induced pain relief in CRPS was not always associated with microcirculatory changes,2 and SCS failed to reduce central sympathetic tone in patients with heart failure.21
Objective biomarkers reflecting the physiological effects of spinal cord stimulation (SCS) in neuropathic pain may help optimize patient selection for this therapy. The assessment of SCS-induced changes in skin temperature could serve as a simple and objective measure, independent of patient perception or reporting. We conducted this prospective observational study to investigate whether SCS leads to measurable increases in skin temperature in patients with neuropathic pain. Our hypothesis was that SCS would result in a regional skin temperature increase of at least 1°C.
Methods
After obtaining ethics approval (Ethics Committee of the State Medical Association of Hesse, 2020–1515-evBO) and registering the study design (DRKS-ID 00022524), the study was conducted at an outpatient pain center in 2020. Participants gave written informed consent. This study complies with the Declaration of Helsinki. Inclusion criteria were patients treated with SCS for neuropathic pain. Exclusion criteria were known peripheral arterial disease, inability to pause SCS for pain control, or lack of consent.
Skin temperature was measured in the target area of stimulation over the first 60 minutes after SCS initiation. Pain intensity was assessed using an 11-point NRS (0 = no pain, 10 = worst imaginable pain). Patients received low-frequency stimulation (80–150 Hz; pulse width 80–350 µsec with a Medtronic™ System). Demographic and clinical data were extracted from patient records.
Temperature data were collected with a commercial infrared camera (Seek Shot Pro™, accuracy ±0.1°C). Each data point represented the average of ~1000 pixel readings. Measurements were taken after a minimum 6-hour SCS pause, in a temperature-controlled room (20°C ± 1°C to 23°C ± 1°C) following a 30-minute acclimatization.
