")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Effect of Sevoflurane on the Deep Neuromuscular Blockade in Obese Patients Undergoing Laparoscopic Sleeve Gastrectomy: A Single Center Prospective Randomized Controlled Study
Authors Shao L, Liu Y, Hao J, Li J , Wang H, Xue FS , Song B, Wan L
Received 22 March 2023
Accepted for publication 29 September 2023
Published 24 October 2023 Volume 2023:17 Pages 3193—3203
DOI https://doi.org/10.2147/DDDT.S413535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Georgios Panos
Liujiazi Shao,1 Yang Liu,2 Junqiang Hao,1 Jiayi Li,1 Hongyu Wang,1 Fu-Shan Xue,1 Bijia Song,1* Lei Wan1*
1Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 2Department of General Surgery, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bijia Song, Email [email protected]; Lei Wan, Email [email protected]
Objective: Our study aimed to demonstrate that the combination of sevoflurane inhalation with continuous intravenous anesthesia can effectively reduce the dosage of muscle relaxants, shorten extubation time under anesthesia while meeting the requirements of laparoscopic deep neuromuscular block (dNMB) in obese patients. Additionally, we sought to assess the potential reduction in postoperative residual muscle relaxants.
Methods: Fifty-nine patients were randomly assigned. Anesthesia-related variables, such as anesthetics dosages, muscle relaxant effective time, clinical muscle relaxant time, muscle relaxant in vivo action time, muscle relaxant recovery time, body movement times, and extubation duration were recorded. Surgery-related variables (the Leiden-Surgical Rating Scale (L-SRS), duration of the procedure) were recorded. Pain was measured using the visual analog scale (VAS) score before leaving the PACU. The duration of the PACU stay and patients’ satisfaction levels in the PACU were also recorded.
Results: Patients who inhaled sevoflurane during the operation required a lower dosage of muscle relaxant to achieve the same deep neuromuscular block (dNMB) effect. The time from stopping the rocuronium pump to T1 recovery of 90% was shorter, and the time for T1 to recover from 25% to 75% was faster among patients who inhaled sevoflurane during the operation. Furthermore, the sevoflurane combined with continuous intravenous anesthesia group exhibited a shorter extubation time for obese patients undergoing laparoscopic bariatric surgery, along with a reduced risk of experiencing hypoxemia and a shorter observation time in the PACU.
Conclusion: Inhaling sevoflurane combined with continuous intravenous anesthesia during the operation effectively reduces the dosage of muscle relaxant required to achieve the same deep neuromuscular block (dNMB) effect. Additionally, this approach significantly shortens the extubation time for obese patients undergoing laparoscopic bariatric surgery and reduces the risk of experiencing hypoxemia, along with reducing the observation time in the PACU.
Keywords: obese, laparoscopy bariatric surgery, rocuronium, sevoflurane, deep neuromuscular block
Introduction
Nowadays, obesity has become an increasingly important problem worldwide, according to a previous study abroad, the prevalence of obesity in adults is 24% in men, and 25% in women, and the prevalence of grade III obesity exceeds 3%.1 Clinically meaningful body weight losses has proven difficult to achieve and especially to maintain through sustained lifestyle change in the form of diet and exercise. Pharmacotherapy against obesity is a non-invasive treatment as an adjunct to lifestyle changes, studies found that long-acting glucagon-like peptide-1 receptor agonists (GLP-1 RAs) liraglutide and semaglutide (a modified version of liraglutide with longer half-life and tripled receptor affinity) could induce significant weight loss and lowering of comorbidities.2,3 Moreover, a strategy combining exercise and liraglutide therapy improved healthy weight loss maintenance more than either treatment alone.4 However, for patients with severe obesity, laparoscopy bariatric surgery is still considered the golden standard in metabolic surgery. Laparoscopic surgery is increasingly widely used in the clinic due to the advantages of small wound, rapid recovery and higher patient satisfaction. For obese patients, establishing pneumoperitoneal access can be challenging as a result of abdominal wall resistance, leading to inadequate exposure.5,6 These obstacles can hinder surgeons from locating appropriate dissection planes, resulting in tissue injury and increased postoperative complications.7,8 Because obesity can increase the possibility of conversion to open surgery, a high BMI is considered a contraindication for laparoscopic surgery.9,10 Therefore, a novel technique alleviating technical difficulties and improving surgical conditions during laparoscopic surgery is required. In order to have a good visualization of the surgical field to operate, deep neuromuscular block (dNMB), which is achieved when there are no responses to train-of-four (TOF) stimulation and one or more responses to post-tetanic count (PTC), is more effective in softening abdominal muscles, reducing the need for high pneumoperitoneum pressure,11 and preventing abdominal muscle contraction, thus reducing the risk of complications associated with surgery. Thus, maintaining “dNMB” in bariatric surgery could help to provide greater space for surgery.
