Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Remimazolam versus Propofol on Hemodynamics in Elderly Hypertensive Patients Undergoing Gastroenteroscopy: A Multicenter, Randomized Controlled Clinical Trial
Authors Gu Q ![]() , Zeng D, Lin D
, Zeng D, Lin D ![]() , Zou J, Sun J
, Zou J, Sun J ![]() , Wang H, Chen S
, Wang H, Chen S ![]() , Zhang H
, Zhang H ![]() , Xu B, Liu W
, Xu B, Liu W ![]() , Shu J
, Shu J ![]()
Received 10 May 2025
Accepted for publication 24 July 2025
Published 28 July 2025 Volume 2025:19 Pages 6423—6434
DOI https://doi.org/10.2147/DDDT.S532746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Yan Zhu
Qian Gu,1,2,* Deling Zeng,3,* Dayong Lin,4,* Jiang Zou,5,* Jiaxin Sun,1 Huaiming Wang,1 Shiwei Chen,2 Hongwei Zhang,1 Bo Xu,1 Wusong Liu,6 Jinjun Shu1
1Department of Anesthesiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Anesthesiology, Xichang People’s Hospital, Xichang, People’s Republic of China; 3Health Management Center, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 4Department of Anesthesiology, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 5Department of Anesthesiology, Sichuan Women’s and Children’s Hospital/Women’s and Children’s Hospital, Chengdu Medical College, Chengdu, People’s Republic of China; 6Department of Endoscopy Center, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinjun Shu, Department of Anesthesiology, Sichuan Cancer Hospital, No. 55, Section 4, South Renmin Road, Chengdu, 610041, People’s Republic of China, Email [email protected] Wusong Liu, Department of Endoscopy Center, Sichuan Cancer Hospital, No. 55, Section 4, South Renmin Road, Chengdu, 610041, People’s Republic of China, Email [email protected]
Purpose: This study aimed to compare the effects of remimazolam and propofol on hemodynamics in elderly hypertensive patients undergoing gastroenteroscopy.
Methods: In this multicenter, single-blind, randomized clinical trial, 220 hypertensive patients (65– 75 years) scheduled for gastroenteroscopy were randomly assigned to receive either remimazolam (group R, n=110; 0.3 mg/kg induction followed by 0.2– 1 mg/kg/h maintenance) or propofol (group P, n=110; 1.5 mg/kg induction followed by 2– 6 mg/kg/h maintenance), both combined with 0.1 μg/kg sufentanil. Flumazenil or placebo was administered for reversal. Hemodynamics were monitored via Continuous Non-Invasive Arterial Pressure (CNAP). The primary outcomes were hypotension incidence and hemodynamic parameters [mean arterial pressure (MAP), heart rate (HR), cardiac output (CO), and systemic vascular resistance (SVR)]; secondary outcomes included the incidence of other adverse events and recovery time.
Results: Group R exhibited significantly lower incidences of hypotension (72.7% vs 37.3%, p < 0.001) and bradycardia (16.4% vs 7.3%, p = 0.037), alongside reduced vasopressor requirements (ephedrine: 3.760 ± 4.133 vs.1.850 ± 3.121, p < 0.001; metaraminol: 0.101 ± 0.208 vs 0.045 ± 0.144, p = 0.012). Both groups exhibited decreased MAP, CO, and SVR at the time point of endoscope entry (T1) compared to 2 minutes before anesthesia induction (T0), while HR reduction was significant only in group P (p < 0.001 vs p = 0.084 in group R). From T1 through 15 minutes post-procedure (T4), group R maintained higher MAP and HR than group P (p < 0.05). Remimazolam was associated with shorter recovery time (p < 0.001), lower rates of respiratory depression (p = 0.002), but higher rates of body movements (p < 0.001) and cough (p = 0.001).
Conclusion: Remimazolam provides superior hemodynamic stability and faster recovery compared to propofol in elderly hypertensive patients undergoing gastroenteroscopy, establishing it as a safer sedation option for this vulnerable patient population.
Trial Number and Registry Url: Registration number, ChiCTR2400083757; https://www.chictr.org.cn/showproj.html?proj=214795.
Keywords: remimazolam, propofol, elderly hypertensive patients, gastroenteroscopy
Introduction
With the accelerating pace of global population aging, the proportion of elderly individuals continues to rise, particularly in China, which accounts for 20% of the world’s elderly population.1 Hypertension is highly prevalent in this demographic, and due to reduced vascular elasticity, elderly patients are more susceptible to anesthesia-induced hypotension, increasing the risk of adverse postoperative outcomes.2–4
Globally, gastrointestinal (GI) malignancies remain a significant public health burden, with approximately 3 million new cases and 1.7 million related deaths reported in 2020.5 Gastroenteroscopy serves as the gold standard for GI cancer diagnosis, with over 98% of gastroenteroscopy procedures performed under sedation to improve patient comfort and procedural accuracy.6
Propofol has long been the cornerstone of sedation for endoscopic examinations due to its rapid onset, quick recovery, antiemetic effects, and enhanced patient compliance.6 Its use has reportedly increased the rate of diagnostic gastroscopies and colonoscopies fourfold.3 However, propofol exhibits several dose-dependent limitations, including hypotension, respiratory depression, and injection pain,7,8 and lacks a specific reversal agent, restricting its use in high-risk populations.
Remimazolam, a novel ultrashort-acting benzodiazepine, offers distinct advantages, including rapid onset and offset, hemodynamic stability, reversibility with flumazenil, minimal accumulation, and reduced cardiorespiratory depression.9–12 Moreover, remimazolam undergoes rapid hydrolysis by tissue esterases, independent of hepatic or renal metabolism, further enhancing its safety profile.13,14 Clinical evidence consistently demonstrates remimazolam’s superior hemodynamic stability compared to propofol,15–19 with specific studies showing equivalent sedation efficacy but significantly reduced hemodynamic and respiratory complications when combined with opioids for elderly gastroscopy patients.10 Furthermore, in hypertensive elderly patients undergoing general anesthesia, remimazolam demonstrates superior hemodynamic stability with a lower risk of post-induction hypotension.20 However, there is a scarcity of data to investigate the impact of remimazolam on hemodynamic stability and the occurrence of intraoperative hypotension compared with propofol in elderly hypertensive patients during gastroenteroscopy.
