Back to Journals » Patient Preference and Adherence » Volume 17
Effect of Patient-Empowerment Interaction Model on Self-Management Ability of Peritoneal Dialysis Patients: A Randomized Controlled Trial
Authors Cao F, Hong F, Ruan Y, Lin M ![]()
Received 26 December 2022
Accepted for publication 9 March 2023
Published 27 March 2023 Volume 2023:17 Pages 873—881
DOI https://doi.org/10.2147/PPA.S402698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Fang Cao, Fuyuan Hong, Yiping Ruan, Miao Lin
Department of Nephrology, Provincial Clinical College, Fujian Medical University, Fujian Provincial Hospital, Fuzhou, 350001, People’s Republic of China
Correspondence: Fang Cao; Miao Lin, Department of Nephrology, Provincial clinical college, Fujian Medical University, Fujian Provincial Hospital, 134 East Street, Fuzhou, People’s Republic of China, 350001, Tel/Fax +86-591-87557768, Email [email protected]; [email protected]
Objective: Patient empowerment can be achieved through the PBL model. The purpose of the present study was to evaluate the effectiveness and feasibility of patient empowerment through the PBL model in health continuing education of peritoneal dialysis (PD) patients.
Methods: From March 2017 to April 2017, a total of 94 participants were randomly assigned to the PBL group and the traditional group, with 47 patients in each group. Patients of the PBL group were divided into 5 study groups; and six PBL health education activities were held. The basic knowledge, self-management behavior, quality of life, anxiety, and depression were assessed among the traditional group and the PBL group. The average follow-up duration was 10.6± 1.5 months.
Results: Compared with patients in the traditional group, patients in the PBL group had higher scores of basic knowledges for PD (84.33± 3.55 vs 91.19± 3.07; P< 0.001), higher scores of self-management (61.19± 3.71 vs 71.47± 2.89; P< 0.001), better scores of quality of life (85.99± 14.33 vs 102.64± 9.43; P < 0.001), and better scores of satisfaction (90.78± 1.32 vs 98.21± 1.25; P < 0.001). Furthermore, the scores of anxieties (52.39± 4.55 vs 46.46± 4.63; P < 0.001) and the scores of depressions were lower (49.95± 6.76 vs 45.80± 8.77; P =0.01) in patients who participated in the PBL mode of education than in the traditional educational group.
Conclusion: The empowerment model of PBL health education can effectively improve the knowledge, skills and quality of life of PD patients.
Relevance to Clinical Practice: The findings identified in this study will help to improve the quality of nursing care and health education for PD patients.
Patient or Public Contribution: The study design involved patients on PD training. The knowledge and skills of PD and quality of life will improve after they participate the PBL health education activities.
Keywords: patient empowerment, PBL, peritoneal dialysis, patient education, quality of life, chronic kidney disease
Introduction
Continuous ambulatory peritoneal dialysis (CAPD) began to be used in clinical practice in China since the 1970s.1 Approximately 11% of people with kidney failure are treated with peritoneal dialysis (PD) globally.2 It is estimated that more than 272,000 patients receive PD treatment.3 PD is a home-based therapy which requires self-management. A comprehensive safety and training program for patient could be important for patients who initiate PD therapy.4 Patients’ knowledge and psychosocial factors will affect quality life and survival. Therefore, effective continuing health education for PD patients is critical to guarantee improvements in patients’ quality of life and long-term survival rates.5
The traditional health education program usually includes distribution of health education materials and giving training courses. The dialysis nurse will perform patient education based on their own experience without considering the context of their interaction with patients or the diversities in patients’ personalities. As most dialysis nurses have little or no formal background in principles of education, the specific needs of PD patients who must learn both procedures and problem solving could be often overlooked.6
Problem-based learning (PBL) is a problem-oriented teaching method in which self-study and discussion is the main mode of learning.7 PBL can help patients be more actively involved in disease self-management, and improve their skills, thereby enhancing their self-care abilities.8 Some systematic studies have examined the effectiveness of PBL educational models in health education, such as coronary artery disease and sleep apnea.9 These studies found that the knowledge obtained from PBL patient-education may contribute to improving patients’ abilities to handle self-care.10,11 Whether PBL could be an effective mode of learning for PD patients remains unknown.
The purpose of the present study was to evaluate the effectiveness and feasibility of patient empowerment through the PBL model in health education of patients on PD.
