")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Effect of Ramadan Fasting on Blood Glucose Level in Pregnant Women with Gestational and Type 2 Diabetes
Authors Alsulami SS , Ghamri KA
Received 6 July 2023
Accepted for publication 2 October 2023
Published 6 October 2023 Volume 2023:16 Pages 3105—3113
DOI https://doi.org/10.2147/DMSO.S429249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Antonio Brunetti
Salhah S Alsulami,1 Kholoud A Ghamri2
1Department of Medicine, Faculty of Medicine Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia; 2Internal Medicine Department, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Salhah S Alsulami, Department of Medicine, Faculty of Medicine Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia, Tel +966563681890, Email [email protected]
Background: Pregnant women with diabetes are strongly advised against Ramadan fasting and have religious exemption, but a large proportion still choose to fast. Unfortunately, there is little information about glycemic control in these patients. This study aims to determine the fasting and postprandial blood glucose levels and to predict the risk factors for hypoglycemia in pregnant women with type 2 diabetes mellitus (DM) and gestational DM (GDM) who fast during Ramadan.
Methods: A prospective cohort research was conducted at a single tertiary hospital between 2021 and 2023 on 70 pregnant women with GDM (n = 53) and type 2 DM (n = 17) in their second and third trimester. Their fasting and postprandial blood glucose levels during Ramadan were compared to those of the previous month, and hypoglycemia was defined as blood glucose levels less than 60 mg/dl. Binary regression was used to predict the risk variables for hypoglycemia.
Results: The GDM and type 2 DM groups were similar in terms of age, parity, number of fasting days, and number of daily fasting hours. Only 26.9% of the women who were permitted to fast were given special instructions for Ramadan fasting. Dietary intervention was more common in the GDM group, whereas insulin and metformin treatment were more common in the type 2 DM group. The fasting glucose level decreased significantly after Ramadan fasting in both groups, from 92.5 (17.4) mg/dl to 90 (17.13) mg/dl (p = 0.033). However, there were a significantly higher number of hypoglycemia events in the type 2 DM group. Further, type 2 DM was identified as a risk factor for hypoglycemia (OR = 6.23; 95% CI = 1.04– 37.54; P = 0.046.
Conclusion: The present findings indicate that Ramadan fasting may improve fasting glucose control. In addition, type 2 DM was identified as a risk factor for hypoglycemia.
Keywords: gestational diabetes, type 2 diabetes, pregnant women, cohort study, Ramadan fasting
Introduction
Diabetes is a common medical problem worldwide. Over the past thirty years, the worldwide prevalence of diabetes mellitus (DM) has been increasing. In Saudi Arabia, the prevalence of diabetes was 16.8% in 2010 and is expected to reach 19.8% in 2030; this would make Saudi Arabia the country with the third highest prevalence in the world, after Nauru and the UAE.1 The median prevalence of gestational DM (GDM) in the Middle East and North Africa is 12.9% (interquartile range, 8.4–24.5%).2 In Saudi Arabia, a large cohort study that included 14,568 women from the capital city of Riyadh revealed that the prevalence of GDM was 24.2% (95% CI: 23.4–25.1%) and that of pre-existing DM was 4.3% (95% CI: 3.9–4.7%).3 In a more recent study conducted on 347 pregnant women in Saudi Arabia, the prevalence of GDM was found to be 19.6%.4 With regard to pre-existing diabetes, a study conducted in Riyadh reported that 116 (3.7%) out of 3157 pregnant women had pre-existing diabetes: 57% had type I DM and 43% had type 2 DM.5 GDM and pre-existing DM in pregnant women are associated with maternal and neonatal risks such as preeclampsia, shoulder dystocia, the need for cesarean delivery, and neonatal macrosomia and hypoglycemia.6 Therefore, glucose monitoring and glycemic control are important in this group of patients.