Conventional non-invasive blood pressure (NIBP) monitoring, typically measured at 3–10 minute intervals, may miss up to 20% of hypotensive episodes and delay detection in another 20%, underscoring its limitations in high-risk patients.21 In contrast, Continuous Non-Invasive Arterial Pressure (CNAP) monitoring provides real-time, beat-to-beat arterial waveform analysis, enabling early detection of hemodynamic instability through continuous measurement of blood pressure, cardiac output (CO), systemic vascular resistance (SVR), and heart rate (HR).22,23 CNAP measurement facilitates detecting hemodynamic instability more rapidly and can improve patient safety.24
This multicenter randomized controlled trial was designed to evaluate the hemodynamic effects of remimazolam versus propofol in elderly hypertensive patients undergoing gastroenteroscopy, utilizing CNAP for precise hemodynamic assessment. We hypothesize that remimazolam will reduce the incidence of hypotension and provide superior hemodynamic stability compared to propofol, offering a safer alternative for sedation in elderly hypertensive patients receiving painless gastroenteroscopy.
Materials and Methods
Ethics and Registration
The study protocol was approved by the Ethics Committee for Medical Research and New Medical Technology of Sichuan Cancer Hospital (SCCHEC-02-2023-145). This trial was registered in the Chinese Clinical Trial Registry (https://www.chictr.org.cn/showproj.html?proj=214795, ChiCTR2400083757, 30 April 2024). Investigators explained the study to all subjects and obtained written informed consent. The study was in line with the Declaration of Helsinki.
Participants
This study was a multicenter, randomized trial conducted across three medical institutions in China: Sichuan Cancer Hospital, Sichuan Provincial People’s Hospital, and Xichang People’s Hospital. Between May 2024 and January 2025, we enrolled 220 elderly hypertensive patients scheduled for elective painless gastroenteroscopy.
Inclusion Criteria
(1) Elderly hypertensive patients scheduled to undergo painless gastroenteroscopy; (2) Aged 65–75 years; (3) American Society of Anesthesiologists (ASA) status of II–III and New York Heart Association (NYHA) functional class I or II; (4) A history of well-controlled primary hypertension (≤ 160/90 mmHg) under standardized antihypertensive therapy.
Exclusion Criteria
(1) Declined to participate in the study; (2) Had uncontrolled hypertension without regular medication; (3) Presented with severe dysfunction of major organ systems (cardiac, cerebral, pulmonary, hepatic, renal, or metabolic); (4) Had a documented history of adverse anesthesia recovery; (5) Exhibited bradycardia (resting HR < 50 beats/min on ECG); (6) Had an active upper respiratory tract infection within the preceding 2 weeks; (7) Had neuromuscular disorders or psychiatric conditions; (8) Were diagnosed with anemia (hemoglobin below the normal range); (9) Had a history of alcohol abuse or dependence on opioids/sedative-hypnotics; (10) Anticipated difficult airway; (11) Had known allergies or contraindications to benzodiazepines, opioids, propofol, or related compounds; (12) Demonstrated uncooperative behavior or impaired communication ability.
Randomization and Blinding
A professional not involved in the subsequent trial performed the central randomization method using the random allocation module of SPSS 27.0, with each center competing for admission. Participants were allocated in a 1:1 ratio to either the propofol group (group P) or the remimazolam group (group R). This study employed a single-blind design, with surgeons, patients, outcome assessors, and data analysts remaining blinded to treatment allocation throughout the trial, while the administering anesthesiologist remained unblinded due to the visual distinctiveness of the study drugs.
Sample Size Calculation
The primary outcomes of this study were the incidence of hypotension and hemodynamic parameters. The sample size was calculated based on the incidence of hypotension. According to previous studies demonstrating a 35.2% incidence of hypotension with propofol-based sedation,25 we hypothesized a 50% reduction in hypotensive events with remimazolam. Using PASS version 2021 with a significance level (α) of 0.05 (two-sided) and power (β) of 0.8, 95 patients per group were required. Accounting for a dropout rate of 10%, 105 patients per group were planned. Ultimately, 110 elderly hypertensive patients were included in each group.
Anesthesia Methods
All patients maintained an 8-hour fast and a 4-hour liquid restriction preoperatively, with no preoperative medications administered. Standardized bowel preparation was completed within 24 hours. On the day of endoscopy, intravenous access was established in the preoperative holding area. Upon entering the endoscopy suite, patients received standardized intravenous saline infusion and were positioned in the left lateral decubitus position. For continuous hemodynamic monitoring, we implemented the CNAP system with a dual-cuff configuration: a standard NIBP cuff was placed on the right upper arm for periodic calibration, while a finger cuff was positioned on the second and third digits of the right hand for continuous measurement. The system automatically recalibrated every 10 minutes using brachial artery pressure as the reference standard. Continuous monitoring of systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), HR, CO, SVR, and other hemodynamic indicators was conducted using a CNAP monitor. A peripheral oxygen saturation probe was secured to the index finger of the left hand to monitor peripheral oxygen saturation (SpO2).
