")
Back to Journals » International Journal of General Medicine » Volume 16
Effect of Prior Antibiotic Treatment on Blood Culture in an Outpatient Department of General Internal Medicine: A Retrospective Case–Control Analysis
Authors Hirosawa T , Sakamoto T, Hanai S , Harada Y , Shimizu T
Received 7 April 2023
Accepted for publication 23 June 2023
Published 29 June 2023 Volume 2023:16 Pages 2709—2717
DOI https://doi.org/10.2147/IJGM.S416235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Takanobu Hirosawa,1 Tetsu Sakamoto,1 Shogo Hanai,2 Yukinori Harada,1 Taro Shimizu1
1Department of Diagnostic and Generalist Medicine, Dokkyo Medical University, Shimotsuga, Tochigi, Japan; 2Departments of Microbiology and Infectious Diseases, Fujita Health University School of Medicine, Aichi, Japan
Correspondence: Takanobu Hirosawa, Department of Diagnostic and Generalist Medicine, Dokkyo Medical University, 880 Kitakobayashi, Mibu-cho, Shimotsuga, Tochigi, 321-0293, Japan, Tel +81 282 87 2498, Fax +81 282 87 2502, Email [email protected]
Purpose: The effect of antibiotics administered before blood cultures performed in general internal medicine outpatient settings is not well known.
Patients and Methods: We conducted a retrospective case–control study including adult patients who underwent blood cultures in the general internal medicine outpatient department of a Japanese university hospital between 2016 and 2022. Patients with positive blood cultures were included as cases and matched patients with negative blood cultures were included as controls. Univariable and multivariable logistic regression analyses were performed.
Results: A total of 200 patients and 200 controls were included. Antibiotics were administered prior to blood culture in 20% of patients (79/400). Oral antibiotics were prescribed to 69.6% of the prior antibiotics (55/79). Prior antibiotic use was significantly lower among patients with positive than negative blood cultures (13.5% vs 26.0%, p = 0.002) and was an independent predictive factor in univariable (odds ratio, 0.44; 95% confidence interval, 0.26– 0.73; p = 0.002) and multivariable (adjusted odds ratio, 0.31; 95% confidence interval, 0.15– 0.63; p = 0.002) logistic regression models for positive blood culture. The area under the receiver operating characteristic (AUROC) curve of the multivariable model for predicting positive blood cultures was 0.86.
Conclusion: There was a negative correlation between prior antibiotic use and positive blood cultures in the general internal medicine outpatient department. Therefore, physicians should interpret the negative results of blood cultures performed after the administration of antibiotics with care.
Keywords: bacteremia, fever, infection, antibacterial agent, antimicrobial, sepsis
Introduction
Sepsis is common and treatable, with an estimated 48.9 million cases annually worldwide and 11 million deaths.1 Sepsis is the most common cause of in-hospital deaths2 and the mortality was still high, contributing to a third to a half of all hospital deaths.3 To detect sepsis and the severe infectious diseases, blood cultures are essential tools.4 The positive blood culture rate is reduced by prior use of antibiotics.5,6 Therefore, it is common practice to obtain blood cultures from patients with suspected infection prior to antibiotic initiation. However, especially in the outpatient department, blood cultures were not drawn for more than half of the cases.7 A number of reasons can explain this discrepancy. Firstly, this is partly because routine blood cultures are rarely positive8 in patients presenting with common infectious diseases, including pneumonia,9,10 urinary tract infection,11,12 and cellulitis.13,14 These common infectious diseases do not cause bacteremia frequently. Some of common infectious diseases are caused by viral infections, which cannot be detected in blood cultures. Additionally, this may be partly because clinicians inappropriately prescribe broad-spectrum antibiotics7 or oral agents, which is certainly common in Japan15,16 without performing blood cultures.7 Moreover, there are limited published data17 and guidance18 regarding blood cultures in outpatient settings.
