Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Effect of Prehabilitation-Based Individualized Dietary Guidance on Nutrition and Short-Term Quality of Life in Locally Advanced Gastric Cancer Patients Undergoing Surgery: A Single-Center Randomized Controlled Trial
Authors Gu QH, Zhou J, He JR, Hou Y
Received 6 December 2025
Accepted for publication 29 March 2026
Published 7 April 2026 Volume 2026:19 587091
DOI https://doi.org/10.2147/JMDH.S587091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Sue Jordan
Qi-Hong Gu, Jin Zhou, Jia-Ru He, Yu Hou
Department of General Surgery, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215000, People’s Republic of China
Correspondence: Yu Hou, Department of General Surgery, the First Affiliated Hospital of Soochow University, No. 899 Pinghai Road, Gusu District, Suzhou, Jiangsu, 215000, People’s Republic of China, Email [email protected]
Objective: To evaluate the effect of individualized dietary guidance based on the prehabilitation concept on nutritional outcomes and quality of life (QoL) in patients with locally advanced gastric cancer (LAGC) undergoing surgery.
Methods: This is a single-center randomized controlled trial (RCT). Patients who underwent radical gastrectomy following neoadjuvant therapy were included at the First Affiliated Hospital of Soochow University between January 2023 and October 2025 and randomly assigned to either the control group or the intervention group. Both groups received standard perioperative care. The control group received nutritional support, while the intervention group received individualized dietary guidance based on the Patient-Generated Subjective Global Assessment (PG-SGA) in combination with the prehabilitation concept. Nutritional parameters [albumin (Alb), prealbumin (PA), and hemoglobin (Hb)] and Prognostic Nutritional Index (PNI) were assessed at preoperative baseline and postoperative day 5– 7 (before discharge). Quality of life (QoL) was evaluated using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) at baseline and 3 months post-intervention. Postoperative safety and short-term outcomes, including length of stay (LOS), complications (classified by Clavien-Dindo grade), mortality, and readmission within 3 months, were also recorded.
Results: A total of 120 patients were eligible for the study between January 2023 and October 2025, of whom 72 were approached and enrolled (response rate: 60%), with 36 in each group. Compared with the control group, the intervention group showed significantly better nutritional indices after the intervention. In contrast, the control group showed significant decreases in PNI (52.64± 4.98 vs 43.28± 4.73), Alb (42.87± 4.73 vs 36.67± 6.28 g/L), PA (229.12± 39.43 vs 179.32± 32.72 mg/L), and Hb (134.92± 21.63 vs 113.54± 18.21 g/L), whereas no significant within-group changes were observed in the intervention group. EORTC QLQ-C30 scores for all functional domains (except cognitive functioning and financial difficulties) significantly increased, while scores for all symptom domains and single items (except financial difficulties) significantly decreased in both groups. Following the intervention, the intervention group demonstrated significantly higher PNI (51.21± 5.27 vs 43.28± 4.73, P< 0.001) and peripheral blood levels of Alb (40.78± 6.91 vs 36.67± 6.28 g/L, P=0.01), PA (223.83± 37.32 vs 179.32± 32.72 mg/L, P< 0.001), and Hb (129.93± 20.74 vs 113.54± 18.21 g/L, P=0.001) compared with the control group. Additionally, the intervention group had significantly higher scores in four of the five functional domains (physical function: 56.84± 4.37 vs 51.73± 4.02, P< 0.001; emotional function: 57.63± 4.82 vs 53.82± 4.77, P=0.001; role function: 64.93± 3.76 vs 59.86± 4.39, P< 0.001; social function: 63.91± 4.63 vs 59.64± 5.21, P< 0.001) and significantly lower scores in all symptom domains and in five of the six single items (fatigue: 26.12± 3.65 vs 30.49± 3.87, P< 0.001; appetite loss: 14.28± 3.02 vs 18.02± 3.29, P< 0.001) than the control group. Regarding postoperative safety, no severe complications (Clavien-Dindo grade ≥III) or deaths occurred in either group during hospitalization or the 3-month follow-up. The incidence of minor complications (Clavien-Dindo grade I–II) was similar between groups (3 vs 2). The intervention group had a numerically shorter postoperative LOS (7.6± 1.8 vs 8.2± 2.1 days), but the difference was not statistically significant. No readmissions within 3 months were recorded in either group.
Conclusion: Prehabilitation-based individualized dietary guidance effectively improves short-term nutritional outcomes and enhances QoL in patients with LAGC undergoing surgery following neoadjuvant therapy. The intervention demonstrated a favorable safety profile, with no increase in complications, mortality, or readmissions. This single-center study provides preliminary evidence, and long-term outcomes (e.g. survival, readmission) were not evaluated.
Keywords: locally advanced gastric cancer, dietary guidance, prehabilitation, quality of life, nutrition, neoadjuvant therapy, postoperative complications
Introduction
Gastric cancer is one of the most common malignant tumors of the digestive system.1 In China, the incidence (113.4 per 100,000 population) and mortality (79.2 per 100,000 population) rank third among all malignant tumors, respectively.2,3 The proportion of early-stage gastric cancer diagnoses in China remains relatively low, with the majority of patients diagnosed at the stage of locally advanced gastric cancer (LAGC).4–7 For both early-stage and LAGC cases, surgery remains the primary treatment, offering curative potential, prolonged survival, and improved quality of life (QoL) through complete tumor resection.2,8 In LAGC, neoadjuvant therapy reduces tumor burden, thereby facilitating standard radical gastrectomy and enabling higher R0 resection and pathological response rates without increasing postoperative complications.6,9 As a result, neoadjuvant therapy followed by radical gastrectomy has gradually become the standard treatment strategy for LAGC.6,9
Both short-term surgical outcomes and long-term survival in patients with gastric cancer are influenced not only by tumor stage, lymph node metastasis, depth of invasion, and overall physical condition, but also by perioperative nutritional status.10–12 Gastric cancer frequently leads to malnutrition, which is further exacerbated by postoperative reductions in nutrient intake and absorption, gastrointestinal adverse effects such as nausea and vomiting, and myelosuppression induced by neoadjuvant and adjuvant chemoradiotherapy.10,13,14 Several studies have demonstrated that individualized prehabilitation can enhance patients’ physiological reserve, thereby reducing the incidence of malnutrition, promoting postoperative recovery, and improving overall prognosis.15,16
Prehabilitation comprises a series of targeted interventions—including nutritional optimization, physical exercise, and psychological preparation—designed to improve physiological reserves and psychological resilience, enabling patients to better tolerate surgical stress and achieve faster postoperative recovery.17–19 Patients with gastric cancer are predominantly middle-aged or elderly and often present with comorbidities such as hypertension, diabetes, hyperlipidemia, and coronary heart disease.
These conditions are associated with reduced compensatory capacity and diminished functional reserves across multiple organ systems, thereby increasing the risk of perioperative complications.20,21 Consequently, comprehensive preoperative assessment using validated tools is essential. A multidisciplinary team should evaluate key parameters, including medical history, functional and nutritional status, exercise capacity, and psychological well-being, to develop a dynamically adjustable, individualized prehabilitation plan. Within this comprehensive assessment, nutritional screening is critical for identifying and grading malnutrition.19,22 The Patient-Generated Subjective Global Assessment (PG-SGA) is the most widely used nutritional screening tool for cancer patients, recognized for its high sensitivity, specificity, and efficiency.22,23 Notably, surgical stress and inflammation can transiently alter biochemical nutritional markers (eg., albumin), which may confound the interpretation of nutritional intervention effects in the early postoperative period.21,24
Although the concept of prehabilitation is gaining increased attention in the perioperative management of gastric cancer, most existing studies focus on single interventions or short-term outcomes. High-quality evidence regarding the long-term effects of PG-SGA-guided nutritional interventions on nutritional status and QoL in patients with LAGC remains limited. Furthermore, comprehensive data on its impact on postoperative safety outcomes, including complication rates and length of hospital stay, are needed. Therefore, this study aims to investigate the impact of an individualized dietary guidance program—based on PG-SGA scores and the prehabilitation framework—on nutritional outcomes and QoL as well as short-term safety in LAGC patients undergoing surgery.
