Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Effect of Personality Traits on Sustained Remission Among Patients with Major Depression: A 12-Month Prospective Study
Authors Nogami W, Nakagawa A ![]() , Katayama N, Kudo Y, Amano M, Ihara S, Kurata C, Kobayashi Y, Sasaki Y, Ishikawa N, Sato Y, Mimura M
, Katayama N, Kudo Y, Amano M, Ihara S, Kurata C, Kobayashi Y, Sasaki Y, Ishikawa N, Sato Y, Mimura M ![]()
Received 9 August 2022
Accepted for publication 9 November 2022
Published 28 November 2022 Volume 2022:18 Pages 2771—2781
DOI https://doi.org/10.2147/NDT.S384705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Waka Nogami,1 Atsuo Nakagawa,1,2 Nariko Katayama,1 Yuka Kudo,1,3,4 Mizuki Amano,1,5 Sakae Ihara,1 Chika Kurata,1 Yuki Kobayashi,1 Yohei Sasaki,1 Natsumi Ishikawa,1,6 Yasunori Sato,7 Masaru Mimura1
1Department of Neuropsychiatry, Keio University School of Medicine, Tokyo, Japan; 2Department of Neuropsychiatry, St. Marianna University School of Medicine, Kanagawa, Japan; 3Department of Psychiatry, Gunma Hospital, Gunma, Japan; 4Department of Clinical, Educational and Health Psychology, University College London, London, UK; 5Department of Psychiatry, Toyosato Hospital, Ibaraki, Japan; 6Department of Child Psychiatry, the University of Tokyo Hospital, Tokyo, Japan; 7Department of Preventive Medicine and Public Health, Keio University School of Medicine, Tokyo, Japan
Correspondence: Atsuo Nakagawa, Department of Neuropsychiatry, Keio University School of Medicine, Shinanomachi 35, Shinjuku-ku, Tokyo, 160-8582, Japan, Tel +81-3-5363-3235, Fax +81-3-5363-3480, Email [email protected]
Purpose: Major depression is a heterogeneous disorder. Therefore, careful evaluation and comprehensive assessment are crucial elements for achieving remission. Personality traits influence prognosis and treatment outcomes, but there is not enough evidence on the association between personality traits and sustained remission (SR). Hence, the present study aimed to evaluate the relationship between personality traits and SR among patients with major depression.
Patients and Methods: The 12-month prospective study evaluated 77 patients diagnosed with major depressive disorder. All patients underwent a comprehensive assessment, including the Temperament and Personality Questionnaire (T&P) at baseline, and depression severity was measured at baseline as well as six and 12 months. SR was defined as remission (the GRID-Hamilton Depression Rating Scale [GRID-HAMD17] score ≦ 7) at both the 6- and 12-month follow-up. We compared eight T&P construct scores at baseline between the SR and non-SR groups. Multivariable logistic regression analyses were performed to determine the T&P personality traits related to SR.
Results: Patients who achieved SR had a lower T&P personal reserve and lower T&P rejection sensitivity. Further, lower scores on the T&P personal reserve trait were independently associated with higher rates of SR among patients with major depression. Patients who achieved SR had a shorter duration of the current depressive episode and milder severity of depression at baseline.
Conclusion: A lower level of personal reserve predicted a higher probability of SR in the treatment of depression. Extended observations in naturalistic follow-up settings with larger sample sizes are required to better understand the personality traits affecting SR in patients with depression.
Keywords: depression, personality traits, personal reserve, sustained remission, temperament and personality questionnaire
Introduction
Major depression is a highly heterogeneous disorder, and the patients often require several courses of treatment to reach remission.1–3 Remission, defined as the state in which individuals have no more than minimal symptoms,4 is one of the main goals in the acute treatment of major depression. Sustained remission (SR) for as long as four or six months decreases the recurrence rate,5 and social functioning has also been reported to improve with continued remission.6 However, the remission rates of patients with depression who seek medical care are low.7,8 Only one-third of patients have shown a remission with initial antidepressant treatment.9 Various treatment modalities are administered to promote remissions, such as cognitive behavioral therapy (CBT) in combination with medication10–12 and long-term medication.13–15 Further, it remains unclear which patients with major depression are able to achieve SR. Therefore, careful evaluations are needed to develop effective treatment strategies in clinical settings.
The Improving Access to Psychological Therapies16 is a national mental healthcare service in the United Kingdom that provides evidence-based psychological therapies to adults with anxiety disorders and depression. The guidelines of this service state that patient-centered assessment and clinical formulation are crucial elements of a comprehensive assessment. Clinical formulation, a fundamental aspect of personalized care, helps clinicians assess patients for major depression and set the treatment goals by identifying patient values, preferences, and relevant factors in the clinical assessment and shared decision-making process. Clinicians are expected to formulate each individual patient from a multidimensional perspective, including biological, psychological, social, and lifestyle factors of the patient. Moreover, for patients with persistent or treatment-resistant depression, the treatment plan is modified according to the results of assessments including family history, developmental history, exposures to childhood environments, personality traits, cognitive schemas, history of psychiatric diagnoses, and social functioning.1,17,18
Personality traits influence the prognosis and treatment outcomes of patients with depression.19–21 Many studies have reported that higher scores on neuroticism and lower scores on extraversion predict poorer outcomes and more chronic course, although the results of studies for extraversion are slightly less consistent than neuroticism.19,21–25 Similarly, a high score on harm avoidance and a low score on self-directedness also predict poor outcomes.26–28 A higher score on neuroticism also influences the response to depression treatment such as antidepressant medication25,29 and CBT.30 Parker et al31 assessed the temperament and personality of patients with depression to develop a model for conceptualizing non-melancholic disorder. Ultimately, they developed the Temperament and Personality Questionnaire (T&P), consisting of eight lower-order constructs. T&P was aimed to provide a basis for determining appropriate treatment for depression,32 and studies have shown that it can be used to predict treatment outcomes.33–35 However, to our knowledge, no study has examined the association between T&P personality traits and SR.