Saudi Arabia is an Islamic state in which Ramadan fasting is widely practiced. Fasting during Ramadan is, in fact, one of Islam’s five pillars. Fasting traditionally lasts 29 to 30 days, with Muslims fasting from sunrise to sunset. The daily fasting period varies according to geographical location and season, and it typically ranges between 13 and 15 h in Saudi Arabia. During the fasting period, practitioners often refrain from eating, drinking, and taking medication. A typical Ramadan day begins with the pre-sunrise meal known as “Suhour”, which is followed by a fast. The fast is broken with the post-sunset meal known as “Iftar”. Iftar dishes are often high in carbohydrates and lipids, which can cause rapid changes in glucose levels that may have adverse effects on patients with diabetes. In fact, it has been reported that the number of hypoglycemia episodes is significantly higher during Ramadan than during other months in patients with type 1 diabetes.7 In 2005, the American Diabetes Association (ADA) published the first statement regarding the management of diabetes during Ramadan. According to the guidelines, pregnant women are advised not to fast, and those who decide to fast are advised to undergo more frequent monitoring and insulin adjustments.8 According to the latest updates on the management of diabetes during Ramadan, based on the consensus of the ADA and the European Association for the Study of Diabetes (EASD), pregnant women with diabetes or GDM are at high risk of negative maternal and fetal outcomes and are advised to avoid fasting.9 It has been reported that Ramadan fasting among women with type 1 and 2 diabetes increases the risk of hypoglycemia episodes.6 Despite this, 76% of high-risk patients choose to fast for Ramadan against medical advice, according to a report from Emarat.10 Further, according to a recent review, at least 80% of healthy Muslim women who are pregnant fast despite medical advice against it and religious exemptions, with more than 50% fasting for the entire month.11 However, this may not be cause for concern, because for pregnant women who do not have diabetes, fasting during Ramadan in the second trimester of pregnancy has been found to have some benefits: for example, it decreases excessive weight gain and the incidence of gestational diabetes.12
Although Ramadan fasting for pregnant women with GDM and pre-existing type 2 DM is considered risky and practiced against medical advice, there is very little information on the safety of this practice. Further, the results of the studies that have been conducted so far are not consistent. That is, while some studies have indicated that the occurrence of hypoglycemia is more common in pregnant women with GDM who fast than in those who do not fast during Ramadan,13–15 others have reported that pregnant women with GDM or pre-existing type 2 GDM were able to fast for more than 15 days without experiencing any hypoglycemic events.15–17 Thus, there is a clear need for more data on the safety of Ramadan fasting in this group of patients. In addition, the difference in the effects of Ramadan fasting on post-prandial and fasting glycemic control are unclear in this group.
The present study attempts to address the gaps in the literature discussed above by analyzing the incidence of hypoglycemia and postprandial and fasting glycemic control in a cohort of pregnant women with GDM or type 2 DM who were practicing fasting during Ramadan. Further, the risk factors for hypoglycemia in this group of patients was also investigated.
Methods
Patient Selection
This is a prospective cohort study in which pregnant patients with diabetes were recruited from a diabetes clinic at a single tertiary hospital in Jeddah, Saudi Arabia. The sample size calculation could not be conducted as there is a lack of information about it in this field. Participants were informed about the study by their physician and participated voluntarily; they provided their verbal consent before commencement of the study. Data collection was carried out from Ramadan 2021 through Ramadan 2023. In the first week of Ramadan, patients with GDM or type 2 DM in their second or third trimester of pregnancy who had chosen to fast and were on dietary, metformin, or insulin intervention were recruited. Patients with type 1 DM and those who refused to provide their consent were excluded. Out of 80 patients who were initially recruited, 6 patients with type 1 DM and 2 patients who did not fast were excluded. All the patients provided their consent prior to enrolment in the study, and 2 patients who did not provide their consent were further excluded. Thus, the final cohort included 70 patients.
Data Collection
The first round of data collection was carried out during the first week of Ramadan. Data on the following variables were collected when the patients visited the clinic: age, gravity, parity, previous occurrence of gestational diabetes, whether they were fasting against their physician’s advice, and whether they had received specific instructions for Ramadan fasting and had been asked about pre-Ramadan home glucose monitoring data (that is, their fasting and post-prandial glucose levels). In addition, the participants were instructed to measure their fasting glucose level 8 h after the Suhour meal, as well as their postprandial glucose level after both meals throughout the Ramadan month.
A second round of data collection was performed during the month following Ramadan, and the fasting and postprandial data from home glucose monitoring during the Ramadan month were reviewed. Additionally, the following information was collected: the number of days on which fasting was completed, the number of hypoglycemia events, the number of days on which the fast was broken due to either hypoglycemia or hyperglycemia, and the medications (and doses) taken to control hypoglycemia.
This research was carried out in compliance with the tenets of the Declaration of Helsinki and received the approval of the King Abdulaziz University Bioethics Unit (approval no. 323–21).