Methods
Study Design
Figure 1 shows the algorithm delineating the study design. The organizers have been trained in unified PBL teaching courses and passed the examination. All participants received health education guidance and assessment before and after peritoneal dialysis. The patients were randomly assigned to PBL group or traditional health education group. For the PBL group, a 90-minute activity in study groups of 9–10 patients was held every 2 months. Patients in the traditional group attended 4 classes of PD training in the first month, and then were followed up in the peritoneal clinic every two months with 30 minutes each time. The assessment tools were questionnaire, interview and observation. There was no difference regarding the opportunities and times for organizers to contact patients in the PBL group and the control group. This study was approved by the local institutional ethic committee of Fujian Provincial Hospital and complies with the Declaration of Helsinki. The permission to distribute the questionnaires for the study was obtained from hospital review board. Informed consent was obtained from all study participants. All the participants were invited voluntarily to be in this study.
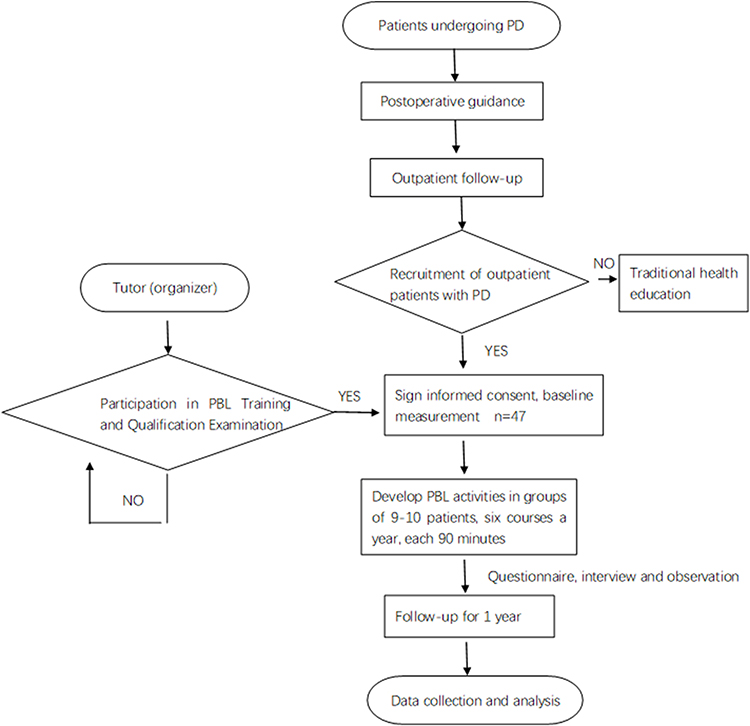 |
Figure 1 Algorithm delineating the study design. Abbreviations: PD, peritoneal dialysis; PBL, problem-based learning. |
Participants
From March 2017 to April 2017, a total of 94 participants who began PD therapy and were regularly followed up from July 2008 to March 2016 in PD clinic were included in this study. The participants were randomly assigned to the PBL group and the traditional group, with 47 patients in each group A random number generator was used to generate singular and even numbers (https://www.random.org/). These random numbers were placed in envelopes and kept by researchers, who selected patients according to inclusion and exclusion criteria and then opened the envelopes to randomly group the subjects. The inclusion criteria were as follows: (1) Patients who received PD therapy due to end stage renal disease (ESRD) more than 3 months; (2) patients older than 18 years of age; (3) patients with the ability to communicate in oral and written form. Exclusion criteria included: (1) patients with hearing impairment; (2) patients with malignancy; (3) life expectancy not exceeding one year; (4) patients with severe cardiovascular complications; (5) patients with the inability to provide written informed consent; (6) patients who received assisted peritoneal dialysis. All the patients completed the follow up.
Data Collection
The baseline data including age, marital status, educational and occupational status, duration of dialysis, complication score and dialysis dosages were collected before the study. The 2nd version of Charlson Comorbidity Index (CCI) was used to measure co-existing diseases.12 After the study, data were collected by questionnaires and interviews. All the questionnaires but the questionnaire of PD basic knowledge had been validated for Chinese population.
Questionnaires
Questionnaire of PD Basic Knowledge
The assessment questionnaire was constructed in accordance with the seven-day training standard of PD patients and common problems identified in the PD process. The 2nd version of questionnaire was used to assess the degree of mastery of basic knowledge of PD.13
Patient’s Self-Management Scale
To evaluate the behavior and attitudes of PD patients on peritoneal dialysis, we used the Chinese version of the self-management scale for PD patients created by Pang et al14 The content validity index of the scale was 0.963, Cronbach’s α was 0.926.
