Back to Journals » International Journal of Women's Health » Volume 17
Effect of Oral Probiotics Use in HR-HPV Clearance, a Retrospective Study
Received 17 May 2025
Accepted for publication 26 September 2025
Published 4 October 2025 Volume 2025:17 Pages 3489—3498
DOI https://doi.org/10.2147/IJWH.S539622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Video abstract of “Effect of oral probiotics use in HR-HPV clearance” [539622].
Views: 59
Mustafa Şahin, Özgün Ceylan
Department of Gynecologic Oncology, Ankara City Hospital, Ankara, Turkey
Correspondence: Mustafa Şahin, Üniversiteler Mahallesi, 1604, Cadde No: 9, Çankaya/Ankara, Turkey, Tel +90 05458585420, Email [email protected]
Purpose: This study investigates the effects of oral administration of Lactobacillus rhamnosus on the clearance of high-risk human papillomavirus (HR-HPV) and cervical cytology outcomes.
Patients and Methods: In this retrospective observational study, histology results were analyzed from patient files and pathology reports of 218 patients who were positive for cervical HR-HPV DNA and had no evidence of high-grade cervical intraepithelial lesions. The study group (n=105) consisted of patients who had used V-Flora oral capsules containing L. rhamnosus and zinc for three months. We compared HR-HPV DNA and cervical cytology results between the study and control groups at 6 and 12 months.
Results: No significant differences were found in HR-HPV clearance or cervical cytology results between users and non-users of L. rhamnosus at both 6 and 12 months (6 months hazard ratio: − 0.0228, 95% CI: − 0.1623 to 0.1167, p=0.777 and 12 months hazard ratio: − 0.1165, 95% CI: − 0.3467 to 0.1088, p=0.295). The hazard ratios and p-values indicate no significant impact on HR-HPV clearance or cytology outcomes, including in patients who remained HPV positive after 6 months (hazard ratio: − 0.1167, 95% confidence interval: − 0.3500 to 0.1165; p=0.333).
Conclusion: The anticipated beneficial effects of oral administration of Lactobacillus rhamnosus on HR-HPV clearance and cervical cytology outcomes were not demonstrated in this study. Further research is needed to confirm these findings.
Keywords: Lactobacillus rhamnosus, human papillomavirus, oral probiotic use, HR-HPV clearance, vaginal microbiota
Introduction
Human papillomavirus (HPV) is an oncogenic DNA virus playing a central role in the development of cervical cancer. Of the more than 200 different HPV types identified, about 40 can infect the anogenital mucosa.1 HPV 16 and HPV 18 are responsible for approximately 70% of all cervical cancer cases.2 However, studies have shown that HPV 16, 31, 51, 52 and 58 are among the most common genotypes found in cervical high-grade lesions.3,4
Following micro-traumas in the squamous epithelium of the cervix, the basal layer cells are exposed, allowing HPV virus access.5 Heparan sulfate proteoglycans serve as critical primary attachment factors for HPV in epithelial cells.6 Lactobacillus species play a key role in maintaining maintaining a low vaginal pH by producing lactic acid and hydrogen peroxide. Alterations in the vaginal microbiota may impact the acquisition of cervical HPV infection by reducing cervical mucus production, thereby decreasing viral capture.7,8 Additionally, many infective agents directly or indirectly affect the immune response to HPV. Caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection induces dysfunction in both innate and adaptive immune responses, impairing viral clearance mechanisms critical for HPV control. Dysregulated interferon responses and reduced cytotoxic T lymphocyte activity observed in COVID-19 patients may facilitate the survival and integration of HPV into host epithelial cells and may cause histopathological skin findings similar to HPV infection.9,10
Vaginal microbiota (VM) can play both protective and detrimental roles in HPV acquisition, clearance, persistence and development of preinvasive/invasive lesions. The predominance of Lactobacillus crispatus (L. crispatus) was protective against the development of bacterial vaginosis (BV) and was mostly observed in “healthy” women, while L. iners was associated with the development of BV.11 King et al reported delayed clearance of HPV in women with bacterial vaginosis.12 In another meta-analysis, BV was associated with increased rates of HPV infection.8 In vitro studies on BV-associated bacteria show that many of them influence proinflammatory responses by modulating immune parameters. These proinflammatory responses can lead to tissue damage, which increases the oncogenic potential of HPV.5
Probiotic strains act on HPV clearance through three mechanisms. First, probiotic strains create a synergistic environment through anti-microorganism effects and production of inhibitory compounds.13 Secondly, they enhance innate and acquired immunity against viral infections.14 Third, a direct antiviral effect is exerted through the secretion of specific metabolite.15
Vaginal microbiota likely plays an important role in the development of immune responses in association with anti-HPV vaccination.16 However, the vaginal microbiota likely plays an essential role in immune responses associated with anti- HPV vaccination. Recent data suggest that VM has an important role in the development of immune responses.17 Today, the vaginal microbiome can be modulated through the use of probiotics. Although the VM is generally considered to be protected from most gut microbiota species, gut microbiota may act as a reservoir for VM.18 Probiotics, when used orally, have the ability to colonize the vaginal area from the gut. Reid et al reported evidence that L. rhamnosus can be delivered to the vagina following oral ingestion.13 L. rhamnosus is considered to be a true probiotic due to its ability to colonize the intestinal/vaginal ecosystem and provide health benefits to the host,19 and it has been successfully used as a commercial pharmaceutical product for over 20 years.