After initial empirical antibiotic treatment, patients with fever or inflammatory reactions tend to be referred from the primary care sites to the general internal medicine (GIM) outpatient department for further investigation. However, the effect of prior antibiotic administration on blood culture is not well known, especially in an outpatient setting. In this study, we evaluated the effects of prior antibiotics on blood culture in the GIM outpatient department. We also analyzed the predictive factors associated with positive blood cultures in that setting.
Materials and Methods
This retrospective case–control study included patients aged >15 years who underwent blood culture in the GIM outpatient department (Department of Diagnostic and Generalist Medicine) of Dokkyo Medical University Hospital, Shimotsuga, Tochigi, Japan, between 1st April 2016 and 31st March 2022. The hospital is a tertiary teaching hospital with 1195 beds. This study was conducted in accordance with the current version of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Dokkyo Medical University Hospital (No. R-62-15J). The approval date was September 16th 2022. Owing to the retrospective nature of the study and the study data were anonymous, the requirement for individual consent was waived by the ethics committee.
Patient Population and Case-Control Selection
During the 6-year observation period, 1849 adult outpatients (aged >15 years) had blood cultures (at least two bottles) taken from the GIM outpatient department. The mean age of all patients was 62.6 ± 20.6 (SD: standard deviation), and 46.9% were male. A total of 256 patients had positive blood culture results. Of these, 40 were interpreted as contamination (23 coagulase-negative Staphylococcus species, 14 Bacillus species, 2 Propionibacterium acnes, and one Corynebacterium species). A further nine were excluded because of follow-up blood culture, and seven were excluded as they had been transferred from other medical institutions where they had been previously hospitalized. The remaining 200 patients were enrolled in this study. Controls were matched in a 1:1 ratio with age and sex using the nearest neighbor propensity score by the R package “MatchIt”19 from 1593 blood culture negative. Patient inclusion, exclusion, and case–control matching are shown in Figure 1.
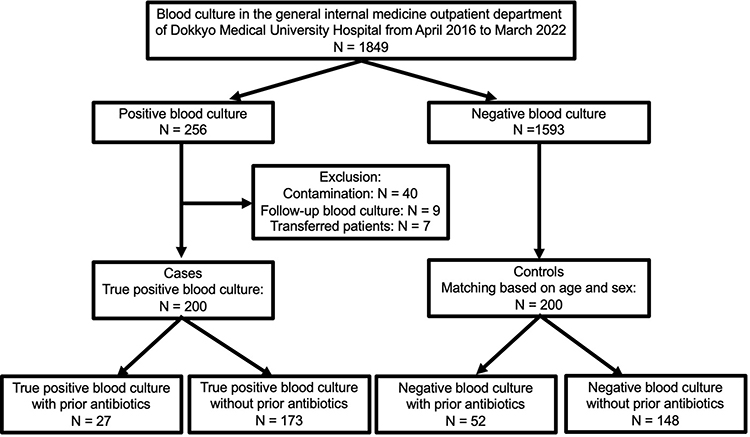 |
Figure 1 Flowchart of patient inclusion, exclusion, and case-control match. |
Outcome and Definition
The primary outcome was a positive blood culture indicative of a true positive blood culture, which is regarded as clinically pathognomonic. A positive blood culture was defined as the presence of a microorganism in at least one blood culture bottle. Bacterial contamination was excluded from analysis. Bacterial contamination was defined as the presence of coagulase-negative Staphylococcus, Bacillus, Propionibacterium acnes, or Corynebacterium species in only a single set of blood cultures.20
We used the quick sequential (sepsis-related) Organ Failure Assessment (qSOFA) score as an indicator of sepsis. The qSOFA was developed for the rapid identification of infected patients at a risk of mortality. This score identifies adult patients with suspected infection if they have at least two of the following clinical criteria: respiratory rate of 22 breaths/min or greater, altered mentation, or systolic blood pressure of 100 mmHg or less.21 Prior antibiotics were defined as those prescribed ≤2 weeks before performing the index blood culture.