Baseline temperature was recorded from the affected area with active SCS turned off. After switching on stimulation, temperature measurements were repeated at 5, 10, 15, 30, 45, and 60 minutes. Pain intensity was recorded at each time point.
Sample size calculations (GraphPad) indicated that 25 measurements with a standard deviation of 0.29 had 80% power to detect a 0.3°C difference (p < 0.05, two-tailed). Data distribution was normal. One-way ANOVA was used for skin temperature and pain scores; other comparisons used non-parametric tests or Fisher’s exact test. In three individual skin temperature measurements, data completion was performed by using an interpolated value (n = 1) or by carrying forward the last valid measurement at the end of the recording sequence (n = 2). All other missing data were excluded from analysis.
Results
Of 35 eligible patients, 25 were included. One had died, three declined, and six could not be contacted. Table 1 summarizes demographic data. Most patients were long-term responders with reduced pain chronification, disability, and improved quality of life. Pain score also declined promptly after stimulation (Figure 1).
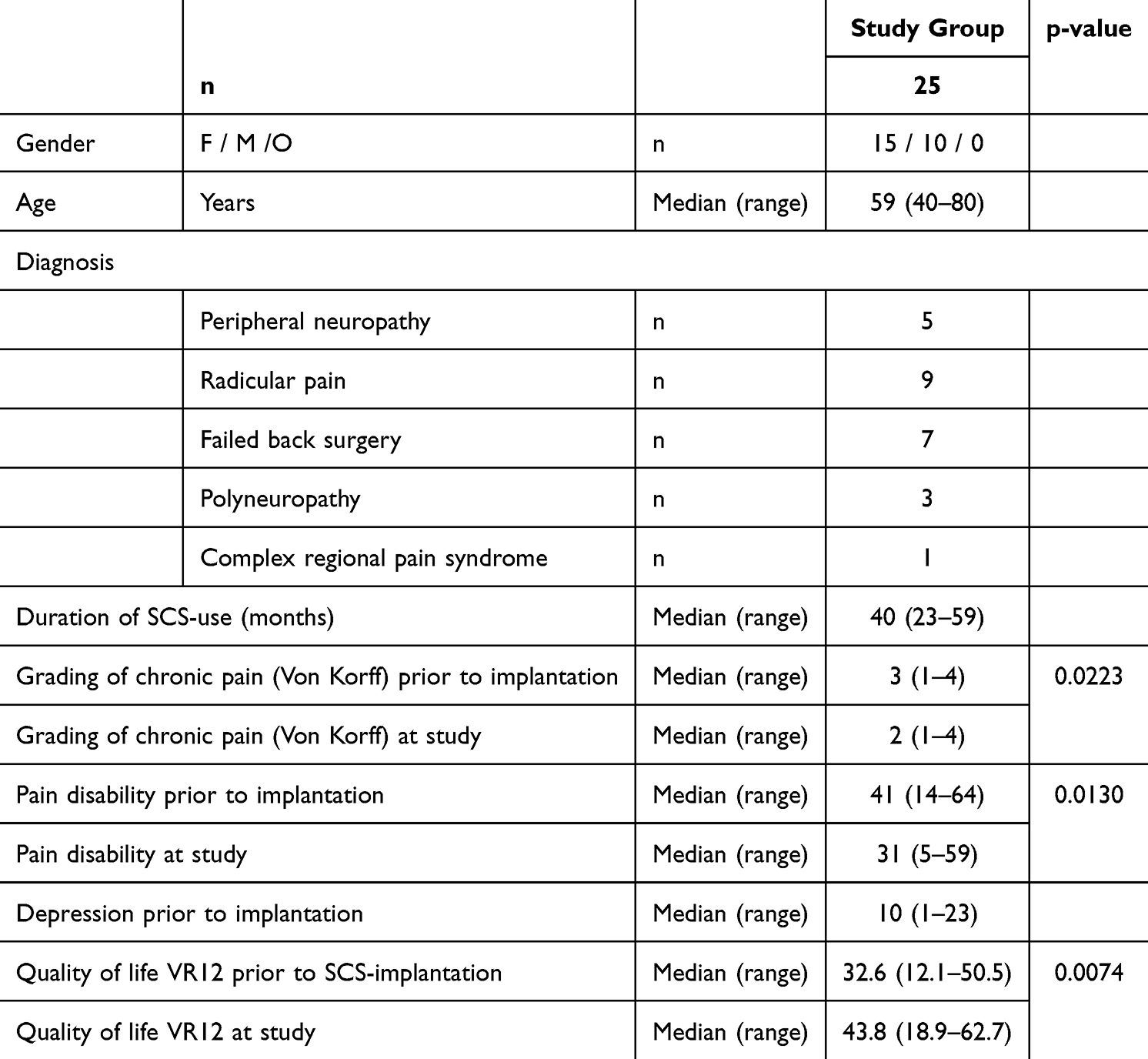 |
Table 1 Descriptive Data |
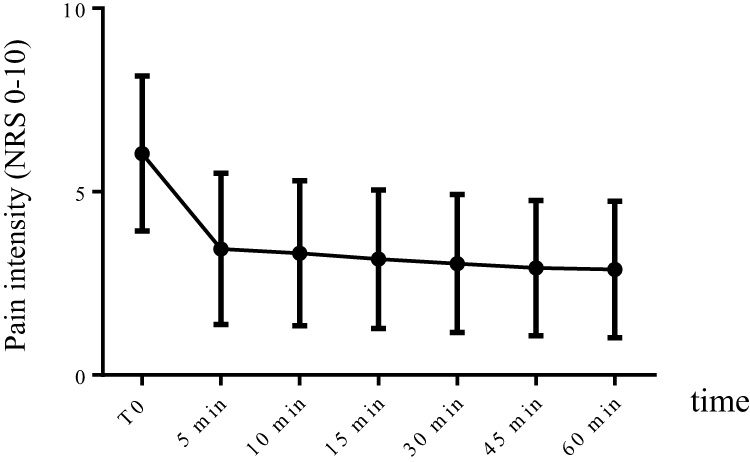 |
Figure 1 Pain intensity in response to spinal cord stimulation (mean ± sem). |
After pausing stimulation pause ≥ 6 hours, reactivation led to a significant increase in skin temperature on the affected side from 29.1 ± 2.3°C to 30.8 ± 1.8°C (p = 0.0002, Figure 2). The contralateral side rose from 29.3 ± 2.2°C to 30.0 ± 1.8°C (p = 0.0037, Table 2). Differences between sides were not statistically significant at baseline or at 60 minutes.
