Back to Journals » Vascular Health and Risk Management » Volume 19
Effect of Some Risk Factors on Over-Anticoagulation Disorders and Bleeding in Patients Receiving Anticoagulant Therapy with Overdosage of Vitamin K Antagonist
Authors Dung Chu S ![]() , Thi Tran M
, Thi Tran M
Received 19 July 2023
Accepted for publication 5 October 2023
Published 18 October 2023 Volume 2023:19 Pages 663—672
DOI https://doi.org/10.2147/VHRM.S410497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Si Dung Chu,1,2 Minh Thi Tran2
1Haiphong - Vinhbao International General Hospital, Hai Phong City, Vietnam; 2Internal Medicine Department, Vietnam University of Traditional Medicine, Hanoi Capital, Vietnam
Correspondence: Si Dung Chu, Department of Internal Medicine, Vietnam University of Traditional Medicine, Hanoi, Vietnam, Tel +84 906086168, Email [email protected]
Objective: Study on effect of risk factors on over-anticoagulation in patients taking anticoagulant drugs with VKAs (vitamin K antagonists).
Methods: Cross-sectional descriptive, prospective research. Study on 79 patients taking anticoagulant drugs with VKAs who had an INR (International Normalized Ratio) index of more than indicated anticoagulation dose with VKAs therapy.
Results: A total of 79 patients, mean age 65.65 ± 12.17 years [33:85], the elderly group is common (73.4%). Patients had hemorrhage disorders account for 22.8%. The INR index had an average value was 5.88 ± 3.0 [3.02– 23.95]; The INR> 5 level group is a higher risk of bleeding than the INR ≤ 5 level group, it’s the statistical significance (p < 0.001). The risk factors such as drugs to treat dyslipidemia, hyperthyroid, amiodarone, beta blocker, prednisone, NSAIDs (Non-steroidal anti-inflammatory), BMI (Body Mass Index), smoke and alcohol that the risk factors of increasing of bleeding when receiving anticoagulants but it’s not statistically significant yet (OR > 1, p > 0.05); These patients using coenzyme Q10 and green vegetable nutrition such as cruciferous vegetables (Brassicaceae, Asteraceae) are quite common (31.6% and 35.4%), its effect on coagulation with vitamin K and cause of the increased in risk of bleeding was statistical significantly with OR = 5.28 (CI: 1.72– 16.17, p < 0.01), and OR = 2.99 (CI: 1.01– 8.80, p < 0.05) respectively.
Conclusion: Most patients in over-anticoagulation were the elderly group. Patients had hemorrhage disorders account for 22.8%. The INR> 5 level group was a higher risk of bleeding than the INR ≤ 5 level group with statistical significance. Patients using Coenzyme Q10 and green vegetable nutrition such as cruciferous vegetables (Brassicaceae, Asteraceae) are quite common, its effect on coagulation and cause of the increased risk of bleeding complication with statistical significance.
Keywords: risk factors, bleeding, VKAs overdose, INR
Introduction
The most important problem that we were faced during VKAs (vitamin K antagonists) anticoagulant drugs treatment to prevent thromboembolic complications is coagulation disorders even such as over-anticoagulant or bleeding can occur.1–3 When complications occur, it is a medical emergency accounting for about 11% of cases4 or more.2,3,5 Many cases of late arrival or late detection can lead to severe blood loss, hemodynamic instability, hemorrhagic shock, and even hemorrhagic stroke5–7 requiring both resuscitation and intervention and/or emergency surgery.3,4,8,9
Our hospital is an International General Hospital founded in 2020 in Vietnam has been put into operation and has quickly provided medical examination and treatment to serve people in the community from many domestic and international regions. In the past time, there have been many cases of medical examination and treatment with coagulation disorders requiring timely emergency treatment, of which the majority of patients were taking anticoagulants with VKAs and stem from many causes. Factors that lead to blood clotting disorders. Vitamin K anticoagulants are drugs used to treat cardiovascular diseases that cause embolism to prevent thromboembolic complications caused by atrial fibrillation, valve disease is an artificial heart valve, prevention of thromboembolic complications and pulmonary embolism in hip surgery;9–11 However, along with such benefits, the use of anticoagulants also often has side effects, including coagulation disorders, the most common manifestation of which is bleeding complications, bleeding may occur, occurs throughout the body such as the central nervous system, extremities, visceral organs, intra-abdominal, intraocular, subcutaneous, etc. Sometimes diarrhea and joint pain occur individually. In some cases, signs of vasculitis, liver damage, hair loss, localized skin necrosis, allergic skin rashes may occur.2,12–14 Vietnam has also had a number of studies on this topic, However, in order to study in depth the factors affecting blood clotting disorders, there are still quite a few studies and there are still many great unknowns related to the process of blood clotting disorders that are still open in the world.2,12–15 Therefore, we conducted this study with the main objective of “Study on the factors affecting the coagulation disorder and bleeding risk in patients with overdosage of vitamin K antagonist anticoagulants”.