Procedure
The decision to perform blood culture was made independently by the treating physicians based on the clinical situation of each patient. Blood (20 mL) was aseptically drawn from the blood vessels and the sample inoculated into aerobic and anaerobic culture bottles (Bactec Plus Aerobic/23F and Anaerobic/22F bottles; Becton Dickinson Instrument Systems, Sparks, MD, USA). This procedure was repeated using another vessel to yield two sets of blood cultures (four bottles). Blood culture bottles were incubated with BACTEC resin beads. The bottles were inspected for bacterial growth over 6 days. The incubation temperature was 35°C. A BACTEC-FX blood culture incubation system (Becton Dickinson) was used to isolate bacteria. Significant isolates were identified and tested for antimicrobial susceptibility according to the guidelines of the National Committee for Clinical Laboratory Standards guidelines.22 Matrix-assisted laser desorption ionization-time of flight mass spectrometry was used to confirm the identity of all isolated bacterial species.
Data Collection
Data on age, sex, number of blood cultures, and type of pathogen detected were extracted from the electronic database. Symptoms (fever, chills, and vomiting),23 comorbidities, vital signs (consciousness, body temperature, heart rate, blood pressure, respiratory rate, and SpO2), laboratory data (white blood cell count, neutrophil count, serum albumin, creatinine, and C-reactive protein), prior antibiotics, indications for blood culture, diagnosis, disposition, and hospital mortality were collected through medical chart review.
Regarding Charlson score, comorbidities included myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic obstructive pulmonary disease, collagen disease, ulcer disease, liver disease, hemiparesis, chronic kidney disease, diabetes, malignancy, leukemia, elevated liver function test, metastasis, acquired immune deficiency syndrome, and catheter insertion.24 Data on prior antibiotics included the class of antibiotics, route, and duration. Indications for blood culture were classified into the following categories: suspected focal infection (lower respiratory tract, urogenital, intra-abdominal, central line-associated, or skin or soft tissue infection), suspected endocarditis, unfocused fever (fever without a source), or other/unknown.23 Indications for blood culture and diagnosis were checked by two independent researchers (TH and TS). Discrepancies in judgments were resolved by consensus. Any covariate in symptoms, comorbidities, and prior antibiotics not noted as present was considered to be absent.
Analysis
We compared the baseline characteristics, including prior antibiotics, vital signs, laboratory data, admission, and hospital mortality, between positive blood cultures (cases) and negative blood cultures (controls). We then performed univariable and multivariable analyses for predictive factors and evaluated the diagnostic accuracy of the predictive models.
Continuous variables are presented as means and standard deviations or medians and interquartile ranges (IQR) and were compared using the Mann–Whitney U-test. Categorical or binary variables are presented as numbers (percentages) and were compared using the chi-squared test.
A logistic regression model was developed to identify factors associated with positive blood cultures. Odds ratios (ORs) and associated 95% confidence intervals (95% CI) were used to estimate the relative risks of potential predictors of positive blood culture in the univariable and multivariable logistic regression models. Variables with p < 0.05 in univariable analysis were included in the multivariable analysis. The diagnostic accuracy of the multivariable logistic regression models was assessed by calculating the corresponding area under the receiver operating characteristic (AUROC) curve. When vital signs or laboratory data were missing, patients were not included in the related univariable and multivariable logistic regression models. Statistical power analysis was performed using G*power version 3.1.9.6 (Department of Psychology of Heinrich Heine University, Düsseldorf, Germany). Statistical significance was defined as p < 0.05. All analyses were performed using R 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria), and the pROC package25 for MacOS X.