However, anaesthetizing morbidly obese individuals requires careful considerations regarding changes in the pharmacokinetic and pharmacodynamic properties of numerous drugs used in anaesthesia. Physiological and anthropometric changes, such as increases in cardiac output, changes in regional blood flow, and increases in fat mass and lean mass affect pharmacokinetic properties. In addition, respiratory pathophysiology such as the increased incidence of OSA, and fat deposition in the oropharynx and chest wall alter pharmacodynamic properties of anaesthetics. Therefore, it is of great significance to explore better anesthetic compatibility, which can not only meet the requirements of laparoscopic dNMB in obese patients, but also reduce the total dose of muscle relaxant and reduce postoperative residual muscle relaxant and other complications. Among the commonly used muscle relaxants, rocuronium is characterized by rapid effect, long action duration and deep muscle relaxants, which is the best choice for quick induction of endotracheal intubation under general anesthesia.12 Meanwhile, the combination of inhaled anesthetics such as sevoflurane in general anesthesia surgery can also enhance the effect of non-depolarized muscle relaxants, reduce the total dose of muscle relaxants, shorten the postoperative recovery time of patients and reduce the residual muscle relaxation postoperatively.13
Based on the above considerations, we performed a randomized controlled trial comparing total intravenous anesthesia vs inhaling sevoflurane combined with continuous intravenous anesthesia to achieve dNMB on surgical conditions in obese patients undergoing bariatric laparoscopic surgery. Additionally, we addressed the issue of patient recovery outcomes and detect a difference of total intravenous anesthesia vs inhaling sevoflurane combined with continuous intravenous anesthesia on pain scores in the post-anesthesia care unit (PACU).
We hypothesize that patients who inhaled sevoflurane combined with continuous intravenous anesthesia during the operation can effectively reduce the dosage of muscle relaxant, meet the requirements of laparoscopic deep neuromuscular block (dNMB) in obese patients, shorten the extubation time of obese patients after receiving laparoscopic sleeve gastrectomy and reduce the risk of suffering hypoxemia and the observation time in PACU.
Methods
The study was approved by the Human Research Ethics Committee of Beijing Friendship Hospital of Capital Medical University (Institutional Review Board registration number 2018-P2-119-01) and was compliant with the Declaration of Helsinki. Written informed consent was obtained from all subjects participating in the trial. The trial was registered with the Chinese Clinical Trial Registry (URL: http://www.chictr.org.cn. Registry number: ChiCTR1900020583).
Participants
Obese patients who underwent laparoscopic sleeve gastrectomy under general anesthesia from 2019. 01.15 to 2021.12.31 at Beijing Friendship Hospital, Capital Medical University were enrolled in this study. The inclusion criteria were as follows:
American Society of Anesthesiologists physical status class (ASA) I–III; ② volunteered to participate in the trial and signed the informed consent; ③ age 18–65 years; ④ Body mass index (BMI) >30 kg/m2. The exclusion criteria included: ① gel electrode allergy; ③ neuromuscular disease; ④ abnormal liver and kidney function; ⑤ drugs known to affect neuromuscular conduction function within two weeks before surgery, such as aminoglycosides (nanomycin, kanamycin, and netefloxacin);14 ⑥hearing, intelligence, and communication disorders.
Standardized Anesthesia
Before the operation, all patients fasted for 8–12h. After arriving in the operating room, standard monitoring was recorded by anesthesia machine (Carestation 650), including electrocardiogram, non-invasive blood pressure (NIBP), heart rate (HR) and peripheral blood oxygen saturation. The arterial pressure was measured by direct puncture of radial artery under local anesthesia with lidocaine. Internal jugular vein cannulation is performed after the completion of endotracheal intubation. After the forehead of all patients were defatted with 75% ethanol, BIS sensor electrode was pasted and BIS index was monitored and kept between 40 and 60 throughout anesthesia.
Intravenous phencyclidine hydrochloride 0.015 mg/kg and midazolam 0.05 mg/kg were given to all the patients 30 min before surgery. Neuromuscular block was detected in the abducted arm by using relevant monitor (GE Healthcare Finland Oy; type: B850). We measured the thumb twitch response to four subsequent electrical stimuli (ie, the train-of-four or TOF). In case zero thumb twitches were detected, the post-tetanic count (PTC) was measured. A deep neuromuscular blockade was defined as a posttetanic count (PTC) 1 to 2. General anesthesia was induced with a continuous intravenous infusion with propofol plasma target concentration of 2.5 μg/mL and a remifentanil effector chamber concentration of 4 ng/mL. After induction of anesthesia but before any administration of rocuronium, the device was calibrated according to the specification of the manufacturer. The calibration electrical stimulation frequency was 0.1Hz, the stimulation pulse width was 0.2ms, the stimulation current was 50 mA, and the muscle contraction response of the electrical stimulation was stabilized at 100% for 3 minutes before the calibration was completed. When the BIS drops to the range of 40 to 60, implement the tonic stimulation with a current of 50 mA. Continuous TOF stimulation monitoring was started at 2 Hz with an interval of 20s and with pulse width of 200μs. After maintaining T1 in the range of 90% to 110% and stabilizing for 3 min, rocuronium 0.6 mg/kg was applied intravenously. When T1 is reduced to 0, tracheal intubation was performed, and each patient was mechanically ventilated with a tidal volume and ventilation rate adjusted to maintain the pressure of end-tidal carbon dioxide (ETCO2) at 35–45mmHg. The effect of muscle relaxant was monitored continuously during the operation, PTC was performed every 6 min when T1 was 0. When PTC≥ 3, rocuronium was started pumping intravenously, the initial intravenous pumping rate was 45 mg/kg/h, and the venous pump rate was adjusted according to muscle relaxation monitoring results (the venous pump rate will be increased by 10% when PTC ≥3). The adjustment was completed within 30 min of the start of intravenous infusion to maintain the intraoperative PTC≤ 2. After tracheal intubation was performed, patients in the sevoflurane combined intravenous anesthesia group (S1.0 group) was inhaled sevoflurane in oxygen-air (50%/50%) to maintain a 1.0 minimum alveolar concentration (MAC) and together with maintained propofol and remifentanil. Patients in the intravenous anesthesia group (I group) were maintained only with propofol and remifentanil. The anesthesiologist adjusted the intravenous speed of remifentanil according to the basis of stress-related parameters and adjusted propofol to maintain BIS between 40 and 60 during the operation. Depending on the surgery, rocuronium intravenous pumping was stopped 40 min before the expected end of the surgery in both groups. In addition, the S1.0 group stopped inhaling sevoflurane 15 min before the end of the operation, continued intravenous infusion of propofol and remifentanil until at the end of operation, and neostigmine was routinely given 0.07 mg/kg for antagonism. By using a warming blanket, the central body temperature was maintained at over 35°C and the peripheral body temperature measured at the thenar eminence of the palm was maintained at 32°C or higher. The endotracheal tube was removed when the TOF-ratio >0.9 and the patient breathed spontaneously and was fully awake.