Materials and Method
Participant
Study on 79 patients who were diagnosed with blood clotting disorders over-anticoagulation drugs when they come to outpatient medical examination and treatment at the Haiphong-Vinhbao International General Hospital in Vietnam during the period from February 2021 to November 2022.
Patients receiving anticoagulant therapy with VKAs who had an INR (International Normalized Ratio) above the required threshold are assessed by the INR test, with the usual target range from 2.5 to 3.5 in patients who had mechanical heart valve replacement, and 2.0–3.0 for the remaining cases. Patients adhere to the dose and time of INR testing periodically every 4 weeks. An overdose of anticoagulants (INR > 3.5 for patients with prosthetic heart valves and INR > 3.0 in the rest) can cause bleeding or doses that are too low to work can have no effective.3,4,10
Research Design and Population
Research design
Cross-sectional descriptive and prospective study.
Research Population
The sample size formula was applying the formula for calculating sample size for cross-sectional descriptive research.4

N is the sampling size; p (prevalence) is the population proportion (select P = 11%);5 d is the margin of error (confidence interval): 0.1;4,5 α (Level of error): 0.05; Z-value is 1.96. We calculate the sample size according to the above formula to get the result is n = 37, to increase the accuracy, we duplicated the sample size above to get a sample size of N = 74.
Research Data Processing
The collected data was analyzed on a computer using the IBM SPSS 23.0 software program.
Continuous variables (Age, BMI, INR index) are expressed mean (Median or SD - standard deviation, interquartile range - IQR) and calculate the categorical variables as independent variables as follow: The Age with two group: “Elderly group” (being 60 years or older) or “young group” (under 60 years); BMI with two group: “Obesity group” or “Non-obesity group”; INR level with two groups: “INR index > 5.0 level” or “INR index ≤ 5.0 level”. And other variables are as follows: gender (male, female), bleeding complications (Yes or None), using coenzyme Q10, cruciferous vegetables (Brassicaceae, Asteraceae), drugs to treat dyslipidemia, hyperthyroid drug, amiodarone, beta blockers, prednisone, nonsteroidal anti-inflammatory drugs, smoking, alcohol. All have two values are “Yes” or “None”. The analysis was performed to determine independent predictors on effects of risk factors: Chi-Square Test of Independence assesses associations between independent variables (risk factors) and dependent variables (bleeding complications).
Use odds ratio analysis OR (OR: Odds ratio – compares the odds of the outcome between one exposure group and a second exposure group) with the 95% confidence interval (CI: 95%). Statistically significant < 0.05 was used to evaluate the significant relationship in the analyzed statistics.16,17
- If OR > 1, the risk factor increases the likelihood of having a disease compared with the possibility of not having a disease.
- If OR = 1, there is no association between the risk factor and the likelihood of disease.
- If OR < 1, then risk factors can reduce the likelihood of having a disease compared with the possibility of not having a disease.3,5,12
Result
General Characteristics and Clinical Characteristics in the Study Group
Basic Characteristics
The results of the basic characteristics of this research (Table 1) showed that the mean age is 65.65 ± 12.17 years, the oldest patient is 85-year-old and the youngest is 33-year-old. The young group accounted for 21/79 (26.6%) and the elderly group accounted for 58/79 (73.4%) with p > 0.05. Male group is 25 patients (31.6%) and female group is 54 patients (68.4%) with p > 0.05. The average value of INR was 5.88 ± 3.0 [range 3.02 to 23.95]. The group with an INR level > 5 has a high risk of bleeding is 41/79 patients (51.9%), while the group with an INR level ≤5 has a low risk of bleeding is 38/79 patients (48.1%), showing that the proportion of patients with coagulation disorders was detected with INR levels at the high-risk and low-risk thresholds were similar (p > 0.05). Patient with hemorrhage signs is 18/79 (22.9%), group with INR > 5 has 17/18 patients (94.4%) while group with INR < 5 has 1/18 patients (5.6%) with p = 0.0001 (< 0.001).