Material and Methods
Study Design and Patients
This single-center randomized controlled trial (RCT) was conducted involving patients with LAGC who received neoadjuvant chemotherapy followed by radical gastrectomy at the Department of General Surgery, First Affiliated Hospital of Soochow University, between January 2023 and January 2025. Eligible participants were randomly assigned to either the control group or the intervention group using a random number table generated by SPSS 25.0 software. The randomization sequence was concealed in sequentially numbered, opaque envelopes, which were opened by an independent researcher who was not involved in patient recruitment or outcome assessment. The study was reviewed and approved by the Hospital Medical Ethics Committee (Approval No. 2022681, Approval Date: September 28, 2022) and adhered to the principles outlined in the Declaration of Helsinki. All study participants provided written informed consent. This randomized controlled trial was reported in accordance with the CONSORT 2010 guidelines.
Inclusion criteria were as follows: (1) histopathologically confirmed diagnosis of gastric cancer; (2) completion of both neoadjuvant chemotherapy and surgical treatment; (3) postoperative hospital stay of ≥3 days; (4) normal mental and cognitive function (defined as a Mini-Mental State Examination (MMSE) score ≥24), (5) provision of informed consent and voluntary participation in the study.
Exclusion criteria included: (1) presence of severe postoperative complications; (2) severe organic diseases involving vital organs; (3) concurrent metabolic disorders; (4) conditions such as intestinal obstruction or short bowel syndrome that preclude enteral nutritional support; (5) history of alcohol abuse or drug addiction; and (6) emergency operations due to gastric cancer-related complications (eg., perforation, obstruction).
Patients were recruited by clinical physicians; questionnaires (EORTC QLQ-C30) were administered by trained research nurses; and the intervention was delivered by registered dietitians in collaboration with the prehabilitation management team.
Intervention Procedure
Patients in the control group received routine care, including health education, pharmacological treatment, and management of chemotherapy-related adverse effects. Nutritional intervention followed the conventional five-step protocol.25 Specifically, if a patient’s dietary intake was deemed adequate to meet energy requirements, a regular diet and nutritional education were provided. If intake was insufficient, oral nutritional supplements (ONS) were administered. When ONS failed to meet energy needs, enteral nutrition support was initiated. Parenteral nutrition was considered only when enteral support remained inadequate. Among the control group, the distribution of nutritional support modes in the control group is detailed in Table 1.
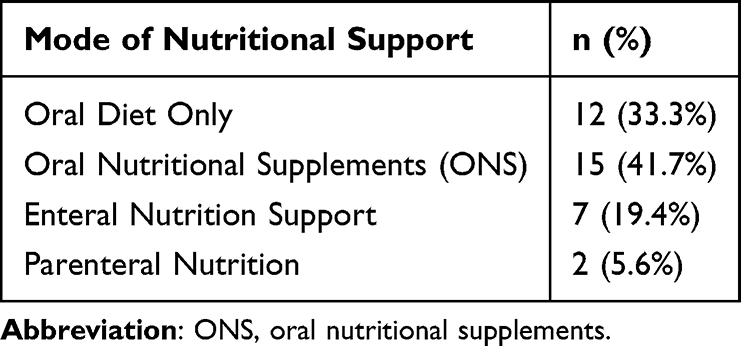 |
Table 1 Nutritional Support Modes in the Control Group (n=36) |
Patients in the intervention group received personalized dietary guidance in addition to the standard care provided to the control group. The intervention consisted of the following components:
- Establishment of a prehabilitation management team: A multidisciplinary team was formed, including charge nurses, the head nurse, clinical physicians, and dietitians.
- Nutritional status assessment: the nutritional status of patients was assessed 2–4 weeks preoperatively using the PG-SGA tool. The PG-SGA comprises two components: the first section records patient-reported data on weight changes, dietary intake, symptoms, and functional capacity; the second section is completed by healthcare professionals and scores factors such as age, metabolic stress, and findings from physical examination. The scores from both sections are summed to yield a total PG-SGA score, with higher scores indicating more severe malnutrition. Based on the total score, patients were categorized as follows: a score of ≤1 (Grade A) indicated a well-nourished status; 2–8 (Grade B) indicated suspected or moderate malnutrition (specifically, scores of 2–3 suggested possible malnutrition, and 4–8 indicated moderate malnutrition); and ≥9 (Grade C) indicated severe malnutrition.
- Individualized dietary intervention plan: A tailored nutritional intervention plan was developed based on the patient’s PG-SGA grade. Patients classified as Grade A did not receive active nutritional intervention but underwent weekly PG-SGA re-evaluation.
Patients in Grade B received nutritional intervention concurrent with their antitumor and surgical treatments, according to the five-step nutritional protocol. Patients in Grade C underwent 2–4 weeks of intensive nutritional support prior to the initiation of antitumor therapy and surgery. Furthermore, dietitians provided personalized dietary counseling once a week (30–45 minutes per session) from preoperative 2–4 weeks until discharge. Adherence was monitored via weekly dietary diaries and monthly follow-up calls, with an overall adherence rate of 89.2% (33 of 36 patients completed ≥80% of the sessions). Additionally, dietitians provided personalized dietary counseling tailored to each patient’s preferences, body weight, economic status, and level of physical activity. This guidance encompassed recommendations on food selection, cooking methods, meal timing, and physical activity.
The recommended diet was high in protein, fiber, and calories, with steaming, boiling, and stewing suggested as the preferred cooking methods. For patients with postoperative symptoms such as vomiting and belching, a dietary approach involving frequent small meals and light and easily digestible food was advised. For patients with poor appetite or indigestion, dishes such as diced hawthorn meat (pork stir-fried with hawthorn fruit, a traditional Chinese dish used to stimulate appetite and aid digestion) and Huangqin yam porridge were recommended to help stimulate appetite. A flowchart of this intervention process is presented in Figure 1.