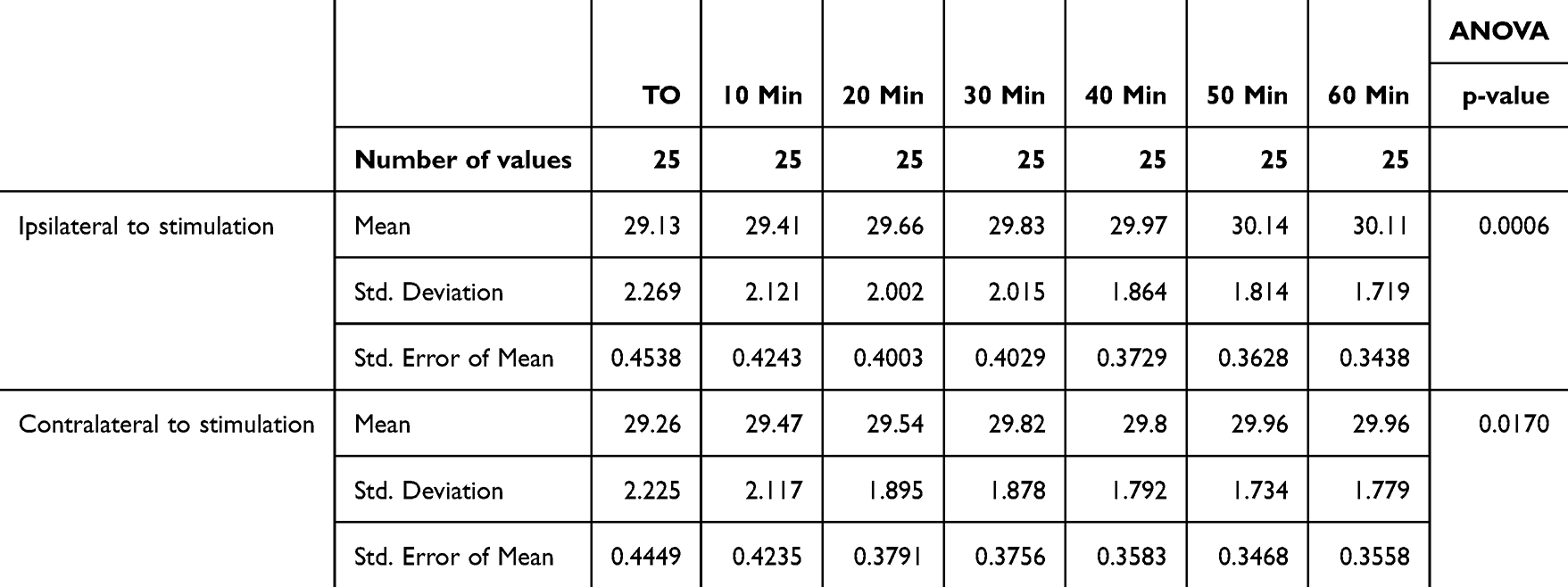 |
Table 2 Skin Temperature After Start of Spinal Cord Stimulation |
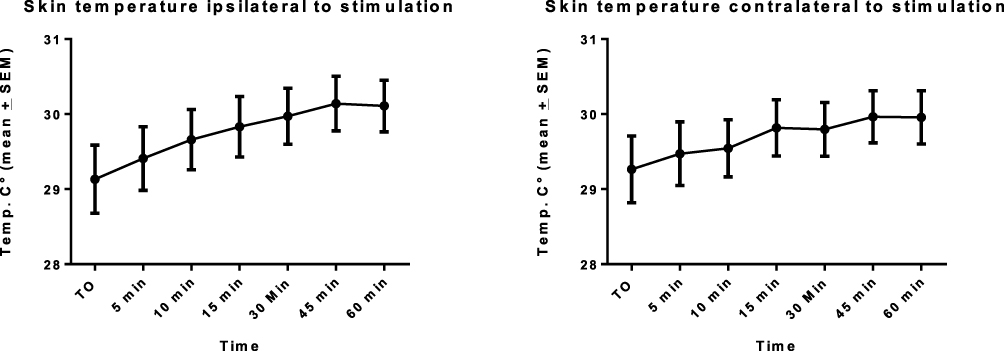 |
Figure 2 Mean skin temperature changes (mean + sem). Ipsilateral (left) and contralateral (right) skin temperature response to spinal cord stimulation. |
Figure 3 illustrates individual variability in temperature responses (Figure 3). A post hoc analysis identified responders (≥1°C increase), who showed greater improvement in Von Korff pain grading (1.6 ± 1.1 vs 0 ± 1.0; p = 0.002; Figure 4).