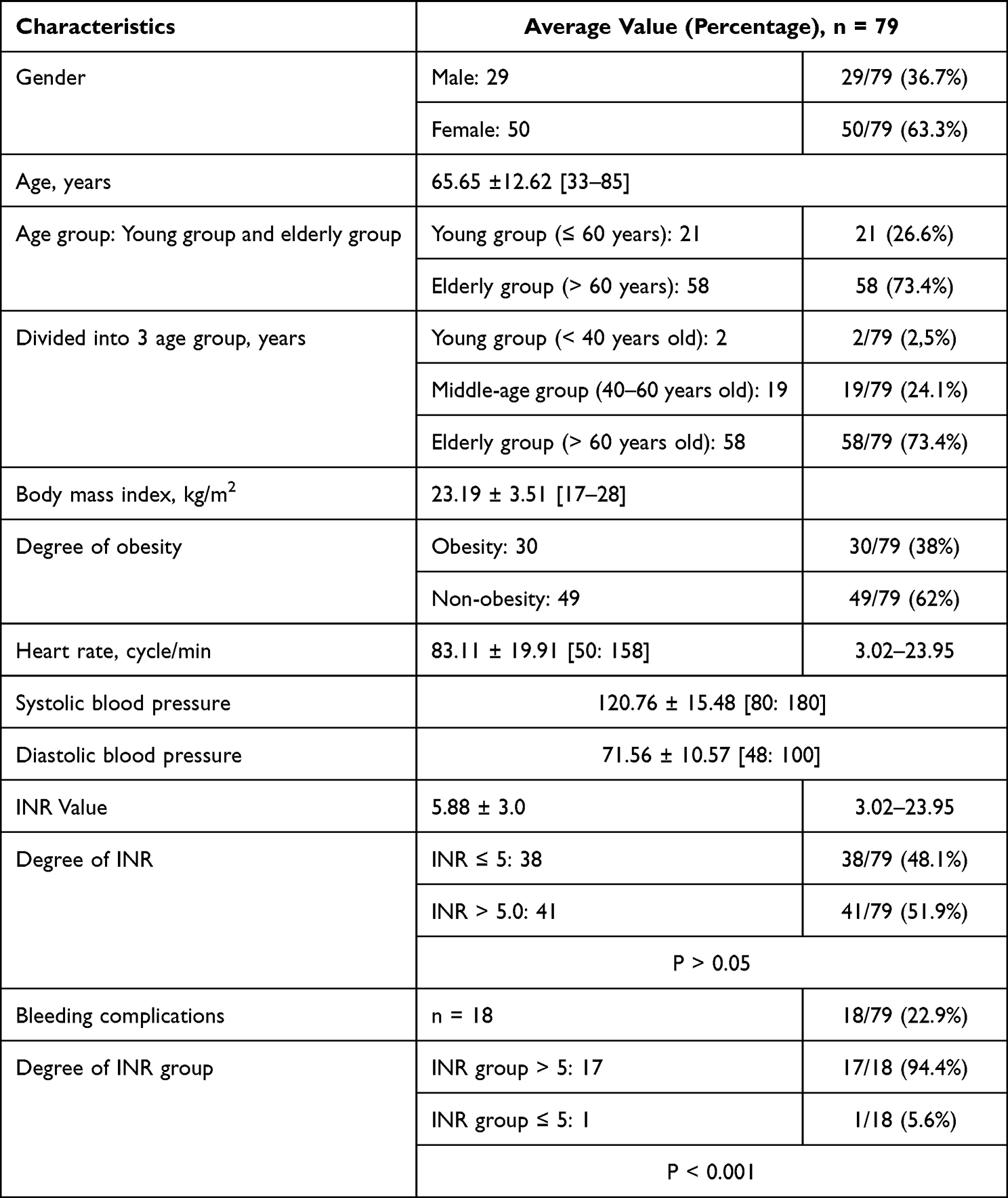 |
Table 1 Basic Characteristics of the Study Group |
Clinical Characteristics
The results about clinical characteristics showed that the most common symptom was shortness of breath found in 14/79 (17.7%), chest palpitations was found in 10/79 (12.7%), chest pain was found in 8/79 (10.1%), swollen joint pain was 11/79 (13.9%), fast heart rate was 5/79 (6.3%), fatigue/weakness was 6/79 (7.9%), nausea/vomiting was 4/79 (5.1%), and shock/dizziness was 3/79 (3.8%). The proportion of patients with bleeding symptoms was 18/79, accounting for 22.8%, of which severe bleeding complications accounted for 6/79 cases (7.6%). Symptoms of bleeding with the main sign of bleeding under the skin accounted for 11/79 (13.9%), bleeding gums accounted for 4/79 (5.1%) and there was one case with nosebleeds due to bleeding; it is quite rare that signs of gastrointestinal bleeding account for 2/79 (2.5%) and subconjunctival hemorrhage occurs in one case accounting for 1.3%. We observed about the main diseases in the study, of the 79 patients surveyed, there are 31 patients with atrial fibrillation (45.6%), 35 patients with heart valve disease has surgery (44.3%), and 8 patients with Heart valve disease without surgery but with atrial fibrillation or heart failure accounted for 10.1%.
Risk Factors
The results (Table 2) showed that the risk factors of the drugs to treat dyslipidemia (68.4%), Beta Blockers (82.3%), Coenzyme Q10 supplements (31.6%) and cruciferous vegetables (35.4%) were the most common.
 |
Table 2 Risk Factors |
The Relationship Between Some Factors and the Risk of Bleeding in Patients Taking Vitamin K Antagonists Anticoagulant
The results in Table 3 show that the risk factors are gender (female), overweight and obesity, smoking, alcohol use or used of drugs to treat dyslipidemia, drugs to treat hyperthyroidism, Cardiac arrhythmias such as amiodarone, beta-blockers, anti-inflammatory drugs (Prednisone, Nonsteroidal anti-inflammatory drug - NSAIDs) have an increased risk of bleeding disorder (OR > 1) but not statistically significant (p > 0.05). However, the use of functional foods that contain Coenzyme Q10 supplements and nutrients from as cruciferous vegetables (Brassicaceae, Asteraceae) in addition to accounting for a fairly common rate in patients with coagulopathy, the Coenzyme Q10 supplements and nutrients from cruciferous vegetables also shows two risk factors of increased risk of bleeding with odds ratio OR (OR > 1) of 5.28 and 2.99, respectively, were statistical significance with p < 0.05.