During the procedure, all patients received supplemental oxygen (6 L/min) via face mask. 0.1 µg/kg of sufentanil (Yichang Renfu Pharmaceutical Co., LTD.) was administered over two minutes before sedative medication. Afterward, in group R, patients received 0.3 mg/kg of remimazolam (Yichang Renfu Pharmaceutical Co., LTD.) intravenously for > 60 seconds. The sedation was maintained through continuous infusion of 0.2–1 mg/kg/h of remimazolam. Patients in group P were given 1.5 mg/kg of propofol (Yangtze River Pharmaceutical Co., Ltd.) intravenously for > 60 seconds, and sedation was maintained by continuous pumping of propofol at 2–6 mg/kg/h. Throughout the procedure, sedation depth was continuously monitored using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale from induction onward. The endoscopic procedure commenced upon achieving adequate sedation (MOAA/S score ≤ 2). Subsequent assessments were performed at 5-minute intervals until full recovery. If MOAA/S was above 2, a 0.1 mg/kg bolus of remimazolam was administered as additional sedation in group R, or a 0.5 mg/kg bolus of propofol was administered accordingly in group P. Failure of sedation was defined as inability to achieve MOAA/S ≤ 2 after two bolus doses within any 5-minute window. In such cases, rescue sedation with propofol (0.5 mg/kg boluses) was administered to facilitate procedure completion.
Upon completion of the endoscopic procedure, all medication infusions were immediately terminated. For patients in group R, flumazenil (Jiangsu Enhua Pharmaceutical) was administered intravenously at a dose of 0.2 mg (2 mL) every two minutes until return of consciousness (defined as MOAA/S score = 5), with a maximum cumulative dose not exceeding 1 mg. Group P received equivalent volumes of normal saline placebo administered on the same schedule until consciousness was regained. All patients were subsequently transferred to the post-anesthesia recovery area where continuous monitoring of SpO₂ and HR was performed, along with serial MOAA/S assessments conducted at one-minute intervals until discharge criteria were met.
Intraprocedural hemodynamic and respiratory management followed a standardized protocol. For hypotension accompanied by HR < 55 bpm, intravenous ephedrine (5–10 mg IV) was administered. Isolated hypotension with normal HR was treated with metaraminol (0.2–0.5 mg IV). Hypertensive episodes received urapidil (10–15 mg IV), while tachycardia (HR > 110 bpm) was managed with esmolol (10 mg IV). Significant bradycardia (HR < 50 bpm) without hypotension warranted atropine (0.3–0.5 mg IV). Respiratory depression prompted immediate intervention with 10 L/min oxygen and jaw-thrust maneuver. If SpO₂ remained <90% for >10 seconds, sustained manual compression was applied to the lower anterior chest wall to increase intrathoracic pressure, assist exhalation, and improve alveolar ventilation. Persistent hypoxemia necessitated the suspension of the procedure for mask ventilation, with tracheal intubation reserved for refractory cases. All interventions were meticulously documented. Postprocedural monitoring continued for 20 minutes in the recovery area; patients meeting discharge criteria (stable vitals, MOAA/S = 5) were transferred to the rest area with family accompaniment.
Outcome Measures
Primary Outcome Measures
1. The incidence of hypotension: Hypotension was defined as the MAP < 65 mmHg or a decrease of 20% from baseline and lasted for more than 10 seconds.25 The incidence of hypotension was determined by dividing the number of subjects who experienced hypotension by the total number of subjects in each respective group.
2. Hemodynamic parameters: Continuous monitoring of SBP, DBP, MAP, HR, CO, and SVR was conducted using CNAP monitor. Baseline values were established at 2 minutes prior to anesthesia induction (T0), with subsequent measurements recorded immediately following endoscope insertion (T1) and thereafter at 5-minute intervals throughout the procedure duration.
Secondary Outcome Measures
1. Procedure-related adverse events: Hypertension (MAP >105 mmHg or an increase of more than 20% above baseline levels that persisted for over 10 seconds26), bradycardia (HR < 50 bpm), tachycardia (HR > 110 bpm) and respiratory depression (SpO₂ < 94% persisting for > 10 seconds).
2. Recovery time: Interval from procedure completion to the first of three consecutive MOAA/S scores of 5.
3. Postoperative adverse effects, such as the incidence of dizziness, postoperative nausea and vomiting (PONV).
Data Analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY), with all continuous variables initially evaluated for normality using the Kolmogorov–Smirnov test. Normally distributed data were expressed as means ± SD and analyzed using independent Student’s t-tests for between-group comparisons or paired t-tests for within-group pre-post analyses. Non-normally distributed data were presented as medians (interquartile range) analyzed using Mann–Whitney U-tests for between-group comparisons or Wilcoxon signed-rank tests for within-group analyses. Categorical variables were expressed as frequencies (percentages) and compared using chi-square or Fisher’s exact tests as appropriate. Longitudinal data were analyzed using generalized estimating equations (GEE) to account for repeated measurements. A p-value < 0.05 (two-sided) was considered statistically significant.
Results
A total of 313 elderly hypertensive patients were screened. 93 were excluded: declined participation (n = 6), age > 75 years (n = 14), irregular treatment or poorly controlled blood pressure (n = 39), cardiac function class of NYHA ≥ III (n = 12), history of significant cardiac conditions (n = 15), secondary hypertension (n = 7). A total of 220 patients were randomized equally to group R (n = 110) and group P (n = 110) (Figure 1). The demographic characteristics of the patients were presented in Table 1, and no statistically significant differences were observed among the groups. (p > 0.05, Table 1).
 |
Table 1 Patient Characteristics |
 |
Figure 1 Patient flowchart with CONSORT guidelines. |
The Incidence of Hypotension and the Dosage of Vasoactive Drugs
The incidence of hypotension, demonstrated a statistically significant difference between groups, occurring in 37.3% (41/110) of group R patients compared to 72.7% (80/110) in group P (p < 0.001). During the procedure, none of the patients in either group received esmolol or urapidil, whereas the usage of ephedrine and metaraminol was lower in group R than group P (p < 0.05), as detailed in Table 2. However, there was no significant difference in the usage of atropine (p > 0.05).