Blinding and Randomization
The sevoflurane jar was covered during the operation, only the attending anesthesiologist knew whether to use sevoflurane or not. The sevoflurane monitoring data was shown on a separate monitor, surgeons could not see the data from the anesthesia monitor. Therefore, the study had a design with the surgeons and patients blinded to treatment, data collector was blinded to the group assignment, whereas the attending anaesthesiologist was un-blinded. Participants were enrolled by anaesthesiologists during the pre-operative visit and randomization was performed after the first evaluation. The method used to generate the random allocation sequence was a computer-generated random list with a sealed envelope.
Data Management
The following variables were collected: patient variables (age, weight, height, BMI, sex, ASA classification), anesthesia-related variables such as anesthetics dosages; clinical muscle relaxant time (the time of stopping the rocuronium pump to T1 recovery to 25%); muscle relaxant in the vivo action time (the time when the rocuronium pump is stopped to T1 returns to 90%); muscle relaxant recovery time (the time when T1 recovers from 25% to 75%); body movement times; extubation duration (from stopping intravenous rocuronium which is 40 min before the expected end of surgery to extubation timepoint) and variables obtained in the PACU (pain in the PACU, staying time in the PACU).
Evaluation of Surgical Conditions
Surgery-related variables (the Leiden-Surgical Rating Scale (L-SRS), duration of the procedure) were also recorded. The L-SRS aims to quantify the quality of the surgical field based on visibility, surgical space, muscle contractions, handling tactics and patient movement. During the operation, the L-SRS was scored by the surgeon performing the laparoscopic bariatric surgery at the beginning of surgery (T0); 1 hour after beginning of surgery (T1); stop pumping rocuronium (T2) and starting close the abdomen (T3). The L-SRS is a Likert scale ranging from 1 to 5 where 1 indicates extremely poor conditions, 2 poor conditions, 3 acceptable conditions, 4, good conditions and 5 optimal conditions.15
Postoperative Outcome
The pain was measured using visual analog scale (VAS) score, ranging from 0 (no pain) to 10 (most pain imaginable) before leaving the PACU.16 The duration in the PACU was also recorded. Record patients’ satisfaction level in the PACU: fairly dissatisfied; medium satisfied; most satisfied; very satisfied. Adverse effects such as bradycardia, nausea and vomiting, dyspnea after extubation and hypoxemia were also treated accordingly.
Sample Size
Based on our preliminary study, we initially powered the study to detect a difference in L-SRS between treatments of 0.7 points with SD 0.7. A sample size of 21 per group was calculated which would provide at least 90% power to detect the expected difference in L-SRS at α = 0.05. Considering potential dropouts about 15%, finally a total of 59 patients were enrolled in this study.
Statistical Analysis
SPSS 23.0 and GraphPad Prism 6.0 software were used for the statistical analyses of study data. The Shapiro–Wilk test was used to assess the distribution of variables. Continuous data are represented as mean ± standard deviation, independent-samples Student’s –-test and the Mann–Whitney U-test were used to analyze. Chi-square test was used to analyze differences in ASA, gender, postoperative adverse effects and satisfaction between groups. Skewed data were presented as median (IQR). Statistical significance tests were conducted using two-sided tests, with P < 0.05 as the criterion to judge the significance of differences.
Result
We initially assessed 78 patients for eligibility to participate in our study (Figure 1), of these 12 patients refused to participate, 7 patients did not meet the inclusion criteria (2 patients were above 65 years old and 5 patients’ BMI < 30 kg/m2), and the remaining 59 patients enrolled in the study. Following the completion of the study, 4 patients in the S1.0 Group were excluded from the study due to transferring to ICU after surgery. Five patients in the I Group were excluded from the study due to transferring to ICU after surgery. Finally, the data from 25 patients in the S1.0 Group and 25 patients in the I Group were analyzed in the present study.
 |
Figure 1 The flow chart of included and excluded patients. |
Demographic Characteristics Between the Two Groups
No statistically differences were found between the two groups in patients’ sex (P = 0.440), age (P = 0.111), hight (P = 0.797), weight (P = 0.946), BMI (P = 0.560), ASA (P = 0.338), (Table 1).