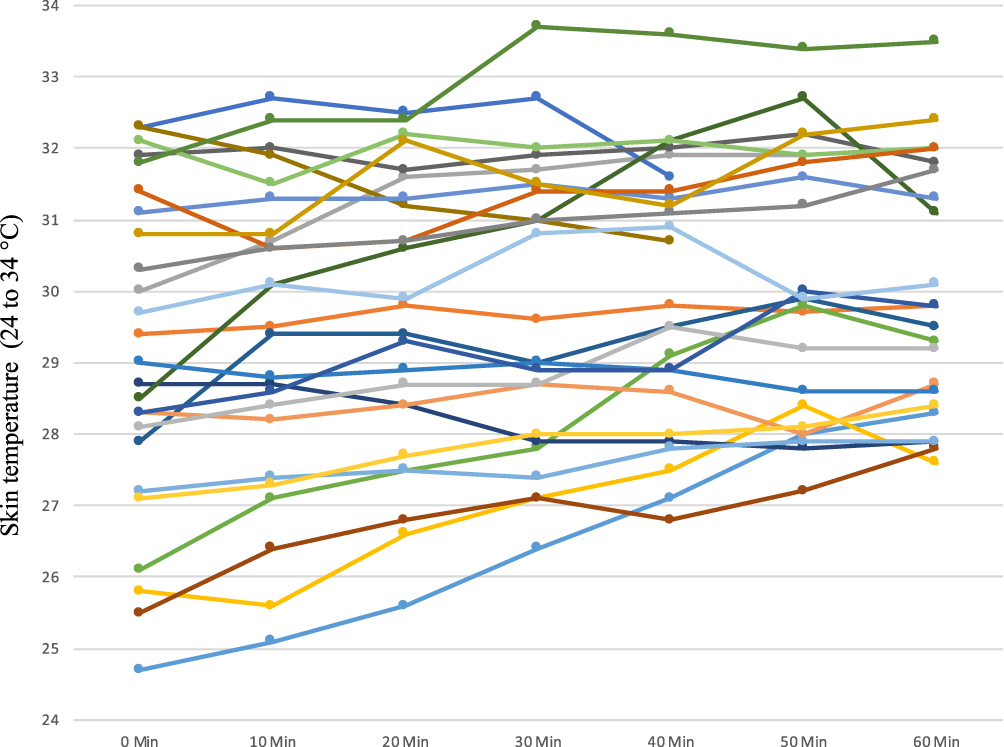 |
Figure 3 Individual patient temperature responses. Colored lines represent individual skin temperature responses to spinal cord stimulation. |
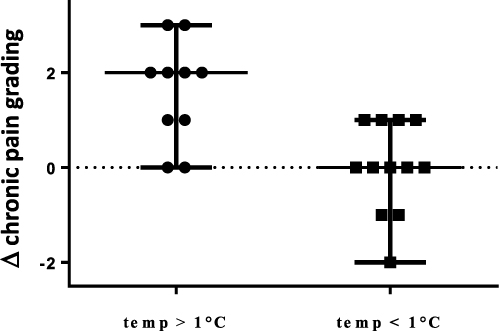 |
Figure 4 Pain grading improvements by thermal response (median and range). Improvement of chronic pain grading in patients with temperature increase > 1°C (black dots) and with temperature increase < 1°C (black squares). |
Discussion
SCS led to a continuous, significant increase in skin temperature in most patients. However, responses varied. Post hoc analysis indicated that only some patients experienced a clinically meaningful rise. These responders also showed better long-term outcomes.