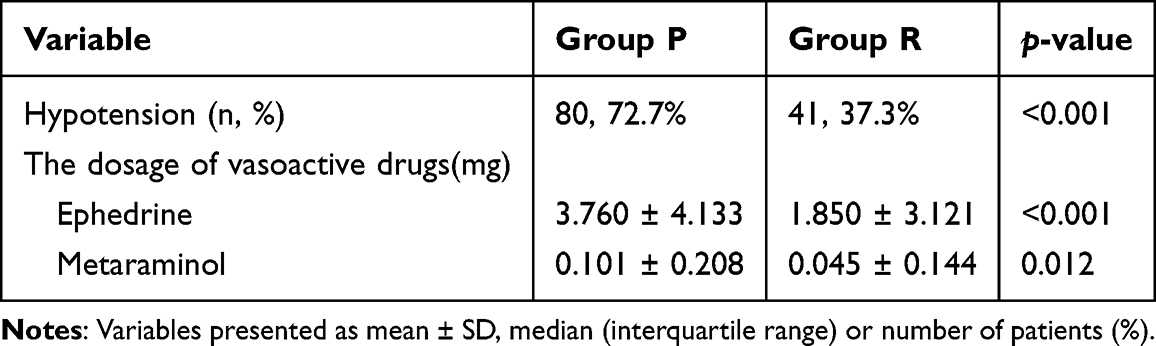 |
Table 2 The Incidence of Hypotension and Dosage of Vasoactive Drugs |
Comparison of Intraoperative Hemodynamic Indicators
The changes in the hemodynamic parameters during sedation are presented in Figure 2. At time point T0, there were no differences in MAP, HR, CO, and SVR between the two groups (p > 0.05). Following endoscope insertion (T1) and at subsequent 5-minute intervals (T2-T4), group R maintained significantly elevated MAP and HR relative to group P (all p < 0.05, Figures 2A and B), while CO and SVR remained similar between groups (p > 0.05, Figures 2C and D). Relative to baseline (T0), both groups exhibited significant reductions in MAP, CO, and SVR at T1 (all p < 0.001; Figures 2E, G-H). However, while group P showed significant HR reduction (p <0.001), group R maintained more stable HR (T1 vs T0: p = 0.084, Figures 2F).
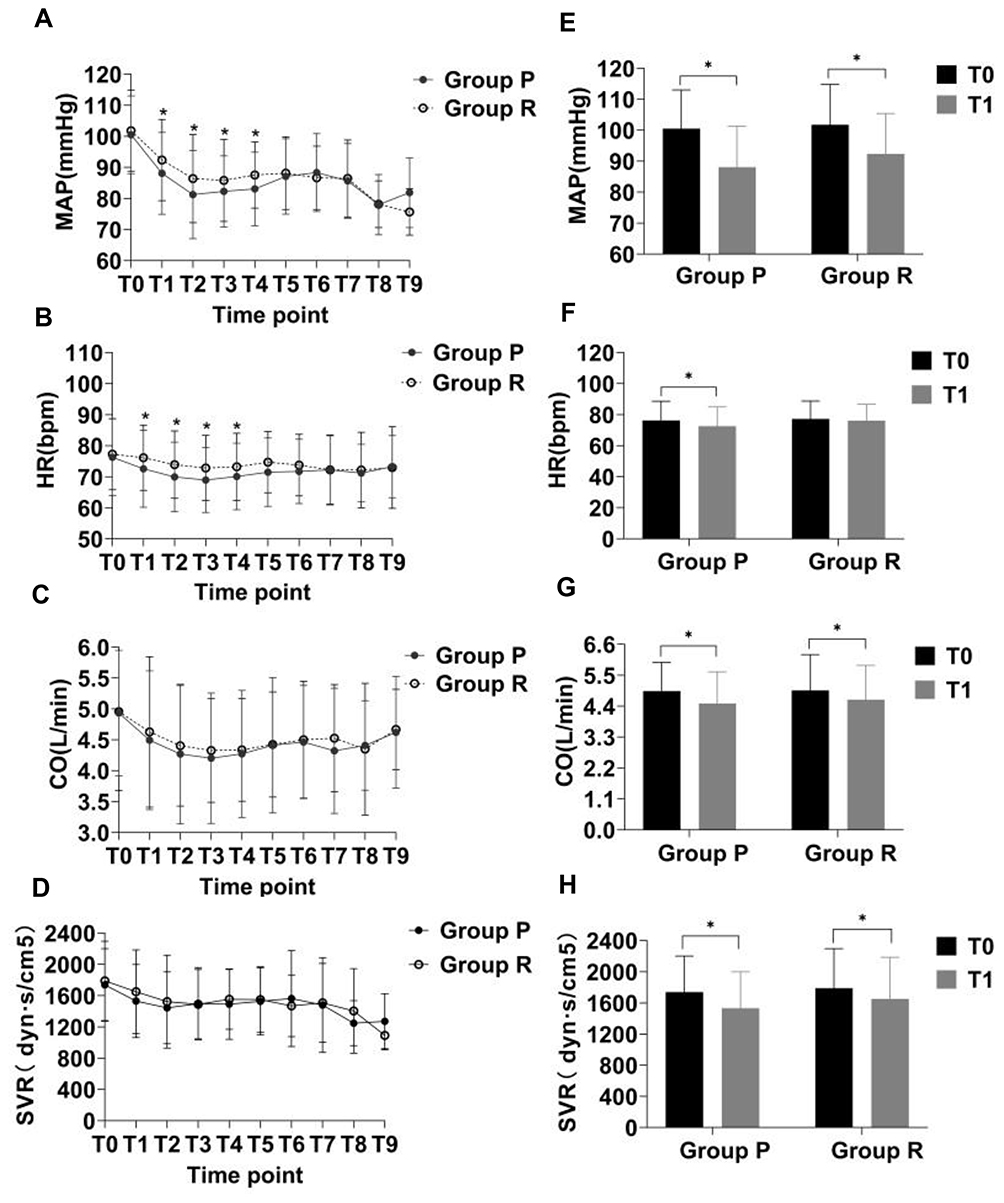 |
Figure 2 Changes in vital signs against elapsed sedation time. (A) MAP at different time points between the two groups; (B) HR at different time points between the two groups; (C) CO at different time points between the two groups; (D) SVR at different time points between the two groups; (E) Comparison of MAP changes at T0 and T1 in each group; (F) Comparison of HR changes at T0 and T1 in each group; (G) Comparison of CO changes at T0 and T1 in each group; (H) Comparison of SVR changes at T0 and T1 in each group. Group P: Group propofol, Group R: Group remimazolam. T0: 2 minutes before anesthesia induction, T1: at the time of endoscope entry, T2: 5 min after the operation, T3: 10 min after the operation, T4: 15 min after the operation, T5: 20 min after the operation, T6: 25 min after the operation, T7: 30 min after the operation, T8: 35 min after the operation, T9: 40 min after the operation. (*p < 0.05). Abbreviations: MAP, Mean arterial pressure; HR, Heart rate; CO, Cardiac Output; SVR, Peripheral vascular resistance. |
Adverse Events and Postoperative Follow-Up
No cases of tachycardia or postoperative re-sedation were reported in either group. Intraoperative hypertension occurred in only one propofol-treated patient (0.9%), which resolved spontaneously without vasoactive drugs following brief procedure suspension, while no hypertension cases were observed in the remimazolam group (p > 0.05). Group R demonstrated significantly lower rates of respiratory depression (34.5% vs 55.5%, p < 0.001) and bradycardia (7.3% vs 16.4%, p = 0.008) compared to group P.