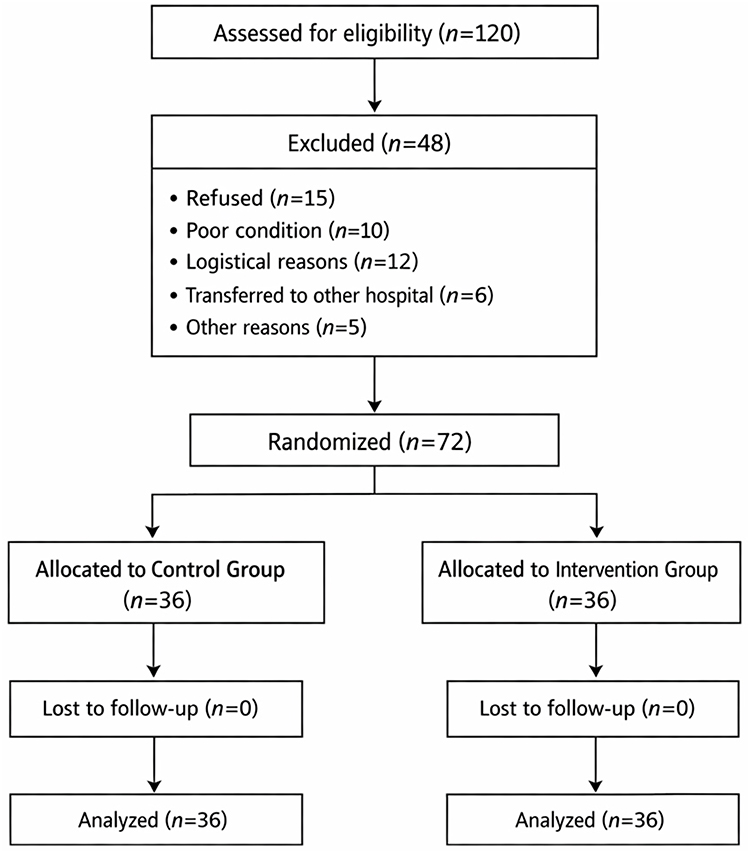 |
Figure 1 CONSORT flow diagram of participant recruitment, randomization, follow-up, and analysis. |
Outcome Measures
Peripheral venous blood samples were collected from all patients after an overnight fast at two time points: during the initial preoperative assessment and postoperative day 5–7 (before discharge) following the individualized dietary intervention (timing standardized across all patients). Nutritional indicators, including serum levels of albumin (Alb, g/L), prealbumin (PA, mg/L), and hemoglobin (Hb, g/L), were measured using a VITROS 5600 Integrated System automated biochemical analyzer (CE certificate number: 0124). Peripheral lymphocyte count (Lym, ×109/L) was measured using a Mindray BC-7500 automatic blood cell analyzer (CE certificate number: 0123). The Prognostic Nutritional Index (PNI) was calculated using the following formula: PNI = [5 × Lym (×109/L)] + Alb (g/L).23
Postoperative safety and short-term outcomes were assessed as follows: Postoperative length of stay (LOS) was recorded in days for each patient. Postoperative complications occurring during hospitalization were documented, categorized by type (eg., none, surgical site infection, pneumonia, anastomotic leak) and severity according to the Clavien-Dindo classification system.26 Mortality, defined as death during hospitalization or within 3 months postoperatively, was recorded. Readmissions to any hospital within 3 months of discharge due to surgery or nutrition-related issues were tracked through medical record review and telephone follow-up.
The patients’ QoL was assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30).27 The assessments were conducted at two time points: during the initial preoperative investigation and three months post-intervention. The QLQ-C30 consists of 30 items organized into 15 multi-item and single-item scales: five functional scales, three symptom scales, one global health status/QoL scale, and six single-item measures. All scale scores were linearly transformed to a 0–100 scale according to the EORTC scoring manual. For the functional scales and the global health status/QoL scale, higher scores indicate better functioning or QoL. In contrast, higher scores on the symptom scales and single items reflect greater symptom severity.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 25.0). The distribution of continuous variables was assessed for normality using the Shapiro–Wilk test. All continuous variables were found to be normally distributed and are presented as mean ± standard deviation. Differences between the two groups were analyzed using independent samples t-tests, while within-group changes before and after the intervention were assessed using paired samples t-tests. Categorical and ordinal data are presented as numbers (percentages). Inter-group comparisons of categorical and ordinal variables were conducted using Chi-square tests or Mann–Whitney-U tests, respectively. For comparisons involving categorical variables with expected cell counts <5 (eg., complication rates), Fisher’s exact test was employed. A P-value <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 120 patients were eligible for the study between January 2023 and October 2025, of whom 72 were approached and enrolled. Among the 120 eligible patients, 72 were approached and enrolled, while 48 were not approached for participation. Of the 120 eligible patients, 48 were not approached for participation for the following reasons: refusal to participate (n=15), inability to complete questionnaires due to poor physical condition (n=10), logistical limitations during the recruitment period (n=12), transfer to other hospitals (n=6), and other administrative reasons (n=5).The detailed reasons are presented in the CONSORT flow diagram (Figure 1). A total of 72 patients with LAGC were enrolled, with 36 patients in each group. As shown in Table 2, all baseline characteristics, including gender, age, tumor location, TNM stage, surgical procedure, PG-SGA grade, and comorbidities, showed no significant differences between the two groups (P>0.05 for all comparisons).
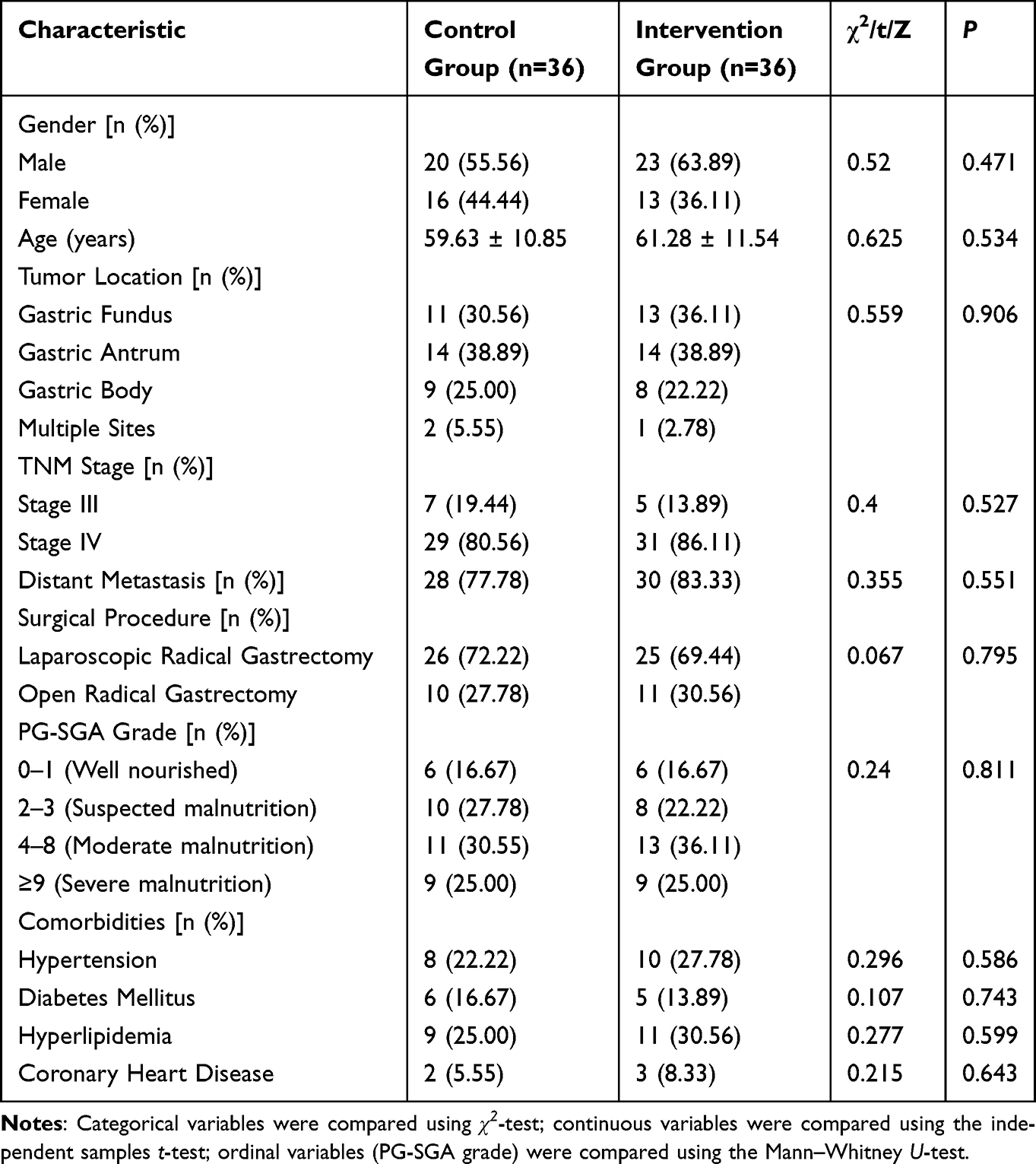 |
Table 2 Comparison of Baseline Characteristics Between the Two Groups |
Prognostic Nutritional Index
No significant difference in PNI was observed between the two groups during the preoperative assessment. Following the intervention, the control group showed a statistically significant decrease in PNI, whereas the intervention group showed no significant change. Consequently, the post-intervention PNI in the intervention group was significantly higher compared with the control group (Table 3).
 |
Table 3 Comparison of Prognostic Nutritional Index (PNI) Between the Two Groups at Preoperative Assessment and Post-Intervention (Postoperative Day 5–7) |
Nutritional Indicators
As shown in Table 4, no significant differences were found in the preoperative serum levels of Alb, PA, and Hb between the two groups. In the control group, post-intervention levels of Alb, PA, and Hb were significantly lower compared with preoperative levels. In contrast, no significant changes in these indicators were observed in the intervention group between the preoperative and post-intervention time points. Moreover, the post-intervention levels of Alb, PA, and Hb in the intervention group were significantly higher than those in the control group.