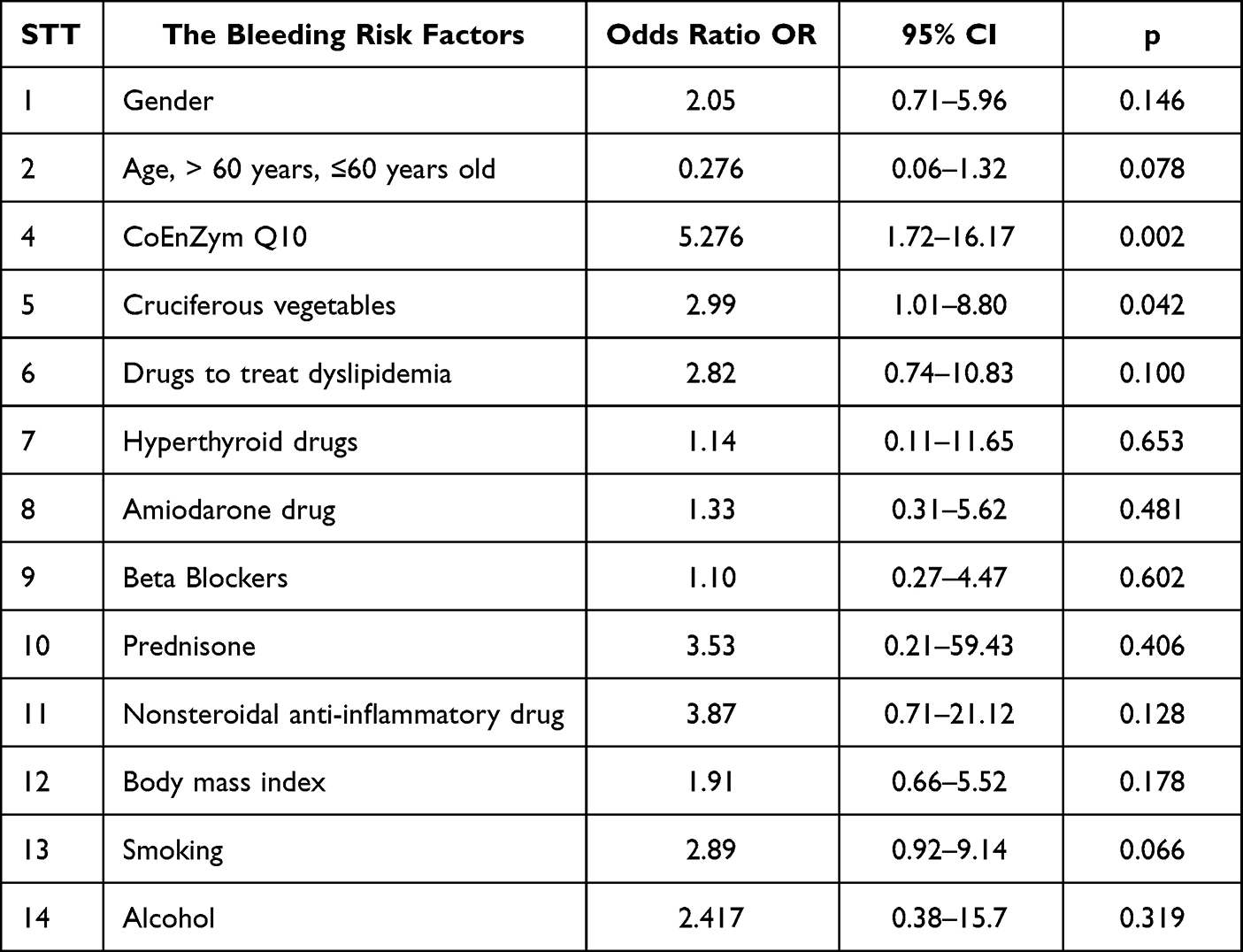 |
Table 3 Relationship Between Some Factors and the Risk of Bleeding |
Discussion
General Characteristic and Clinical Characteristics in the Study Group
Basic Characteristics
The results indicated that the majority of patients in our study belong to the elderly group (Table 1) which is quite consistent with the research of other authors as the majority of patients fall into the elderly group, although the average age in many studies has an average age. The average is higher in our study because most of these countries have a higher life expectancy than Vietnam.8,14,15 Our study had a rather high percentage of women compared with men but it’s no statistically significant (p > 0.05). Some studies show that men are taller than women but the difference is not statistically significant; Gualtiero P (1996) shows a roughly equal ratio of men to women (43.0% of women while men have a higher proportion of 57.0%),3 Connolly S shows a higher proportion of men than women but it was not significantly different.8
Results of our research showing that the proportion of clinical cases with coagulation disorders was detected with INR levels at the high-risk of bleeding (INR level > 5) and low-risk thresholds (INR level ≤5) were similar (p > 0.05). Most of the patients accounting for 17/18 (94.4%) with signs of bleeding were in the group with INR > 5, while there was also 1 case of bleeding with INR = 4.82 in the INR group ≤ 5 (p < 0.001) with subcutaneous hemorrhage at the tips of the toes seen in patient with systolic versus diastolic heart failure from persistent atrial fibrillation pathology is received anticoagulants with VKAs and this time has used cruciferous vegetables for some weeks leading to coagulation disorders and has timely treatment by us when patients come for medical examination and treatment at the hospital (Table 1). Therefore, it is necessary to manage and manage patients well when detecting INR > 5, but for patients with coagulopathy whose index is not too high in the INR ≤ 5 group, it is still necessary to monitor and evaluate their clinical status, ready for timely treatment when there are signs of bleeding.9,10
Clinical Characteristics
The proportion of patients with bleeding symptoms was 22.8%, of which severe bleeding complications accounted for 7.6%. Symptoms of bleeding with the main sign of bleeding under the skin bleeding accounted for 13.9%, bleeding gums accounted for 5.1% and there was one case with nosebleeds due to bleeding thrombocytopenia. It is quite rare that signs of gastrointestinal bleeding account for 2.5% and subconjunctival hemorrhage occurs in one case accounting for 1.3%.