Therefore, the aim of the current study was to determine whether personality traits influence SR among patients with major depression. Towards this goal, we assessed the personality traits of patients with depression who had achieved SR, using the T&P, in a 12-month prospective study.
Materials and Methods
Study Design and Patients
This prospective study recruited patients diagnosed with major depressive disorder between April 2014 and December 2020. The inclusion criteria were as follows: 20–75 years old, outpatients diagnosed with major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV) criteria.36 The exclusion criterion was the presence of remarkable psychotic symptoms and psychomotor disturbances, a core symptom of melancholic depression,37 clinically assessed by the psychiatrists involved in the study at the initial interview. The study was conducted at three hospitals: a clinic at a university hospital and two psychiatric hospitals in the Greater Tokyo Area. The patients received usual care for depression including clinical consultation and medication management by their treating psychiatrists. This study was approved by the Research Ethics Committee of Keio University School of Medicine, Gunma Hospital, and Toyosato Hospital, and was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from each patient prior to enrolment in the study.
Assessment
At baseline, all patients underwent a comprehensive evaluation consisting of a semi-structured interview conducted by the psychiatrists and psychologists involved in the study and an assessment battery that included the T&P and the Dysfunctional Attitudes Scale (DAS-24)38–40 for assessing personality traits and the degree of dysfunctional schemas, respectively. A Structured Clinical Interview for DSM-IV-TR Axis I Disorders-Patient Edition41 was administered to confirm the depression diagnosis, and the GRID-Hamilton Depression Rating Scale (GRID-HAMD17)42,43 and the Beck Depression Inventory-Second Edition (BDI-II)44 were used to determine the depression severity. The following sociodemographic and clinical data were collected: age, sex, marital status, habitation setting, educational attainment, occupational history, history of physical condition, family history of psychiatric disorders, alcohol and tobacco use, total number of depressive episodes, lifetime duration of clinically diagnosed depression, and duration of the current depressive episode.
We conducted follow-up interviews at 6 and 12 months from baseline. The interview comprised a depression severity rating at the time of assessment and longitudinal information including the Clinical Global Impressions scale (CGI-S).45 Procedures for using the Longitudinal Interval Follow-up Evaluation (LIFE) were used to conduct the interview and make CGI ratings.46 In brief, the interview was conducted to help the patients recall their state at that time point and to obtain an overview of what happened to them over the past six months. Depression severity was measured at the 6- and 12-month follow-up assessments using the same measurement scales as at baseline (ie, GRID-HAMD17 and BDI-II). SR was defined as a GRID-HAMD17 score ≤ 7 at both the 6- and 12-month follow-up.
Measures
GRID-HAMD17
The GRID-HAMD17 was an observer-rated scale to assess the severity of depressive symptoms, which was developed to establish criteria for scoring and administering the original HAMD.43 It is used to evaluate the intensity and frequency of symptoms in the past seven days, with high scores indicating increased severity (range, 0–52 points). The validity and reliability of the Japanese version of the GRID-HAMD17 have been reported elsewhere.42
BDI-II
The BDI-II is a 21-item self-report scale used for rating the severity of depressive symptoms in adults and adolescents.44 High scores represent increased depression severity (range, 0–63 points). The Japanese version of BDI-II has been found to be valid and reliable.47
CGI-S
The CGI-S is an observer-rated scale for the overall impression of depression severity.45 It is rated from 1 to 7, and higher scores show a more severe depression state. LIFE is a longitudinal procedure for assessing mental disorders,46 and the CGI-S was assessed retrospectively over time using LIFE.
T&P
The T&P is a 109-item self-report questionnaire that dimensionally assesses eight personality traits related to non-melancholic depression.31 Each item is scored on a 4-point Likert scale, with high scores indicating an increased tendency toward that personality trait. The eight-trait constructs of the T&P are as follows: (1) anxious worrying (easily stressed, worried, and anxious), (2) self-criticism (very hard on oneself), (3) rejection sensitivity (worried about rejection or abandonment), (4) irritability (hot-tempered, losing control when stressed, and being irritated by little things), (5) self-focused (prioritizing own needs over others), (6) perfectionism (very responsible, high standards for oneself, and being fully committed to things), (7) personal reserve (keeping one’s inner feelings to oneself), and (8) social avoidance (being introverted and reserved in social situations).48,49 The eight constructs of the T&P are consistent with those of the five-factor model, one of the widely used models of personality traits. The Japanese version of the T&P has also been found to be valid and reliable.50
DAS-24
The DAS-24 is a 24-item instrument that measures the intensity of dysfunctional schemas,38 and each item is scored on a 7-point scale ranging from totally agree to totally disagree. It includes three subscales: achievement, self-control, and dependency. The validity and reliability of the Japanese version of DAS-24 (DAS-24J) have been proven previously.39
Statistical Analysis
The patients’ characteristics were compared between the groups, namely patients who did (SR group) and did not achieve SR (non-SR group), using a chi-square test or Fisher’s exact test for categorical variables and t-test or Mann–Whitney U-test for continuous variables, as appropriate. We performed the paired t-test to assess the mean GRID-HAMD17 score changes from baseline to 6 months and from 6 to 12 months in each group. Also, we compared the treatment modality between the groups using a chi-square test.