Considering the role of vaginal flora in HPV acquisition and persistence, it is conceivable that the use of L. rhamnosus may have a positive role in HPV clearance. Prospective, observational studies are needed to determine the role of vaginal flora alteration in HPV acquisition, clearance, prevention of persistence and regression of cervical preinvasive lesions. In our retrospective, non-randomized study, the effects of oral administration of Lactobacillus rhamnosus on HR-HPV clearance and cervical smear results will be investigated.
Material and Methods
Study Participants
Patients who were HR-HPV DNA positive and had either no cervical dysplasia or only a low-grade lesion detected in colposcopic biopsy was considered for inclusion in the study. Eligible participants were women aged 30 to 65 years who had not received HPV vaccination, had no history of partial or total cervical excision, no systemic disease or medication use that could affect the vaginal flora, no symptomatic cervico-vaginal infection, and no gastrointestinal dysfunction.
Patients with other sexually transmitted diseases (STDs) outside of HPV were excluded from the study. During the study, patients were excluded if they received HPV vaccination, became pregnant, were diagnosed with a cervical high-grade lesion or cervical cancer, underwent cervical excisional, destructive, or ablational procedures, or were taking medication that could affect the vaginal flora.
The use of medication was not at the discretion of the clinician. The study group consisted of patients who used V-Flora oral capsules (Assos Pharmaceuticals, Umraniye, Istanbul) twice a day for the first 10 days and then once a day for a total of 3 months (each V-Flora oral capsule contains L. rhamnosus (Lcr) 11.25 mg and Zinc 7.5 mg). HPV DNA and Pap smear results were recorded at baseline, and at 6 and 12 months after diagnosis in the study group. In the L. rhamnosus group, results were also noted from the beginning of treatment. We used the HPV Genotyping Detection Kit (Fluorescence Polymerase Chain Reaction-PCR Method), which has a detection limit of 1000 copies/mL. The liquid-based cytology preparation was conducted using the NOVAprep® system from Novaprep Inc., Russia, and the Max-prep® system from Corebiotech Co., Ltd., Korea. HPV DNA was subsequently identified and classified using the QIAscreen HPV PCR kit (Qiagen Inc., Germany). Colposcopy was performed in HR-HPV positive and/or abnormal smear results. Patients with a cervical high-grade lesion reported on colposcopic biopsy were excluded from the study.
Finally, a total of 326 women were evaluated for eligibility. Sixty-six individuals were excluded because they did not meet the criteria. The remaining 260 women with HR-HPV infection were enrolled (130 patients in the study group and 130 patients in the control group). Seventeen women in the control group and 25 women in the study group were further excluded from analysis due to lost follow-up or discontinued treatment. The study was completed with a total of 218 patients: 105 in the study group and 113 in the control group. The process flow chart for selecting patients is shown in Figure 1.
 |
Figure 1 Patient selection flow chart. Flow chart showing the selection process of study participants. The diagram illustrates the systematic approach used to identify and enroll eligible patients from the initial screening population. Starting from 266 patients who were initially screened, the chart demonstrates the step-by-step exclusion criteria applied and the final number of participants included in the study analysis. Each box represents a distinct stage in the selection process, with exclusion criteria and numbers clearly indicated at each decision point. The final study population consisted of 202 patients who met all inclusion criteria and completed the 6-month follow-up period. |
Various factors, including age, parity, use of intrauterine devices (IUDs), educational level, menopausal status, smoking habits, and oral contraceptive use, were compared between the two groups. Additionally, we compared smear results, HR-HPV type, and colposcopy outcomes. Specific comparisons included HPV DNA status (positive or negative), smear results categorized as NILM (Negative for intraepithelial lesion or malignancy), ASC-US (Atypical Squamous Cells of Undetermined Significance), LSIL (Low-grade Squamous Intraepithelial Lesion), ASC-H (Atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion), HSIL (High-grade Squamous Intraepithelial Lesion), and Unsatisfactory. Histology results (Normal, CIN1, CIN2, and CIN3) were also compared between patients in the V Flora group post-treatment and those in the control group.