Our study has not encountered any case of cerebral hemorrhage, however, the presence of bleeding under the eye conjunctiva also suggests a high risk of cerebral hemorrhage due to the structure of the cerebral arteries and the structure of blood vessels in the eye have similarities; Connolly SJ (2009) showed a serious complication rate with a hemorrhagic stroke rate of 3.4% and a mortality rate of 4.1% per year in the warfarin group.8
In 2 cases of high gastrointestinal bleeding, there was 1 case of a male patient (85 years old) who was hospitalized with vital signs of fainting, low blood pressure, and black stools due to severe stomach bleeding because the patient took an overdose of vitamin K antagonists on the background of gastritis. Although the INR is not too high (INR = 6.82), there are symptoms of severe gastrointestinal bleeding. Therefore, in addition to the patient’s emergency treatment, severe gastrointestinal bleeding due to gastric ulcer duodenal bulb with PPI regimen intravenous bolus 80 mg, and followed by a continuous intravenous infusion with 8 mg/hour in 72 hours, concurrently with blood transfusion, fresh frozen plasma due to severe blood loss, oxygen through the nose.
The case with the highest INR in this study (INR = 23.95), was seen in a male patient (62 year old) who was admitted to the hospital because of signs of bleeding under the skin in many places along with bleeding in the nose, discovered that the patient was taking anticoagulants and this time was using functional food is CoEnzyme Q10. The patient was treated with emergency and resuscitation, inserted a nose mask first to stop bleeding and used intravenous vitamin K to treat anticoagulant overdose, after treatment, the patient’s blood clotting disorder was stabilized.3,10
The pathological physiology process and causes of increased in bleeding risks were multifactorial.2 They may be direct consequence of an urea-associated to platelet dysfunction, impaired platelet adhesion and aggregation. The glycoprotein IIIa/IIb receptors activation cause of the impaired platelet as well as subsequent glycoprotein binding.4,9,16 Vitamin K is one of the fat-soluble vitamins which are structurally similar and plays an important role for the regulation of blood clotting, which is necessary for the assistance in blood clot. Vitamin K function as a coenzyme for carboxylase which is dependent on vitamin K and required for the synthesis of proteins involved in hemostasis (blood clot), bone metabolism as well as diverse physiological functions. The clotting factor II (Prothrombin) is a plasma vitamin K and dependent protein directly involved in blood clot. Therefore, patients receiving these VKAs anticoagulant must maintain a consistent intake of vitamin K to avoid coagulation disorders.3,4,9
Our study encountered a higher bleeding rate than other studies such as the study of Eichinger S. in 2016 in Austria with a bleeding rate of about 11.0%;4 The result of our study is that this rate is higher because the hospital has a team of Cardiologists with more specialized specialties than neighboring hospitals, so it is easier for patients to choose to come for check-up and follow-up when they have a problem or have an abnormal signs; Furthermore, some patients do not really compliance with the patient’s medication dose, many patients had the habit of using functional foods containing active ingredients Coenzyme Q10 that interact with VKAs drugs; Beside, the surrounding areas had a tradition of growing green vegetables, therefore many patients still habit of using functional foods a lot of green vegetable belong to cruciferous vegetables or Asteraceae vegetables family with rich in vitamin k, ect. These supplement functional foods as well as these nutritious green vegetables have the effect of interacting with VKAs, this may lead to an upward adjustment of the anticoagulation dose according to the INR index which can be affected to difficulty controlling anticoagulant dose and until there is an imbalance or lack of the above factors that easily cause blood disorders. Its are a number of factors as a possible risk factor for the increase the likelihood of blood disorders and bleeding risk.