KDQOL-36TM (Kidney Disease Quality of Life)
To evaluate the burden of kidney disease, symptoms/problems of kidney disease, and effects of kidney disease scales, the mandarin version KDQOL-36™1.2 was used in this study.15 The reliability and validity of the questionnaire in Chinese population had been validated previously. The questionnaire consists of 36 questions covering 5 dimensions, including physical health (6 problems), mental health (6 problems), kidney burden (4 problems), symptoms and discomforts (12 problems), and effects of kidney disease (8 problems). The higher scores indicated the better quality of life.
Self-Rating Anxiety Scale (SAS) (Zung 1971)
The scale focused on the most common general anxiety disorders, which has been validated in Chinese patients on dialysis.16,17
Self-Rating Depression Scale (SDS) (Zung 1965)
A short self-administered survey was applied to quantify the depressed status of a patient.18
Patients’ Satisfaction Score
We investigated the satisfaction of the patients using a standardized questionnaire developed by the service center of the Fujian Provincial Hospital. This questionnaire was slightly modified from well-validated instruments for measuring patients’ overall satisfaction, and had been used in our previous studies.19,20
Intervention
Figure 2 summarizes the process of PBL health education method. The team of education and follow-up included one head nurse, two nephrologist and two specialist nurses. The head nurse was the organizer. According to PBL concept, patients in the PBL group were assigned in 5 study groups with 9–10 patients in each. During one year, 6 PBL health education activities were held. There were four sessions in a 90-minute activity, including 40 minutes of multimedia teaching, 30 minutes of discussion, 10 minutes of peer education, and 10 minutes of games. The tutor encouraged patients to think freely, ask questions and share learning experiences. Dialysis nurses distributed learning materials to the participants. The patients recorded their questions and brought them to the class for discussion. The content was based on the knowledge of PD, and problems they identified during self-management. The games were suitable for the physical abilities of PD patients, including playing table tennis, playing health Puzzles, and quizzes with prizes. A sample of the materials used in PBL sessions had been showed in the Supplemental Data.
 |
Figure 2 The process of PBL health education method. Abbreviation: PBL, problem-based learning. |
Data Analysis
All data were analyzed using the SPSS 18.0 software package (Chicago, IL). Continuous variables were expressed as means ± standard deviations, and the paired t-test or Wilcoxon signed-rank test was used. The categorical variables were expressed as frequencies. P<0.05 was considered statistically significant.
Results
As shown in the Table 1, there were no significant differences in age, education level, gender and occupation between the two groups. For baseline clinical parameters, there were no significant differences in baseline levels of dialysis dosages and complication score. The scores of basic knowledge, self-management behavior ability, anxiety and depression, QoL, and satisfaction were no significantly different between the two groups (Supplemental Table 1). The average follow-up duration was 10.6±1.5 months.
 |
Table 1 Baseline Characteristics of Study Patients |
Table 2 shows the comparison of basic knowledge of patients between the traditional group and the PBL group at the end of the study. Although the scores of environmental requirements were unchanged, the scores for PD fluid exchange, PD catheter and exit-site care, complication, diet, and volume control were significantly improved after the PBL module. Compared with patients in the traditional group, patients in the PBL group have higher PD fluid exchange scores (27.22±2.63 vs 28.34±2.01; P=0.032), better scores of complications (15.34±1.765 vs. 18.04±1.4; P<0.001), higher dietetic scores (4.75±1.46 vs.5.94±0.44; P<0.001), and better volume control (9.01±1.64 vs 10.15±1.47; P<0.001). Total scores of the two groups were 84.33±3.55 and 91.19±3.07 (P<0.001), respectively.