The differential response may be explained by variation in sympathetic nerve function and damage. Animal studies suggest that SCS induces peripheral vasodilation not only via regional sympathetic inhibition,22,23 but also through antidromic depolarization of sensory C- and A-delta fibers.24–26 These fibers release calcitonin gene-related peptide (CGRP), which stimulates nitric oxide production in endothelial cells, promoting vasodilation.26
While these mechanisms are well documented, direct links between sympatholysis and analgesia remain unproven. Pain relief via SCS is thought to involve spinal and supraspinal mechanisms, including GABA release27,28 and modulation of nociceptive signaling via microglia and serotonergic pathways.29
Clinical data on thermographic effects of SCS are sparse. Augustinsson et al (1985) reported increased skin temperature in vascular patients. Robaina et al (1989) observed similar effects in a mixed cohort including CRPS and Raynaud’s. Velasco et al (2009) reported temperature increases with motor cortex stimulation in neuropathic pain.30–32 However, Devulder et al (1996) found no temperature change in a thermography study involving post-laminectomy patients.20 Our methodology differed in terms of measurement site, duration, and pre-conditioning, which may explain these discrepancies.
The study design and sample size do not allow for confirmatory statistical analysis. Although our sample was small, it was representative of our treatment population. Infrared thermography proved to be a reliable, non-invasive tool, independent of subjective factors, with potential value in SCS evaluation.
Conclusion
Our findings suggest that a skin temperature increase ≥1°C following SCS may indicate favorable long-term outcomes in patients with neuropathic pain. Infrared thermography may offer an objective clinical marker. Further studies are needed to determine sensitivity, specificity, and underlying mechanisms.
Acknowledgment
During the preparation of this work the authors used ChatGPT in order to edit the translation After using this tool/service, the author(s) reviewed and edited the content as needed and takes full responsibility for the content of the published article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. North RB, Kidd DH, Lee MS, Piantodosi S. A prospective, randomized study of spinal cord stimulation versus reoperation for failed back surgery syndrome: initial results. Stereotact Funct Neurosurg. 1994;62(1–4):267–272. doi:10.1159/000098631
2. Kemler MA, Barendse GA, van Kleef M, Egbrink MG. Pain relief in complex regional pain syndrome due to spinal cord stimulation does not depend on vasodilation. Anesthesiology. 2000;92(6):1653–1660. doi:10.1097/00000542-200006000-00024
3. de Vos CC, Meier K, Zaalberg PB, et al. Spinal cord stimulation in patients with painful diabetic neuropathy: a multicentre randomized clinical trial. Pain. 2014;155(11):2426–2431. doi:10.1016/j.pain.2014.08.031
4. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz high-frequency therapy (HF10 therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi:10.1097/ALN.0000000000000774
5. Shanthanna H, Eldabe S, Provenzano DA, et al. Evidence-based consensus guidelines on patient selection and trial stimulation for spinal cord stimulation therapy for chronic non-cancer pain. Reg Anesth Pain Med. 2023;48(6):273–287. doi:10.1136/rapm-2022-104097
6. Meier PM, Zurakowski D, Berde CB, Sethna NF. Lumbar sympathetic blockade in children with complex regional pain syndromes: a double blind placebo-controlled crossover trial. Anesthesiology. 2009;111(2):372–380. doi:10.1097/ALN.0b013e3181aaea90
7. Rocha Rde O, Teixeira MJ, Yeng LT, et al. Thoracic sympathetic block for the treatment of complex regional pain syndrome type I: a double-blind randomized controlled study. Pain. 2014;155(11):2274–2281. doi:10.1016/j.pain.2014.08.015
8. Sun H, He M, Pang J, Guo X, Huo Y, Ma J. Continuous lumbar sympathetic blockade enhances the effect of lumbar sympatholysis on refractory diabetic neuropathy: a randomized controlled trial. Diabetes Ther. 2020;11(11):2647–2655. doi:10.1007/s13300-020-00918-7
9. Makharita MY, Amr YM, El-Bayoumy Y. Effect of early stellate ganglion blockade for facial pain from acute herpes zoster and incidence of postherpetic neuralgia. Pain Physician. 2012;15(6):467–474.