The research of Wysowski DK author for used of warfarin has increased in bleeding from warfarin taking is a prevalent reaction and very important cause of mortality such as a review article published (2001, USA) showed that the incidence of major bleeding in people indicated warfarin range from 0.0% to 16.0%, and the incidence rate of fatal bleeding was 0.0% to 2.9%. Our data in this study is consistent with literature reports of major bleeding frequencies for warfarin as high as 10.0% to 16.0% (Wysowski DK et al, 2007).5 Our research also showed result as equivalent even in the study of Koutrouvelis et al about the rate of bleeding can be up to 10.0% but in fact, up to 25.0% of patients are likely to bleed at least once per year.9
The main disease to indicate the use of VKAs is mainly atrial fibrillation, with atrial flutter accounting for 45.6%, a valvular disease with heart valve has surgery also accounts for 44.3%, the rest is The group of valvular heart valve disease without heart valve surgery but with atrial fibrillation or heart failure accounted for 10.1%.3,9,16 Our study has a higher rate of people with atrial fibrillation and heart valvular disease than some other studies such as Koutrouvelis et al found 35.0% of patients with atrial fibrillation and 20.0% of patients with valvular disease had surgery.11,16 Many doctors have thought that the use of Coenzyme Q10 in the cardiovascular disease will help them get better, so there is a habit of using coenzyme q10 in these patients. Normally, a diet rich in green vegetables is also good for patients with cardiovascular disease, However, we are also need to be careful in the drug interactions.
Risk Factors (Table 2)
The proportion of patients using CoEnzyme Q10 is quite common (31.6%), indicating that the occurrence of clotting disorders is quite common in people being treated with anticoagulants with VKAs along with functional foods contains the active ingredient coenzyme Q10.18,19 The number of patients using cruciferous vegetables (Brassicaceae, Asteraceae) is also quite common (35.4%), this is a nutritious food group with a lot of vitamin K, in which mainly cabbage, broccoli, lettuce; It is shown that in patients using anticoagulants, blood clotting disorders with high INR are quite common in patients who have a habit of eating green vegetables such as cruciferous vegetables.13,14,20
The Relationship Between Some Factors and the Risk of Bleeding in Patients Taking Vitamin K Antagonists Anticoagulant
The results in Table 3 show that the most risk factors have an increased in risk of bleeding with OR > 1 but not statistically significant on the sample size for this study (p > 0.05), perhaps a larger sample size study is needed for these risk factors. However, the use of functional foods that contain Coenzyme Q10 supplement and nutrients from as cruciferous vegetables (Brassicaceae, Asteraceae family…) accounted for a fairly common rate in patients with coagulopathy, also shows a risk of increased risk of bleeding with OR > 1 of 5.28 and 2.99, respectively, were statistically significant (p < 0.05). This proves that there is indeed a causal relationship between the use of dietary supplements containing Coenzyme Q10 and cruciferous vegetables for coagulation disorders and a high risk of bleeding due to an overdose of anticoagulants.
Vitamin K is a fat-soluble vitamin essential for a synthesis parameter of many factors on the coagulation cascade such as the Factors II, VII, IX, and X which are all very important for the intrinsic and common pathways of coagulation. Vitamin K is also protein synthesized in with cells make proteins including the Protein C, Protein Z, Protein S, and anticoagulation proteins that degrade specific coagulation factors, preventing excessive thrombosis. Therefore, in the case patients have a Vitamin K deficiency is associated with impaired coagulation function and excessive bleeding and hemorrhage; This can be cause by poor diet, malabsorption in the intestines, or liver failure, even there is an imbalance between the dosage of anticoagulant drugs and the added other factors. The process affects an enzyme is called tenase, and converts prothrombin to thrombin, beside that Calcium and phospholipids are required cofactors for prothrombin activation enzyme complexes to function.1,2,4
Our study also showed that some patients using VKAs when using supplements containing CoEnzymQ10 active ingredient are prone to high INR and at risk of severe bleeding complications. CoEnzymQ10 is a fat-soluble compound, is a dietary supplement containing the main ingredient Ubidecarenon also known as ubiquinone, which is an endogenous coenzyme structurally similar to vitamin K, Ubidecarenone has many functions, where it is an essential component of electron transport and energy production (ATP) chain processes; CoEnzymQ10 neutralizes free radicals, so it has a very effective antioxidant effect; It is involved in cellular energy production, so it plays an important role in energy metabolism. These properties help protect cells and prevent and aid in the treatment of a number of chronic diseases. Coenzyme Q10 has been shown to improve heart health and blood sugar regulation, aid in cancer prevention and treatment, and relieve migraines, it may also reduce oxidative damage that leads to fatigue muscle, skin damage, and brain and lung diseases. Coenzyme Q10 supplements alone or in combination with nutrients can prevent or