T&P construct scores at baseline were compared between the SR and non-SR group using the t-test. We then performed multivariable logistic regression analyses to assess the association between SR/non-SR and the T&P personality constructs. SR/non-SR was entered as the dependent variable. Independent variables were each T&P construct and baseline clinical characteristics showing significant differences (p < 0.05) in the univariate analyses in order to control for the effect of potential confounders between T&P construct and baseline characteristics. Next, we assessed correlations between depression severity at baseline, 6- and 12- month follow-up, and the significant T&P constructs in the univariate analyses by using Pearson’s correlation coeffeicient. All statistical analyses were performed using JMP Version 16.0.0 (SAS Institute, NC). A two-tailed p-value of 0.05 was considered statistically significant.
Results
We initially examined 98 patients; 85 met the inclusion criteria and participated in the study. Of the 85 patients, three were not contactable at the 6-month follow-up, and five were not contactable at the 12-month follow-up. Seventy-seven patients completed the 12-month follow-up; their baseline sociodemographic and clinical features and the differences between the SR and non-SR groups are shown in Table 1. Most of the patients (72 patients [93.5%]) were prescribed antidepressants. Selective serotonin reuptake inhibitors (SSRIs) were the most used antidepressant medication at baseline (40 patients [51.9%]; Supplementary Table 1). In total, 40.3% (n=31) of the patients achieved SR. The depression severity of the SR group was significantly lower than that of the non-SR group (GRID-HAMD17: p = 0.012; BDI-II: p = 0.001), and the median duration of the current depressive episode of the SR group was significantly shorter than that of the non-SR group (p=0.029). There were no significant differences with regard to the other characteristics.
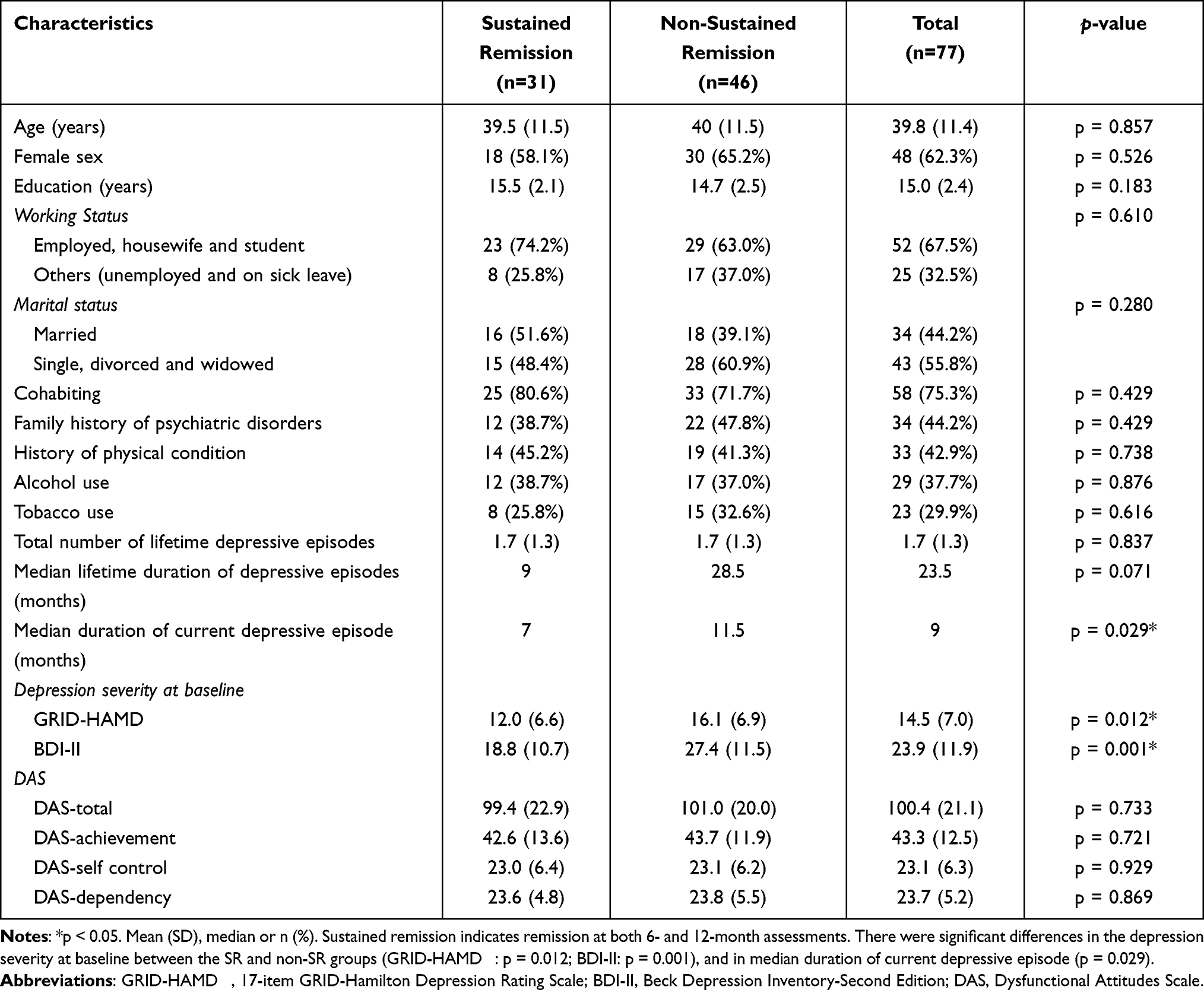 |
Table 1 Characteristics of the Overall Population, Stratified by Group (n=77) |
The treatment received for over 12 months stratified by groups and the changes in antidepressant medication between baseline and 6 months, and between 6 and 12 months, are shown in Table 2. Within the 12-month follow-up, 50 patients (64.9%) received medication treatment only, and 27 (35.1%) received a combination of medication treatment and CBT. There was no significant difference in those who received combination treatment between the SR/non-SR groups (SR vs non-SR: n=13 [41.9%] vs n=14 [30.4%]; χ2 =1.07, p=0.301).