Statistical Analysis
The data collected were entered into an Excel sheet and analyzed using SPSS for Windows 20 (IBM New York, USA). We compared the clinical outcomes of participants with GDM to those of participants with type 2 DM. The normality of continuous variables was examined. Normally distributed variables were expressed as mean (SD), and non-normally distributed variables were expressed as median (IQR). Continuous variables were compared using the Mann–Whitney U-test or independent t-test, and categorical variables were compared using the chi-square or Fisher exact tests, according to whether they were normally or non-normally distributed. Glycemic control data before and throughout Ramadan were compared using the paired sample t-test. Participants were divided into two groups according to whether they had hypoglycemia episodes during Ramadan fasting. Hypoglycemia was defined as glucose level below 60 mg/dl. The hypoglycemia group included participants with one or more hypoglycemic episodes based on glucose levels measured at home during the Ramadan fasting period, and the non-hypoglycemic group included participants who did not have any hypoglycemia episode over the entire fasting period. The risk factors for hypoglycemia during Ramadan fasting were predicted using binary logistic regression, after controlling for cofounders such as age, parity, number of fasting hours, whether the participant was working during the fasting period, whether their physician had permitted them to fast, and education level. Diabetes type and management were assessed as independent factors. The significance level was set at 0.05.
Results
Participants’ Characteristics According to Type of Diabetes