HPV infection was detected using polymerase chain reaction (PCR) amplification of viral DNA followed by dot hybridization to identify relevant subtypes. Cervico-vaginal smear (cytology) was evaluated by expert pathologists. Cervical biopsies (histology) were evaluated by expert pathologists using the Bethesda system (TBS) and the cervical intraepithelial neoplasia (CIN) classification terminology.20 Colposcopy assessment was performed on the basis of the terminology introduced by the Nomenclature Committee of the International Federation for Cervical Pathology and Colposcopy in 2011.21
Data Collection Process
The study was a retrospective, non-randomized study conducted in the gynecologic oncology surgery clinic of Ankara City Hospital, Ankara, Turkey between May 15, 2021, and November 15, 2022. This study complies with the Declaration of Helsinki. Informed consent was obtained from all patients. Data were obtained from the electronic database system, patient files and pathology reports.
To achieve 75% power at a 0.05 significance level, an overall sample size of at least 180 subjects was necessary (90 in the control group and 90 in the treatment group). With an alpha (α) of 0.05 for the type I error level and a beta (β) of 0.10 for the type II error level, the study’s power was 0.90, and the number of samples determined for inclusion in the study was n=210.
Statistical Analysis
Compatibility of quantitative variables with normal distribution was examined by Shapiro Wilk test. For variables that conform to a normal distribution, independent two-group comparisons were analyzed using the independent samples t-test. For variables that did not conform to normal distribution, independent two-group comparisons were performed with Mann Whitney u-test. Differences between frequency distributions according to groups in qualitative variables were analyzed with Chi Square test and Fisher exact test. Statistical significance was accepted as p<0.05. Statistical parameters were expressed as mean, standard deviation, median (25% quartile-75% quartile), n (number) and % (percentage). IBM SPSS version 22 (IBM SPSS for Windows version 22, IBM Corporation, Armonk, New York, United States) program was used to evaluate the data.
Results
The mean age of the control group was 39.9±10.1 years and ranged between 30 and 63 years. The mean parity of the patients was 1.85±1.21. There were 25 (22.1%) IUD users, 52 (46%) patients with a bachelor’s degree or higher, 88 (77.9%) in premenopause, 44 (38.9%) smokers, and 32 (28.3%) oral contraceptive users. There were 64 (46.6%) patients with NILM and 49 (43.4%) with AS-CUS/LSIL. There were 16 (14.2%) with HPV 16, 13 (11.5%) with HPV 18 and 84 (74.3%) with other HR-HPV types. In colposcopy, there were 65 (47.5%) patients with normal and 34 (40.1%) with CIN1 (Table 1).
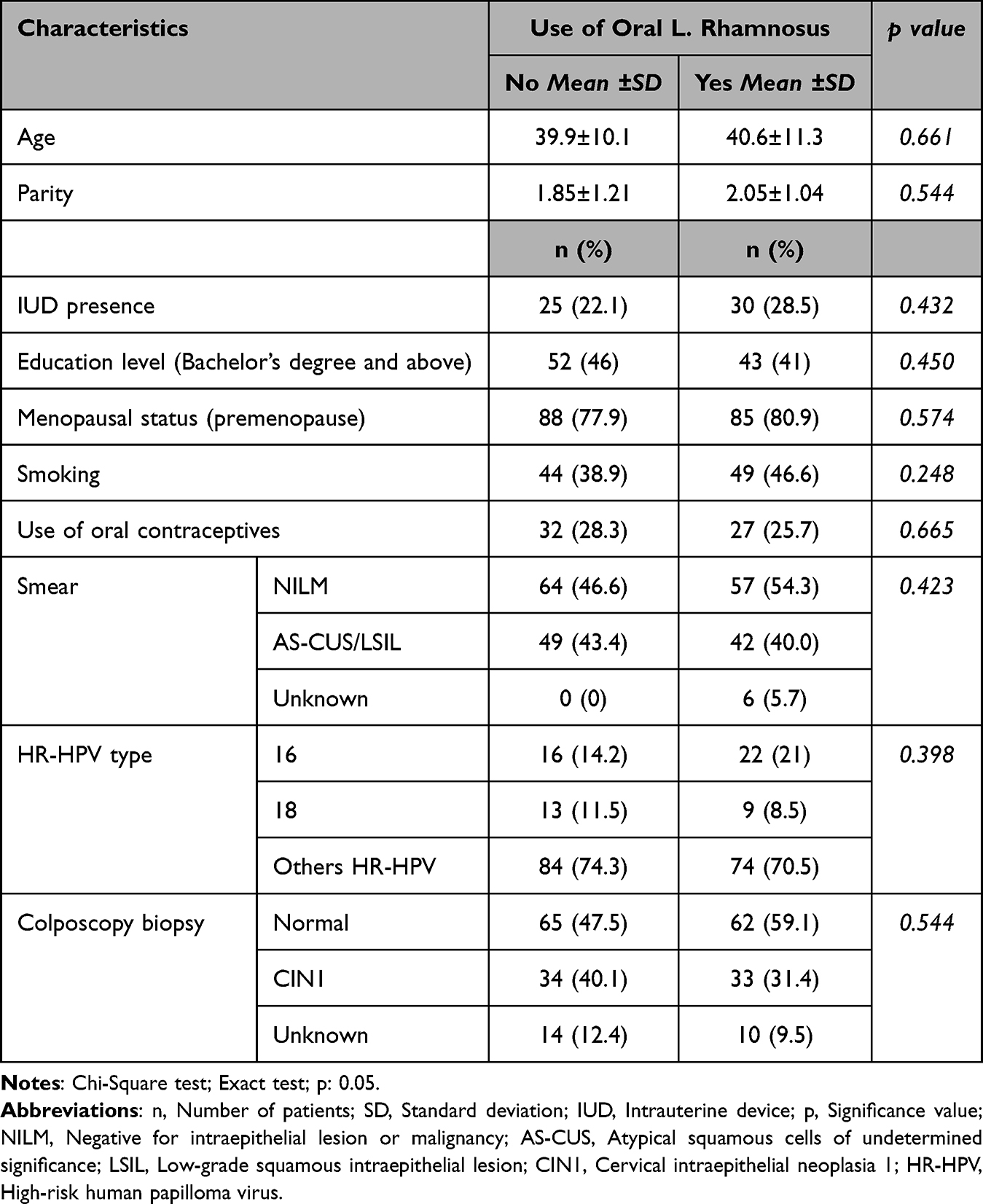 |
Table 1 Demographic and Clinico-Pathologic Characteristics of the Control Group and the Oral L. rhamnosus Group |