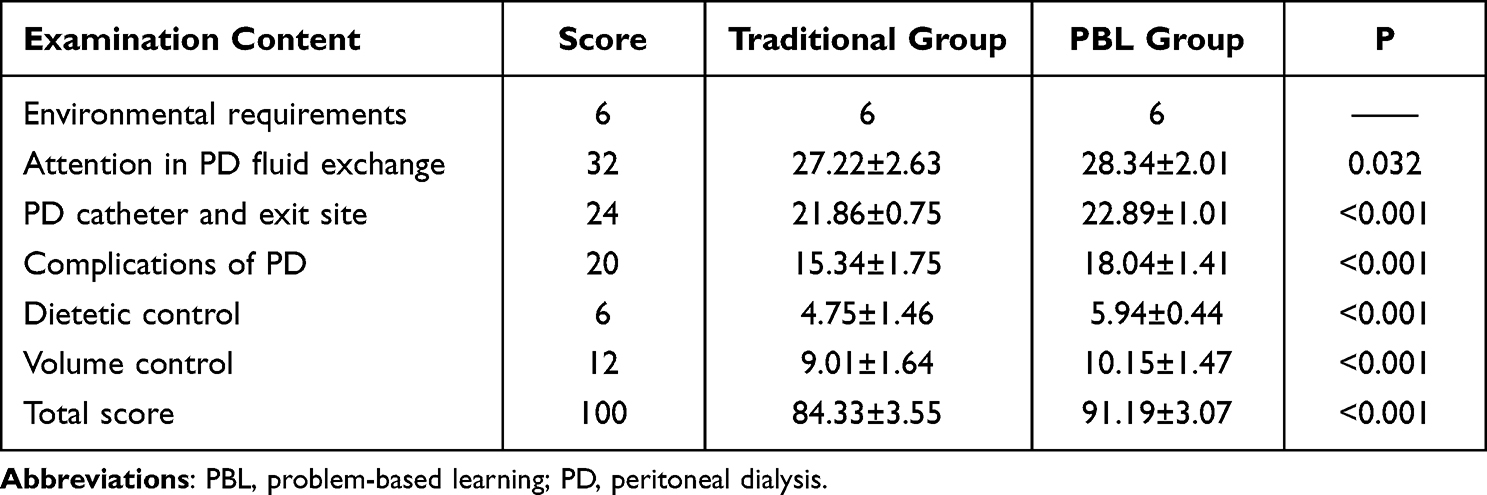 |
Table 2 Basic Knowledge of Patients Between the Two Groups (n=47) |
Table 3 shows the comparison of patient’s Self-management Behavior Ability scores between the traditional group and the PBL group. The empowerment model of PBL health education improved self-management behavior of patients. The total scores were 61.19±3.71 and 71.47±2.89 (P<0.001), respectively. Compared with the traditional group, patients in the PBL group had better skills for PD fluid exchange (16.46±1.35 vs.18.60±1.80; P<0.001), better abilities to handle actual problems in (9.06±1.07 vs.10.09±0.83; P<0.001), and higher scores for diet management (10.43±1.60 vs.12.26±1.53; P<0.001). The scores of complication monitoring score were higher (17.65±2.26 vs 20.31±1.08; P<0.001) than the traditional group. Patients in the PBL group had better abilities of emotion control, and were more willing to return to their daily life (7.61±1.14 vs 10.26±0.71; P<0.001).
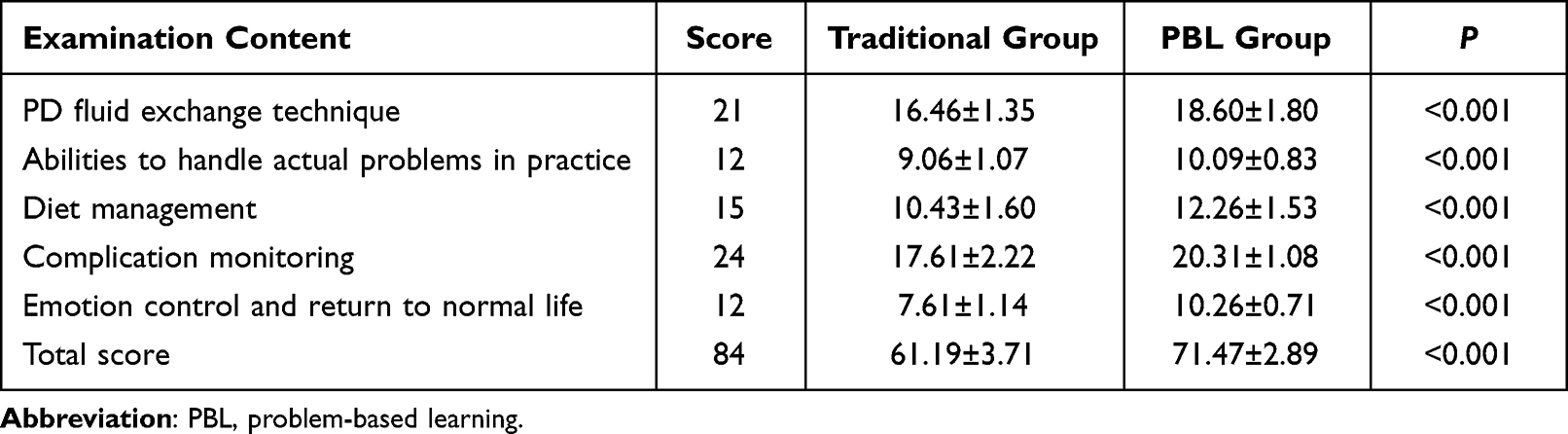 |
Table 3 Patient’s Self-Management Ability Between the Two Groups n=47) |
Table 4 shows the comparison of anxiety and depression scores between the traditional group and the PBL group. The empowerment model of PBL health education significantly improved anxiety and depression of the patients. Anxiety score among the traditional group and the PBL group were 52.39±4.56 vs 46.46±4.63 (P<0.001); depression score were 49.95±6.76 vs.45.80±8.77 (P=0.01).