However, group R showed a higher incidence of intraoperative body movements and cough (both p < 0.05), all of which were successfully managed with supplemental sedation without procedural interruptions, and there were no cases of sedation failure. The incidence of intraoperative arrhythmia and hiccups showed no significant differences between the groups (p > 0.05).
During 24-hour follow-up, PONV rates were 5.5% (propofol) versus 0.9% (remimazolam) (p = 0.124), while dizziness occurred in 30.9% (propofol) and 33.6% (remimazolam) of cases (p = 0.665), with no statistical difference, as comprehensively detailed in Table 3.
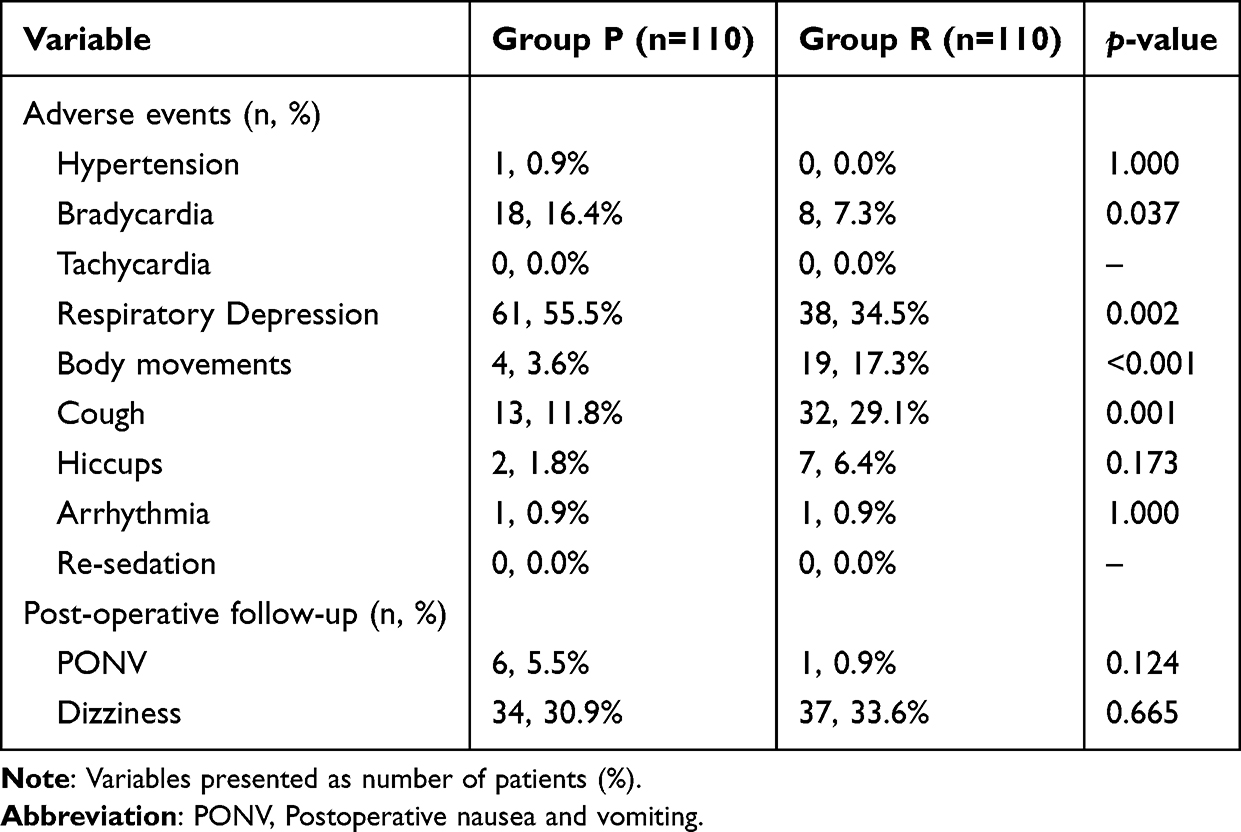 |
Table 3 Adverse Events and Post-Operative Follow-Up |
Procedure Time and Recovery Time
There were no significant differences in gastroscopy time, and colonoscopy time between the two groups (p > 0.05). Compared to group P, patients in group R had shorter recovery time following flumazenil administration [2 (range 2 to 3) vs 5 (range 4 to 6), p < 0.001]. As depicted in Table 4.