10. Jivegard LE, Augustinsson LE, Holm J, Risberg B, Ortenwall P. Effects of spinal cord stimulation (SCS) in patients with inoperable severe lower limb ischaemia: a prospective randomised controlled study. Eur J Vasc Endovasc Surg. 1995;9(4):421–425. doi:10.1016/S1078-5884(05)80010-3
11. Mannheimer C, Eliasson T, Augustinsson LE, et al. Electrical stimulation versus coronary artery bypass surgery in severe angina pectoris: the ESBY study. Circulation. 1998;97(12):1157–1163. doi:10.1161/01.cir.97.12.1157
12. Norrsell H, Eliasson T, Mannheimer C, et al. Effects of pacing-induced myocardial stress and spinal cord stimulation on whole body and cardiac norepinephrine spillover. Eur Heart J. 1997;18(12):1890–1896. doi:10.1093/oxfordjournals.eurheartj.a015197
13. Klomp HM, Spincemaille GH, Steyerberg EW, Habbema JD, van Urk H. Spinal-cord stimulation in critical limb ischaemia: a randomised trial. Lancet. 1999;353(9158):1040–1044. doi:10.1016/s0140-6736(98)05069-7
14. Lobov GI, Gerasimenko YP, Moshonkina TR. Mechanisms of blood flow regulation in the skin during stimulation of the spinal cord in humans. Doklady Biol Sci. 2019;485(1):27–29. doi:10.1134/s0012496619020030
15. Salavatian S, Ardell SM, Hammer M, Gibbons DD, Armour JA, Ardell JL. Thoracic spinal cord neuromodulation obtunds dorsal root ganglion afferent neuronal transduction of the ischemic ventricle. Am J Physiol Heart Circulatory Physiol. 2019;317(5):H1134–H1141. doi:10.1152/ajpheart.00257.2019
16. Wasner G, Schattschneider J, Heckmann K, Maier C, Baron R. Vascular abnormalities in reflex sympathetic dystrophy (CRPS I): mechanisms and diagnostic value. Brain. 2001;124(Pt 3):587–599. doi:10.1093/brain/124.3.587
17. Kemler MA, de Vet HC, Barendse GA, van den Wildenberg FA, van Kleef M. Effect of spinal cord stimulation for chronic complex regional pain syndrome Type I: five-year final follow-up of patients in a randomized controlled trial. J Neurosurg. 2008;108(2):292–298. doi:10.3171/JNS/2008/108/2/0292
18. Ubbink DT, Spincemaille GH, Prins MH, Reneman RS, Jacobs MJ. Microcirculatory investigations to determine the effect of spinal cord stimulation for critical leg ischemia: the Dutch multicenter randomized controlled trial. J Vasc Surg. 1999;30(2):236–244. doi:10.1016/s0741-5214(99)70133-3
19. Ather M, Di Vadi P, Light D, Wedley JR, Hamann WC. Spinal cord stimulation does not change peripheral skin blood flow in patients with neuropathic pain. Eur J Anaesthesiol. 2003;20(9):736–739. doi:10.1097/00003643-200309000-00010
20. Devulder J, Duprez D, De Laat M, Rolly G. Epidural spinal cord stimulation does not improve microvascular blood flow in neuropathic pain. Angiology. 1996;47(12):1145–1149. doi:10.1177/000331979604701204
21. Naar J, Jaye D, Linde C, et al. Effects of spinal cord stimulation on cardiac sympathetic nerve activity in patients with heart failure. Pacing Clin Electrophysiol. 2017;40(5):504–513. doi:10.1111/pace.13050