The mean age of the L. rhamnosus group was 40.6±11.3 years and ranged between 30 and 65 years. The mean parity of the patients was 2.05±1.04. There were 30 (28.5%) IUD users, 43 (41%) with a bachelor’s degree or higher, 85 (80.9%) in premenopause, 49 (46.6%) smokers, and 27 (25.7%) oral contraceptive users. There were 57 (54.3%) NILM patients and 42 (40%) with AS-CUS/ LSIL. There were 22 (21%) with HPV 16, 9 (8.5%) with HPV 18 and 74 (70.5%) with other HR-HPV types. While 62 (59.1%) patients had normal histopathology in colposcopy biopsy, CIN1 was detected in 33 (31.4%) patients. The demographic and clinico-pathologic characteristics of the control and oral administration of Lactobacillus rhamnosus groups are summarized in Table 1. There were no statistically significant differences between the control and L. rhamnosus groups in terms of age, parity, presence of intrauterine device (IUD), education level, menopausal status, smoking, oral contraceptive use, smear, HPV type, colposcopy (p=0.582, p= 0.544, p=0.432, p=0.450, p=0.574, p=0.248, p=0.665, p=0.423, p=0.398, p=0.544 respectively).
After 6 months, there were 79 (69.9%) patients with NILM results, 28 (24.8%) with AS-CUS and 6 (5.3%) with LSIL in the control group. There were 73 (64.6%) HPV negative and 40 (35.4%) HPV positive patients. There were 15 (13.3%) with HPV 16, 3 (2.7%) and 22 (19.4%) with other HR-HPV types. On colposcopy biopsy, there were 10 (50%) patients with normal histopathology, 9 (45%) with CIN1, and 1 (5%) with CIN2 (Table 2).
 |
Table 2 Smear, HPV, and Colposcopy Results After 6 months for the Control Group and the Oral L. rhamnosus Group (n=113 and n=105, Respectively) |
After 6 months, there were 70 (66.7%) patients with NILM results, 29 (27.6%) with AS-CUS and 6 (5.7%) with CIN1 in the L. rhamnosus group. There were 70 (66.7%) HPV negative and 35 (33.3%) HPV positive patients. There were 9 (8.6%) patients with HPV 16, 4 (3.8%) and 22 (20.9%) with other HR-HPV types. On colposcopy biopsy, there were 5 (31.8%) patients with normal histopathology, 5 (31.3%) with CIN1, 5 (31.3%) with CIN2 and 1 (6.3%) with CIN3 in the L. rhamnosus group. The smear, HR-HPV and colposcopy results of patients in the control and oral administration of Lactobacillus rhamnosus groups after 6 months are summarized in Table 2 (n=113 and n=105, respectively). After 6 months, no statistically significant difference was found between the groups in terms of smear results (p=0.875), HPV status (hazard ratio: −0.0228, 95% confidence interval: −0.1623 to 0.1167; p=0.777), HPV types (p=0.585), and colposcopy results (p=0.172) between L. rhamnosus non-users and users.
After 6 months, since 1 patient with CIN2 in the control group, 5 patients with CIN2 and 1 patient with CIN3 in the study group underwent excisional procedures, the data of these patients were not included in the results after 12 months.