 |
Table 4 Procedure and Sedation-Related Outcomes |
Discussion
This randomized clinical trial aimed to evaluate the hemodynamic effects of remimazolam and propofol when administered in combination with sufentanil to elderly hypertensive patients undergoing painless gastroenteroscopy. The remimazolam induction dose of 0.3 mg/kg was determined based on comprehensive evidence from a recent meta-analysis of seven endoscopic studies, which demonstrated that doses exceeding 0.2 mg/kg provided optimal balance between procedural efficacy and safety profile.27 This is further supported by population pharmacodynamic modeling studies confirming the appropriateness of this dosage without the need for age-related adjustment in elderly patients.28 For propofol, the 1.5 mg/kg induction dose was selected in accordance with established dosing regimens from previous geriatric sedation studies.10
Our studies demonstrate that remimazolam offers superior hemodynamic stability, with significantly lower rates of hypotension compared to propofol. Additionally, remimazolam was associated with a reduced risk of respiratory depression. However, the incidence of intraoperative body movements and cough was higher in patients sedated with remimazolam than in those sedated with propofol. Notably, remimazolam facilitates a quicker recovery of consciousness when combined with flumazenil. Furthermore, remimazolam did not increase the risk of postoperative adverse reactions, such as dizziness, PONV.
Our findings are consistent with previous studies demonstrating remimazolam’s favorable hemodynamic profile in elderly patients.29,30 However, the incidence of hypotension remained relatively high in both group R and group P in our study (37.3% vs 72.7%)—a significant increase over the rates reported by Dong et al.25 Several explanations include: (1) Our study specifically enrolled elderly hypertensive patients, a population with diminished physiological reserve and impaired metabolic regulation, resulting in prone to disturbance of water and electrolyte metabolism (such as hypovolemia, hypokalemia, hyponatremia, etc.) in the intestinal preparation stage, increasing the risk of perioperative hemodynamic instability. Additionally, some researchers have found that adult hypertensive patients scheduled for elective noncardiac surgery under general anesthesia are more likely to develop post-induction hypotension than normotensive patients.31 (2) We utilized the CNAP system (CNSystems Medizintechnik AG, Graz, Austria), a continuous noninvasive blood pressure monitoring technology based on vascular unloading principles, while providing beat-to-beat arterial waveform analysis and hemodynamic parameters (CO, SVR, HR).22 However, NIBP cannot be continuously monitored, and may miss approximately 20% of hypotensive episodes and detect another 20% with delay.21
In the comparative analysis of hemodynamic parameters, both remimazolam (group R) and propofol (group P) cohorts exhibited comparable reductions in MAP, CO, and SVR at time point T1 relative to baseline (T0). However, a significant intergroup difference emerged in HR changes: group P demonstrated a significant reduction in HR, whereas group R maintained HR stability throughout the procedural period. Notably, compared with group P, patients in group R exhibited significantly elevated MAP and HR at time points T1, T2, T3, and T4. Concurrently, the incidence of clinically relevant hypotension and bradycardia was markedly reduced in group R, accompanied by a diminished requirement for vasoactive pharmacological intervention. These findings collectively indicate that remimazolam confers superior hemodynamic stability in elderly hypertensive patients undergoing painless gastroenteroscopy. The observed hemodynamic differences may be attributed to the distinct pharmacological properties of these agents. Propofol exerts vasodilatory effects primarily through blockade of calcium and potassium channels in vascular smooth muscle, resulting in decreased systemic vascular resistance and subsequent hypotension.32 In contrast, remimazolam appears to preserve hemodynamic stability through sympathetic activation, a characteristic shared with other benzodiazepines, which mitigates its potential depressant effects on cardiovascular function.10
Respiratory complications represent a significant safety concern in procedural sedation. Current evidence indicates that propofol administration during gastroenteroscopy is associated with respiratory depression in 42.8% of cases (SpO₂ <90% for >10 seconds), including severe hypoxemia (SpO₂ <80%) in 11.9% of patients.33 In our study population, remimazolam demonstrated an improved respiratory safety profile, with hypoxemic events (SpO₂ <94% for >10 seconds) occurring in 34.5% of cases - representing a clinically meaningful 21% relative risk reduction compared to propofol. Our conclusions align with prior studies,10,25 while extending the evidence base for remimazolam’s application in high-risk populations.
Our study also evaluated the recovery time of remimazolam. We detected that the recovery time of remimazolam was significantly reduced; this may be due to the use of flumazenil as an antagonist after ceasing to infuse the remimazolam in group R, allowing patients to regain consciousness more quickly. This pharmacological reversal mechanism, unique to benzodiazepine-based anesthetics, enables prompt restoration of consciousness - a clinically significant advantage over propofol, which lacks an equivalent specific antagonist. However, this clinical benefit must be weighed against the risk of re-sedation, a recognized complication following flumazenil use. Prior research reported resedation in 22% patients within 15 minutes of postanesthesia care unit (PACU) admission.34 Accordingly, after the administration of flumazenil, patients should be monitored for re-sedation, respiratory depression, and other persistent or recurrent hypnotic effects for a sufficient time period.35 In our trail, the sedation time was relatively shorter, and the dosage of remimazolam was lower, so none of 220 patients experienced re-sedation.
This study still has some limitations. Firstly, sedation depth was assessed exclusively through MOAA/S score without incorporating objective measures such as bispectral index (BIS) or Narcotrend monitoring, potentially leading to excessive sedation. Secondly, this experiment did not include a remimazolam without flumazenil reversal group, preventing us from assessing the added benefit of flumazenil except for the advantages of remimazolam. Finally, this study only targeted elderly patients aged between 65 and 75, whether the results are also appropriate for very elderly patients remains uncertain. More trials are needed to verify those.