support the treatment of some diseases. So this product has many health benefits, so it is also widely used. However, for patients who use anticoagulants with vitamin K, because Coenzyme Q10 has similar properties to a vitamin with a structure similar to vitamin K, it will cause drug interactions, reducing the effect of anticoagulants K, this invisibly leads to the need to increase the dose of anticoagulants vitamin K to achieve the dose or adjust the increase or decrease erratically according to the INR index, more difficult to control in anticoagulation dose adjustment, when there is an imbalance in the number of anticoagulants. Coenzyme Q10 put into the body will easily cause coagulation disorders, including bleeding complications with an elevated INR. It is recommended to be cautious and not to use the active ingredient ConEnzyme Q10 during treatment with VKAs because it is easy to cause coagulation disorders and high risk for hemorrhagic complications.18,19
The study also showed that patients who consumed cruciferous vegetables (Brassicaceae, Asteraceae family) while taking VKAs were also more linked to experience high INR index and also had an increased risk of major bleeding complications. Classical studies also indicated that Vitamin K is a nutritious vitamin found in a variety of green leafy vegetables such as cabbage, mustard greens, brassica juncea (Chinese mustard greens), broccoli, and brussel sprouts, and cauliflower, all belonging to the Brassicaceae family;13,14 Similar to other green leafy vegetables such as green vegetables of the daisy family (Asteraceae) are common lettuce, chrysanthemum, similar to cruciferous vegetables and also contain a lot of vitamin K including bleeding disorders with high INR. Some patients were advised to avoid cruciferous vegetables, but they did not find out in fact all the green vegetables that belong to this family. Besides, it should also be noted that some vegetables such as lettuce, and chrysanthemum, although belonging to the daisy family, it is close to the cruciferous family and also gives similar drug interactions for VKAs anticoagulants.20,21
Therefore, when appointing patients to take anticoagulants, and vitamin K antagonists, it is necessary to avoid dietary supplements containing the active ingredient CoenzymeQ10 in it. For nutritional foods, it is necessary to carefully consult the foods belonging to the group of cruciferous vegetables, including other foods containing the vitamin K component. On the other hand, the response to anticoagulants is also related to the intravascular volume, diet, food intake, vitamin K deficiency, drug interactions, changes in drug metabolism, and patient adherence.13,15
Finally, the need for close clinical monitoring as well as the need to adjust the dose during the treatment of each patient in order to control the INR within safe limits for treatment and prevention of thrombosis is extremely important, patients need to be regularly checked and monitored for blood clotting function during monitoring and treatment.
Conclusion
The mean age of all patients mostly in elderly group with an average age of 65.65 ± 12.17 [33:85]. Men (31.6%) had a lower rate than women (68.4%) but there is no statistically significant difference (p > 0.05). The proportion of patients with bleeding signs accounted for 22.8% and severe bleeding complications accounted for 7.6%. The average value of INR was 5.88 ± 3.0 [3.02–23.95]. There was no difference between the group with INR level > 5 and the group with INR level ≤5, p > 0.05. The high-risk INR group (INR > 5) causing coagulopathy and higher risk of bleeding than the low-risk INR group (INR ≤ 5) with significantly (p < 0.001).
Many factors affect the risk in bleeding complications, in which the use of supplements containing Coenzyme Q10 and nutritional foods from the cruciferous green vegetables (Brassicaceae, Asteraceae) are quite common in patients with coagulation disorders; both factors can affect coagulation disorders such as an increase the risk in bleeding complications, this is statistically significant with OR = 5.28 (CI: 1.72–16.17, p < 0.001) and OR = 2.99 (CI: 1.01–8.80, p < 0.05), respectively.
Limitations and Recommendations
The study has shown that the some risk factors are affected bleeding risk by mathematical statistics through the research, but the sample size is still not big enough, so it has not revealed all the other risk factors maybe that have been statistically significant, if the sample size is larger, it is possible to detect some more factors that have a statistically significant influence.
Abbreviations
VKAs, Vitamin K antagonist anticoagulants; INR, International Normalized Ratio; BMI, Body Mass Index; OR, Odds ratio; CI, Confidence interval; P, Prevalence; NSAID, Nonsteroidal anti-inflammatory drug.
Data Sharing Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Ethical Statement
The authors confirmed that the guidelines outlined in the Declaration of Helsinki were followed. Informed consent was obtained from each participant. The study protocol was previously approved by Haiphong-Vinhbao International General Hospital’s Ethics committee for research on humans (Number of the ethical approval in research: 45a/QD-DKQTVB).
Acknowledgment
The authors are grateful to the Internal Medicine Department - Vietnam University of Traditional Medicine and Haiphong–Vinhbao General Hospital in Vietnam for their assistance and data collect.