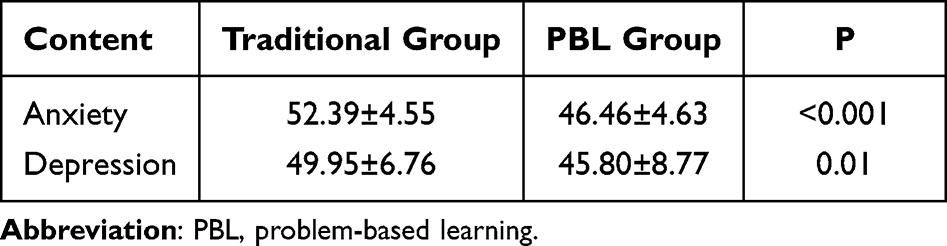 |
Table 4 Comparison of Anxiety and Depression in Patients Between the Two Groups (n=47) |
Table 5 shows the comparison of quality of life and satisfaction scores of the patients between the two groups. The model of PBL health education improved the quality of life of PD patients. Both scores of physical and mental health were significantly improved after the PBL education. Burden on the kidney score for traditional group was 10.02±3.60, and 8.47±3.32 in the PBL group (P=0.014). Furthermore, scores for symptoms/discomfort and impact of kidney disease were also significantly improved (P<0.001). Additionally, the satisfaction degree scores were 90.78±1.32 in the traditional group, and 98.21±1.25 in the PBL group (P<0.001).
 |
Table 5 Quality of Life and Satisfaction of Patients Between the Two Groups (n=47) |
Discussion and Conclusion
Discussion
Patient education is an important component of chronic disease management and a key factor in the treatment of peritoneal dialysis. Patient empowerment can strengthen capacity for self-management and improve treatment outcomes.21 In this study, we showed that the empowerment model of PBL health education could effectively improve the self-management knowledge, skills, anxiety, depression, and quality of life of PD patients. In addition, PBL health education significantly improved PD patients’ satisfaction with the hospital.
The empowerment model of PBL health education can consolidate the basic knowledge of PD patients. It has been indicated that the health education model is useful in experiential learning, coping with problems, problem solving and learning goal setting.22 PD learner education and training program are crucial to ensuring positive outcomes of PD therapy.23 The patients should be taught self-management skills as well as the concepts. Attention will be particularly paid to the communication skills between PD educator and patients to avoid losing participants’ enthusiasm for learning. Some patients may require individualized PD education, such as face-to-face support, telemedicine and re-training. PBL could be used as the vehicle to not only promote learning of concepts, but also the development of problem-solving abilities, and communication skills. Our findings were consistent with a previous study in cardiac rehabilitation in which the PBL intervention exhibited positive effects on risk factors for compared to home-sent patient information.24
Promoting self-management has been found to be effective in improving the health of patients with diabetes and other chronic diseases.25 Studies have shown that psycho-social and educational interventions should be considered as effective strategies to improve dialysis compliance in adults with end-stage renal disease. Similarly, in our study, the PBL health education improved self-management behavior of patients.