Results
Participant Profiles
Four hundred patients enrolled in the analysis. The mean age of all patients was 72.3 ± 13.7 (SD: standard deviation) years, and 51% (204/400) were male. Among the patients, 67% (268/400), 33.5% (134/400), and 11.3% (45/400) complained of fever, chills, and vomiting, respectively. The mean Charlson Score was 4.7 ± 2.5. Regarding indication of performing blood cultures, urogenital infection was the most frequent infection (27.8%, 111/400), followed by intra-abdominal infection (16%, 64/400), lower respiratory tract infection (14.5%, 58/400). Urogenital infection was also the most commonly diagnosed infection (28.5%, 114/400), followed by intra-abdominal infection (12.3%, 49/400), and lower respiratory tract infection (11%, 44/400).
20% is the percentage of patients with prior antibiotics in the overall cohort of cases and controls (79/400). Of these, 69.6% (55/79) were prescribed oral antibiotics. Fluoroquinolones were the most frequently used antibiotics (29.1%, 23/79), followed by cephalosporins (20.3%, 16/79), penicillins (13.9%, 11/79), and macrolides (12.7%, 10/79). The most common type of cephalosporins were third-generation (87.5%, 14/16), followed by first-generation (12.5%, 2/16).
Two hundred patients with true-positive blood cultures were identified. Polybacterial growth was detected in 9.5% of patients (19/200). Thirty-eight percent (76/200) were gram-positive organisms, while 51.5% (103/200) were gram-negative organisms. Escherichia coli was the most common pathogen (36.5%, 73/200), including six extended-spectrum beta-lactamase (ESBLs)-producing Escherichia coli. The second most found pathogen was Streptococcus spp. (19%, 38/200), including 5 cases of Streptococcus pneumoniae. The third most common pathogen was Staphylococcus spp. (12.5%, 25/200), including 17 methicillin-sensitive Staphylococcus aureus and 3 methicillin-resistant Staphylococcus aureus.
Patient characteristics, including baseline, comorbidity, symptoms, vital signs, and laboratory data of positive blood culture and negative blood culture, are summarised in Table 1. Regarding comorbidity and symptoms, patients with positive blood culture had significantly lower prior antibiotic use (13.5% vs 26.0%, p = 0.002), higher vomiting (16.0% vs 6.5%, p = 0.004), and higher past medical history of congestive heart failure (10.0% vs 4.0%, p = 0.02) than those with negative blood culture. In terms of vital signs, patients with a positive blood culture had a significantly higher qSOFA (mean 0.77 vs 0.39, p < 0.001), body temperature (38.3°C vs 37.5°C, p < 0.001), and heart rate (100.2/min vs 93.6/min, p < 0.001). Meanwhile, the diastolic blood pressure (72.2 mmHg vs 76.1 mmHg, p = 0.006) and SpO2 (95.8% vs 96.0%, p = 0.02) were low. In the laboratory data, patients with a positive blood culture had a significantly higher total white cell count (mean 12.1 x109/l vs 10.0 x109/l, p < 0.001), neutrophil count (10.8 x109/l vs 7.8 x109/l, p < 0.001), C-reactive protein (11.6 mg/dl vs 7.3 mg/dl, p < 0.001), and creatinine (1.5 mg/dl vs 1.1 mg/dl, p < 0.001). Meanwhile, platelet count (190 x109/l vs 237 x109/l, p < 0.001) and serum albumin (3.2 g/dl vs 3.5 g/dl, p = 0.004) were low. Patients with positive blood cultures had a significantly higher admission rate (85.5% vs 42.5%, p < 0.001) and different indications for blood culture (p < 0.001) than those without positive blood cultures. The details of comorbidities and final diagnoses are shown in Table S1.