After 12 months, there were 93 (83%) patients with NILM results, 16 (14.3%) with AS-CUS and 3 (2.7%) with LSIL in the control group. There were 94 (83.9%) HPV negative and 18 (16.1%) HPV positive patients. There were 4 (3.6%) with HPV 16 and 12 (10.7%) with other HR-HPV types (Table 3).
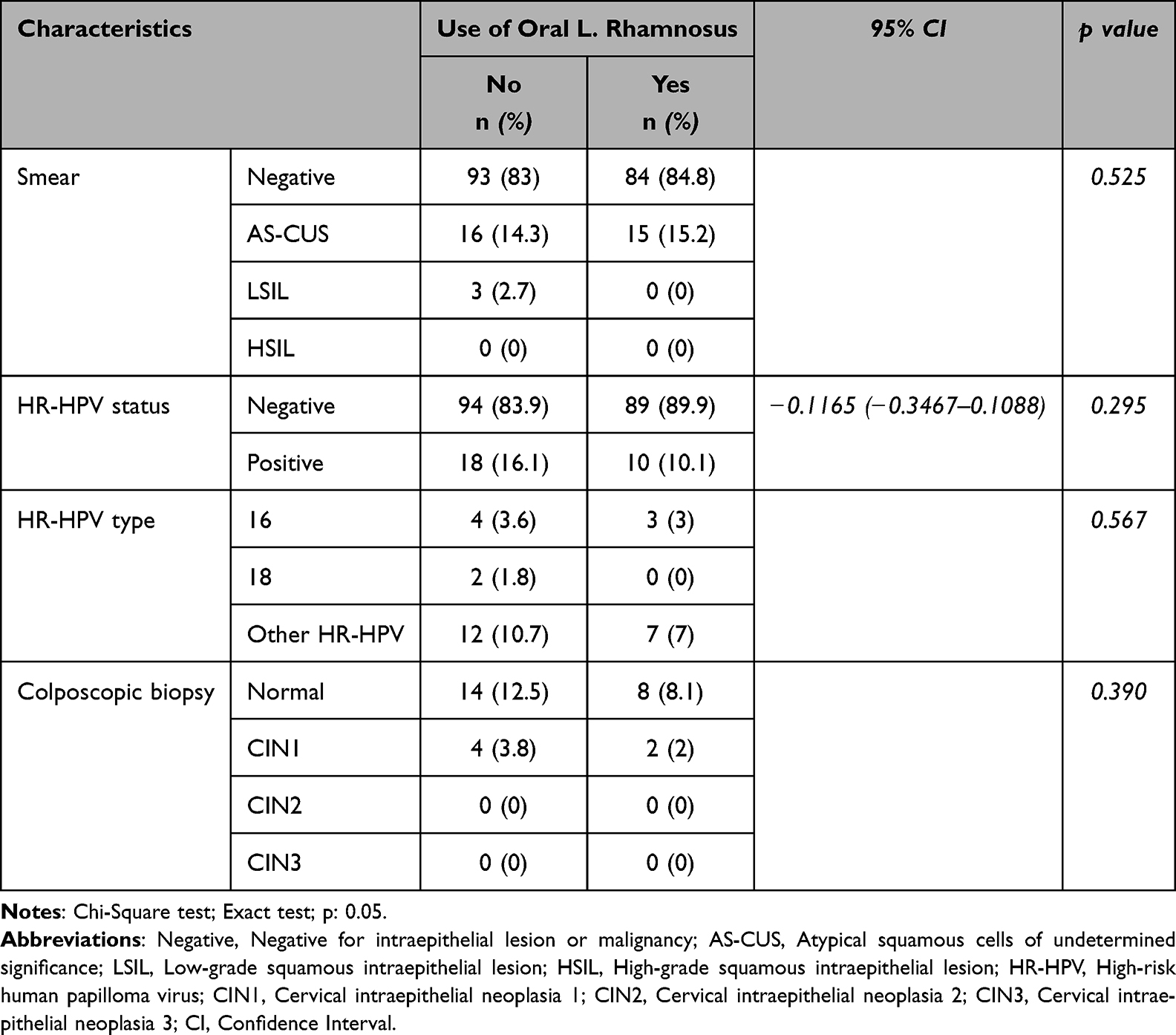 |
Table 3 Smear and HPV Results After 12 months for the Control and Oral L. rhamnosus Groups (n=112 and n=99, Respectively) |
After 12 months, there were 84 (84.8%) patients with NILM results and 15 (15.2%) patients with AS-CUS in the L. rhamnosus group. There were 89 (89.9%) HPV negative patients and 10 (10.1%) HPV positive patients. There were 3 (3%) patients with HPV 16 and 7 (7%) with other HR-HPV types. The smear and HPV results of the control and oral administration of Lactobacillus rhamnosus groups after 12 months are summarized in Table 3. After 12 months, no statistically significant difference was detected in the smear results (p=0.525), HPV status (hazard ratio: −0.1165, 95% confidence interval: −0.3467 to 0.1088; p=0.295), HPV types (p=0.567) and colposcopic biopsy (p=0.390) between L. rhamnosus non-users and users (Table 3).