Conclusion
Remimazolam can be stably and effectively used in elderly hypertensive patients during gastroenteroscopy. Compared with propofol, remimazolam provides superior hemodynamic stability, characterized by significantly lower rates of hypotension and other sedation-related adverse events.
Abbreviations
ASA, American Society of Anesthesiologists; BMI, Body Mass Index; CO, Cardiac Output; DBP, Diastolic Blood Pressure; HR, Heart rate; MAP, Mean Arterial Pressure; PONV, Postoperative nausea and vomiting; SBP, Systolic Blood Pressure; SpO2, peripheral oxygen saturation; SVR, Systemic Vascular Resistance.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding author if reasonable.
Ethics Statement
This study was approved by Ethics Committee of Medical Research and New Medical Technology of Sichuan Cancer Hospital (SCCHEC-02-2023-145) and written informed consent was obtained from all subjects participating in the study.
Acknowledgments
The authors thank the Gastrointestinal Endoscopy Center and the Department of Anesthesiology for their help and support (Sichuan cancer hospital, Sichuan Provincial People’s Hospital and Xichang People’s Hospital).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Healthcare Committee of Sichuan Province (2023-805); Anesthesia special research project of Sichuan Medical Association (2024HR76).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-lancet commission. Lancet. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
2. Schonberger RB, Dai F, Michel G, et al. Association of propofol induction dose and severe pre-incision hypotension among surgical patients over age 65. J Clin Anesth. 2022;80:110846. doi:10.1016/j.jclinane.2022.110846
3. Sneyd JR, Absalom AR, Barends CRM, Jones JB. Hypotension during propofol sedation for colonoscopy: a retrospective exploratory analysis and meta-analysis. Brit J Anaesth. 2022;128(4):610–622. doi:10.1016/j.bja.2021.10.044
4. Takaki R, Yokose M, Mihara T, et al. Hypotension after general anaesthesia induction using remimazolam or propofol in geriatric patients undergoing sevoflurane anaesthesia with remifentanil: a single-centre, double-blind, randomised controlled trial. Brit J Anaesth. 2024;133(1):24–32. doi:10.1016/j.bja.2024.04.013
5. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
6. Tang L, Ye C, Wang N, et al. The median effective doses of propofol combined with two different doses of nalbuphine for adult patients during painless gastroscopy. Front Pharmacol. 2022;13:1014486. doi:10.3389/fphar.2022.1014486
7. Hao L, Hu X, Zhu B, Li W, Huang X, Kang F. Clinical observation of the combined use of propofol and etomidate in painless gastroscopy. Medicine. 2020;99(45):e23061. doi:10.1097/MD.0000000000023061
8. Park S, Choi SL, Nahm FS, Ryu JH, Do SH. Dexmedetomidine-remifentanil vs propofol-remifentanil for monitored anesthesia care during hysteroscopy. Medicine. 2020;99(43):e22712. doi:10.1097/MD.0000000000022712
9. Sneyd JR, Gambus PL, Rigby-Jones AE. Current status of perioperative hypnotics, role of benzodiazepines, and the case for remimazolam: a narrative review. Brit J Anaesth. 2021;127(1):41–55. doi:10.1016/j.bja.2021.03.028
10. Hu B, Jiang K, Shi W, et al. Effect of remimazolam tosilate on respiratory depression in elderly patients undergoing gastroscopy: a multicentered, prospective, and randomized study. Drug Design Dev Ther. 2022;16:4151–4159. doi:10.2147/DDDT.S391147
11. Lohmer LL, Schippers F, Petersen KU, Stoehr T, Schmith VD. Time-to-event modeling for remimazolam for the indication of induction and maintenance of general anesthesia. J Clin Pharmacol. 2020;60(4):505–514. doi:10.1002/jcph.1552
12. Kleiman RB, Darpo B, Thorn M, Stoehr T, Schippers F. Potential strategy for assessing QT/QTc interval for drugs that produce rapid changes in heart rate: electrocardiographic assessment of the effects of intravenous remimazolam on cardiac repolarization. Brit J Clin Pharmacol. 2020;86(8):1600–1609. doi:10.1111/bcp.14270
13. Hu Q, Liu X, Wen C, Li D, Lei X. Remimazolam: an updated review of a new sedative and anaesthetic. Drug Design Dev Ther. 2022;16:3957–3974. doi:10.2147/DDDT.S384155
14. Stöhr T, Colin PJ, Ossig J, et al. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Brit J Anaesth. 2021;127(3):415–423. doi:10.1016/j.bja.2021.05.027
15. Zhu X, Wang H, Yuan S, et al. Efficacy and safety of remimazolam in endoscopic sedation—a systematic review and meta-analysis. Front Med. 2021;8:655042. doi:10.3389/fmed.2021.655042
16. Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543–553. doi:10.1007/s00540-020-02788-6
17. Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34(4):491–501. doi:10.1007/s00540-020-02776-w
18. Guo J, Qian Y, Zhang X, Han S, Shi Q, Xu J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: a prospective, randomized and controlled study. BMC Anesthesiol. 2022;22(1):180. doi:10.1186/s12871-022-01713-6
19. Qiu Y, Gu W, Zhao M, Zhang Y, Wu J. The hemodynamic stability of remimazolam compared with propofol in patients undergoing endoscopic submucosal dissection: a randomized trial. Front Med. 2022;9:938940. doi:10.3389/fmed.2022.938940
20. Zhou C, Wang X, Zhou M, et al. Comparison of remimazolam and propofol on post-induction hypotension in elderly hypertensive patients: a randomized controlled trial. Drug Design Dev Ther. 2025;19:3425–3435. doi:10.2147/DDDT.S510431