Anxiety and depression are common in dialysis patients, which may predict technique and patient survival26 The PBL model of health education could provide a relaxed, harmonious and active learning environment between doctors and patients. After the empowerment of patients, learning can effectively avoid the increase of psychological burden due to poor knowledge. Previous studies showed that PD at home aided preservation of pre-illness identity, but resulted in the feelings of isolation and being misunderstood.27 After intervention such as telemedicine, patients felt a greater sense of control, and achieved positive attitude.28 In our study, the empowerment model of PBL health education could be another effective intervention to improve anxiety among PD patients.
Moreover, the empowerment model of PBL health education improved PD patients’ satisfaction with the hospital. Patient-centred care has become the dominant paradigm in modern health care. Shared decision making is the essence of the process and needs to be a standard principle of care, which requires patient engagement, education and empowerment.28 When patients are empowered, they may feel they are co-decision makers, which may promote care individualization, improve their trust and loyalty to the hospital and medical providers.
Principal Findings in Comparison to the Existing Literature
Although the field of PBL is developing, there are few systematic studies on the use and effect of PBL education technology in patient health education. The research is a well randomized controlled, providing benefit to the participants both in terms of knowledge and psychosocial quality of life measures.
Strengths and Limitations of the Study
Our strength of this study was its focus on effectiveness within a model of chronic disease management with a standardized collected data. However, there were several limitations. First, the relatively small sample size might contribute to lower statistical efficiency than a study with a larger sample size. Second, the follow-up duration was relatively short. The long term effects of this model on the outcomes of PD patients should be investigated further. Third, the age group was relatively young in this study because we only included the patients who were able to communicate in oral and written form. Those who were on assisted peritoneal dialysis had been ruled out which may have led to selection bias. Fourth, the single-centre design was useful for standardized implementation of our study intervention, but it limits the generalizability of findings. Finally, a lack of blinding may lead to possible performance bias.
Conclusion
The empowerment model of PBL health education can improve the quality of life of PD patients. This study’s findings point to the need for more effective management procedures to improve health-related quality of life in patients at all stages of chronic kidney diseases.
Relevance to Clinical Practice
The results of this study show that the empowerment model of PBL health education in health education of patients with continuous peritoneal dialysis is effective. As the basis of learning process, PBL can be used to assess the impact of various types of health education models on patients’ ability. This new model of health education can consolidate the basic knowledge of peritoneal dialysis, improve the ability of self-management behavior, improve the state of anxiety and mental illness, and improve the quality of life of peritoneal dialysis patients.
Abbreviations
PBL, Problem-based learning; PD, peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis; ESRD, end stage renal disease; KDQOLTM (Kidney Disease Quality of Life); SAS, Self-rating Anxiety Scale; SDS, Self-rating Depression Scale.
Acknowledgment
This project was supported by the 2014 Appropriate Technology Promotion Funding Plan for primary organizations and cities, the Fujian Provincial Health and Family Planning Commission, the Clinical Specialty Discipline Construction Program of Fujian, a special grant for education and research from Fujian Department of Finance(2022)840, Provincial Natural Science Foundation of Fujian province (No. 2019J01172) and Young and middle-aged Scholars Program of Fujian Health Commission (No. 2019-ZQN-7).
Part of the results was presented in abstract form at the World Congress of Nephrology, April 12 to 15, 2019, in Melbourne, Australia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Fang Cao is the first author.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Wang F, Zhang L, Wang H. China national survey of CKDWG. awareness of CKD in China: a national cross-sectional survey. Am J Kidney Dis. 2014;63(6):1068–1070. doi:10.1053/j.ajkd.2014.01.012
2. Hurst H, New Peritoneal A. Dialysis training guideline from the ISPD nursing committee. Perit Dial Int. 2016;36(6):585–586.
3. Li PK, Chow KM, Van de Luijtgaarden MW, et al. Changes in the worldwide epidemiology of peritoneal dialysis. Nat Rev Nephrol. 2017;13(2):90–103.
4. Baillie J, Lankshear A, Featherstone K. Perspectives on peritoneal dialysis at home: implications for the management of a chronic condition. A study protocol. J Adv Nurs. 2012;68(8):1847–1857.
5. Grangier JP. Usage de la télémédecine en dialyse et nouvelles pratiques professionnelles [The use of telemedicine in dialysis and new professional practices]. Soins. 2016;61(810):38–40. French.
6. Hult H, Lindblad Fridh M, Lindh Falk A, Thorne K. Pedagogical processes in healthcare: an exploratory study of pedagogic work with patients and next of kin. Educ Health. 2009;22(3):199.