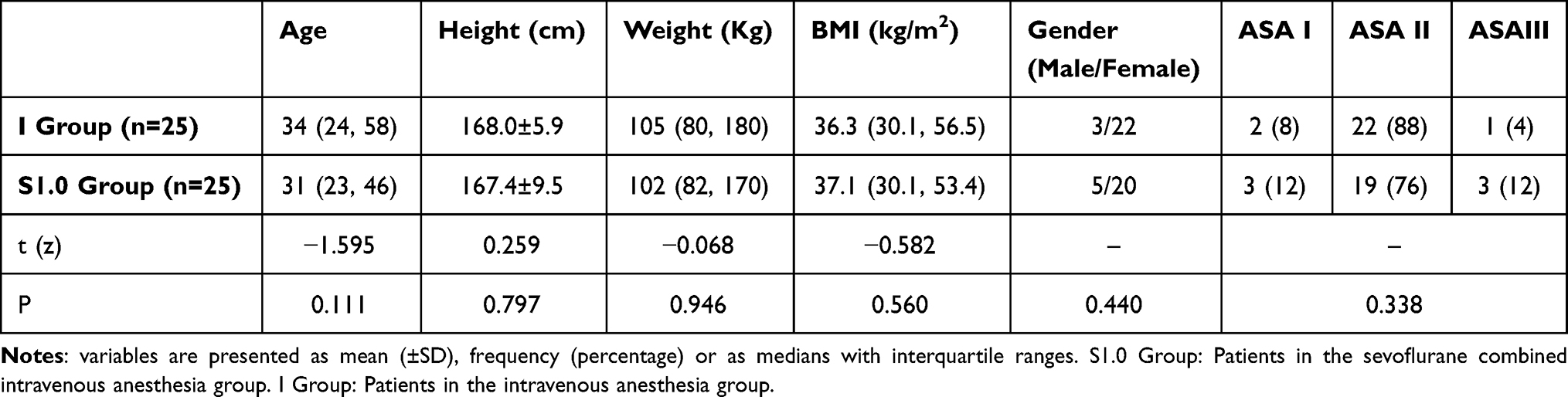 |
Table 1 Comparison of Demographic Characteristics Between the Two Groups |
Comparison of Intraoperative and Postoperative Measurements
As shown in Table 2, the total dose of propofol (mg) and remifentanil (ug) in the S1.0 Group was statistically lower than that in the I Group (P < 0.001, respectively). Furthermore, the total dose of rocuronium during the operation of patients in the S1.0 Group was also significantly less than that of patients in the I Group (P = 0.028). While the body movement times during the operation between the two groups were not statistically significant (P = 0.317). No difference was found in the total dose of sufentanil between the two groups (P = 0.784 and P = 0.693). Patients in the S1.0 Group had significantly shorter extubation times than that in the I Group (P = 0.039).
 |
Table 2 Measurements Obtained During and Following Surgery |
Comparison of the Effect of Rocuronium Between the Two Groups
As shown in Figure 2a, there is no significant difference in clinical muscle relaxant time between the two groups during the operation (P = 0.566). Muscle relaxant in the vivo action time (min) was longer in the I group when compared to that in the S1.0 group (58.7±14.1 vs 50.5±10.0, P = 0.022 Figure 2b). Patients in the S1.0 groups seem to recover faster when T1 recovers from 25% to 75% than patients in the I group (4.7±4.6 vs 11.5±8.5 P = 0.001 Figure 2c).
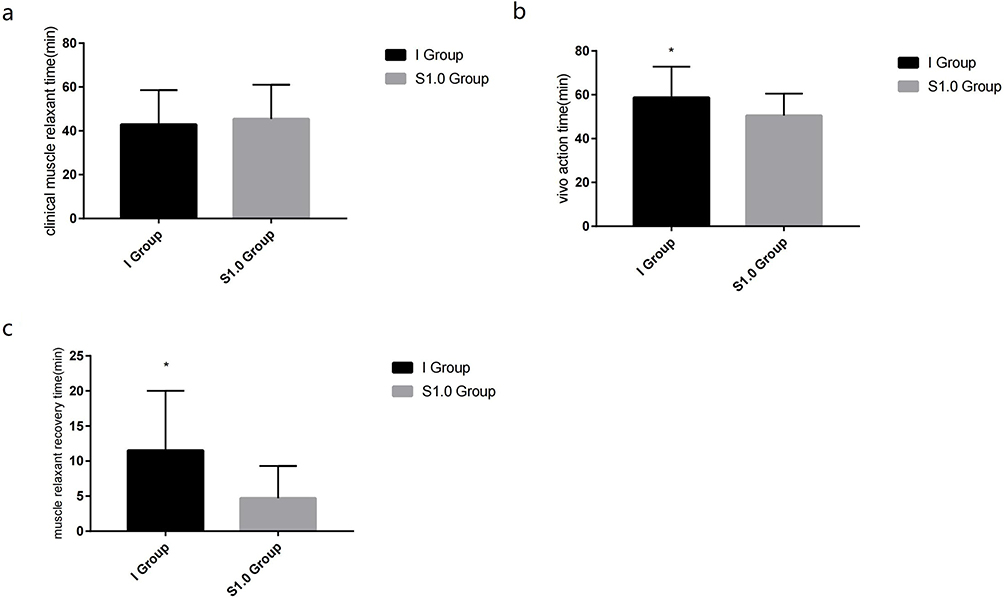 |
Figure 2 The comparison of effect of rocuronium between the two groups. (a) Clinical muscle relaxant time (the time of stopping the rocuronium pump to T1 recovery to 25%); (b) muscle relaxant in the vivo action time (the time when the rocuronium pump is stopped to T1 returns to 90%); (c) muscle relaxant recovery time (the time when T1 recovers from 25% to 75%). *P < 0.05 when compared to S1.0 group. |
The Leiden-Surgical Rating Scale During Bariatric Surgery
There were no statistical differences in LSR scale scores between the two groups at the beginning of surgery, 1 hour after the beginning of surgery and at the time when stop pumping rocuronium (P = 0.166, P = 0.510, P = 0.561 respectively). While the LSR scale score was higher in the S1.0 group than that in the I group when starting close to the abdomen (P < 0.001) (Figure 3).