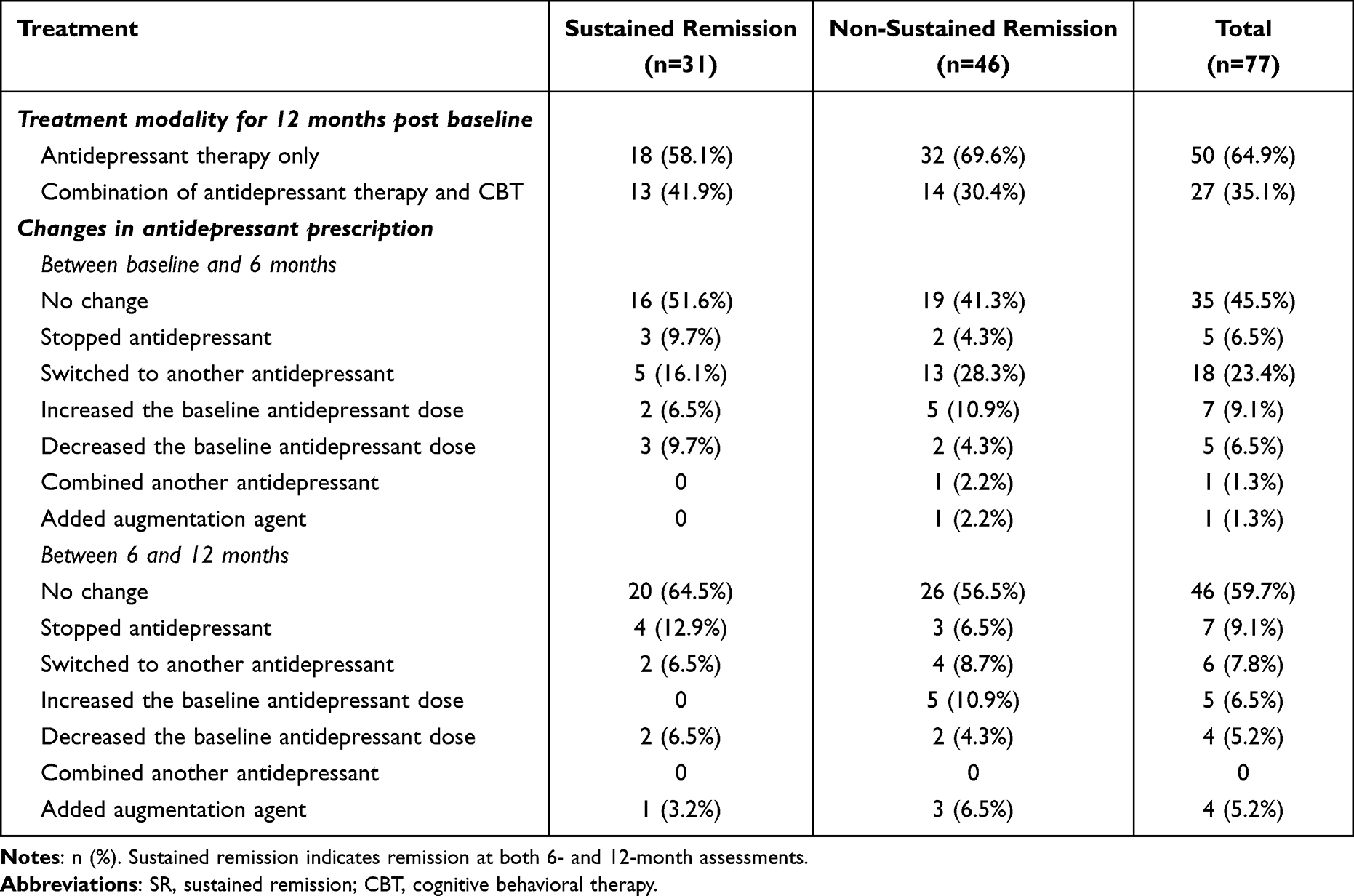 |
Table 2 Engaged Depression Treatment for 12 Months by SR/Non-SR Group (n=77) |
The mean changes in depression severity over time between the SR and non-SR groups are shown in Figure 1. The mean changes in total GRID-HAMD17 scores showed that the improvement in depression severity between baseline and 6 months was significantly greater than that between 6 and 12 months in both groups, especially in the SR group. The depression severity at 6 and 12 months in terms of GRID-HAMD17 and BDI-II scores are shown in Supplementary Table 2. Further, the 12-month CGI-S obtained in the longitudinal interview is shown in Supplementary Figure 1; there were no serious CGI-S fluctuations between 6 and 12 months in the SR group.
 |
Figure 1 Changes in depressive symptoms based on the mean GRID-HAMD17 scores. Abbreviation: GRID-HAMD17, 17-item GRID-Hamilton Depression Rating Scale. Notes: *p < 0.05. Sustained remission indicates remission at both 6- and 12-month assessments. The mean changes in depression severity between baseline and 6 months was significantly greater than those between 6 and 12 months in both groups. Error bars indicate 95% CIs. |
Independent Influencing Personality Factors of SR/Non-SR
The comparison of the T&P construct scores between the SR and non-SR groups at baseline is shown in Table 3. Of the eight T&P construct scores, T&P rejection sensitivity and T&P personal reserve of the SR group were significantly lower than those of the non-SR group (T&P rejection sensitivity: p = 0.007; T&P personal reserve: p = 0.013). Table 4 showed multivariable logistic regression with SR/non-SR as the dependent variable, and T&P personal reserve construct score, duration of the current depressive episode, as well as GRID-HAMD17 scores at baseline, which were significantly different in the univariate analyses, as the independent variables. The T&P personal reserve construct score and baseline GRID-HAMD17 score were independently associated with SR/non-SR (T&P personal reserve: p = 0.043; GRID-HAMD17: p = 0.016). We then put the T&P rejection sensitivity score into the same model instead of the T&P personal reserve score; however, there were no significant factors found in this model.