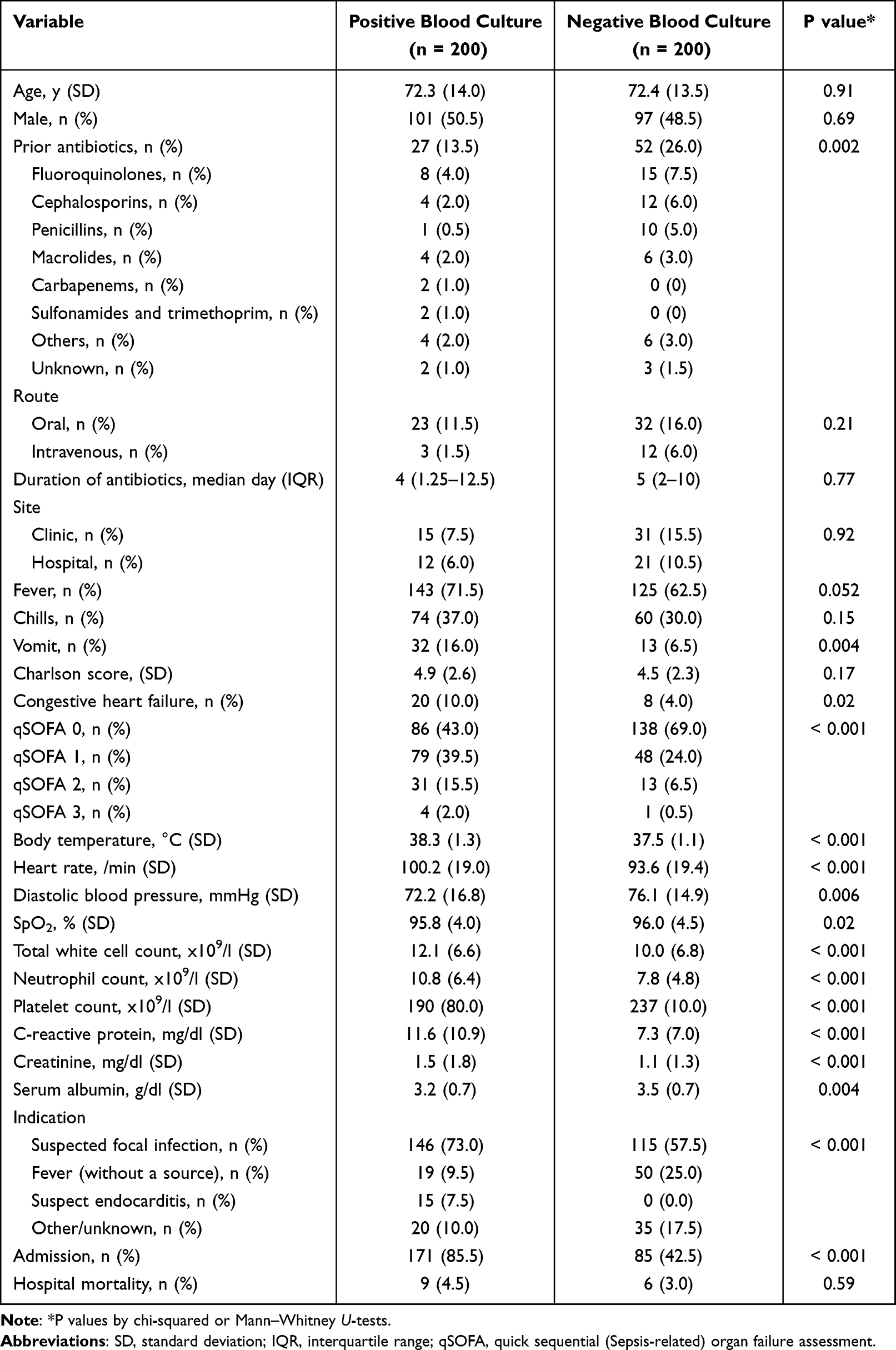 |
Table 1 Baseline, Symptoms, Comorbidity, Vital Sign, Laboratory Data, Admission, and Hospital Mortality of the Positive Blood Culture Group Compared to Negative Blood Culture Group |
Prior Antibiotics
The results of univariable and multivariable analyses are listed in Table 2. In univariable analysis, prior antibiotics were significantly lower among patients with positive blood cultures than in those with negative blood cultures (OR, 0.44; 95% CI, 0.26–0.73; p = 0.002). Prior antibiotic use remained an independent predictive factor for negative blood culture after adjustment for other variables in a multivariable logistic regression model (OR, 0.31; 95% CI, 0.15–0.63; p = 0.002).
 |
Table 2 Odds Ratios of Variables for Predicting Positive Blood Culture |
Power analysis revealed that the statistical power for prior antibiotic use between both groups exceeded 0.99.