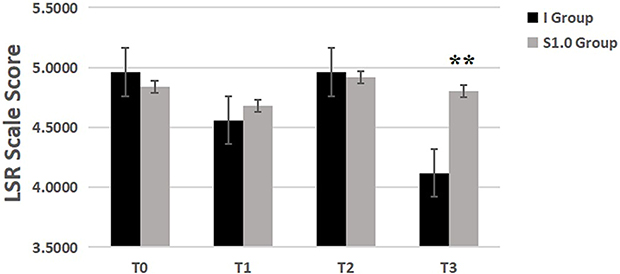 |
Figure 3 The Leiden-Surgical Rating Scale during Bariatric Surgery. The beginning of surgery (T0); 1 hour after beginning of surgery (T1); stop pumping rocuronium (T2) and starting close the abdomen (T3). **P < 0.001 when compared to I Group. |
Measurements in the PACU
No difference in the pain scores was found between the S1.0 group and I group in the PACU (P = 0.144). While the duration in the PACU of the I group seems longer than that in the S1.0 group (P = 0.039) (Table 2). There is only one patient in the I group suffered dyspnea after extubation, which was not comparable with the S1.0 group (P = 0.312). And patients’ satisfaction level seems not significantly different between the two groups either (P=0.297). None of the patients presented fairly dissatisfied during their perioperative period (Table 3).
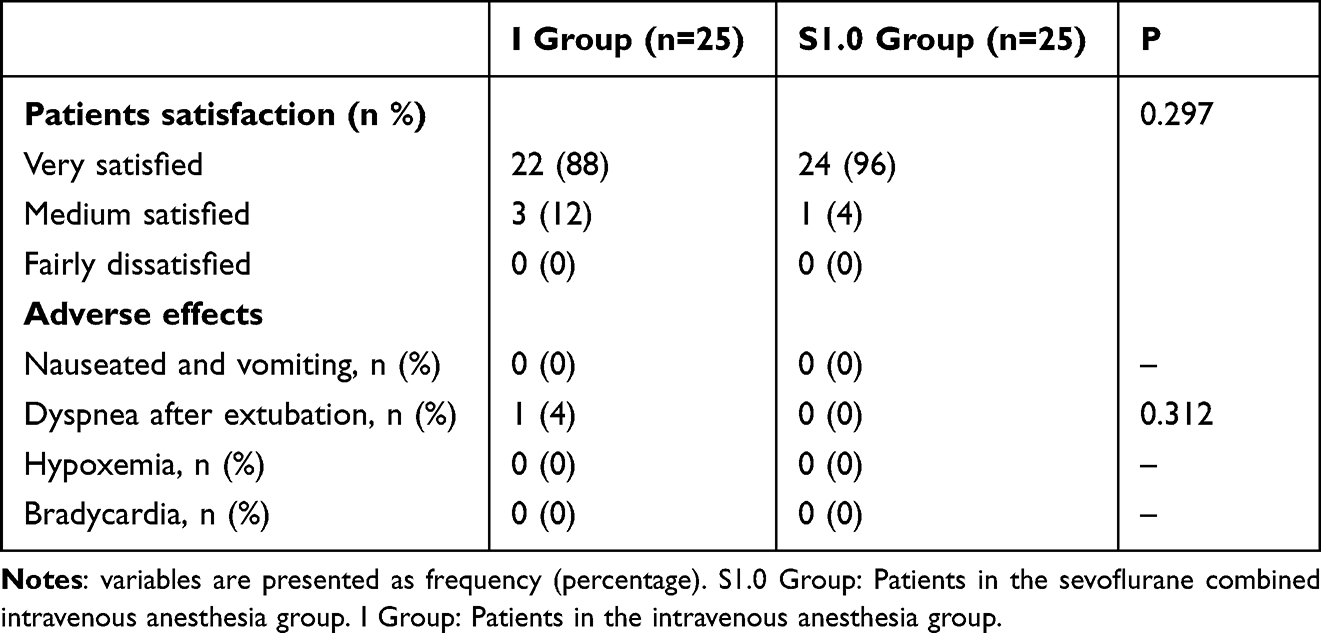 |
Table 3 Postoperative Outcomes Between the Two Groups |
Discussion
The findings of our study proved that inhaling sevoflurane combined with continuous intravenous infusion during the operation can effectively reduce the dosage of muscle relaxant to achieve the same dNMB effect, and shorten the muscle relaxant in the vivo action time and recovery time. Meanwhile, inhaling sevoflurane combined with continuous intravenous infusion during the operation could effectively shorten the extubation time of obese patients after receiving laparoscopic sleeve gastrectomy and reduce the risk of suffering hypoxemia and the observation time in PACU.