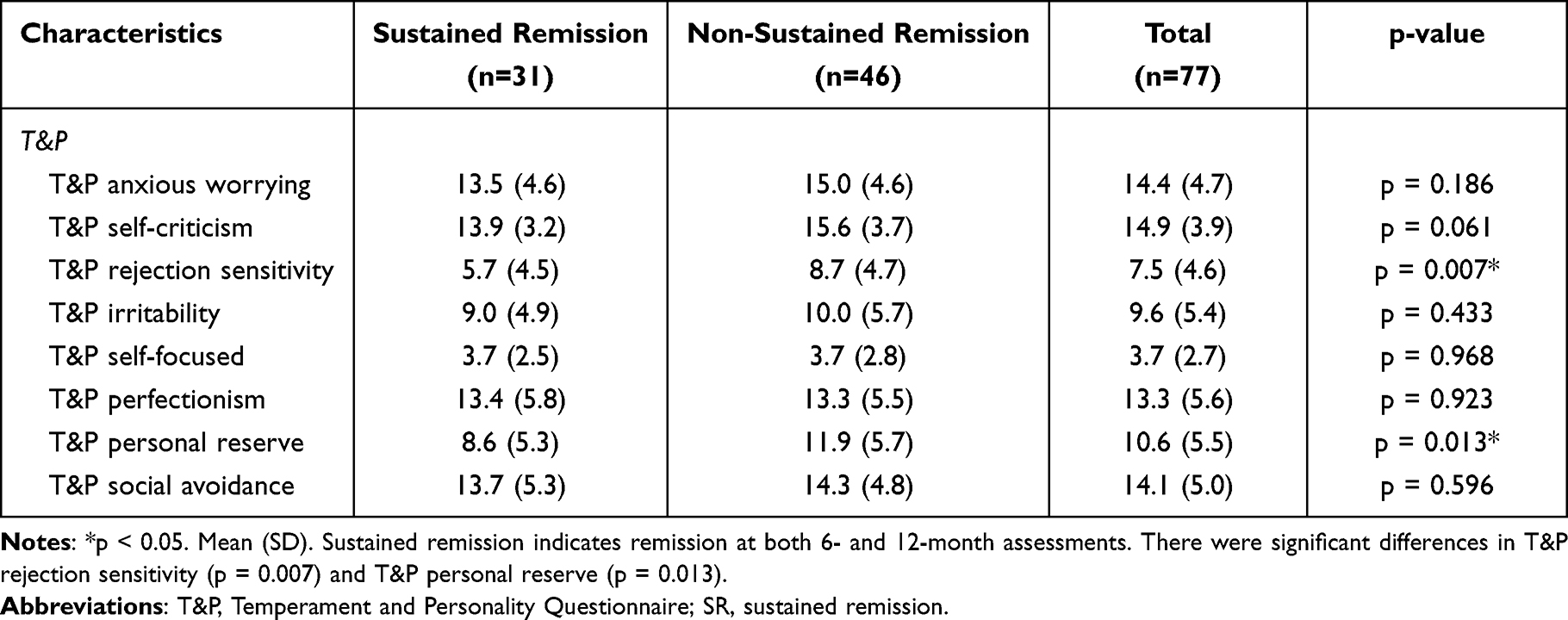 |
Table 3 Comparisons of T&P Constructs at Baseline by SR/Non-SR Group |
 |
Table 4 Multivariable Logistic Regression Analyses of SR and Non-SR for Major Depression (n=77) |
Next, we examined the association between GRID-HAMD17 over time and the two T&P personality constructs, which showed a significant association with SR in the univariate analyses (Supplementary Table 3). We found weak-to-moderate correlations between T&P rejection sensitivity and GRID-HAMD17 scores at each time point. In contrast, T&P personal reserve correlated with GRID-HAMD17 at 6 and 12 months, however, this correlation was not found at baseline.
Discussion
In this study, we investigated whether T&P personality traits influence SR among patients with major depression. In our study, approximately 40% of patients with depression achieved SR, and those who achieved SR had a shorter duration of the current depressive episode and milder severity of depression at baseline. We also found that those who achieved SR were associated with lower levels of T&P rejection sensitivity and T&P personal reserve. Furthermore, after we controlled for duration of the current depressive episode and baseline depression severity, T&P personal reserve trait showed association with SR in major depression.