Among the 70 women who were included in the final cohort, 53 (75.7%) had GDM and 17 (24.3%) had type 2 DM. The mean (SD) age of the participants was 35.5 (5.3) years and was comparable between the GDM and type 2 DM groups, and the median parity was 3 for both groups. A significantly greater proportion of women in the type 2 DM group than in the GDM group had previously experienced GDM (8 [47.1%] vs 10 [19.6%]; p = 0.05) and hypoglycemia (14 [82.4%] vs 21 [39.6%]; p = 0.004]).
The median number of fasting days and daily fasting hours, which were 29 (7) days and 13.5 (0.5) h, respectively, for the entire cohort, were comparable between the two groups. The median number of gestational weeks at which the month of Ramadan started was significantly greater in the GDM group than in the type 2 DM group (30 [7.5] weeks vs 25 [15.3] weeks; p = 0.036). This means that the women in the GDM group started fasting much later in their pregnancy. Further, fasting was approved by the physician in a significantly higher number of cases in the GDM group than in the type 2 DM group (23 [45.1%] vs 3 [17.6%]; p = 0.05). However, only 26.9% of the women in the entire cohort were provided with special education regarding the management of diabetes during fasting, although the percentage was similar between the groups. Insulin and insulin combined with metformin were used to manage hyperglycemia in a significantly higher percentage of patients in the type 2 DM group than in the GDM group (p = 0.002 for both). In contrast, diabetes was managed with dietary interventions and metformin in a significantly higher proportion of patients in the type 2 DM group than in the GDM group (p = 0.002 for both). The participants’ characteristics are listed in Table 1.
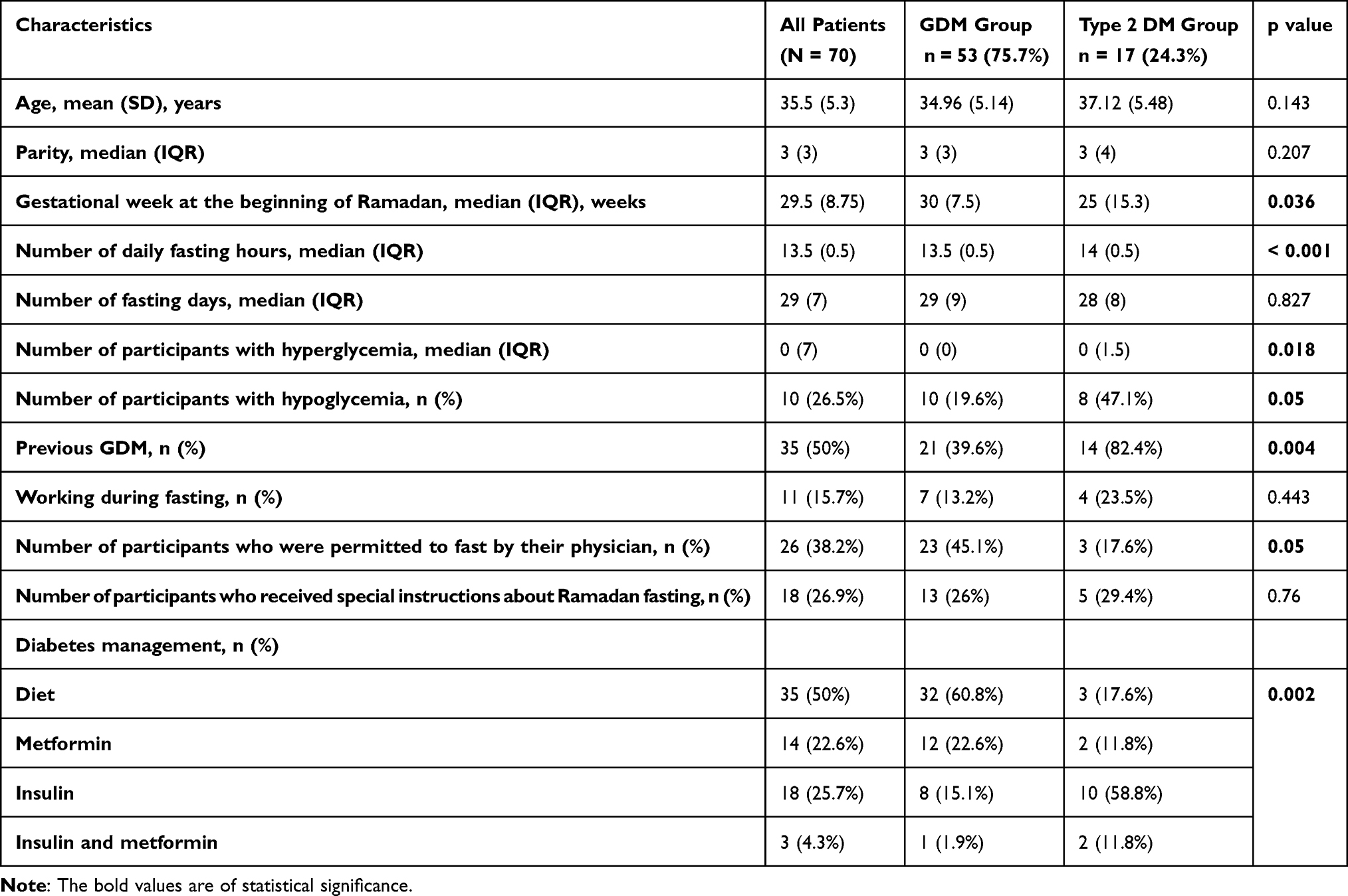 |