In HPV-positive patients after 6 months, no statistically significant difference was found between L. rhamnosus users and non-users in terms of HPV clearance rates after 12 months (hazard ratio: −0.1167, 95% confidence interval: −0.3500 to 0.1165; p=0.333). The HPV results after 12 months in patients who remained HPV positive after 6 months are summarized in Table 4.
 |
Table 4 HR-HPV Results After 12 months in the Control and Oral L. rhamnosus Groups for Those Who Remained HR-HPV Positive After 6 months (n=39 and n=29, Respectively) |
Discussion
L. rhamnosus is a true probiotic due to its ability to colonize the intestinal and vaginal ecosystem and confer health benefits to the host. In addition to its positive probiotic activity, L. rhamnosus is known to inhibit the growth of Gardnerella vaginalis.22 Forestier et al showed that L. rhamnosus has antibacterial activity against various pathogens.23
Although the vaginal flora is partially protected from the intestinal flora, the latter appears to serve as a reservoir for the former.18 Contamination of the vagina by intestinal flora may occur through the neighborhood. These results suggest that oral administration of Lactobacillus rhamnosus use may have an auxiliary role in HPV clearance. In our study, we found no statistically significant difference in HPV clearance, smear and colposcopy biopsy results after 6 months and 12 months in oral administration of Lactobacillus rhamnosus users compared to non-users (p=0.777, p=0.295, p=0.875, p=0.525 and p=0.172, p=0.390, respectively). There was no statistically significant difference in the rate of HPV clearance after 12 months in those who used L. rhamnosus and were still HPV positive after 6 months (p=0.333).
The use of some Lactobacillus species in the treatment of bacterial vaginosis may be beneficial. Studies by Kumari et al, Chew et al, and Ho et al, showed that bacterial vaginosis regressed with the use of L. rhamnosus and Lactobacillus reuteri (L. reuteri).20,23,24 Verhoeven et al found a significant decrease in abnormal cervical smear results when oral Lactobacillus Shirota was given to patients with HPV positive and low-grade cervical lesions (p=0.05).25 However, there was no statistically significant difference in HPV clearance rates (p=0.41). However, the small sample size is the most important disadvantage of this study, and it would be appropriate to evaluate the results on this scale.
Zeng et al showed that vaginal Lactobacillus and interferon treatment may increase HPV clearance in patients.26 Palma et al compared two groups with active bacterial vaginosis or fungal vaginitis who received vaginal L. rhamnosus for 3 months and 6 months after standard anti-infective therapy.27 HPV clearance was significantly increased in those who used L. rhamnosus for at least 6 months (p=0.044) and the reduction in abnormal smear rates was significant (p=0.041). The study by Palma et al is significant as it demonstrates that long-term vaginal L. rhamnosus use after standard anti-infective therapy may aid in HPV clearance and regression of the cervical smear abnormalities.27 Unlike the study by Palma et al, which administered vaginal L. rhamnosus, in our study, only oral L. rhamnosus was administered to the patient group. In contrast to anti-infective therapy, patients using medications that could affect the vaginal flora or those with symptomatic cervico-vaginal infections were not included in the study. In our study, there was no difference between the groups in HPV clearance and smear results. Differences in vaginal and oral use of Lactobacillus rhamnosus or the administration of anti-infective therapy may have affected HPV clearance and smear results.
However, there are very few studies evaluating the relationship between oral administration of Lactobacillus rhamnosus use and HPV clearance and smear results in HPV positive patients. In the study by Ou et al, in which oral administration of Lactobacillus rhamnosus and L. reuteri versus placebo was given to the control group, there was no statistically significant difference in HPV clearance rates between the groups (p=0.741).28 However, abnormal cervical smear results were significantly reduced in the group given L. rhamnosus and L. reuteri (p=0.017). Our study is the second to investigate HPV clearance and smear results with oral administration of Lactobacillus rhamnosus, following the study by Ou et al. It is more comprehensive in terms of the number of patients. The limitation of Ou et al’s study is that factors affecting HPV clearance such as BV status, smoking and oral contraceptive use were not included in the analysis. Unlike Ou et al’s study, our study also analyzed age, parity, presence of an IUD, education level, menopause status, smoking, or oral contraceptive use, and there were no differences between the groups.
In the study by Perisic et al, the reduction in abnormal cervical smear results was significant in the group of patients receiving additional anti-infective treatment with oral administration of Lactobacillus rhamnosus and L. reuteri.29 A similar result was obtained anti-infective treatment with vaginal use of probiotics in the study by Palma et al.27 These results suggest that anti-infective treatments may help probiotic effects.