Our results showed that those who achieved SR had a shorter duration of the current depressive episode and milder severity of depression at baseline. These findings are consistent with those of previous studies reporting on the recurrence or relapse as outcome of depression.28,51–53 Further, Furukawa et al indicated that baseline characteristics such as the severity of depression, age, education, and length of the current episode predicted remission in the acute phase of antidepressant treatment and even at six months.54 Depressive patients with more severe symptoms are more heterogenous and their courses may quite vary in a naturalistic study.55
Among eight constructs of T&P personality traits, T&P rejection sensitivity and T&P personal reserve were associated with SR in the univariate analyses, although T&P rejection sensitivity was not after control for the duration of the current depressive episode and severity of depression. T&P rejection sensitivity matches neuroticism in the five-factor model. Previous studies showed that higher neuroticism was associated with poorer prognosis for depression,19,21,22,25 which was similar with our findings. Our results on correlation analyses showed that T&P rejection sensitivity was associated with depression severity over time, while T&P personal reserve did not correlate with baseline depression severity. Perhaps, this may indicate that T&P rejection sensitivity was more reflective of depression severity. Additionally, this finding is consistent with previous reports showing that neuroticism is associated with depression severity.56
The T&P personal reserve trait was the only construct that was independently associated with SR, after duration of the current depressive episode and severity of depression were excluded in the adjusted multivariable analysis. T&P personal reserve matches introversion, which is on the opposite end of extraversion in the five-factor model.31 Our findings are in line with those of prior studies that reported an association of a lower level of extroversion with poorer treatment outcomes23 and chronic depression.24,57 One study showed that social inhibition, including the trait of personal reserve, is associated with treatment-resistant depression.58 Mulder et al reported that personality pathology is the robust clinical predictor of poor outcomes for patients with depression based on the five-year naturalistic study.28 Thus, the personal reserve trait should be included in the comprehensive assessment to plan a more suitable treatment strategy for each patient in clinical settings. T&P personal reserve trait indicates features such as reluctance to let people get too close at an emotional level, willingness to keep feelings to oneself, or avoidance of seeking advice from others.48 An approach that provides psychoeducation to help patients reflect on personal reserve trait and encourages them to disclose and discuss their problems related to their depressive symptoms may be helpful in treating depression, which ultimately may lead to SR.
Some limitations of this study are to be mentioned. First, it was conducted at only three tertiary medical institutions; as such, the characteristics of patients may have limited generalizability. Second, the number of patients was relatively small, which limits the statistical power of the results. Third, treatment outcomes were followed up only for 12 months. Fourth, personality traits were assessed using a self-reported questionnaire only, hence the risk of bias cannot be discarded. Finally, we cannot control the treatment due to the nature of a naturalistic study, although the difference in treatment modality did not show an association with SR in our sample.
Conclusion
Lower scores of T&P personal reserve predicted higher rates of SR in patients with major depression. This finding suggests that when developing a clinical formulation for each patient in clinical settings, the personal reserve trait should be included in the comprehensive assessment, which may lead to desirable maintenance treatment. Consequently, future extended observations in naturalistic treatment settings, including larger sample sizes and a broader range of demographic characteristics, are needed to cultivate our understanding of the effect of personality traits on the treatment of depression.
Abbreviations
aOR, Adjusted Odds Ratio; BDI-II, Beck Depression Inventory-Second Edition; CBT, cognitive behavioral therapy; DAS-24, Dysfunctional Attitudes Scale; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders-IV; GRID-HAMD17, GRID-Hamilton Depression Rating Scale; SR, sustained remission; T&P, Temperament and Personality Questionnaire.
Ethics Approval and Informed Consent
This study was approved by the Research Ethics Committee of Keio University School of Medicine, Gunma Hospital and Toyosato Hospital, and was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from each patient prior to enrolment in the study.
Acknowledgments
We would like to thank Dr. Dai Mitsuda, Mses. Sayaka Odagiri, Mire Ozawa, Erika Hyo and Yoshie Taguchi, and Mr. Shunsuke Kido for assistance with the study management. We also would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Japan Agency for Medical Research and Development (AMED grant No. JP21dk0307084) and in part by the MGH-SAFER grant. The funders had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, preparation, review, or approval of the manuscript, and decision to submit the manuscript for publication.
Disclosure
Prof. Dr. Masaru Mimura reports personal fees from Biogen Japan, personal fees from Byer Pharmaceutical, grants, personal fees from Daiichi Sankyo, personal fees from Dainippon-Sumitomo Pharma, personal fees from Demant Japan, grants, personal fees from Eisai, personal fees from Eli Lilly, personal fees from Fuji Film RI Pharma, personal fees from Hisamitsu Pharmaceutical, personal fees from H.U. Frontier, personal fees from Janssen Pharmaceutical, personal fees from Mochida Pharmaceutical, personal fees from MSD, personal fees from Mylan EPD, personal fees from Nippon Chemipher, personal fees from Novartis Pharma, personal fees from Ono Yakuhin, personal fees from Otsuka Pharmaceutical, personal fees from Pfizer, grants from Shionogi, grants from Takeda Yakuhin, personal fees from Teijin Pharma, personal fees from Viatris, personal fees from Fronteo, grants from Tanabe Mitsubishi, grants from Tsumura, outside the submitted work. All authors declare that they have no conflicts of interest regarding this study.