Table 1 Participants’ Characteristics are Categorized According to Diabetes Type |
Risk Factors for Hypoglycemia
A total of 50 (73.5%) participants completed Ramadan fasting without any hypoglycemic events. Among the patients who did report hypoglycemia events, there was a significantly higher percentage in the type 2 DM group than in the GDM group (8 [47.1%] vs 10 [19.6%]; p = 0.05). In addition, a higher percentage of patients who received insulin than those who received metformin developed hypoglycemia, but the difference was not significant (7 [38.9%] vs 3 [23.1%]; p = 0.434). The occurrence of hypoglycemia according to the demographic and clinical risk factors illustrated in Table 2.
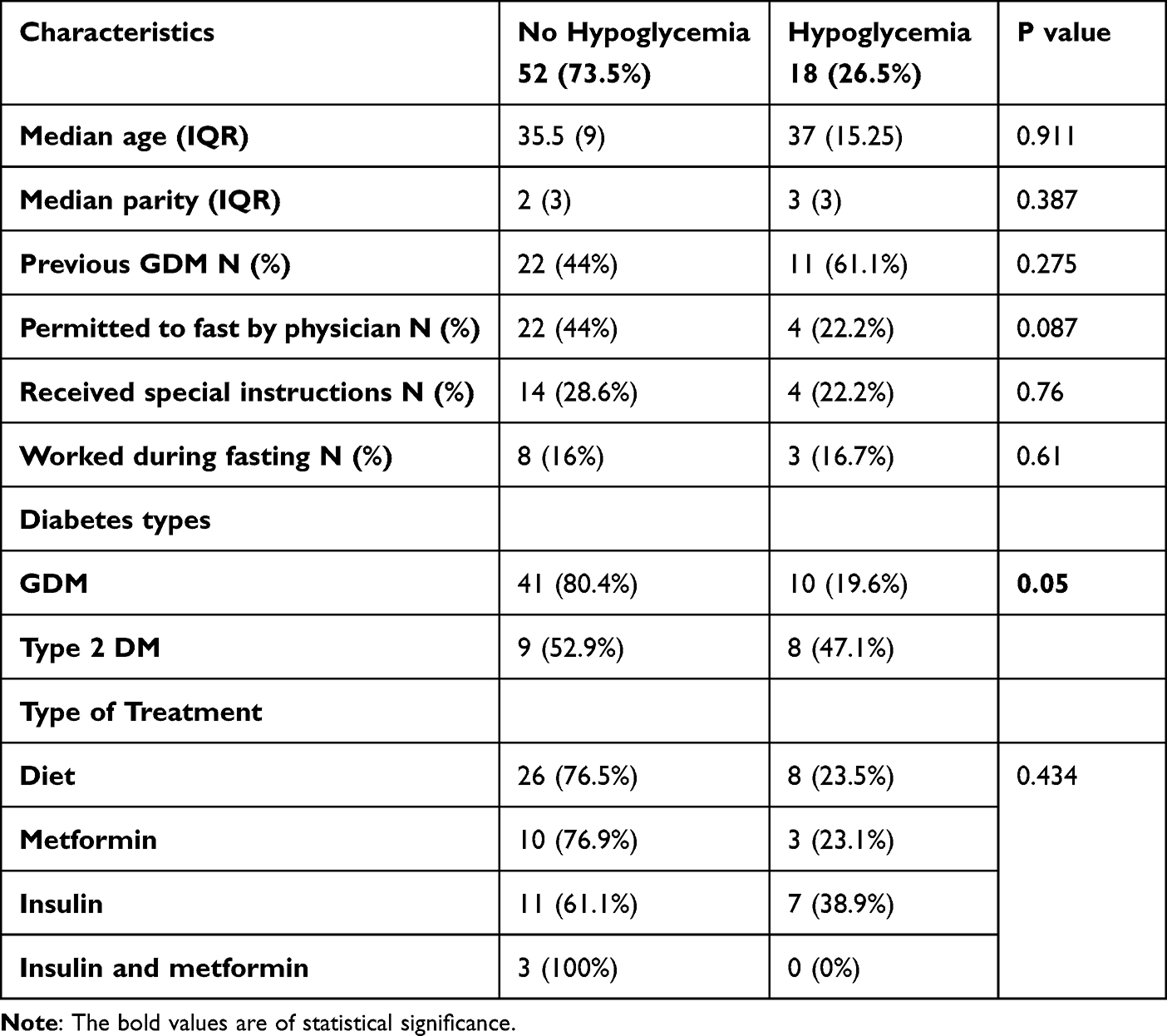 |
Table 2 Demographic and Clinical Risk Factors According to the Occurrence of Hypoglycemia |
Glycemic Control Before and Throughout Ramadan
Fasting glucose improved significantly during Ramadan, from 92.5 (17.4) mg/dl to 90 (17.13) mg/dl (p = 0.033), but there was no significant change in postprandial glucose before and during Ramadan (Table 3).
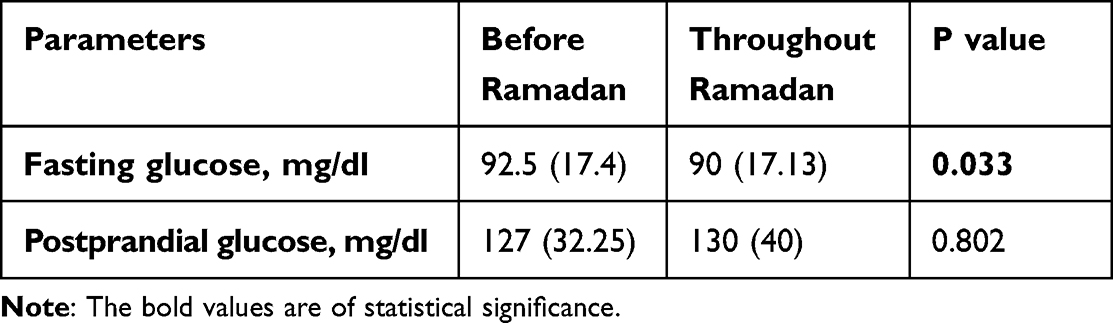 |
Table 3 Glycemic Control Before and Throughout Ramadan |
Predictors of Hypoglycemia During Ramadan Fasting
Binary logistic regression analysis was performed to assess the predictors of hypoglycemia, with diabetes type and management to control hyperglycemia evaluated as independent risk factors after adjusting for age, parity, number of fasting hours, whether the patients were working during the fasting period, whether their physician had permitted them to fast, and whether they had received special instructions for fasting. Type 2 DM emerged as an independent risk factor for hypoglycemia (OR: 6.23; 95% CI = 1.04–37.54; p = 0.046) (Table 4).