Author Contributions
All authors contributed to data analysis, revised the manuscript, drafting or revised the article during the review process, agreed on the journal to which the manuscript will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vos M, Esposito G, Edirisinghe JN, et al. Vitamin K2 is a mitochondrial electron carrier that rescues pink1 deficiency. Science. 2012;336(6086):1306–1310. doi:10.1126/science.1218632
2. Watson HG, Baglin T, Laidlaw SL, et al. A comparison of the effectiveness and rate of response to oral and intravenous Vitamin K in reversal of over-anticoagulation with warfarin. Br J Haematol. 2001;115(1):145–149. doi:10.1046/j.1365-2141.2001.03070.x
3. Palareti G, Leali N, Cocheri S, et al. Bleeding complications of oral anticoagulation treatment: an inception – cohort, prospective collaborative study (ISCOAT). Italian study on complications of oral anticoagulant therapy. Lancet. 1996;348(9025):423–428. doi:10.1016/S0140-6736(96)01109-9
4. Eichinger S. Reversing vitamin K antagonists: making the old new again. Am Soc Hematol. 2016;1(1):605–611. doi:10.1182/asheducation-2016.1.605
5. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167(13):1414–1419. doi:10.1001/archinte.167.13.1414
6. Steffel J, Collins R, Antz M, et al. The 2021 European heart rhythm Association practical guide on the use of non – vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: executive summary. Europace. 2021;23(10):1612–1676. doi:10.1093/europace/euab065
7. Shah M, Tsadok MA, Jackevicius CA, et al. Warfarin use and the risk for stroke and bleeding in patients with atrial fibrillation undergoing dialysis. Circulation. 2014;129(11):1196–1203. doi:10.1161/CIRCULATIONAHA.113.004777
8. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–1151. doi:10.1056/NEJMoa0905561
9. Koutrouvelis A, Abouleish A, Indrikovs A, et al. Case scenario: emergency reversal of oral anticoagulation. Anesthesiology. 2010;113(5):1192–1197. doi:10.1097/ALN.0b013e3181f7a7a3
10. Gunther GE, Conway G, Leibach L, et al. Low-dose oral vitamin K is safe and effective for outpatient management of patients with an INR>10. Thromb Res. 2004;113(3–4):205–209. doi:10.1016/j.thromres.2004.03.004
11. Bhatia HS, Hsu JC, Kim RJ. Atrial fibrillation and chronic kidney disease: a review of options for therapeutic anticoagulation to reduce thromboembolism risk. Clin Cardiol. 2018;41(10):1395–1402. doi:10.1002/clc.23085
12. Lee J, Kim BJ, Kim E, et al. Dissipation kinetics and the pre-harvest residue limits of acetamiprid and chlorantraniliprole in kimchi cabbage using ultra-performance liquid chromatography-tandem mass spectrometry. Molecules. 2019;24(14):2616. doi:10.3390/molecules24142616
13. O’Sullivan SM, Galvin K, Heneghan C, et al. Does daily consumption of vitamin K1 from cruciferous vegetables reach the circulation and the knee joint? Proc Nutr Soc. 2018; 77: E68.
14. Kurosu M, Began E. Vitamin K2 in electron transport system: are enzymes involved in vitamin k2 biosynthesis promising drug targets? Molecules. 2010;15(3):1531–1553. doi:10.3390/molecules15031531
15. Davis E, Darais D, Fuji K, et al. Prescribing and safety of direct-acting oral anticoagulants compared to warfarin in patients with atrial fibrillation on chronic hemodialysis. Pharmacy. 2020;8(1):37. doi:10.3390/pharmacy8010037
16. Aktan A, Güzel T, Aslan B, et al. Comparison of the real-life clinical outcomes of warfarin with effective time in therapeutic range and non-vitamin K antagonist oral anticoagulants: insight from the AFTER-2 trial. Cardiol Pol. 2023;81(2):132–140.
17. Aktan A, Guzel T, Arslan B, et al. The effect of COVID-19 pandemic on time in therapeutic range in patients using warfarin. Int J Cardiovasc Acad. 2022;8(1):20. doi:10.4103/ijca.ijca_54_21
18. Fotino A, Thompson-Paul AM, Bazzano LA. Effect of coenzyme Q10 supplementation on heart failure: a meta-analysis. Am J Clin Nutr. 2013;97(2):268–275. doi:10.3945/ajcn.112.040741
19. Qu H, Guo M, Chai H, et al. Effects of coenzyme Q10 on statin-induced myopathy: an updated meta-analysis of randomized controlled trials. J Am Heart Assoc. 2018;7(19):e009835. doi:10.1161/JAHA.118.009835
20. Ashirova ZB, Kuzhantaeva ZZ, Abdrassulova ZT, et al. Studying phytochemical features of three Asteraceae herbs growing wild in Kazakhstan. Floresta e Ambiente. 2021;28(4):e20210060. doi:10.1590/2179-8087-floram-2021-0060
21. Michel J, Abb Rani NZ, Husain K. A review on the potential use of medicinal plants from Asteraceae and Lamiaceae plant family in cardiovascular diseases. Pharmacol. 2020;11(852):1–26.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk of Intracranial Hemorrhage in Persons with Hemophilia A in the United States: Real-World Retrospective Cohort Study Using the ATHNdataset
Hu J, Chandler M, Manuel CM, Caicedo J, Denne M, Ewenstein B, Mokdad AG, Xing S, Recht M
Journal of Blood Medicine 2024, 15:191-205
Published Date: 24 April 2024
The Value of Using Bedside Point of Care Testing for International Normalized Ratio in Patients on Warfarin Undergoing Dental Procedures and Bleeding Assessment; A Single Center Prospective Study
Albarkheel A, Alshareef H, Albar A, Altbaili SY, Alminaqash MA, Alotibie A, Sheikh A, Alahmadi A, Alaifan B, Tamim H, Owaidah T
Journal of Blood Medicine 2025, 16:337-348
Published Date: 23 July 2025