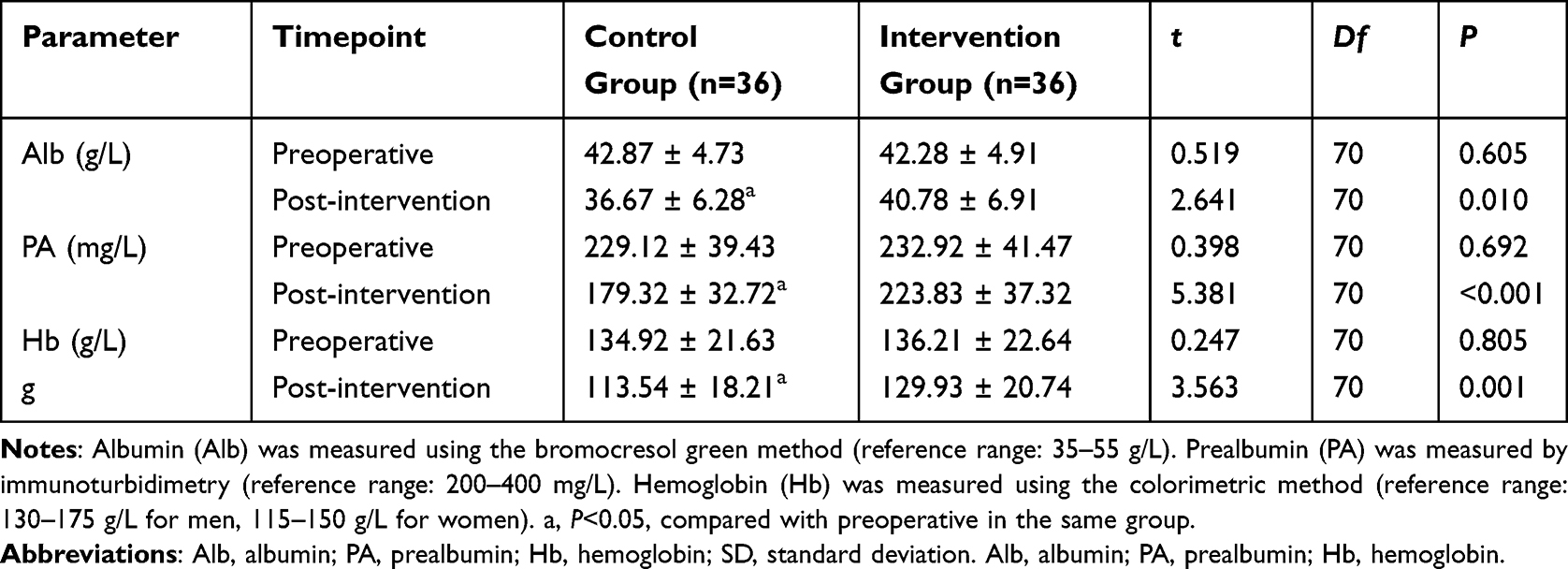 |
Table 4 Comparison of Nutritional Indicators Between the Two Groups of Patients |
EORTC QLQ-C30 Scores
The analysis of EORTC QLQ-C30 outcomes revealed significant improvements in health-related QoL following the nutritional intervention. The intervention group exhibited superior outcomes compared to the control group across multiple domains.
As shown in Table 5, both groups demonstrated significant within-group improvements in most functional scales at the 3-month follow-up. However, the intervention group achieved significantly higher scores than the control group in physical functioning (56.84 vs. 51.73, P<0.001), emotional functioning (57.63 vs. 53.82, P=0.001), role functioning (64.93 vs. 59.86, P<0.001), and social functioning (63.91 vs. 59.64, P<0.001). No significant between-group differences were observed in cognitive functioning.
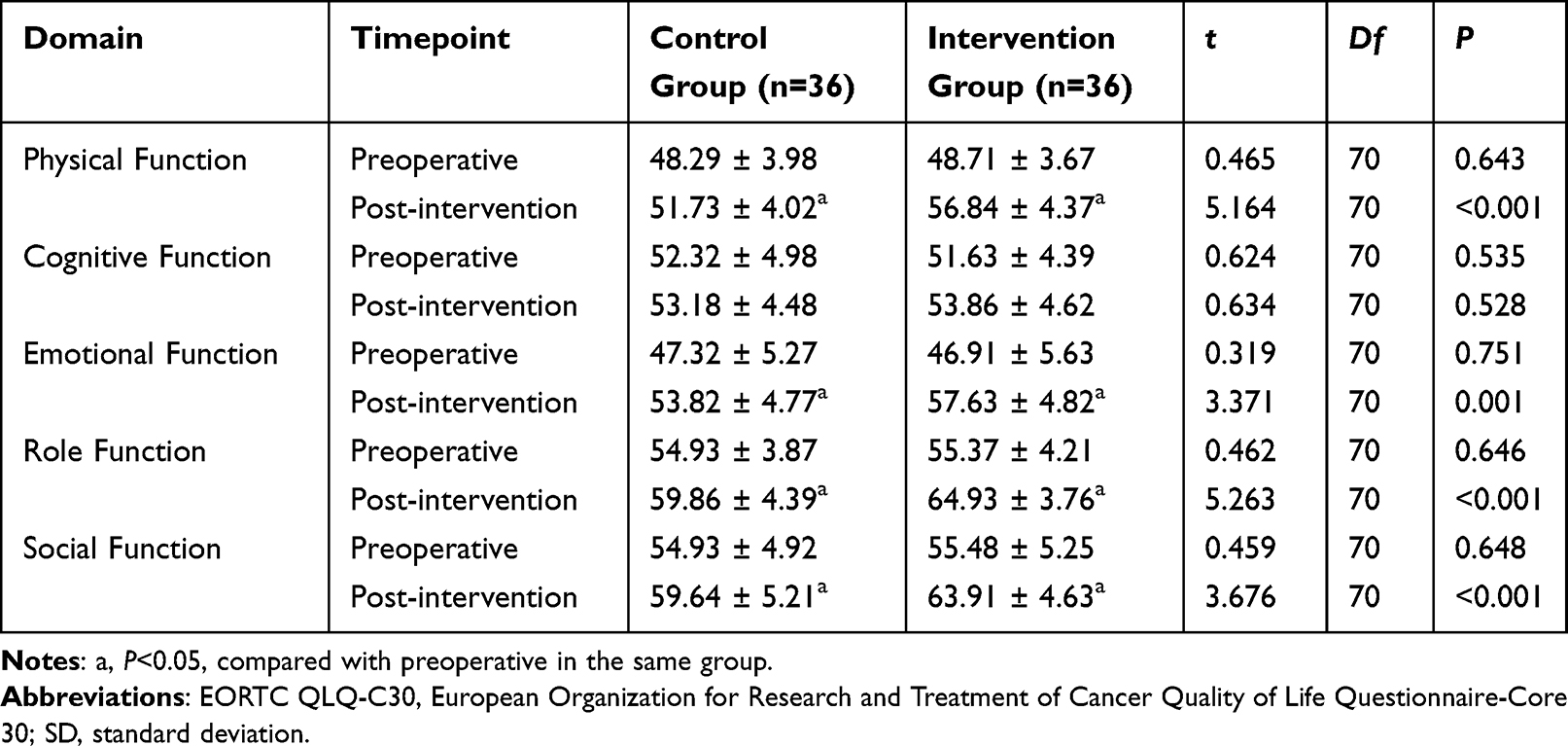 |
Table 5 Comparison of EORTC QLQ-C30 Functional Scale Scores Between the Two Groups |
Regarding symptom scales (Table 6), both groups experienced significant reductions in fatigue and pain post-intervention. However, the intervention group showed significantly greater improvements in fatigue (26.12 vs. 30.49, P<0.001), pain (14.89 vs. 17.21, P=0.014), and nausea/vomiting (11.81 vs. 13.81, P=0.038) compared to the control group.