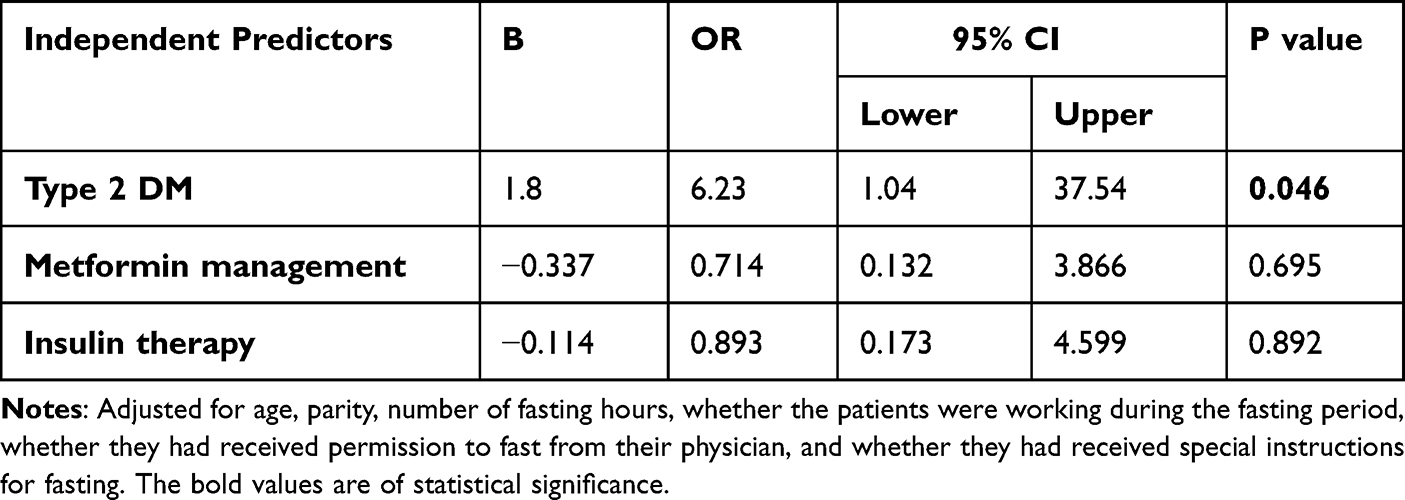 |
Table 4 Predictors of Hypoglycemia During Ramadan Fasting |
Number of Fasting Days Broken Because of Hypoglycemia and Hyperglycemia Episodes
The number of days on which the fast was broken due to hypoglycemia is illustrated in Figure 1. One patient with type 2 DM broke seven Ramadan fasting days due to hypoglycemic events. Additionally, one patient with type 2 DM broke four days of fast for the same reason. Further, four patients with type 2 DM and three with GDM broke one fasting day each due to hypoglycemia. The number of days on which fasting was broken due to hyperglycemia is illustrated in Figure 2. One patient with GDM broke their fast on 10 days, and one with type 2 DM broke their fast on 9 days due to hyperglycemia.
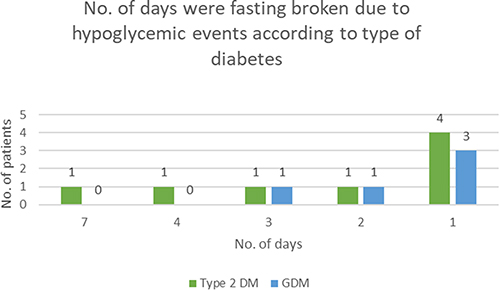 |
Figure 1 Number of days the fast was broken due to hypoglycemia. |
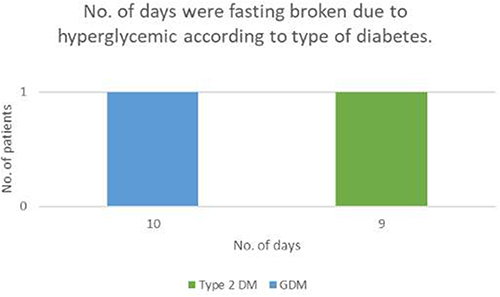 |
Figure 2 Number of days the fast was broken due to hyperglycemia. |
Discussion
The present study examines the effect of Ramadan fasting on the occurrence of hypoglycemia and patterns of fasting and postprandial glucose levels in a cohort of pregnant women with GDM and type 2 DM. The literature on this topic so far has mostly focused on GDM, and only one other study conducted in Iran has compared glycemic control between fasting pregnant women with GDM and type 2 DM.17 However, the previous study only included patients on insulin treatment, while the present one included patient on other regimens, too. Further, the effects of Ramadan fasting on postprandial and fasting glucose in pregnant women with diabetes have not been considered separately so far in a similar setting. Therefore, these findings present a new perspective on glycemic control in this group of patients and may help shape guidelines for monitoring and managing diabetes in pregnant women who choose to fast for Ramadan and ensuring their safety.