7. Ng ML, Bridges S, Law SP, Whitehill T. Designing, implementing and evaluating an online problem-based learning (PBL) environment--A pilot study. Clin Linguist Phon. 2014;28(1–2):117–130.
8. Williams B, Pace AE. Problem based learning in chronic disease management: a review of the research. Patient Educ Couns. 2009;77(1):14–19.
9. Karner A, Nilsson S, Jaarsma T, et al. The effect of problem-based learning in patient education after an event of CORONARY heart disease--A randomised study in PRIMARY health care: design and methodology of the COR-PRIM study. BMC Fam Pract. 2012;13:110.
10. Mayner L, Gillham D, Sansoni J. Anatomy and physiology for nursing students: is problem-based learning effective? Prof Inferm. 2013;66(3):182–186. doi:10.7429/pi.2013.663182
11. Khatiban M, Sangestani G. The effects of using problem-based learning in the clinical nursing education on the student’s outcomes in Iran: a quasi-experimental study. Nurse Educ Pract. 2014;14(6):698–703. doi:10.1016/j.nepr.2014.10.002
12. Rattanasompattikul M, Feroze U, Molnar MZ, et al. Charlson comorbidity score is a strong predictor of mortality in hemodialysis patients. Int Urol Nephrol. 2012;44(6):1813–1823. doi:10.1007/s11255-011-0085-9
13. Sarian M, Brault D, Perreault N. Self-management support for peritoneal dialysis patients. CANNT J. 2012;22(3):18–24.
14. Wang X-H, Pang J-H, Lin L, et al. Development and testing of self-management scale for PD patients. Perit Dial Int. 2015;35(3):342–350. doi:10.3747/pdi.2013.00190
15. Tao X, Chow SKY, Wong FKY. Determining the validity and reliability of the Chinese version of the kidney disease quality of life questionnaire (KDQOL-36™). BMC Nephrol. 2014;15(1):115. doi:10.1186/1471-2369-15-115
16. Zung WWK. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
17. Wang C, Zhang X, Zhu B, et al. Relationships between tumour necrosis factor-α, interleukin-12B and interleukin-10 gene polymorphisms and hepatitis B in Chinese Han haemodialysis patients. Nephrology. 2012;17(2):167–174. doi:10.1111/j.1440-1797.2011.01539.x
18. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515.
19. Grogan S, Conner M, Norman P, Willits D, Porter I. Validation of a questionnaire measuring patient satisfaction with general practitioner services. Qual Health Care. 2000;9(4):210–215.
20. Cao F, Li L, Lin M, Lin Q, Ruan Y, Hong F. Application of instant messaging software in the follow-up of patients using peritoneal dialysis, a randomised controlled trial. J Clin Nurs. 2018;27(15–16):3001–3007.
21. Llambi L, Barros M, Parodi C, Cora M, Garces G. Teaching tobacco cessation to large student cohorts through train-The-trainers and problem based learning strategies. Educ Health. 2016;29(2):89–94.
22. Tang TS, Funnell MM, Brown MB, Kurlander JE. Self-management support in “real-world” settings: an empowerment-based intervention. Patient Educ Couns. 2010;79(2):178–184.
23. Schaepe C, Bergjan M. Educational interventions in peritoneal dialysis: a narrative review of the literature. Int J Nurs Stud. 2015;52(4):882–898.
24. Kohler AK, Jaarsma T, Tingstrom P, Nilsson S. The effect of problem-based learning after coronary heart disease - A randomised study in primary health care (COR-PRIM). BMC Cardiovasc Disord. 2020;20(1):370.
25. Su CY, Lu XH, Chen W, Wang T. Promoting self-management improves the health status of patients having peritoneal dialysis. J Adv Nurs. 2009;65(7):1381–1389.
26. Feroze U, Martin D, Kalantar-Zadeh K, Kim JC, Reina-Patton A, Kopple JD. Anxiety and depression in maintenance dialysis patients: preliminary data of a cross-sectional study and brief literature review. J Ren Nutr. 2012;22(1):207–210.
27. Duncanson E, Chur-Hansen A, Jesudason S. Patient perspectives of coping with automated peritoneal dialysis. Perit Dial Int. 2022;42(4):344–352.
28. Krishna VN, Managadi K, Smith M, Wallace E. Telehealth in the delivery of home dialysis care: catching up with technology. Adv Chronic Kidney Dis. 2017;24(1):12–16.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.