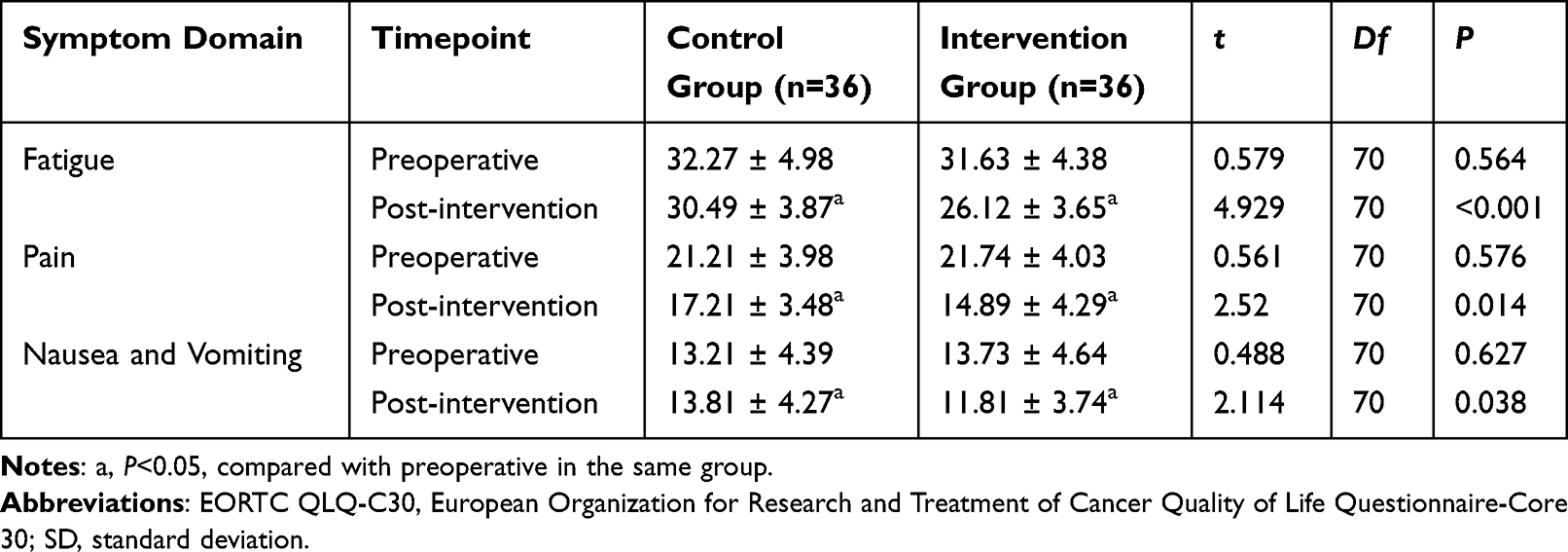 |
Table 6 Comparison of EORTC QLQ-C30 Symptom Scale Scores Between the Two Groups |
For single-item symptoms (Table 7), the intervention group demonstrated significantly greater improvements in dysphagia (16.74 vs. 18.19, P=0.033), appetite loss (14.28 vs. 18.02, P<0.001), insomnia (20.12 vs. 22.87, P=0.020), constipation (15.10 vs. 17.29, P=0.011), and diarrhea (10.19 vs. 12.18, P=0.002) compared to the control group. No significant between-group difference was observed in financial difficulties.
 |
Table 7 Comparison of EORTC QLQ-C30 Single-Item Scale Scores Between the Two Groups |
Overall, these findings consistently demonstrate that the integrated prehabilitation program with individualized nutritional intervention provided broad benefits across multiple QoL domains, particularly in physical functioning and symptom control, compared to standard care alone. The novelty of the findings lies in the application of PG-SGA-guided individualized dietary guidance in LAGC patients undergoing neoadjuvant therapy followed by surgery, which addresses the unmet need for personalized nutritional support in this specific population.
Postoperative Safety and Short-Term Outcomes
Postoperative safety and short-term outcomes are summarized in Table 8. No severe complications (Clavien-Dindo grade III or above, such as anastomotic leak or reoperation) occurred in either group. Minor complications (Clavien–Dindo grade I–II) were reported in 3 patients in the control group and 2 patients in the intervention group. (1 diarrhea, 1 surgical site erythema treated with topical antibiotics).
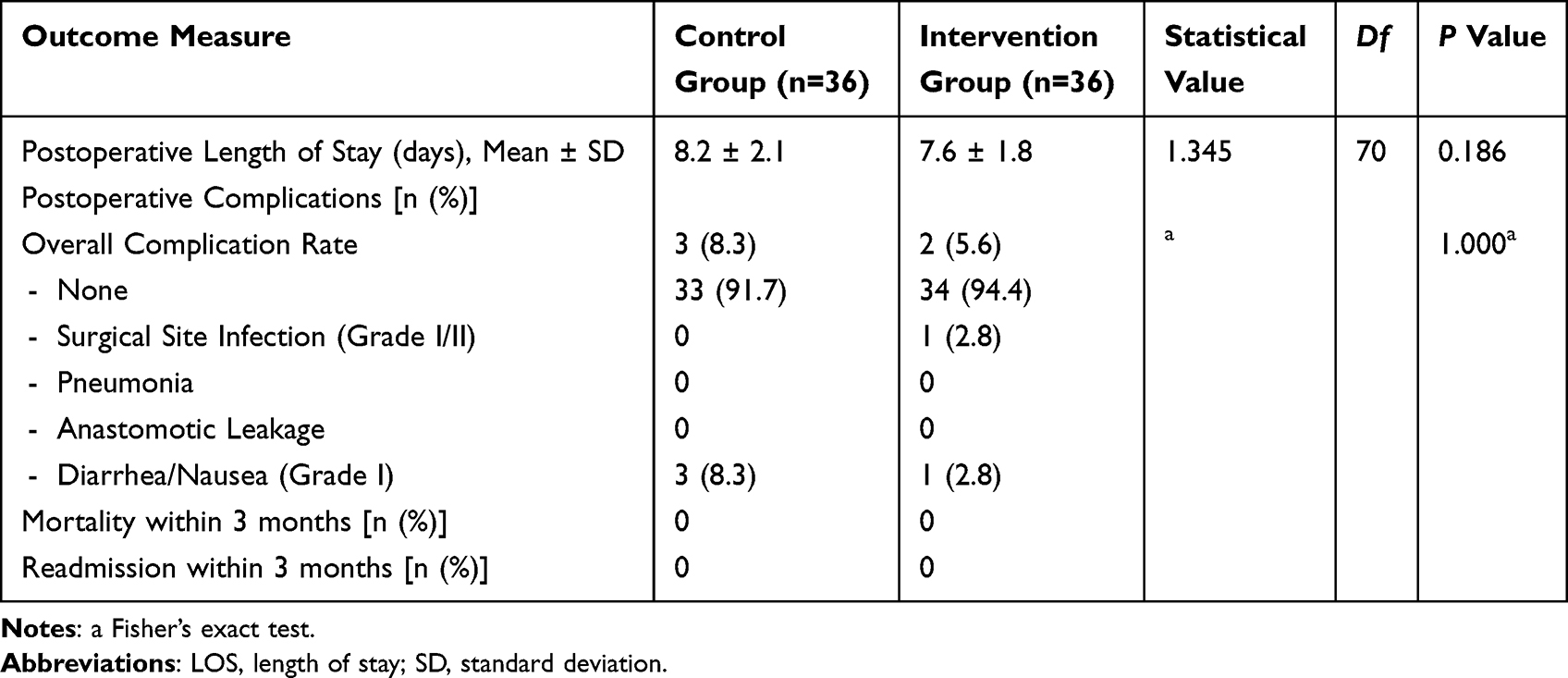 |
Table 8 Comparison of Postoperative Safety and Short-Term Outcomes Between the Two Groups |
The difference in overall complication rate was not statistically significant. The mean postoperative LOS was 8.2 ± 2.1 days in the control group and 7.6 ± 1.8 days in the intervention group. Although the intervention group had a shorter mean LOS, the difference did not reach statistical significance (t=1.345, P=0.186). No deaths occurred during hospitalization or within the 3-month follow-up in either group, and no patient required readmission within 3 months due to surgery- or nutrition-related issues.