Other Predictive Factors
Body temperature (OR 1.44; 95% CI 1.11–1.91), platelet count (OR 0.96; 95% CI 0.92–0.99), C-reactive protein (OR 1.05; 95% CI 1.01–1.09), and admission (OR 4.37; 95% CI 2.29–8.56) were independent predictive factors for positive blood cultures in the univariable and multivariable logistic regression models. The total white cell count (OR 1, 95% CI 1–1) and neutrophil count (OR 1; 95% CI 1–1) were not associated with positive blood cultures for the univariable and multivariable logistic regression models. Other predictive factors (vomiting, medical history of congestive heart failure, qSOFA, heart rate, diastolic blood pressure, creatinine, and serum albumin) were identified as significant predictive markers in univariable logistic regression models, but not in multivariable logistic regression models.
Predictive Models
The AUROC of the multivariable model was 0.86 (N=334). The model included the following predictors: prior antibiotics, vomiting, congestive heart failure, qSOFA score, body temperature, heart rate, diastolic blood pressure, total white cell count, neutrophil count, platelet count, C-reactive protein level, creatinine level, serum albumin level, and admission decision. The corresponding ROC curves are displayed in Figure 2.
 |
Figure 2 Area under the receiver-operating characteristic (AUROC) curves* of the multivariable model (0.86) associated with positive blood culture for the prior antibiotics, vomit, congestive heart failure, qSOFA, body temperature, heart rate, diastolic blood pressure, total white cell count, neutrophil count, platelet, c-reactive protein, creatinine, serum albumin, and admission decision. Abbreviation: qSOFA, Quick Sequential (Sepsis-Related) Organ Failure Assessment. Note: N = 334. |
Discussion
Principal Findings
Positive blood culture was significantly lower with prior antibiotics in the GIM outpatient department, not only in a univariable but also after adjustment for other variables in a multivariable logistic regression model. These results suggest that prior antibiotics masked the positive blood cultures in outpatient setting same as hospitalized setting.6 Therefore, physicians should carefully interpret the negative blood culture results obtained after the administration of antibiotics. Additionally, the predictive model combined with the historical variables, including prior antibiotics, vital signs, laboratory data, and admission decision, is useful for predicting a positive blood culture. The AUROC of the multivariable model was >0.85, indicating that the score had good discriminatory ability. Taken together, these results suggest that there is a low possibility that unknown important variables or unknown important confounding factors remained other than the variables investigated in this study. Therefore, prior antibiotic use was an important variable affecting positive blood cultures with a high degree of internal validity. In the real world, physicians carefully interpret the negative results of blood culture after initiation of antibiotics.
Comparison with Prior Work
When we predicted that the rate of prior antibiotics in the whole negative blood culture was the same as that of the controls, the predicted rates of positive blood cultures with and without prior antibiotics were 6% and 13%, respectively. Compared with a previous study,26 the absolute difference in the predicted proportion of positive blood cultures between those with and without prior antibiotics was relatively small (predicted differences 7% vs 12%). This was partly due to differences in the following: the setting between GIM outpatients and emergency departments, the study design between retrospective case-control and prospective studies, the primary outcome between positive blood culture and severe sepsis, and between countries as Japan is one of the most aged countries as compared to the United States.