21. Dewhirst E, Corridore M, Klamar J, et al. Accuracy of the CNAP monitor, a noninvasive continuous blood pressure device, in providing beat-to-beat blood pressure readings in the prone position. J Clin Anesth. 2013;25(4):309–313. doi:10.1016/j.jclinane.2013.01.010
22. Flick M, Hoppe P, Matin Mehr J, et al. Non-invasive measurement of pulse pressure variation using a finger-cuff method (CNAP system): a validation study in patients having neurosurgery. J Clin Monitoring Computing. 2022;36(2):429–436. doi:10.1007/s10877-021-00669-1
23. Wagner JY, Körner A, Schulte-Uentrop L, et al. A comparison of volume clamp method-based continuous noninvasive cardiac output (CNCO) measurement versus intermittent pulmonary artery thermodilution in postoperative cardiothoracic surgery patients. J Clin Monitoring Computing. 2018;32(2):235–244. doi:10.1007/s10877-017-0027-x
24. Nicklas JY, Beckmann D, Killat J, et al. Continuous noninvasive arterial blood pressure monitoring using the vascular unloading technology during complex gastrointestinal endoscopy: a prospective observational study. J Clin Monitoring Computing. 2019;33(1):25–30. doi:10.1007/s10877-018-0131-6
25. Dong SA, Guo Y, Liu SS, et al. A randomized, controlled clinical trial comparing remimazolam to propofol when combined with alfentanil for sedation during ERCP procedures. J Clin Anesth. 2023;86:111077. doi:10.1016/j.jclinane.2023.111077
26. Gao W, Li J, Nguyen-Buckley C, et al. Intraoperative hypertension and thrombocytopenia associated with intracranial hemorrhage after liver transplantation. Transplantation. 2020;104(3):535–541. doi:10.1097/TP.0000000000002899
27. Zhao M-J, Hu H-F, Li X-L, Li XM, Wang DC, Kuang MJ. The safety and efficacy between remimazolam and propofol in intravenous anaesthesia of endoscopy operation: a systematic review and meta-analysis. Int J Surg. 2023;109(11):3566–3577. doi:10.1097/JS9.0000000000000638
28. Zhou J, Curd L, Lohmer LRL, et al. A population pharmacodynamic Markov mixed-effects model for determining remimazolam-induced sedation when co-administered with fentanyl in procedural sedation. CTS-Clin Transl Sci. 2021;14(4):1554–1565. doi:10.1111/cts.13023
29. Jeon Y-G, Kim S, Park J-H, et al. Incidence of intraoperative hypotension in older patients undergoing total intravenous anesthesia by remimazolam versus propofol: a randomized controlled trial. Medicine. 2023;102(49):e36440. doi:10.1097/MD.0000000000036440
30. Kuang Q, Zhong N, Ye C, Zhu X, Wei F. Propofol versus remimazolam on cognitive function, hemodynamics, and oxygenation during one-lung ventilation in older patients undergoing pulmonary lobectomy: a randomized controlled trial. J Cardiothoracic Vasc Anesth. 2023;37(10):1996–2005. doi:10.1053/j.jvca.2023.06.027
31. Zhang H, Gao H, Xiang Y, Li J. Maximum inferior vena cava diameter predicts post-induction hypotension in hypertensive patients undergoing non-cardiac surgery under general anesthesia: a prospective cohort study. Front Cardiovasc Med. 2022;9:958259. doi:10.3389/fcvm.2022.958259
32. Hasegawa G, Hirata N, Yoshikawa Y, Yamakage M. Differential effects of remimazolam and propofol on heart rate variability during anesthesia induction. J Anesth. 2022;36(2):239–245. doi:10.1007/s00540-022-03037-8
33. Goyal R, Hasnain S, Shreevastava S, Mittal S. A randomized, controlled trial to compare the efficacy and safety profile of a dexmedetomidine-ketamine combination with a propofol-fentanyl combination for ERCP. Gastrointest Endos. 2016;83(5):928–933. doi:10.1016/j.gie.2015.08.077
34. Oh EJ, Chung YJ, Lee JH, et al. Comparison of propofol vs. remimazolam on emergence profiles after general anesthesia: a randomized clinical trial. J Clin Anesth. 2023;90:111223. doi:10.1016/j.jclinane.2023.111223
35. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med. 2022;17(1):1–11. doi:10.17085/apm.21115
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Study About Different Doses of Remimazolam in Short Laparoscopic Surgery: A Randomized Controlled Double-Blind Trial
Luo L, Jiang J, Zhang M, Guo Z, Zhang X, Wang F, Yang F
Therapeutics and Clinical Risk Management 2023, 19:829-837
Published Date: 20 October 2023
Effect of Remimazolam on Induction and Maintenance of General Anesthesia in Kidney Transplant Patients
Chen L, Qin W, Wu J, Zhao G, Jiang X, Li M, Huang Z, Du X
International Journal of General Medicine 2024, 17:2455-2463
Published Date: 28 May 2024
Comparing Remimazolam and Propofol for Postoperative Anesthesia Satisfaction in Outpatient Gynecological Surgery: A Randomized Clinical Trial
Wang XL, Dai LL, Li YN, Zhang JW, Qu MC, Zhou YY, Xing N
Drug Design, Development and Therapy 2024, 18:4615-4627
Published Date: 18 October 2024
Comparing Cognitive Recovery of Remimazolam versus Propofol in Elderly Patients Undergoing Colonoscopy: A Randomized Controlled Trial

Lin S, Wei Y, Zhuo Y, Que S, Jin X, Yao Y, Qian B
Clinical Interventions in Aging 2024, 19:2133-2143
Published Date: 16 December 2024
Comparison of Remimazolam and Propofol on Post-Induction Hypotension in Elderly Hypertensive Patients: A Randomized Controlled Trial
Zhou C, Wang X, Zhou M, Guo S, Qi Y, Sun J, Wang L
Drug Design, Development and Therapy 2025, 19:3425-3435
Published Date: 29 April 2025