Discussion
Nutritional Outcomes: Role of PG-SGA-Guided Prehabilitation
Guided by the prehabilitation concept, this study implemented individualized dietary guidance based on the PG-SGA assessment for gastric cancer patients undergoing surgery. The intervention group demonstrated significant advantages in preserving nutritional and immune status, with key parameters (including PNI, Alb, PA, Hb) remaining stable during the perioperative period, in contrast to the significant declines observed in the control group. Quality of life, assessed using the EORTC QLQ-C30, showed superior outcomes in the intervention group across multiple functional and symptom domains. The integrated prehabilitation program, which combined nutritional, physical, and psychological interventions, effectively enhanced patients’ physiological reserve and psychological resilience. Targeted guidance on food selection, eating strategies, and exercise training alleviated eating-related discomfort and improved physical function. These findings support the role of preoperative prehabilitation in helping patients better tolerate surgical stress, maintain nutritional status, and ultimately improve quality of life, supporting its value as a component of standard perioperative care for gastric cancer patients.
Patients with LAGC frequently experience inadequate nutrient intake and malnutrition due to tumor-related metabolic demands, impaired digestion and absorption, and the adverse effects of anticancer treatments.28 Poor preoperative nutritional status is associated with reduced immune function, muscle wasting, and diminished QoL, which collectively compromise surgical tolerance, increase the risk of postoperative complications, and worsen prognosis.29 Nutritional status is thus a critical component of preoperative assessment for patients with gastric cancer. One study reported that few gastric cancer patients were well-nourished, with the prevalence of moderate to severe malnutrition reaching as high as 75%.30 Consequently, preoperative nutritional support aimed at correcting malnutrition is essential to improve surgical outcomes, expedite postoperative recovery, and enhance prognosis. The initial step in providing nutritional support is screening, which serves to identify patients at risk of malnutrition or already malnourished, assesses the severity of their condition, and develops appropriate nutritional intervention strategies.31 The PG-SGA is a validated nutrition screening tool specifically designed for cancer patients, integrating patient self-assessment with professional evaluation by healthcare providers.32 Compared with the Nutritional Risk Screening 2002 (NRS2002), the PG-SGA demonstrates a higher positive screening rate for identifying LAGC patients undergoing surgery who require nutritional support.33,34 In this study, personalized dietary guidance was provided to LAGC patients undergoing neoadjuvant chemotherapy followed by surgery, based on PG-SGA screening results and guided by the prehabilitation concept. The intervention group exhibited better nutritional status compared to the observation group, supporting the sensitivity and specificity of the PG-SGA as a nutritional screening tool for cancer patients.
Prognostic Value of PNI and Nutritional Markers
The PNI, calculated from Lym and serum Alb level, is a key indicator for assessing perioperative nutritional and immune status, as well as surgical risk. It serves as a reliable predictor of postoperative complications and survival outcomes in gastric cancer patients, with higher PNI values indicating better immune function and nutritional status.35 Studies have shown that a low PNI correlates with poorer survival outcomes and shorter overall survival in cancer patients.36,37 In a study by Du et al35–38 involving 79 patients with esophagogastric junction adenocarcinoma who received neoadjuvant chemoradiotherapy. The results showed that inflammatory-nutritional indicators, such as the neutrophil-to-lymphocyte ratio (NLR) and PNI—as well as postoperative pathological stage, were identified as significant predictors of 5-year overall survival and progression-free survival. Good nutritional status and muscle mass are also recognized as important predictors of postoperative complications and recovery speed.
In the present study, guided by the prehabilitation concept and informed by PG-SGA assessment, the intervention group received routine care supplemented with individualized dietary guidance. Compared with the control group, the intervention group maintained more stable levels of PNI, Alb, PA, and Hb, indicating improved nutritional status and immune function, which may contribute to a better prognosis. These findings are consistent with previous studies that emphasize the prognostic value of PNI and other nutritional markers, and they provide interventional evidence supporting the benefits of nutritional support in gastric cancer patients undergoing surgery.39,40
Quality of Life Improvements and EORTC QLQ-C30 Utility
The EORTC QLQ-C30 is a widely used cancer-specific instrument for assessing health-related QoL. A multicenter cohort study reported significantly reduced QoL in gastric cancer patients with cachexia, with specific scales of the EORTC QLQ-C30—particularly appetite loss, social functioning, and survival outcomes—showing strong associations with cachexia.41 A qualitative interview study by Cocks et al further demonstrated the tool’s utility in capturing patient experiences with cancer and its treatment, as well as its value in guiding clinical practice.42 In the present study, most patients with locally advanced gastric cancer were malnourished or cachectic in the preoperative period, exhibiting low social functioning and high symptom burden (eg., appetite loss, dysphagia, diarrhea), indicative of impaired QoL. The prehabilitation-guided individualized dietary intervention significantly improved functional and symptom scores, reflecting enhanced nutritional status, physical function, and patient confidence. By addressing nutritional, physical, and psychological needs, this approach aligns with prehabilitation principles, strengthening physiological reserves and resilience, reducing symptom burden, and supporting perioperative recovery. These results provide interventional evidence for the relationship between nutritional support and improved QoL in patients with gastric cancer.
Postoperative Safety and Short-Term Recovery
Beyond improvements in nutritional and QoL benefits, the safety profile of the intervention is crucial for clinical adoption. Our results indicate that prehabilitation-based dietary guidance did not increase the risk of postoperative complications. The incidence of minor complications was low and comparable between groups, and no severe complications (Clavien-Dindo ≥III) occurred. These findings are reassuring and support the principle that optimizing preoperative nutritional status can enhance, rather than compromise, surgical safety. Although the intervention group had a numerically shorter postoperative LOS (7.6 vs. 8.2 days), the difference was not statistically significant in this modest sample, suggesting a potential trend towards enhanced recovery. The absence of mortality and readmissions within 3 months in both groups reflects the overall standard of care and the selection of patients without severe baseline organ dysfunction. These preliminary safety outcomes support the feasibility of integrating such nutritional prehabilitation into perioperative pathways without adding risk.