Worldwide, the prevalence of obesity has nearly tripled in over the past 40 years. Comorbidities are more common in obese people, including those requiring surgical intervention.17 It is estimated that approximately 30% of the general surgical population present with obesity.18 With an improved safety profile, and evidence to support its long-term efficacy, the volume of bariatric surgery is expected to increase.19 The fundamental basis for bariatric surgery to achieve weight loss is the determination that severe obesity is a disease associated with multiple adverse effects on health, which can be reversed or improved by successful weight loss in patients who have been unable to sustain weight loss by non-surgical means. The continuous progress of laparoscopic surgery is due to its advantages, such as less postoperative pain, short hospital stay, early recovery of normal physical activity, better aesthetic effect, and reduction of incisional hernia. It also reduces both systemic and immune stress changes. Since laparoscopic surgery is a minimally invasive technique, it will benefit morbidly obese patients because they have a variety of related comorbidities, making them more prone to complications during the postoperative period.20 However, intraoperative pneumoperitoneum can adversely affect all aspects of the patient, which make it become an important factor in the postoperative complications of laparoscopic surgery. Elevated pneumoperitoneal pressure could not only reduce lung compliance and cardiac output, it could also cause hypercapnia and respiratory acidosis, activate the inflammatory response in the body, and eventually lead to damage to tissues and organs, and affect the postoperative recovery of patients.21 Thus, dNMB is more effective in softening abdominal muscles, improving surgical vision, reducing the need for high pneumoperitoneum pressure, and preventing abdominal muscle contraction, then reducing the risk of complications associated with surgery.1 But laparoscopy significantly reduces the time span for recovery from intraoperative NMB, deep NMB puts the patient at risk for residual postoperative NMB and associated postoperative hypoxemia, which also attracted the attention of anesthesiologists.22,23 Previous studies proved that even minimal residual NMB with a TOFR of 0.8 is associated with impaired respiratory function, as witnessed by reductions of forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) in healthy volunteers.24 And 100% of patients after bariatric surgery had at least one hypoxic event (oxygen saturation <90% for more than 30 seconds).25 Therefore, it is more critical to seek a drug combination that can achieve a good dNMB state without increasing the perioperative risk.
In our study, we enrolled 59 obese patients who received laparoscopic bariatric surgery, we used total intravenous anesthesia as the control group and inhaled sevoflurane combined with intravenous anesthesia as the experimental group to both achieve PTC ≤2 as dNMB requirement during the operation. We found that inhaling sevoflurane can effectively reduce the dosage of muscle relaxants. And its time when the rocuronium pump is stopped to T1 returns to 90% was shorter and its time when T1 recovers from 25% to 75% was faster. While, T1 recovery of 25%, also known as clinical muscle relaxant time, was also used in our study. The lack of a noticeable difference between the two groups may be attributed to the fact that during the peak period of the action of neuromuscular blockers, the neuromuscular joint site is greatly inhibited, and the neuromuscular joint is in a deep block degree, which is less affected by inhalation drugs.26 Meanwhile, inhaling sevoflurane could also effectively shorten the extubation time of obese patients after receiving laparoscopic bariatric surgery and reduce the risk of suffering hypoxemia and the observation time in PACU. The possible mechanisms may be due to that inhaled anesthetics mainly enhance the effect of non-depolarized muscle relaxants through synergistic action, and the main site of action occurs in the neuromuscular joint site. The prolongation of the effect of rocuronium during sevoflurane anesthesia is probably caused by a faster and more complete equilibrium among the end-tidal, blood, and muscle concentrations of sevoflurane because of its smaller muscle-gas partition coefficient, resulting in an increased duration of action and slower recovery.27 Inhaled anesthetics can reduce the sensitivity of the posterior membrane to depolarization, increase the threshold of the endplate potential by changing the Na+-K+ channel, enhance the activity of inhibitory postsynaptic combination, and inhibit the activity of excitatory synapse combination.28–30 Moreover, inhaled anesthetics can be mechanically ventilated out of patients through the anesthesia machine, which will not prolong the awakening time of the patient, nor have the risk of postoperative residual dyspnea and hypoxemia.
In addition, a good surgical vision is undoubtedly the key to the success of the operation. In the study of the effect of dNMB on the surgical visual field, Fuchs Buder et al31 designed a single-center randomized controlled study, and the results showed a great improvement of dNMB in the surgical visual field. The outcome measurement of studies mostly used the surgeon’s subjective score such as LSR scale. Similar to the previous study, we found that both of the two groups in our study reached the satisfied LSR scale scores at the beginning of surgery, 1 hour after the beginning of surgery and at the time when stop pumping rocuronium. While the LSR scale score was still higher in the S1.0 group when starting close the abdomen, the possible reason may be that though the sevoflurane was stopped 15 min before the end of the operation, the residual sevoflurane in the respiratory circuit still works. Even so, the duration in the PACU of the S1.0 group was shorter than that in the I group. And patients’ satisfaction level seems not significantly different between the two groups.