References
1. Herrman H, Patel V, Kieling C., et al. Time for united action on depression: a Lancet–World Psychiatric Association Commission. Lancet. 2022;399:957–1022. doi:10.1016/S0140-6736(21)00897-7
2. Kraus C, Kadriu B, Lanzenberger R, Zarate CA, Kasper S. Prognosis and improved outcomes in major depression: a review. Transl Psychiatry. 2019;9(1):127. doi:10.1038/s41398-019-0460-3
3. Malhi GS, Mann JJ. Depression. Lancet. 2018;392:2299–2312. doi:10.1016/S0140-6736(18)31948-2
4. Frank E, Prien RF, Jarrett RB, et al. Conceptualization and rationale for consensus definitions of terms in major depressive disorder. Remission, recovery, relapse, and recurrence. Arch Gen Psychiatry. 1991;48:851–855. doi:10.1001/archpsyc.1991.01810330075011
5. Furukawa TA, Fujita A, Harai H, Yoshimura R, Kitamura T, Takahashi K. Definitions of recovery and outcomes of major depression: results from a 10-year follow-up. Acta Psychiatr Scand. 2008;117:35–40. doi:10.1111/j.1600-0447.2007.01119.x
6. Furukawa TA, Takeuchi H, Hiroe T, et al. Symptomatic recovery and social functioning in major depression. Acta Psychiatr Scand. 2001;103:257–261. doi:10.1034/j.1600-0447.2001.00140.x
7. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163:1905–1917. doi:10.1176/ajp.2006.163.11.1905
8. Souery D, Amsterdam J, de Montigny C, et al. Treatment resistant depression: methodological overview and operational criteria. Eur Neuropsychopharmacol. 1999;9:83–91. doi:10.1016/s0924-977x(98)00004-2
9. Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006;163:28–40. doi:10.1176/appi.ajp.163.1.28
10. Cuijpers P, Berking M, Andersson G, Quigley L, Kleiboer A, Dobson KS. A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can J Psychiatry. 2013;58:376–385. doi:10.1177/070674371305800702
11. Nakagawa A, Mitsuda D, Sado M, et al. Effectiveness of supplementary cognitive-behavioral therapy for pharmacotherapy-resistant depression: a randomized controlled trial. J Clin Psychiatry. 2017;78:1126–1135. doi:10.4088/JCP.15m10511
12. Wiles NJ, Thomas L, Turner N, et al. Long-term effectiveness and cost-effectiveness of cognitive behavioural therapy as an adjunct to pharmacotherapy for treatment-resistant depression in primary care: follow-up of the CoBalT randomised controlled trial. Lancet Psychiatry. 2016;3:137–144. doi:10.1016/S2215-0366(15)00495-2
13. Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet. 2003;361:653–661. doi:10.1016/S0140-6736(03)12599-8
14. Glue P, Donovan MR, Kolluri S, Emir B. Meta-analysis of relapse prevention antidepressant trials in depressive disorders. Aust N Z J Psychiatry. 2010;44:697–705. doi:10.3109/00048671003705441
15. Hirschfeld RM, Schatzberg AF. Long-term management of depression. Am J Med. 1994;97:33S–38S. doi:10.1016/0002-9343(94)90361-1
16. NHS England & NHS Improvement, 2018. The Improving Access to Psychological Therapies (IAPT) pathway for people with long-term physical health conditions and medically unexplained symptoms. Available from: https://www.england.nhs.uk/publication/the-improving-access-to-psychological-therapies-iapt-pathway-for-people-with-long-term-physical-health-conditions-and-medically-unexplained-symptoms/.
17. Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2015;49:1087–1206. doi:10.1177/0004867415617657
18. Wright CD, Tiani AG, Billingsley AL, Steinman SA, Larkin KT, McNeil DW. A framework for understanding the role of psychological processes in disease development, maintenance, and treatment: the 3P-disease model. Front Psychol. 2019;10:2498. doi:10.3389/fpsyg.2019.02498
19. Klein DN, Kotov R, Bufferd SJ. Personality and depression: explanatory models and review of the evidence. Annu Rev Clin Psychol. 2011;7:269–295. doi:10.1146/annurev-clinpsy-032210-104540
20. Morris BH, Bylsma LM, Rottenberg J. Does emotion predict the course of major depressive disorder? A review of prospective studies. Br J Clin Psychol. 2009;48:255–273. doi:10.1348/014466508X396549
21. Mulder RT. Personality pathology and treatment outcome in major depression: a review. Am J Psychiatry. 2002;159:359–371. doi:10.1176/appi.ajp.159.3.359
22. Duggan CF, Lee AS, Murray RM. Does personality predict long-term outcome in depression? Br J Psychiatry. 1990;157:19–24. doi:10.1192/bjp.157.1.19
23. Quilty LC, De Fruyt F, Rolland JP, Kennedy SH, Rouillon PF, Bagby RM. Dimensional personality traits and treatment outcome in patients with major depressive disorder. J Affect Disord. 2008;108:241–250. doi:10.1016/j.jad.2007.10.022
24. Robison EJ, Shankman SA, McFarland BR. Independent associations between personality traits and clinical characteristics of depression. J Nerv Ment Dis. 2009;197:476–483. doi:10.1097/NMD.0b013e3181aad5fc
25. Steffens DC, McQuoid DR, Smoski MJ, Potter GG. Clinical outcomes of older depressed patients with and without comorbid neuroticism. Int Psychogeriatr. 2013;25:1985–1990. doi:10.1017/S1041610213001324
26. Balestri M, Porcelli S, Souery D, et al. Temperament and character influence on depression treatment outcome. J Affect Disord. 2019;252:464–474. doi:10.1016/j.jad.2019.04.031
27. Mulder RT, Frampton CM, Luty SE, Joyce PR. Eighteen months of drug treatment for depression: predicting relapse and recovery. J Affect Disord. 2009;114:263–270. doi:10.1016/j.jad.2008.08.002
28. Mulder RT, Frampton CMA, Jordan J, Luty SE, McIntosh VVW, Carter JD. The five year outcome of major depression: effects of baseline variables and type of treatment. J Psychiatr Res. 2022;145:13–17. doi:10.1016/j.jpsychires.2021.11.039
29. Bock C, Bukh JD, Vinberg M, Gether U, Kessing LV. The influence of comorbid personality disorder and neuroticism on treatment outcome in first episode depression. Psychopathology. 2010;43:197–204. doi:10.1159/000304176
30. Spek V, Nyklícek I, Cuijpers P, Pop V. Predictors of outcome of group and internet-based cognitive behavior therapy. J Affect Disord. 2008;105:137–145. doi:10.1016/j.jad.2007.05.001
31. Parker G, Manicavasagar V, Crawford J, Tully L, Gladstone G. Assessing personality traits associated with depression: the utility of a tiered model. Psychol Med. 2006;36:1131–1139. doi:10.1017/S0033291706007562
32. Parker G, Malhi G, Mitchell P, et al. Progressing a spectrum model for defining non-melancholic depression. Acta Psychiatr Scand. 2005;111:139–143. doi:10.1111/j.1600-0447.2004.00474.x
33. Kudo Y, Nakagawa A, Wake T, et al. Temperament, personality, and treatment outcome in major depression: a 6-month preliminary prospective study. Neuropsychiatr Dis Treat. 2017;13:17–24. doi:10.2147/NDT.S123788
34. Lye MS, Tey YY, Tor YS, et al. Predictors of recurrence of major depressive disorder. PLoS One. 2020;15:e0230363. doi:10.1371/journal.pone.0230363
35. Parker G, Crawford J. Personality and self-reported treatment effectiveness in depression. Aust N Z J Psychiatry. 2009;43:518–525. doi:10.1080/00048670902873730
36. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
37. Parker G. Defining melancholia: the primacy of psychomotor disturbance. Acta Psychiatr Scand Suppl. 2007;433:21–30. doi:10.1111/j.1600-0447.2007.00959.x
38. Power MJ, Katz R, McGuffin P, Duggan CF, Lam D, Beck AT. The Dysfunctional Attitude Scale (DAS). J Res Pers. 1994;28:263–276. doi:10.1006/jrpe.1994.1019
39. Tajima M, Akiyama T, Numa H, et al. Reliability and validity of the Japanese version of the 24-item Dysfunctional Attitude Scale. Acta Neuropsychiatr. 2007;19:362–367. doi:10.1111/j.1601-5215.2007.00203.x