Influence of Surgical Stress and Confounding Factors
It is important to acknowledge that the observed changes in nutritional biomarkers (eg., Alb, PA) may partially reflect acute surgical stress and inflammatory responses, rather than solely the effect of dietary guidance.17 This limitation is common in early postoperative nutritional assessments, as surgical trauma transiently alters hepatic protein synthesis.17 Failure to consider this biological phenomenon may lead to overestimation of the intervention’s direct impact on nutritional status.
Additionally, postoperative complications and prolonged hospital stay can impair nutritional intake and absorption, which may influence postoperative recovery and nutritional outcomes.16 In this study, no severe complications were observed in either group, and the difference in hospital stay was small (control group: 8.2±2.1 days; intervention group: 7.6±1.8 days), which may minimize this confounding effect.16 These factors are critical to consider when interpreting the findings, as they underscore the complexity of attributing biochemical changes solely to nutritional intervention.
Comparison with Existing Literature
The findings of this study are consistent with existing literature on nutritional prehabilitation, while providing targeted evidence for LAGC patients undergoing neoadjuvant therapy.43
Limitations and Future Directions
This study has several limitations. First, a sample size calculation was not performed prior to the study, which may limit the statistical power for secondary outcomes. Meanwhile, as a single-center study with a relatively small sample size, the generalizability of the findings may be limited due to potential selection bias. Second, the assessments of nutritional status, exercise tolerance, and psychological condition were assessed using standardized self-reported questionnaires, which may be influenced by cultural background, education level, and individual psychological factors, thereby introducing a degree of subjectivity. Third, data analysts were not blinded to the intervention group assignment, which may introduce detection bias.14 Additionally, the risk of the Rosenthal effect (observer bias) cannot be excluded for non-laboratory outcomes (eg., QoL scores). Fourth, all operations were performed by the same team of 3 senior surgeons to ensure consistency, which may limit generalizability to other surgical teams. Fifth, long-term data on mortality and readmission were not available, as follow-up was limited to 3 months. Finally, surgical stress and inflammation may have confounded the interpretation of early postoperative nutritional biomarkers. Additionally, the absence of long-term follow-up limits the ability to evaluate the sustained effects of individualized prehabilitation on survival and QoL. Future research should prioritize large-scale, multicenter randomized controlled trials to investigate the impact of multidimensional prehabilitation—encompassing nutritional, physical, comorbidity-related, and psychological interventions—on long-term postoperative outcomes in patients with gastric cancer. Such evidence is critical to support the standardized implementation of prehabilitation in clinical practice.
Conclusion
In conclusion, prehabilitation-based individualized dietary guidance, guided by PG-SGA, effectively improves short-term nutritional status (maintaining PNI, albumin, prealbumin, and hemoglobin levels) and enhances quality of life (improving physical, emotional, role, and social function, while reducing symptom burden) in patients with LAGC undergoing surgery following neoadjuvant therapy. This single-center study provides preliminary evidence for the feasibility and efficacy of personalized nutritional prehabilitation. However, claims regarding reductions in postoperative complications, shorter hospital stays, and enhanced recovery are not substantiated by the current data, and long-term outcomes (eg., survival, readmission) were not evaluated. Integrating standardized prehabilitation assessments and interventions into a multidisciplinary, team-based care model may be a promising strategy to optimize perioperative management in patients with LAGC. Future large-scale, multicenter RCTs with extended follow-up are warranted to validate these findings.
Abbreviations
LAGC, Locally Advanced Gastric Cancer; QoL, Quality of Life; PG-SGA, Patient-Generated Subjective Global Assessment; PNI, Prognostic Nutritional Index; Alb, Albumin; PA, Prealbumin; Hb, Hemoglobin; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; Lym, Peripheral Lymphocyte Count; ONS, Oral Nutritional Supplements; NLR, Neutrophil-to-Lymphocyte Ratio; NRS2002, Nutritional Risk Screening 2002; TNM, Tumor-Node-Metastasis; CSCO, Chinese Society of Clinical Oncology; NCCN, National Comprehensive Cancer Network.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was reviewed and approved by the Hospital Medical Ethics Committee (Approval No. 2022681, Approval Date: September 28, 2022) and adhered to the principles outlined in the Declaration of Helsinki. All study participants provided written informed consent.
Acknowledgments
We thank Medjaden Inc. for scientific editing of this manuscript. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors made substantial contributions to the conception and design of the study, data acquisition, analysis, and interpretation; participated in drafting, revising, or critically reviewing the manuscript; provided final approval of the version to be published; agreed on the journal to which the article has been submitted; and accepted responsibility for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82372887), which is a General Program titled “Mechanism of Exosomal circGOSR1-mediated Cytoplasmic Translocation of PTBP1 Regulating Alternative Splicing of REG4 to Promote Peritoneal Metastasis of Gastric Cancer”. (Direct Cost: 490,000 RMB; Execution Period: 2024.01-2027.12; Principal Investigator: Jin Zhou; Affiliated Institution: Soochow University).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhang YX, Qin JJ, Guan XQ. Pharmacological Insights into Scleromitrion diffusum (Willd.) Against Gastric Cancer: active Components and Mechanistic Pathways. Oncol Adv. 2025;3:87–14.
2. Li P, Li Z, Linghu E, Ji J. Chinese national clinical practice guidelines on the prevention, diagnosis, and treatment of early gastric cancer. Chin Med J. 2024;137(8):887–908. doi:10.1097/CM9.0000000000003101
3. Zhu J, Wei R, Hu G, et al. Development of Injectable Thermosensitive Nanocomposite Hydrogel for Ratiometric Drug Delivery to Treat Drug Resistant Chondrosarcoma In Vivo. Small. 2024;20(31):e2310340. doi:10.1002/smll.202310340
4. Li XY, Wang SL, Chen DH, et al. Construction and Validation of a m7G-Related Gene-Based Prognostic Model for Gastric Cancer. Front Oncol. 2022;12:861412. doi:10.3389/fonc.2022.861412
5. Shen YQ, Wei QW, Tian YR, Ling YZ, Zhang M. Coagulation indices and fibrinogen degradation products as predictive biomarkers for tumor-node-metastasis staging and metastasis in gastric cancer. World J Gastrointest Oncol. 2025;17(1):98725. doi:10.4251/wjgo.v17.i1.98725
6. Wang FH, Zhang XT, Tang L, et al. The Chinese Society of Clinical Oncology (CSCO): clinical guidelines for the diagnosis and treatment of gastric cancer, 2023. Cancer Commun. 2024;44(1):127–172. doi:10.1002/cac2.12516
7. Smith J, Guapo F, Strasser L, et al. Development of a Rapid Adeno-Associated Virus (AAV) Identity Testing Platform through Comprehensive Intact Mass Analysis of Full-Length AAV Capsid Proteins. J Proteome Res. 2023;23(1):161–174. doi:10.1021/acs.jproteome.3c00513
8. Li GZ, Doherty GM, Wang J. Surgical Management of Gastric Cancer: a Review. JAMA Surg. 2022;157(5):446–454. doi:10.1001/jamasurg.2022.0182
9. Ajani JA, D’Amico TA, Bentrem DJ, et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20:167–192.
10. Triantafillidis JK, Papakontantinou J, Antonakis P, Konstadoulakis MM, Papalois AE. Enteral Nutrition in Operated-On Gastric Cancer Patients: an Update. Nutrients. 2024;16:1639.