There might be several limitations in the present study. First, we found that keeping dNMB during the operation could significantly improve the surgical field and conditions. However, Söderström et al’s study found no difference of the surgical visual field score in laparoscopic hernia repair surgery by keeping dNMB during the operation.32 The outcome indicator of the surgeon in the current study was subjective to the evaluation of surgical visual field conditions, which may be an important reason for the controversial results. The improvement effect of dNMB on the surgical visual field still needs more objective evaluation in further study. Second, we did not use sugammadex in our study as specific antagonist. Though sugammadex is known to reverse neuromuscular blockade (NMB) of rocuronium and vecuronium more rapidly and reliably, however, there were also many postoperative complications in recovery outcomes among patients. Moreover, in China, sugammadex is expensive, even if some hospitals have sugammadex, patients have to be at their own expense because it is not covered by medicare, which limits its application in clinical practice. We use neostigmine routinely at the end of surgery, which may be even more convenient for Chinese hospitals and patients who refuse to use sugammadex. Third, in our study, we acknowledge that the attending anesthesiologist was un-blinded during the study, we adopted a blinded design in which the surgeons and patients were unaware of the treatment assignment. Additionally, the data collector was also blinded to the group allocation. It is essential to emphasize that the indicators recorded intraoperatively were objective and did not involve subjective assessments that required input from the anesthesiologist. Fourth, this is a single-center analysis character focusing only on one specific hospital and one population, and a multicenter experiment should be further studied.
Conclusion
The findings of this study can be understood as patients inhaled sevoflurane combined with continuous intravenous anesthesia during the operation can effectively reduce the dosage of muscle relaxant to achieve the same dNMB effect with only using total continuous intravenous anesthesia. Meanwhile, inhaling sevoflurane combined with continuous intravenous anesthesia during the operation could effectively shorten the extubation time of obese patients after receiving laparoscopic sleeve gastrectomy and reduce the risk of suffering hypoxemia and the observation time in PACU. This may be considered a promising aspect of promoting postoperative recovery outcomes of obese patients undergoing laparoscopic sleeve gastrectomy.
Data Sharing Statement
The datasets generated and analyzed during the current study are not yet publicly available. These data will be available from the corresponding author on reasonable request.
Funding
This research was funded by grants from Scientific Research Common Program of Beijing Municipal Commission of Education (Grant number: KM202010025021), Beijing Hospitals Authority Youth Programme (Grant number: QML20190101), Beijing Municipal Administration of Hospitals Incubating Program (Grant number: PX2019001), Capital’s Funds for Health Improvement and Research (2020-4-20210).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nightingale CE, Margarson MP, Shearer E, et al.; Members of the Working Party. Peri-operative management of the obese surgical patient 2015: Association of Anaesthetists of Great Britain and Ireland Society for Obesity and Bariatric Anaesthesia. Anaesthesia. 2015;70(7):859–876. doi:10.1111/anae.13101
2. Engelbrechtsen L, Lundgren J, Wewer Albrechtsen NJ, et al. Treatment with liraglutide may improve markers of CVD reflected by reduced levels of apoB. Obes Sci Pract. 2017;3(4):425–433. doi:10.1002/osp4.133
3. Christensen RM, Juhl CR, Torekov SS. Benefit-risk assessment of obesity drugs: focus on glucagon-like peptide-1 receptor agonists. Drug Saf. 2019;42(8):957–971. doi:10.1007/s40264-019-00812-7
4. Lundgren JR, Janus C, Jensen SBK, et al. Healthy weight loss maintenance with exercise, liraglutide, or both combined. N Engl J Med. 2021;384(18):1719–1730. doi:10.1056/NEJMoa2028198
5. Zhou Y, Wu L, Li X, et al. Outcome of laparoscopic colorectal surgery in obese and nonobese patients: a meta-analysis. Surg Endosc. 2012;26:783–789. doi:10.1007/s00464-011-1952-2
6. McIlwaine K, Cameron M, Readman E, et al. The effect of patient body mass index on surgical difficulty in gynaecological laparoscopy. Aust N Z J Obstet Gynaecol. 2010;8:145–149.
7. Pikarsky AJ, Saida Y, Yamaguchi T, et al. Is obesity a highrisk factor for laparoscopic colorectal surgery? Surg Endosc. 2002;16:855–858. doi:10.1007/s004640080069
8. Dhar DK, Kubota H, Tachibana M, et al. Body mass index determines the success of lymph node dissection and predicts the outcome of gastric carcinoma patients. Oncology. 2000;59:18–23. doi:10.1159/000012131
9. Senagore AJ, Delaney CP, Madboulay K, et al. Laparoscopic colectomy in obese and nonobese patients. J Gastrointest Surg. 2003;7:558–561. doi:10.1016/S1091-255X(02)00124-5
10. Lee JH, Paik YH, Lee JS, et al. Abdominal shape of gastric cancer patients influences short-term surgical outcomes. Ann Surg Oncol. 2007;14:1288–1294. doi:10.1245/s10434-006-9235-1
11. Fuchs⁃Buder T, De Robertis E, Brunaud L. Neuromuscular block in laparoscopic surgery. Minerva Anestesiol. 2018;84(4):
12. Deshko Iu V, Mizikov VM, Stamov VI, Golovkin AS, Vinitskii LI. Use of average-acting nondepolarizing myorelaxants in abdominal surgery. Anesteziol Reanimatol. 2006;5:66–70.