In this study, despite the comparable age and parity of the type 2 DM and GDM groups, both hypoglycemia and hyperglycemia were reported more frequently in the type 2 DM group. Accordingly, a smaller proportion of patients in the type 2 DM group than in the GDM group were permitted to fast by their physician. This is in contrast to the previous study from Iran that reported no hypoglycemia events in either the type 2 DM or GDM groups.17 Afandi et al and Hassanein et al reported that Ramadan fasting was associated with an increase in hypoglycemia events in pregnant women with GDM.14,15 However, these studies included only pregnant women with GDM and not type 2 DM. Nonetheless, the significantly higher number of events reported in the type 2 DM group in the present study may point to the need for more close glucose monitoring and individualized treatment modifications in pregnant women with type 2 DM who practice Ramadan fasting.
The fasting glucose levels showed a significant decrease over the Ramadan period in the present group of patients, but this trend was not observed in the postprandial glucose levels. Similarly, Azlin et al also reported a decrease in fasting glucose levels in pregnant women with GDM, type 1 DM, and type 2 DM over the Ramadan period.16 Further, the previous studies by Afandi et al and Hassanein et al also reported a decrease in blood glucose levels over the fasting period in pregnant women with GDM, but these studies did not distinguish between fasting and postprandial measurements.14,15 The decrease in fasting glucose levels observed in this study may be indicative of an improvement in glycemic control over the fasting period. Improvement in glycemic control, along with weight reduction, has been observed in other types of fasting, including intermittent fasting.18 This can be explained by the shift in the main source of energy from glucose to ketone bodies, which are potent regulators of body metabolism pathways, during fasting.19
The majority of the patients in the present study decided to fast against medical advice, and only 26.9% received special instructions on Ramadan fasting. An interesting observation was that a significantly higher proportion of patients in the GDM group were considered to be at low risk and had been permitted to fast by their physician. The most recent guidelines advice against Ramadan fasting in pregnant women with both GDM and type 1 or 2 DM.9 Further, as there is no evidence to indicate that Ramadan fasting may be safer in pregnant women with GDM than in pregnant women with type 2 DM, this is a trend that needs to be examined closely, perhaps through survey-based studies for physicians on the reasons for permitting fasting among certain patient groups. In addition, for women who choose to fast regardless of their physician’s advice, continuous glucose monitoring should be recommended as it has been proven to be more reliable for the detection of hypoglycemia events in women with GDM during Ramadan fasting.20 In general, it is recommended that the standards of care for pregnant women with type 2 DM who fast during Ramadan should be similar to those applied to high-risk patients with diabetes.15
In the current study, the majority of women with GDM were managed with dietary intervention and metformin, while the majority of women with type 2 DM were treated with dietary interventions, insulin, and insulin combined with metformin. As the number of hypoglycemia events were significantly lower in the GDM group, metformin could be considered to be safe in pregnant women with GDM during Ramadan fasting. However, in the current study, we did not specifically examine the safety of each of the regimens, so it is difficult to comment on whether insulin, metformin, dieting, or a combination of all three would be more beneficial in this group of women. Future investigations should focus on the optimal strategy for ensuring glycemic control and safety in pregnant women.
There are certain limitations of this study that need to be addressed. First, the sample was small, so the findings need to be confirmed in larger cohorts. Second, this was a single-center study, so studies on more centers are required to confirm the generalizability of the findings. Finally, larger studies comparing fasting and non-fasting groups are required to highlight the effects of Ramadan fasting on gestational weight gain, glycemic control, and metabolic control.
Conclusion
The present findings make an important contribution to what is known about glycemic control in pregnant women with diabetes who fast during Ramadan. The main findings that emerged were that Ramadan fasting improves fasting glucose control and that type 2 DM increases the risk of hypoglycemia. These findings point to the need for more close and careful monitoring of glucose levels and diabetes management strategies in pregnant women with diabetes who decide to fast during Ramadan. In addition, there is a clear need for future studies on the safety aspects of this practice and the diabetes interventions recommended.
Data Sharing Statement
The data used in this study can be made available upon request to the corresponding author (email: [email protected]).
Ethics Approval and Informed Consent
This research was carried out in compliance with the tenets of the Declaration of Helsinki and received the approval of the King Abdulaziz University Bioethics Unit (approval no. 323-21). In addition, all the patients provided their informed consent before the start of the study.
Consent for Publication
Consent for publication obtained.