11. Sun X, Huang X, Lu X, et al. The expression and clinical significance of the tRNA aspartic acid methyltransferase 1 protein in gastric cancer. Int J Clin Oncol. 2021;26:2229–2236. doi:10.1007/s10147-021-02019-2
12. Ishiguro T, Aoyama T, Ju M, et al. Prognostic Nutritional Index as a Predictor of Prognosis in Postoperative Patients With Gastric Cancer. Vivo. 2023;37(3):1290–1296. doi:10.21873/invivo.13207
13. Lovey J, Molnar A, Banky B. Long-term nutrition in patients candidate to neoadjuvant and adjuvant treatments. Eur J Surg Oncol. 2024;50(5):106850. doi:10.1016/j.ejso.2023.02.007
14. Kang MK, Lee HJ. Impact of malnutrition and nutritional support after gastrectomy in patients with gastric cancer. Ann Gastroenterol Surg. 2024;8(4):534–552. doi:10.1002/ags3.12788
15. Minnella EM, Awasthi R, Loiselle SE, Agnihotram RV, Ferri LE, Carli F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: a Randomized Clinical Trial. JAMA Surg. 2018;153(12):1081–1089. doi:10.1001/jamasurg.2018.1645
16. Molenaar CJL, Minnella EM, Coca-Martinez M, et al. Effect of Multimodal Prehabilitation on Reducing Postoperative Complications and Enhancing Functional Capacity Following Colorectal Cancer Surgery: the PREHAB Randomized Clinical Trial. JAMA Surg. 2023;158(6):572–581. doi:10.1001/jamasurg.2023.0198
17. Gronska D, Wojnarski M, Budzynski A, et al. Effectiveness of dietary prehabilitation in patients with gastric, pancreatic, and colorectal cancers: a systematic review. Pol Arch Intern Med. 2025;135(7–8):17015. doi:10.20452/pamw.17015.
18. Girnyi S, Marano L, Skokowski J, et al. Prehabilitation approaches for gastrointestinal cancer surgery: a narrative review. Rep Pract Oncol Radiother. 2024;29(5):614–626. doi:10.5603/rpor.103136
19. Cho AR, Vongchaiudomchoke W, Balde D, Kim DJ, Carli F. Enhancing postoperative recovery with multimodal prehabilitation: the journey begins before surgery. Korean J Anesthesiol. 2025;78(5):401–417. doi:10.4097/kja.25320
20. Kamiya H, Komatsu S, Ohashi T, et al. Postoperative complications and open gastrectomy affect non-cancer-related death and shorten life expectancy in elderly patients with gastric cancer. Am J Cancer Res. 2021;11(10):5038–5044.
21. Takemoto Y, Tanabe K, Chikuie E, et al. Preoperative High C-Reactive Protein to Albumin Ratio Predicts Short- and Long-Term Postoperative Outcomes in Elderly Gastric Cancer Patients. Cancers. 2024;16(3):616. doi:10.3390/cancers16030616
22. Zhang L, Ding Z, Zhao Y, Cheng Z, Hu J, Huo L. Advances and challenges in nutritional screening and assessment for cancer patients: a comprehensive systematic review and future directions. Front Nutr. 2025;12:1688344. doi:10.3389/fnut.2025.1688344
23. Han Y, Wu J, Ji R, et al. Preoperative sarcopenia combined with prognostic nutritional index predicts long-term prognosis of radical gastrectomy with advanced gastric cancer: a comprehensive analysis of two-center study. BMC Cancer. 2023;23(1):751. doi:10.1186/s12885-023-11251-0
24. Vu H, Giorgi S, Clifton JDW, Balasubramanian N, Schwartz HA. Modeling Latent Dimensions of Human Beliefs. Proc Int AAAI Conf Weblogs Soc Media. 2022;16:1064–1074. doi:10.1609/icwsm.v16i1.19358
25. Chen L, Zhao M, Tan L, Zhang Y. Effects of Five-Step Nutritional Interventions Conducted by a Multidisciplinary Care Team on Gastroenteric Cancer Patients Undergoing Chemotherapy: a Randomized Clinical Trial. Nutr Cancer. 2023;75(1):197–206. doi:10.1080/01635581.2022.2104329
26. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
27. Fayers P, Bottomley A. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. EurJ Cancer. 2002;38(4):S125–133. doi:10.1016/S0959-8049(01)00448-8
28. Williams GR, Dunne RF, Giri S, Shachar SS, Caan BJ. Sarcopenia in the Older Adult With Cancer. J Clin Oncol. 2021;39(19):2068–2078. doi:10.1200/JCO.21.00102
29. Martínez-Ortega AJ, Piñar-Gutiérrez A, Serrano-Aguayo P, et al. Perioperative Nutritional Support: a Review of Current Literature. Nutrients. 2022;15(1):14. doi:10.3390/nu15010014
30. Bossi P, Delrio P, Mascheroni A, Zanetti M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: a Narrative Review. Nutrients. 2021;13(6):1980. doi:10.3390/nu13061980
31. Cederholm T, Jensen GL, Correia M, et al. GLIM criteria for the diagnosis of malnutrition - A consensus report from the global clinical nutrition community. Clin Nutr. 2019;38(1):1–9. doi:10.1016/j.clnu.2018.08.002
32. Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr. 2002;56(8):779–785. doi:10.1038/sj.ejcn.1601412
33. Yang D, Zheng Z, Zhao Y, Zhang T, Liu Y, Xu X. Patient-generated subjective global assessment versus nutritional risk screening 2002 for gastric cancer in Chinese patients. Future Oncol. 2020;16(3):4475–4483. doi:10.2217/fon-2019-0539
34. Chen X, Liu X, Ji W, et al. The PG-SGA outperforms the NRS 2002 for nutritional risk screening in cancer patients: a retrospective study from China. Front Nutr. 2023;10:1272420. doi:10.3389/fnut.2023.1272420
35. Bullock AF, Greenley SL, McKenzie GAG, Paton LW, Johnson MJ. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: systematic review, narrative synthesis and meta-analysis. Eur J Clin Nutr. 2020;74(11):1519–1535. doi:10.1038/s41430-020-0629-0
36. Ni L, Huang J, Ding J, et al. Prognostic Nutritional Index Predicts Response and Prognosis in Cancer Patients Treated With Immune Checkpoint Inhibitors: a Systematic Review and Meta-Analysis. Front Nutr. 2022;9:823087. doi:10.3389/fnut.2022.823087
37. Zhang L, Ma W, Qiu Z, et al. Prognostic nutritional index as a prognostic biomarker for gastrointestinal cancer patients treated with immune checkpoint inhibitors. Front Immunol. 2023;14:1219929. doi:10.3389/fimmu.2023.1219929
38. Du R, Ming J, Geng J, et al. Establishment of prognostic models for adenocarcinoma of oesophagogastric junction patients with neoadjuvant chemoradiotherapy: a real-world study. Radiat Oncol. 2022;17(1):45. doi:10.1186/s13014-022-02016-3
39. Hong YJ, Han S, Lim JU, et al. Association Between Quality of Life Questionnaire at Diagnosis and Survival in Patients With Lung Cancer. Clin Lung Cancer. 2023;24(5):459–466. doi:10.1016/j.cllc.2023.03.007
40. McKernan M, McMillan DC, Anderson JR, Angerson WJ, Stuart RC. The relationship between quality of life (EORTC QLQ-C30) and survival in patients with gastro-oesophageal cancer. Br J Cancer. 2008;98(5):888–893. doi:10.1038/sj.bjc.6604248
41. Zhang X, Dai XT, Wang C, et al. A Comprehensive Analysis of the Association Between the EORTC QLQ-C30 Questionnaire and Cachexia in Patients With Gastric Cancer. J Cachexia Sarcopenia Muscle. 2025;16(3):e13859. doi:10.1002/jcsm.13859
42. Cocks K, Wells JR, Johnson C, et al. Content validity of the EORTC quality of life questionnaire QLQ-C30 for use in cancer. EurJ Cancer. 2023;178:128–138. doi:10.1016/j.ejca.2022.10.026
43. Gillis C, Carli F. Promoting Perioperative Metabolic and Nutritional Care. Anesthesiology. 2015;123(6):1455–1472. doi:10.1097/ALN.0000000000000795
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.