22. Linderoth B, Fedorcsak I, Meyerson BA. Peripheral vasodilatation after spinal cord stimulation: animal studies of putative effector mechanisms. Neurosurgery. 1991;28(2):187–195. doi:10.1227/00006123-199102000-00003
23. Linderoth B, Herregodts P, Meyerson BA. Sympathetic mediation of peripheral vasodilation induced by spinal cord stimulation: animal studies of the role of cholinergic and adrenergic receptor subtypes. Neurosurgery. 1994;35(4):711–719. doi:10.1227/00006123-199410000-00018
24. Hilton SM, Marshall JM. Dorsal root vasodilatation in cat skeletal muscle. J Physiol. 1980;299(1):277–288. doi:10.1113/jphysiol.1980.sp013124
25. Wu M, Linderoth B, Foreman RD. Putative mechanisms behind effects of spinal cord stimulation on vascular diseases: a review of experimental studies. Autonomic Neurosci. 2008;138(1–2):9–23. doi:10.1016/j.autneu.2007.11.001
26. Wu M, Komori N, Qin C, Farber JP, Linderoth B, Foreman RD. Sensory fibers containing vanilloid receptor-1 (VR-1) mediate spinal cord stimulation-induced vasodilation. Brain Res. 2006;1107(1):177–184. doi:10.1016/j.brainres.2006.05.087
27. Cui JG, O’Connor WT, Ungerstedt U, Linderoth B, Meyerson BA. Spinal cord stimulation attenuates augmented dorsal horn release of excitatory amino acids in mononeuropathy via a GABAergic mechanism. Pain. 1997;73(1):87–95. doi:10.1016/s0304-3959(97)00077-8
28. Linderoth B, Stiller CO, Gunasekera L, O’Connor WT, Ungerstedt U, Brodin E. Gamma-aminobutyric acid is released in the dorsal horn by electrical spinal cord stimulation: an in vivo microdialysis study in the rat. Neurosurgery. 1994;34(3):484–488. discussion 488–9. doi:10.1227/00006123-199403000-00014
29. Joosten EA, Franken G. Spinal cord stimulation in chronic neuropathic pain: mechanisms of action, new locations, new paradigms. Pain. 2020;161 Suppl 1(1):S104–S113. doi:10.1097/j.pain.0000000000001854
30. Augustinsson LE, Carlsson CA, Holm J, Jivegard L. Epidural electrical stimulation in severe limb ischemia. Pain relief, increased blood flow, and a possible limb-saving effect. Ann Surg. 1985;202(1):104–110. doi:10.1097/00000658-198507000-00017
31. Robaina FJ, Dominguez M, Diaz M, Rodriguez JL, de Vera JA. Spinal cord stimulation for relief of chronic pain in vasospastic disorders of the upper limbs. Neurosurgery. 1989;24(1):63–67. doi:10.1227/00006123-198901000-00010
32. Velasco F, Carrillo-Ruiz JD, Castro G, et al. Motor cortex electrical stimulation applied to patients with complex regional pain syndrome. Pain. 2009;147(1–3):91–98. doi:10.1016/j.pain.2009.08.024
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Smart Processing and Intelligent Navigation for Evaluation (SPINE): Comparing Clinicians and AI Language Model (GPT-4) in Spinal Cord Stimulation Candidate Selection
Lo Bianco G, Therond A, D’angelo FP, Kapural L, Diwan S, Staats P, Li S, Christo PJ, Deer TR, Robinson CL
Journal of Pain Research 2026, 19:559514
Published Date: 17 January 2026