Probiotics well-known for their role in the treatment and prevention of BV and vulvovaginal candidiasis, but their role in HPV infection has not been fully elucidated. Although increased HPV clearance with vaginal L. rhamnosus use has been shown in a limited number of studies, the results of these studies are contradictory. Similarly, although a few studies have shown a decrease in abnormal cervical smear results with oral administration of Lactobacillus rhamnosus, no study has demonstrated an increase in HPV clearance. The type, route of administration, dose, duration and mechanisms of action of the probiotic should be clarified.
Our study is the most comprehensive study investigating the relationship between oral administration of Lactobacillus rhamnosus and HR-HPV clearance and smear results. There were no significant limitations in our study, as the sample size and follow-up period were adequate compared to similar studies. Risk factors that may be associated with HPV persistence in patients were also included in the analysis.
Conclusion
The anticipated beneficial effects of oral administration of Lactobacillus rhamnosus on HPV clearance have not been conclusively demonstrated in empirical studies. While some studies suggest a positive impact on smear results, these findings remain inconsistent. Future studies should aim to elucidate the optimal type of probiotic, route of administration, dosage, and duration, as well as the underlying mechanisms of action, to provide clearer insights.
Abbreviations
AS-CUS, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion; BV, bacterial vaginosis; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR-HPV, high risk human papillomavirus; HSIL, high-grade squamous intraepithelial lesion; IUD, intrauterine device; L. rhamnosus, Lactobacillus rhamnosus; LEEP, loop electrosurgical excision procedure; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; PCR, polymerase chain reaction; VM, vaginal microbiota.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author (Mustafa Şahin).
Ethics Approval and Informed Consent
The study was approved by the University of Health Sciences Turkey, Ankara Bilkent City Hospital Clinical Research Ethics Committee (approval number: E2-21-447, date: 05.05.2021).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding for this research.
Disclosure
The authors have declared they have no conflicts of interest.
References
1. De Villiers EM. Cross-roads in the classification of papillomaviruses. Virology. 2013;445(1–2):2–10. doi:10.1016/j.virol.2013.04.023
2. Arbyn M, Tommasino M, Depuydt C, Dillner J. Are 20 human papillomavirus types causing cervical cancer? J Pathol. 2014;234(4):431–435.
3. Pruski D, Millert-Kalinska S, Klemenska P, Jach R, Przybylski M. Clinical use of the Onclarity test with extended HPV genotyping and phenotyping in patients with suspected squamous intraepithelial lesions. Ginekologia Polska. 2024;95(5):328–334. doi:10.5603/gpl.96712
4. Iacobone AD, Bottari F, Radice D, et al. Distribution of High-Risk human papillomavirus genotypes and multiple infections in preneoplastic and neoplastic cervical lesions of unvaccinated women: a cross-sectional study. J Low Genit Tract Dis. 2019;23(4):259–264. doi:10.1097/LGT.0000000000000487
5. Schiller JT, Day PM, Kines RC. Current understanding of the mechanism of HPV infection. Gynecol Oncol. 2010;118(1):12–17. doi:10.1016/j.ygyno.2010.04.004
6. Raff AB, Woodham AW, Raff LM, et al. The evolving field of human papillomavirus receptor research: a review of binding and entry. J Virol. 2013;87(11):6062–6072. doi:10.1128/JVI.00330-13
7. Oh HY, Kim BS, Seo SS, et al. The association of uterine cervical microbiota with an increased risk for cervical intraepithelial neoplasia in Korea. Clin Microbiol Infect. 2015;21(7):674. doi:10.1016/j.cmi.2015.02.026
8. Gillet E, Meys JF, Verstraelen H, et al. Bacterial vaginosis is associated with uterine cervical human papillomavirus infection: a meta‐analysis. BMC Infect Dis. 2011;11(1):10. doi:10.1186/1471-2334-11-10
9. Primorac D, Vrdoljak K, Brlek P, et al. Adaptive immune responses and immunity to SARS-CoV-2. Front Immunol. 2022;13:848582. doi:10.3389/fimmu.2022.848582
10. Torge D, Bernardi S, Arcangeli M, Bianchi S. Histopathological features of SARS-CoV-2 in extrapulmonary organ infection: a systematic review of literature. Pathogens. 2022;11(8):867. doi:10.3390/pathogens11080867