In the previous Japanese trend of prescribed antibiotics, 93% were administered orally.15 The majority of prior antibiotics in this study were administered orally the same (approximately 70%) as in the previous study. In terms of the AUROC, our multivariable model (0.86) was better than the previous model (0.80) in the Emergency department.23
Limitations
This study had some limitations. The most important limitations are the study design, specifically this was a case–control study conducted in a single institution, and a single department. The controls were matched based on age and sex. However, the controls were not matched based on severity of the disease and probable site of infection. These limitations are the potential for selection biases. Second, the identification of predictors, including prior antibiotic use, has not been validated. Therefore, these results may not be well-generalizable outside of the population studied, especially to other medical systems where other trends of prescribed antibiotics pertain. In future, they should have been matched for severity of illness, probable site of infection, and prior antibiotics use with external validity. Third, the decisions to obtain blood cultures and to admit the patients were made individually by the attendant physicians without reference to particular standardized criteria. In this study, the true positive rate of blood cultures was 11%. This was an adequate positive rate of blood culture (6–12%) suggested by the American Society of Microbiology.27 However, there may have been risk to underdiagnosed the patients with true bacteremia. Additionally, the admission decision relied on complex clinical judgment; hence, further analysis is required to clarify the decision-making process for admission. Fourth, we did not perform a physical examination because of the lack of data. Indeed, the results of the predictive model would likely improve with the inclusion of physical examination. Fifth, we did not evaluate other techniques available to detect infections including patients with negative blood culturesfor example, real-time polymerase-chain reaction assay on whole-blood samples28 and multiplex PCR.29 Sixth, this study was conducted on medical chart review. There is the potential for information bias. In future studies, a full predictive model with standardized criteria, physical examination, and other techniques to detect infections should be investigated prospectively.
Conclusion
In summary, this study suggested a correlation between prior antibiotic use and negative blood cultures in the GIM outpatient department. Therefore, physicians should carefully interpret the negative blood culture results obtained after the administration of antibiotics.
Abbreviations
GIM, general internal medicine; SD, standard deviation; qSOFA, the quick Sequential (Sepsis-Related) Organ Failure Assessment; SpO2, oxygen saturation; IQR, interquartile range; OR, Odd ratio; AUROC, area under each receiver operating characteristic; CI, confidence interval; ESBL, Extended-spectrum beta-lactamase.
Acknowledgments
This study was made possible using resources from the Department of Diagnostic and Generalist Medicine, Dokkyo Medical University.
Disclosure
Dr. Yukinori Harada reports personal fees from PRECISION, Inc., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
2. Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90–92. doi:10.1001/jama.2014.5804
3. Cohen J, Vincent J-L, Adhikari NKJ, et al. Sepsis: a roadmap for future research. Lancet Infect Dis. 2015;15(5):581–614. doi:10.1016/S1473-3099(15)70112-X
4. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
5. Scheer CS, Fuchs C, Gründling M, et al. Impact of antibiotic administration on blood culture positivity at the beginning of sepsis: a prospective clinical cohort study. Clin Microbiol Infect. 2019;25(3):326–331. doi:10.1016/j.cmi.2018.05.016
6. Grace CJ, Lieberman J, Pierce K, Littenberg B. Usefulness of blood culture for hospitalized patients who are receiving antibiotic therapy. Clin Infect Dis. 2001;32(11):1651–1655. doi:10.1086/320527
7. Hase R, Hosokawa N. Patterns of outpatient ceftriaxone use in a Japanese general hospital: an increased need for development of outpatient parenteral antimicrobial therapy programs. Infect Dis. 2015;47(9):668–671. doi:10.3109/23744235.2015.1031174
8. Laupland KB, Church DL, Gregson DB. Blood cultures in ambulatory outpatients. BMC Infect Dis. 2005;5(1):35. doi:10.1186/1471-2334-5-35
9. Chalasani NP, Valdecanas MA, Gopal AK, McGowan JE, Jurado RL. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest. 1995;108(4):932–936. doi:10.1378/chest.108.4.932
10. Theerthakarai R, El-Halees W, Ismail M, Solis RA, Khan MA. Nonvalue of the initial microbiological studies in the management of nonsevere community-acquired pneumonia. Chest. 2001;119(1):181–184. doi:10.1378/chest.119.1.181
11. Karakonstantis S, Kalemaki D. Blood culture useful only in selected patients with urinary tract infections - a literature review. Infect Dis. 2018;50(8):584–592. doi:10.1080/23744235.2018.1447682
12. Miller O, Hemphill RR. Urinary tract infection and pyelonephritis. Emerg Med Clin North Am. 2001;19(3):655–674. doi:10.1016/S0733-8627(05)70208-X
13. Perl B, Gottehrer NP, Raveh D, Schlesinger Y, Rudensky B, Yinnon AM. Cost-effectiveness of blood cultures for adult patients with cellulitis. Clin Infect Dis. 1999;29(6):1483–1488. doi:10.1086/313525
14. Stevenson A, Hider P, Than M. The utility of blood cultures in the management of non-facial cellulitis appears to be low. N Z Med J. 2005;118(1211):U1351.