13. Yoo YC, Kim NY, Shin S, et al. The intraocular pressure under deep versus moderate neuromuscular blockade during low-pressure robot assisted laparoscopic radical prostatectomy in a randomized trial. PLoS One. 2015;10(8):e0135412. doi:10.1371/journal.pone.0135412
14. Qu W. Quantitative Analysis of the Effect of Different Concentrations of Sevoflurane on the Myosasone Intensity of Rocuronium. Dalian Medical University; 2021.
15. Martini CH, Boon M, Bevers RF, Aarts LP, Dahan A. Evaluation of surgical conditions during laparoscopic surgery in patients with moderate vs deep neuromuscular block. Br J Anaesth. 2014;112:498–505. doi:10.1093/bja/aet377
16. El Sherif FA, Othman AH, Abd El-Rahman AM, Taha O. Effect of adding intrathecal morphine to a multimodal analgesic regimen for postoperative pain management after laparoscopic bariatric surgery: a prospective, double-blind, randomized controlled trial. Br J Pain. 2016;10(4):209–216. doi:10.1177/2049463716668904
17. World Health Organization. Obesity and overweight 2020; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
18. Tsai A, Schumann R. Morbid obesity and perioperative complications. Curr Opin Anaesthesiol. 2016;29(1):103–108. doi:10.1097/ACO.0000000000000279
19. O’Brien PE, Hindle A, Brennan L, et al. Long-term outcomes after bariatric surgery: a systematic review and meta-analysis of weight loss at 10 or more years for all bariatric procedures and a single-centre review of 20-year outcomes after adjustable gastric banding. Obes Surg. 2019;29(1):3–14. doi:10.1007/s11695-018-3525-0
20. Luján JA, Frutos MD, Hernández Q, et al. Laparoscopic versus open gastric bypass in the treatment of morbid obesity: a randomized prospective study. Ann Surg. 2004;239(4):433–437. doi:10.1097/01.sla.0000120071.75691.1f
21. Boggett S, Chahal R, Griffiths J, et al. A randomised controlled trial comparing deep neuromuscular blockade reversed with sugammadex with moderate neuromuscular block reversed with neostigmine. Anaesthesia. 2020;75:1153–1163. doi:10.1111/anae.15094
22. Kopman AF, Naguib M. Is deep neuromuscular block beneficial in laparoscopic surgery? No, probably not. Acta Anaesthesiol Scand. 2016;60:717–722. doi:10.1111/aas.12699
23. Madsen MV, Staehr-Rye AK, Claudius C, Gätke MR. Is deep neuromuscular blockade beneficial in laparoscopic surgery? Yes, probably. Acta Anaesthesiol Scand. 2016;60:710–716. doi:10.1111/aas.12698
24. Eikermann M, Groeben H, Hüsing J, Peters J. Accelerometry of adductor pollicis muscle predicts recovery of respiratory function from neuromuscular blockade. Anesthesiology. 2003;98:1333–1337. doi:10.1097/00000542-200306000-00006
25. Gallagher SF, Haines KL, Osterlund LG, Mullen M, Downs JB. Postoperative hypoxemia: common, undetected, and unsuspected after bariatric surgery. J Surg Res. 2010;159:622–626. doi:10.1016/j.jss.2009.09.003
26. Saitoh Y. Recovery from vecuronium is delayed in patients with hypercholesterolemia. Can J Anaesth. 2006;53(6):556–561. doi:10.1007/BF03021845
27. Lowry DW, Mirakhur RK, McCarthy GJ, Carroll MT, McCourt KC. Neuromuscular effects of rocuronium during sevoflurane, isoflurane, and intravenous anesthesia. Anesth Analg. 1998;87(4):936–940. doi:10.1213/00000539-199810000-00036
28. Kleijn HJ, Zollinger DP, van den Heuvel MW, Kerbusch T. Population pharmacokinetic-pharmacodynamic analysis for sugammadex-mediated reversal of rocuronium-induced neuromuscular blockade. Br J Clin Pharmacol. 2011;72(3):415–433. doi:10.1111/j.1365-2125.2011.04000.x
29. Amin AM, Mohammad MY, Ibrahim MF. Comparative study of neuromuscular blocking and hemodynamic effects of rocuronium and cisatracurium under sevoflurane or total intravenous anesthesia. Middle East J Anaesthesiol. 2009;20(1):39–51.
30. Berg H, Roed J, Viby-Mogensen J, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997;41(9):1095–1103. doi:10.1111/j.1399-6576.1997.tb04851.x
31. Fuchs⁃Buder T, Schmartz D, Baumann C, et al. Deep neuromuscular blockade improves surgical conditions during gastric bypass surgery for morbid obesity: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(7):486–493. doi:10.1097/EJA.0000000000000996
32. Söderström CM, Medici B, Assadzadeh S, et al. Deep neuromuscular blockade and surgical conditions during laparoscopic ventral hernia repair: a randomised, blinded study. Eur J Anaesthesiol. 2018;35(11):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.