Acknowledgments
We would like to acknowledge the help of all the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi:10.1016/j.diabres.2009.10.007
2. Zhu Y, Zhang C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: a global perspective. Curr Diab Rep. 2016;16(1):1–11. doi:10.1007/s11892-015-0699-x
3. Wahabi H, Fayed A, Esmaeil S, et al. Correction: Riyadh mother and baby multicenter cohort study: the cohort profile. PLoS One. 2016;11(12):e0168420. doi:10.1371/journal.pone.0168420
4. Alsaedi SA, Altalhi AA, Nabrawi MF, Aldainy AA, Razaz M. Wali prevalence and risk factors of gestational diabetes mellitus among pregnant patients visiting national guard primary health care centers in Saudi Arabia. Saudi Med J. 2020;41(2):144–150. doi:10.15537/smj.2020.2.24842
5. Wahabi HA, Esmaeil SA, Fayed A, Al-Shaikh G, Alzeidan RA. Pre-existing diabetes mellitus and adverse pregnancy outcomes. BMC Res Notes. 2012;5(1):1–5. doi:10.1186/1756-0500-5-496
6. Relph S, Patel T, Delaney L, Sobhy S, Thangaratinam S. Adverse pregnancy outcomes in women with diabetes-related microvascular disease and risks of disease progression in pregnancy: a systematic review and meta-analysis. PLoS Med. 2021;18(11):e1003856. doi:10.1371/journal.pmed.1003856
7. Salti I, Bénard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27(10):2306–2311. doi:10.2337/diacare.27.10.2306
8. Al-Arouj M, Bouguerra R, Buse J, et al. Recommendations for management of diabetes during ramadan. Diabetes Care. 2005;28(9):2305–2311. doi:10.2337/diacare.28.9.2305
9. Ibrahim M, Davies MJ, Ahmad E, et al. Recommendations for management of diabetes during Ramadan: update 2020, applying the principles of the ADA/EASD consensus. BMJ Open Diabetes Res Care. 2020;8(1):e001248. doi:10.1136/bmjdrc-2020-001248
10. Afandi B. Ramadan challenges: fasting against medical advice. J Fasting Health. 2017;5(3):1–5. doi:10.22038/JFH.2018.27312.1100
11. Kumar S, Diamond T. Ramadan fasting and maternal and fetal outcomes in pregnant women with diabetes mellitus: literature review. Front Endocrinol. 2022;13:900153. PMID: 35813638; PMCID: PMC9263982. doi:10.3389/fendo.2022.900153
12. Safari K, Piro TJ, Ahmad HM. Perspectives and pregnancy outcomes of maternal Ramadan fasting in the second trimester of pregnancy. BMC Pregnancy Childbirth. 2019;19(1):1–10. doi:10.1186/s12884-019-2275-x
13. Hui E, Reddy M, Bravis V, Rahman M, Darko D, Hassanein M. Fasting among pregnant women with diabetes during Ramadan. Int J Clin Pract. 2012;66(9):910–911. doi:10.1111/j.1742-1241.2012.02983.x
14. Afandi BO, Hassanein MM, Majd LM, Nagelkerke NJD. Impact of Ramadan fasting on glucose levels in women with gestational diabetes mellitus treated with diet alone or diet plus metformin: a continuous glucose study. BMJ Open Diabetes Res Care. 2017;5(1):e000470. PMID: 29299329 PMCID: PMC5728276. doi:10.1136/bmjdrc-2017-000470
15. Hassanein M, Abuelkheir S, Alsayyah F, et al. Evaluation of optimum diabetes care on glycemic control of patients with gestational diabetes during Ramadan fasting. Diabetes Res Clin Pract. 2012;173:108669. doi:10.1016/j.diabres.2021.108669
16. Nor Azlin MI, Adam R, Sufian SS, et al. Safety and tolerability of once or twice daily neutral protamine hagedorn insulin in fasting pregnant women with diabetes during Ramadan. J Obstet Gynaecol Res. 2010;37(2):132–137. doi:10.1111/j.1447-0756.2010.01330.x
17. Ismail NA, Olaide Raji H, Abd Wahab N, Mustafa N, Kamaruddin NA, Abdul Jamil M. Glycemic control among pregnant diabetic women on insulin who fasted during ramadan. Iran J Med Sci. 2011;36(4):254–259.
18. Obermayer A, Tripolt NJ, Pferschy PN, et al. Efficacy and safety of intermittent fasting in people with insulin-treated type 2 diabetes (INTERFAST-2)—A randomized controlled trial. Diabetes Care. 2023;46(2):463–468. doi:10.2337/dc22-1622
19. De Cabo R, Mattson MP. Effects of intermittent fasting on health, aging, and disease. New Engl J Med. 2019;381(26):2541–2551. doi:10.1056/NEJMra1905136
20. Afandi B, Hassanein M, Roubi S, Nagelkerke N. The value of continuous glucose monitoring and self-monitoring of blood glucose in patients with gestational diabetes mellitus during ramadan fasting. Diabetes Res Clin Pract. 2019;151:260–264. doi:10.1016/j.diabres.2019.01.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.