40. Weissman AN. The Dysfunctional Attitude Scale: A Validation Study. University of Pennsylvania; 1979.
41. First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM-IV-TR Axis I Disorders. Patient Ed. New York, NY: Biometrics Research Department, Columbia University; 2005.
42. Tabuse H, Kalali A, Azuma H, et al. The new GRID Hamilton Rating Scale for Depression demonstrates excellent inter-rater reliability for inexperienced and experienced raters before and after training. Psychiatry Res. 2007;153:61–67. doi:10.1016/j.psychres.2006.07.004
43. Williams JB, Kobak KA, Bech P, et al. The GRID-HAMD: standardization of the Hamilton Depression Rating Scale. Int Clin Psychopharmacol. 2008;23:120–129. doi:10.1097/YIC.0b013e3282f948f5
44. Beck AT, Steer RA, Brown GK. Bdi-Ii Manual. Antonio S. TX: The Psychological Corporation; 1996.
45. Guy W. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: US Department of Health, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration. Mental Health Administration; 1976.
46. Keller MB, Lavori PW, Friedman B, et al. The Longitudinal Interval Follow-up Evaluation. A comprehensive method for assessing outcome in prospective longitudinal studies. Arch Gen Psychiatry. 1987;44:540–548. doi:10.1001/archpsyc.1987.01800180050009
47. Kojima M, Furukawa TA, Takahashi H, Kawai M, Nagaya T, Tokudome S. Cross-cultural validation of the Beck Depression Inventory – II in Japan. Psychiatry Res. 2002;110:291–299. doi:10.1016/s0165-1781(02)00106-3
48. Parker G, Manicavasagar V. Modelling and Managing the Depressive Disorders: A Clinical Guide. Cambridge: Cambridge University Press; 2005.
49. The Black Dog Institute, 2013. Temperament and Personality (T&P) Questionnaire. Available from: https://www.blackdoginstitute.org.au/education-services/health-professionals/psychological-toolkit/.
50. Kudo Y, Nakagawa A, Tamura N, et al. The reliability and validity of the Japanese version of the Temperament and Personality Questionnaire for patients with non-melancholic depression. J Affect Disord. 2016;198:237–241. doi:10.1016/j.jad.2016.03.046
51. O’Leary D, Costello F, Gormley N, Webb M. Remission onset and relapse in depression. An 18-month prospective study of course for 100 first admission patients. J Affect Disord. 2000;57:159–171. doi:10.1016/s0165-0327(99)00086-5
52. Kennedy N, Abbott R, Paykel ES. Remission and recurrence of depression in the maintenance era: long-term outcome in a Cambridge cohort. Psychol Med. 2003;33:827–838. doi:10.1017/s003329170300744x
53. Klein NS, Holtman GA, Bockting CLH, Heymans MW, Burger H. Development and validation of a clinical prediction tool to estimate the individual risk of depressive relapse or recurrence in individuals with recurrent depression. J Psychiatr Res. 2018;104:1–7. doi:10.1016/j.jpsychires.2018.06.006
54. Furukawa TA, Kato T, Shinagawa Y, et al. Prediction of remission in pharmacotherapy of untreated major depression: development and validation of multivariable prediction models. Psychol Med. 2019;49:2405–2413. doi:10.1017/S0033291718003331
55. Chin WY, Choi EP, Wan EY. Trajectory pathways for depressive symptoms and their associated factors in a Chinese primary care cohort by growth mixture modelling. PLoS One. 2016;11:e0147775. doi:10.1371/journal.pone.0147775
56. Farmer A, Redman K, Harris T, et al. Neuroticism, extraversion, life events and depression. The Cardiff Depression Study. Br J Psychiatry. 2002;181:118–122. doi:10.1017/s0007125000161823
57. Boschloo L, Schoevers RA, Beekman AT, Smit JH, van Hemert AM, Penninx BW. The four-year course of major depressive disorder: the role of staging and risk factor determination. Psychother Psychosom. 2014;83:279–288. doi:10.1159/000362563
58. Crawford JG, Parker GB, Malhi GS, Mitchell PB, Wilhelm K, Proudfoot J. Social inhibition and treatment‐resistant depression. Pers Ment Health. 2007;1:62–73. doi:10.1002/pmh.5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.