11. Wang W, Ma Y, Li R, Chen X, Wan L, Zhao W. Associations of cervicovaginal lactobacilli with HR-Human papillomavirus infection, cervical intraepithelial neoplasia, and cancer: a systematic review and Meta-Analysis. J Infect Dis. 2019;220(8):1243–1254. doi:10.1093/infdis/jiz325
12. King CC, Jamieson DJ, Wiener J, et al. Bacterial vaginosis and the natural history of human papillomavirus. Infect Dis Obstet Gynecol. 2011;2011:1–8. doi:10.1155/2011/319460
13. Reid G. Probiotic agents to protect the urogenital tract against infection. Am J Clin Nutri. 2001;73(2):437–443. doi:10.1093/ajcn/73.2.437s
14. Anukam KC, Osazuwa EO, Osadolor HB, Bruce AW, Reid G. Yogurt containing probiotic L. rhamnosus GR-1 and L. reuteri RC-14 helps resolve moderate diarrhea and increases CD4 Count in HIV/AIDS patients. J Clin Gastroenterol. 2008;42(3):239–243. doi:10.1097/MCG.0b013e31802c7465
15. Van Baarlen P, Troost F, Van Der Meer CG, Boekschoten M. Brummer RJM, et al. Human mucosal in vivo transcriptome responses to three lactobacilli indicate how probiotics may modulate human cellular pathways. Proc Natl Acad Sci USA. 2011;108(1):4562–4569. doi:10.1073/pnas.1000079107
16. Stanley M, Pinto LA, Trimble C. Human papillomavirus vaccines–immune responses. Vaccine. 2012;30(5):F83–7. doi:10.1016/j.vaccine.2012.04.106
17. Rose WA, McGowin CL, Spagnuolo RA, Eaves-Pyles TD, Popov VL, Pyles RB. Commensal bacteria modulate innate immune responses of vaginal epithelial cell multilayer cultures. PLoS One. 2012;7(3):32728. doi:10.1371/journal.pone.0032728
18. Dewhirst FE, Chen T, Izard J, et al. The human oral microbiome. J Bacteriol. 2010;192(19):5002–5017. doi:10.1128/JB.00542-10
19. Forestier C, De Champs C, Vatoux C, Joly B. Probiotic activities of Lactobacillus casei rhamnosus: in vitro adherence to intestinal cells and antimicrobial properties. Res Microbiol. 2001;152(2):167–173. doi:10.1016/S0923-2508(01)01188-3
20. Nayar R, Wilbur DC. The bethesda system for reporting cervical Cytology-definitions, criteria and explanatory notes.
21. Bornstein J, Bentley J, Bösze P, et al. 2011 Colposcopic terminology of the international federation for cervical pathology and colposcopy. Obstetrics Gynecol. 2012;120(1):166–172. doi:10.1097/AOG.0b013e318254f90c
22. Li J, Aroutcheva AA, Faro S, Chikindas ML. Mode of action of lactocin 160, a bacteriocin from vaginal Lactobacillus rhamnosus. Infect Dis Obstet Gynecol. 2005;13(3):135–140. doi:10.1080/10647440500148156
23. Chew SY, Cheah YK, Seow HF, Sandai D, Than LTL. Probiotic Lactobacillus rhamnosus GR ‐1 and L actobacillus reuteri RC ‐14 exhibit strong antifungal effects against vulvovaginal candidiasis‐causing C andida glabrata isolates. J Appl Microbiol. 2015;118(5):1180–1190. doi:10.1111/jam.12772
24. Ho M, Chang -Y-Y, Chang W-C, et al. Oral Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 to reduce Group B streptococcus colonization in pregnant women: a randomized controlled trial. Taiwanese J Obstetrics Gynecol. 2016;55(4):515–518. doi:10.1016/j.tjog.2016.06.003
25. Verhoeven V, Renard N, Makar A, Royen PV, Bogers J-P, Lardon F. Probiotics enhance the clearance of human papillomavirus-related cervical lesions: a prospective controlled pilot study. Eur J Cancer Prev. 2013;22(1):46–51. doi:10.1097/CEJ.0b013e328355ed23
26. Zeng M, Li X, Jiao X, et al. Roles of vaginal flora in human papillomavirus infection, virus persistence and clearance. Front Cell Infect Microbiol. 2023;12:1036869. doi:10.3389/fcimb.2022.1036869
27. Palma E, Recine N, Domenici L, Giorgini M, Pierangeli A, Panici PB. Long-term L. rhamnosus BMX 54 application to restore a balanced vaginal ecosystem: a promising solution againstHPV-infection. BMC Infect Dis. 2018;18(1):13. doi:10.1186/s12879-017-2938-z
28. Ou Y-C, Fu H-C, Tseng CW, Wu C-H, Tsai -C-C, Lin H. The influence of probiotics on genital HR-human papilloma virus clearance and quality of cervical smear: a randomized placebo-controlled trial. BMC Women’s Health. 2019;19(1):103. doi:10.1186/s12905-019-0798-y
29. Perisić Z, Perisić N, Golocorbin Kon S, Vesović D, Jovanović AM, Mikov M. The influence of probiotics on the cervical malignancy diagnostics quality. Vojnosanit Pregl. 2011;68(11):11. doi:10.2298/VSP100809001P
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vaginal Microecological Imbalance, Human Papillomavirus Infection, and Cervical Carcinogenesis: Mechanisms and Clinical Implications
Gao W, Liu Y, Wang Q, Xiao H, Wang F, Wang L
International Journal of General Medicine 2026, 19:621765
Published Date: 30 June 2026