15. Tsutsui A, Yahara K, Shibayama K. Trends and patterns of national antimicrobial consumption in Japan from 2004 to 2016. J Infect Chemother. 2018;24(6):414–421. doi:10.1016/j.jiac.2018.01.003
16. Komagamine J, Kobayashi M, Mori T. Prevalence of and rationale for antimicrobial prescription during ambulatory care visits in Japan: a prospective, multicentre, cross-sectional study. BMJ Open. 2020;10(8):e039329. doi:10.1136/bmjopen-2020-039329
17. Wilson ML. Outpatient blood cultures: progress and unanswered questions. Eur J Clin Microbiol Infect Dis. 2004;23(12):879–880. doi:10.1007/s10096-004-1234-1
18. Fabre V, Milstone AM, Keller SC, Carroll KC, Cosgrove SE. Prescribers’ knowledge, attitudes and perceptions about blood culturing practices for adult hospitalized patients: a call for action. Infect Control Hosp Epidemiol. 2018;39(11):1394–1396. doi:10.1017/ice.2018.224
19. Zhang Z. Propensity score method: a non-parametric technique to reduce model dependence. Ann Transl Med. 2016;5(1):7. doi:10.21037/atm.2016.08.57
20. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
21. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801. doi:10.1001/jama.2016.0287
22. Wayne P. Performance Standards for Antimicrobial Susceptibility Testing CLSI Supplement M100S.
23. Shapiro NI, Wolfe RE, Wright SB, Moore R, Bates DW. Who needs a blood culture? A prospectively derived and validated prediction rule. J Emerg Med. 2008;35(3):255–264. doi:10.1016/j.jemermed.2008.04.001
24. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
25. Robin X, Turck N, Hainard A, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011;12:77. doi:10.1186/1471-2105-12-77
26. Cheng MP, Stenstrom R, Paquette K, et al; FABLED Investigators. Blood culture results before and after antimicrobial administration in patients with severe manifestations of sepsis: a diagnostic study. Ann Intern Med. 2019;171(8):547–554. doi:10.7326/M19-1696
27. Gilligan PH, York MK. General detection and interpretation. In: Leber AL, editor. Clinical Microbiology Procedures Handbook.
28. Rello J, Lisboa T, Lujan M, et al.; DNA-Neumococo Study Group. Severity of pneumococcal pneumonia associated with genomic bacterial load. Chest. 2009;136(3):832–840. doi:10.1378/chest.09-0258
29. Idelevich EA, Silling G, Niederbracht Y, et al.; Molecular Diagnostics of Sepsis Study Group. Impact of multiplex PCR on antimicrobial treatment in febrile neutropenia: a randomized controlled study. Med Microbiol Immunol. 2015;204(5):585–592. doi:10.1007/s00430-014-0385-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.